
Infectious Disorders
Creutzfeldt-Jakob disease
Dec. 27, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Brain abscess is an important complication of both systemic and pericranial infections (sinusitis, otitis, etc.), of cranial trauma, and of neurosurgical procedures. If diagnosed early in its course, the disorder is highly treatable–usually with antibiotics and surgery but at times with antibiotics alone. If misdiagnosed, however, it may cause severe neurologic injury or death. In this article, the author discusses the pathogenesis and clinical presentation of brain abscess and provides an approach to diagnosis and treatment of the disorder.
|
• Brain abscess most commonly arises by hematogenous spread. Less frequently, it may occur as a complication of sinusitis, otitis, mastoiditis, or penetrating trauma. Brain abscess may be caused by a single agent, but in a minority of cases, it may also be polymicrobial. | |
|
• The classic presentation of brain abscess is headache, fever, and focal neurologic signs. However, this triad is not present in most patients, and presentation is often that of a subacutely developing intracerebral mass lesion. | |
|
• Brain abscesses often have a thinner wall on the ventricular surface of the abscess allowing the abscess to expand medially. Rupture of the abscess into the ventricle may produce rapid clinical deterioration with high mortality. | |
|
• The diagnostic procedure of choice for brain abscess is contrast-enhanced MRI. CT scan with contrast, although useful, is less sensitive. | |
|
• Treatment of brain abscess, in the great majority of patients, consists of antibiotic therapy and surgical drainage. Until identification of the causative organism(s), initial antibiotic therapy should be directed against Staphylococcus aureus and other potential Gram-positive agents, Gram-negative agents, and anaerobes. | |
|
• Occasionally, small abscesses may respond to antibiotics alone. Patients being treated with antibiotics alone, however, need to be followed carefully by clinical examination and MRI to detect enlargement of the abscess in the face of antibiotic treatment. |
The notion that ear infections could progress to delirium and death, a series of clinical events consistent with brain abscess as well as subdural empyema or septic venous thrombophlebitis, was known to ancient writers, including Hippocrates (56). Morand, in the 16th century, is the first individual credited with successful drainage of a brain abscess. Methodical development of surgical approaches to brain abscess, however, did not begin until the latter part of the 19th century (16). Beginning at this same time, development of effective surgical treatment of chronic otitis, a major cause of purulent intracranial infections, caused a fall in the incidence of otogenic brain abscess long before the advent of antibiotics.
Prior to CT, diagnosis of brain abscess remained elusive, with treatment ultimately surgical; antibiotics were assigned an adjunctive, but not usually curative, role. Since the late 1970s, however, the introduction of CT and subsequently MRI has allowed rapid, noninvasive methods for diagnosing and monitoring brain abscess (33; 32; 45; 113; 13; 104). With the widespread use of these neuroimaging techniques, mortality from brain abscess has fallen, and it has become possible to treat a portion of brain abscesses with antibiotic therapy alone (79; 48; 104; 17), or to drain abscesses using stereotactic, CT-, or MR-guided needle aspiration (66; 74; 59; 46; 03; 104; 17; 30).
|
• Fever, headache, and focal neurologic signs represent the classical triad of symptoms associated with brain abscess. However, this triad is present in only a minority of patients with brain abscess. | |
|
• The most common presentation of brain abscess is that of a rapidly or subacutely developing intracranial lesion. | |
|
• Fewer than 50% of patients presenting with brain abscess will have fever. |
Fever, headache, and focal neurologic signs comprise the classical clinical triad of brain abscess. However, these three clinical features occur in only a minority of patients (64; 38; 56; 46; 15; 14; 17; 07). In most cases, brain abscess presents as a rapidly or subacutely developing space-occupying lesion, and fever or other signs of active infection may be absent (56; 46; 15; 14; 17). Approximately 75% of patients will present with symptoms of less than two weeks’ duration (38; 56; 46; 15; 14; 07). In occasional cases, however, clinical signs may develop so rapidly as to suggest cerebral infarction or acute meningitis, or they may evolve over weeks or even months to suggest the presence of an intracranial neoplasm (64; 96; 100). Headache occurs in 65% to 75% of patients, and nausea and vomiting in about 50% of cases (38; 56; 46; 15; 14; 17; 27; 07). Fever is present in less than 50% of patients and may be attributed to coexisting sinusitis, otitis, or systemic infection. Focal neurologic signs are present in less than 50% of patients and, even when present, may be extremely subtle (38; 56; 15; 14; 27). Approximately one third of patients present with seizures. These are most frequently generalized and are most closely associated with frontal or frontoparietal abscesses (21; 94; 20; 07) but can also occur with otogenic abscesses (27). Nuchal rigidity is present in about 25% of patients. In the current era, papilledema is present in no more than 25% of patients and is frequently absent in rapidly developing abscesses (38; 56). Ventricular rupture may be manifested by severe headache and developing signs of meningeal irritation, and rapid deterioration in clinical course (105; 46; 80).
