Epilepsy & Seizures
Tonic status epilepticus
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Absence status epilepticus is a prolonged, generalized absence seizure that usually lasts for hours and can even last for days. The cardinal symptom is the altered state of consciousness while the patient is usually fully alert and partially responsive. Absence status epilepticus may be typical, occurring in patients with idiopathic generalized epilepsy, or atypical, occurring in patients with neurocognitive impairment as with developmental and epileptic encephalopathies. Absence status epilepticus may also appear de novo, mainly in adults without a previous history of epilepsy. Absence status epilepticus is often misdiagnosed as focal status epilepticus or a confusional nonepileptic condition or epileptic prodrome. Frequently, absence status epilepticus occurs in the setting of medication nonadherence or because of ill-advised antiepileptic drug treatment, such as with tiagabine or carbamazepine in patients with idiopathic generalized epilepsy.
|
• Absence status epilepticus is a prolonged, generalized absence seizure that usually lasts for hours and can even last for days. | |
|
• The cardinal symptom is the altered content of consciousness while the patient is usually fully alert and partly responsive. | |
|
• Most patients suffer from idiopathic generalized epilepsy, but absence status epilepticus may also appear de novo. Other types of seizure such as absences, myoclonic jerks, and generalized tonic-clonic seizures may predate the first occurrence of absence status epilepticus by many years. | |
|
• Absence status epilepticus is often misdiagnosed as focal status epilepticus, confusional nonepileptic condition, or epileptic prodrome. | |
|
• Medication nonadherence is a common trigger for the occurrence of absence status epilepticus. | |
|
• Frequently, absence status epilepticus occurs because of ill-advised antiepileptic drug treatment such as tiagabine, carbamazepine, gabapentin, oxcarbazepine, pregabalin, or vigabatrin. |
According to Wolf and colleagues, the first historical case of absence status epilepticus seems to be described on an ex-voto table from 1501 AD in the parish church of Gmünd in Austria (107). The table describes the story of a child with “the falling sickness” who for 3 days “lay with eyes open, speechless…did not recognize or see anybody” before he experienced a spontaneous recovery, which was attributed to prayer.
The first unequivocal documentation of absence status epilepticus with EEG was by Putman and Merritt (74) and Lennox (55). Prolonged episodes of nonconvulsive status epilepticus were described on many occasions before the EEG-era, most of which may have been of focal origin (temporal lobe) (85; 82).
Absence status epilepticus is the name proposed by the Commission on Classification and Terminology of the International League Against Epilepsy (22; 23). Absence status is not synonymous with nonconvulsive status epilepticus. Nonconvulsive status epilepticus is a term that rightly has been discarded in the new ILAE diagnostic scheme because it encompasses heterogeneous conditions, which may be focal, such as limbic status epilepticus, or generalized, such as absence status epilepticus (32; 31; 60; 64). According to an expert consensus, "nonconvulsive status epilepticus is a term used to denote a range of conditions in which electrographic seizure activity is prolonged and results in nonconvulsive clinical symptoms” (103). However, convulsive elements and, particularly, myoclonic jerks are common in generalized nonconvulsive status epilepticus, as in eyelid or perioral absence status epilepticus. If the term “nonconvulsive” is used, the distinction between “focal nonconvulsive” and “generalized nonconvulsive” should be made for clinical and management purposes (38; 36). Petit mal status epilepticus and various other synonyms have also been used in the past. Unified EEG terminology and criteria for nonconvulsive status epilepticus have been proposed (14), and its various types, including absence status epilepticus, have been systematically classified (91).
Classification. Considering that absence status epilepticus is a prolonged absence seizure, it is reasonable to adopt for this condition a definition and classification similar to that recognized for epileptic seizures and syndromes manifested with absences (23; 66; 64; 32; 31; 84; 103; 54; 42; 41).
|
Typical absence status epilepticus | ||
|
(Typical) absence status epilepticus in order of prevalence: | ||
|
• Simple absence status epilepticus (mainly in idiopathic generalized epilepsy and juvenile absence epilepsy) | ||
|
Absence status epilepticus of developmental or epileptic encephalopathies including Lennox-Gastaut syndrome | ||
|
Situation-related absence status epilepticus due to: | ||
|
I. Benzodiazepine withdrawal | ||
Absence seizures are broadly divided into: (1) typical absences of mainly idiopathic generalized epilepsy with generalized, greater than 2.5 Hz spike or polyspike-and-slow waves, and (1) atypical absences in developmental and epileptic encephalopathies with slower, less than 2.5 Hz generalized discharges (22; 79). The ILAE classification of seizure types classifies all absences as “nonmotor seizures of generalized onset” as follows: typical, atypical, myoclonic, and eyelid myoclonia absences (42; 41).
Similarly, absence status epilepticus is divided into typical absence status epilepticus of mainly idiopathic generalized epilepsy and atypical absence status epilepticus of developmental or epileptic encephalopathies.
Furthermore, to comply with seizure and syndrome classification, absence status epilepticus may be situation-related and caused by the introduction or withdrawal of certain drugs, intoxication, or electrolyte or metabolic disturbances. Symptomatic absence status may also be caused by severe brain anoxia or other brain damage.
