



Peripheral Neuropathies
Lead neuropathy
Feb. 06, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Historically, Lyme disease, an infection with the tick-borne spirochete Borrelia burgdorferi (Bb), has been said to involve the nervous system in 10% to 15% of infected individuals–both in Europe and the U.S.–although data suggest this proportion may be decreasing with earlier diagnosis and treatment. Controlled studies indicate that neuroborreliosis is generally curable with oral antibiotics, particularly doxycycline, often with relatively rapid resolution of neurologic deficits. Although much is said about “neurologic” symptoms, symptoms such as fatigue, “brain fog,” and concentration difficulty, which present after microbiological cure of this infection, studies indicate that months after treatment these symptoms are not only unrelated to nervous system infection but occur with essentially the same frequency in treated patients and in healthy controls. Lyme disease diagnosis generally relies on 2-tier serologic testing, with positive or equivocal ELISAs validated by either a Western blot or by a second, independent ELISA. Demonstrated synthesis of anti-Bb antibody in the CSF (intrathecal antibody production; ITAb) is considered necessary to make a diagnosis of definite CNS Lyme neuroborreliosis, a diagnosis that may be further supported by demonstrated elevation of CSF CXCL13 concentration.
|
• Lyme disease, an infection with the tick-borne spirochete B burgdorferi, historically has been reported as affecting the central or peripheral nervous system in up to 10% to 15% of patients–a number that may be declining with earlier diagnosis and treatment. | |
|
• Clinical phenomena associated with Lyme neuroborreliosis (LNB) typically include one or more of the following: cranial neuropathy (most often the facial nerve), radiculopathy, and lymphocytic/monocytic meningitis. | |
|
• Diagnosis of definite CNS Lyme neuroborreliosis requires demonstration of a CSF pleocytosis and intrathecal production of anti-Bb antibody. If either is absent, cases are considered possible/probable, not definite. | |
|
• Serodiagnosis after the first month of infection has high sensitivity and specificity. | |
|
• Treatment with 2- to 4-week courses of oral antibiotics is curative in most; parenteral treatment is recommended either if there is evidence of parenchymal brain or spinal cord involvement or if objectively demonstrable active disease persists after appropriate oral treatment. | |
|
• Persisting difficulties after treatment, often referred to as “post-treatment Lyme disease syndrome,” may occur but are not associated with nervous system infection and, in most studies, are no more common than in controls. | |
|
• Misinterpretation of testing and clinical observations results in many patients being treated unnecessarily for what is incorrectly thought to be Lyme disease, with considerable potential for side effects and patient expense. |
The term "Lyme arthritis" was first introduced in 1977 and was subsequently broadened to "Lyme disease" when it was recognized that the disorder commonly involved multiple organ systems in addition to joints (73). However, the syndrome was described much earlier in the 20th century. In 1910, Afzelius first reported the typical cutaneous lesion, erythema migrans (formerly known as erythema chronicum migrans). In 1922, Garin and Bujadoux described tick bite-associated meningoradiculitis, the most typical neurologic presentation in this disorder. Following a more detailed description of this syndrome by Bannwarth, the notion that bites of Ixodes ticks could lead to a syndrome of lymphocytic meningitis with painful radiculoneuritis became widely accepted by European clinicians. The first reports of Lyme arthritis described cases of what had been thought to be juvenile rheumatoid arthritis among children in the region of Lyme, Connecticut (73). Detailed epidemiologic studies led to the association of this disorder with bites of Ixodes ticks. In 1979, Reik and colleagues described a neurologic syndrome in American patients with Lyme disease virtually identical to that described by Garin and Bujadoux (62). In 1983, the responsible spirochete, Borrelia burgdorferi, was identified as the causative agent in American patients with Lyme disease. Shortly thereafter, closely related microorganisms were identified in European patients. Subsequent work has both broadened the scope of the neurologic disorders recognized as associated with this infection (known collectively as "Lyme neuroborreliosis") and refined the microbiological understanding of the responsible organisms. Advances in genomics have led to a proposed change in taxonomy, differentiating the organisms responsible for Lyme disease and related disorders, with the recommended name Borreliella, from the relapsing fever Borrelia (07)--a proposal that has yet to gain widespread acceptance. The broad group formerly termed B burgdorferi sensu lato would be termed Borreliella burgdorferi, with corresponding changes in the names for B afzelii and B garinii.
