






















































Epilepsy & Seizures
Tonic status epilepticus
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Neonatal brachial plexus palsy can be a debilitating injury that leads to long-term disability in the infant. Although the majority of cases do recover full function of their arm, others must undergo surgery or other treatments to improve function. This article describes the pathology and anatomy of brachial plexus palsy, provides tips to examine an affected patient, and reviews the available treatment options.
|
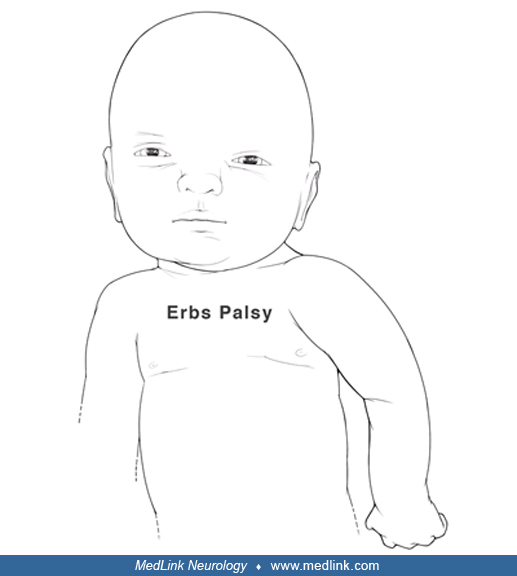
• The most common brachial plexus palsy involves the upper roots, C5 and C6, and is called Erb palsy. | |
|
• The spontaneous recovery rate is 60%, and some children suffer permanent impairment. | |
|
• Surgical treatment is usually offered between 3 to 6 months of age for primary repair; otherwise, patients can undergo secondary procedures around 12 to 18 months of age. | |
|
• A multidisciplinary approach with the pediatrician, physical and occupational therapists, and the surgeon is very helpful when treating an infant with brachial plexus palsy. |
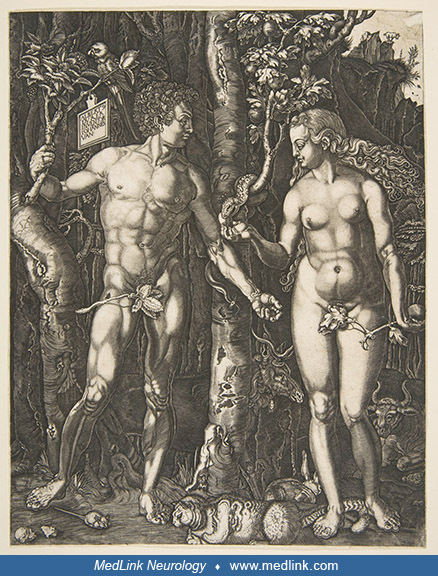
Several authors have suggested that German artist Albrecht Dürer (1471–1528) painted a case of Erb palsy in his Haller Madonna (before 1505), in part because of the internal rotation and pronation of the left arm, with accentuation of the skin folds of the anterior axillary region and drooping of the left shoulder (92; 139; 146). A suggested alternative diagnosis is pseudoparalysis from a fractured clavicle or humerus, which can resemble a brachial plexus palsy (139), although clavicular fractures can coexist with neonatal brachial plexopathies in about 10% of cases of obstetric brachial plexus palsy. However, despite the common modern practice of assigning putative diagnoses to centuries-old art, the child is holding a piece of fruit in his left hand, with the same posture that Dürer painted Eve holding a piece of fruit in her left hand (139). A child with an Erb palsy would be very unlikely to hold a piece of fruit in the pathologic hand. The posture of the child is typical of the Mannerism style of northern European paintings at the time, which featured hyper-idealization, exaggerated poses, distorted human forms, and awkward movement.
