




Neuro-Ophthalmology & Neuro-Otology
Diplopia
Jan. 08, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Benign paroxysmal positional vertigo is the most common vestibular disorder. Canalolithiasis of the posterior semicircular canal is now widely accepted as the biological basis for typical benign paroxysmal positional vertigo. Better understanding of its pathophysiological concepts has led to specific therapeutic strategies, which aim to clear the affected semicircular canal from mobile particles. In this article, the authors have added updated insight into the treatment of recurrent benign paroxysmal positional vertigo.
|
• Benign paroxysmal positional vertigo is the most common vestibular disorder, affecting about 10% of the general population at some point during their lives. | |
|
• Canalolithiasis of the posterior semicircular canal is the most common underlying pathophysiology. | |
|
• Several variants have been recognized, reflecting involvement of the posterior, horizontal, or anterior semicircular canal by canalolithiasis or cupulolithiasis. | |
|
• Conservative treatment with specific positional maneuvers is almost always effective at improving or resolving the clinical manifestations. |
The first detailed description of benign paroxysmal positional vertigo of the posterior canal was published by Barany in 1921. He described a 27-year-old woman who had experienced attacks of positional vertigo for 2 weeks (05). Barany noted the rotatory-vertical nystagmus, the brief duration of the attacks, and the fatigability with repetition of the provocative maneuver, but he did not recognize the latency of onset and the reversal of nystagmus after moving away from the provoking position. In 1952 Dix and Hallpike supplied the first complete description of the cardinal manifestations of benign paroxysmal positional vertigo (25). In their report, they also described a positioning test, today known as the Dix-Hallpike maneuver, to elicit benign paroxysmal positional vertigo.
Since its first recognition, benign paroxysmal positional vertigo has been considered almost unanimously a peripheral vestibular disorder. However, its pathophysiology has been a matter of debate and an intellectual challenge (67). Barany, as well as Dix and Hallpike, speculated that the dysfunction must involve the otoliths, but they did not propose a specific pathophysiological mechanism (05; 25). In 1962 Schuknecht was the first to provide a pathophysiological concept of benign paroxysmal positional vertigo that explained the clinical features of the disease as a mechanical irritation of the posterior semicircular canal (85). On the basis of pathological studies, he later coined the term “cupulolithiasis,” indicating that heavy particles attached to the cupula would render it sensitive to gravity (86). Later it was noted that several clinical features cannot be explained by the concept of cupulolithiasis, such as the limited duration of the attack even though the provocative head position is maintained, the fatigability on repeated testing, and the lack of nystagmus with slow head tilts (87; 11). This problem was solved when Hall, Ruby, and McClure formulated the concept of “canalolithiasis” (34); this term has become widely accepted. Canalolithiasis has provided the basis for effective treatment (88; 27) and the pathophysiological understanding of all variant manifestations of benign paroxysmal positional vertigo (11; 40).
Benign paroxysmal positional vertigo is the most common vestibular disorder, accounting for about 20% of referrals in specialized dizziness clinics. The evolution of its pathophysiological concepts (67) has led to therapeutic strategies that have made it the most successfully treatable cause of vertigo. The cardinal feature of the disorder is disabling vertigo provoked by changes of head position. Several variants of benign paroxysmal positional vertigo are known that reflect involvement of different semicircular canals. They all can be diagnosed on the basis of clinical observation. Diagnostic criteria for established and emerging syndromes of benign paroxysmal positional vertigo have been published by the Bárány Society (98). A simple questionnaire that consists of three questions makes a diagnosis of benign paroxysmal positional vertigo with a sensitivity of 87% and a specificity of 90% (60).
Benign positional vertigo of the posterior canal. The involvement of the posterior canal accounts for about 80% to 95% of cases and causes brief attacks of vertigo that are precipitated by rapid extension or flexion of the head and lateral head tilts. Patients typically experience vertigo when turning over in bed, lying down from the sitting position, sitting up from supine, extending the neck to look up, or bending over. They may wake up with vertigo when turning in bed. The illusion of movement is usually rotatory, but a sensation of body tilt can also occur. Other complaints during the attack include imbalance, oscillopsia, and vegetative symptoms such as nausea, sweating, and tachycardia. Patients are usually aware that certain head movements precipitate attacks of vertigo. They often develop strategies to avoid vertiginous attacks, eg, sleeping upright or holding their neck stiff, but this may lead to immobility and prolongation of the natural course of the disorder.
A single attack of posterior canal benign paroxysmal positional vertigo usually lasts 10 to 20 seconds and no longer than 1 minute. However, after a flurry of attacks, patients may complain of prolonged nonspecific dizziness and imbalance lasting from hours to days. Typically, posterior canal benign paroxysmal positional vertigo manifests itself with symptomatic episodes lasting from a few days to several months, interspersed by asymptomatic intervals of several months to years in duration.
The diagnosis is confirmed by provocation of vertigo by positioning testing and observation of typical nystagmus. The classic test to precipitate benign positional vertigo of the posterior semicircular canal is the Dix-Hallpike maneuver.