|
• Lyme disease is a multisystem infectious disease. Skin involvement (erythema migrans) occurs in most; joint (Lyme arthritis) and nervous system (Lyme neuroborreliosis) involvement occur in a significant minority. | |
|
• Nervous system involvement typically involves all or part of a triad of mononuclear cell meningitis, cranial neuritis, and radiculoneuropathy–the latter typically a painful radicular disorder virtually indistinguishable from a mechanical radiculopathy. | |
|
• Historically, Lyme arthritis has been considered the most frequent extracutaneous manifestation in North America, and Lyme neuroborreliosis has been the most frequent in Europe. Recent data suggest these numbers have evolved with both occurring less frequently than previously, and now the nervous system being the second most common site in both regions. | |
|
• In both Europe and North America, facial nerve palsy is the most common neurologic manifestation, occurring in more than half of Lyme neuroborreliosis patients. Radiculoneuritis occurs less frequently and is rarely identified in children. Whether it is less common in North American than European patients is debated. | |
|
• The diagnosis of definite CNS Lyme neuroborreliosis requires an appropriate clinical picture, CSF pleocytosis, and demonstration of intrathecal antibody production. If any one element is absent, the diagnosis is considered possible/probable Lyme neuroborreliosis. These criteria are often not met in Lyme neuroborreliosis limited to peripheral nerve. |
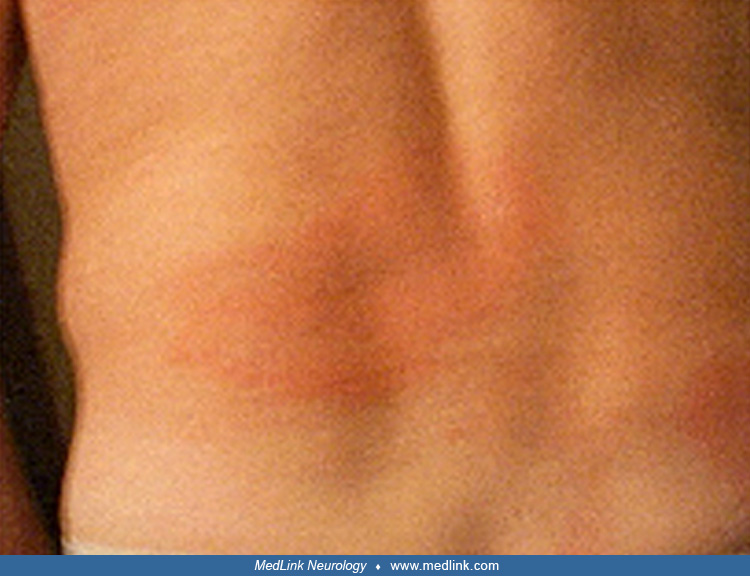
Lyme disease, or Lyme borreliosis, is a multisystem infectious disease. The most commonly affected organ systems are skin, joints, nervous system, and heart. The most frequent manifestation is a characteristic erythematous, macular, usually painless rash at the site of an Ixodes tick bite, typically evolving over days to weeks to become many centimeters in diameter, known as erythema migrans. United States Centers for Disease and Prevention data indicate erythema migrans occurs in 70% to 75% of patients overall (69). Notably, it is described in as many as 90% of infected children (23). Whether this reflects a biologic difference between children and adults, or more complete surveillance of small children by their parents, remains to be determined.
This erythroderm is virtually unique, although a disorder known as Southern Tick Associated Rash Illness (STARI), occurring primarily in the central midwest United States, quite rarely in Lyme endemic areas, causes a self-limited erythroderm that is identical in appearance, is not caused by borrelia, and is not antibiotic responsive. Following erythema migrans, which is an acute and usually localized cutaneous infection, patients may develop subacute problems secondary to bacterial dissemination. This dissemination may be accompanied by what is often referred to as a flu-like syndrome with fever, malaise, and diffuse aches and pains. In some, bacterial dissemination will result in a multicentric erythema migrans. Historic epidemiologic data indicate that in the United States arthritis occurs in 25% to 30%, with objective neurologic manifestations in about 12%--the latter similar to the usually quoted 15% Lyme neuroborreliosis incidence in European patients. Fewer than 2% of patients will develop cardiac conduction abnormalities (69). Others may develop a mild hepatitis or myositis.
In both Europe and North America, nervous system involvement typically consists of all or part of the triad of lymphocytic/monocytic meningitis (occurring in isolation in about 2% of CDC-confirmed Lyme disease cases), cranial neuritis, (primarily facial nerve palsy, occurring in about 8% of Lyme disease patients), and radiculoneuropathy (in about 4% of confirmed cases) (69). Data suggest these numbers may either have been overestimated or have changed over time. One systematic study from Ontario found that most patients reported as having “arthritis” actually had arthralgias, with frank arthritis occurring in just 2.8% of Lyme disease patients (33), a number identical to the estimate of 2.8% from analysis of a large German database (13). Similarly, the Ontario data found just 3.7% of Lyme disease patients had facial nerve palsy. In the German data just 3.8% of Lyme disease patients had Lyme neuroborreliosis (not stratified by site of involvement) in contrast to the usually quoted 10% to 15% of European patients–the latter based primarily on older Scandinavian studies. Given the recent observation that the duration of erythema migrans is two to three times longer in patients who develop Lyme neuroborreliosis than in those without disseminated disease, this may reflect earlier recognition and treatment of this infection (54). Alternatively, the possible role of referral and anchoring biases, imprecisely applied diagnoses, or other issues cannot be underestimated.
