Neuro-Oncology
Visual pathway gliomas
Jan. 14, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
This article discusses isocitrate dehydrogenase (IDH)-mutant astrocytoma, World Health Organization (WHO) grade 2, including its classification, natural history, and management options.
|
• Astrocytoma IDH mutant, WHO grade 2, presents with a wide spectrum of neurologic manifestations. | |
|
• The median age at presentation is in the 40s, with a slightly higher incidence in males. | |
|
• Magnetic resonance imaging with and without contrast is the standard approach for evaluating brain lesions. | |
|
• Tissue diagnosis by biopsy or surgery is essential. | |
|
• Extent of resection is associated with outcomes. | |
|
• Radiation and chemotherapy prolong survival, but the exact timing is not well delineated. | |
|
• Inhibitors of mutant isocitrate dehydrogenase hold promise for improved progression-free survival. | |
|
• Observation may be a reasonable option for select cases, keeping in mind that regular imaging is needed in this setting. |
Brain tumors were managed historically with surgical resection and radiotherapy starting in the era of Harvey Cushing. In 1976, adjuvant chemotherapy began to be utilized when cyclohexyl chloroethyl nitrosourea (CCNU) was found to increase survival—albeit by only a few months (14). During this era, our understanding and classification of gliomas was based entirely on histology and anatomical location of the tumors. This approach continued until 2016 when a new classification system was developed, guided by a new molecular understanding of gliomas. In particular, mutations in the genes encoding isocitrate dehydrogenase (IDH1 and IDH2), as well as chromosomal 1p/19q co-deletion were found to be strongly associated with improved prognosis (40; 55; 45). The 2021 World Health Organization (WHO) classification further refined the classification system to include the following glioma subtypes:
|
• Astrocytoma, IDH-mutant |
Although the 2021 WHO classification emphasizes the tumor molecular features, the tumor grade continues to play a role in clinical studies and patient care. The focus of this article is on astrocytoma IDH mutant, WHO grade 2.
The clinical presentation of patients with primary brain tumors can include overt focal neurologic deficits and new-onset seizures (47; 25). The presentation can also be more subtle and manifest as memory impairment, personality changes, and symptoms of elevated intracranial pressure—progressive headaches, nausea, vomiting, blurred vision, and diplopia. Focal deficits depend on the affected region and result from compression of surrounding structures. Tumors of the brainstem, spinal cord, infratentorium, and eloquent cortices are identified earlier due to overt neurologic deficits, such as sensorimotor or cranial nerve deficits. IDH-mutant astrocytomas most often manifest in the cerebral cortex and subcortical tissue, especially the frontal lobe (27). Patients with IDH-mutant astrocytomas are more likely to present with seizures (5% to 74%) than IDH-wildtype gliomas (18% to 34%) (12). The increased seizure risk is thought to be due to mutant IDH-mediated accumulation of D-2-hydroxyglutarate, which can function as an NMDA receptor agonist (12). It is likely there are other mechanisms at play as well.
Prognosis. IDH-mutant diffuse astrocytomas carry a better prognosis than wildtype tumors. The histological grade of gliomas is less useful for prognosis than their mutational status. As such, many studies pool data between grade 2 and grade 3 gliomas.
