
Stroke & Vascular Disorders
Neoplastic and infectious aneurysms
Dec. 29, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Aortic atherosclerotic plaques are recognized as significant contributors to cerebral infarction, with occurrences both spontaneous and iatrogenic, particularly during perioperative periods. The presence of large and complex atheromas increases the risk of cerebral infarction. Management strategies include addressing modifiable risk factors and considering antiplatelet therapy or anticoagulation. However, the effectiveness of these interventions awaits clarification through further studies to establish clear treatment protocols.
|
• Aortic arch atherosclerosis is a known cause of ischemic stroke. | |
|
• Plaques measuring 4 mm or greater and lipid rich core carry the highest risk of stroke, as compared to calcified plaques. | |
|
• Stroke often tends to be right hemispheric due to the location of plaque within the aorta. | |
|
• Specific guidelines regarding antiplatelet versus anticoagulation therapy are still underway; however, the usual treatments for ischemic stroke, such as antithrombotic therapy, statin therapy, and lifestyle changes, are recommended. |
Stroke is the fifth leading cause of death in the United States. Of the 795,000 strokes occurring annually in the United States, 87% are ischemic stroke and 10% are hemorrhagic stroke (106).
Atherosclerosis is a diffuse systemic vascular disorder affecting large and medium-sized arteries, causing patchy intimal plaques known as atheromas.
Aortic atheromatous plaques were first identified as a possible cause of stroke in the early 1990s, when transesophageal echocardiographic examination of three patients with cryptogenic stroke to identify potential cardiac sources demonstrated the presence of "large, protrusive plaques. . . with mobile projections that moved freely with the blood flow" (108). This was followed by a larger study in 1991 that demonstrated a higher incidence of embolism when aortic plaques had mobile elements (48). The association of aortic atheroma and stroke was first described by Amarenco and colleagues in a landmark autopsy study of 500 patients with cerebrovascular and other neurologic diseases. The prevalence of ulcerated plaques is 26% in patients with cerebrovascular diseases compared to 5% among patients with other neurologic diseases. Ulcerated plaques were present in 61% of cryptogenic cerebral infarcts compared to 22% with a known cause (06). Plaques that were at least 4 mm in thickness were found to be an independent risk factor for ischemic stroke (04; 71; 70).
Clinical manifestations are based on the system involved: (1) neurologic, including stroke and transient ischemic attack; and (2) peripheral organs, including renal, gastrointestinal, and limb ischemia.
The underlying mechanisms involved include (1) atheroembolism, the rupture and embolism of an unstable plaque, which is often acute in presentation and associated with ischemia; and (2) cholesterol embolism, the dislodgement and embolism of cholesterol crystals into small arteries, which is often subacute in presentation and associated with inflammation.
There is evidence of a higher incidence of stroke lesions in the right hemisphere as compared to the left hemisphere. This is due to the anatomical pattern and branches of the internal carotid system. Aortic emboli originate and travel through the right common carotid artery, which branches off directly from the brachiocephalic trunk (innominate artery) on the right side, leading to a more direct pathway to the right cerebral hemisphere.
In contrast, cardioembolic sources typically travel through the left side of the heart and into the systemic circulation. However, the left common carotid artery branches off directly from the aortic arch, and the left internal carotid artery supplies the left hemisphere.
Prognosis with regard to vascular events, subsequent stroke, or mortality is a function of plaque (size and morphology) and other associated comorbidities, including atrial fibrillation and atherosclerosis in other vascular beds.
Plaque size. In the French Study of Aortic Plaques, the recurrent stroke rate and vascular event rate was 12% and 26%, respectively, in the group with plaques greater than 4 mm, compared to 2.8% and 6% in those with plaques less than 1 mm, respectively (odds ratio 3.9 for plaques 1 to 3.9 mm, 13.8 for plaques greater than 4 mm) (08). Similarly, mortality was significantly higher in the group with plaques greater than 4 mm, compared to those with plaques 1 to 3.9 mm, and those with plaques less than 1 mm. Other groups have reported similar results (70; 24).
Plaque morphology. The highest risk for embolic stroke is found when aortic atheromas have mobile components, are hypoechoic (reflecting a lipid-rich core), or are ulcerated (21; 101).
Atrial fibrillation. The risk of stroke in patients with atrial fibrillation is significantly increased when associated with aortic atheroma. The Stroke Prevention in Atrial Fibrillation study, which examined the outcome of patients with high-risk nonvalvular atrial fibrillation (greater than 75 years, hypertension, previous stroke), included 382 patients who underwent transesophageal echocardiography. In the 35% of patients with complex aortic atheroma on transesophageal echocardiography (greater than 4 mm, mobile, ulcerated) the risk of stroke during one year ranged from 12% to 20%. In contrast, it was only 1.2% in patients without aortic atheroma (09). This discrepancy in stroke risk suggests a potential role of aortic atheromas in the mechanism of stroke even in patients with atrial fibrillation.
Coexisting hypercoagulable states. Thromboembolism appears to be much more frequent than atheroembolism in patients with severe aortic arch plaques, with a frequency reported to be as high as 33% at 1 year, compared with only 0.7% for atheroembolism. It is, therefore, conceivable that the coexistence of a hypercoagulable state in a patient with aortic arch plaque may increase the likelihood of superimposed thrombus formation and further enhance the embolic potential of the plaque. The APRIS study suggested a role for coagulation activation in the stroke mechanism on the basis of finding elevated prothrombin fragment F 1.2 an indicator of thrombin generation (27).