Studies do suggest neurologic symptomatology differs in children and adults, which may factor into differences among studies, many of which have been skewed towards one group or the other. Among Czech patients with Lyme neuroborreliosis-related motor weakness (72), weakness affected a limb in 20% of adults (radiculoneuropathy) and the face in 75%; in children these numbers were 3% and 97%, respectively, a disparity corroborated in a Dutch study (82) (not limited to patients with motor weakness, as in the Czech study) in which polyradiculitis occurred in 51% of adults with any form of Lyme neuroborreliosis, but just 3% of children.
Virtually any cranial nerve may be involved, although the seventh is the most common, with facial nerve palsies occurring in greater than 50% of all patients with Lyme neuroborreliosis. Lyme disease is one of the small number of disorders (along with sarcoidosis and Guillain-Barre syndrome) commonly associated with bilateral facial palsies, occurring in up to 30% of adults with Lyme-associated facial nerve palsies but less than 6% of children. Painful radiculitis, historically considered the most common presentation in European adults with Lyme neuroborreliosis, may precisely mimic a mechanical monoradiculopathy or may be more disseminated, causing an apparent plexitis or even a diffuse disorder that may clinically resemble Guillain-Barre syndrome (82). Although it is often stated that painful radiculopathy is much less common in the United States than in Europe, a study of U.S. patients with Lyme facial nerve palsy found that a third had concomitant radicular symptoms (46). Rare patients (up to 3% in one European series) may develop a focal encephalitis with prominent white matter involvement, or a myelopathic picture, the latter reported to occur in 7% of European patients with radiculitis (70; 37). No systematic data are available in U.S. patients (34). Studies of experimental infection in primates have demonstrated meningeal and radicular infection, but not CNS parenchymal infection (26).
Some patients will come to medical attention only when the disease has been present for a longer period of time. Lyme arthritis is generally considered a subacute or late manifestation. This is typically an asymmetric, large joint (eg, knee, elbow, hip) recurring oligoarthritis (73). The other common late manifestations are neurologic. At one extreme (fortunately rare), this may include a chronic encephalomyelitis, with focal abnormalities on neurologic examination and brain MRI scans (28). At the other neuroanatomic extreme, neurologic manifestations may entail a mild peripheral neuropathy that may resemble a symmetric distal polyneuropathy, a more focal mononeuropathy multiplex, or even a polyradiculopathy (26). One European report suggests that peripheral nerve involvement may be more common than is commonly assumed (74). A large proportion of experimentally infected primates develop a vasculopathic neuropathy, a mononeuropathy multiplex analogous to that seen clinically. Demyelinating neuropathies have been reported rarely in patients with this disorder, an association that may well be coincidental (68). Some patients with chronic B burgdorferi infection will develop mild difficulty with memory and complex intellectual tasks in the context of symptomatic multisystem involvement (26). This may, in rare patients, be due to a mild encephalomyelitis but almost always is due to the remote effects of systemic infection and inflammation (ie, a metabolic encephalopathy).
|
Peripheral nerve | ||
|
• Mononeuropathy multiplex | ||
|
- Cranial neuropathy | ||
|
Central nervous system | ||
|
• Infection in subarachnoid space | ||
|
- Radiculitis | ||
|
• Parenchymal infection | ||
|
- Encephalitis (“MS-like”) | ||
|
Not nervous system infection | ||
|
• Toxic/metabolic encephalopathy | ||
Diagnosis requires combining clinical observations with laboratory data. Clinical diagnostic criteria (case definition) used by the Centers for Disease Control are useful but somewhat restrictive, being designed for surveillance purposes and, therefore, rigor and consistency rather than sensitivity. These require either a physician-diagnosed erythema migrans, measuring at least 5 cm in diameter, or laboratory evidence of infection with B burgdorferi (culture, significant change in antibody level, a single positive 2-tier serology (blood), or disproportionate antibody elevation in CSF) in combination with either (a) acute onset of otherwise unexplained heart block; (b) a relapsing large joint oligoarthritis; or (c) mononuclear cell meningitis, cranial neuritis, radiculoneuritis, or encephalomyelitis. The last in particular should be confirmed by demonstration of production of anti-B burgdorferi antibody in the CSF. In general clinical practice, acceptance of the diagnosis is reasonable if a patient has an epidemiologically plausible exposure, has a clinical disorder within the realm of those reported to occur in this infection (40), and has had either an erythema migrans (early disease) or a positive serology. IgG antibodies should be demonstrable by 2-tiered testing in all patients with disease of more than 4 to 6 weeks duration. The common causes of false-positive serology (eg, syphilis, polyclonal B cell expansion) should be excluded. In patients with positive serologies and atypical disorders, or with negative serologies and typical syndromes, the diagnosis is possible but must be entertained with caution.