The patient is seated on a couch with the head rotated 45 degrees to the left. He is then laid down rapidly on his back with the head both hanging and turned 45 degrees to the side. With this procedure the affected posterior canal is rotated in a plane parallel to the gravitational vector that ensures its maximal stimulation. Alternatively, a lateral tilt of the trunk from a sitting position can be performed with the head turned 45 degrees to the opposite side; this positions the head with the lateral aspect of the occiput onto the couch. With both maneuvers, the actual positioning of the posterior semicircular canal is identical. Before the maneuver is carried out, it is important to instruct the patient to keep the eyes open without blinking and to stay in the precipitating position, even if vertigo occurs. The maneuver should be hand-guided by the examiner who leads the head of the patient to ensure rapid and proper performance. Frenzel glasses are helpful for observation of nystagmus. However, they are not mandatory, as the characteristic torsional nystagmus cannot be suppressed by fixation. It may be useful to start testing for benign paroxysmal positional vertigo on the right side, unless the history clearly points to affection of the left labyrinth; because benign paroxysmal positional vertigo affects the right labyrinth 1.4 times more often than the left side, possibly due to the habit of most patients to sleep on the right side (102).
The diagnosis of benign paroxysmal positional vertigo of the posterior canal can be reliably made when the positional nystagmus fulfills the following criteria (02; 11):
|
• Torsional-vertical nystagmus. The most prominent direction of nystagmus is a torsional component, rotating with the upper pole of the eyes toward the undermost ear appearing when the patient is positioned to the symptomatic side. In addition, there is a smaller vertical-upbeating nystagmus component most prominent on the uppermost eye. | |
|
• Latency. Typically, nystagmus and vertigo start a few seconds after the precipitating head position is reached. Nystagmus intensity increases rapidly and then decays (crescendo-decrescendo). | |
|
• Duration. Nystagmus usually lasts 10 to 20 seconds and never exceeds 60 seconds. | |
|
• Reversal. A few seconds after the patient has returned to the sitting position, a transient nystagmus of lesser intensity beating in the opposite direction can be observed. | |
|
• Fatigability. Vertigo and nystagmus decrease with repeated positioning in most cases. |
Rarely, torsional-vertical positional nystagmus as described above lasts longer than 60 seconds indicating cupulolithiasis of the posterior canal. The intensity of nystagmus is strongest with a “half Dix-Hallpike maneuver” with the head resting slightly raised from supine and subsides when the head is brought to a reclined position (46).
Benign paroxysmal positional vertigo of the horizontal canal. The involvement of the horizontal canal accounts for 5% to 20% of all patients presenting with benign paroxysmal positional vertigo (40). The horizontal canal variants are important to recognize because they have features that have formerly been attributed to positional vertigo of central origin. In benign paroxysmal positional vertigo of the horizontal canal, attacks of vertigo are provoked by turning the head to either side in the supine position, whereas sitting up or lying down produces only minimal symptoms. Bouts during which attacks of vertigo can be provoked tend to be shorter than with involvement of the posterior canal. To test for benign paroxysmal positional vertigo of the horizontal canal, the head is turned rapidly to either side with the patient lying supine. Eye movements should be observed with Frenzel glasses. Two variants have been described, namely, the more common canalolithiasis and the rarer cupulolithiasis of the horizontal canal.
With canalolithiasis of the horizontal canal, the supine lateral head turn provokes transient horizontal nystagmus beating toward the ground (geotropic nystagmus), regardless of whether the head is turned to the right or left (75; 03). Typically, the nystagmus starts with no or minimal latency, beats purely horizontally with respect to the head, lasts up to 1 minute, changes direction depending on the direction of head turn, and shows no or minimal fatigue with repetitive provocative maneuvers. If this position is maintained, a less intense but longer lasting nystagmus with reversed direction may appear. For treatment, it is important to identify the side of the affected ear. The response is usually stronger with the head turned to the side of the affected horizontal canal. On this side, nystagmus reversal is more pronounced. It should be noted that the net angle and acceleration of the head rotation should be similar for head turns to the right and left to allow for comparison of nystagmus intensity. In addition, the change from sitting to supine may provoke a slight transient horizontal nystagmus to the healthy side, whereas bending forward usually induces nystagmus to the affected side (22). Sometimes, the supine roll test evokes geotropic nystagmus of equal intensity on both sides. In this case, turning the head 180° from the right to the left lateral position and vice versa may help to identify the affected side (70).
Patients with cupulolithiasis of the horizontal canal have positional vertigo and nystagmus that persist as long as the precipitating head position is held (04; 93). Typically, a head turn to either side in the supine position provokes long-lasting horizontal nystagmus beating away from the ground (apogeotropic nystagmus). The nystagmus increases in intensity over 10 to 20 seconds and decays eventually but persists as long as the head is turned to the side. It is more intense with the head turned to the healthy side. When the patient lies face up, a weak persistent nystagmus is usually present that beats to the affected side and subsides when the head is turned slightly to that side (08). Besides positional nystagmus, pseudospontaneous nystagmus may also be observed in the upright head position beating to the affected ear. Pseudospontaneous nystagmus is a form of positional nystagmus, which occurs with the head in the upright position, making it appear superficially similar to spontaneous nystagmus. Pseudospontaneous nystagmus is attributed to the 30º inclination between the horizontal canal and the horizontal gravitational plane when in the upright position that places the ampulla in a higher position than the rest of the canal. Gravity causes deflection of the cupula and produces horizontal nystagmus beating typically to the side of the horizontal canal affected by cupulolithiasis (08). Pseudospontaneous nystagmus is not specific to cupulolithiasis but may also be observed in canalolithiasis of the horizontal canal (68).
