



Stroke & Vascular Disorders
Neoplastic and infectious aneurysms
Dec. 29, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Carotid-cavernous fistulas are abnormal communications between the cavernous sinus and the internal carotid artery, external carotid artery, their branches, or both. There are two broad categories of carotid-cavernous fistulas—direct and indirect—each with a different clinical presentation. In this article, the author discusses the clinical presentation, pathogenesis, and methods of diagnosis for this condition. This article provides an in-depth review of the current treatments for carotid-cavernous sinus fistulas, including endovascular repair via transarterial or transvenous embolization.
|
• Carotid-cavernous sinus fistulas are abnormal connections between the cavernous sinus and the carotid arterial system. | |
|
• The clinical manifestation of carotid-cavernous sinus fistulas reflects the vascular and neurologic structures of the cavernous sinus involved. | |
|
• The cavernous sinus communicates with the internal carotid artery in “direct” fistulas, and with branches of the internal carotid, the external carotid, or both arteries in “indirect” fistulas. | |
|
• “Direct” fistulas are typically caused by head trauma or a ruptured cavernous carotid aneurysm. Their presentation is dramatic, with proptosis, ophthalmoplegia, and vision loss. | |
|
• “Indirect” or “dural” fistulas present more subtly in hypertensive elderly women. | |
|
• Although there is no randomized controlled study of treatments, most carotid-cavernous sinus fistulas can be closed successfully by endovascular intervention. | |
|
• Surgery and radiotherapy are used in failures of endovascular therapy. |
Carotid-cavernous fistulas are abnormal communications between the cavernous sinus and the carotid arterial system: the internal carotid artery, external carotid artery, and its meningeal branches. Carotid-cavernous fistulas are direct or indirect. In “direct” or “high-flow” fistulas, the internal carotid artery communicates directly with the cavernous sinus. The “indirect” or “dural” carotid-cavernous fistula connects the branches of the internal or external carotid artery and the cavernous sinus. There are four types of carotid-cavernous fistulas (07). Type A is a direct fistula between the cavernous internal carotid artery and the cavernous sinus. It is mostly caused by a traumatic tear in the arterial wall or a rupture of a cavernous carotid aneurysm.
Type B fistulas connect the meningeal branches of the internal carotid artery and the cavernous sinus. Type C fistulas occur between the meningeal branches of the external carotid artery and the cavernous sinus. In type D, the shunt is between the meningeal branches of the internal and external carotid artery and the cavernous sinus.
Thus, the traditional “direct” fistula is equivalent to type A carotid-cavernous fistula, whereas “indirect” (or “dural”) fistulas encompass Types B, C, and D. This classification gives the treating physician a more precise anatomical guide for treatment.
|
• Direct fistulas present dramatically due to high blood flow and are seen in younger patients. | |
|
• Indirect fistulas present more insidiously and occur more in elderly patients. | |
|
• The most common symptom of carotid-cavernous sinus fistulas is orbital bruit. | |
|
• Headache, vision loss, and limited eye motion suggest cavernous sinus involvement. | |
|
• Anterior drainage of carotid-cavernous sinus fistulas causes ocular congestion, whereas posterior drainage results in a “white-eyed shunt.” | |
|
• The third cranial nerve is the most affected cranial nerve. | |
|
• A nosebleed resulting from a fistula may be life threatening. |
The clinical manifestations of a carotid-cavernous fistula are determined by the structures within the cavernous sinus affected. Therefore, the presentation may include palsies of the cranial nerves III, IV, V1, V2, or VI. Anterograde venous flow may cause orbital and ocular venous congestion, manifested as proptosis, chemosis, arterialized venous loops on the sclera, increased intraocular pressure, glaucomatous vision loss, and limited eye movement. One distinguishing feature of direct and indirect carotid-cavernous sinus fistulas is the presence of orbital bruit on auscultation.
Direct carotid-cavernous sinus fistulas present dramatically due to high blood volume flow.
