





Epilepsy & Seizures
Gelastic seizures with hypothalamic hamartoma
Dec. 23, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
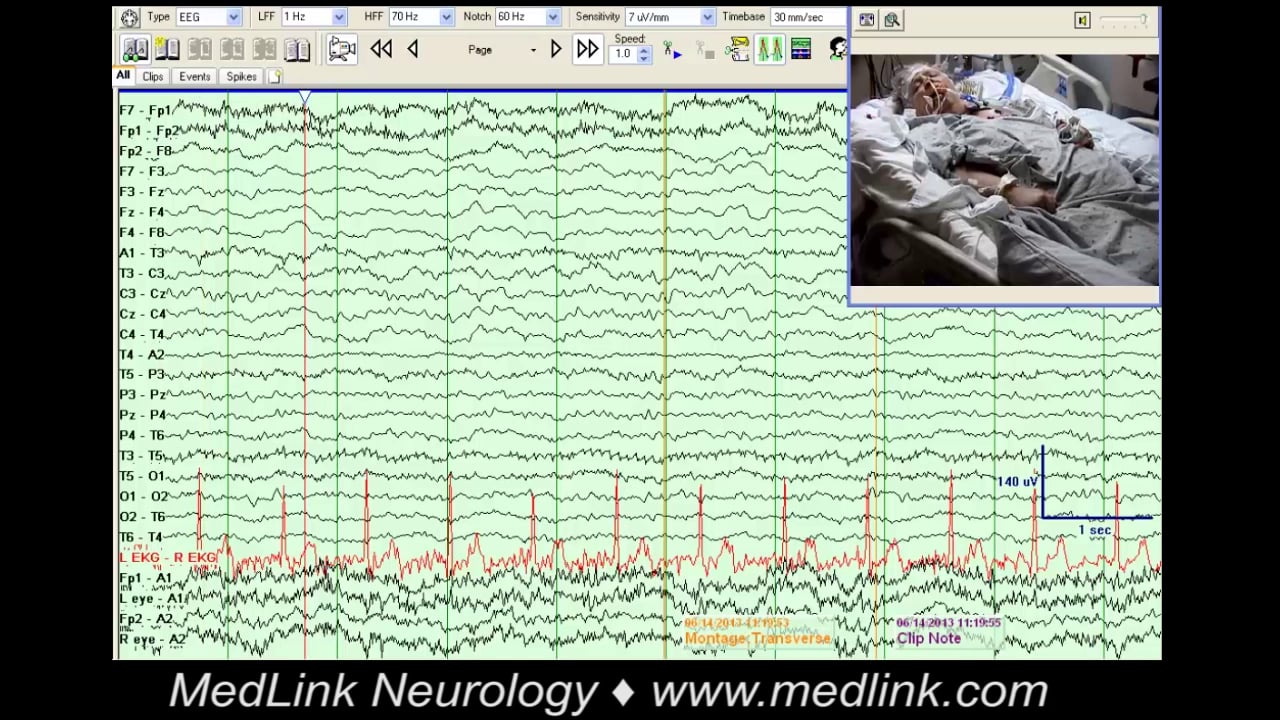
The initial diagnosis of seizure is based on the history. If first-line treatment fails, the diagnosis is (or should be) questioned and verified. At epilepsy centers, where selected challenging patients are seen, the evaluation typically begins with video-EEG monitoring, which allows a clear diagnosis in the vast majority of cases (10; 08). Typically, video-EEG will answer the following questions:
(1) Is it epilepsy or not?
(2) If it is not epilepsy, what is it?
(3) If it is epilepsy, what type?
(4) If seizures are focal, where is the focus?
In this article, we will focus on the first two questions. Is it epilepsy or not? If it is not epilepsy, what is it? In the vast majority of cases, the question of “epilepsy or not” is easily answered, so we will focus on the relatively small proportion of situations in which, despite good EEG or video-EEG recordings, the question remains difficult to answer. We will divide “ambiguous” events into clinical and electrographic events.
Cell phone videos can be particularly helpful at clarifying ambiguous events, and studies have shown excellent diagnostic value (27; 02).