One study found a high proportion of subtle, horizontal, direction-changing apogeotropic positional nystagmus detectable only with video oculography in patients with isolated chronic dizziness and normal MRI of the brain. After treatment with Brandt-Daroff-exercise, dizziness and positional nystagmus subsided in 25% of patients. The authors speculate on a very mild but chronic form of cupulolithiasis of the horizontal canal (52).
Occasionally, both the posterior and horizontal canals of one labyrinth are simultaneously involved. These patients present with horizontal and torsional nystagmus of almost equal magnitude in the Hallpike or supine ear-down position (01).
Benign paroxysmal positional vertigo of the anterior canal. Benign positional vertigo of the anterior canal is rare, accounting for 1% to 2% of patients with benign paroxysmal positional vertigo in large case series (40; 76), although some reports have yielded a considerably higher incidence (49; 16). The rarity of affection of the anterior canal is probably related to the anatomical orientation of this canal, which allows particles to leave the canal simply after lying down and sitting up again. Benign paroxysmal positional vertigo of the anterior canal is provoked by Dix-Hallpike positioning, which, no matter to which side the head is turned, stimulates particle migration within the affected anterior canal (06). The straight head-hanging position seems to be the most sensitive diagnostic test for benign paroxysmal positional vertigo of the anterior canal (16; 107). Thus, diagnostic positioning maneuver cannot identify reliably the side of the affected anterior canal. Theoretically, the symptomatic side can be recognized from the nystagmus direction: it is downbeating and the torsional component always points to the affected ear, irrespective of the side of the Dix-Hallpike maneuver. However, the nystagmus appears to be predominately downbeating with only a small torsional component that can be easily missed in clinical practice, rendering identification of the affected side unreliable (01; 65; 16). The positional downbeating nystagmus in canalolithiasis of the anterior canal may show no latency and no crescendo-decrescendo time course and often does not reverse direction when sitting up from the provoking position (17; 16; 107).
The understanding and treatment of benign paroxysmal positional vertigo has become increasingly complex with refinement of its pathophysiological concepts. The transition from one canal to another and from canalolithiasis to cupulolithiasis of the horizontal canal is a known complication of therapeutic positioning (36; 93) and can also occur spontaneously. In up to 20% of cases, more than one canal is affected producing an atypical directional pattern of positional nystagmus (02; 76). Bilateral involvement has been reported in benign paroxysmal positional vertigo of the posterior canal in 8% (40), but unilateral mimicking bilateral posterior canal benign paroxysmal positional vertigo has also been described (92). As a rule, all patients with suspected benign paroxysmal positional vertigo should be tested for the posterior and horizontal canal variants on both sides.
A group of patients who reported short vertigo spells when sitting up and for a short time immediately afterwards was described (13). These patients did not experience vertigo in the Dix-Hallpike position, but when coming up from a Dix-Hallpike position. Furthermore, positional nystagmus could not be provoked. In some patients, the sitting-up movement was interrupted by retropulsion of the trunk. The authors speculated that symptoms were caused by otoconial debris that moves within the utricle and gravitates towards the utricular side of the cupula of the posterior canal during the act of sitting up. After performing the Dix-Hallpike maneuver once daily at home, all patients became asymptomatic after 2 weeks. The existence of this variant of benign paroxysmal positional vertigo remains highly speculative and needs further confirmation.
The attribute “benign” refers to the time course of benign paroxysmal positional vertigo that is usually self-limiting. However, it can cause considerable distress and morbidity. Elderly patients have a high prevalence of falls (79). Secondary anxiety disorders may develop in predisposed individuals and may persist after an acute bout has settled.
In most patients, positional vertigo resolves spontaneously within weeks or months. The natural course of benign paroxysmal positional vertigo is often characterized by spontaneous remissions and recurrences. The average duration of untreated benign paroxysmal positional vertigo of the posterior canal was estimated at 39 days (45). The natural history of benign paroxysmal positional vertigo of the horizontal canal is shorter as compared to the posterior canal variant: the mean period between the onset and spontaneous remission is 7 days in canalolithiasis and 4 days in cupulolithiasis of the horizontal canal (90). The recurrence rate after successful treatment has been estimated at 15% per year (77). Eighty percent of recurrences occur within the first year after treatment (10).
The liberatory maneuvers have no serious adverse effects. During therapy, the clot may move from one semicircular canal to another instead of staying in the utricular cavity (36), but there is also appropriate therapy for the resulting variants of benign paroxysmal positional vertigo.