Atherosclerosis in other vascular bed. Patients with carotid artery disease often exhibit concurrent aortic arch atherosclerosis, increasing the risk of embolic events to the brain. The incidence of ascending aortic atherosclerotic plaques was 62.9% in the overall population and increased to 82.8% in those with carotid atherosclerotic plaques. Additionally, there was a progressive rise in the percentage of patients with aortic plaques with increasing severity of carotid atherosclerosis (47). Patients with severe aortic stenosis showed a 47% prevalence of severe, complex aortic plaque, contrasting with 9% in controls. Nonobstructive aortic valve calcification correlated with aortic plaque in 86% of cases versus 30% in controls (118).
The presence and characteristics of aortic plaque have significant prognostic implications across vascular beds, emphasizing the importance of screening and management. Hypertension in individuals with aortic plaque may be due to renal artery stenosis, emphasizing the need for screening in such cases. Severe thoracic aortic plaque is correlated with abdominal aortic aneurysm, suggesting a need for abdominal aortic aneurysm screening in patients with significant thoracic plaque (84).
A 70-year-old, right-handed man with no prior medical history presented to the emergency room with a history of recurrent, transient left arm numbness. He had also experienced two transient episodes of left homonymous visual field deficits in the preceding week. He smoked two packs of cigarettes per day for at least 50 years.
Examination showed a blood pressure of 152/70 mm Hg, with a regular heart rate at 60 beats per minute. Language and memory were intact. Visual field examination was unremarkable. Motor examination showed a left pronator drift with reduced rapid alternating movements but intact strength on formal muscle testing. Gait and cerebellar examinations were normal, and there was no sensory loss.
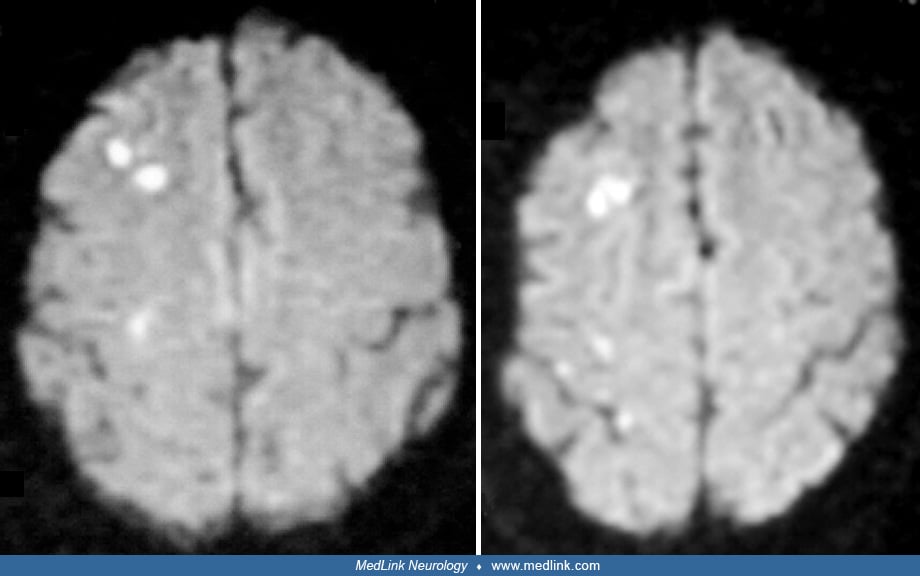
ECG showed normal sinus rhythm. CT of the head without contrast was normal. MRI of the brain demonstrated several small white matter lesions in the deep right middle cerebral artery/anterior cerebral artery watershed arterial territories on diffusion-weighted imaging and FLAIR sequences.
MR angiography of the intracranial vessels showed no hemodynamically significant stenosis. Carotid duplex ultrasound showed minimal atherosclerotic disease bilaterally in both the proximal internal and distal common carotid arteries. Transthoracic echocardiogram was normal. Transesophageal echocardiography revealed a large 1.2 to 1.5 cm plaque in the ascending aortic arch without ulceration or mobility.
Atherosclerotic changes of the aorta occur as early as during the third decade of life and precede those of the coronary, cerebrovascular, and peripheral arteries. Plaque initiation and progression is a complex process initiated locally and modulated by various systemic, hemodynamic, and biological factors (124). Wall shear stress, defined as the frictional force exerted by the flowing blood on the vessel wall, plays a pivotal role in atherosclerosis. Low wall shear stress has been implicated in the initiation of plaque formation (20). Conversely, increased shear stress has an atheroprotective effect. The mechanical effect of lower shear stress alters gene expression in the endothelial cells triggering an inflammatory cascade and increased expression of adhesion molecules (112). LDL influx is high in areas of low wall shear stress. Accumulated LDL undergoes oxidation and initiates an inflammatory response by activating monocytes (through the expression of monocyte chemoattractant protein) and differentiation of monocyte to macrophage (35; 76). Macrophages, in turn, engulf modified LDL forming cholesterol laden foam cells and also secrete cytokines IL-1 and TNK-alpha, stimulating expression of adhesive molecules and, in turn, recruiting more monocytes, thus, propagating the cycle of inflammation (39; 12). The secretion of growth factors and metalloproteinases by the macrophages also results in cell proliferation and matrix degeneration, making the plaque unstable and prone to rupture (110).