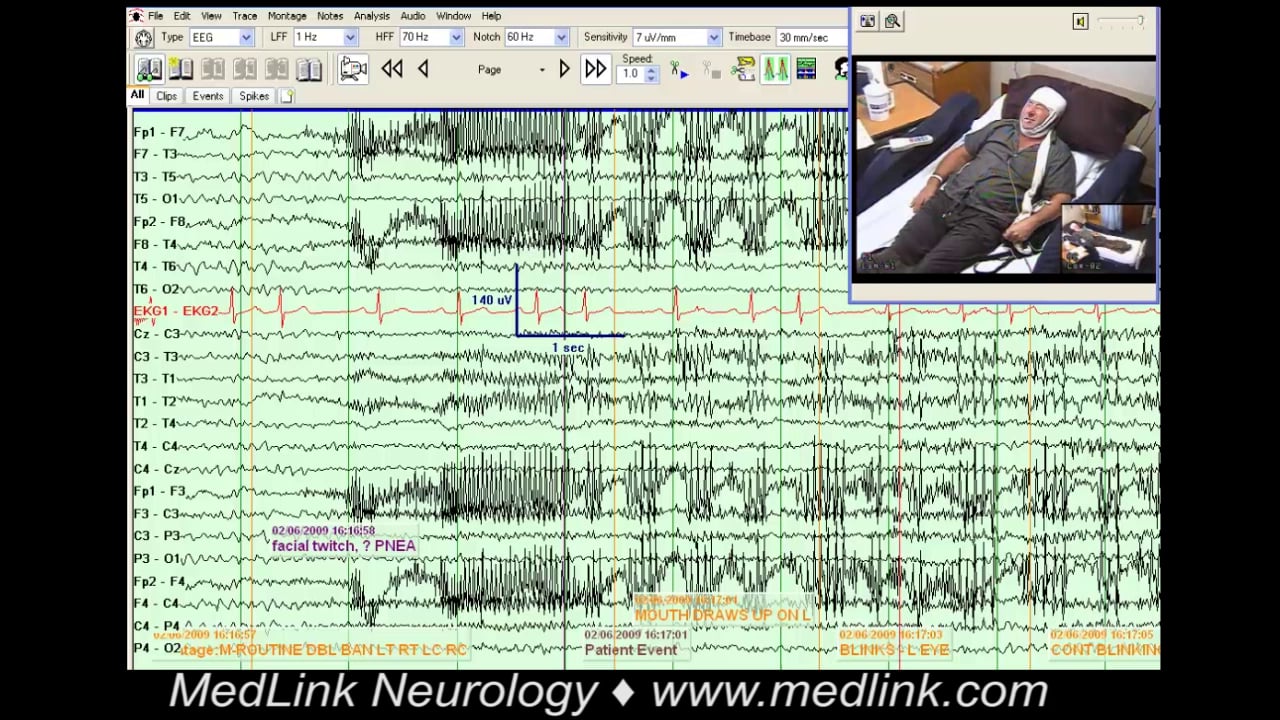
Facial movements. Mouth movements may be misinterpreted as seizure activity because partial seizures often include clonic facial twitching or oral automatisms. Nonepileptic facial movements can represent tics, hemifacial spasm, or other abnormal movements (04). Tics are brief and stereotyped in a given patient, and although they are worse under stress, they tend to occur regularly throughout the day rather than in discrete episodes. Tics are also suppressible by the patient with concentration. However, when suppressed, the urge builds up (like a compulsion), and the tic is eventually produced, triggering a brief feeling of “just right.” Tics may be related to involvement of the basal ganglia and related cortico-striato-thalamo-cortical circuits, and the dopaminergic neuronal system (25).
Hemifacial spasm can superficially resemble focal motor seizures, but the unilateral facial twitching typically affects the periorbital muscles initially, rather than the perioral area, and then spreads to other ipsilateral facial muscles over months or years. Unlike seizures, hemifacial spasms are sometimes suppressible by engagement in motor activity and can decrease during sleep (15). Hemifacial spasm is a progressive disorder that eventually results in fixed facial weakness or blepharospasm. It is related to hyperexcitability at the facial nucleus and brainstem structures (23).
Oculomasticatory myorhythmias are rare (though relatively common in Whipple disease) vermicular movements of masticator muscles accompanied by supranuclear gaze paresis or other central ocular manifestations (26).
Eye movements may at times be misinterpreted as seizure activity. Abnormal eye movements, like nystagmoid eye jerks, hippus, repeated blinking, and sustained eye deviation in any direction, are in fact an important clue in suspecting nonconvulsive status epilepticus in encephalopathic patients (18). Various nonepileptic eye movements are also often seen in this setting, eg, abnormal saccadic eye movement in hepatic encephalopathy and ocular bobbing in pontine lesions (20).