ILAE Task Force classification. The ILAE Task Force report (31) classifies absence status epilepticus as:
(A) Typical and atypical absence status epilepticus. When absence status epilepticus occurs in the idiopathic epilepsies, it has features similar to atypical absence and can be terminated by antiepileptic drugs. In the developmental and epileptic encephalopathies, there is overlap with focal status epilepticus due to lesions of certain frontal lobe areas. The absence status epilepticus occurring in elderly patients without a prior history of epilepsy, as well as drug-induced and drug-withdrawal absence status epilepticus, have been characterized and most likely represent similar mechanisms; however, there may be several types of typical and atypical absence status epilepticus.
(B) Myoclonic absence status epilepticus. Myoclonic absence status epilepticus consists of proximal, predominantly upper extremity myoclonic jerks corresponding with 3 Hz spike-wave discharges in the EEG. It can last hours or even days and is usually resistant to therapy.
|
• The cardinal symptom shared by all cases of absence status is the altered content of consciousness while the patient is alert and partly responsive. | |
|
• Absence status epilepticus may terminate spontaneously or with a generalized tonic-clonic seizure. | |
|
• Often the patient and family can recognize the clinical occurrence of status epilepticus. | |
|
• Absence status epilepticus should be identified early as a neurologic emergency to avoid delays in treatment. |
Absence status epilepticus is a prolonged, generalized absence seizure, which is defined as lasting more than half an hour but usually lasts for hours and even for days. It is associated with typically regular and symmetrical generalized discharges of 1 to 4 Hz spike or multiple spike-and-slow wave complexes. Though the sharing symptom of absence status epilepticus is impairment of cognition, this is often associated with other clinical manifestations that may be syndrome related. It should be emphasized that absence status epilepticus, like the brief absence seizure, is not one but many types of a prolonged, generalized, absence seizure (08; 22; 23; 47; 30; 77; 82; 03; 84; 103; 97; 64; 65; 54).
Impairment of consciousness, memory, and higher cognitive functions. The cardinal symptom shared by all cases of absence status is the altered content of consciousness while the patient is alert and partly responsive.
Memory and higher cognitive intellectual functions such as abstract thinking, computation, and personal awareness are the main areas of disturbance (08; 47; 03; 84; 103; 64; 65). This varies from extremely mild to extremely severe with intermediate states of severity occurring more often. Mild impairment of consciousness manifests with slow reaction, behavior, and mental functioning.
Descriptions of this state as perceived by patients with idiopathic generalized epilepsies are well illustrative:
|
My mind slows down…able to understand but takes longer to formulate answers…I become slow but can communicate verbally with others…slow down in my behavior…muddling with words…like in a trance…missing pieces of conversation… |
Moderate and severe impairment of consciousness manifest with varying degrees of confusion, global disorientation, and inappropriate behavior, and these are described by witnesses as follows:
|
Confused…cannot recognize people other than close relatives…disorientated in time and place…very quiet, disturbed, vague, uncooperative, confused...markedly confused…goes into a dreamy state…able to formulate some answers to simple questions…puts trousers over pajamas...confused…makes coffee twice…fades away mentally and physically…disoriented in time and place (03). |
Usually, the patient with absence status of idiopathic generalized epilepsy is alert, attentive, and cooperative. Verbal functioning is relatively well preserved but is often slow with stereotypic and usually monosyllabic answers. Movement and coordination is intact. Although the patient may rarely become completely unresponsive, this author is not aware of any such case with idiopathic generalized epilepsy. It is surprising how often physicians are deceived by the general good appearance, alertness, and cooperation of the patient. Based on previous experiences, patients and relatives usually recognize the condition. However, medical intervention to stop the absence status and prevent an impending convulsion may not be offered because attending physicians may not appreciate this as an emergency.
Basic testing of memory and higher cognitive functions are essential for diagnosis. Serial Montreal Cognitive Assessment examinations are one example of a formal cognitive assessment tool which has been used to evaluate for qualitative improvement in patients being treated for absence status epilepticus (76).
Behavioral abnormalities and experiential phenomena. Though the most common behavioral changes refer to daily activities disturbed by the impairment of consciousness, some patients become depressed, agitated, and occasionally, hostile. More commonly than usually appreciated are experiential and sensational phenomena such as: "sensation of viewing the word through a different medium,” “a feeling of not being in the same world as everyone else,” “uncontrollable rush of thoughts,” “a feeling of fear of losing control of my mind," "a feeling of closeness," "a funny feeling that I can not elaborate," "a strange feeling of not being myself," "edgy, worried, and uncomfortable,” "my character changes completely, I become extremely snappy…have a severe headache," or "weird" (03; 64).
Simple gestural and ambulatory automatisms, autonomic behavior, and fugue-like states may occur in 20% of the patients who also have severe impairment of consciousness as described by witnesses: "…replies yes to any question and fumbles with his clothes," "…she wanders about without later having any recollection."
Myoclonic jerks. Segmental, usually eyelid or perioral and less often limb, myoclonic jerks frequently occur during typical absence status and vary in degree and severity. They are most likely to occur in syndromes manifesting with similar myoclonic phenomena during brief absences (03; 64).