|
• The RTOG 9802 trial specifically examined grade 2 gliomas and demonstrated an association between survival and mutational status of the tumors (51; 05). Patients with IDH-mutant astrocytoma had a greater median overall survival than IDH-wildtype astrocytoma (11.3 vs. 1.9 years). This study also showed that patients with IDH-mutant and 1p/19q co-deleted oligodendrogliomas had the greatest overall survival, with median survival not reached during the study (05). Many, if not all, of the IDH-wildtype tumors would likely now be classified as glioblastoma IDHwt. | |
|
• The RTOG 9402 trial assessed the benefit of adjuvant chemotherapy to radiotherapy for the treatment of WHO grade 3 gliomas. This trial was focused on oligodendrogliomas but allowed for mixed oligoastrocytomas, a category that does not exist in the current WHO classification system. Post-hoc genetic analysis of these samples in 2012 and 2014 demonstrated that patients with IDH-mutant astrocytomas (1p/19q non-co-deleted) had an overall survival of 5.5 years, and those with IDH-wildtype astrocytoma had an overall survival of 1.0 years (10; 11). These studies demonstrated the same effect in patients treated with radiation therapy alone (3.3 years in IDH-mutant astrocytoma, and 1.3 years in IDH-wildtype astrocytoma). | |
|
• A study pooled data from the UCSF Adult Glioma Study, the Mayo Clinic, and The Cancer Genome Atlas to examine the association between mutational status and survival in patients with grade 2, 3, and 4 gliomas (42). It found that patients with grade 2/3 IDH-mutant astrocytomas had a median survival of 9.3 years, whereas median survival was 1.9 years in IDH-wildtype astrocytoma. |
Complications. Complications experienced by a patient depend on the treatment modality employed. Surgical resection aims to maximize tumor excision while avoiding eloquent brain regions. There has been widespread adoption of awake craniotomy, fMRI, and fluorescent dyes to guide surgical resection to maximize tumor excision while avoiding eloquent brain regions. However, there continues to be a risk of damage to regions important for speech, judgment, motor function, etc. Radiation therapy has been associated with adverse effects on cognition (08; 15; 17). Nitrosoureas in specific and temozolomide to a lesser degree have been associated with toxicity of gonadal function and sperm production and quality, which can be particularly harmful for patients interested in having children (57; 06).
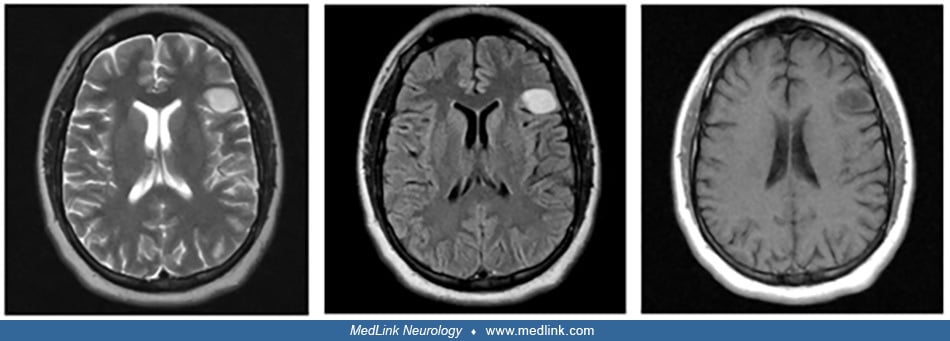
A 30-year-old female with a history of schizoaffective disorder presented initially with loss of consciousness while driving, resulting in a motor vehicle collision and development of new-onset focal seizures with secondary generalization. The initial head CT demonstrated a left frontal hypodensity. Subsequently, an MRI demonstrated a 26 mm x 23 mm x 18 mm T2 FLAIR (fluid-attenuated inversion recovery) bright mass, without enhancement on T1 post-contrast.
The patient had an awake craniotomy that achieved gross total resection—resection without visual residual tumor on post-operative contrast-enhanced brain MRI (24). Pathology demonstrated astrocytoma IDH1 mutant, WHO grade 2. Further treatment with chemotherapy or radiation was deferred, but monitoring was ongoing every 3 months. Nine months after the operation, there was no evidence of disease recurrence.
The brain has long been considered a postmitotic organ wherein all cells had already differentiated and there were no resident stem cells. As a result, gliomas were believed to originate from the dedifferentiation of mature glial cells. Subsequent advances revealed that neural stem cells and glial progenitor cells can be found in multiple regions of the brain. As such, there is suspicion that gliomas originate from these stem cells or progenitor cells. As with other cancers, spontaneous mutations in oncogenes and tumor suppressor genes drive the formation of the initial glioma cells. Subsequently, additional genetic and epigenetic changes are acquired to facilitate the propagation, invasiveness, and angiogenic properties of these tumors (49).