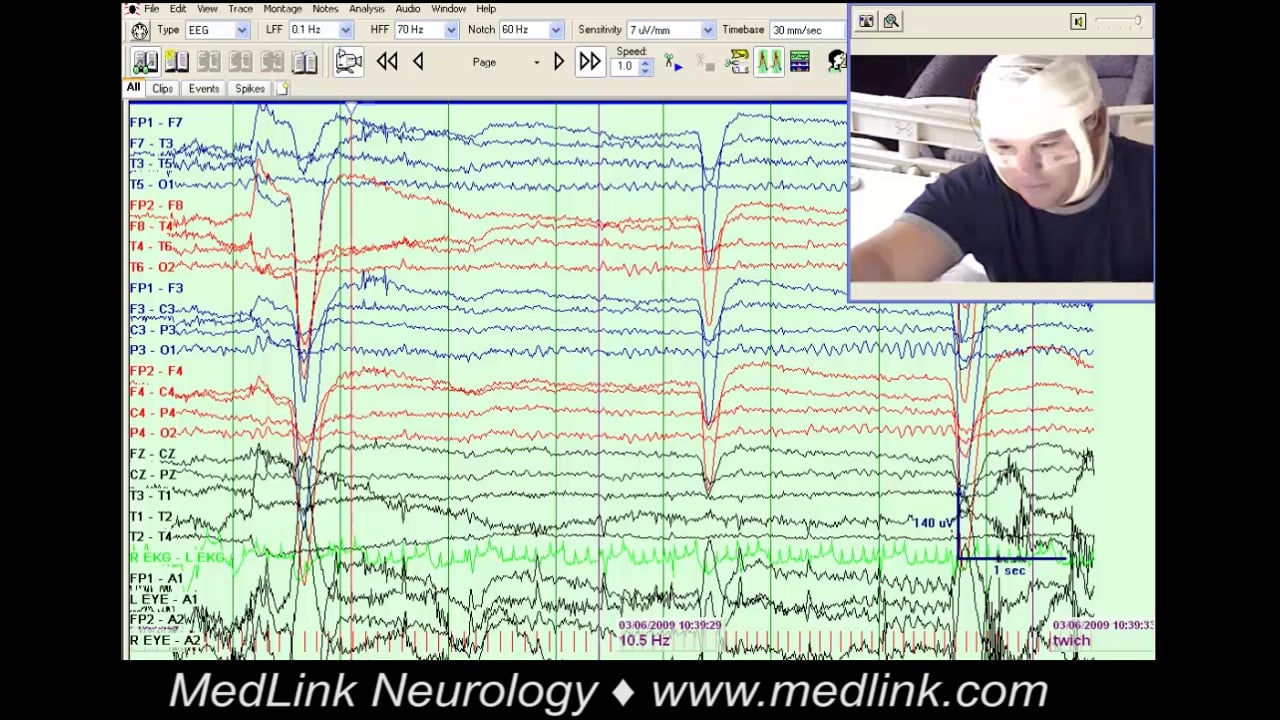
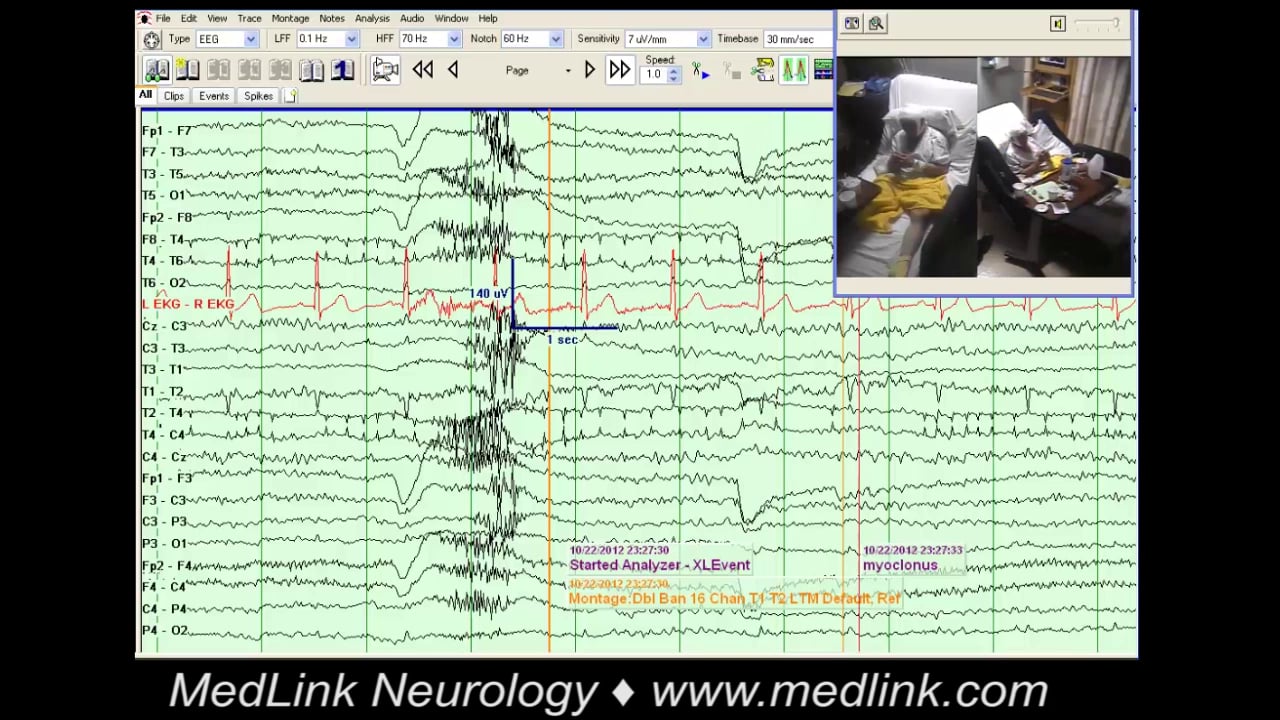
Brief isolated jerks. Myoclonus is a sudden, brief, involuntary movement caused by contraction or inhibition of muscle groups. Myoclonus can be epileptic (cortical) or nonepileptic (subcortical). The latter is mostly seen in patients with toxic (eg, medications) or metabolic (eg, uremia, electrolyte abnormalities, or cerebral anoxia) causes. Because they have large homunculus representation, epileptic clonic/myoclonic jerks typically involve distal limbs or the face, whereas nonepileptic myoclonus usually involves muscles with little homuncular representation.
For example, myoclonic jerks are frequently seen with cardiac arrest. Postanoxic myoclonus occurs soon after the inciting event and commonly displays EEG abnormalities, which can be epileptiform. Myoclonic jerks can also develop days or weeks after an anoxic injury (when a patient has regained consciousness) and be associated with epileptiform EEG changes as well (17). Postanoxic tonic eyelid openings (PATEO) are slower, tonic eyelid opening movements, which are preceded by EEG ictal activity and considered poor prognostic signs (01).
Hypnic jerks are a physiologic type of myoclonus that commonly occurs in the healthy population during the transition to N1 non-REM sleep. The person will often have the sensation of falling followed by a stereotyped body jerk. This is a benign and common occurrence and is easily identified by video-EEG, with absent EEG correlate associated with the jerk.
Segmental spinal myoclonus is associated with various spinal cord lesions, including neoplastic, infectious, traumatic, and B12 deficiency (28). The context (evidence for myelopathy) makes the diagnosis relatively easy. It may be caused by loss of inhibitory function of dorsal horn interneurons and abnormal hyperactivity of anterior horn cells of the spinal cord. Segmental myoclonus can be brainstem such as palatal myoclonus.