The protective effect of HDL stems from its ability to promote an efflux of cholesterol from foam cells (72) and the inhibition of oxidative modification of LDL (66) by transporting antioxidants like paraoxonase (67) and apolipoproteins Apo-A1 and Apo-A2, which have intrinsic antioxidant properties (36). HDLs also inhibit cytokine and C-reactive protein–induced expression of adhesion molecules by endothelial cells (120; 115). HDL levels and Apo B/A-I ratio have been shown to be the strongest predictors of atherosclerotic plaques (53). Therapies aimed at increasing HDL levels will be highly effective in preventing plaque change.
The causal relationship between characteristic features of aortic atheromas and stroke is now well established. Various characteristics of plaque size and thickness, morphology, location, and progression have been studied.
Grading of aortic plaques (plaque size/thickness). The thickness of atheromas has a direct correlation with the risk of embolic vascular events. The risk of a neurologic event is 1.7 times higher for severe atherosclerosis than mild-to-moderate disease (24). At present, no universal grading system exists, with some authors describing plaques 5 mm in thickness as complex plaques (49; 104; 111) and others using a thickness of 4 mm as the criterion (34).
In 1996, a classification of aortic plaques based on plaque morphology as visualized by transesophageal echocardiography was proposed by Montgomery and colleagues (73).
|
Grade |
Morphology |
|
I |
Normal intima |
|
II |
Minimal intimal thickening |
|
III |
Atheroma less than 5 mm in thickness |
|
IV |
Complex protruding plaque 5+ mm in thickness |
|
V |
Mobile plaques irrespective of thickness |
On the contrary, an analysis from the Stroke Prevention: Assessment of Risk in a Community (SPARC) study reached a different conclusion, stating that complex aortic plaques (> 4 mm or mobile) did not significantly increase the risk of cerebrovascular events after adjusting for age, sex, and other clinical risk factors.
Definition of aortic plaques. Unstable or complex plaques are more frequently echolucent, heterogeneous, and noncalcified with or without mobile elements, and they are more prone to rupture. Mobile elements of the plaque are often referred to as aortic debris, superimposed thrombi, or complex plaque (27). Plaques with mobile elements are classified as complex, regardless of the plaque thickness. A nomenclature has been proposed for plaques in the coronary circulation. “Culprit” plaques refer to those causing the acute vascular event whereas “vulnerable” plaques refer to those plaques that have the potential to transform into culprit plaques. This classification aims to define plaques based on their potential to undergo acute change, which is dependent on morphology and plaque composition (74). A similar classification for aortic arch plaques would be of use in predicting future vascular events.
Plaque progression, such as the fibrous cap thickness, amount of lipid core, and the degree of active inflammation, play a role in determining plaque vulnerability.
A follow-up transesophageal echocardiographic study of patients with aortic atheroma over a period of 12 months reported an overall stability in the disease process, with close to 61% having the same atheroma grade at the end of the study period. Although none of the patients with atheromas smaller than 5 mm developed mobile lesions, 62% of those with more severe grades developed new mobile lesions. However, 70% of mobile lesions identified at baseline evaluation resolved spontaneously. Whether this is due to embolism of the mobile fragment or due to the healing process is uncertain. Therefore, though the overall disease process is stable, individual lesions are unpredictable and dynamic, demonstrating progression and regression over time (73).
Aging of the vasculature results in increased expression of proinflammatory transcription factors like nuclear factor (NF)-kappaB and decreased protective factors like hypoxia inducible factors, resulting in increased production of inflammatory cytokines (123). In addition, microbiological infection of the vessel wall triggers inflammation by direct cytopathogenicity, bystander effects, epitope spreading, and molecular mimicry (65).
Further progression of the disease process is also influenced by systemic factors like cigarette smoking, hypercholesterolemia, diabetes mellitus, and genetic influences. With further progression of the disease process, vascular smooth muscle cells and myofibroblasts migrate and deposit extracellular matrix, forming the fibrous cap. The oxygen-deprived central core contains extracellular lipids, cholesterol esters, and sometimes calcifications (15; 88). As the atherosclerotic process encroaches into the aortic lumen, the luminal diameter is preserved with the vessel wall undergoing outward remodeling. Thus, a normal lumen contour during an angiogram could be masking a severe atherosclerotic process (81). Vulnerable plaques typically have a thin fibrous cap, a larger lipid core, an increased number of inflammatory cells, and increased neoangiogenesis. The central role of inflammation has always raised the possibility of using inflammatory markers to detect disease progression. C-reactive protein has been shown to play an important role by decreasing eNOS-mediated dilatation in vivo. Maternal levels of C-reactive protein have been shown to predict atherosclerosis in children of hypercholesterolemic mothers (63). Serum amyloid A has been shown to increase proteoglycan synthesis, leading to increased LDL proteoglycan-binding affinity (119).
The potent amalgamation of inflammation, oxidized LDL, and vascular ageing results in plaque vulnerability to rupture. Local expression of matrix metalloproteinases and collagenase combined with smooth muscle apoptosis predispose to plaque rupture. Plaque rupture occurs at the plaque shoulder where mechanical strain is maximum, resulting in exposure of procoagulant factors like tissue factor (68). This activates the coagulation cascade, leading to superimposed thrombus formation and systemic embolism.