Atypical absence status epilepticus. Atypical absence status is clinically characterized by fluctuating impairment of consciousness, often with other ictal symptoms such as repeated serial tonic or atonic seizures and segmental or generalized jerks. The ictal EEG pattern is of slow, less than 2.5 Hz, generalized spike-wave activity. Both the clinical patterns and the EEG abnormalities are more variable than those of typical absence status epilepticus. Atypical absence status epilepticus occurs mainly in children with developmental and epileptic encephalopathies, including Lennox-Gastaut syndrome, who also have a plethora of other types of frequent seizures such as atypical absences, tonic and atonic seizures, myoclonic jerks, and generalized tonic-clonic seizures. Most of them also have moderate or severe learning and physical handicaps. In addition, interictal EEG is often very abnormal with slow background and frequent brief or long runs of slow spike-wave discharges, paroxysmal fast activity, and paroxysms of polyspikes. It is often difficult to define the boundaries (ie, the onset and termination) of atypical absence status epilepticus because these children frequently have alterations of behavior and alertness as well as long interictal slow-spike and slow-wave discharges. Additional discriminating features of atypical absence status epilepticus are: gradual onset and offset; level of consciousness and other coexistent types of seizure tend to fluctuate sometimes for weeks with little distinction between ictal and interictal phases; their initiation or termination with a convulsion is exceptional; and, incontinence is common.
Prognosis depends on the type of absence status epilepticus and syndrome. It may occur only once in a lifetime (situation related); it may be infrequent or preventive (as in most cases of idiopathic generalized epilepsy with typical absences); it may be frequent and intractable (which is often the case with developmental and epileptic encephalopathies and atypical absences); or it may be associated with death due to the underlying severe medical condition (as in absence status epilepticus of severe brain anoxia).
Absence status epilepticus often terminates spontaneously or with a generalized tonic-clonic seizure. In most cases of idiopathic absence status epilepticus, the patient is aware of this condition and the risk of ending with a convulsive seizure. Patients or their family members who can recognize the clinical state of absence status epilepticus may self-administer abortive medications such as intranasal midazolam or rectal diazepam in order to stop the absence status and prevent the impending convulsive seizure (48; 100; 102).
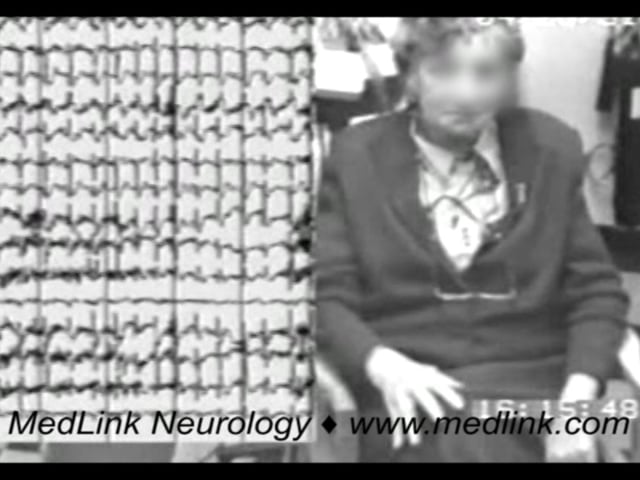
A 76-year-old woman is presented for three reasons:
(1) She is a typical case of absence status documented with video-EEG.
(2) She was unjustifiably misdiagnosed for 28 years as having complex partial seizures with secondary generalized tonic-clonic seizures, and she was inappropriately treated with primidone and sulthiame.
(3) She demonstrates how a new syndrome can be recognized with our dual approach, which uses a retrospective and prospective collection of clinico-EEG data. The syndrome in her case is “phantom absences, generalized tonic-clonic seizures, and frequent absence status,” mainly of adult onset (69; 53).
Her first overt seizure occurred at the age of 30 years. She was moderately confused for 12 hours prior to a convulsive seizure.
Despite an EEG showing brief discharges of 3 Hz spike-and-slow waves and no clinical evidence of brief complex partial seizures of temporal lobe symptomatology, she was misdiagnosed as having temporal lobe epilepsy and was treated with high doses of primidone and sulthiame until her referral to this author’s clinic in 1990.
Through the years, she had at least 30 episodes of absence status, lasting from three hours to 10 days and often progressing to GTCS. Also, questioning revealed that she frequently had brief episodes of two to five seconds wherein she experienced a lack of concentration (absences) or of memory for a few seconds, which could be misinterpreted as normal variations in daily life. She was free of seizures for the previous nine years on monotherapy with sodium valproate 1000 mg daily. Her last EEG in 1997 still showed some brief generalized discharges of 3 Hz spike-and-slow waves on overbreathing without clinical manifestations. A similar case has been reported (73).
Syndromic classification of this illustrative case. We initially categorized this woman amongst the unclassified cases, suggesting that "she may be a case of late-onset absence status, absences, and GTCS” (67). Later, on the basis of another 12 similar cases, we concluded that she suffered from a previously unrecognized syndrome of idiopathic generalized epilepsy with absences, generalized tonic-clonic seizures with onset in adulthood, and frequent absence status epilepticus (69).
|
• Absence status epilepticus is most likely due to abnormal bilateral and synchronous oscillatory bursts of interconnected thalamocortical neurons. | |
|
• Absence status epilepticus does not appear to cause permanent neurologic damage. |
By definition, absence status epilepticus is a prolonged, generalized absence seizure.