|
• Overall mortality in brain abscess is roughly 12% to 20%. | |
|
• Mortality is heavily influenced by delay in diagnosis and by the neurologic status of the patient on presentation. |
Brouwer and colleagues performed a meta-analysis of 123 studies including 9699 patients reported between 1935 and 2012, and they recorded a 20% mortality rate in brain abscess (14). In one study, mortality was 6% at the time of discharge and 12% after six months (07). Survival in brain abscess approaches 100% in patients who are fully alert at presentation and remains over 90% in patients who are stuporous but not comatose when first seen (77; 38; 46). However, only 41% of patients responsive to pain will survive, and survival has remained unchanged over the past three decades (11% to 18%; 82% to 89% mortality) in patients who are without pain response (77; 46). Adverse prognostic factors include delay in diagnosis; choice of inappropriate antibiotics; inadequate aspiration or drainage; multiple, large, deep, or multiloculated abscesses; posterior fossa abscesses; and intraventricular rupture (21; 56; 46; 15; 14). Severity of residual neurologic defects is heavily influenced by neurologic status at the time of admission and may also be better in cases successfully treated with antibiotics alone or with antibiotics plus aspiration (38; 03; 27). Both morbidity and mortality are higher with Gram-negative than with Gram-positive infections (85; 111). Neurologic deficits will be found in 30% to 55% of patients surviving brain abscess and are incapacitating in 17% (56): these may be secondary to the abscess itself or to complications of surgical intervention. Although residual long-term cognitive impairment will be present in 22% of surviving patients at 1 year, 45% of patients will have been able to return to work (93). Incidence of seizures in different series has ranged from 11% to 35% of patients and usually occurs within 12 months after surgery (60; 92; 56; 07; 08).
A 52-year-old diabetic female was in her usual state of health until six weeks prior to admission, when she had a 3-week episode of apparent “flu” characterized by fatigue, aching joints, nausea, vomiting, and headache. She recovered briefly, but then had recurrence of headaches. Two weeks prior to admission the patient became confused and was hospitalized. On admission she was found to be febrile to 104.6°F and significantly dehydrated. Hematocrit was normal. White blood count was 15,000, with 94% polymorphonuclear leukocytes. Blood sugar was 230 mg/dl, but ketones were absent. CT scan without contrast was normal. Lumbar puncture was unsuccessful, and the patient was empirically treated with cefotaxime and ofloxacin. Lumbar puncture three days later showed 75 white blood cells, with 48% neutrophils, protein of 111 mg/dL, and glucose of 105 with serum glucose over 330 mg/dl. Subsequent lumbar puncture was reported to show a decrease in numbers of white blood cells. The patient improved clinically and was discharged on oral ampicillin. The patient did well initially at home but then developed episodes of disorientation. On the morning of admission, she was found vomiting, incontinent of stool, and unresponsive to voice. Hospital evaluation revealed the patient to be afebrile, with white blood count of 7500. Head CT scan showed a possible brain abscess, with several patchy areas of edema.
The patient was transferred for further care.