William Smellie. Neonates who have neurologic deficits have been observed since the time of the ancient Greeks and Hippocrates (76). Brachial plexus palsy related to the birth process, “obstetric brachial palsy,” was described by Scottish obstetrician William Smellie (1697–1763) in a textbook originally published in 1754 titled A sett of anatomical tables, with explanations, and an abridgment, of the practice of midwifery (158; 160; 161; 162; 111; 134; 150; 157).
Smellie was highly regarded for his obstetrical skills and for his monographs and atlas showing elaborate depictions of the development of the fetus, the birth process, and obstetric problems (158; 160; 161; 159; 162). Smellie is particularly known for his incredible illustrations of pregnant women and fetuses, drawn from cadavers. Some of his illustrations vividly show the circumstances that often led to obstetrical brachial plexus palsies in neonates. However, the large number of pregnant cadavers that Smellie was able to amass for his huge atlas led to recent allegations that he and the Hunter brothers encouraged or arranged for the murder of pregnant women to complete their projects (150).
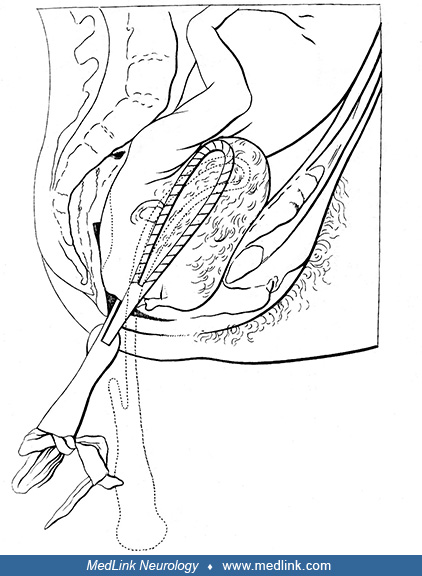
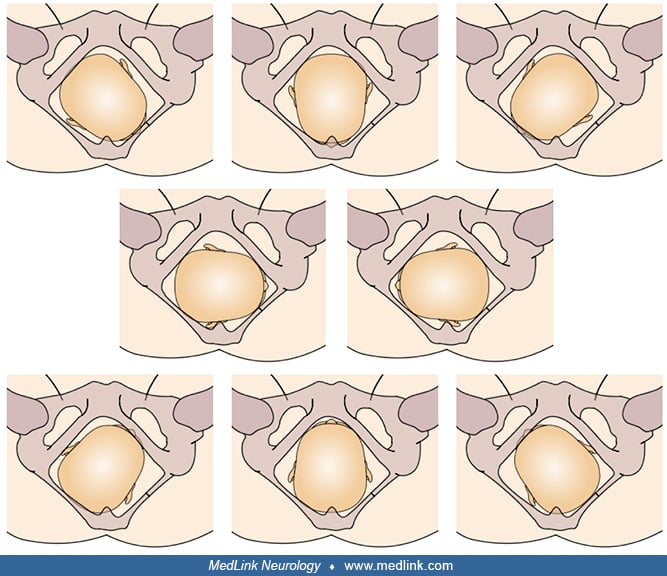
Traction on the arm at this point can lead to severe traction on the brachial plexus and cervical nerve roots. (Source: Smellie W. A treatise on the theory and practice of midwifery, to which is added, a set of anatomical plate...
(Source: Smellie W. A treatise on the theory and practice of midwifery, to which is added, a set of anatomical plates, exhibiting the various cases that occur in practice, accurately engraved, with explanations. London: Alexand...
Although Smellie is frequently credited with describing obstetrical brachial plexus palsy, his description was quite limited. He described, in rather vague terms, transient bilateral arm weakness in a neonate following a complicated delivery that occurred in 1746 (161). The initial presentation was breech, but this was converted to a face presentation that resulted in the arrest of labor. Smellie was able to deliver the child with forceps. As Smellie later recounted, "The long compression had rendered the arms paralytic for several days, though this misfortune was soon remedied by friction and embrocations [a liquid used for rubbing on the body to relieve pain from sprains and strains]" (161).
