







































































Neuro-Oncology
NF2-related schwannomatosis
Dec. 13, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The author explains the clinical presentation, pathophysiology, prevention, diagnostic workup, and management of superficial siderosis of the central nervous system. Superficial siderosis is a potentially devastating syndrome usually caused by recurrent subarachnoid hemorrhage with accumulation of hemosiderin and other iron-containing pigments in the leptomeninges, brain surface, brainstem, cerebellum, cranial nerves, and spinal cord. Superficial siderosis can mimic many other central nervous system degenerative or multifocal disorders, including amyotrophic lateral sclerosis and multiple sclerosis.
|
• Superficial siderosis is a rare and potentially devastating syndrome caused by recurrent subarachnoid hemorrhage with accumulation of hemosiderin and other iron-containing pigments in the leptomeninges, brain surface, brainstem, cerebellum, cranial nerves, and spinal cord. | |
|
• Common features include progressive sensorineural hearing loss, cerebellar ataxia, pyramidal signs (eg, spastic paraparesis, quadriparesis, etc.), ataxia, and headache. | |
|
• Superficial siderosis is caused by recurrent subarachnoid hemorrhage with dissemination of heme by circulating cerebrospinal fluid and subsequent accumulation of hemosiderin and other iron-containing pigments in the leptomeninges, brain surface, brainstem, cerebellum, cranial nerves, and spinal cord. | |
|
• The condition may be progressively disabling or fatal. Even with successful surgical resection of the causative lesion (when that is identified), significant functional recovery cannot be anticipated. However, progression generally is lessened or averted, at least in the short periods of follow-up reported. | |
|
• A wide variety of conditions may cause superficial siderosis, including various cerebral or spinal vascular abnormalities, neoplasms or other mass lesions of the brain and spinal cord or surrounding structures, trauma, and rarely some neurosurgical procedures, congenital abnormalities, and other sources of vascular damage. | |
|
• Management is directed at resection of the source of bleeding. |
Superficial siderosis is a rare and potentially devastating syndrome caused by recurrent subarachnoid hemorrhage with accumulation of hemosiderin and other iron-containing pigments in the leptomeninges, brain surface, brainstem, cerebellum, cranial nerves, and spinal cord (68). Although superficial siderosis had been produced experimentally in dogs as early as 1960 (51), superficial siderosis had been considered a rare condition, usually diagnosed postmortem, until the advent of CT and MRI in the mid-1980s (98). It is now increasingly recognized.
|
• Common clinical features of superficial siderosis include progressive sensorineural hearing loss, cerebellar ataxia, myelopathy, pyramidal signs (eg, spastic paraparesis, quadriparesis, etc.), ataxia, radiculopathy, and headache. | |
|
• The progressive sensorineural hearing loss of superficial siderosis may be the presenting or predominant symptom, may be slowly progressive over many years, and may be caused by a combination of retrocochlear and cochlear damage. | |
|
• Other clinical features of superficial siderosis seen in a minority of patients include seizures, corticobasal syndrome, cranial nerve abnormalities, spinal myoclonus, polyradiculopathy and sciatica, neck or back ache, urinary incontinence, somatosensory deficits, acute intracranial pressure crisis superimposed on chronic intracranial hypertension, and episodic encephalopathy with associated headache and vomiting. |
Common clinical features of superficial siderosis include progressive sensorineural hearing loss, cerebellar ataxia, myelopathy, pyramidal signs (eg, spastic paraparesis, quadriparesis, etc.), ataxia, radiculopathy, and headache (74; 107; 40; 52; 80; 88; 65; 142; 62; 155; 75; 92; 121; 68; 131; 12; 87; 109; 41; 45; 123).
The progressive sensorineural hearing loss may be the presenting or predominant symptom (62; 92; 121; 03), may be slowly progressive over many years (92; 121), and may be caused by a combination of retrocochlear and cochlear damage (126).
C and D are the left and right sides, respectively, of the same patient. (Source: Artukarslan E, Matin F, Donnerstag F, Gärtner L, Lenarz T, Lesinski-Schiedat A. Cochlea implantation in patients with superficial hemosiderosis. ...
Hearing loss is typically sloping and asymmetric, exceeds hearing loss expected for age and gender, and may be associated with decreased word recognition (121). Superficial siderosis should be considered in all patients presenting with progressive sensorineural hearing loss and ataxia (134). Sudden sensorineural hearing loss has also been attributed anecdotally to superficial siderosis, but whether the superficial siderosis was causal or incidental is not clear (71). Some patients develop peripheral vestibular disorders in conjunction with hearing loss with associated caloric weakness, disequilibrium, dizziness, and vertigo (140; 136; 155).
Neuropsychological disturbances are common in classical superficial siderosis (13). Neuropsychological testing has demonstrated impairments in speech production, visual recall memory, executive functions, and ability to represent other people’s mental states (135).
Other clinical features seen in a minority of patients include seizures, corticobasal syndrome, cranial nerve abnormalities, spinal myoclonus, polyradiculopathy and sciatica, neck or back ache, urinary incontinence, somatosensory deficits, acute intracranial pressure crisis superimposed on chronic intracranial hypertension, and episodic encephalopathy with associated headache and vomiting (48; 62; 155; 75; 43; 138; 68; 106; 26; 53; 08; 37; 137; 128). Cranial nerve abnormalities can include anosmia or hyposmia, anisocoria, optic neuropathy, visual field deficits, fourth nerve palsy, diplopia, nystagmus, trigeminal neuropathy, hemifacial spasm, sensorineural hearing loss, intermittent vertigo, bilateral vestibulopathy, and dysarthria (62; 70; 127; 56).
Infratentorial superficial siderosis results from recurrent or continuous bleeding into the subarachnoid space (141).
Sagittal susceptibility-weighted imaging of the spinal cord in a 73-year-old woman with a ventral dural defect at the level of the second thoracic vertebra with spontaneous intracranial hypotension and recurrent subarachnoid bl...
Causes of infratentorial superficial siderosis include spinal dural pathology resulting in CSF leakage, neurosurgical interventions, trauma, and arteriovenous malformations. Typical manifestations of infratentorial superficial siderosis include slowly progressive sensorineural hearing impairment and cerebellar symptoms (eg, ataxia), action tremor, nystagmus, and dysarthria. In contrast, cortical superficial siderosis is restricted to the supratentorial compartment and occurs especially in older people, often from cerebral amyloid angiopathy (141).
CT and MRI in a 74-year-old woman suffering from recurrent cortical subarachnoid hemorrhage in cerebral amyloid angiopathy. (a-d) The first cortical subarachnoid hemorrhage in the right frontal area on (a) axial CT (arrow) with...
Acute cortical subarachnoid hemorrhage on (b) axial FLAIR, (c) axial susceptibility-weighted, and (d) axial diffusion-weighted images (arrow). (a, e) Enlarged perivascular spaces on axial T2-weighted images (arrow). (b, f) Foca...