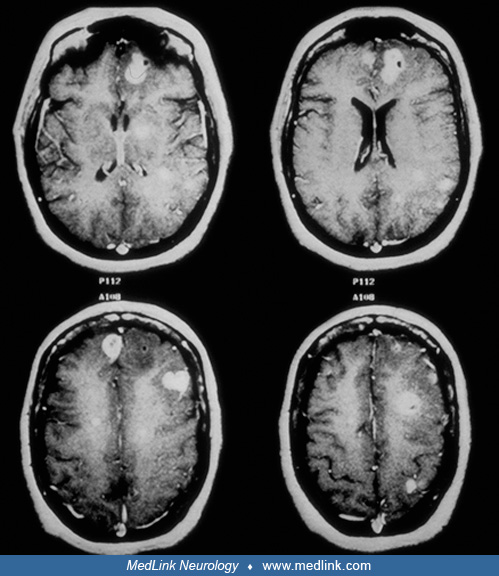
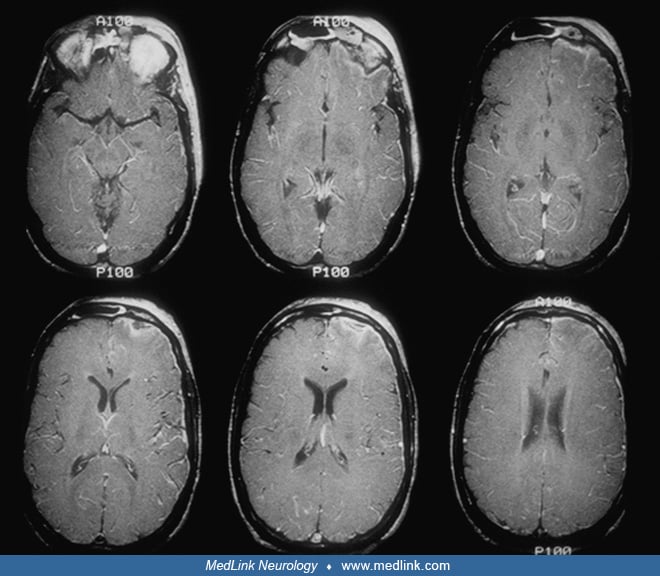
On examination, the patient was normotensive and afebrile. General physical examination was normal except for early bilateral papilledema. On neurologic examination, the patient was obtunded. She was able to move all four extremities spontaneously and in response to pain but was unresponsive to voice. Reflexes were hypoactive throughout and absent at the ankles. Babinski sign was absent on the left but present on the right. Head MRI showed in excess of 10 ring-enhancing and solid lesions scattered throughout both cerebral hemispheres, with surrounding edema.
The patient was placed on intravenous ceftriaxone, 2 grams every 12 hours, metronidazole given as a 1 gram loading dose followed by 500 mg every 6 hours, and intravenous oxacillin at 2 grams every 4 hours. The patient stabilized and then regained consciousness, with slowed but otherwise intact mental status, mild right arm drift, and right Babinski sign; neurologic examination was otherwise intact except for distal decrease in light touch and pinprick sensation, consistent with a diabetic peripheral neuropathy. CT-guided stereotactic biopsy failed to yield organisms. The patient was maintained on all three antibiotics and followed with serial MRI scans to rule out enlargement of any of the lesions despite antibiotic therapy; scans were obtained at 48-hour intervals during the first week of therapy and then at progressively longer intervals as the patient improved.
After discharge from hospital, one month after admission, the patient was maintained on intravenous ceftriaxone and placed on oral metronidazole and oral dicloxacillin plus probenecid to increase serum concentrations and reduce active transport of the drug from cerebrospinal fluid. With antibiotic treatment, the patient’s lesions steadily diminished in size, with complete disappearance of most of the lesions.
Metronidazole was discontinued after eight weeks of therapy; ceftriaxone was discontinued after 12 weeks of therapy, and dicloxacillin was discontinued one week later. An MRI scan was obtained one week following discontinuation of each antibiotic to rule out recurrence of an abscess in any of the areas of residual abnormality, with a follow-up MRI one month after the last medication had been discontinued. The patient continued to improve mentally and was discharged to her private physician. On follow-up four years later, the patient was neurologically normal except for her diabetic peripheral neuropathy. An MRI scan revealed areas of gliosis at the sites of some of the previous abscesses, but no other abnormality.
The causative agents of brain abscess vary according to the age and immunological status of the patient. In adults, aerobic, microaerophilic, and anaerobic streptococci, in particular agents of the Streptococcus milleri group (Streptococcus anginosus and Streptococcus intermedius), are found in 60% to 70% of cases and are common in abscesses arising from sinusitis or dental infections (24; 56; 15; 14; 07). Bacteroides species and enteric bacteria, including Escherichia coli, Proteus species, and Pseudomonas species, have been reported in 20% to 40% of cases (24; 56; 15; 14; 88; 07). Staphylococcus aureus has been reported in 10% to 27% of cases and is the most common isolate from brain abscesses associated with penetrating trauma or neurosurgical procedures (56; 23). In a series by Corsini Campioli and colleagues, methicillin-resistant Staphylococcus aureus is of increasing concern as an etiologic organism (73; 99). Multiple organisms have been documented by culture methods in approximately 18% of cases and are most frequent in brain abscesses associated with sinusitis or otitis (92; 56; 07; 29). However, this number may be falsely low. Studies employing 16S rRNA-based amplification, cloning, and high-throughput sequencing suggest that agents in brain abscess are polymicrobial in up to 65% of cases, with frequent presence of at least one anaerobic bacterium (69; 29). Staphylococcus aureus, however, may be present as a single organism in cases associated with trauma or endocarditis (38). Isolates in brain abscesses arising from oral infection have more commonly included S. viridans (in particular S. anginosus), as well as Actinomyces, Peptostreptococcus, Prevotella, Fusobacterium, Aggregatibacter actinomycetemcomitans, and Eikenella corrodens (70). Other, less frequently isolated organisms, in addition to Fusobacterium and Actinomyces species, may include members of the Clostridium species (38; 71). Listeria monocytogenes, although usually associated with meningitis, may rarely cause brain abscesses in immunocompetent as well as immunosuppressed individuals (110). The fungus, Cladophialophora bantiana, has been associated with cases of brain abscess, with most cases occurring in Asia (18). In approximately 25% of cases, no organism is detected (92; 56).