Out of sleep events. Several events can occur during sleep that may be confounding for seizures to family and providers. This includes periodic limb movements of sleep, and NREM and REM related parasomnias. Some differentiating characteristics in favor of seizures are short duration, stereotyped events, and presence of a tongue laceration. Age of onset can also be a clue. For example, NREM parasomnias frequently present in childhood and resolve by adulthood (14).
Limb shaking TIAs. Typically, sustained or transient hypoperfusion to the brain results in negative symptoms such as weakness, numbness, or communication difficulties. Limb shaking TIAs are an unusual phenomenon whereby positive symptoms, ie, involuntary rhythmic, jerky movements of an arm or leg, can occur in the setting of hypoperfusion from carotid stenosis. Episodes can reoccur several times a day with maneuvers that trigger hypoperfusion such as neck extension. In contrast to focal seizures, there is no involvement of the face, eyes, mouth, or Jacksonian march (22; 16).
Amyloid spells or transient focal neurologic episodes. These are brief, recurrent, and stereotyped events that can consist of negative or positive symptoms that can mimic migraines or seizures. These symptoms are thought to result from the irritant effect of hemosiderin on the cortex (12; 16).
Syncope. Syncope is a transient self-limited loss of consciousness due to transient global hypoperfusion and is mistaken for seizures when it is “convulsive.” The tonic or clonic movements are brief (less than 15 seconds) (21). EEG have very low diagnostic yield in evaluating syncope cause. Vasovagal syncope, arrhythmias, carotid hypersensitivity, and aortic stenosis are recognizable causes of syncope, as well as drugs (beta and alpha blockers) and metabolic causes (13).
Pseudosyncope. Pseudosyncope refers to episodes that look like syncope, but are psychogenic. Whatever the cause, syncope results in a predictable sequence of EEG changes when captured on EEG: high-amplitude slowing followed by suppression (29). Thus, a syncope-like event (complete loss of consciousness) with a normal alpha rhythm is diagnostic of psychogenic pseudosyncope. Because most patients with refractory syncope do not undergo video-EEG monitoring, it is likely that pseudosyncope is underdiagnosed and could account for a significant proportion of “syncope of unknown origin” (07).
Transient global amnesia. Episodes characteristically involve profound anterograde amnesia for several hours, or even up to a day. There is no loss of consciousness or loss of identity with this, and reoccurrence is not common. By contrast, seizures with loss of awareness are brief (less than an hour) and anterograde amnesia is not persistent after episode resolution (03; 16).
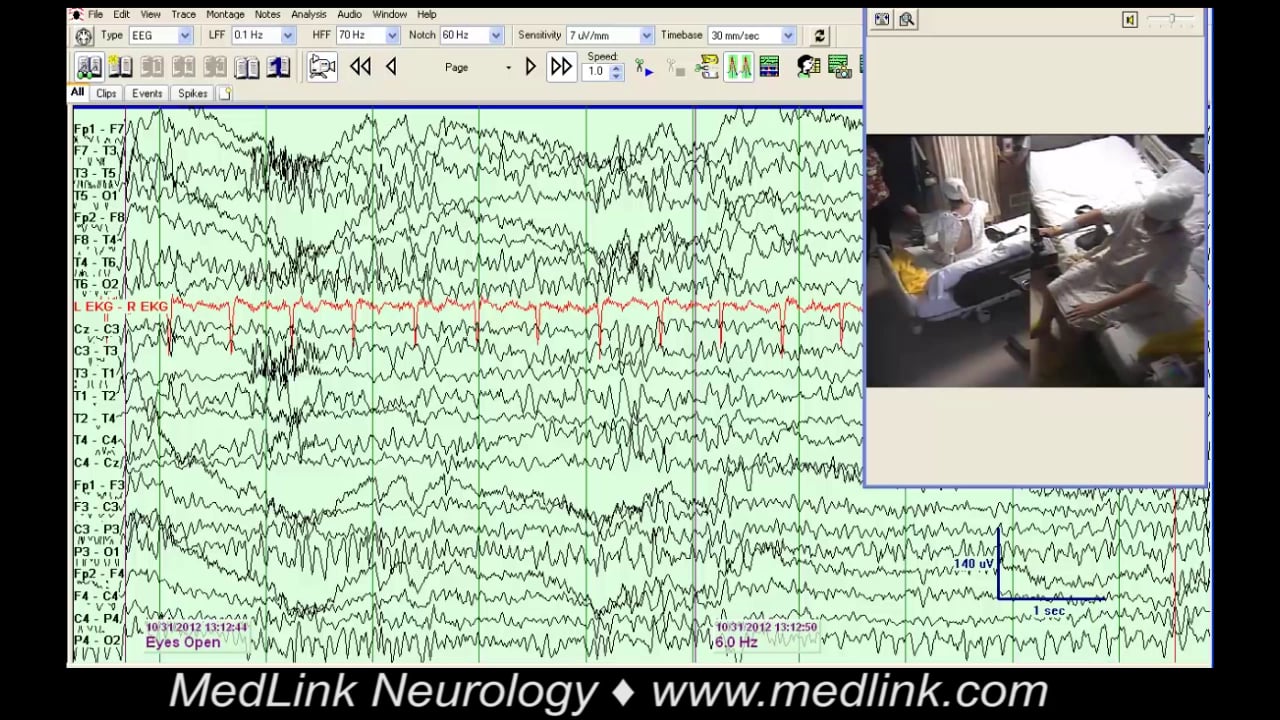
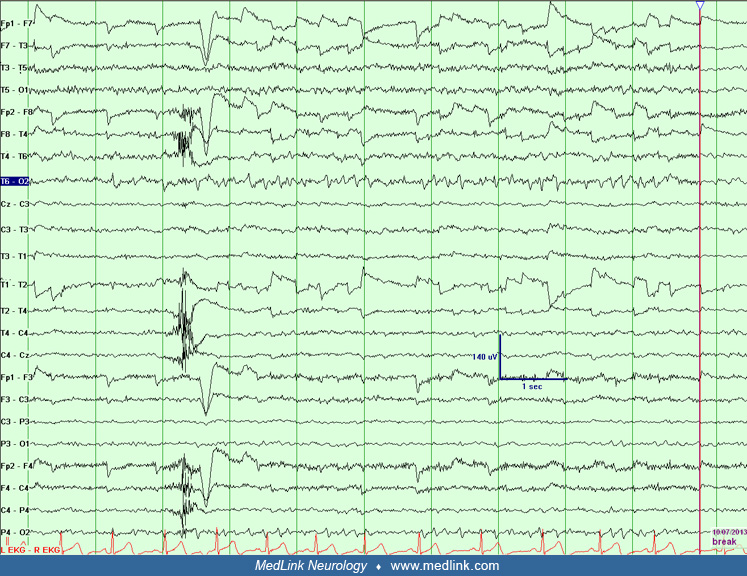
Focal motor seizures without EEG change. Because focal seizures in clear consciousness usually have no surface EEG change, the diagnosis cannot depend on the absence of ictal EEG. Thus, if symptoms are consistent with this type of seizure, semiology becomes more important than ictal EEG. In this situation, the diagnosis is entirely based on semiology (video) and whether the movements are the type seen in epileptic seizures (clonic or tonic).