Wilhelm Heinrich Erb. German neurologist and neurophysiologist Wilhelm Heinrich Erb (1840–1921) first compared neonatal brachial plexus palsy with that found in adults and concluded that it involved the upper roots (184; 147).
Guillaume-Benjamin-Amand Duchenne (de Boulogne). The term “Duchenne-Erb palsy” was coined because French neurologist Guillaume-Benjamin-Amand Duchenne (de Boulogne) (1806–1875) received credit for describing the brachial plexus palsy following delivery of affected newborns (46; 22; 142; 86; 64; 129; 143; 147).
In 1862, Duchenne published a pioneering collection of photographic images of patients with various neuromuscular diseases, including one with an Erb (upper plexus) palsy (47). Duchenne also recognized an association with clavicular fractures, subacromial dislocations, and ipsilateral brachial plexus injuries.
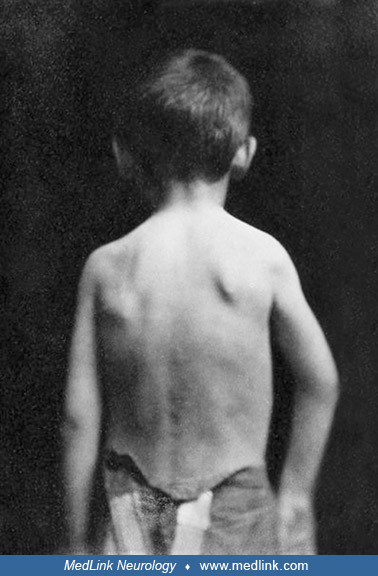
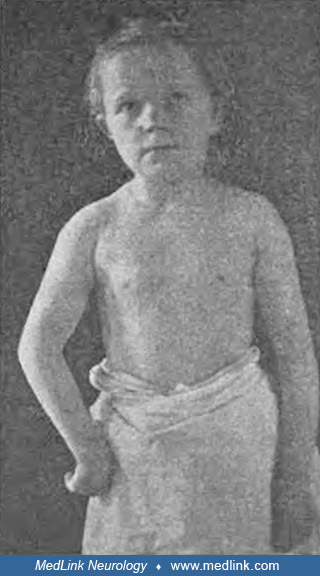
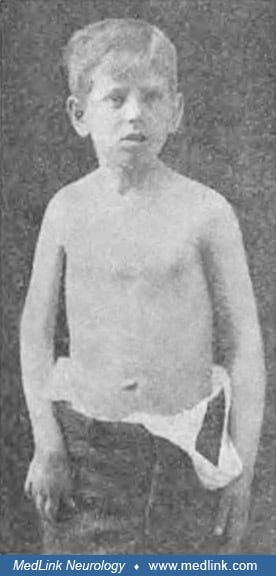
As described by Duchenne: Posterior and external dislocation of the shoulder (subacromial dislocation), dating from birth, in a 6-year-old boy, characterized: (1) by a relief located below the posterior angle of the acromion, f...
In 1872, Duchenne further described the child that he had photographed in 1857. A 6-year-old boy was presented to Duchenne for treatment of congenital right arm weakness (46).
|
In March 1857, a young boy named Théophile Bigot, aged 6, was presented to me to be treated for a congenital paralysis of the upper right limb. The movements of the latter were, in fact, so hampered since his birth that he could not use them. All muscles responded normally to electrical excitation. His right shoulder was deformed; the attitude of the arm on this side was abnormal (see the figure drawn from the photograph I took of it). One noticed on the posterior face of the stump of the shoulder, a little below the posterior angle of the acromion, a rounded relief that indicated, in this point, the presence of the head of the humerus, which, moreover, one recognized perfectly by touch. Anteriorly, the shoulder stump presented a slight subacromial depression, but without apparent relief of the coracoid process, and the head of the humerus was no longer found in its normal position. This head of the humerus appeared to be straddling the posterior edge of the glenoid cavity. It was certainly not in the infraspinatus fossa; it was difficult to explain it, but what was indisputable was that it had remained thus incomplete for 6 years. The elbow, carried a little forward, was set aside from the body and could not be brought closer to it; attempts to obtain it caused pain. The humerus was kept in rotation inwards [internally rotated], and one could not mechanically impart to it the slightest movement in the opposite direction without making the child cry out. The forearm was a little flexed on the arm, without it being possible to extend it completely. The voluntary movements of the arm were weak and limited like those of the forearm. | |
|
(46), translation by Dr. Douglas J Lanska |
(Source: Duchenne [de Boulogne] GB. Paralysies obstétricales infantiles des membres supérieurs avec ou sans fractures, luxations ou autres complications. In: De l'électrisation localisée et de son application à la physiologie, ...