|
Generalized epileptic seizures are conceptualized as originating at some point within, and rapidly engaging, bilaterally distributed networks. Such bilateral networks can include cortical and subcortical structures, but do not necessarily include the entire cortex. Although individual seizure onsets can appear localized, the localization and lateralization are not consistent from one seizure to another. Generalized seizures can be asymmetric (15). |
The pathophysiology of absence status epilepticus (typical or atypical) is unknown. It is likely that the generating mechanisms of absence seizures and absence status epilepticus are the same because their clinico-EEG features show marked syndrome-related similarities (03; 64). The difference is in the duration of the discharge, which may also perpetuate more severe cognitive impairment. Absence seizures last for only a few seconds, whereas absence status epilepticus is prolonged for hours and days, which indicates that the major deficit is inability of “seizure-terminating” mechanisms. Therefore, the continuation of absence seizure may be due to a failure of brain systems, neurotransmitters, or neurophysiological circuits that usually interfere to terminate the abnormal discharge. Absence seizures are probably terminated by persistent activation of a depolarizing current in thalamocortical neurons that inactivates T-type calcium channels. Thus, absence status epilepticus could result from dysfunction of T-type calcium channels or mechanisms that hyperpolarize thalamocortical neurons such as decreased cortical inhibition, increased reticular thalamic neuronal activity, or increased thalamocortical neuron GABA(B)-receptor activation (84). It may also be possible that self-sustained feedback loops or other mechanisms perpetuate and sustain the absence seizure process (97). One study suggests a contributing role of the frontal region in absence status epilepticus by showing that scalp EEG recordings of patients with absence status epilepticus have higher power and frontally predominant fast ripples compared to patients with typical absence seizures (49). In a 17-year-old girl with absence status epilepticus, ictal positron emission tomography using [(18)F]fluorodeoxyglucose revealed hypermetabolism of the bilateral thalamus and cerebellum and hypometabolism of the frontal, parietal, and posterior cingulate cortices (81). Animal models suggest that activation of the alpha-2a adrenergic receptor may play a role in the activation of absence status epilepticus (genetic mutants, pentylenetetrazole-induced), and there is relatively scarce neuropathology that can be attributed directly to status epilepticus (108).
We also do not know why and how an absence seizure or absence status epilepticus may progress to a convulsive seizure.
In a study, seven severely ill adult patients with symptomatic absence status epilepticus and generalized spike-wave patterns were investigated by EEG spectral analysis, LORETA (Low Resolution Electromagnetic Tomography) source imaging, and LSC (LORETA Source Correlation) analysis, which estimates cortico-cortical EEG functional connectivity among 23 regions of interest in each hemisphere (71). Maximum Z-scored spectral power was found in the 1-6Hz and 12-14Hz frequency bands. LORETA showed that the uppermost synchronized generators of 1-6Hz band activity were localized in frontal and temporal cortical areas that are parts of the limbic system. For the 12-14Hz band, abnormally synchronized generators were found in the antero-medial frontal cortex. Unlike the rather stereotyped spectral and LORETA findings, the individual EEG functional connectivity patterns were very dissimilar (71).
Absence status epilepticus does not appear to cause permanent neurologic damage (29; 84).
|
• Typical absence status epilepticus is more common among patients with idiopathic generalized epilepsies with absence seizure types. | |
|
• Atypical absence status epilepticus is more common among patients with Lennox-Gastaut syndrome and other developmental or epileptic encephalopathies. |
The incidence and prevalence of the various types of absence status epilepticus are not precisely known. Typical absence status epilepticus is more common in certain syndromes of idiopathic absence epilepsy and mainly juvenile absence epilepsy, idiopathic generalized epilepsy with absence seizures, and perioral myoclonia with absences (03). Atypical absence status epilepticus is more common in Lennox-Gastaut syndrome and patients with other developmental or epileptic encephalopathies. Risk factors include inappropriate antiepileptic drug treatment.
Absence status epilepticus may be misdiagnosed as epileptic prodrome or prolonged confusional or psychotic state (64; 07; 58). Owing to the protean clinical features and absence of gross motor manifestations, the diagnosis of absence status epilepticus is frequently missed. The diagnosis of absence status epilepticus should always be entertained in patients who present with otherwise unexplained prolonged, confusional states or altered mental status. Ictal EEG confirms the diagnosis.
A high degree of suspicion is necessary, particularly among patients with known epilepsy, as absence status epilepticus is frequently misdiagnosed with presentations of intoxication or toxic ingestion, psychiatric illness, and encephalopathy from toxic metabolic or infectious states (87).
|
• Ictal EEG with greater than 2.5 Hz generalized spike-and-slow wave complexes is the hallmark of typical absence status epilepticus. |
A combination of history, EEG, ancillary testing, and physical examination findings can be used in order to subclassify the absence status epilepticus by the underlying epileptic syndrome or etiology. In idiopathic (typical) absence status epilepticus, all patients by definition are of normal physical and mental state and have normal brain imaging. Ictal EEG confirms the diagnosis with continuous, greater than 2.5 Hz generalized spike-and-slow wave complexes (64; 07).
Ictal EEG during the absence status may consist of repetitive discharges of multiple spikes and slow waves.
Interictal EEG of idiopathic generalized epilepsy usually shows brief discharges with similar characteristics as those of the ictal EEG.
In absence status epilepticus in patients with developmental or epileptic encephalopathy, video-EEG may be essential for diagnosis. Also, a high-resolution MRI or positron emission tomography may be needed because of the possibility of a distinct epileptogenic focus amicable to surgery.