The clinical presentation of cortical superficial siderosis includes transient focal neurologic episodes ("amyloid spells") (141). Spontaneous and amyloid beta immunotherapy-associated microbleeding and inflammation may cause cortical superficial siderosis in cerebral amyloid angiopathy (141).
Based on the characteristic clinical syndrome of patients with infratentorial superficial siderosis and its short-term progression in case of ongoing subarachnoid hemorrhage, a clinical framework of key features has been proposed for an “acute superficial siderosis syndrome” (41).
(Source: Friedauer L, Foerch C, Steinbach J, et al. The acute superficial siderosis syndrome: clinical entity, imaging findings, and histopathology. Cerebellum 2023;22[2]:296-304. Creative Commons Attribution 4.0 International ...
A significant number of cases may be asymptomatic, possibly reflecting a milder form of disease or a presymptomatic state (48; 74; 53; 131; 37).
The prognosis is often poor. The condition may be progressively disabling or fatal. Even with successful surgical resection of the causative lesion (when that is identified), significant functional recovery cannot be anticipated. However, generally, progression is lessened or averted, at least in the short periods of follow-up reported (114).
In survivors of spontaneous symptomatic intracerebral hemorrhage related to probable or possible cerebral amyloid angiopathy, disseminated cortical superficial siderosis predicts early recurrent lobar hemorrhage (103; 19; 17; 78). The evolution of cortical superficial siderosis over time may be a useful biomarker for assessing disease progression and risk of intracerebral hemorrhage in cerebral amyloid angiopathy (20).
Cortical superficial siderosis results from fairly advanced cerebral amyloid angiopathy of the leptomeningeal vessels and may trigger secondary ischemic injury in affected areas (24). Patients with cortical superficial siderosis and suspected cerebral amyloid angiopathy are at high risk for cerebral amyloid angiopathy-related incident intracranial hemorrhage and poor functional outcome (147).
In patients with acute intracerebral hemorrhage, cortical superficial siderosis severity is an independent predictor of diffusion-weighted imaging lesions (102). In a memory clinic population, cortical superficial siderosis was related to cerebrovascular disease and may be a manifestation of severe cerebral amyloid angiopathy, even in patients without intracerebral hemorrhage (113).
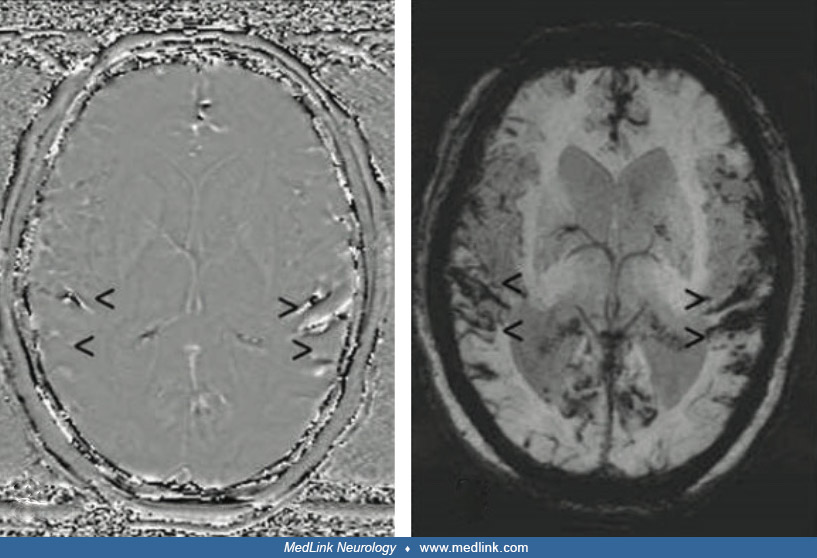
Case 1. Cervical spinal meningeal melanocytoma presenting as intracranial superficial siderosis (117). A 62-year-old man presented with difficulty walking, diffuse weakness, falls, and syncope (117). He had a 1-week history of rapidly progressive hand weakness and weakness of the limbs. There was no history of recent or remote trauma, but he had a history of subarachnoid hemorrhage 6 months before evaluation that had been managed conservatively. MRI of the brain showed mild effacement of the sulcal spaces on T1- and T2-weighted images, and there was a positive phase shift and blooming along the sulcal spaces on phase-contrast and maximum-intensity projection susceptibility-weighted images suggestive of superficial siderosis, but evident source of bleeding.
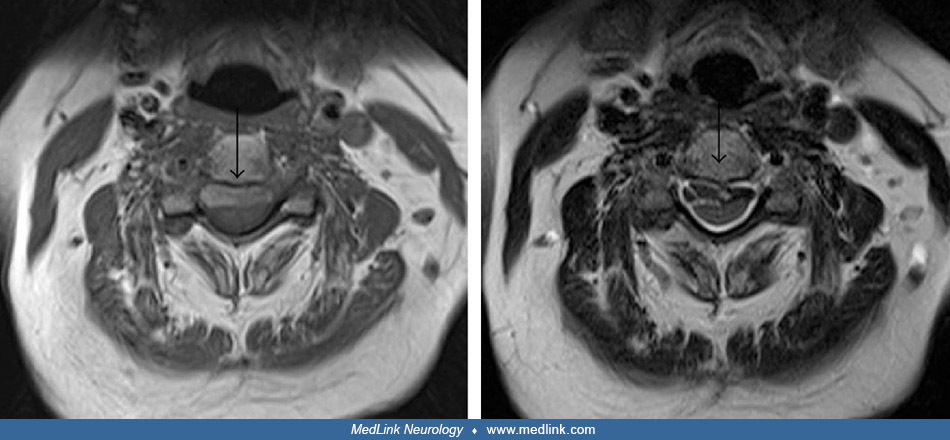
Cervical spinal MRI revealed an intradural extramedullary mass occupying the anterior intradural space, compressing and displacing the spinal cord posteriorly, with hyperintense signal on T1-weighted images and hypointense signal on T2-weighted images.
There was no clear contrast enhancement of the mass on postcontrast, fat-saturated, T1-weighted images because of strong T1 hyperintensity on the unenhanced images, but mild heterogeneous peripheral enhancement of the mass was seen on the subtracted images.
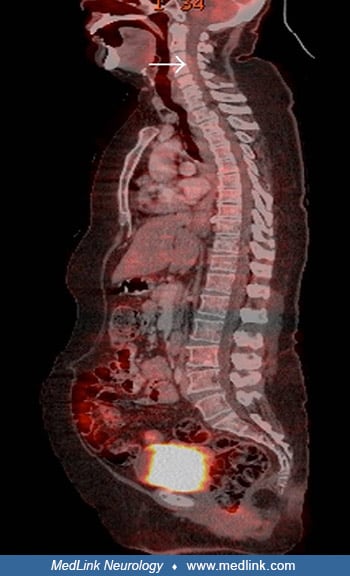
Sagittal PET-CT images showed a moderately fluorodeoxyglucose-avid, extramedullary, intradural mass with no other foci of fluorodeoxyglucose avidity elsewhere.