Plaque distribution. Distribution of clinically significant atherosclerotic plaques on the aorta varies depending on the location. The portion of the aorta upstream to the take-off of the left subclavian artery has the highest potential for atheroembolism leading to stroke. The ascending aorta is the least involved segment of the thoracic aorta in the atherosclerotic process (Barbut and Gold 1996; 82; 02). This proximal-to-distal gradient could be a reflection of the hemodynamics peculiar to the aorta. If complex plaques (greater than 4 mm) are found in the proximal thoracic aorta rather than the descending aorta, the odds of stroke increase from 1.5 to 13.8 (04).
Anomalies of the aortic arch are not infrequent and are associated with increased stroke events during carotid stenting procedures. This is due to increased technical difficulties secondary to distorted aortic arch and branching vessel anatomy (32). In the most frequent aortic arch variant, the left common carotid and innominate arteries share a common origin from the aortic arch. Rarely, the left common carotid may take origin directly from the innominate artery and is the second most common variant. Both variants are referred to as the bovine aortic arch, which is, in fact, a misnomer. The aortic arch in cattle has a single brachiocephalic trunk arising from the arch, which gives rise to both subclavian arteries and a bicarotid trunk (60).
Studies of embolic stroke following heart surgery have contributed significantly to understanding the role of aortic plaques. Aortic manipulation during coronary artery bypass grafting is considered to be one of the main causes of embolic stroke in the postoperative period. Patients with atheromatous change of the ascending aorta have increased incidence of postoperative stroke and a decreased 5-year stroke-free survival (113). Aortic debris collected from coronary catheters after advancement into the ascending aorta show signs of plaque disruption in up to 55% of plaques, with large lumen catheters having increased incidence of aortic debris (29).
More than 50% of neurologic events following cardiac catheterization occur in the posterior circulation (26), indicative of a predisposition of the posterior circulation to vascular insults. Early postoperative stroke is defined as stroke occurring within the first 24 hours of surgery or when the patient wakes up from anesthesia with a neurologic deficit. Delayed stroke refers to a new deficit after an initial normal recovery up to 30 days postoperatively. Aortic atherosclerosis can cause both types of stroke, being more significant in early strokes (43). Early postoperative stroke may present with multiple infarcts, secondary to a shower of emboli from aortic manipulation, whereas delayed strokes usually have single territory infarcts associated with fibrillation episodes (11).
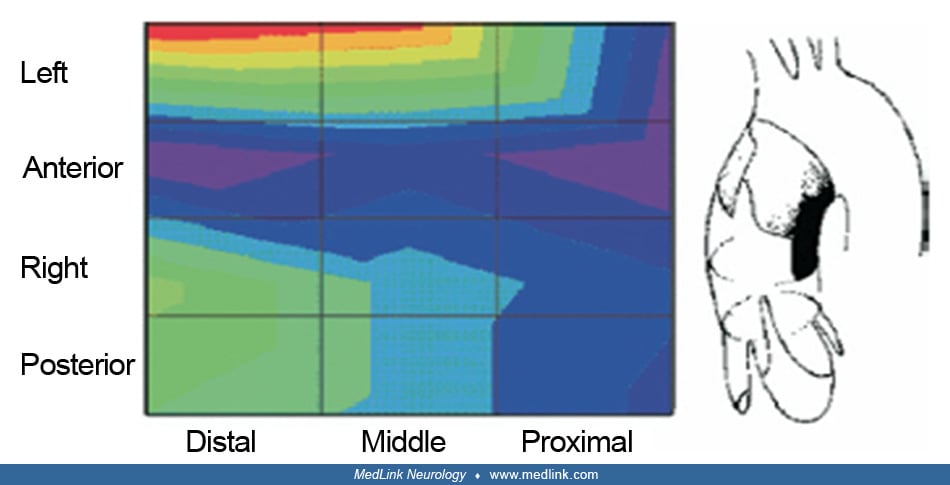
Further studies have shown that involvement of the distal ascending aorta increases the stroke risk 5-fold. This is also the site where surgeons commonly place the aortic clamp. Another independent predictor of postoperative stroke is involvement of the middle lateral segment of the ascending aorta (114). This could be due to the altered hemodynamics secondary to the aortic arch anatomy, with higher blood flow velocities in the lateral aspect. Thus, the lesions in the lesser curvature of the ascending aorta are associated with higher stroke risk. Nevertheless, plaques from the descending aorta have been shown to embolize to the left subclavian artery during periods of retrograde blood flow, causing infarctions in the posterior circulation (41). In a study of patients with acute stroke by transesophageal echocardiogram and 3D MRI, retrograde flow was observed in as much as 31.7% of patients (41) with the average retrograde flow being 26 mm. The capacity of this flow to transport debris from plaques in the descending aorta to the left subclavian artery, leading to infarcts in the posterior circulation, cannot be overlooked (113).