Brain abscess in neonates is frequently a complication of meningitis. In this setting, Gram-negative organisms are, thus, the most frequent isolates and include Proteus mirabilis, Escherichia coli, Serratia marcescens, and Citrobacter species, especially Citrobacter diversus (37; 91; 34; 15; 14). In children, brain abscess may be associated with Fusobacterium species, in particular Fusobacterium necrophorum, an organism also associated with cerebral vein thrombosis and internal jugular vein thrombosis (Lemierre syndrome) (98).
Isolates from brain abscesses in immunocompromised patients may differ from those recovered from abscesses in immunologically intact individuals. Enterobacteriaceae and Pseudomonas aeruginosa may be associated with brain abscess in immunosuppressed children and adults, as may Listeria monocytogenes (12; 28). Fungi including Cryptococcus neoformans, Candida, Mucor, and Aspergillus species may be associated with brain abscess in diabetics and other immunocompromised patients, as well as in patients abusing intravenous drugs (56). Although most commonly isolated from immunocompromised patients, Nocardia asteroides may cause brain abscess in patients without known impairment of immune function (23). Other Nocardia species may also be associated with brain abscess, including Nocardia farcinica, Nocardia wallacei, and Nocardia cyriacigeorgica (23); brain abscess due to Nocardia cyriacigeorgica has been reported in patients with multiple myeloma treated with bortezomib and other agents (83). The most common cause of focal intracranial infection in patients with AIDS is Toxoplasma gondii, followed by Cryptococcus neoformans and Mycobacterium tuberculosis (86; 68). Although M. avium intracellulare (MAI) is a frequent cause of systemic infection in patients with advanced AIDS, brain abscess due to MAI is infrequent (55).
Brain abscesses may be single or multiple. Each abscess begins as a microscopic focus of septic, microvascular injury, usually within white matter or at the gray-white junction. Growth of bacteria within this focus produces a localized encephalitis or "cerebritis," which undergoes liquefaction (11; 33; 84; 15). The developing abscess elicits an inflammatory response of lymphocytes and polymorphonuclear leukocytes, with localized, frequently intense cerebral edema. Over time, an abscess capsule forms, consisting of both fibrotic and gliotic elements. The abscess capsule tends to be thickest on its cortical surface and thinnest medially, causing the abscess to expand toward and rupture into the ventricular system (56). Death in brain abscess may result from tonsillar herniation, caused by the mass effect of the abscess and its surrounding cerebral edema, or from rupture of the abscess into the ventricular system.
Historically, brain abscesses have most frequently arisen following hematogenous dissemination of organisms from distant sites of infection. The most common associated systemic infections are chronic lung infections, in particular bronchiectasis and lung abscess, and acute bacterial endocarditis (42; 04; 56; 87). Brain abscess is particularly likely in conditions in which a right-to-left cardiac shunt allows organisms to move directly from the venous circulation into left-sided systemic circulation. For this reason, children with cyanotic congenital heart disease are at particular risk for hematogenous brain abscess (22; 82), as are patients with hereditary hemorrhagic telangiectasia (25; 104; 114). Rarely, brain abscess may also complicate pulmonary arteriovenous fistulae not associated with hereditary hemorrhagic telangiectasia or in the setting of a patent foramen ovale (58; 104).