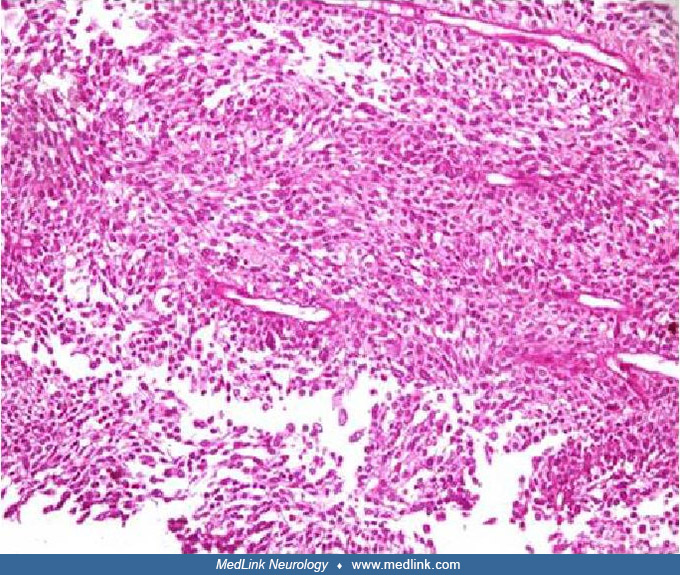
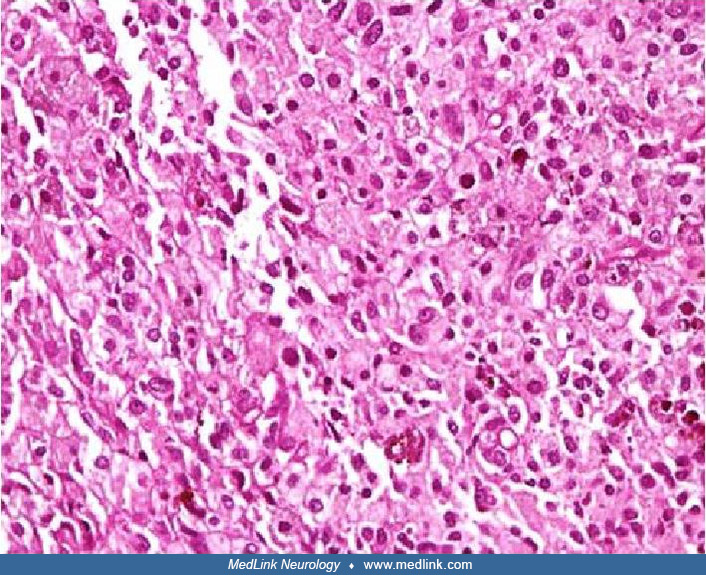
The patient underwent C3-C5 laminectomy with excision of a firm, smooth-surfaced, and blackish-colored intradural extramedullary mass lesion. Histopathological examination showed a diffusely pigmented tumor with a peritheliomatous arrangement of cells (ie, tumor cells around blood vessels with necrosis of tumor cells further away from vessels), which obscured the cytological details.
After bleaching, the tumor cells had pleomorphic, round-to-oval nuclei with inconspicuous nucleoli and a moderate amount of cytoplasm.
On higher magnification, the tumor cells had mild nuclear pleomorphism and moderate-to-abundant cytoplasm, with occasional cells containing a blackish-brown pigment. No significant increase in mitosis was evident.
On immunostaining with Ki-67 (the Ki-67 protein, also known as MKI67, which is a cellular marker for proliferation), the tumor had a low proliferation index (less than 1%), which is characteristic of melanocytomas. Subsequent careful examination of the skin and the fundus of the eye did not reveal any melanotic lesions. Therefore, the tumor was considered a primary melanocytoma of the cervical spine. The patient improved symptomatically in the postoperative period.
Case 2. Superficial siderosis after parietal meningioma and myxopapillary ependymoma (12). A 61-year-old man reported a 12-year history of progressive unsteady gait, accompanied by progressive limb weakness and muscle wasting (proximal more than distal, lower more than upper limbs), cramping in the legs, general clumsiness, and fine motor impairment. He walked only with a walker and was unable to climb stairs. His medical history included the removal of a left parietal meningioma (WHO Grade I) and successful resection of a myxopapillary ependymoma (WHO Grade I) near the conus terminalis (L3/4) at age 51 years.
Perioperative neurologic evaluation identified a spastic ataxic gait. He experienced progressive motor and gait dysfunction over the subsequent years. Clinical examination around age 61 revealed bilateral wasting of abductor pollicis brevis, first dorsal interosseous, and abductor digiti minimi muscles as well as bilateral atrophy of the shoulder and calf muscles. Manual muscle strength tests showed weakness (MRC 4) in the hand interossei and hip flexors and more severe weakness (MRC 3) in the plantar flexors and dorsiflexors of the feet. Muscle stretch reflexes were symmetrically brisk in the arms and legs with spread, but plantar responses were reportedly normal. Sensory examination showed a reduced vibration sense at both medial malleoli. Standing and walking were only possible with support. He had a wide-based gait. Neuropsychological examination showed mild cognitive impairment affecting multiple domains (memory, language, attention, and visual-spatial function).
Electrodiagnostic testing showed a normal sensory nerve conduction of the median, ulnar, and sural nerves. Motor nerve conduction studies suggested a reduced compound muscle action potential amplitude in the peroneal and tibial nerves without conduction block. The F-wave latencies of the median, ulnar, peroneal, and tibial nerves were normal. Needle electromyography of the extensor digitorum communis, tibialis anterior, and vastus lateralis muscles demonstrated a few fibrillation potentials and a prolonged motor unit potential duration. Thoracic paraspinal and deltoideus muscles had no spontaneous activity. Transcranial magnetic stimulation showed prolonged central motor conduction times in both the abductor digiti minimi and tibialis anterior muscles.
MRI of the entire neuroaxis was performed twice in a 10-year span, showing slowly progressive cerebral and spinal superficial siderosis,
Specifically, the follow-up brain MRI in 2019 demonstrated progressive basal, intraventricular, and superficial siderosis affecting the entire CNS in the form of extensive hypointensities on T2-weighted gradient-echo images, fluid-attenuated inversion recovery (FLAIR), and susceptibility-weighted imaging (SWI) sequences. The hemosiderosis in the brain and spinal cord was severe and far more pronounced than in 2010. No intraspinal fluid-filled collections were found. Digital subtraction angiography disclosed no evidence of further vascular pathology or the source of the bleeding.
Two years after disease onset, CSF was normal without signs of bleeding or elevated CSF ferritin.
The patient was discharged and treated with the chelating agent deferiprone (750 mg three times daily), but this produced no significant effects on the clinical evolution over 1 year of treatment.