Pathophysiology. Embolism from the aortic arch can be either due to thromboemboli from aortic mural thrombi secondary to plaque disruption with superimposed thrombosis or due to atheroemboli leading to cholesterol embolization. The more significant of these in relation to stroke appears to be thromboemboli. The frequency of thromboembolic episodes was 33% at a mean follow-up duration of 14 months in 42 patients with protruding aortic plaques (109). The incidence of emboli has a direct correlation with the grading of atheroma. One in three atheromas greater than 5 mm in thickness cause systemic emboli (93). This association was also demonstrated in a study of 335 patients undergoing transesophageal echocardiogram with the odds ratio for embolism increasing from 4 to 9.7 for grade 2 and 3 atheromas respectively (71). In another study, complex aortic plaques were more likely to be associated with small cortical infarctions than large artery atherosclerosis and cardioembolic etiologies. In addition, a subcortical pattern was more common in those with complex aortic plaque than those with cardioembolic mechanisms (51).
The prevalence of ulcerated plaques is three times higher in cases of cryptogenic stroke, compared to patients with known cause (06). In another study of 49 patients with cryptogenic stroke, transesophageal echocardiogram showed a high incidence of thoracic aortic atheroma of 46.9%, with microembolic signals being detected by transcranial Doppler in three of 10 patients with complex plaques (19). The prevalence rate of aortic plaques in a community screening of random individuals over 45 years of age for stroke prevention approached 51% (7.6% being complex plaques) (02). In another study, the prevalence of aortic arch plaques was greater in patients with severe aortic stenosis as compared to age- and gender-matched control subjects (74% vs. 41%) (97). Patients with significant intracranial atherosclerotic disease are more likely to have aortic arch atherosclerosis than those without (60.9% vs. 49.0%) (45). In a population-based cohort, aortic arch atherosclerosis was associated with an increased burden of white matter disease on MRI in people without known clinical stroke (107).
Ethnic differences are also present, with whites having a higher plaque burden and increased complex plaques compared to African Americans even though they had less severe arterial hypertension and diabetes mellitus (38). Another study demonstrated increased plaque burdens found in Jewish patients as compared to Arabic patients, but no differences were noted in the distribution of plaques by location or complexity (100). Gender differences have also been shown to exist. The established aortic plaque thickness of 4 mm for increased stroke risk may not hold true for both men and women. Plaque thickness between 3 and 3.9 mm was also associated with increased stroke risk in women (28). The reason for this remains unclear, with the influence of varied lipid profiles and inflammatory markers playing a possible role.
Traditional risk factors for atherosclerosis such as age, hypertension, dyslipidemia, and smoking have been associated with aortic atheroma (01; 02; 105). Tribouilloy and colleagues reported that hyperhomocysteinemia is not only an independent risk factor for aortic arch atheroma but also for atheroma progression (105; 92). In a cross-sectional study of 145 stroke-free patients, leukocyte count correlated with aortic arch plaque thickness in accordance with the inflammatory component of atherosclerosis (31).
Transesophageal echocardiography. Transesophageal echocardiography (TEE) has traditionally been the preferred modality of choice in the assessment of the thoracic aorta. Other modalities such as CT and MRI have generally been considered complementary to the TEE.
Advantages. The proximity of the transducer with the aorta when placed in the esophagus has made measurement and grading of atheroma and detection of mobile elements with a high degree of accuracy.
TEE can predict plaque composition, including plaque calcification.
The predictive power of TEE in detecting atheromas in the nonvisualized portions of the thoracic aorta has shown that TEE is an effective tool to rule out disease in the ascending aorta (54). The negative predictive value was shown to be 100% in the absence of plaque in the visualized regions. This correlates well with the normal distribution of plaques, with the ascending aorta being the least involved segment, making its involvement highly unlikely in the absence of disease in the descending aorta.
There is good interrater reliability, particularly for the detection of plaques that are 4 mm or greater (42; 122; 116). Significant findings on TEE in patients for heart surgery are often an indication for an epiaortic ultrasound to visualize the segments not seen on routine TEE.
Newer technology in TEE allowed for 3D reconstruction of images to predict plaque burden and localization (10).
Disadvantages. There is difficulty in visualizing the distal ascending aorta and the proximal aortic arch (regions that are important predictors of stroke) due to the tracheal air column and up to 42% of the ascending aorta not being visualized (55), leading to underestimation of the actual plaque burden.
Other disadvantages include invasiveness and the requirement for conscious sedation.
Epiaortic ultrasound. Epiaortic scanning of the aorta is a technique of intraoperative evaluation of the aorta for atherosclerotic disease.
Advantages. A complete evaluation of the aorta is possible, eliminating the blind spot in transesophageal echocardiography.
EAS can assist with detection of high-risk aortic lesions, helping with further surgical strategy, and decreasing postoperative stroke incidence (23; 87).
EAS has consistently proved to be superior to both TEE (25) and preoperative CT (14). A significant decrease in the incidence of postoperative cerebrovascular events has prompted some surgeons to advocate epiaortic ultrasound as a standard of care in cardiac surgery patients (125).
Disadvantages. EAS can only be used in open chest heart procedures. It is becoming less available for use as more surgeries are converting to minimally invasive heart surgeries.
Current guidelines recommend EAS primarily for patients “at high risk for embolic stroke, such as those with a history of cerebrovascular or peripheral vascular disease, and in those patients who have evidence of aortic atherosclerosis or calcification by other imaging modalities like preoperative or intraoperative TEE, MRI, CT, chest radiograph, etc.” Training protocols have also been devised. Lesions greater than 3 mm in thickness or mobile elements and their location are reported to the surgeon who decides further management (37).