Although carotid-cavernous sinus fistulas occur most commonly on the side of head trauma, the contralateral side may also be affected (29). In a series of 98 consecutive patients with direct fistulas, the most common symptom was a prominent orbital bruit (80%), followed by proptosis (72%), and chemosis (55%). Isolated ipsilateral abducens palsy occurred in 49%, retro-orbital pain or headaches in 24%, ophthalmoplegia in 23%, and vision loss in 17% (53).
Intracranial hemorrhage may develop in 5% of patients with direct carotid-cavernous fistula. About 2% of these hemorrhages can present with life-threatening nosebleeds (96).
A rare presentation of direct carotid-cavernous sinus fistulas is brainstem venous congestion, resulting in reduced consciousness, facial numbness, dysarthria, and gait ataxia (14). Unilateral limb weakness was observed in a patient with contralateral basal ganglia congestion (31).
By contrast, indirect (“dural”) carotid-cavernous fistulas present more insidiously due to the smaller volume of shunted blood. These patients are typically middle-aged or elderly women.
Indirect carotid-cavernous fistulas, draining posteriorly into the petrosal sinuses, lack proptosis or the orbital bruit. The absence of conjunctival congestion gives the indirect carotid-cavernous fistula the nickname “white-eyed shunt” (01). These fistulas are often asymptomatic. A sudden presentation of isolated ocular motor nerve palsy, almost always associated with ocular or orbital pain, was described. The third nerve is the most often involved cranial nerve, and pupil involvement may be complete, incomplete, or absent. Cerebral angiography can distinguish it from a cerebral aneurysm or microvascular palsy.
Anterior-draining indirect fistulas usually produce orbital and visual symptoms resembling direct carotid-cavernous fistulas. These manifest as conjunctival congestion, proptosis, chemosis, ocular motor paresis, and orbital pain. Close inspection reveals the characteristic radial pattern of arterialization that distinguishes it from chronic conjunctivitis.
Increased intraocular pressure, retinal vessel occlusion, ischemic optic neuropathy, or proliferative retinopathy lead to tractional retinal detachment and vision loss in 30% of patients (64). Increased intraocular pressure can also follow angle closure from massive choroidal effusion (92). However, anteriorly draining indirect carotid-cavernous fistulas may present without ocular or orbital signs. One patient presented only with headache and isolated abducens nerve palsy. The anastomosis between the superior ophthalmic vein and angular facial vein prevented pressure buildup and the typical ocular or orbital signs (42).
Another distinguishing feature of indirect carotid-cavernous fistula is the waxing and waning nature with spontaneous improvement or closure in up to 60% of patients (83). Spontaneous closure may occur even in those with florid clinical symptoms such as optic neuropathy and orbital congestion (13). Thrombosis of the fistula may contribute to this improvement. Recurrence or change in clinical symptoms may occur if the thrombus dissolves or migrates.
A retrospective study of 47 patients with cavernous-carotid fistulas (26 indirect, 21 direct) revealed a similar presentation of both groups with headache and ocular manifestations like proptosis, conjunctival injection, ophthalmoparesis, chemosis, and visual acuity loss. Direct cavernous-carotid fistulas occurred more often in younger patients than indirect fistulas (48 vs. 62 years). Vision loss on presentation was three times more likely to result in residual symptoms, independent of the classification (33).
The overall prognosis of a carotid-cavernous fistula is good, with over 80% experiencing complete cure after endovascular treatment (28).
Indirect carotid-cavernous sinus fistulas may have a fatal outcome if intracerebral hemorrhage occurs with a rate of approximately 1.8% per year (22). Up to 60% of indirect carotid-cavernous fistulas close spontaneously or after diagnostic angiography alone (83; 15). Close observation, while the ocular symptoms are mild and the neurologic symptoms are absent, is reasonable. Elevated intraocular pressure may respond to medical management alone. In one series of 14 eyes, nine had elevated intraocular pressure, of which only three were difficult to control, and one of these eyes required glaucoma surgery (43). The indications for carotid-cavernous sinus fistula closure are refractory intraocular hypertension, intractable exposure keratopathy from proptosis, unacceptable diplopia, or intracerebral hemorrhage.