A combination of history, EEG, ancillary testing, and physical examination findings should be used in order to subclassify the absence status epilepticus by the underlying epileptic syndrome or etiology as follows:
Idiopathic (typical) absence status epilepticus. Idiopathic (typical) absence status epilepticus is easy to diagnose, providing that the associated syndrome of idiopathic generalized epilepsy with typical absences is correctly identified. This is often combined with myoclonic jerks and GTCS. With the possible exception of childhood absence epilepsy, all other syndromes of idiopathic generalized epilepsy with typical absences may manifest with typical absence status, either as a spontaneous expression of their natural course or provoked by external factors or inappropriate treatment maneuvers (03; 64; 65). In these conditions, the patient or relatives are well aware of the clinical manifestations of absence status epilepticus, which often heralds GTCS. The most common misdiagnosis is made because absences are not recognized or are misdiagnosed as focal seizures with impairment of awareness (previously complex partial seizures) (03; 12; 64; 65). A previous or a new EEG invariably shows generalized discharges in idiopathic generalized epilepsy. It may be normal or may show specific focal spikes in focal epilepsies, mainly temporal lobe epilepsy.
The clinical manifestations of idiopathic (typical) absence status epilepticus, a lengthened absence seizure, are syndrome related (03; 64; 65). Though mild or severe impairment of consciousness is the sharing symptom, other associated manifestations such as perioral or eyelid myoclonia depend on the underlying epileptic syndrome (Table 1).
Impairment of consciousness and myoclonic jerks. Impairment of consciousness, memory, and higher cognitive function, as detailed in the clinical manifestations, may be the same irrespective of idiopathic generalized epilepsy syndrome. It is not the absence but the other associated clinical manifestations (ie, myoclonic jerks) that betray the underlying syndrome of idiopathic generalized epilepsy. These may be segmental (usually eyelid or perioral and less often limb) myoclonic jerks occurring during typical absence status. They are of varying degree and severity. They are most likely to occur in syndromes manifesting with similar myoclonic phenomena during brief absences. Thus, continuous and disturbing eyelid myoclonia is a consistent symptom of typical absence status in the syndrome of eyelid myoclonia with absences. Similarly, perioral myoclonia is the relevant clinical manifestation of absence status in perioral myoclonia with absences. Random myoclonic jerks of the limbs or eyelids may be seen in absence status epilepticus of juvenile absence epilepsy. In juvenile myoclonic epilepsy, absence status epilepticus is rare as opposed to the frequently occurring long series of myoclonic jerks and myoclonic status epilepticus prior to a generalized convulsion (44). It is possible that in juvenile myoclonic epilepsy, absence status epilepticus consists of a mixture of myoclonic jerks interspersed with absences. The relation of the typical absences and typical absence status epilepticus is epitomized as follows by the presented illustrative patient:
|
The absences lasted a couple of seconds; the other state [absence status] was much longer, for 24 hours or more. They may be linked I suppose...I was doing silly things like making coffee without coffee, putting my pajamas over my clothes. I was able to answer the phone or the door and people would not understand that I was in that state. My husband knew and protected me. Once a physician was called but did not think that there was anything serious with me...there was nothing else abnormal, only in the mind...once, my daughter came while I was in that state. I remember that she was hungry. I could not help her. She did not realize that I was ill. |
In some patients with generalized epilepsy, there may be brief tonic spasms of facial muscles intermixed with mild absence seizures (03; 64; 65).
Onset, duration, and evolution. Though of sudden onset, the severity of symptoms may be initially mild and inconspicuous. The patient or relatives, with the experience of previous episodes, recognize this state that may progress to more serious disturbances and probably a generalized convulsion. These initial symptoms may be mild slowness of thought and mental functioning, an increasing number of perioral or eyelid jerks interspersed with mild impairment of concentration, or just a familiar, habitual personal feeling heralding the status. Soon after this initial phase, half of the patients reach a more or less steady state that, mild or severe and with or without clinical manifestations other than impairment of consciousness, is stereotype for each patient. In another one fourth of patients, the impairment of consciousness deteriorates with time. For the remaining one fourth of patients, severity shows marked fluctuations in the course of the absence status epilepticus. It is important to remember that more than half of the patients are aware of the situation when entering or during absence status epilepticus, which is of great practical significance regarding termination of this state and prevention of the impending GTCS by self-administration of appropriate medication.
Generalized tonic-clonic seizures associated with idiopathic typical absence status. Ending with a convulsive seizure is not uncommon irrespective of syndrome (08; 47; 03; 64; 65; 54). However, in only one third of patients does absence status epilepticus end with a convulsive seizure when untreated. In the remaining patients, it may also terminate spontaneously without GTCS. It is exceptional for GTCS to precede or intersperse with typical absence status (34; 03). It is also exceptional for more than one GTCS to occur following absence status epilepticus.
Duration and frequency. Idiopathic (typical) absence status epilepticus usually lasts for an average of three to four hours, rarely a minimum of half an hour, often exceeding six to 10 hours, and occasionally enduring for two to 10 days. Frequency also varies from one in a lifetime to an average of 10 to 20 or catamenial. This depends on treatment strategies and syndromic classification (03; 64; 65).
Postictal state. Amnesia of the event is exceptional. The patient is usually aware of what happens during the absence status; some are able to write down their experiences, even when in status, and others have a patchy recollection of the events, usually missing the last part prior to GTCS. Following a GTCS, the patient feels tired, has a headache, and is confused for a varying duration of time.
Age at onset and sex. It is rare for absence status epilepticus in idiopathic generalized epilepsy to start before the first decade. Other types of seizures such as absences, myoclonic jerks, and GTCS may predate the first occurrence of absence status epilepticus for many years. In the study of Agathonikou and colleagues, mean age at onset of absence status epilepticus was 29 years with a range of nine to 56 years (03). In seven of 21 patients, absence status epilepticus was the first overt type of seizure. Twelve of the 21 patients were women.