For 6 weeks a 58-year-old bank clerk experienced attacks of vertigo lasting about 10 seconds whenever he turned in bed, laid down, or sat up from the supine position. Six years previously he had suffered similar symptoms that resolved spontaneously after a few weeks. Otherwise, he was in good health and on no medication. Dix-Hallpike positioning with the right ear down provoked the patient's typical symptoms and revealed a predominantly torsional nystagmus beating with the fast phase to the lower ear. The nystagmus started after a latency of several seconds, increased rapidly in intensity, and faded out after 15 seconds. A few seconds after sitting up, a few beats of a reversed nystagmus appeared. The neurologic examination was otherwise normal. After a single Epley procedure, no more positional vertigo and nystagmus could be provoked and symptoms resolved.
Benign paroxysmal positional vertigo is caused by dislodged otoconia from the utricle that have entered a semicircular canal where they move freely within the endolymph.
Seven factors that predispose to benign paroxysmal positional vertigo are (1) advanced age, (2) head trauma, (3) other ear disease, (4) migraine, (5) osteoporosis and decreased serum vitamin D, (6) vascular risk factors, and (7) bed rest. In a large series of patients, the condition was idiopathic in about half of the cases, with the incidence increasing with age (02). There is evidence that the number of otoconia attached to the utricle and sacculus decreases with age, possibly due to spontaneous dislodgement (44). The fate of loosened otoconial debris is not known. It has been suggested that they dissolve rapidly in the endolymph (108). However, if this was correct, one would expect the dissolution of otoconia attached to the otolith organs as well. In patients with idiopathic benign paroxysmal positional vertigo, impairment of the otolith-ocular reflex has been documented, suggesting an underlying degeneration of the utricle (101). In 18% of cases, benign paroxysmal positional vertigo commenced within 3 days after head trauma (02). The concussion of the labyrinth may dislodge otoconia from the gelatinous matrix of the utricular macula, leading to benign paroxysmal positional vertigo as soon as these particles have entered a semicircular canal. In a large cohort, 14% of patients with posttraumatic benign paroxysmal positional vertigo had bilateral involvement, compared to 6% of idiopathic cases (54). Vestibular neuritis or other peripheral vestibular disease preceding the onset of benign paroxysmal positional vertigo has been documented in 15% of patients (02), leading to a coexistence of caloric hyporesponsiveness and benign paroxysmal positional vertigo. This seemingly paradoxical finding is explained by the sparing of the posterior semicircular canal in most cases of vestibular neuritis (28). The coexistence of benign paroxysmal positional vertigo with Ménière disease, sudden hearing loss, and other ear disease has been reported (02; 42). Migraine is a predisposing factor as it is more common in patients with idiopathic benign paroxysmal positional vertigo than in those with benign paroxysmal positional vertigo secondary to an identifiable cause (48). The association with migraine has been attributed to recurrent damage to the inner ear during migraine attacks (Baloh and Honrubia 1998; 48; 23). Familial incidence has been described (31). The detachment of otoconia seems to be related to calcium homeostasis. The association between vitamin D levels and the incidence of benign paroxysmal positional vertigo has been demonstrated in a meta-analysis (105). A large population-based retrospective cohort study from South Korea showed that patients with osteoporosis have a 1.75 times higher risk of developing benign paroxysmal positional vertigo than individuals without osteoporosis (15). Hypertension may cause vascular damage to the macula of the utricle, resulting in dislodgment of otoliths (100; 26). An association between benign paroxysmal positional vertigo and stroke has been shown in two population-based studies (100; 53) and may be mediated by the effect of hypertension. A meta-analysis found that patients with benign paroxysmal positional vertigo have higher cholesterol level than controls (19). Also, the disease frequently manifests itself in the postoperative phase of ear or general surgery (02; 32).
The serum level of glycoprotein otolin-1 is increased in patients with benign paroxysmal positional vertigo as compared to controls (71). Otolin-1 is connecting otoliths and otoconial core matrix proteins to the inner ear sensory epithelia and has been suggested as a potential diagnostic marker.
Benign paroxysmal positional vertigo is a peripheral vestibular disorder. The peripheral origin has been ultimately proven by surgical treatment, such as selective dissection of the posterior ampullary nerve (30) and occlusion of the posterior canal (81), which completely abolishes the attacks. The critical role of the posterior canal is supported by the mixed torsional-vertical nystagmus; this reflects the known excitatory connections of the posterior canal with the ipsilateral superior oblique and the contralateral inferior rectus muscle. Finally, peripheral vestibular disorders that often precede the development of benign paroxysmal positional vertigo probably indicate that damage to the otolith organs may be a precondition (25; 02).
Two conflicting theories have been developed to explain the pathophysiology of benign paroxysmal positional vertigo on the basis of a mechanical irritation of vestibular hair cells. The first was the so-called “cupulolithiasis theory” that claimed that heavy particles attached to the cupula render it sensitive to gravitation (85). A change of the position of the head relative to the gravitational vector would cause cupular deflection, and, thus, excitation or inhibition of the hair cells. However, several clinical signs of benign paroxysmal positional vertigo are not explained with this model (11; 67), in particular the short duration of nystagmus.