Duchenne noted that three other children were referred at around the same time with the same deformity of the shoulder and with the same disturbances in the movements of the arm on the shoulder. He recognized the characteristic signs of scapulohumeral dislocation in all these children. The cause of this dislocation appeared to be identical in all these cases and, in particular, to be the result of extreme force being applied during delivery:
|
The parents of the children said in fact that their birth had been laborious—that, to extract them, [the midwife or physician] had to exercise long and violent pulls, using a finger or a hook passed under one of the armpits, and that the limb exposed to these pulls had been deprived of movements after their birth. It was precisely on this side that the dislocation existed, the production of which is very well explained by the violence exerted on the armpit. | |
|
(46), translation by Dr. Douglas J Lanska |
With more extensive obstetric brachial plexus palsies, Duchenne also noted the effects of the weakness on the posture of the arm and hand, the development of contractures, and the changes in strength over time. One child was born in "dire circumstances" with a shoulder presentation—a malpresentation in which the fetus is in a transverse lie (ie, its vertebral column is perpendicular to that of the mother) so that the leading part (the part that first enters the birth canal) is an arm, a shoulder, or the trunk. In addition, the umbilical cord was wrapped around his neck, and the delivery was "long and arduous." He sustained perinatal asphyxia and was "hardly brought back to life." As further evidence of birth trauma, he had a fractured ulna near the elbow joint. After his birth, he did not move his upper right arm. Initially, Duchenne noted no clear difference in the appearance of the right arm and hand, but in a few months, the hand gradually became deformed and less developed than the opposite arm. Duchenne concluded that, "Atrophic paralysis and deformation of the hand are the result of the lesion of some nerves involved in the fracture of the bones of the forearm during the maneuver of childbirth" (46), translation by Dr. Douglas J Lanska.
Duchenne applied faradic currents to the arm, and, over time, the child's hand function and appearance improved, though the child still had limited function of the arm and hand.
|
I saw .... the shape of the hand return to its normal state by the return of their tonic force. [This figure] was drawn from the photograph I made of the hand of the sick little one after his treatment. If we compare it to [the hand] photographed and then drawn during the treatment, we notice that the claw no longer exists ... that the last two phalanges have extended and that the first have flexed a little. This reestablishment of the normal shape of the hand was due to the development of the interossei. The eminences had also developed as well as the atrophied muscles of the forearm. ... [T]he movements of the upper limb had gained in strength and extent, but they had not recovered their independence. ... I was hopeful that with the help of certain gymnastic exercises prescribed by me, [he would continue to improve]. Two years later, this young boy came to show me that this hope had come true; he used that hand almost as well as the other. | |
|
(46), translation by Dr. Douglas J Lanska |
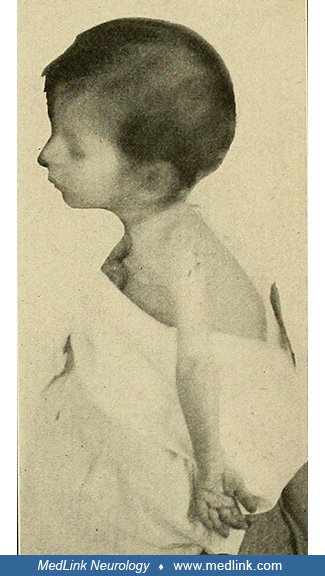
Duchenne presented one further illustration of the "deformation of the hand,” following a childhood obstetric subacromial dislocation.