Less frequently, brain abscesses result from spread of organisms through emissary veins during sinusitis, otitis, or mastoiditis (04), although Bodilsen and colleagues reported a strong association between brain abscess and oropharyngeal bacterial (07). Historically, otitis represented the major pericranial infection associated with brain abscess; at present, however, brain abscess is more frequently associated with frontal, ethmoidal, and sphenoidal sinusitis (56), and the most common site of brain abscess is the frontal lobe (92). Less frequent causes of brain abscess include penetrating trauma, neurosurgical procedures, facial infections, and dental sepsis (56; 116). A single case report lists brain abscess as a complication of tongue piercing (47). Brain abscesses of hematogenous origin are most common in the distribution of the middle cerebral artery, followed by those of the anterior cerebral artery and posterior circulation (56). Abscesses arising from frontal and ethmoidal sinusitis are most commonly located within the frontal lobe (04). Sphenoid sinusitis may cause frontal or temporal lobe abscesses. Infections of the middle ear or mastoid may spread through emissary veins into the middle fossa to cause temporal lobe abscesses or into the posterior fossa to cause cerebellar abscess (04; 56).
|
• Brain abscess may occur at any age, but in most studies, they have been most common in the third decade of life. | |
|
• Brain abscesses are uncommon and are usually associated with sinusitis, otitis, mastoiditis, head trauma, or meningitis. | |
|
• An increased incidence of brain abscess following sinusitis or otitis in the setting of COVID-19 infection has been reported by some authors. | |
|
• Brain abscess in children with cyanotic congenital heart disease – once a common cause of brain abscess – is now unusual. |
Brain abscess occurs worldwide with an incidence of approximately four per million population and accounts for approximately one in 10,000 hospitalizations (56), with an annual incidence of 0.8 to 1.0 cases per 100,000 adults (07). In most series, males are affected more frequently than females (21; 56; 15; 14; 104; 07). Historically, brain abscess has been most common in the third decade of life but may occur at any age (92; 56), and one study reported a median age of 59 years (07). Abscesses due to paranasal infections are most common between the ages of 10 and 30 years. Otogenic abscesses are most common in childhood and after 40 years of age. Brain abscess in children is uncommon and has a peak incidence between 4 and 7 years of age (97). Predisposing factors, in particular sinusitis, otitis, mastoiditis, head trauma, or meningitis, are present in up to 81% of affected children (97). An apparent increased incidence of brain abscess following COVID-19 infection has been reported (51). In the past, roughly 25% of children with brain abscess had cyanotic congenital heart disease. At present, however, this association is unusual (34; 97).
Risk of brain abscess is significantly increased by the presence of any of several underlying host pathologies.
Rapidly developing brain abscess may mimic bacterial or aseptic meningitis, epidural abscess, or subdural empyema (56). The clinical presentation of temporal lobe abscesses may resemble that of herpes simplex virus encephalitis (115). More slowly developing abscesses may be mistaken for primary or metastatic tumors (56; 109; 15; 14). Brain abscesses presenting with abrupt change in patient condition may occasionally be mistaken for evolving cerebral or brainstem infarction, brain hemorrhage, subarachnoid hemorrhage, or, rarely, tumefactive multiple sclerosis (01). Diagnosis may be difficult in the patient who presents with an essentially encephalopathic picture, without fever and without focal neurologic signs.
|
• Major risk factors for developing brain abscess include sinusitis or otitis, especially if associated with intracranial epidural abscess or subdural empyema. | |
|
• Additional important systemic risk factors include cyanotic congenital heart disease with right-to-left shunt, hereditary hemorrhagic telangiectasia, infective endocarditis, chronic, pyogenic lung abscess, and AIDS. |
Major risk factors for development of brain abscess are sinusitis or otitis, in particular if these conditions are complicated by epidural abscess or subdural empyema (56; 104; 27). Risk factors associated with brain abscesses of hematogenous origin include cyanotic congenital heart disease with right-to-left shunt; hereditary hemorrhagic telangiectasia; acute infective endocarditis, at times in the setting of intravenous drug abuse; chronic, pyogenic lung abscess; and AIDS and other conditions of impaired host immune response (38; 56; 41; 25; 15; 14; 10; 104; 05; 07; 114). Brain abscess in hereditary hemorrhagic telangiectasia is particularly associated with patients harboring mutations in the ENG gene (HHT1) (10). In a few instances, hematogenous brain abscess has been associated with patent foramen ovale (57; 19). Rarely, brain abscess may develop within an intraparenchymal hemorrhage or cerebral infarct with hemorrhagic transformation (101; 62).