Now, the alternative concept of canalolithiasis has become widely accepted as it is compatible with the clinical features and variants of benign paroxysmal positional vertigo (34; 11). According to the canalolithiasis concept, mobile otoconia enter the posterior semicircular canal and tend to gravitate to the most dependent point. When the patient is upright, they are located at the base of the cupula and do not have any effect. During the Dix-Hallpike test, the head is rotated backwards in the plane of the posterior canal, inducing movement of the particles within the long arm of the canal away from the cupula (ampullofugal). A gravitating clot of otoconial debris would act like a plunger, causing ampullofugal endolymph and cupular displacement. The ensuing excitation of the posterior canal receptors then results in the mixed torsional-vertical nystagmus. The latency of nystagmus may be attributed to the time taken for the particles to traverse the ampulla before they reach the beginning of the narrow part of the semicircular canal (33). The nystagmus subsides after the particles have reached the most dependent point of the canal and the cupula has returned to the resting position. When the patient sits up again the particles will be shifted in the opposite direction to induce ampullopetal deflection of the cupula and inhibition of the hair cells, resulting in a reversed nystagmus of lower intensity. The clot may disperse with repeated provocations, and this would explain a fatiguing response.
The canalolithiasis concept is supported by several histological and intraoperative findings. Schuknecht described granular deposits both on the cupula and within the semicircular canal in patients who suffered from posterior canal benign paroxysmal positional vertigo prior to death from unrelated disease (85). Mobile endolymph particles have been observed intraoperatively within the posterior canal in patients with benign paroxysmal positional vertigo (82). A prospective study observed particulate matter in the posterior canal in patients with benign paroxysmal positional vertigo during canal occlusion, but not in patients with labyrinthine surgery for other ear disorders (104). In one patient, some particles could be recovered and proved morphologically consistent with degenerated otoconia when studied by electron microscopy (104). It has been shown by means of physio-mathematical models that the prerequisites for benign paroxysmal positional vertigo are an amount of approximatively 62 otoconia within the affected semicircular canal and that these particles have to form an agglomeration in order to exert a hydrodynamic effect when moving in the canal (41). The characteristic time course of nystagmus in benign paroxysmal positional vertigo can be simulated in an animal model with free-floating otoconia using isolated frog semicircular canals (96). However, the most convincing proof for canalolithiasis is provided by the efficacy of positioning maneuvers, which aim to clear the affected canal from mobile particles (88; 27).
Variants of benign paroxysmal positional vertigo can be similarly explained by the canalolithiasis concept (40). In canalolithiasis of the horizontal canal, a turn of the head toward the affected ear while supine induces ampullopetal movement of the clot and endolymph flow. Excitation of the hair cells results in transient horizontal nystagmus beating ipsilaterally, ie, to the undermost ear. The direction of nystagmus reverses with a head turn to the other side as the clot is shifted in the opposite direction. Only the rare variant of persistent direction-changing horizontal nystagmus beating away from the ground is not compatible with canalolithiasis. It is best explained with cupulolithiasis of the horizontal canal that renders the cupula sensitive to gravitation and causes nystagmus as long as the head remains in the precipitating position (04). In cupulolithiasis of the horizontal canal, the persistent horizontal nystagmus in supine position reflects the orientation of the cupula of the horizontal canal with respect to the head; when the patient lies with face up, gravity causes an utriculopetal deflection of the cupula, resulting in a nystagmus beating to the affected side. Horizontal nystagmus ceases in a null position when the patient turns his head slightly to the affected side, thus, aligning the cupula with the gravity vector (08).
Benign paroxysmal positional vertigo is said to be the most common cause for vertigo, particularly in the elderly. Estimates of the prevalence of benign paroxysmal positional vertigo range widely as the time course is transitory and often patients are examined during the symptom-free period. A population-based survey in Germany found a lifetime prevalence of 3.2% in women and 1.6% in men, whereas the 1-year prevalence was 2.3% and 0.9% respectively. The cumulative incidence reached almost 10% at the age of 80 years (100). Another study that did not require strict diagnostic criteria estimated the incidence to be 107 cases per 100,000 per year (29). The prevalence of benign paroxysmal positional vertigo in unselected geriatric populations is about 10% (79; 64). In dizziness clinics, about one out of five patients presents with benign paroxysmal positional vertigo.
In idiopathic benign paroxysmal positional vertigo, women outnumber men by about 1.75:1, and the incidence increases with age. This preponderance of age and sex is less evident in benign paroxysmal positional vertigo after head trauma and peripheral vestibular disorder (02). In childhood, the disease is exceedingly rare.
A seasonal variation of benign paroxysmal positional vertigo peaking in winter and spring has been observed. A vertigo outpatient clinic found a moderate negative correlation between 25-hydroxyvitamin D levels and benign paroxysmal positional vertigo numbers each month (91).
Epley advised patients to keep the head upright for 48 hours after successful treatment to ensure that the particles would not fall back into the posterior canal (27). Posttreatment restrictions have been shown to be effective in a meta-analysis (43). However, they are unpleasant for patients, have only a minor effect on the recurrence rate, and are, thus, not recommended by many experts.