|
The disorders caused, in these children, in the movements and in the attitude of the limb, by the subacromial dislocation [of the acromioclavicular joint], may well suggest the existence of a congenital cerebral palsy of the upper limb; in either case, the elevation of the arm is difficult and limited. Furthermore, the hand is pronated, and the arm internally rotated... [I]n all these children, there existed, moreover, a veritable paralysis that had been occasioned by the lesion of the brachial plexus and which was more or less complete and more or less serious. Thus, in one of them ... some muscles were atrophied or responded weakly to electrical excitation (the biceps and the anterior brachialis) or had lost their electrical contractility (flexors of the fingers and interossei). | |
|
(46), translation by Dr. Douglas J Lanska |
Augusta Klumpke. In addition, brachial plexus injury to the lower roots (C8-T1) was first described by American-born French neurologist Augusta Klumpke (1859-1927) in 1885 (95; 132; 20; 21; 64; 153; 188; 51).
Erb palsy in Kaiser Wilhelm II of Germany. In 1859 Wilhelm was born in Berlin to Victoria (or "Vicky"; 1840-1901), Princess Royal, the eldest daughter of Britain's Queen Victoria (1819-1901), and Prince Frederick William of Prussia (the future Frederick III; 1831-1888)--a marriage intended to unite the royal families of Britain and Germany. A traumatic breech birth resulted in an Erb palsy, which left Wilhelm as an adult with a withered left arm about 6 inches (15 centimeters) shorter than his right. In a letter to her mother, Queen Victoria, Vicky wrote, "The idea of his remaining a cripple haunts me." She felt a cure had to be found, and subjected Wilhelm to various bizarre procedures that served only to traumatize the boy. Beginning at 6 months of age and continuing for years, a hare was slaughtered in his presence twice a week to provide "animal baths"; the still-warm flesh of the dead hare was then tied around boy's left arm, with the hope that the vitality of the wild animal would somehow be transferred into the boy's dysfunctional arm. As the boy became more mobile, they tied his good arm behind his back thinking that this would force him to use and strengthen his weak arm, but this was of course a plan destined to fail and one that only heaped frustration and agony on the growing boy. In another letter to her mother, Queen Victoria, Vicky wrote: "It [He] gets so fretful and cross and violent and passionate that it makes me quite nervous sometimes." For most of his childhood, Wilhelm's withered arm was also subjected to electrotherapy treatments that were not only painful but that succeeded only in provoking a nervous reaction in the young boy. It was only at age 12 that the many, varied, and painful attempts to cure his disability were finally abandoned. Even then, Wilhelm's deformity was considered an embarrassment that had to be kept hidden from public view, but the deformity was, of course, still present, to his mother's shame. Vicky viewed the delivery of a less than physically perfect heir to the Prussian throne as a personal failure and, moreover, one that raised concerns about the ability of her son to thrive in the militant court atmosphere that was his destiny. In still another letter to her mother, Vicky confessed that the deformity "spoils all the pleasure and pride I should have in him." Although her rejection of her son stemmed in part from her failure to bring forth a strong male heir, no doubt compounded by the responsibility she felt (or blame she perceived) as the English mother of a German heir, it was nevertheless a quite terrible reaction by a mother toward her own son and one that Wilhelm reacted to in anger and resentment.
In most of the extant photographs and paintings, the royal photographers and painters concocted a remarkable diversity of subterfuges to obscure the left hand or to otherwise conceal its deformity (although some paintings and sculptures adopted an altogether different approach: just portray the arm and hand as if they were normal!). Photographs and paintings show Wilhelm holding a pair of white gloves in his left hand to make the arm seem longer, hiding his left hand under crossed arms, hiding his left arm behind his back, covering his left hand with his right on the hilt of a sword, putting his left hand in a pocket, holding his left hand with his right, holding a cane to give the illusion of a useful limb posed at a dignified angle, or hiding his hand and arm under a cape. There are also some officially sanctioned paintings and sculptures that portray his left arm and hand as if they were normal.