Absence status epilepticus may rarely be the first or only apparent clinical manifestations in children or teenagers (68; 58; 02; 18; 70) and a proposition was that this may be a syndrome of idiopathic generalized epilepsy with good prognosis and excellent response to anti-absence treatment (18; 70). Rarely absence status epilepticus may be the first symptom in children with idiopathic generalized epilepsy and absences (68).
Bauer and colleagues reported four cases of absence status with presentation after the age of 60 years (10). All patients had suffered from idiopathic generalized epilepsy with absence seizures, which had resolved after puberty. A second peak of idiopathic generalized epilepsy, with repeated episodes of absence status after menopause and without identifiable triggering factors is the likely explanation. Similar is the case of Fernandez-Torre and Rebollo (39). Recurrent absence status epilepticus in idiopathic generalized epilepsy may be of late onset after the remission of other seizures (62).
Genton and colleagues reported 11 idiopathic generalized epilepsy patients with recurrent, unprovoked episodes of typical absence status epilepticus as the predominant seizure type (45). The onset of absence status epilepticus was mostly after puberty or in early adulthood. Generalized tonic-clonic seizures were infrequent, but sometimes they were the first seizure type. Absences were rarely encountered.
Szucs and colleagues described three patients with onset of absence status epilepticus after the age of 50 years (92). They reviewed 16 studies of 146 patients with absence status epilepticus over the age of 50 years and found that this occurred predominantly in women (71%) (p < 0.00001).
Absence status epilepticus of late onset idiopathic generalized epilepsy has been reviewed by Brigo and colleagues (17). They identified nine patients with median age at seizure onset 71 years (range: 60 to 80) and a female prevalence (67%). A family history of epilepsy was reported in 67% of cases. All patients had generalized tonic-clonic seizures, and 44% also had myoclonic seizures. Treatment and outcome were reported for six patients, all of whom reached seizure freedom under monotherapy with valproic acid (83%) or lamotrigine (17%) (range of follow-up: three to 24 months). The authors concluded that late-onset idiopathic generalized epilepsy are entities with unknown prevalence and incidence and should be differentiated on the basis of late-onset reactivation of previous idiopathic generalized epilepsy (17).
Precipitating factors. These are also syndrome- and treatment-related. Inappropriate use or discontinuation of anti-absence medication is the most common precipitant of idiopathic absence status epilepticus. Sleep deprivation, stress, and excess of alcohol consumption, alone or usually combined, are common precipitating factors. Some patients may have catamenial precipitation. In others, this mainly starts on awakening. Lights precipitate absence status epilepticus in eyelid myoclonia with absences, a mainly photosensitive type of epilepsy.
Absence status epilepticus in the developmental and epileptic encephalopathies. Absence status epilepticus in patients with developmental and epileptic encephalopathies, including Lennox-Gastaut syndrome, is clinically characterized by fluctuating impairment of consciousness, often with other ictal symptoms such as repeated serial tonic or atonic seizures and segmental or generalized jerks. The ictal EEG pattern is of slow, less than 2.5 Hz spike-and-slow wave generalized activity (22; 23; 04; 85; 82). Both the clinical patterns and the EEG abnormalities are more variable than of the typical absence status epilepticus.
The main distinction of atypical from typical absence status is that it occurs mainly in children with developmental or epileptic encephalopathies who also have a plethora of other types of frequent seizures such as atypical absences, tonic and atonic seizures, myoclonic jerks, and GTCS. Most of them also have moderate or severe learning and physical handicaps. In addition, interictal EEG is often abnormal with slow background and frequent brief or long runs of slow generalized spike-and-slow waves, paroxysmal fast activity, and paroxysms of polyspikes. It is often difficult to define the boundaries, onset, and termination of atypical absence status epilepticus because these children frequently have alterations of behavior and alertness as well as long interictal slow spike-and-slow wave discharges.
As Aicardi stated, “No doubt, Lennox-Gastaut syndrome is commonly associated with distinct episodes of absence status, but in this condition all transitions may be found between distinct episodes of absence status and prolonged bad periods during which paroxysmal EEG activity is permanent and mental efficiency is fluctuating, at times, only in certain specific tasks” (04). Atypical absence status epilepticus occurs in many patients with Lennox-Gastaut syndrome. It may last days, weeks, or months and is highly resistant to treatment. "The EEG often becomes hypsarrhythmic, and these status-like seizures constitute a reversible aggravation of the interictal symptomatology."
Additional discriminating features of atypical absence status epilepticus are:
|
• Onset and offset are gradual. | |
|
• The level of consciousness and other coexistent seizures tend to fluctuate, sometimes for weeks, with little distinction between ictal and interictal phases. | |
|
• Initiation or termination with a GTCS is exceptional. | |
|
• Incontinence is common (85; 82). |
Situation-related absence status epilepticus. De novo absence status epilepticus is often misdiagnosed as a psychotic state or dementia. EEG is probably mandatory in adults on neuroleptic drugs or withdrawal of diazepines who present with a confusional state.