A randomized controlled trial showed that recurrences of benign paroxysmal positional vertigo can be prevented with supplementation of vitamin D 400 IE and 500 mg of calcium carbonate twice a day in patients with serum vitamin D levels lower than 20 ng/mL (50). A meta-analysis including the above-mentioned trial and four nonrandomized studies supported this finding (51).
Benign paroxysmal positional vertigo must be primarily differentiated from central positional vertigo and nystagmus due to a lesion to the vestibular nuclei or caudal cerebellum. Usually, the diagnosis of benign paroxysmal positional vertigo is not problematic. However, variants may exhibit features formerly attributed to central positional vertigo, such as the change of nystagmus direction in horizontal canal benign paroxysmal positional vertigo. A central lesion should generally be suspected when features different from those described for benign paroxysmal positional vertigo are present or when brainstem or cerebellar signs are found. Single characteristics of benign paroxysmal positional vertigo like latency, duration, and time course of nystagmus, and fatigability with repeated positioning can also occur in central positioning vertigo (14; 66). However, it is unlikely that a central lesion mimics the entire nystagmus pattern of benign paroxysmal positional vertigo.
Central positional nystagmus often exhibits a mixture of horizontal, vertical, and torsional components, with a variable combination of each component, depending on the positional maneuver (21). The most common types of central positional nystagmus are downbeating nystagmus in the head-hanging position and apogeotropic nystagmus in the lateral supine position (07; 21; 20). Central positional nystagmus may present with direction-changing apogeotropic nystagmus in the supine roll test, mimicking cupulolithiasis of the horizontal canal. However, in central positional nystagmus, the intensity of nystagmus is at its peak initially and decreases exponentially over time (21), whereas it gradually builds up over 10 to 20 seconds and then decreases slowly in cupulolithiasis of the horizontal canal (04). In addition, patients with apogeotropic positional nystagmus usually exhibit horizontal nystagmus in the upright and in the supine position that may help to differentiate central positional vertigo from benign paroxysmal vertigo: in the latter the intensity of this nystagmus increases from the upright to the supine position whereas in the former this is usually not the case (20). Purely vertical or torsional nystagmus, verified by examination under Frenzel glasses, should always be considered of central origin; however, positional vertigo and transient positional predominantly downbeating nystagmus during the Dix-Hallpike maneuver or in the straight head hanging position have also been attributed to canalolithiasis of the anterior semicircular canal in some patients (06). These patients had normal imaging studies and further neurologic examination was unremarkable except for signs of posterior canal canalolithiasis in some of them. In contrast, patients with central positional downbeating nystagmus rarely complain about positional vertigo.
Central positional nystagmus often persists as long as the precipitating head position is maintained, and it usually does not fatigue with repetitive positioning. Typically, patients with central positional nystagmus present with additional neurologic findings that cannot be explained by benign paroxysmal positional vertigo such as truncal ataxia, perverted head-shaking nystagmus, gaze-evoked nystagmus, and impaired smooth pursuit (21).
Sometimes, benign paroxysmal positional vertigo can be mimicked by vestibular migraine. However, several features help to distinguish this disorder from benign paroxysmal positional vertigo: short-duration symptomatic episodes and frequent recurrences, manifestation early in life, migrainous symptoms during episodes with positional vertigo, and atypical positional nystagmus (99). Other causes for positional nystagmus can be neurovascular compression of the eighth cranial nerve, perilymph fistulas, positional alcohol nystagmus, and rarely, macroglobulinemia.
The term “light cupula” has been coined to describe persistent geotropic direction-changing positional nystagmus in the supine lateral head positions in patients without central neurologic signs and with normal results in cerebral imaging (39; 47). This type of nystagmus is neither compatible with mobile otoconia in a semicircular canal nor with dense otoconia attached to a cupula. However, there seems to be an association between this disorder and canalolithiasis and cupulolithiasis, as some of these patients have developed classical variants of benign paroxysmal positional vertigo at follow-up (39; 47; 83). Furthermore, an association with sudden sensorineural hearing loss has been described (56). It has been suggested that this rare type of positional vertigo and nystagmus may be due to changes of the density of the cupula or the endolymph (61), but this remains speculative. Spontaneous remission within 1 week has been described in 60% of patients (83).
The observation of typical nystagmus during positional testing confirms the diagnosis of benign paroxysmal positional vertigo. Further investigations are not required. In cases with suspected coexisting peripheral vestibular disease, the appropriate vestibular and audiologic tests should be performed. When central positional vertigo cannot be ruled out on clinical grounds, MRI of the posterior fossa is required.
Vestibular abnormalities have been found in patients but do not contribute to the diagnosis. Caloric hyporesponsiveness has been described in 30% of patients with idiopathic posterior canal benign paroxysmal positional vertigo (02) and horizontal canal benign paroxysmal positional vertigo (03). Caloric hyporesponsiveness in horizontal canal benign paroxysmal positional vertigo can be reversible after a successful liberatory maneuver and has been attributed to partial plugging of the horizontal canal (94).