Prince Wilhelm c1871 as a 12-year-old boy in Berlin. Note the small size of his left hand, a result of his Erb palsy from obstetric trauma. The white glove is a prop, intended to suggest, by extension, a longer left arm. Despit...
Kaiser Wilhelm II in 1905. Wilhelm in dress military regalia, wearing an elaborate "eagle spike" Pickelhaube helmet. He is resting his diminutive and deformed left hand on a sword hilt and then covering it with his normal right...
The disability from obstetric brachial plexus palsy clearly affected Wilhelm’s emotional development, and seemingly caused him to over-compensate through aggressiveness and competitiveness. Instead of his life providing a bridge to strengthen the ties of Britain and German, he ultimately initiated actions that split them apart.
Surgical case series from Leon Pierce Clark and colleagues (1905–1907). In 1905, neurologist and psychiatrist Leon Pierce Clark (1870–1933), neurosurgeon Alfred S Taylor (1869–1942), and pathologist Thomas P Prout described the results of 20 dissections and many experiments on infantile cadavers as well as a series of operations on seven clinical cases, which indicated that tension (overstretching) of the nerve roots of the brachial plexus was the basis of obstetric brachial plexus palsies. In this surgical case series from the beginning of the 20th century, two of seven cases (29%) died in the perisurgical period (34). This series gives a useful perspective on the range of presentations, the operative findings, and the degree of recovery achieved at that time.
Case 1. A 25-month-old girl with complete paralysis of her left arm. She was a first child and with vertex presentation. Labor was prolonged and difficult. Instruments were used, and strong traction was exerted on the head. Complete paralysis of the left arm was noted a few days after birth. No spontaneous improvement resulted during the first 2 months after birth. After 4 months, slight flexion of the fingers and wrist was possible. Contractures contributed to the deformity. The child died 19 hours after surgery in 1903.
Case 2. A 10-year-old girl with typical "laceration" (stretch) brachial birth palsy. Typical birth palsy of a milder grade was present. She was the fourth child and with vertex presentation and marked asphyxiation after labor lasting 7 hours. "Forceps were used and great force employed in delivery." Palsy of the right arm was at once noticed. Improvement began at the end of 4 months and continued for 1 year. Slight contractures occurred in all the paralyzed muscles, producing a characteristic deformity. At operation in 1903, the fifth and sixth nerve roots were found to be damaged. A 1 cm portion was excised, and the proximal and distal ends were sutured. Marked return of muscle power began 3 months after surgery and continued for 2 years.
Case 3. An 8-year-old boy with typical "laceration" (stretch) brachial birth palsy. Obstetric birth palsy of the right arm (Erb palsy) was present. He was the third child and with vertex presentation. Labor lasted 14 hours, and instrumentation was finally used. After prolonged and forceful traction, he was born asphyxiated and with total paralysis of the right arm. During the first year, there was some slight return of power, but there was no subsequent improvement. The right arm and shoulder girdle were distinctly underdeveloped compared to the left side and in x-ray images. The shoulder was a flail joint. The elbow could not be extended more than 150 degrees. The wrist was markedly flexed and adducted (toward the ulna). The extremity was cooler than the normal one, and the hand was purple-colored. The bones on the damaged side were between 12% and 20% shorter than the corresponding bones on the opposite side. There was a pronounced posteroinferior dislocation of the shoulder. The coracoid and acromion processes were longer, more pointed, and bent more downward and forward than normal. At operation in 1903, the upper trunk of the brachial plexus was found to have been torn apart, and the torn ends were displaced and adherent to other structures with connective tissue. The damaged tissue was excised, and the ends sutured. The boy made steady but very slow progress postoperatively, and after 9 months, he was able to move his arm slightly.