Case 3. Acute superficial siderosis syndrome (41). A 61-year-old man was diagnosed with malignant melanoma with pulmonary metastasis at age 58. At age 59, during a pause from checkpoint inhibitor therapy (ipilimumab and nivolumab) due to medication-induced autoimmune pneumonitis, he developed four cerebral metastases, which were treated by a single session of radiosurgery. The reinitiated maintenance therapy with nivolumab resulted in complete remission, and three of the cerebral metastases resolved after radiosurgery, but the right frontal lobe metastasis underwent a post-therapeutic pseudoprogression. Two months later, he was hospitalized for a first generalized tonic-clonic seizure. Cerebral MRI showed a cerebral hemorrhage localizing around the right frontal metastasis, and a follow-up MRI 3 months later showed cystic transformation of the metastasis with an intratumoral hemorrhage. One month later, he presented with executive dysfunction and a subtle paresis of the left arm with minor spasticity, which were considered a consequence of metastasis progression in the right frontal cortex. Pronounced gait ataxia limited his walking distance to approximately 50 meters.
MRI identified both acute and subacute hemorrhages in the subarachnoid space and the right lateral ventricle, indicating repetitive or continuous metastatic bleeding. In addition, progressive superficial siderosis coating large parts of the brain (with an infratentorial and temporal focus) and the spinal cord was detected. Siderosis became visible on susceptibility-weighted imaging as hypointense (“black-appearing”) coating of increasing thickness within the ventricles and on the brain surface. Although the distribution was generally symmetric, an accentuation on the top of the cerebellum and around the brainstem was apparent.
Sequential transverse susceptibility-weighted imaging (SWI) of the cerebrum acquired over a 64-day period. The progression of the superficial sideroses is visible as a black coating of the brain surface most pronounced on the t...
Sequential transverse susceptibility-weighted imaging (SWI) of the brain at the level of the pons, 4th ventricle, and cerebellum that was acquired over a 64-day period. The progression of the superficial sideroses is visible as...
Sequential transverse susceptibility-weighted imaging (SWI) of the brain at the level of the medulla and cerebellum that were acquired over a 64-day period. The progression of the superficial sideroses is visible as a black coa...
MRI of the spine further substantiated the extent of the bleeding, showing superficial siderosis of the spinal cord, marked clouding of the CSF, and sedimentation of blood products in the lumbar spinal canal.
Lumbar puncture confirmed the presence of large amounts of blood in the CSF. Because asymptomatic diffusion-weighted imaging lesions were detected with cranial MRI, checkpoint inhibitor therapy-associated vasculitis was considered and may have contributed to increased metastatic bleeding. The presumed vasculitis was treated with high-dose cortisone and infliximab. Subsequent pathological examination could not confirm the presence of vasculitis with certainty. Following in-hospital rehabilitation, he was discharged home, but only 6 weeks later he became wheelchair-bound due to progressive gait disturbance.
After surgical removal of the hemorrhagic melanoma metastasis, histopathological analysis depicted iron deposits covering the superficial layer of the cortex as well as hemosiderin deposits in the molecular layer of the cortex.
Superficial cortical tissue from the right frontal lobe (Perls Prussian blue stain). Covering the superficial layers of the cortex, ribbon-like iron deposits are appreciable (arrowheads). (Source: Friedauer L, Foerch C, Steinba...
Combined with the reactive astrocytes and the CD68-positive macrophages in the superficial layer of the cortex as signs of astrogliosis and immune response, these findings are consistent with iron toxicity and the diagnosis of a recently developed superficial siderosis.
Superficial cortical tissue from the right frontal lobe (GFAP immunohistochemistry). Within the superficial cortex area, iron deposits are accompanied by reactive astrocytes (arrowheads). (Source: Friedauer L, Foerch C, Steinba...
Superficial cortical tissue from the right frontal lobe (CD68 immunohistochemistry). Superficially located within the cortex, CD68-positive macrophages can be observed (arrowheads). (Source: Friedauer L, Foerch C, Steinbach J, ...
Case 4. Superficial siderosis due to an occult spinal dural defect (45). A 31-year-old man consulted an otolaryngologist with an 18-month history of progressive bilateral hearing loss, distressing tinnitus, and imbalance. He had a background in boxing and rugby but no history of major injuries. Pure-tone thresholds showed profound hearing loss above 500 Hz; acoustic reflexes were absent, and he had profound impairment of speech discrimination.
The first (shown in green) and last (shown in brown) pure-tone audiograms. Legend: left ear (x) and right ear (o). (Source: Halmagyi GM, Parker GD, Chen L, et al. Progressive loss of hearing and balance in superficial siderosis...
MRI was reportedly normal, but later review (at age 40) showed that there was, in fact, evidence of superficial siderosis. He declined a cochlear implant because he was concerned about possible aggravation of his tinnitus.
At age 40, he consulted a neurologist because of progressively deteriorating balance. He had no postural headache or other symptoms of intracranial hypotension. On examination, he had anosmia and profound hearing impairment. He had direction-changing, gaze-evoked, horizontal nystagmus, a bidirectionally positive horizontal and vertical clinical head impulse test, impaired smooth pursuit and visually enhanced vestibulo-ocular reflex (VOR), lower limb and gait ataxia, brisk lower limb muscle stretch reflexes, extensor plantar reflexes, and a Romberg sign on foam. The VOR from all six semicircular canals was severely impaired on video head impulse testing.
Brain MRI showed widespread superficial siderosis, especially in the posterior fossa, but no changes in intracranial hypotension.
Spine MRI showed an epidural CSF collection from T2 to T8 and a T5/6 disc protrusion with a large osteophyte impinging on the dura, whereas a dynamic CT myelogram via lumbar puncture suggested that the CSF leak was at this level.
CSF was xanthochromic, containing 4000 red cells and one white cell per milliliter and protein 0.93 g/L (normal < 0.45).
At laminectomy, the dural defect found slightly rostral to the bony spur was repaired via an intradural approach. The spinal cord was noted to be xanthochromic.
Dorsolateral view of spinal cord after laminectomy and opening of dura--rotated up to show the ventral dural defect. Legend: A. branch of anterior spinal artery; B. rostral and caudal margins of ventral dural defect with anteri...
Unfortunately, there was no improvement in his hearing or balance 8 years after surgery.
Case 5. Superficial siderosis with spinal dural defect (76). A 55-year-old man who worked as a builder presented with a 15-year history of progressive bilateral sensorineural hearing loss and a 4-year history of gait ataxia. His background included mild head trauma from a cycling accident at age twelve and a severe blunt-force injury to the thoracic spine 8 years prior to presentation. He had brisk reflexes throughout with down-going plantar reflexes and marked gait ataxia. Sensory examination was intact.
MRI demonstrated extensive siderosis affecting both cerebral and cerebellar hemispheres. Spine MRI with contrast demonstrated a ventral cervicothoracic epidural collection.
Sagittal spine T2-weighted SPC MRI revealed a large ventral epidural fluid collection extending from C3 to L3. (Source: Lobo R, Batbayar B, Kharytaniuk N, et al. Targeted detection and repair of a spinal dural defect associated...
The retro-odontoid venous plexus was prominent below C1, suggestive of a CSF leak. No vascular abnormality was identified. Standard and dynamic CT myelography did not identify the exact location of the CSF leak. However, reverse CT myelography involving direct contrast injection into the collection demonstrated a ventral dural defect at T9/10.