Therapeutic maneuvers. New treatments have been developed on the basis of the canalolithiasis theory with the aim of clearing the affected canal from debris. This approach is unique because it addresses the underlying pathogenetic mechanism, whereas in other vestibular disorders rehabilitation seeks to promote central compensation of an established vestibular deficit.
Benign paroxysmal positional vertigo of the posterior canal. There are two highly effective conservative therapies for the common posterior canal benign paroxysmal positional vertigo that induce the displacement of the otolithic debris through the open end of the posterior semicircular canal into the utricular cavity where they no longer produce positional vertigo.
Epley introduced a procedure wherein the posterior canal is rotated backwards close to its planar orientation (27).
The maneuver consists of a series of successive head positions each of about 90 degrees displacement. Each positioning is performed rapidly and is maintained for 30 seconds or until positional nystagmus has disappeared, indicating cessation of endolymph flow. Patients should, therefore, be asked to keep their eyes open. A positional nystagmus appearing in the second and third head position and beating in the same direction with respect to the head indicates successive movement of the particles toward the utricular cavity and predicts a favorable outcome (80). Vibration of the mastoid during the procedure has been recommended by some authors, but it does not improve treatment outcome (43). Accurate video demonstration of the Epley maneuver is available on video-sharing websites such as YouTube (55).
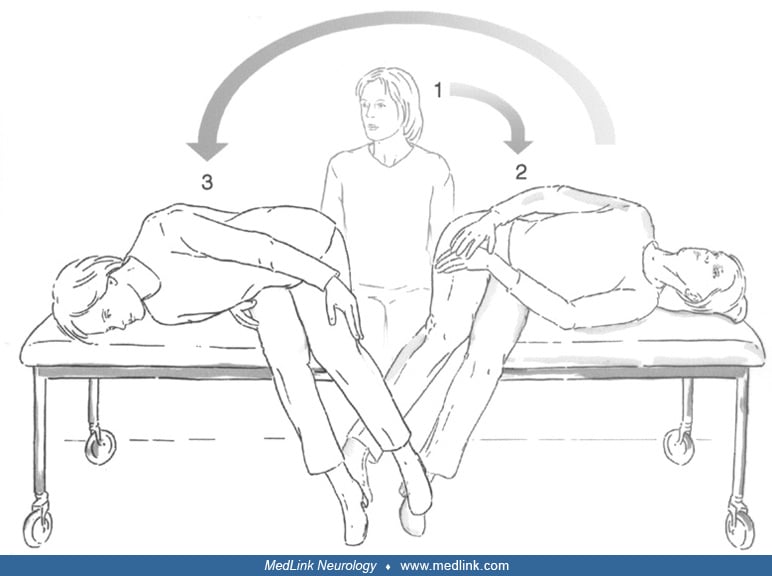
The Semont maneuver involves a 180-degree swing of the head in the plane of the posterior semicircular canal (88).
The examiner stands in front of the patient who is seated on a couch with the head rotated 45 degrees away from the affected ear. Then the patient is brought with a fast movement to a lying position on the side of the pathologic ear with the lateral occiput resting onto the couch. In this position vertigo is triggered with torsional nystagmus beating toward the undermost ear. After being kept in this position for a minute, the patient is swung rapidly onto the opposite side of the couch, maintaining the turn of the head. The maneuver is effective when another bout of vertigo with nystagmus beating toward the affected, now uppermost ear, appears in this position. The efficacy of the Sémont maneuver can be increased with an overextension of the head by 60° below the earth horizontal line during the movement of the patient toward the affected side (95).
Epley’s and Semont’s maneuvers are highly effective when performed properly. After a single maneuver, complete recovery is achieved in 50% to 80% of patients (88; 37; 89). The maneuvers should be repeated immediately when positional vertigo and nystagmus are still present, as this increases the success rate to 80% to 90% (27; 89; 73). Randomized, controlled trials have shown that the Epley maneuver is clearly more effective than a sham procedure or no treatment (38). The short-term efficacy of Epley’s maneuver as assessed 24 hours after a treatment session has been shown to be 80% versus 10% spontaneous remissions in a control group (103). A meta-analysis identified 11 randomized, controlled trials of the Epley maneuver. Patients treated with the Epley maneuver were about four times more likely to demonstrate symptom resolution at the time of first follow-up than patients treated with a sham maneuver and untreated controls (38). When the Epley maneuver fails, the Semont maneuver can be performed as an alternative, or vice versa. Both maneuvers are equal in terms of efficacy (38). A double-blind randomized trial has shown that the short-term efficacy of a single Semont maneuver as assessed 24 hours after treatment is 87% versus 0% in a control group (73).
There is evidence that therapeutic maneuvers are even useful in patients who, in spite of a typical history, do not show nystagmus on diagnostic positioning (97; 35). The reason may be a limited amount of particles in the affected semicircular canal that is sufficient to evoke vertigo but not to stimulate vestibulo-ocular pathways.
For patients who do not respond immediately to the Epley or Semont procedure, as well as for those with frequent recurrences, a modified Epley procedure can be used for self-treatment at home (84).