Mechanistic understanding of the survival benefits associated with IDH mutations. Mutation in IDH1 or IDH2 is a common driver of gliomagenesis that appears to precede secondary mutations. IDH genes encode isocitrate dehydrogenase, an enzyme that catalyzes the conversion of isocitrate to alpha-ketoglutarate in the citric acid cycle. Gliomas have mutations in only one copy of the IDH genes, suggesting that mutations may not simply result in a loss of function (03; 16). Instead, Dang and colleagues demonstrated that mutations in arginine 132 lead to a gain of function in the ability to catalyze the conversion of alpha-ketoglutarate to 2-hydroxyglutarate (16). Patients with inborn errors of 2-hydroxyglutarate metabolism that result in its accumulation are at increased risk of malignant brain tumors (01). 2-HG competes with alpha-KG at the binding sites of histone demethylases. This leads to genome-wide histone and DNA methylation alterations that block cell differentiation and, hence, facilitate malignant cell formation (53).
According to the Central Brain Tumor Registry of the United States (CBTRUS), primary central nervous system tumors have an average annual age-adjusted incidence of 24.71 per 100,000; 28.4% of these are malignant, with an annual incidence of 7.02 per 100,000. Glioblastoma accounted for 50.1% of all malignant tumors, and the remaining 49.9% have multiple histopathologic types. IDH-mutant diffuse astrocytoma account for approximately 6% of malignant tumors. Brain tumors as a whole have an overall rate in females of 27.62 versus males at 21.60 per 100,000. The overall rate in non-Hispanics versus Hispanics was 25.09 versus 22.95 per 100,000. Glioblastoma is 1.39-fold more common in males than females, whereas diffuse astrocytoma is 1.27-fold more common in males (36).
There are currently no clear preventative strategies. Exposure to ionizing radiation has been associated with an increased risk of developing gliomas (36). On the other hand, individuals with allergies or atopic diseases are at decreased risk.
|
• Primary versus secondary tumors: isolated tumors in the brain may be a metastasis from a peripheral cancer. | |
|
• Primary tumor types: there are several other types of primary brain tumors, many of which are not malignant (eg, glioneuronal tumors). |
|
• Seizure disorders: patients with a brain tumor may often have seizures due to the tumor’s mass effect on surrounding tissue. | |
|
• Headache disorders: patients with brain tumors often have headaches that are worst on awakening in the morning. It is important to consider a brain tumor on the differential for new-onset headaches. | |
|
• Strokes: focal neurologic deficits often represent a cerebrovascular accident, but it is important to assess for signs of elevated intracranial pressure that would suggest a brain tumor. | |
|
• Maffucci syndrome: this is a disorder of germline IDH mutation. It is associated with enchondromas and subcutaneous hemangiomas. In addition, patients are at increased risk of IDH-mutant gliomas. A related disorder, Ollier disease, also appears associated with an increased risk of IDH-mutant gliomas. |
Contrast-enhanced MRI is the standard approach to identify and characterize mass lesions in the brain. Diffuse gliomas are characterized by a poorly marginated mass that infiltrates the surrounding tissue. For IDH-mutant low-grade astrocytomas, an imaging modality known as the T2-FLAIR (fluid-attenuated inversion recovery) mismatch sign has been developed (41; 07). A meta-analysis examining 1053 patients with mismatch had high specificity but poor sensitivity (39). This mismatch sign is defined as a complete or near-complete homogeneous high-signal intensity on T2-weighted images and a relative suppression of the signal intensities on the FLAIR sequence (41). Nevertheless, the current standard for tumor classification includes surgical resection, histological grading, and molecular genotyping (28). Extent of resection is associated with outcomes in this patient population.
Gross total resection and possibly supratotal resection, if it can be safely done, is the next step in glioma management. Sometimes, it is necessary to perform a subtotal resection, which can be used for diagnostic purposes, particularly if the tumor invades eloquent brain regions. As discussed below, gross total resection has been associated with improved survival compared to subtotal resection (51; 22). There are some authors who argue in favor of supramaximal resection. Histopathological grading is next done based on the following classification system and histological features.