Direct carotid-cavernous sinus fistulas have higher morbidity and mortality compared to indirect ones. Out of 127 patients with direct carotid-cavernous sinus fistulas, 3.9% died, whereas no one died from indirect carotid-cavernous sinus fistulas. Additionally, the rates of intracerebral or subarachnoid hemorrhage (3.1% vs. 0%), life-threatening epistaxis (3.1% vs. 0%), and increased intracranial pressure (8.7% vs. 3.6%) were much higher for direct versus indirect carotid-cavernous fistulas. Subarachnoid hemorrhage from a direct fistula portends a grim prognosis, with all four of these patients dying quickly (35).
History. A 47-year-old man was hit by a car several months before evaluation. Since the accident, he had developed swelling and redness in the left eye. The eye hurt when exposed to light.
Physical examination. The physical examination revealed visual acuity of 20/40 bilaterally. He had proptosis and periorbital swelling of the left eye and a thrill detected by auscultation present over the left eye. The intraocular pressure was 8 and 16 mmHg in the right and left eye, respectively.
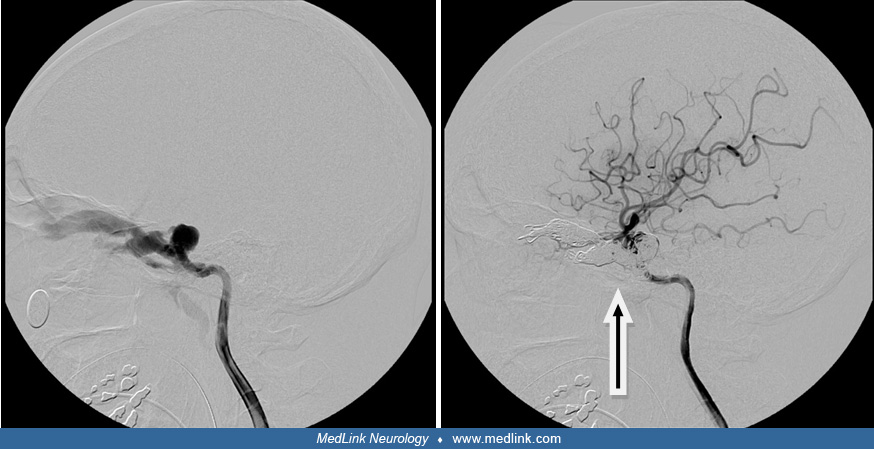
Diagnostic tests. A catheter angiogram revealed a direct carotid-cavernous sinus fistula in the left proximal posterior genu and cavernous sinus. There was significant dilatation of the superior ophthalmic vein. There was so much shunting that there was little to no filling in the left hemispheric arteries. Type A carotid-cavernous sinus fistulas were diagnosed.
Treatment. The fistula was treated with a microcatheter guided up the internal carotid artery and through the rent in the carotid to the superior ophthalmic vein. Multiple coils were placed in the superior ophthalmic vein. As the coils filled the superior ophthalmic vein, shunting decreased and the arteries of the left hemisphere became visible. Once the ophthalmic vein was coiled, a stent was placed in the internal carotid artery over the rent to prevent coils from falling back into the parent vessel. Additional coils were then placed to occlude the cavernous sinus.
Outcome. The patient’s pain proptosis and chemosis significantly improved after the procedure. He had no restriction of extraocular movements, and the diplopia resolved.
|
• Direct carotid-cavernous sinus fistulas occur after caused by trauma, invasive procedures, or weakened blood vessel walls. | |
|
• Indirect carotid-cavernous sinus fistulas are associated with cerebrovascular risk factors like hypertension, atherosclerosis, and thrombosis. |
Most direct carotid-cavernous sinus fistulas are posttraumatic. Cranial fractures or shearing forces during acceleration or deceleration cause arterial wall tearing (78). When the cranial fracture is absent, arterial damage may be caused by sudden neck flexion leading to suddenly increased intraluminal pressure (39). Post-surgical or endovascular causes of carotid-cavernous sinus fistulas include craniofacial surgery, stent-assisted coil embolization of an intracavernous carotid aneurysm, and mechanical thrombectomy for stroke (15; 02; 104; 67).