|
• Appropriate antimicrobial treatment is highly effective in effecting microbiologic cure and symptom resolution, although as in any neuropathologic process residual damage to nerve or CNS may not reverse entirely. | |
|
• Post Lyme disease treatment symptoms, such as fatigue, “brain fog,” concentration difficulty, mood disorders, and others, occur rarely in patients who have had CNS Lyme neuroborreliosis and overall occur with about the same frequency in Lyme disease patients as in the general population. The extent to which these may be examples of a more common postinfectious syndrome remains to be determined, but they clearly do not relate to brain infection–either persistent after treatment or during the acute infection itself. |
With appropriate antimicrobial therapy of early Lyme disease (erythema migrans), approximately 90% to 95% of patients will be cured. Improvement of neurologic symptoms is typically rapid. In children with facial nerve palsy or radiculoneuritis, 79% recovered fully in 3 weeks and 97% at 3 months. Among 147 adults, 68% recovered fully by 3 months, and five had residual symptoms at 1 year—one with bilateral facial weakness and four with residual lower extremity weakness (72). The exact proportion of patients cured after more long standing involvement is unclear but is probably in the range of 80% to 85% (56). Some patients will develop late sequelae despite early treatment, although prospective studies indicate that this is rare with adequate initial treatment (40). Late manifestations may consist of chronic large joint oligoarthritis, which may be HLA-linked, or, potentially more problematic but fortunately rarely seen, encephalomyelitis. Many patients with significant neurologic impairment improve substantially if treated with appropriate antimicrobial therapy.
Controlled studies indicate that prognosis after treatment, even of later disease, is excellent (43; 71; 83; 40; 04). Although many have focused on persistent nonspecific symptoms following treatment of Lyme disease, labeling this “post-treatment Lyme disease syndrome,” the existence of such an entity is questionable. Although one study found a very slight excess of such symptoms (prevalence 27.2%, or 3.9% greater than in the general population), virtually all others have found no excess compared to healthy controls (15; 78; 90; 86; 79; 03; 02). Even chronic fatigue, commonly thought of as a key element of post Lyme disease syndromes, does not appear to be a particularly common after-effect (88; 85; 86; 03). Interestingly, the best predictors of which patients will have persistent symptoms include (a) at initial presentation having either paresthesias or elevation in the sum of the Beck Depression Inventory score plus number of pain sites (87); or (b) pretreatment expectations that treatment would be effective and the patient’s presumption that they were receiving active, not placebo therapy (81). One plausible conclusion might be that receiving the diagnosis of Lyme disease heightens awareness of these subjective symptoms but does not cause them, a form of anchoring bias. Importantly, multiple studies indicate these chronic symptoms are not associated with nervous system infection (17; 25; 53; 03). Most importantly, it is clear that additional antimicrobial therapy provides such patients no meaningful benefit (32; 35; 38; 22; 21; 08; 09).
A 38-year-old woman was seen in early October for new onset of facial palsy. She had been in excellent health until early August of that year when, while summering in a Lyme endemic area, she noted an expanding erythematous rash on her abdomen, ultimately about 8 inches in diameter and lasting about 3 weeks. This improved following treatment with an oral first-generation cephalosporin, but she then developed 6 weeks of diffuse arthralgias and headaches. She next developed acute right facial paralysis, evolving over 24 hours, with retroauricular pain, hyperacusis, and decreased sense of taste. Past medical history was otherwise unremarkable, and examination was notable only for a complete peripheral right seventh nerve palsy.
She was treated with oral penicillin 2 g daily for 2 weeks. Although she improved, she had significant residual symptoms and underwent lumbar puncture. Fluid was completely normal. Serum Lyme ELISA was strongly positive, with the patient's value being 12.7 times the negative cut-off; the spinal fluid value, after appropriate correction, was identical to that in the serum. She then received 2 weeks of intravenous ceftriaxone and over the next month recovered completely.
|
• Lyme disease/Lyme borreliosis is caused by infection with B burgdorferi sensu lato spirochetes, which are transmitted to humans exclusively by bites of infected Ixodes ticks—a transmission that requires at least 24 hours attachment with U.S. B burgdorferi strains. | |
|
• Pathogenesis of nervous system infection is unclear. Presence of viable spirochetes is essential as antimicrobial therapy is usually curative. The immune response clearly amplifies the impact of the infection–both as demonstrated by the high concentrations of some cytokines in CSF of infected patients and the clinical deficits elicited when only a very small spirochete load appears to be present. | |
|
• Some data suggest a possible role for spirochete-glial interactions. |
Lyme disease is caused by spirochetes of the B burgdorferi complex, transmitted by the bite of Ixodes ticks. Six members of this family (B burgdorferi sensu stricto, B mayonii, B garinii, B afzelii, B spielmanii, and B bavariensis) are pathogenic for humans, causing the predominant clinical forms of Lyme borreliosis (45). All but B mayonii cause disease in Europe, where most cases with nervous system involvement appear to be caused by B garinii or the closely related strain B bavariensis (45). B burgdorferi sensu stricto is the agent of almost all North American Lyme disease, with rare cases caused by B mayonii (58).