|
• Grade 1 tumors (eg, pilocytic astrocytoma) are well-circumscribed or lack cytological atypia. | |
|
• Grade 2 tumors (eg, diffuse glioma) are diffusely infiltrative and have cellular atypia. | |
|
• Grade 3 tumors (eg, anaplastic glioma) have features found in grade 2 tumors but also show anaplasia and mitotic activity. | |
|
• Grade 4 tumors (eg, glioblastoma) have the aforementioned features with additional microvascular proliferation or necrosis (27). |
Beginning with the WHO 2016 classification, it has become standard management to genotype the tumor for IDH mutations and 1p/19q co-deletion (27). Testing is often also performed for additional driver mutations in H3K27M, MYBL1, FGFR1, BRAF, MAPK, and CDKN2A/B. CKDN2A/B is of particular relevance as it is a strong adverse prognostic factor in patients with IDH-mutant astrocytoma (52; 02). The CKDN2A/B mutation carries a hazard ratio of 2.12 for progression-free survival and a ratio of 1.72 for overall survival (02). In fact, homozygous deletion of CDKN2A/B leads to a grade 4 classification regardless of the presence of microvascular proliferation or necrosis (31). The prognostic value of the other aforementioned mutations is not as strong (26). Methylation studies should also be performed as the MGMT promoter methylation status may be associated with improved survival and response to temozolomide (53; 05).
Surgical resection. Per the National Comprehensive Cancer Network (NCCN) guidelines, gross total resection has long been established as a mainstay of glioma treatment. Shaw and colleagues found that patients with diffuse gliomas in whom resection resulted in greater than 1 cm of residual tumor had a worse survival compared to those who had less than 1 cm residual (HR: 3.54, 95% CI 1.83-6.84, p=0.0002) (51). In patients with diffuse grade 2 gliomas, gross total resection has been found to result in improved outcome compared to observation (22). Jakola and colleagues compared two hospitals--one with a conservative observational approach to treatment and the other with a preference for early resection--and found that there was improved survival in patients at the hospital that favored early resection (22). In fact, this effect was observed across all three glioma subgroups analyzed (1p/19q/IDH-mutant oligodendroglioma, IDH-mutant astrocytoma, and IDH-wild type astrocytoma). Bauman and colleagues compared gross total resection with subtotal resection in patients with diffuse gliomas and found worse survival in patients with subtotal resection (HR: 1.59, 95% CI 1.06-2.38, p=0.026) (04). There may be promise for supratotal (sometimes termed “supramaximal”) resection, ie, resection of both the contrast-enhancing tumor and the surrounding T2-FLAIR signal that represents edema, although this is not established as the standard of care (48).
Foregoing resection in favor of biopsy can further complicate care as it can result in the misdiagnosis in as many as 49% of cases (21). Another study supported the importance of gross total resection by demonstrating that it was associated with improved survival over subtotal resection, partial resection, and biopsy (13). In contrast to the aforementioned studies, Wijnenga and colleagues performed a retrospective cohort study examining radiologically presumed low-grade gliomas to compare observation, biopsy, and early resection (54). They found that observation had no difference in survival compared to early resection. However, consistent with above, they did find that only a biopsy was associated with worse survival (HR: 2.69, 95% CI 1.19-6.06, p=0.02) (54). This may be influenced by the patient selection for biopsy versus resection.
Laser interstitial thermal therapy (LITT) has emerged as a viable alternative to surgical resection. This minimally invasive approach utilizes lasers that are absorbed by tumor tissue, heating to around 42°C and coagulating the tissue (19). It is particularly useful in the treatment of patients who have deep-seated tumors or if the patients have comorbidities that make them poor surgical candidates. One small study specifically examined the use of LITT in the treatment of IDH-mutant low-grade gliomas and found that these patients had a 72.5% progression-free survival at 3 years and 54.4% at 5 years, which is on par with results in patients with surgical resection (23). There is a need for a prospective clinical trial comparing LITT to surgical resection in order to assess whether it truly is a viable alternative.
Radiation therapy. Radiotherapy is also often utilized in the treatment of diffuse gliomas--as well as higher-grade gliomas. In 2005, van den Bent and colleagues demonstrated that radiotherapy in addition to gross total resection increased patients’ progression-free survival from 3.4 years without radiotherapy to 5.3 years with it (56). However, the study did not demonstrate an overall survival benefit with radiotherapy. Another trial compared low-dose versus high-dose radiotherapy for patients with grade 2 gliomas (50). These studies were conducted prior to the year when molecular characteristics were used to classify these tumors, making interpretation of the results somewhat difficult. The American Society of Clinical Oncology-Society for Neuro-oncology (ASCO-SNO) guidelines recommend offering radiation therapy with resection for patients with grade 2 IDH-mutant gliomas, though chemotherapy can be delayed (32).