Drugs or electrolyte and metabolic disturbances. De novo absence status epilepticus is coined for this condition if it appears in adults, mainly middle-aged women, without antecedent history of epileptic seizures (96; 95; 94; 92; 25; 17). Most of the patients have a history of psychiatric disorders, and the main cause of absence status epilepticus is withdrawal of benzodiazepines. Thomas and colleagues reported absence status epilepticus in 11 middle-aged patients (10 female, one male; mean age: 58.6 years) without a history of seizures (96). Absence status epilepticus coincided with benzodiazepine withdrawal in eight cases. Cofactors included excessive use of mainly psychotropic drugs, hypocalcemia, hyponatremia, and chronic alcoholism. CT demonstrated mild cerebral atrophy in six cases. There was no recurrence, even without chronic antiepileptic treatment. The impairment of consciousness was mild, more often moderate, and rarely reached severe states of the patient becoming bedridden, stuporous, and incontinent. Half of the patients also had mainly facial myoclonic jerks, and one third had automatisms. One fourth of patients had GTCS either prior to or during the absence status epilepticus. The EEG pattern varied with continuous or more often short, repetitive recurrent bursts of generalized 0.5 to 4 Hz spike- or polyspike-and-slow waves.
Typical absence status manifested as prolonged confusional state with continuous 3 Hz spike-and-slow waves is also well documented after metrizamide myelography in nonepileptic patients (101; 63). The clinical and EEG features are easily reversible with diazepam intravenously. Rarely, the antibiotic cefuroxime may induce de novo absence status epilepticus in adults (37).
Hypoglycemia (55), hypocalcemia (50), uremia (93) and cerebral hypoxia-ischemia (57) may also induce de novo situation-related absence status epilepticus.
Absence status epilepticus in comatose or critically ill patients (61; 11; 21; 38). Comatose, mainly after severe brain anoxia, or critically ill patients may have EEG features of absence status with continuous generalized spike-and-wave complexes at 1 to 3 Hz. When clinically possible to determine, this may be associated with additional impairment of consciousness and segmental facial, trunk, or limb jerking. These features are usually associated with a fatal outcome. Prognosis does not appear to improve with treatment.
|
• First-line therapy includes intravenous benzodiazepines and valproate, with additional antiseizure medications such as levetiracetam shown to be effective as well. | |
|
• Self-administration of intranasal, buccal, or rectal benzodiazepines by patients or family members who can recognize the onset of absence status epilepticus may terminate the ictal state and prevent an impending GTCS. | |
|
• Avoidance of antiseizure medications known to induce or worsen absence seizures may prevent absence status epilepticus. |
Absence status epilepticus of any cause is treated in hospitalized patients with intravenous diazepam, lorazepam, other benzodiazepines, or sodium valproate (106; 84; 99; 60; 64; 104).
Also, levetiracetam has been shown to be efficacious in terminating absence status epilepticus (06). Reports on lacosamide efficacy in benzodiazepine-resistant absence status epilepticus are conflicting (27; 28; 88; 75) and may rarely induce absence status epilepticus (05). However, it appears that lacosamide may be efficacious in poststroke nonconvulsive status epilepticus in elderly patients (13). Use of intravenous brivaracetam in absence status epilepticus has not been studied extensively but a report described a case of absence status epilepticus in a young woman who failed trials with lorazepam, levetiracetam, lamotrigine, topiramate, and valproate and went on to obtain a sustained respond to a load of intravenous brivaracetam 100 mg (26). A previous report showed that although bolus injection of brivaracetam up to 300 mg in two patients with absence status epilepticus was well tolerated, it did not result in cessation of status epilepticus (90). These reports suggest that intravenous bolus of brivaracetam is well tolerated and may be effective in some patients with refractory absence status epilepticus.
Absence status epilepticus does not warrant the same aggressive treatment as convulsive status epilepticus (35). Furthermore, aggressive treatment of elderly patients with nonconvulsive status epilepticus may worsen prognosis (99).
Out-of-hospital management of absence status epilepticus. Patients, including older children and teenagers, frequently know when they are in absence status epilepticus and can terminate it before a GTCS occurs by self-administration of available medications. Rectal diazepam or buccal or intranasal midazolam, administered as soon as the first symptoms appear, may stop absence status epilepticus and prevent an impending GTCS (80; 64; 83; 109). Because of the inconvenience and, often, embarrassment of administering rectal medications, buccal and intranasal routes are currently preferred. Another less effective option is an oral bolus dose of valproate (usually twice the daily prophylactic dose). Oral clonazepam (1 to 4 mg) at the onset of generalized nonconvulsive status epilepticus is another option for patients with mainly myoclonic jerks.
Rectal diazepam (0.5 mg/kg for children and 10 to 20 mg for adults) has been used for many years. It has the most rapid and consistent absorption of all the benzodiazepines from this route of administration. It has a near-intravenous efficacy, stopping recurrent seizures in around 70% of patients. Suppositories or intramuscular diazepam are not useful because absorption is very slow.
Buccal midazolam (0.4 to 0.5 mg/kg in children and 10 to 20 mg in adults) is gaining wide acceptance as “a safe and more effective choice” for terminating prolonged seizures in the home (83; 109; 24). It is more convenient and more socially acceptable and is preferred by parents to rectal diazepam. Midazolam is now available in convenient formulations for buccal administration (24). However, some authors argue that keeping the solution in the buccal pouch may be difficult to achieve in a convulsive emergency and that placement of an object or fingers in the mouth of a patient having a seizure runs counter to standard first aid advice (56).