Focal seizures with subjective symptoms (auras). These include common epileptic auras such as rising epigastric sensation, déjà-vu, and fear and usually do not show any ictal surface EEG discharge. Because they are also relatively common in patients without epilepsy, these symptoms can only be diagnosed as epileptic if the EEG shows epileptiform discharges or if they evolve into more obvious seizures (the company they keep). Less specific symptoms (cephalic, “indescribable” sensations) are even more difficult to diagnose and, when in doubt, should not lead to a diagnosis of epileptic seizures.
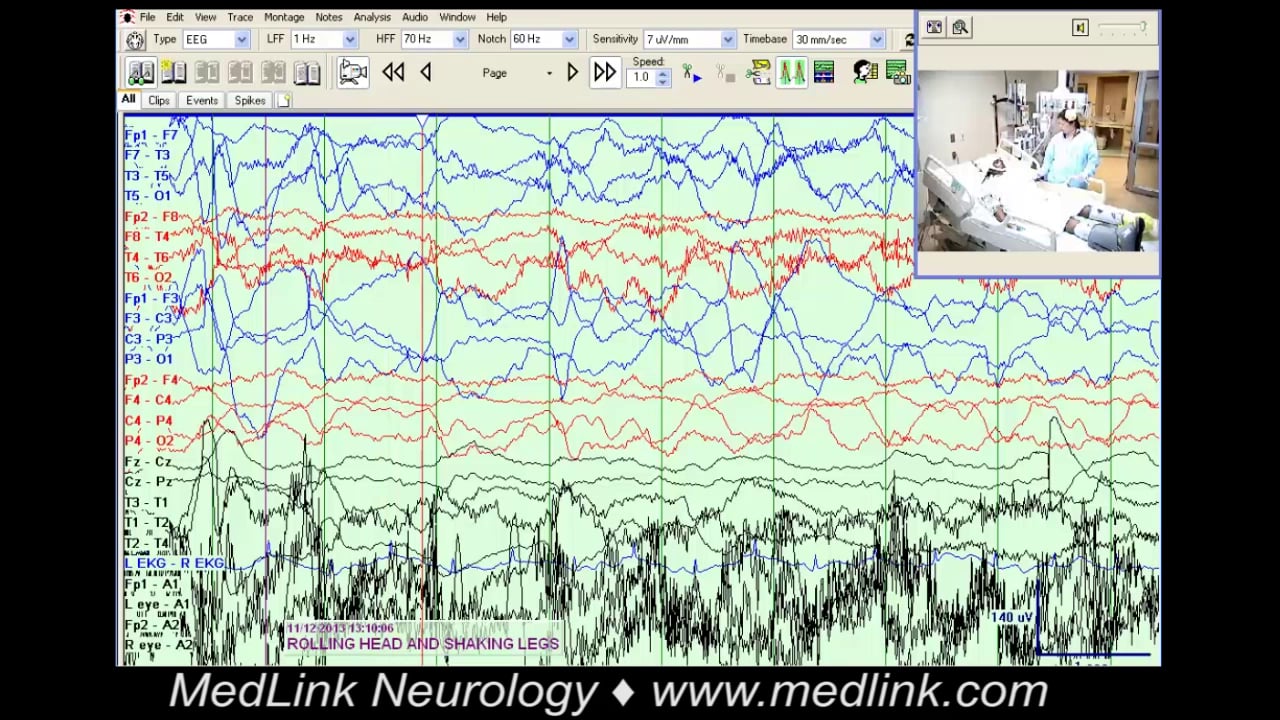
In the ICU setting. Patients often have various movements or behaviors that are not epileptic, but can superficially mimic seizures.
Decorticate or decerebrate posturing typically occur in response to noxious stimuli. Decorticate posturing occurs when there has been interruption to the corticospinal pathways above the midbrain. Clinically, the patients will have adduction and slow flexion of the arms, wrists, and fingers in the upper extremities. In the lower extremities, there will be extension, internal rotation, and plantar flexion. Decerebrate posturing occurs with brainstem damage below the level of the red nucleus. Clinically, patients may have extension of the head and trunk (opisthotonus); arms will be adducted, extended, and internally rotated; and legs will be extended and internally rotated, with plantar flexion and inversion of the feet (05).