Taylor and Prout presented further information on the surgical treatment of brachial birth palsy in 1907 (169). Further return of function was evident in the arm of this patient 2 years and 7 months following the first operation.
Case 4. An 8-month-old boy with typical "laceration" (stretch) brachial birth palsy of the right arm. “Typical birth palsy” was present. He was the third child and with vertex presentation. Labor was 72 hours long and was conducted by a midwife, who, when the head was born, pulled forcibly on it to deliver the shoulders, which were caught (shoulder dystocia). Two days later, paralysis of the right arm was noticed. No improvement occurred prior to operation. At operation, only the fifth and sixth cervical roots were affected near where they join to form the upper trunk of the brachial plexus. The child died 3 days after surgery.
Case 5. A 4.5-year-old boy with a mild degree of "laceration" (stretch) brachial birth palsy of the right arm. He was the second child and with vertex presentation. “Very difficult labor. Instruments used after 19 hours and 'great pulling' was employed." The right arm was paralyzed at birth. Movements began to return at the end of 3 months, but by the age of 6 months, the improvements had stopped. Paralysis, deformity, contractures, and atrophy were typical of a medium-grade birth palsy. At operation in 1904, a portion of the damaged fifth and sixth roots and the proximal portion of the upper trunk of the brachial plexus were resected and the free ends sutured. No movement was evident in C5- and C6-innervated muscles for 3 months. Slow improvement occurred thereafter, but the child was poorly cooperative with instructions, so little hope of significant further progress was expected.
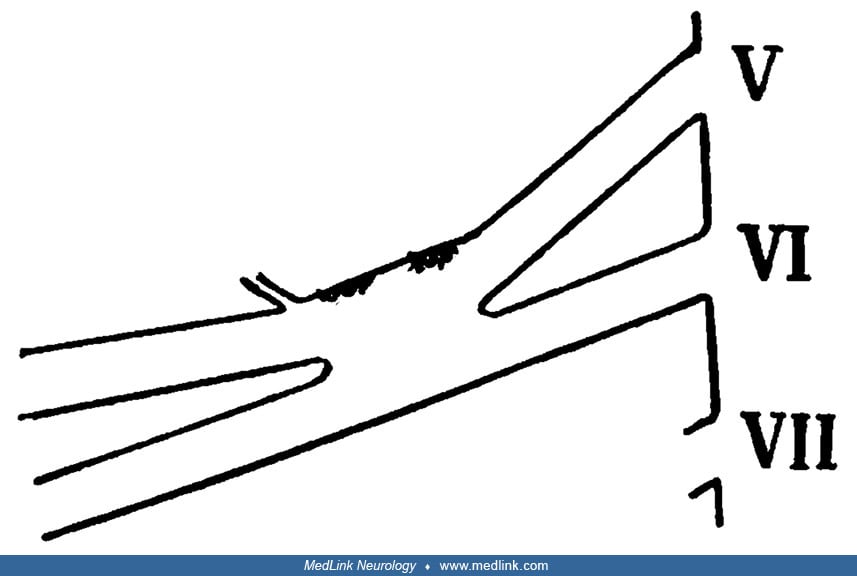
Case 6. An 11-year-old girl with a mild degree of "laceration" (stretch) brachial birth palsy of the left arm. She was the first child and with vertex presentation. "Delivered by a midwife, who pulled on the head." Partial paralysis of the left arm was noticed within the first 2 days. After several months, improvement began and continued for about 2 years, appearing first in the hand muscles and then extending upward. At operation in 1904, a lesion was found in the fifth nerve root and the outer part of the junction of the fifth and sixth nerve roots (upper trunk of the brachial plexus). The damaged portion was excised and the free ends sutured. The lesion resulted from a traction injury, with rupture of the perineural sheath and hemorrhage into its substance and into the meshes of the epineurium.
Schematic representation of a rupture of the perineural sheath and hemorrrhage into its substance and into the meshes of the epineurium, resulting in the formation of a hematoma. Legend: (a) epineurium, (b) perineurium, (c) ner...
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125