Intranasal midazolam (0.2 mg/kg in children and 5 mg in adults) is already recommended in some consensus guidelines for out-of-hospital treatment of status epilepticus (56; 105). The drug should be delivered to both nostrils to increase absorption surface area. Intranasal administration of drugs may cause considerable but transient discomfort and often results in leakage out of the nose, thus, delaying or decreasing absorption (56).
For any of these medications, a repeat dose can be given at least 10 minutes after the first dose.
Intramuscular midazolam is at least as safe and effective as intravenous lorazepam for prehospital seizure cessation (86). Furthermore, midazolam shows no degradation over 60 days in a prehospital environment, even in high-heat conditions (59).
Prophylactic treatment of patients with recurrent absence status epilepticus. Absence status epilepticus is syndrome- and seizure-related. Appropriate treatment of the responsible syndrome will also prevent absence status (65).
Sodium valproate and ethosuximide are the established antiepileptic drugs licensed as monotherapy for absence seizures (72; 46; 64). Sodium valproate controls absences in 75% of patients, GTCS in 70%, and myoclonic jerks in 75%, but because of adverse reactions may be undesirable for women. Ethosuximide controls 70% of absences but has no effect on GTCS.
If patients with idiopathic generalized epilepsy are unwilling to receive treatment with sodium valproate, other antiepileptic drugs such as levetiracetam, lamotrigine, and topiramate are effective therapeutic drug agents (Table 2) (16; 40; 65). Levetiracetam, because of its efficacy probably in all seizures, photosensitivity, and safer adverse reaction profile appears to be the most promising substitute for valproate (01; 43; 78), though its effect on absences may be weak. Lamotrigine is effective in absences and GTCS but often exaggerates myoclonic jerks (19; 65). Topiramate is effective in generalized tonic-clonic seizures, but it is associated with significant adverse reactions both in children and adults.
|
Valproate |
Levetiracetam |
Lamotrigine |
Topiramate | |
|
Myoclonic jerks |
Very effective |
Very effective |
Exaggerates in 50% |
Probably effective |
|
Generalized tonic-clonic seizures |
Very effective |
Very effective |
Very effective |
Very effective |
|
Absences |
Very effective |
Weakly effective |
Very effective |
Weakly effective |
|
Photosensitivity |
Very effective |
Very effective |
Probably effective |
Undetermined |
|
Serious adverse reactions |
Yes |
No |
Yes |
Yes |
|
Titration |
Optional (2 to 3 weeks) | |||
|
Optional (1 to 2 weeks) |
Mandatory (6 to 8 weeks) |
Mandatory (6 to 8 weeks) | ||
|
Drug-drug interactions |
Mainly with lamotrigine |
None |
Many |
Many |
|
Need for laboratory tests |
Yes |
No |
Yes |
Yes |
|
| ||||
A combination of two antiseizure medications may be needed for resistant cases. Minute doses of lamotrigine added to sodium valproate have a dramatic beneficial pharmacodynamic effect; small doses are also mandated because of increased adverse effects (64; 65). Levetiracetam alone or in combination with lamotrigine or other anti-absence medications may prove a potent efficacious option if sodium valproate is unwanted (65).
Clonazepam, particularly in absences with myoclonic components or idiopathic generalized epilepsy with myoclonic jerks is a useful adjunctive drug. Acetazolamide may be also be used as an add-on drug (64; 65).
For patients with refractory cases of recurrent absence status epilepticus, surgical management may offer additional therapeutic benefit. In a case series of patients with recurrent myoclonic absence status epilepticus, two patients underwent corpus callosotomy (20). One of these patients achieved complete seizure freedom within 8 months of surgery, whereas the other experienced a more than 50% reduction in seizure frequency.
Contraindicated drugs. Contraindicated drugs in syndromes with absence seizures, which make seizures worse and may induce status epilepticus irrespective of cause and severity are: carbamazepine, gabapentin, oxcarbazepine, phenobarbitone, phenytoin, pregabalin, tiagabine, and vigabatrin (98; 64; 65). In particular, vigabatrin and tiagabine, which are GABA agonists, may induce absence seizures and absence status epilepticus.
There are an increasing number of reports of absence and myoclonic status epilepticus induced by certain antiepileptic drugs introduced for the treatment of "epilepsy." Vigabatrin and tiagabine are notable examples (66; 33; 51; 98; 64; 65). They even induce "de novo" absence status in patients with partial seizures. Despite their pro-absence effect, these drugs are used for the treatment of idiopathic generalized epilepsy because the official bodies are casual in appropriately informing physicians regarding treatment and other respects of "epilepsies" (64). Carbamazepine (64), gabapentin (89), and pregabalin (52) are other examples of antiepileptic drugs to avoid, particularly in patients with myoclonic elements of seizures.
Tiagabine may also induce prolonged episodes of stupor associated with gradual decline in responsiveness to verbal stimuli, intermittent twitching of the upper extremities, and urinary incontinence, which may represent a form of toxic encephalopathy rather than nonconvulsive status epilepticus (09).
The outcome of absence status epilepticus is syndrome and cause related. It is relatively good in most of the idiopathic generalized epilepsies with absences but usually fatal in comatose or critically ill patients.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Jonathan M Gursky MD
Dr. Gursky of Montefiore Medical Center/Albert Einstein College of Medicine received a consulting fee from Epitel.
See Profile
Solomon L Moshé MD
Dr. Moshé of Albert Einstein College of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jan. 20, 2025
Sleep Disorders
Jan. 18, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Epilepsy & Seizures
Jan. 09, 2025