Brain abscess should be considered in any patient presenting with recent onset of severe headache, including patients without fever or leukocytosis, or with symptoms or signs of a rapidly developing space-occupying intracranial process. Brain abscess should also be kept in mind in the patient with new onset of focal or generalized seizures. A history of systemic infection, sinusitis, otitis, carious teeth, drug abuse, or risk factors for AIDS should increase diagnostic concern (38; 07). Fever is present in less than 50% of patients; even when present, it may be 38°C or less (56; 15; 14; 104; 27). The peripheral white blood cell count is normal in 40% of patients and is elevated above 20,000 cells/mm3 in less than 10% of patients (56). The erythrocyte sedimentation rate is usually minimally elevated but may be normal (56). C-reactive protein levels are frequently elevated and do not correlate with the erythrocyte sedimentation rate (96). Kamra and colleagues have reported three patients in whom unsuspected brain abscess with intraventricular rupture presented as meningitis poorly responsive to antibiotic treatment (54).
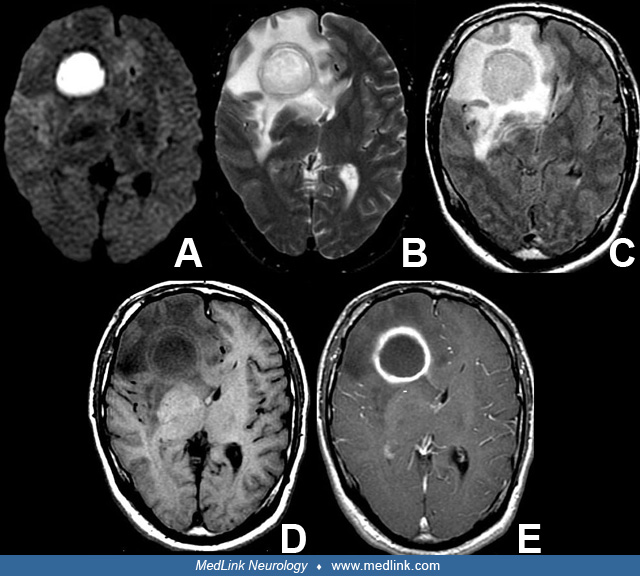
MRI with use of gadolinium enhancement is the diagnostic procedure of choice in suspected brain abscess (103; 32; 15; 14; 88; 104; 27; 102). Diffusion-weighted (DWI) or susceptibility-weighted (SWI) MRI or MR spectroscopy may allow differentiation between brain abscess and tumor with central necrosis (90; 36; 02) and may also help differentiate between bacterial, tuberculous, and fungal abscesses (53; 65; 76). Typically, brain abscesses will show increased signal on diffusion-weighted images and corresponding hypodensity on apparent diffusion coefficient (ADC) images (15). Diffusion tensor imaging may also provide a useful adjunctive MRI sequence to differentiate between abscesses and glial or metastatic tumors (108; 76). Limited data also suggest that MRI with diffusion-weighted images may be of value in identifying and following ventricular rupture of abscesses (89; 31). One study has reported that apparent diffusion coefficient may allow differentiation of culture-positive and culture-negative abscesses (107). Contrast-enhanced CT may fail to detect lesions easily discernible on MRI but should be used if MRI is not available (103). The sensitivity of contrast-enhanced CT may be increased if the scan is repeated 30 to 60 minutes after contrast infusion (11; 33). Both MRI and CT will delineate the amount of edema surrounding the abscess and may also document the presence of accompanying sinusitis or otitis. Ultrasound has been used by some practitioners to allow real-time localization of the abscess at the time of aspiration (103; 35).
Midazolam HCl (Versed), titrated in 0.5 mg increments to the desired level of sedation, (usually less than 5 mg total dose), may be required to prevent motion artifact in delirious or agitated patients. Careful physician monitoring of respiratory and neurologic status is essential if sedation is employed. Lumbar puncture is relatively contraindicated in brain abscess: spinal fluid abnormalities are usually nonspecific. In earlier reports, the procedure itself was accompanied by a 10% to 18% risk of brain herniation and death (21), although this risk may have fallen with more modern diagnostic methods. In their 2023 report, Bodilsen and colleagues identified only one case of transtentorial herniation among 118 patients with brain abscess undergoing the procedure (07). The patient should be evaluated for remote sources of infection with appropriate cultures of blood and other fluids such as sputum, pus from sinuses, or material obtained at myringotomy. Next generation (metagenomic) sequencing holds promise as a rapid and sensitive method of detecting etiologic organisms in brain abscess, including in patients with polymicrobial abscesses (49; 44; 117). However, the technique is not immediately available in all hospital laboratories, and its overall role in diagnosis compared to more traditional methods has not been established.