Subsequent tracking of contrast to the right posterior thoracic cord delineating the site of the dural defect, T9-10. (Source: Lobo R, Batbayar B, Kharytaniuk N, et al. Targeted detection and repair of a spinal dural defect ass...
Postoperative resolution of the large ventral epidural fluid collection. (Source: Lobo R, Batbayar B, Kharytaniuk N, et al. Targeted detection and repair of a spinal dural defect associated with successful biochemical resolutio...
Lumbar puncture revealed a CSF ferritin of 413 ng/mL and a red cell count of 4160.
Given the marked continued clinical progression and biochemical evidence of ongoing bleeding into the subarachnoid space, he underwent a T8-10 laminectomy with intradural repair of a ventral T9-10 dural defect. Intraoperatively, the leak was identified secondary to prolapse of arachnoid through a ventral dural defect between the right T9 and T10 exiting nerve roots.
Postoperative imaging performed at 6 months demonstrated resolution of the epidural collection with stable intracranial siderosis.
Reverse dynamic CT myelogram demonstrating contrast injection into the ventral epidural collection. (Source: Lobo R, Batbayar B, Kharytaniuk N, et al. Targeted detection and repair of a spinal dural defect associated with succe...
Twelve months later, on lumbar puncture, CSF ferritin had declined to a near-normal value of 18 ng/mL, and CSF red blood cells were absent. Eighteen months after surgery, his ataxia remained stable, and there had been no further progression in his other neurologic symptoms.
|
• Superficial siderosis is caused by recurrent subarachnoid hemorrhage with dissemination of heme by circulating cerebrospinal fluid and subsequent accumulation of hemosiderin and other iron-containing pigments in the leptomeninges, brain surface, brainstem, cerebellum, cranial nerves, and spinal cord. | |
|
• Cerebral amyloid angiopathy patients, who are prone to develop superficial siderosis, may prove to be a useful subgroup in whom to explore pathogenetic mechanisms for superficial siderosis. |
Superficial siderosis is caused by recurrent subarachnoid hemorrhage with dissemination of heme by circulating cerebrospinal fluid and subsequent accumulation of hemosiderin and other iron-containing pigments in the leptomeninges, brain surface, brainstem, cerebellum, cranial nerves, and spinal cord along with astrogliosis (60; 41). Hemosiderin may be intracellular or extracellular. Large mononuclear phagocytes containing hemosiderin granules (ie, siderophages) can be demonstrated pathologically. Histologic sections demonstrate severe damage to the eighth cranial nerve and cerebellum (59; 97; 60), presumably from preferential deposition from glial catabolism of ferritin within these structures (34). In the cerebellum, Bergmann glia and abundant microglia synthesize heme-oxygenase-1 and ferritin in response to heme (60). Hearing loss can be caused by degeneration of spiral ganglion cells (92). Localized deposition of hemosiderin in the cortex may produce specific cognitive impairments and hallucinations, depending on the location and severity of deposition (130).
Patients with cerebral amyloid angiopathy are prone to develop superficial siderosis (22; 14; 116; 07; 63; 82; 91; 14; 28; 103; 18; 04). In cerebral amyloid angiopathy, the multifocality of cortical superficial siderosis correlates with disease severity, suggesting that cortical superficial siderosis is caused by discrete hemorrhagic foci (18). In addition, MRI-visible centrum semiovale perivascular spaces are highly prevalent and are associated with cortical superficial siderosis, although the basis of this association has not been established (22); MRI-visible centrum semiovale perivascular spaces are a potential biomarker of impaired interstitial fluid drainage in sporadic cerebral amyloid angiopathy, and it is possible that severe leptomeningeal and cortical vascular amyloid is related to impaired interstitial fluid drainage from cerebral white matter, and the subsequent development of superficial siderosis (22). In addition, superficial siderosis is inversely associated with counts of cerebral microbleeds and with the APOE ε2 genotype (whereas cerebral microbleeds are associated with the APOE ε4 genotypes) (116); these results suggest that cerebral amyloid angiopathy-related superficial siderosis and cerebral microbleeds may arise from distinct vasculopathic mechanisms (116). There is a strong local relationship between cortical iron deposits and reactive astrocytes in cortical superficial siderosis due to cerebral amyloid angiopathy; iron deposits and reactive astrocytes are mainly found in the most superficial layers of the cortex, and iron is present within both astrocytes and activated microglia and macrophages (04).
(Source: Auger CA, Perosa V, Greenberg SM, van Veluw SJ, Kozberg MG. Cortical superficial siderosis is associated with reactive astrogliosis in cerebral amyloid angiopathy. J Neuroinflammation 2023;20[1]:195. Creative Commons A...
Bleeding from the epidural venous plexus may cause superficial siderosis associated with ventral dural defects (125; 151), presumably CSF leaks into the epidural space through the ventral dural defect, and repetitive bleeding occurs from the epidural vessels that connect back to the subarachnoid space through the dural defect, leading to hemosiderin deposition on the surface of the brain, the central nerves, and the spinal cord.
|
• Almost all reported cases of superficial siderosis have been single case reports or small case series. | |
|
• Little is known about the epidemiology of the condition, although it is being increasingly recognized by MRI. | |
|
• The prevalence of superficial siderosis is higher in a memory disorders clinic population than reported in the general population. | |
|
• The presence of superficial siderosis has been associated with lower cognitive scores, microbleeds, white matter hyperintensities, and APOE ε4, independent of diagnosis. |
Almost all reported cases of superficial siderosis have been reported as single case reports or small case series. Little is known about the epidemiology of the condition, although it is being increasingly recognized by magnetic resonance imaging.
The prevalence of superficial siderosis is higher in a memory disorders clinic population than reported in the general population (156). There is an increased prevalence of dementia in patients with preexisting cortical superficial siderosis (154). Down syndrome patients also have a significantly higher mean microbleed count and greater likelihood of superficial siderosis than age-matched controls (112). Superficial siderosis occurs in approximately 6% to 40% of those with cerebral amyloid angiopathy (21; 146), compared with nearly 5% of those with Alzheimer disease, 2.5% of those with other types of dementia, 2% of those with mild cognitive impairment, and in less than 1% of those with subjective memory complaints or other disorders (156). In a clinical series of 41 patients with bilateral vestibulopathy, superficial siderosis was identified as the cause in three (7%) (55). The presence of superficial siderosis has been associated with lower cognitive scores, microbleeds, white matter hyperintensities, and APOE ε4, independent of diagnosis (146; 156), although not all studies agree (25).
A synthetic study that combined Framingham (n=1724; 2000 to 2009) and Rotterdam (n=4325; 2005 to 2013) study participants who underwent brain MRI, a total of 6049 participants were identified, of whom 401 (7%) had deep/mixed microbleeds, 776 (13%) had lobar microbleeds without cortical superficial siderosis, and 26 (0.4%) had cortical superficial siderosis with/without microbleeds (115). Participants with cortical superficial siderosis were older, had overrepresentation of the APOE ɛ4 allele, and greater prevalence of intracerebral hemorrhage. During a mean follow-up of 5.6 years, 42% of those with cortical superficial siderosis had a stroke, 19% had transient neurologic deficits, and 4% developed incident dementia.