Tremors or shiver-like movements are relatively frequent in the ICU setting or in patients coming out of general anesthesia. One key to distinguishing tremors is that a tremor is a to-and-fro oscillating movement across a joint. Tremors are not tonic, clonic, or myoclonic in nature.
Wickets waves. Wickets waves are 6 to 11 Hz medium- to high-voltage sharp transients in the temporal regions. They do not clearly stand out and arise from ongoing activity of the same frequency. These are, by far, the most common benign waveforms misinterpreted as epileptiform and are often responsible for the erroneous diagnosis of epilepsy (11; 05).
Lambda waves and positive occipital sharp transients of sleep (POSTS). Both are occipital and have a similar morphology. Lambda waves occur during visual scanning, whereas POSTS occur during non-REM sleep.
Small sharp spikes (SSS). SSS are sporadic unilateral or bilateral temporal spikes that occur during light sleep. They are “small” (< 50 microV) and “sharp” (< 50 msec), and are known as benign epileptiform transient of sleep (BECTS).
Subclinical rhythmic electrographic discharge of adults (SREDA). SREDA typically consists of rhythmic theta activity over the posterior temporoparietal region lasting for many seconds to several minutes, but without the evolution typical of focal seizures. This is a pseudoictal pattern.
Rhythmic midtemporal theta of drowsiness (RMTD). RMTD, also known as “psychomotor variant,” are 4 to 7 Hz rhythmic discharges, maximum in the midtemporal region, unusually unilateral, and, again, without evolution. The morphology is typically notched, flat-topped, or sharply contoured. Bursts last for 1 to 30 seconds.