Instructions for the patient: (A) Start by sitting on a bed and turn your head 45 degrees to the left. Place a pillow behind you so that on lying back it will be under your shoulders. (B) Lie back quickly with shoulders on the ...
This procedure has proved more effective than the conventional Brandt-Daroff exercises that have the merit of being the first positional procedure for self-treatment of benign paroxysmal positional vertigo (09).
Benign paroxysmal positional vertigo of the horizontal canal. In canalolithiasis of the horizontal canal, the supine patient is rotated 270 degrees in steps of 90 degrees in the plane of the horizontal semicircular canal toward the healthy side to free the affected canal from debris (69).
With this maneuver, positional vertigo resolves in about 70% of patients after one treatment session (78). Alternatively, the patient can be advised to sleep with the head turned to the healthy side for one night (forced prolonged positioning). A randomized controlled trial showed that forced prolonged positioning resolves canalolithiasis of the horizontal canal in 77% versus 11% with a sham maneuver as assessed after 24 hours (74). Compared to both aforementioned maneuvers, two randomized trials have shown that the Gufoni maneuver is similarly effective with response rates of 61% (63) and 89% (72), evaluated 1 hour after treatment with two maneuvers: the patient is brought quickly from a sitting position with the head straight ahead into a side-lying position on the unaffected side and remains in this position for 1 minute after the end of geotropic nystagmus. Then the head of the patient is quickly turned 45 degrees to the unaffected side (with the face downwards) for 2 minutes. Finally, the patient returns to sitting. Up to now, there is no convincing evidence that one of these three maneuvers is more effective than the others (63).
Cupulolithiasis of the horizontal canal can be treated with a head-shaking maneuver, mastoid oscillation, forced prolonged positioning, or a variant of the Gufoni maneuver. In a randomized controlled trial, shaking the head for 15 seconds at about 3 Hz with the head pitched forward approximately 30° resolved vertigo and nystagmus in 47% of patients within 30 minutes after treatment (62). A variant of the Gufoni maneuver is similarly effective (62a): the patient is quickly brought from the sitting position into a side-lying position on the affected ear. After 1 minute, the head is quickly turned 45° upward (with the face upward). After 2 minutes, the patient returns to sitting (24). A randomized controlled study showed that mastoid oscillation with a vibrator in both lateral supine positions is as effective as the Gufoni maneuver (57). During these maneuvers, transition from cupulolithiasis to canalolithiasis of the horizontal canal often occurs, which requires additional therapeutic maneuvers for the latter condition (24; 62; 58). A randomized controlled trial showed that forced prolonged positioning in patients with cupulolithiasis of the horizontal canal leads to resolution or conversion to canalolithiasis in 61% versus 18% with a sham maneuver (74).
Benign paroxysmal positional vertigo of the anterior canal. Treatment of this rare variant has not been thoroughly evaluated. For liberation of the anterior canal from particles, positional treatment should start from sitting with the head straight. Then the patient should be reclined until reaching a deep head-hanging position with the head still straight. After 30 seconds the patient’s head is quickly moved forward “chin to chest.” Finally, the patient should sit up again (106; 18; 107). Gentle head percussion may help to dissolve otoconia from the cupula when cupulolithiasis is suspected and to promote particle migration through narrow passages of the canal. Plugging of the affected anterior canal can be effective in patients who do not respond to positioning maneuvers (12).
Recurrent benign paroxysmal positional vertigo. As patients with benign paroxysmal positional vertigo often experience recurrences, self-treatment at home with the maneuver initially effective for treatment may be advised. However, this approach is limited as the type of benign paroxysmal positional vertigo was identical to that observed during the previous episode in only 24% of patients in a case series (58). A web-based system for identification of the affected canal on the basis of three questions and allocation of a tailored self-treatment maneuver has shown to be more effective for self-treatment of recurrent benign paroxysmal positional vertigo than self-treatment with the maneuver effective for the previous episode (59).
Drug treatment. Medication is usually not a reasonable approach for treatment of benign paroxysmal positional vertigo. However, when positional testing has provoked nausea, vestibular sedatives can be administered before performing a therapeutic maneuver.
Surgery. Surgery of the posterior semicircular canal can be considered in those very rare patients with longstanding benign paroxysmal positional vertigo who have not responded to appropriate and repeated therapeutic positions. As surgical procedures, both plugging of the posterior semicircular canal by the transmastoid approach (81) and transection of the posterior ampullary nerve by the middle ear approach (30) have proven effective for permanent relief from posterior canal benign paroxysmal positional vertigo.
There is no known correlation between benign paroxysmal positional vertigo and pregnancy.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Michael von Brevern MD
Dr. von Brevern of Charité University Hospital has no relevant financial relationships to disclose.
See Profile
Thomas Lempert MD
Dr. Lempert of Charite University Hospital has no relevant financial relationships to disclose.
See Profile
Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
Neuro-Oncology
Dec. 13, 2024
Neuro-Ophthalmology & Neuro-Otology
Dec. 02, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 24, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuromuscular Disorders
Oct. 29, 2024