There are often long delays between symptom onset and definitive diagnosis of superficial siderosis (43). Superficial siderosis can mimic many other central nervous system degenerative or multifocal disorders. For example, cases have been reported that have been confused with amyotrophic lateral sclerosis (with slowly progressive weakness, fasciculations, and hyperreflexia) (35) and multiple sclerosis (with oligoclonal bands in some cases) (96).
There are often long delays between symptom onset and definitive diagnosis of superficial siderosis (43). Superficial siderosis can mimic many other central nervous system degenerative or multifocal disorders. For example, cases have been reported that have been confused with amyotrophic lateral sclerosis (with slowly progressive weakness, fasciculations, and hyperreflexia) (35) and multiple sclerosis (with oligoclonal bands in some cases) (96). Cortical vein thrombosis is another possible mimic of cortical superficial siderosis (141).
MRI in a 27-year-old woman with right-sided headache and sensory Jacksonian seizures demonstrates a hyperintense cortical lesion in the right postcentral parietal area on (a) axial T2-weighted and (b) axial FLAIR images (arrow)...
A wide variety of conditions may cause superficial siderosis, including the following (05; 22; 54; 68; 106; 116; 150; 07; 63; 82; 91; 139; 06; 14; 31; 32; 84; 93; 149; 124; 10; 85; 01; 153; 95; 39; 76; 77; 78; 87; 104; 109; 151; 46; 111):
|
Cerebral or spinal vascular abnormalities | |
|
• Cerebral or spinal arteriovenous malformation | |
|
Neoplasms or other mass lesions | |
|
• Spinal pilocytic astrocytoma | |
|
Trauma | |
|
• Chronic subdural hematoma | |
|
Postsurgical | |
|
• Ventriculoperitoneal shunt placement | |
|
Other sources of vascular damage | |
|
• Hereditary transthyretin-related amyloidosis | |
According to Lee and colleagues, superficial siderosis should also be considered in cases of rapidly progressive hearing loss occurring over weeks (69); the following table was modified by Dr. Douglas Lanska using information from Lee’s study.
|
• Intracranial (noninfectious) | ||
|
- superficial siderosis | ||
|
• Paraneoplastic syndrome | ||
|
- small cell lung carcinoma | ||
|
• Inflammatory or autoimmune disorders | ||
|
- autoimmune inner-ear disease | ||
|
• Infectious disorders | ||
|
- meningitis | ||
|
• Medication-induced causes | ||
|
| ||
Despite thorough evaluation (eg, with MRI, CT, angiography, and myelography), no cause is identified in a significant fraction of cases (62; 27).
|
• Superficial siderosis should be suspected in patients with progressive sensorineural hearing loss, ataxia, and pyramidal dysfunction. | |
|
• A thorough evaluation is needed when superficial siderosis is suspected to localize the source of bleeding. MRI is the most important diagnostic study, in conjunction with lumbar puncture and selective use of angiography. | |
|
• MRI studies demonstrate hemosiderin deposition along the superficial surfaces of the brain, brainstem, cerebellum, and spinal cord. Hypointense rims around the brain, brainstem, cerebellum, cranial nerves, or spinal cord are commonly seen on T2-weighted images, and hyperintense rims may be demonstrated on T1-weighted images. | |
|
• CT may show widespread meningeal enhancement or cerebellar atrophy. | |
|
• Although CT may suggest the diagnosis of superficial siderosis, MRI is more sensitive and specific. | |
|
• Cortical superficial siderosis in combination with other small vessel disease imaging markers is highly indicative of cerebral amyloid angiopathy. | |
|
• When superficial siderosis is diagnosed on brain imaging and no source is identified, spinal imaging is essential. Dural diverticula, pseudomeningoceles, and other dural defects (including transdural leaks) are usually best shown on myelography or CT myelography. The location of a dural defect associated with longitudinally extensive intraspinal collections may be best localized by dynamic CT myelography. | |
|
• Lumbar puncture may demonstrate recurrent or persistent xanthochromia, red cells, a slightly elevated white cell count, increased protein, increased iron and ferritin levels in the cerebrospinal fluid, and siderophages. |
Superficial siderosis should be suspected in patients with progressive sensorineural hearing loss, ataxia, and pyramidal dysfunction (27). A long asymptomatic phase and the lack of a predictive relationship between the duration and severity of hearing loss impede use of audiometry to diagnose superficial siderosis (122). However, asymmetric hearing loss exceeding expectations, particularly with a history of head trauma or a previous neurosurgical procedure, should raise suspicion for the disorder. Nevertheless, superficial siderosis may be misdiagnosed as idiopathic or age-associated bilateral sensorineural deafness (44).
A thorough evaluation is needed when superficial siderosis is suspected to localize the source of bleeding. MRI is the most important diagnostic study, in conjunction with lumbar puncture and selective use of angiography. Although used in the past (143), there is little role for brain biopsy any longer to diagnose this condition. Nevertheless, even with thorough diagnostic evaluation, the source of bleeding remains unidentified in many cases (89; 62).
Neuroimaging. CT may show widespread meningeal enhancement or cerebellar atrophy (98; 118) and can show dural tears and disc protrusions (09). Although CT may suggest the diagnosis of superficial siderosis, MRI is more sensitive and specific (118; 62).
MRI studies demonstrate hemosiderin deposition along the superficial surfaces of the brain, brainstem, cerebellum, and spinal cord (62; 36). Hypointense rims around the brain, brainstem, cerebellum, cranial nerves, or spinal cord are commonly seen on T2-weighted images, and hyperintense rims may be demonstrated on T1-weighted images (118; 100; 133; 67; 40; 80; 62). However, clinical symptoms may precede the development of cortical superficial siderosis prior to it being detectable on brain MRI (02).
Comparison of axial MRI on days 0 and 14 in a 74-year-old, right-handed man, with no past medical history or vascular comorbidities and no prior head trauma, who presented with sudden left arm weakness, paresthesias, word-findi...
Comparison of axial MRI on days 0 and 14 in a 74-year-old, right-handed man, with no past medical history or vascular comorbidities and no prior head trauma, who presented with sudden left arm weakness, paresthesias, word-findi...
Various MRI sequences can contribute to the detection of superficial siderosis (141).
MRI sequences from a 61-year-old man with superficial siderosis due to ongoing hemorrhage from a melanoma metastasis in the right frontal cortex. In T2*-GRE (f) and susceptibility-weighted imaging (b, g), superficial siderosis ...
In T2*-GRE (multiecho gradient recalled echo T2*-weighted imaging) (129) and susceptibility-weighted imaging, superficial siderosis is revealed by dark rims on the surface of affected structures, with susceptibility-weighted imaging being more sensitive. Minimum intensity projections of susceptibility-weighted images can further enhance the conspicuousness of superficial siderosis. In addition, filtered phase images of susceptibility-weighted imaging can distinguish paramagnetic (hemorrhage or iron appears dark) from diamagnetic substances (calcification appears bright) as they have opposite signal intensities. In general, susceptibility effects are more pronounced on images acquired at 3T than on images acquired at 1.5T.