Lyme disease is a zoonosis, in which humans are an inadvertent host. The sole vectors are hard-shelled Ixodes ticks (Ixodes scapularis in most of the United States, Ixodes pacificus in California, and Ixodes ricinus in Europe). These ticks go through a 3-phase, 2-year (in temperate climates) life cycle, partaking of one blood meal in each phase. In the first phase, the larva, which is the size of a print period and hatches uninfected, will typically feed on a small mammal, most often a white-footed mouse. If this host is already infected with B burgdorferi, the tick can become infected. The tick will then mature into a nymph and subsequently have its second meal. If previously infected, the tick can now transmit spirochetes; if not previously infected, the tick again can acquire infection if it feeds on an infected host. Transmission of the infection from tick to host takes time – typically, the tick must feed for at least 24 to 48 hours (for B burgdorferi SS; shorter attachments may allow transmission with the common European vectors and borrelia) before the probability becomes high that the new host on which it is feeding will become infected with the Lyme agent. During this interval, ingested blood triggers proliferation of spirochetes in the tick gut. They then disseminate in the tick, reach its salivary glands and can then be injected into the host. Even in areas where a high proportion of ticks carry Borrelia, only about 5% of humans with identified Ixodes tick bites will become infected, only half of whom will be symptomatic (84).
The mature adult tick will subsequently take its third meal, preferring to attach to a large mammal such as a bear or deer, giving rise to the common names attached to these ticks—the "deer tick" in the northeast United States and the "bear tick" in the Midwest. Although other arthropod hosts have been shown to carry B burgdorferi (horseflies, mosquitoes), the unique nature of the tick's feeding cycle is probably essential for transmission to other species, making it highly unlikely that vectors other than Ixodes ticks would transmit Lyme disease in all but the most extraordinary circumstances.
The pathophysiology of peripheral nerve and brain involvement remains unclear (63; 60; 26). The few available pathologic studies demonstrate multifocal perivascular inflammation in nerves (24; 20; 48). MRI imaging suggests a similar multifocal inflammatory process in brain and spinal cord. With the exception of one report identifying B garinii in a biopsied sural nerve of an affected patient, it has generally been impossible to demonstrate intact spirochetes in nerves or the brain (65). However, active infection is clearly an essential element, as elimination of organisms with antimicrobial treatment prevents further neurologic damage and typically leads to significant improvement (27). Notably, cytokines released in response to outer surface protein A (OspA) from B burgdorferi, and even from nonviable spirochetes, can induce both astrocyte proliferation and apoptosis in vitro potentially providing a mechanism by which infection with a small number of organisms could cause a disproportionate effect (55; 60). Studies suggest glia play an important role in this cytokine production (51; 59). Interestingly, the in vitro production of cytokines induced in cultured astrocytes by Borrelia OspA is inhibited by the clinically effective antibiotics, doxycycline and minocycline (10). Whether such mechanisms play a role in human disease and its response to treatment remains to be determined.
|
• Approximately 30,000 U.S. cases of Lyme disease are confirmed annually. The actual number is probably substantially greater. | |
|
• Despite expansion of the range of infected ticks and animal vectors, the vast majority of U.S. cases continue to be along the upper eastern seaboard and the upper Midwest, with exposure most likely in suburban and rural areas. |
The Centers for Disease Control reports approximately 30,000 confirmed cases of Lyme disease annually in the United States (69). How accurately this reflects the actual incidence of this disorder is debated. A study based on commercial laboratory testing suggested the actual number might be 10 times as high (31); however, that estimate was based on the assumption that 85% of patients had just one test performed, which may be a substantial underestimate. (If all patients had at least two tests, the estimate would decrease by half; a higher number of tests would further decrease this number.) Regardless of the actual number, endemic areas have been gradually expanding in recent years (06).
Cases have been reported from 47 states, but enzootic cycles (ie, areas where infected ticks and hosts are known to be present) have only been reported from 19. Connecticut, Delaware, Maine, Maryland, Massachusetts, Minnesota, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, Vermont, Virginia, and Wisconsin account for 95% of reported cases (69). In most of the United States, incidence is seasonal, with tick bites and infection occurring from spring through autumn, although in California a more uniform year-round distribution of acute infection is seen. The disease is prevalent in much of temperate Europe and Asia. Isolated cases have been reported from all continents except Antarctica.
|
• Because infection is spread solely by hard shelled Ixodes ticks, and these ticks preferred hosts are field mice and other small animals, avoidance of tick habitats (rural, suburban) is effective. | |
|
• If exposure to tick habitats is likely, wearing light colored clothing makes ticks more visible; spraying clothing with acaricides or tick repellants is effective. | |
|
• In North America, where 24 hours of tick attachment is necessary for infection, a tick check at the end of the day, with removal of any that are found, is usually effective. | |
|
• In the event of a tick bite, a single dose of doxycycline at the time substantially decreases the risk of infection. |
The best method to avoid becoming infected with B burgdorferi is to avoid Ixodes tick bites. Standard recommendations include the wearing of light-colored, long-sleeved shirts and long pants tucked into socks when in tick-infested areas. Achieving this goal in young children in summer is problematic, at best. Extensive spraying of skin with tick repellants or acaricides may be ill-advised, as these are partially absorbed and may be neurotoxic, particularly in small children. Spraying clothes with these agents, however, can be helpful. Because ticks must be attached for many hours before transmission is likely, a simple and thorough tick check at the end of the day will often suffice. Prophylactic antibiotics, specifically a single 200-mg dose of doxycycline (in adults) (40), can lessen the risk of infection following tick bites if in highly endemic areas. However, the risk of adverse drug reactions must be weighed against the need to treat 50 patients to prevent one case of Lyme disease.