Chemotherapy. RTOG 9802 examined the utility of procarbazine, CCNU (lomustine), and vincristine (PCV) chemotherapy in patients with grade 2 gliomas. It demonstrated that patients who received adjuvant PCV after radiotherapy had an improved median overall survival versus radiotherapy alone (not reached vs. 7.5 years) (51). As a substantial percentage of patients in the radiotherapy-only arm subsequently received chemotherapy, the trial results could be interpreted to support earlier combinatorial over sequential therapy. Examination of molecular subtypes of gliomas in this study demonstrated that adjuvant PCV chemotherapy led to improved survival in patients with 1p/19q codeletion/IDH-mutant oligodendrogliomas and IDH-mutant astrocytomas. There was no survival benefit in patients with IDH-wildtype astrocytomas (05), although the study was not specifically powered to answer questions for molecular subtypes. The utility of adjuvant chemotherapy was again investigated by Buckner and colleagues, who investigated survival in patients who received PCV chemotherapy after radiation therapy compared to patients who received radiation therapy only (09). Those who received chemotherapy had an improved median overall survival (13.3 vs. 7.8 years; P=0.003). Furthermore, at 10 years, those who had adjuvant chemotherapy had an improved progression-free survival of 51%, compared with 21% in those who were treated with radiation therapy only (09).
Temozolomide is another chemotherapy that has widely been used for high-grade glioblastoma; however, there are limited data on its efficacy in patients with low-grade gliomas, and molecular subtypes were not assessed. Initial studies demonstrated that low-grade gliomas respond to temozolomide, but these studies had a limited sample size (38; 44). A more robust study, RTOG 0424, was a single-arm trial examining the efficacy of temozolomide alongside radiotherapy in high-risk low-grade gliomas (both astrocytoma and oligodendroglioma); the 3-year overall survival of 73.5% was better than the historical 3-year overall survival of patients who did not receive temozolomide (18). There are ongoing randomized controlled cooperative group trials (CODEL, CATNON) that are assessing the efficacy of temozolomide in patients with grade 2 and 3 gliomas, many of whom harbor IDH mutations.
IDH inhibitors. There have been efforts to assess the therapeutic utility of inhibitors of mutant IDH enzymes. Mutant IDH leads to the accumulation of D-2-hydroxyglutarate, which facilitates tumor growth. INDIGO is a phase 3 trial that investigated vorasidenib in 331 patients with WHO grade 2 IDH-mutant astrocytomas and oligodendrogliomas (29). Patients with residual or recurrent tumor who had not previously been treated with chemotherapy were treated with vorasidenib or placebo. Patients treated with vorasidenib were found to have significantly prolonged median progression-free survival (27.7 vs. 11.1 months; P< 0.001), and the time to the next intervention was also significantly improved in patients taking vorasidenib (hazard ratio: 0.26). However, vorasidenib was associated with increased risk of hepatotoxicity of level grade 3 or higher (9.6% vs. 0%) (29). These results will likely result in a change of the standard of care for these patients, which would include early use of vorasidenib. At the time of this publication, vorasidenib is being reviewed by the Food and Drug Administration.
Other therapies. Although immunotherapy with checkpoint inhibitors has been a successful therapeutic approach for other cancers, it has not thus far proven to be effective in gliomas (46). This is thought to be due to an immunosuppressive environment in gliomas, which may be driven by D-2-hydroxyglutarate accumulation in IDH-mutant gliomas (31). There are multiple ongoing trials further exploring the utility of immunotherapy in gliomas, including clinical trials such as NCT04056910 that combine IDH inhibitors with checkpoint inhibitors (31).