Breach rhythm. Breach rhythm consists of high-voltage activity over a skull defect and can contain sharp transients that can mimic interictal epileptic discharges. However, they are usually accompanied by a baseline amplitude asymmetry (09).
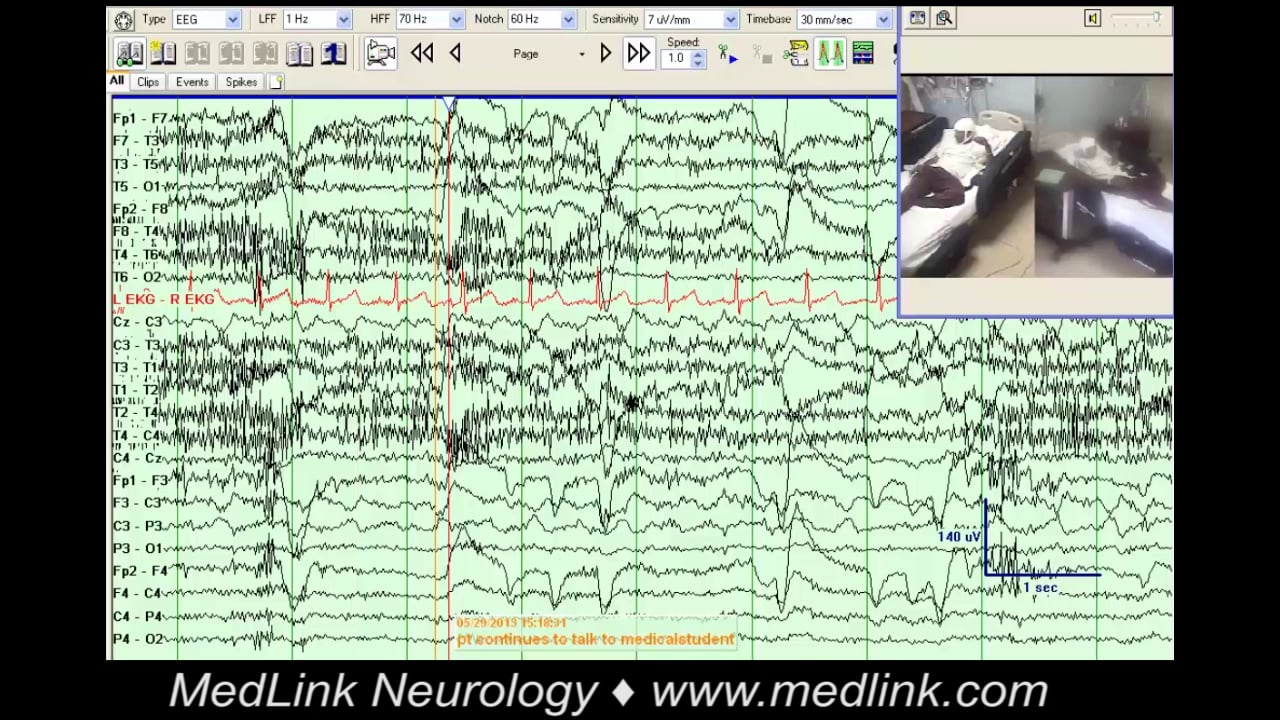
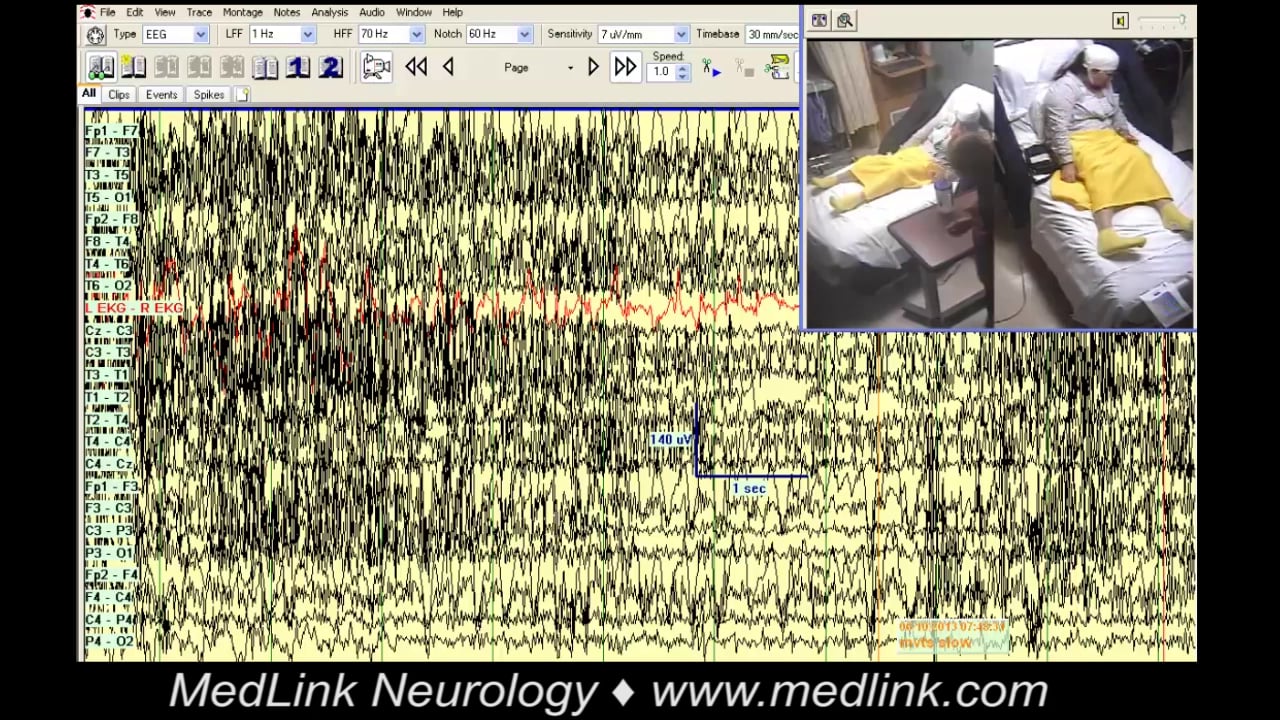
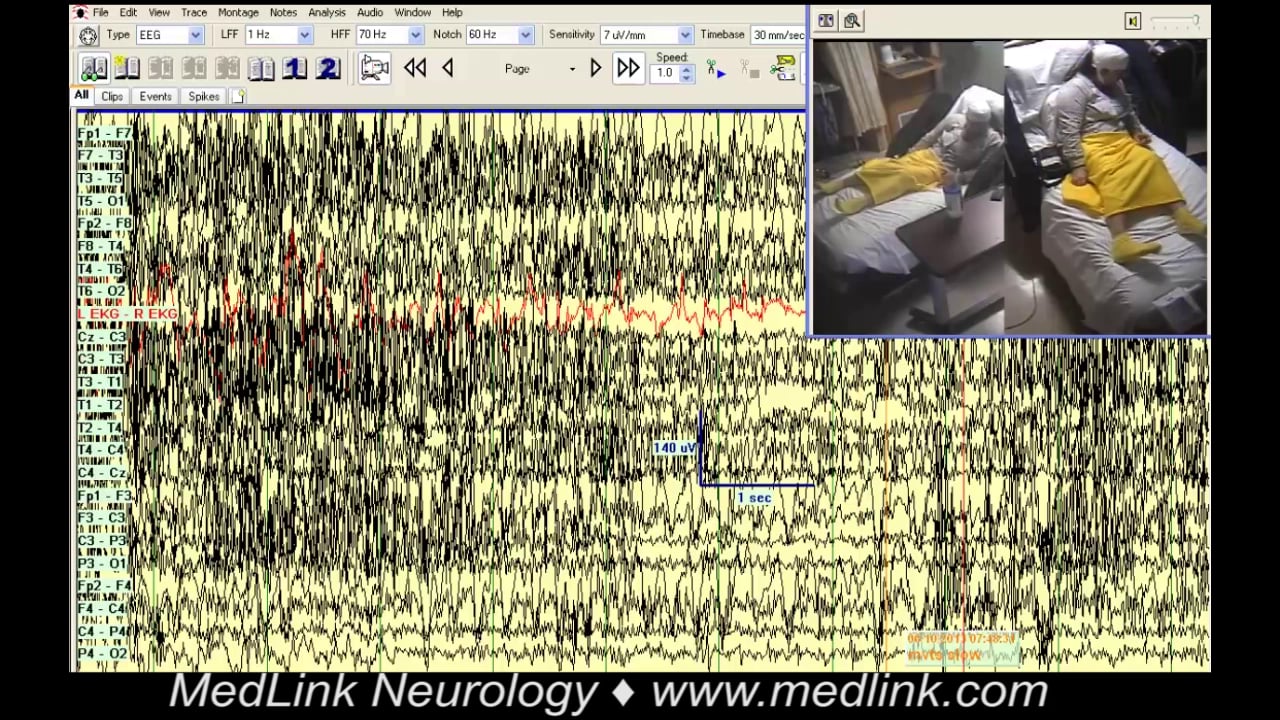
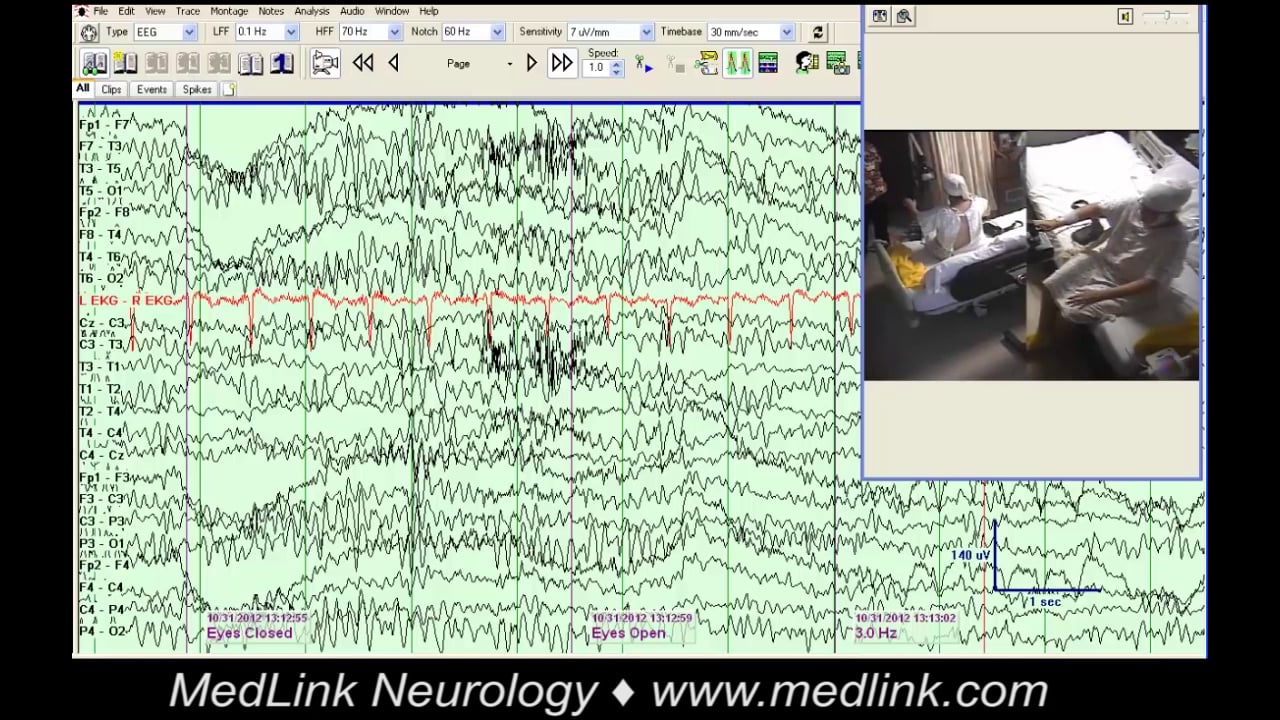
Artifacts due to rhythmic movements (voluntary or tremors) are usually easily clarified by review of video.
Hyperventilation can produce diffuse slowing during hyperventilation in healthy patients, and this may be prolonged in the context of hypoglycemia or hypoxia. Slowing may persist after the termination of hyperventilation in patients with syncopal episodes. Slowing can rebuild after hyperventilation in Moyamoya disease.
A harmonic of a normal alpha rhythm can occasionally generate a rhythmic discharge that mimics seizures, although there is no evolution. This discharge is identified by the fact that the rhythmic activity is half or twice the alpha frequency.
Periodic lateralized epileptiform discharges (PLEDs), generalized periodic epileptiform discharges (GPEDs), and other generalized patterns such as triphasic waves are easy to identify and are only “ambiguous” in terms of their significance, ie, ictal, interictal, or nonepileptogenic. PLEDs and GPEDs are EEG discharges, usually epileptiform in appearance, that occur at a relatively constant periodic interval. In most cases, PLEDs