Computed tomography. Angiographic assessment of the thoracic aorta has been replaced by less invasive modalities such as CT and MRI. The major limitation of CT has been the presence of respiratory and motion artifacts during respiration and aortic wall motion synchronous with the cardiac cycle. Irregular heart rhythms pose another challenge, creating motion artifacts. Respiratory motion artifacts can be reduced by imaging during each inspiratory breath hold. Multidetector CT uses multiple parallel detector rows and decreases the time required to obtain a complete study with increased spatial and temporal resolution. In addition, cardiac cycle gating with the assistance of ECG eliminates cardiac motion artifacts (86). In a prospective study of patients with ischemic stroke, cardiac cycle-gated CT (CGCT) was found to be more effective than transesophageal echocardiography in detecting atheromas 4 mm in size. Atheromas larger than 4 mm were detected with similar efficacy by both investigative modalities. CGCT has a higher sensitivity to calcification, and morphological features like ulceration and protrusion appear to be better visualized by CGCT (46). CGCT has also been proved to be a reliable study with good interobserver and intraobserver variability (80).
Spiral CT, compared to TEE, can detect 89% of protruding aortic atheromas seen on TEE, and rules out disease in 82% of patients who have no lesions on TEE. Ultrafast imaging techniques have made it feasible to complete the actual study in a single breath hold. Tenenbaum and colleagues have proposed the usage of noncontrast CT as a rapid screening tool for protruding aortic atheromas (102). Multislice CT can detect greater than 4 mm aortic arch atheroma in almost half of patients with transient ischemic attack (69). The major pitfall of CT is its inability to detect noncalcified lesions, including aortic mural thrombi, and also the inability to diagnose mobile lesions that have high embolic potential. Additional contrast enhancement could be of use in detecting noncalcified plaques or thrombi in the ascending aorta, which may not be visualized on the plain CT (102). A major advantage of CT over other studies lies in its rapidity of assessment. Concerns about CT-based assessment include exposure to contrast-induced nephropathy and radiation-induced diseases such as malignancy and accelerated atherosclerosis.
Magnetic resonance imaging. The advent of MRI has provided a better understanding of atherosclerotic plaque physiology. The ability of MRI to differentiate between lipid, fibrous, and cellular components makes it a valuable tool in predicting plaque change. Based on studies in mouse models, it can be utilized for the serial evaluation of plaque progression or regression (117). The major limitation of MRI is artifact secondary to respiratory movements and blood flow. An MRI technique described by Fayad and colleagues was able to overcome this limitation, with aortic plaque assessment having good correlation with TEE findings (33). A 3D MRI protocol has been devised that is able to detect more high-risk plaques than TEE (40). It could be a valuable tool in the assessment of patients with contraindications to TEE and in the evaluation of cryptogenic stroke. In patients at high risk for cardiac embolism, cardiac MRI can be combined with MRI of the brain and carotid and vertebral circulation in a single examination (89). This can prove to be highly useful in the assessment of multiple infarcts. Contraindications to MRI include hardware-like implanted defibrillators, pacemakers, cochlear implants, etc. In addition, patient characteristics like claustrophobia and the ability to maintain a good breath hold and regular heart rhythms also play a role.
Combining the aortic wall proximity of TEE and the tissue characterization capabilities of MRI has resulted in the transesophageal MRI (TEMRI) with better signal-to-noise ratio. It requires the placement of an MRI coil in the esophagus adjacent to the descending aorta, similar to a TEE. One of the major advantages of MRI is its ability to visualize the entire aortic wall thickness, and this combined with the better signal-to-noise ratio, makes TEMRI a promising tool for the future. However, the routine usage of this technique requires further trials and is also limited by its semi-invasiveness and cost of acquisition of equipment (94).
Positron emission tomography. An ideal investigational tool in the detection of vulnerable plaques should be noninvasive and have the ability to detect active inflammation in the aortic wall. FDG-PET is based on detecting the glucose uptake in the aortic wall secondary to glycolytic activity. The normal aortic wall has negligible amounts of glycolytic activity, and its increase indicates the presence of active inflammation in the vessel wall. FDG uptake has also been shown to increase with age, which correlates with the increase in inflammation with aging (17). However, PET as an independent modality is limited by its inability to precisely locate sites with increased uptake (13). The combination of inflammatory imaging capabilities of PET with the anatomical detail provided by the CT or MRI theoretically yields a method of localizing vulnerable plaques. A study by Bural and colleagues demonstrated the plausibility of using positron emission tomography in the assessment of the aortic arch (16). In a study of 18 patients, FDG-PET was used to calculate the standard uptake volume whereas the CT scan provided the aortic wall volume. The atherosclerotic burden could be computed by multiplying the two variables. This relatively noninvasive imaging protocol could be of use in screening patients at high risk. In a retrospective study of 85 consecutive patients with cancer with FDG-PET and CT, younger patients had isolated FDG uptake without calcifications and older patients had both increased FDG uptake and aortic wall calcifications (99). Sites with increased FDG uptake in younger patients may indicate early lesions that progress to calcification with vascular aging. Thus, PET scanning could be useful in detecting early lesions and earlier implementation of plaque intervention strategies. At present, further studies are required to firmly establish the role of this technique in aortic plaque imaging.