Another promising approach makes use of a peptide vaccine targeting the IDH mutations. A phase 1 trial demonstrated that this vaccine induced immune responses and gave hints that it may lead to survival benefits (43). Lastly, yet other trials are beginning to explore PARP inhibitors for low-grade gliomas as they have shown promise in other cancers (30).
Observation. Because surgical resection, radiotherapy, and chemotherapy carry risks and adverse effects, observation of less malignant gliomas has been examined. As discussed above, gross total resection is the standard of care, and observation is not a standard approach prior to resection. According to the NCCN, observation may, however, play a role in patients with low-risk features—those younger than 40 years who have had a gross total resection (34). However, imaging to monitor for recurrence is critical.
Observation has also been examined as an approach for patients with incidentally identified low-grade gliomas. No randomized controlled trials or prospective studies have examined incidentally identified low-grade gliomas, but a retrospective study examining grade 2 gliomas demonstrated that these tumors can become symptomatic approximately 48 months after discovery (20). This study showed that patients with incidentally identified low-grade gliomas have survival benefits associated with surgical resection. As a result, this study provides indirect evidence that resection may be a better approach than observation for the management of grade 2 gliomas.
In summary, it is clear that radiotherapy and chemotherapy prolong survival, but the exact timing is not well understood. Early radiotherapy is associated with improved progression-free survival but does not change overall survival (EORTC 22845). PCV improved survival (RTOG 9802), though it is possible temozolomide does as well. The results of RTOG 9802 showed that there is a significant improvement in median overall survival in patients with high-risk low-grade glioma treated with radiation therapy followed by PCV chemotherapy compared with radiation therapy alone. However, the study did not directly address whether all of these patients should be treated sooner rather than later. Observation may be a reasonable option for patients with high-risk low-grade gliomas who are asymptomatic or stable or those with low-risk low-grade gliomas keeping in mind that regular imaging will be needed. Alternatively, the survival benefit seen with upfront radiation therapy and chemotherapy over radiation therapy followed by probable chemotherapy at progression allow one to argue in favor of treating sooner rather than later. Oftentimes, the clinical management decisions are based on a number of patient-specific factors and necessitate extensive discussion with the patient and other key decision makers.
Adverse effects. As described above, there are risks associated with treatment. Surgical resection may damage important brain regions, radiotherapy may adversely impact cognition and quality of life (08; 15; 17), and chemotherapy can impair fertility or have other side effects depending on which drug is used (57; 06). In this young patient population, it is reasonable to consider referral to oncofertility prior to initiating any treatments.
Chemotherapy has been associated with toxicity of gonadal function and sperm production and quality, which can be particularly impactful for patients interested in having children (57; 06). Current chemotherapeutic options of temozolomide and PCV have been shown to be teratogenic, and the United States Food and Drug Administration recommends against their use during pregnancy. As patients with IDH-mutant diffuse astrocytoma have relatively good survival compared to other gliomas, shared decision-making is important, and patients should be educated to weigh the risks and benefits of each treatment modality.
Risks associated with anesthesia during tumor resection are the same as those for other surgical procedures.
The median age of presentation of diffuse astrocytomas is in the 40s (37).
Diffuse astrocytoma is 1.27-fold more prevalent in males than females (35).
The vast majority of gliomas are not believed to be heritable, although some rare inherited genetic syndromes may predispose patients to gliomas. These syndromes include Li Fraumeni syndrome, neurofibromatosis, Lynch syndrome, melanoma-neural system tumor syndrome, Maffucci syndrome, Ollier disease, and tuberous sclerosis (33).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
John Paul Aboubechara MD PhD
Dr. Aboubechara of UC Davis Health has no relevant financial relationships to disclose.
See ProfileOrwa Aboud MD PhD
Dr. Aboud of UC Davis Medical Center received consultant fees from Aptitude Health LLC.
See Profile
Rimas V Lukas MD
Dr. Lukas of Northwestern University Feinberg School of Medicine received honorariums from Novartis and Novocure for speaking engagements, honorariums from Cardinal Health, Novocure, and Merck for advisory board membership, and research support from BMS as principal investigator.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Stroke & Vascular Disorders
Dec. 29, 2024
Neuro-Oncology
Dec. 13, 2024
Neuro-Oncology
Dec. 05, 2024