Axial T2-weighted MRI indicates siderosis of the cranial nerves VII, VIII, and IX from their pontine emergence up to the entry in the inner auditory canal (white arrows) and the cerebellar cortex (white arrowheads). (Source: Ar...
Axial T2-weighted MRI indicates siderosis of the quadrigeminal plate (double white arrows) and the upper cerebral vermis (white arrowheads) with sparing of the cortex of both temporal lobes (curved white). (Source: Artukarslan ...
Typical MRI findings in superficial intraventricular surface siderosis. T2-weighted axial image shows hemosiderin deposits along the cerebellar peduncles, around the fourth ventricle (green arrow). (Source: Harizi E, Shemsi K, ...
Typical MRI findings in superficial intraventricular surface siderosis. T2-weighted axial image shows hemosiderin deposits around the mesencephalon) (blue arrow). (Source: Harizi E, Shemsi K, Ahmetgjekaj I, et al. Superficial i...
Typical MRI findings in superficial intraventricular surface siderosis. T2-weighted gradient echo (GRE) image shows hemosiderin deposits along the peripontine cistern, pons, aqueduct of Sylvius, tentorium, temporal horn of the ...
Typical MRI findings in superficial intraventricular surface siderosis. T2-weighted gradient echo (GRE) image shows hemosiderin deposits along the mesencephalon, suprasellar pons cistern (white arrow). (Source: Harizi E, Shemsi...
Typical MRI findings in superficial intraventricular surface siderosis. T2-weighted gradient echo (GRE) image shows hemosiderin deposits along the third ventricle (yellow arrow). (Source: Harizi E, Shemsi K, Ahmetgjekaj I, et a...
Typical MRI findings in superficial intraventricular surface siderosis. T2-weighted gradient echo (GRE) image shows hemosiderin deposits along the frontal horns (black arrow). (Source: Harizi E, Shemsi K, Ahmetgjekaj I, et al. ...
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Noncontrast sagittal 3D T1 MRI shows superior cerebellar atrophy (yellow crooked arrow). (Source: Bonomo G, Cusin A, Rubiu E, et al. Diagnost...
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Noncontrast coronal T2 Fluid-attenuated inversion recovery (FLAIR) image shows superior cerebellar atrophy (yellow crooked arrow). (Source: B...
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Noncontrast axial TSE T2 image shows superior cerebellar atrophy (yellow crooked arrow) associated with infratentorial diffuse superficial si...
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Noncontrast gradient echo (GRE) image shows superior cerebellar atrophy (yellow crooked arrow) associated with infratentorial diffuse superfi...
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Noncontrast susceptibility-weighted image (SWI) shows superior cerebellar atrophy (yellow crooked arrow) associated with infratentorial diffu...
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Apparent diffusion coefficient (ADC) image shows superior cerebellar atrophy (yellow crooked arrow) associated with infratentorial diffuse su...
Supratentorial superficial siderosis (yellow arrowhead) along the interhemispheric and Sylvian fissures and within temporal and occipital sulci is well demonstrated by the axial susceptibility-weighted (SW) sequence. (Source: B...
A temporal bone MRI protocol including 3D-constructive interference in steady state (3D-CISS) and susceptibility-weighted imaging (SWI) may be helpful in patients with sensorineural deafness or vestibular deficits and ataxia due to superficial siderosis (137). In cerebral amyloid angiopathy, cortical superficial siderosis on MRI corresponds to accumulated iron-positive deposits in the superficial cortical layers, representing the chronic manifestation of prior bleeding episodes from leptomeningeal vessels (24).
MRI studies can also demonstrate underlying pathology, such as disk protrusions, dural tears, and epidural fluid collection (09).
MRI in a 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Noncontrast sagittal constructive interference in steady state (CISS) MRI of the cervical and upper thoracic spine shows an anterior w...
MRI in a 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Sagittal turbo-spin echo (TSE) T2 MRI of the cervical and upper thoracic spine shows an anterior wedge degenerative deformation of the...
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Axial turbo-spin echo (TSE) T2 MRI through the T6-T7 disc shows a dural defect just to the right of midline at the level of the spur and furt...
MRI in a 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Sagittal T1-weighted MRI of the cervical and upper thoracic spine shows an anterior wedge degenerative deformation of the T6 vertebral...
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Axial T1-weighted MRI through the T6-T7 disc shows a dural defect just to the right of midline at the level of the spur and further delineate...
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Sagittal gradient echo (GRE) T2 MRI of the thoracic spine shows extensive superficial siderosis around the spinal cord, from below a dural de...
Cortical superficial siderosis in combination with other small vessel disease imaging markers is highly indicative of cerebral amyloid angiopathy; in contrast, cortical superficial siderosis is absent in CADASIL, whereas other small vessel disease imaging features are similar to those of cerebral amyloid angiopathy patients with cortical superficial siderosis (145). In a meta-analysis, the most frequently reported CT features of cerebral amyloid angiopathy-associated intracerebral hemorrhage were subarachnoid extension and an irregular intracerebral hemorrhage border (108). Acute convexity subarachnoid hemorrhage in association with radiologic evidence of cortical superficial siderosis is likely due to cerebral amyloid angiopathy without lobar hemorrhage (15; 101). Cerebral amyloid angiopathy-associated intracerebral hemorrhage was more likely to be multiple on CT than noncerebral amyloid angiopathy-associated intracerebral hemorrhage (108). Superficial siderosis on MRI was present in about half (52%) of cerebral amyloid angiopathy-associated intracerebral hemorrhage (108). In patients with cerebral amyloid angiopathy, the presence and extent of cortical superficial siderosis are the most important MRI prognostic risk factors for future intracerebral hemorrhage (16). Cortical superficial siderosis evolution on MRI is common in patients with symptomatic cerebral amyloid angiopathy (99).
Cerebellar superficial siderosis is also common in cerebral amyloid angiopathy and is present in approximately 10% of cases (58).
In a prospective observational cohort study of spontaneous intracerebral hemorrhage, clinical and radiologic markers associated with cortical superficial siderosis were predictive of underlying cerebral amyloid angiopathy (90). Clinical factors independently associated with the presence of cortical superficial siderosis included increasing age, preexisting dementia, and history of intracerebral hemorrhage. Among radiologic biomarkers, factors independently associated with the presence of cortical superficial siderosis were lobar location of intracerebral hemorrhage, severe white matter hyperintensities, and absence of lacunes. During a median follow-up of 6 years, only the presence of disseminated cortical superficial siderosis was associated with recurrent symptomatic intracerebral hemorrhage.
When superficial siderosis is diagnosed on brain imaging and no source is identified, spinal imaging is essential (72; 43). Dural diverticula, pseudomeningoceles, and other dural defects (including transdural leaks) are usually best shown on myelography or CT myelography but can be demonstrated on MRI (62; 144; 141). The location of a dural defect associated with longitudinally extensive intraspinal collections may be best localized by dynamic CT myelography (62).