Intravascular ultrasound. Intravascular ultrasound is a research tool capable of characterizing plaque core; it has limited sensitivity in detecting lipid-rich cores, necessitating the use of newer methods like integrated back scatter and elastography. Assessment of the radiofrequency envelope of the plaque with integrated back scatter enhances detection of the lipid-rich core. Elastography is a technique that combines intravascular ultrasound with radiofrequency measurements of the plaque to detect regions of the vessel wall with increased strain, indicative of lipid-rich plaques (30). Aortic wall stiffness has been associated with stroke based on transesophageal echocardiography studies, and measurement of aortic stiffness could be used to predict stroke risk (96). Measurement of the plaque distensibility by intravascular ultrasound provides an additional measure of the vessel wall stiffness. A study of patients with cardiac disease has shown the effectiveness of intravascular ultrasound in the assessment of aortic atherosclerosis (98).
Optical coherence tomography. Optical coherence tomography (OCT) is an analogue of intravascular ultrasound, measuring optical echoes instead of ultrasound echoes. An infrared light source is pointed at the region of interest, and the backscattered light is measured. A superior resolution capability than ultrasound facilitates better identification of lipid-rich plaques and intimal hyperplasia. It has also proved equivalent, if not superior, to intravascular ultrasound in identifying the different plaque components.
Studies have shown good inter and intraobserver reliability with a high sensitivity for lipid-rich plaques (121). However, in vivo usage is limited due to the necessity to prevent interference from blood, requiring saline injection or proximal balloon occlusion. This limitation is also shared by angioscopy, which allows direct visualization of the atheroma and identification of vulnerable plaques based on the intensity of yellow discoloration of the plaque. In addition, only the luminal surface can be analyzed. Although various methods analyze the structural details of plaque, spectroscopy is used to analyze the chemical composition of plaques based on the pattern of reflected light and may prove to be synergistic with intravascular ultrasound and OCT in identifying plaque progression. Near infrared spectroscopy has better tissue penetration compared to conventional Raman spectroscopy and is comparable to OCT. Inflammatory changes in the plaque cause local pockets of elevated temperature that can be detected by thermography and can be used to detect vulnerable plaques (44).
Intravascular MRI. When compared to conventional MRI, intravascular MRI with the use of intravascular coils offers better resolution of the plaque. Also, the device need not necessarily be introduced into the aorta; adjacent structures such as veins can be used. There is a 74% agreement with histopathology for necrotic core grading (22), suggesting the possibility of using intravascular MRI to detect vulnerable plaques. The level of intraobserver and interobserver concordance is superior to intravascular ultrasound (59). Additional studies show that gadolinium enhancement during intravascular MRI helps to better identify the fibrous constituents that determine plaque stability (58). This could be used to assess the response to plaque-stabilizing therapies. Incorporation of the magnet and coil within the same scanner eliminates the necessity for an external scanner. It provides a color-coded image of the plaque composition rather than anatomic detail (44).
Molecular plaque imaging. Molecular plaque imaging with MRI utilizes newer contrast agents that are plaque-specific and can be used to identify vulnerable and culprit plaques. A major advantage is its noninvasiveness. Ultra-small particles of iron oxide are phagocytosed avidly by activated macrophages, homing to sites of active inflammation. Gadolinium-tagged nanoparticles that are targeted to attached fibrin can detect thrombi (62). Many of these studies focus on the coronary circulation, but with similar pathophysiology of atherosclerosis throughout the vasculature, it is conceivable that these novel techniques can be applied to the evaluation of the thoracic aorta as well. These techniques would be useful in the rapid detection of culprit plaques in patients presenting with stroke as well as for follow up evaluations of vulnerable plaques.
Antiplatelet versus anticoagulation. There are no proven guidelines for secondary prevention in patients with stroke and aortic arch atheromas. Prior clinical trials were not found to be significant and were, therefore, inconclusive.
Thus far, the only randomized trial to be completed is the Aortic Arch Related Cerebral Hazard (ARCH) trial, which compared warfarin with a target INR of 2 to 3 versus a combination of aspirin 75 to 150 mg daily and clopidogrel 75 mg daily in patients with stroke with aortic arch atheromas greater than 4 mm and no other source (05). The primary outcome was stroke, myocardial infarction, peripheral embolism, and death. The study was stopped prematurely because enrollment lagged, and there was insufficient funding to continue the trial. At the time of study termination, 349 patients had been randomized, 172 to aspirin and clopidogrel, and 177 to warfarin. Median follow-up was 3.4 years with the primary endpoint occurring in 7.6% of dual antiplatelet and 11.3% of anticoagulation patients (p=0.5). Major hemorrhage occurred in 2.3% and 3.4% of these patients, respectively. Because the study was underpowered relative to its initial plan of enrolling between 744 and 1488 patients, the authors concluded that there was insufficient information to make a final conclusion, and the trial could only help generate additional hypotheses.
In the NAVIGATE-ESUS trial, an exploratory analysis found no difference in the rate of recurrent stroke in a subgroup of patients with complex aortic arch atherosclerosis assigned to rivaroxaban versus aspirin (four versus four) (78). The annualized rate of recurrent stroke was higher overall in those with complex versus noncomplex versus no aortic arch atherosclerosis (7.2% versus 4.2% versus 5.6%, respectively).