are caused by acute focal destructive structural lesions (most commonly stroke). GPEDs can be due to severe metabolic disturbances, including anoxia, and can be indicative of nonconvulsive status epilepticus. In practice, whether a continuous generalized periodic pattern represents status epilepticus will usually require a very careful clinical assessment, CT/MRI, and other investigations (04). PLEDs that evolve or are associated with rhythmic fast, or sometimes rhythmic delta, activities (PLEDS-plus) are strongly associated with clinical seizures and status epilepticus (24).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Priyanka Atit DO
Dr. Atit of University of South Florida has no relevant financial relationships to disclose.
See ProfileSelim R Benbadis MD
Dr. Benbadis of the University of South Florida and Tampa General Hospital received honorariums from Catalyst, Jazz, LivaNova, Neurelis, SK Life Science, Stratus, and UCB as consultant, speaker, or advisory board member. He received grant support from Cerevel Therapeutics, Elsai, Jazz, LivaNova, Longboard, Marinus, Neuropace, SK Life Science, Takeda UCB, and Xenon Pharmaceuticals.
See Profile
Jerome Engel Jr MD PhD
Dr. Engel of the David Geffen School of Medicine at the University of California, Los Angeles, has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Dec. 23, 2024
Epilepsy & Seizures
Dec. 03, 2024
Epilepsy & Seizures
Dec. 03, 2024
Epilepsy & Seizures
Nov. 11, 2024
Epilepsy & Seizures
Nov. 04, 2024
Epilepsy & Seizures
Oct. 14, 2024
Epilepsy & Seizures
Oct. 04, 2024
Neuro-Oncology
Oct. 03, 2024