Outer surface protein A vaccines can provide some protection against infection and were approved by the U.S. Food and Drug Administration. However, limited demand, combined with litigation about possible immune-mediated complications led to their withdrawal from the market.
|
• In patients with plausible exposure and either a recent erythema migrans or current positive 2-tier serology with +IgG, if symptoms of more than 4 to 6 weeks duration and disorders are within the usual Lyme neuroborreliosis spectrum, Lyme neuroborreliosis can be the presumptive diagnosis and treatment initiated. | |
|
• In patients with other CNS disorders and plausible exposure to infected Ixodes ticks, 2-tier testing should be performed. If uncertainty remains, CSF should be examined. Presence of a CSF pleocytosis with increased intrathecal production of specific antibody confirms a diagnosis of CNS Lyme neuroborreliosis. |
The differential diagnosis in patients with Lyme disease ranges from the remarkably simple to the quite complex. In patients with erythema migrans or a positive serology and part of the classic neurologic triad (meningitis, cranial neuritis, or painful radiculoneuritis), diagnostic confusion is unlikely. In patients with subacute disseminated peripheral nerve involvement, confusion with Guillain-Barre syndrome can be problematic, particularly with a facial diplegia. However, patients with severe Lyme-associated disseminated neuropathy frequently have a significant CSF pleocytosis. Some patients may develop a primarily motor polyradiculitis that can resemble a motor neuronopathy, particularly if subacute. Generally, evaluation of the CSF will differentiate among these entities.
One of the most difficult clinical dilemmas involves patients with encephalomyelitis. This very rare disorder can resemble clinically, and on MRI scan, a first episode of multiple sclerosis. Moreover, as in neurosyphilis and other chronic CNS infections, patients with nervous system Lyme disease may have oligoclonal bands in the CSF as well as increased intrathecal immunoglobulin synthesis. However, patients with this as a manifestation of Lyme disease usually have more cells in the CSF than typically seen in multiple sclerosis and almost always have demonstrable intrathecal production of anti-B burgdorferi antibodies. Large, atypical appearing lymphocytes have occasionally been reported in the CSF as well. The most difficult situation occurs when a patient previously treated for suspected Lyme encephalomyelitis has a second attack. Differentiating between inadequately treated Lyme disease and a new attack of multiple sclerosis may not be possible using generally available laboratory techniques.
|
• Because direct microbiologic diagnosis (culture, nucleic acid testing) has very low technical sensitivity, diagnosis rests on demonstration of synthesis of specific anti-B burgdorferi antibody within the CSF, which requires simultaneous measurement of immunoreactivity in CSF and serum, normalizing for the total amount of immunoglobulin in each (intrathecal antibody production; ITAb). | |
|
• Patients with demonstrated ITAb may have increased total CSF IgG synthesis and oligoclonal bands. | |
|
• Because of potential serologic cross reactivity, neurosyphilis should be excluded. | |
|
• Apparent ITAb often persists long after curative therapy. In the absence of evidence of active CNS inflammation, this result must be interpreted with caution. | |
|
• The European literature has emphasized that in clinically appropriate patients, there may be active CNS infection—and apparent ITAb—in a seronegative patient. In such patients, the first tier test has usually been positive or borderline, but the confirmatory test is negative– not an unusual finding early in infection. Therefore, in such 2-tier negative patients CSF may well be informative. |
Laboratory diagnosis of Lyme disease is generally indirect. Although B burgdorferi can be grown in vitro and can often be cultured from the typical cutaneous lesion (erythema migrans) or from large volume blood cultures in research labs, clinical sensitivity of CSF culture is typically no better than 10% to 15%. The needed culture medium is not routinely available in most clinical microbiological laboratories, so even this is usually impractical. Even inoculating CSF directly into culture medium at the time of the lumbar puncture, incubating for 2 to 6 weeks, then testing using polymerase chain reaction (PCR) to detect bacterial nucleic acid, does not meaningfully increase the diagnostic sensitivity (41). Consequently, CSF PCR or culture is not recommended for clinical diagnosis (40). In the absence of the typical cutaneous lesion, serologic testing for immunologic evidence of exposure to B burgdorferi is generally used, typically using ELISAs that measure immunoreactivity to either the entire spirochete or one or several recombinant peptides. This approach is subject to all the usual limitations of serologic diagnosis. Generally, several weeks are required following exposure before enough antibodies are present in peripheral blood for the response to be detectable. Particularly if infection was present for an extended period of time, patients may continue to produce antibody for years following successful treatment. This makes it difficult to use antibody measurements either to differentiate between current infection and past exposure or to assess treatment response. As with other serologic tests, cross-reactions to other bacteria occur. Spirochetal disorders such as syphilis, relapsing fevers, and even periodontal disease due to Treponema denticola are particularly prone to cause false positives. However, other causes of polyclonal B cell stimulation, such as subacute bacterial endocarditis, have also been shown to produce cross-reactive false positives in ELISAs.