Therapy of brain abscess involves prompt administration of appropriate antibiotics, surgical drainage or removal where indicated, and control of cerebral edema. No controlled trials comparing antibiotic regimens in brain abscess exist (50). However, antibiotics used for brain abscess fall into four major groups (Table 1).
|
Suspected Organism |
Recommended Antibiotic |
|
Streptococci and other Gram-positive organisms excluding S aureus |
Penicillin, vancomycin, ceftriaxone, or cefotaxime |
|
Staphylococcus aureus |
• Vancomycin, until sensitivity to Oxacillin or Nafcillin is confirmed • Oxacillin or Nafcillin (Oxacillin is less apt to produce thrombophlebitis at the infusion site) • Use vancomycin if patient is allergic to penicillin |
|
Gram-negative organisms excluding Pseudomonas aeruginosa |
Ceftriaxone or cefotaxime |
|
Pseudomonas aeruginosa |
Ceftazidime |
|
Bacteroides species |
Metronidazole |
Many abscesses contain a mixed culture of organisms, requiring two or more agents (69). Although many workers will initially use a third-generation cephalosporin alone (15; 14), or use a third generation cephalosporin plus metronidazole (06), initial therapy, where the source of infection is unknown, should consider the combined use of vancomycin, plus ceftriaxone, plus metronidazole (63; 50; 61; 104; 23). Vancomycin should be used until nafcillin or oxacillin resistance sensitivity is confirmed, in particular in abscesses arising after neurosurgical procedures or head trauma. Vancomycin should also be used in patients known to be allergic to penicillin. Successful antibiotic therapy of brain abscess with ceftriaxone and metronidazole alone has been reported (52), and a report suggests that treatment with carbapenems may result in lower mortality than treatment with ceftriaxone and metronidazole (67). In this study, meropenem was significantly less likely to be associated with seizures than was imipenem. Cefuroxime has been used to treat surgically drained abscesses caused by S aureus (78), and linezolid has been used to treat abscesses caused by methicillin-resistant Staphylococcus aureus (MRSA) and by Peptostreptococcus (95; 73). However, the efficacy of these regimens have not been established where there is possibility of cure by antibiotic therapy alone, and Norgaard and colleagues (78) did not encounter methicillin-resistant strains of S aureus. Ceftazidime should be used in place of ceftriaxone if Pseudomonas aeruginosa is strongly suspected (56). Intracranial mass lesions in patients with AIDS should be treated initially as being due to Toxoplasma gondii, with sulfadiazine and pyrimethamine (86). The antibiotic regimen used in a given patient may need to be revised as data become available from cultured abscess material. Length of therapy is determined by patient course and follow-up MRI or CT. In general, antibiotics should be continued for at least eight weeks if surgery is not undertaken, or at least four weeks if the abscess is drained or excised. Early transition to oral antibiotic therapy has been used with success in some cases. The overall efficacy of early transition to oral therapy has not been determined, however, and is being explored in an ongoing controlled clinical trial (09).
Surgical therapy of brain abscess may involve aspiration or excision (81; 43; 46; 30). Aspiration, particularly under stereotactic CT or MRI guidance, is becoming increasingly favored because it is less traumatic to the central nervous system than is excision and carries a lower risk of subsequent seizures (66; 74; 50; 59; 112; 30). Aspiration also provides a less traumatic approach to abscesses involving an eloquent area of the brain or the brainstem (39). Aspiration removes the purulent center of the abscess, rendering the abscess more amenable to antibiotic therapy, and often effectively reduces intracranial pressure. Recurrence of the abscess may require repeat aspiration. However, no controlled trial of aspiration versus excision has been reported, and excision should be considered in large or multiloculated abscesses, abscesses that do not respond to aspiration and may be necessary in cases in which ventricular rupture is considered imminent (38). Excision is also indicated in cases in which there is a foreign body, in which there is gas within the abscess, or in abscesses due to Nocardia (38). Cerebellar abscesses may cause obstructive hydrocephalus and may, hence, require placement of a ventricular shunt to avoid further increase in intracranial pressure (72). Although many neurosurgeons have instilled antibiotics directly into the abscess cavity, the efficacy of this procedure is not known.
Brain abscess with intraventricular rupture has a fatality rate that may reach 80%. However, in one case following intraventricular treatment with vancomycin, survival has been reported following open craniotomy with debridement of abscess cavity and ventricular lavage, followed by six weeks of intravenous antibiotics, intraventricular gentamicin twice daily for six weeks, and intraventricular drainage for six weeks (118) and in a subsequent case occurring in a patient with brain abscess in the setting of hereditary hemorrhagic telangiectasia (75). Limited reports suggest that survival following ventricular rupture may be improved by neuroendoscopic ventricular irrigation (100% survival) versus use of a ventricular drain (37.5% survival) (106; 26).