Superficial siderosis of the spinal cord on sagittal T2*-weighted images (arrows) in a 59-year-old man suffering from progressive gait ataxia within 6 months and traumatic nerve root injury C7 and C8 30 years previously. (Sourc...
Enlarged empty nerve root pouches (arrows) on the left at C7 and C8 on sagittal T2*-weighted MRI in a 59-year-old man suffering from progressive gait ataxia within 6 months and traumatic nerve root injury C7 and C8 30 years pre...
Enlarged empty nerve root pouches (arrows) in the lower cervical area on the left on sagittal T2*-weighted MRI in a 59-year-old man suffering from progressive gait ataxia within 6 months and traumatic nerve root injury C7 and C...
Axial post-contrast T1-weighted MRI in the lower cervical area showing inhomogeneous contrast enhancement (arrow) in a 59-year-old man suffering from progressive gait ataxia within 6 months and traumatic nerve root injury C7 an...
Persisting spinal dural CSF leaks can frequently be identified in patients with a symmetric infratentorial siderosis pattern. Evaluation of such cases should include MRI of the whole spine. A retrospective analysis of 93 adult cases of superficial siderosis at a tertiary medical center from 2007 to 2018 included 42 patients with isolated supratentorial siderosis, 30 with symmetric infratentorial siderosis, and 21 with limited (asymmetric) infratentorial siderosis (42). Amyloid angiopathy and subarachnoid hemorrhage were identified as causes for isolated supratentorial siderosis. Spinal dural abnormalities were detected in all four cases with a symmetric infratentorial siderosis pattern without a history of a causative intracranial bleeding event sufficient to explain the siderosis. When the evaluation algorithm was modified to search for spinal dural leaks in cases of symmetric infratentorial siderosis either (1) without an intracranial bleeding event sufficient to explain the siderosis or additional (2) with a history of intracranial bleeding event without known bleeding etiology (spinal dural CSF leaks may also cause intracranial hemorrhage), one additional spinal dural leak was detected among the eight cases in this combined group.
Lumbar puncture. Lumbar puncture may demonstrate recurrent or persistent xanthochromia, red cells, a slightly elevated white cell count, increased protein, increased iron and ferritin levels in the cerebrospinal fluid, and siderophages (ie, hemosiderin-containing macrophages) (118; 143; 83; 62; 62; 46; 141). However, because of intermittent bleeding in small amounts, CSF may be normal (62).
CSF is from a 73-year-old woman with a ventral dural defect at the level of the second thoracic vertebra with spontaneous intracranial hypotension and recurrent subarachnoid bleeding over more than 10 years. (Source: Weidauer S...
Microscopic examination of CSF in a 59-year-old man suffering from progressive gait ataxia within 6 months and traumatic nerve root injury C7 and C8 30 years previously. (Source: Weidauer S, Neuhaus E, Hattingen E. Cerebral sup...
Angiography. Angiography may reveal various vascular malformations (48). In some cases, vascular malformations identified on angiography were not identified with MRI or myelography. In many cases, angiography also does not identify the source of bleeding, probably because of the small volume of ongoing, intermittent blood leakage (64; 62; 62; 144).
|
• Management is directed at resection of the source of bleeding. | |
|
• Despite the retrocochlear nature of the disorder, bilateral profound hearing loss from superficial siderosis is not an absolute contraindication for cochlear implants. | |
|
• Pharmacotherapy with iron-chelation therapy is not of demonstrated effectiveness, nor is shunting of cerebrospinal fluid or corticosteroid therapy. |
Management is directed at resection of the source of bleeding (118; 73; 62; 61; 114; 43; 68; 109; 79).
A 69-year-old woman with slowly progressive gait disturbances and hearing impairment. Sagittal gradient echo (GRE) T2 MRI of the thoracic spine shows extensive superficial siderosis around the spinal cord, from below a dural de...
Superficial siderosis can arise as a complication of spontaneous intracranial hypotension although it has been assumed that superficial siderosis can arise only in the context of long-term persistent, ongoing, CSF leak and spontaneous intracranial hypotension. However, superficial siderosis can develop after spontaneous intracranial hypotension from a spinal CSF leak is treated with epidural patching and after complete resolution of spontaneous intracranial hypotension (11). This indicates that there are two separate pathophysiological processes following a spinal ventral dural tear: (1) CSF loss causing spontaneous intracranial hypotension and (2) persistent low-level bleeding from the spinal dural tear causing superficial siderosis. Epidural patching may successfully treat spontaneous intracranial hypotension but does not prevent superficial siderosis progression. Microsurgical sealing of spinal CSF leaks may stop progression and improve symptoms in patients with superficial siderosis in a time-dependent manner (38).
Symptomatic treatment is directed as well at various features of the condition, including headache, seizures, etc.
During follow-up of patients with ischemic stroke or transient ischemic attack with cortical superficial siderosis, the risk of ischemic stroke exceeds that of intracranial hemorrhage for patients receiving antiplatelet or anticoagulant treatment alone, but the risk of intracranial hemorrhage exceeds that of ischemic stroke in patients receiving both treatments (81). Either antiplatelet or anticoagulant treatment alone should not be avoided if otherwise clinically indicated in patients with cortical superficial siderosis, but combined antithrombotic therapy might be hazardous (81).
Despite the retrocochlear nature of the disorder, bilateral profound hearing loss from superficial siderosis is not an absolute contraindication for cochlear implants (33; 49; 57; 148; 120; 152; 92; 121; 119; 132; 105; 94). The reported success of cochlear implantation in such cases is variable (120; 152; 132), with some anecdotal reports of benefit (49; 57; 119), other reports showing below average results among all postlingual deaf cochlear implantation patients (03), and still others showing lack of benefit or only marginal benefit (148; 105). Furthermore, the apparent initial benefit from cochlear implants in patients with superficial siderosis may not be long-standing, particularly in those with progressive underlying disease (152; 132). Long-term outcomes depend on the lesion site, the degree of cochlear nerve function, and the ongoing neural deterioration (132).
Pharmacotherapy with iron-chelation therapy is not of demonstrated effectiveness (118), nor is shunting of cerebrospinal fluid (86) or corticosteroid therapy (110). Improvement in hearing and mobility has been anecdotally reported following treatment with deferiprone, an iron chelation therapy that can penetrate the blood-brain barrier (30; 29), but this therapy has also been associated with agranulocytosis (50), so controlled studies will be necessary to establish the efficacy and overall utility of this therapy.
Among patients with superficial siderosis and spinal dural defect, operative closure leads to improvement or stabilization of CSF evidence of bleeding (CSF red cell count and CSF ferritin levels) as well as improvement or stabilization of symptoms in most patients (76; 109; 79). However, some aspects of the disease may continue to progress for years after correction of the responsible defect (109).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
Dec. 13, 2024
Neuromuscular Disorders
Dec. 09, 2024
General Neurology
Dec. 09, 2024
Neuro-Oncology
Dec. 05, 2024
Neuro-Ophthalmology & Neuro-Otology
Dec. 02, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 24, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024