Increased specificity is provided by sequentially performing two tests with differing individual specificities—samples with borderline or positive results on a first ELISA then undergo a second, different test. Although useful in clarifying results in samples with borderline or low positive results on the first ELISA, samples negative on the first test should not be subjected to a second one; this does not increase sensitivity and typically decreases specificity. Recent work has focused on assays measuring reactivity to single spirochete antigens such as the VlsE lipoprotein of B burgdorferi. VlsE testing appears to be more reliable than 2-tier testing in European patients where substantially greater borrelia strain variability makes Western blot-based diagnosis more challenging (12; 67).
The CDC recommends the universal use of 2-tiered testing. Since 1994, the recommended second test has been the Western blot, which identifies the specific antigens to which the patient's antibodies react. Results are interpreted by standard, well-validated (for North American patients) criteria (See Table 2), that optimize positive and negative predictive values. If five of the 10 specified IgG bands, or two of the three IgM bands are present in patients with long- or short-standing symptomatology respectively, the blot is considered positive (18).
In United States patients, replacing the Western blot as the second tier test with ELISAs measuring reactivity to an antigen different from the one(s) used in the initial test, such as VlsE, provides sensitivity and specificity comparable to using Western blots and is now considered an acceptable alternative (11; 49). Importantly, regardless of the methodology used, patients with symptoms of more than 1 to 2 months duration should have a demonstrable IgG response; purely IgM results in any such patient are far more likely to be spurious than informative (40).
|
IgG (5 of 10) |
IgM (2 of 3) |
|
18 kD |
23 kD |
In general, serologic testing should only be performed when there is a reasonable pretest likelihood of Lyme disease (ie, when an epidemiologically plausible exposure occurs and the clinical symptoms are within the spectrum of those known to be caused by this infection) (40). Indiscriminate serologic testing in other circumstances will result in more false than true positive results, with consequent unnecessary diagnostic confusion, patient apprehension, unneeded therapy, and treatment complications. Early concerns about patients remaining seronegative beyond the first or second month of infection, particularly if given subcurative doses of antibiotics, have not been supported by subsequent studies.
When attempting to confirm central nervous system infection, the most useful and readily available technique is to examine cerebrospinal fluid, both for nonspecific markers of inflammation and for evidence of production of anti-B burgdorferi antibodies within the central nervous system (75; 28; 40). Current European guidelines require that patients have either a CSF pleocytosis or intrathecal antibody production to make the diagnosis of both possible and definite neuroborreliosis (52). Demonstrating intrathecal antibody production requires comparing specific CSF and serum antibody concentrations, adjusting for blood-brain barrier function, and correcting for the amount of antibody present in peripheral blood. Technically, this can be accomplished with a capture assay, mathematically (61), or by measuring CSF and serum immunoglobulin concentration, diluting both fluids so that the final immunoglobulin concentration is identical, and then performing the Lyme-specific ELISA. Regardless of the technique used, it is essential that both CSF and serum antibody be measured and the two compared. Estimates of the technique’s sensitivity vary between 50% in patients with more chronic syndromes (44) and 90% in acute CNS disease (30). The specificity is likely over 95% (after excluding neurosyphilis), but sensitivity may be lower very early in disease and, not surprisingly, in patients in whom the peripheral but not central nervous system is involved (42).
One important question has been whether there are circumstances in which intrathecal antibody production may be present in a seronegative patient. European studies have long suggested this occurs occasionally–a finding that would suggest a need for CSF testing in clinically relevant settings even in a seronegative individual. A study that may help address this reviewed findings in 30 seronegative Dutch patients with ITAb (91). In 28 of these patients, the ELISA or CLIA (chemoluminescent assay) was positive or borderline but the Western blot was negative. In two patients, no confirmatory test was performed. Although this was correctly interpreted as seronegativity, in fact it likely reflects the fact that it takes time for the immune response to fully develop. Lyme neuroborreliosis often occurs quite early in infection; in these patients, tests were presumably obtained before the full range of antibody specificities had developed. Presumably, the reason CSF antibody is more apparent is the much lower background of other antibodies in CSF constituting background signal. However, the implication is that in a clinically appropriate setting, in patients with a positive or borderline ELISA/CLIA but negative confirmatory test, CSF exam may well be informative and worth considering–if it will impact treatment decisions. At the other end of the disease continuum, a different shortcoming of this method is that, even after successful treatment, this measure of intrathecal antibody production may remain elevated for years.