The availability of CT and MRI imaging has made it possible, in selected cases, to treat brain abscesses with antibiotics alone (79; 81; 66; 40; 48). Abscesses at the stage of cerebritis do not contain material that can be drained. In many cases, surgery may be deferred if the abscess is less than 2.5 cm in diameter and if the patient is neurologically stable. This recommendation is not based on controlled trials, however, and abscesses treated with antibiotics alone must be followed with great care, and a follow-up MRI or CT should be obtained within 24 to 48 hours after initiation of therapy. It is extremely important to remember that abscesses may enlarge despite antibiotic therapy (66). For this reason, frequent follow-up MRI or CT is essential if a decision is made to treat with antibiotics alone. Intervals between subsequent CT and MRI studies are determined in part by the patient's neurologic status but should not be greater than 3 to 5 days in the first two weeks. MRI and CT may remain abnormal for many weeks despite apparent clinical recovery (56; 61).
Several additional therapeutic issues must be faced in the patient with brain abscess (56; 07). Cerebral edema may require emergent treatment with hyperventilation, mannitol, or dexamethasone (06). Hyperventilation is used short-term to a pCO2 of less than 28 torr. Mannitol may be given as a 20% solution with an initial dose of 0.5 to 1.0 g/kg over 10 minutes followed by 0.25 to 0.5 g/kg every 3 to 5 hours. The patient should be catheterized before mannitol is begun, and careful attention should be given to serum electrolytes and osmolality. Dexamethasone is effective in reducing vasogenic edema, and a short course of 10 mg intravenously initially followed by 4 mg intravenously every 4 to 6 hours should be considered where control of intracranial pressure is of major concern over time. Use of a transcranial or intraventricular pressure monitor may be invaluable in guiding therapy. Inappropriate secretion of antidiuretic hormone or development of diabetes insipidus may require strict attention to fluid and electrolyte balance. Administration of 5% dextrose in water, without other electrolytes, may lead to profound hyponatremia. Subcutaneous heparin should be considered in patients remaining at bed rest for extended periods of time. Adjacent or remote sources of infection, including sinuses, middle ear, mastoid, and teeth may also require antibiotic or surgical therapy. Seizures may develop over time in up to 27% of patients (08). Adjacent or remote sources of infection, including sinuses, middle ear, mastoid, and teeth may also require antibiotic or surgical therapy. Seizures may be treated with intravenous diazepam, 10 mg, or lorazepam, 4 mg, given over two minutes and repeated after 15 minutes if seizures persist. Therapy with these short-acting agents should be followed by a loading dose of intravenous fosphenytoin given as the equivalent of 10 to 15 mg/kg phenytoin in normal saline at a rate no faster than 50 mg/min (1 mg/kg per minute in neonates). If phenytoin is used rather than fosphenytoin, the electrocardiogram and blood pressure should be monitored during administration. Alternate agents to control seizures include intravenous levetiracetam or valproic acid. It should be noted, however, that there are no comparative data as to the efficacy of these three agents in achieving seizure control. Maintenance therapy with phenytoin or other longer-term anticonvulsants should be continued once seizures are controlled. Midazolam, propofol, phenobarbital, or other agents may be required to control seizures unresponsive to phenytoin or levetiracetam. Onset of seizures that may occur weeks to months after recovery may require late initiation of therapy with phenytoin or other agents. Careful withdrawal of anticonvulsants should be considered after two years in those patients who have seizures early in their course but remain seizure-free and without focal neurologic deficits or electroencephalographic abnormalities.
The likelihood of subsequent seizures may be reduced by early therapy with anticonvulsant medication.
Incidence, clinical symptomatology, and treatment of abscess in pregnancy do not differ from that seen in nonpregnant individuals.
Brain abscess is not a contraindication to the use of anesthesia. Many patients with brain abscess will have significantly elevated intracranial pressure. Caution must be used in such patients if anesthetic agents such as halothane, methoxyflurane, or ketamine are used. These agents cause intracranial vasodilatation and, thus, may further increase intracranial pressure and the risk of herniation.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

John E Greenlee MD
Dr. Greenlee of the University of Utah School of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Infectious Disorders
Dec. 27, 2024
Infectious Disorders
Dec. 12, 2024
Infectious Disorders
Dec. 10, 2024
Infectious Disorders
Dec. 10, 2024
Peripheral Neuropathies
Nov. 16, 2024
Infectious Disorders
Nov. 15, 2024
Infectious Disorders
Nov. 12, 2024
Infectious Disorders
Nov. 12, 2024