Though statins have not been tested specifically in patients with concomitant stroke and aortic arch atheroma, current evidence supports their use in these patients. The Stroke Prevention by Aggressive Reduction of LDL (SPARCL) trial found that atorvastatin 80 mg daily in patients with stroke significantly reduced the risk of recurrence, irrespective of the stroke subtype (03). Further, more than 50% reduction in baseline LDL levels was associated with a significantly decreased stroke occurrence (07).
The American College of Chest Physicians currently recommends aspirin (50 to 100 mg) for patients with ischemic stroke associated with aortic atherosclerosis. Patients with mobile atheromas can be treated with either warfarin to achieve a therapeutic INR of 2 to 3 or with low-dose aspirin (90; 18). One study has shown that the combination of ACE inhibitors and aspirin is more effective in reducing the inflammatory markers in carotid atheromas compared to single-agent therapy (91). Whether this combination is of benefit for aortic atheromas is uncertain. Further trials are needed to establish effective treatments of aortic atheroma.
Statins. Lipid-lowering agents, such as high-intensity statins, have been recommended for secondary prevention, atheroma stabilization, and, in turn, reducing the risk of emboli irrespective of LDL levels due to the additional pleiotropic effects of statins as well as their ability to stabilize and regress plaque progression (64). Regression of plaques was demonstrated in familial hypercholesterolemia (82), in addition to reducing aortic wall stiffness (103). Pitavastatin has been shown to decrease intima media thickness in plaques of thoracic aorta (79). The Stroke prevention by aggressive reduction of LDL (SPARCL) trial has suggested that aggressive reduction of LDL levels by statins can significantly reduce both primary and recurrent stroke risk, irrespective of the stroke subtype (03). Also, a more than 50% reduction in baseline LDL levels was associated with a significantly decreased stroke occurrence (07). Combination therapy of atorvastatin plus etidronate for 12 months reduced thickness of abdominal and thoracic aortic plaques by 12% to 14% (50). Combination therapy was more effective than either treatment alone.
Surgical management. Thoracic aortic replacement surgeries for atherosclerosis are usually performed only in patients undergoing cardiac surgery for other indications like coronary artery bypass grafting or valve replacement, etc. Severe atheroma in the ascending aorta detected preoperatively with TEE or helical CT and intraoperatively by epiaortic scanning often leads to ascending aortic replacement. Some authors have advocated surgical management of aortic atheromas with high embolic potential as the most effective therapy. In 2002, a patient with recurrent cerebral emboli from friable aortic atheromas refractory to medical therapy was successfully treated by aortic arch replacement with a Dacron graft. No further emboli were detectable at 1-year follow-up by transcranial Doppler (57). Some authors have advocated replacement of the affected ascending aortic arch segment and reported decreased stroke incidence (56). However, the 3-year survival was only 40%, probably secondary to the diffuse nature of the atherosclerotic disease process, affecting multiple body systems (56; 85). There was a 10-fold increase in mortality for ascending aortic replacement for atherosclerosis compared to aortic replacement for aneurysmal repair (52). However, another study showed a favorable 3-year cumulative survival rate approaching 85.6% (126). Aortic endarterectomy has also not proven to be useful on a routine basis (95). At this time, surgical management is reserved for cases refractory to medical therapy. Endovascular treatment of aortic plaques is still a developing technology and may prove to be a viable alternative in the future.
Prevention of stroke following cardiac surgery. The mortality and morbidity of stroke (83) following cardiac surgery has spawned the introduction of screening techniques to identify patients with high risk of embolism and minimize aortic manipulation in the presence of severe plaques. Preoperative assessment of the aortic arch with CT and TEE and intraoperative epiaortic scanning have contributed significantly to detecting high-risk plaques. All these modalities significantly reduce postoperative stroke events by appropriate surgical modifications of aortic clamping and cannulation sites (61). For most surgeons, EAS with its superior visualization of the ascending aorta remains the “gold standard” in assessment of the aorta. In the presence of severe aortic disease detected by EAS, the site of aortic cannulation is of paramount importance, being decided by ultrasound guidance or manual palpation. The presence of aortic arch atheromas is considered a contraindication for the use of minimally invasive port-access techniques employing the intra-aortic EndoClamp because the latter may lead to dislodgement of emboli. A right brachial, instead of a femoral, approach may be chosen to restrict catheter contact to the segment of the aorta proximal to the innominate artery, where thrombus formation is comparatively rare. A protocol combining preoperative CT and epiaortic ultrasound assessment of the aortic arch has proven effective in identifying patients at high risk (75). Patients with moderate (greater than 3 mm) and severe plaques managed with aortic no-touch off-pump coronary artery bypass grafting had significant reduction in stroke events. Aortic plaque density, measured in gray scale medians (GSM), can also be used to determine stroke risk in the postoperative period. This can be computed from B-mode ultrasound measurements of the aortic plaque during transesophageal echocardiography. Increase in lipid content results in decreased echo-density. A GSM of less than 100 in plaques larger than 3 mm is associated with a significantly increased stroke risk. These patients may be candidates for off-pump coronary artery bypass grafting (77).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Aparna M Prabhu MD MRCP
Dr. Prabhu of Thomas Jefferson University and Jefferson Einstein Medical Center has no relevant financial relationships to disclose.
See ProfileVarsha Muddasani MD
Dr. Muddasani of Thomas Jefferson University Hospital has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
Dec. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Sleep Disorders
Oct. 14, 2024
Developmental Malformations
Sep. 22, 2024