The B cell attracting chemokine, CXCL13, may be demonstrable in CSF very early in infection, potentially supporting the diagnosis and seems to decline rapidly with successful treatment (64; 66). Similar, though often less marked, elevations occur in other inflammatory disorders, including neurosyphilis and HIV (47; 57; 19). Although CXCL13 concentration may provide a useful marker of disease activity, its limited specificity requires it be used in conjunction with other indicators such as measures of intrathecal antibody production (57; 19). Another marker that has been investigated, plasma neurofilament light, which has been found to be elevated in other CNS insults, has been found to be elevated in Lyme neuroborreliosis, decreasing rapidly with successful treatment (50). Importantly, NFl is not elevated in patients with posttreatment symptoms.
Many groups have applied the polymerase chain reaction to detect bacterial DNA. Diagnostic sensitivity in CSF is unfortunately extremely low; a review by the Mayo Clinic lab, in which pretest probability was unknown, found PCR to be positive in just 0.06% of submitted CSF samples (58). The difficulty in specificity relates to eliminating the risk of contamination. Urine Lyme antigen assays are no longer commercially available and appear to be unreliable (36). ELISA spot assays (analogous to TB spot tests), purporting to demonstrate cell mediated immunity to the spirochete, have not been found to be reliable (80).
|
• Antibiotic treatment of Lyme neuroborreliosis is microbiologically and clinically curative in the overwhelming majority of cases. | |
|
• Treatment with oral doxycycline or amoxicillin, parenteral ceftriaxone, cefotaxime or high dose penicillin is largely equivalent. | |
|
• Courses longer than 3 to 4 weeks of any agent add significant risk with no demonstrable benefit. |
Although some still debate what constitutes the optimal treatment of nervous system Lyme disease, the evidence supports several conclusions (40). In patients with early cutaneous disease, amoxicillin 1.5 g daily or doxycycline 200 mg daily for 2 to 4 weeks is generally effective. Erythromycin, although effective in vitro, is less efficacious in vivo. Some macrolides such as azithromycin or clarithromycin have some role, although they may be somewhat less effective than amoxicillin or doxycycline. In patients with meningitis or other CNS infections, most centers in the United States have used either meningeal doses of penicillin or parenteral third-generation cephalosporins with good CNS penetration, such as ceftriaxone (2 g daily) or cefotaxime (6 g daily) (40). Several studies have suggested that ceftriaxone and cefotaxime are about equally efficacious; most authorities in the United States consider them to be superior to penicillin. A metaanalysis of European studies comparing oral doxycycline to parenteral regimens in patients with Lyme meningitis or cranial neuritis suggests oral regimens are as effective in this population (29), an approach considered acceptable in current European and U.S. guidelines (52; 40). Interestingly, a metaanalysis of 31 randomized controlled treatment trials concluded all currently recommended regimens–oral and parenteral–are equally effective (89), a conclusion supported by an European study in a pediatric population as well (04). The question is being studied in patients in the United States, but no data are available. Although there are strain differences between European and U.S. Borrelia, antimicrobial sensitivities are generally comparable. Until this question is rigorously tested in the United States, it is probably reasonable to use oral doxycycline in mildly-affected patients and ceftriaxone or cefotaxime in those with more severe CNS Lyme disease, pending further studies.
Glucocorticoids, used in some patients concurrently with antibiotics to control radicular pain, or facial palsy, can be used, but with caution. No controlled clinical studies have been carried out, but animal studies suggest they may potentially play a helpful role (60). Retrospective studies in facial nerve palsy have provided conflicting conclusions but in aggregate suggest that use of corticosteroids does not worsen outcomes (05; 46).
Anecdotal reports have described fetal loss and malformations in some women with untreated acute Lyme disease infection (tick bite, erythema migrans) during pregnancy (39), but no consistent congenital syndrome has been observed. Several large epidemiologic studies have indicated no increase in the frequency of adverse pregnancy outcomes in women who are found to be seropositive or are found to have other nonacute disorders associated with Lyme disease (14; 01; 77; 76). In women with acute infection during pregnancy, aggressive antimicrobial treatment is appropriate. Notably, longstanding concerns about the use of tetracyclines such as doxycycline during pregnancy, because of potential effects on bone and teeth, have been called into question, leading to recommendations allowing the use doxycycline during pregnancy (16). Some have suggested that use of ceftriaxone in the third trimester might be associated with fetal hyperbilirubinemia. High-dose ampicillin or penicillin is usually recommended in this setting.
No data are present to address this issue. No evidence provides reason to believe that anesthesia would pose any additional risk for patients with Lyme disease.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
John J Halperin MD
Dr. Halperin of Overlook Medical Center and Sidney Kimmel Medical College of Thomas Jefferson University has stock ownership in Johnson & Johnson and has received consultant honorariums from Pfizer.
See Profile
John E Greenlee MD
Dr. Greenlee of the University of Utah School of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Feb. 06, 2025
Peripheral Neuropathies
Feb. 05, 2025
Peripheral Neuropathies
Jan. 19, 2025
Peripheral Neuropathies
Jan. 19, 2025
Peripheral Neuropathies
Dec. 30, 2024
Peripheral Neuropathies
Dec. 30, 2024
Peripheral Neuropathies
Dec. 30, 2024
Peripheral Neuropathies
Dec. 30, 2024