Spontaneous direct carotid-cavernous sinus fistulas result from a weakened arterial wall by an aneurysm, pseudoxanthoma elasticum, osteogenesis imperfecta, fibromuscular dysplasia, or Ehlers-Danlos syndrome (84; 26; 41; 66). A patient with recurrent direct carotid-cavernous sinus fistulas has been found to have a novel mutation in the COL3A1 gene (94).
Indirect carotid-cavernous sinus fistulas are rarely caused by trauma. They usually appear spontaneously and insidiously in middle-aged and elderly women following the rupture of the thin-walled dural arteries within the cavernous sinus (73). Collateral anastomoses may develop after venous thrombosis in the cavernous sinus (93; 85). This may explain why dural carotid-cavernous sinus fistulas are more common in women, especially during pregnancy and the early postpartum period (98). Additionally, a congenital defect is suggested by indirect carotid-cavernous sinus fistulas in infants without an obvious risk factor (52; 30). Mechanical thrombectomy may also cause indirect carotid-cavernous sinus fistulas (54).
|
• Direct carotid-cavernous sinus fistulas occur after head trauma associated with basal skull fractures or surgical procedures. | |
|
• Posttraumatic carotid-cavernous sinus fistulas occur mostly in young men. | |
|
• Carotid-cavernous sinus fistulas occurring after aneurysm rupture are more frequent in older women. |
Direct carotid-cavernous fistulas occur with an incidence ranging from 0.17% to 1.01% after traumatic brain and facial injury (91). In a series of 100 consecutive direct carotid-cavernous fistulas, 76 were caused by trauma, 22 by a ruptured aneurysm, and two were iatrogenic. Motor vehicle accidents and falls were the most common traumatic causes. Most trauma-related cases occurred in young men, whereas aneurysm rupture occurred predominantly in older women (53).
A retrospective chart review of 312 patients showed that in basal skull fractures, the incidence of direct carotid-cavernous fistula is 3.8% and up to 8.3% if the middle cranial fossa is usually involved (55). In another retrospective study, 11.5% of patients developed a direct cavernous carotid fistula within two weeks of treatment of a cavernous aneurysm with a flow diverter (86).
Intracranial dural arteriovenous fistulas account for 10% to 15% of all intracranial arteriovenous malformations (72). Of these, indirect carotid-cavernous fistulas account for approximately 12% and are the second most common type of intracranial dural carotid-cavernous fistula after those involving the transverse sigmoid sinus. Thus, at most 0.0018% (approximately 5400 people) of the United States population would be expected to have an indirect carotid-cavernous fistula.
|
• Direct carotid-cavernous fistulas may be prevented by avoiding head trauma and by mapping the vasculature before the high-risk associated procedures. | |
|
• Indirect carotid-cavernous fistulas preventive measures include control of the risk factors: hypertension, atherosclerosis, and thrombophilia. |
As most direct carotid-cavernous fistulas occur after trauma, head protection against trauma is reasonable. Iatrogenic-related direct carotid-cavernous fistula can be prevented by thorough knowledge of the patient’s carotid vasculature and medical history. For example, the accidental creation of a direct carotid-cavernous fistula during transsphenoidal surgery for pituitary adenoma is more common in patients with a history of previous transsphenoidal surgery or radiation treatment. Preoperative evaluation of intracranial vasculature with magnetic resonance or digital subtraction angiography may prevent the creation of a direct carotid-cavernous fistula during tumor resection (51).
Although there is no proven way to reduce the incidence of indirect carotid-cavernous fistulas, treating hypertension, atherosclerosis, and thrombophilia appears sensible.
Direct carotid-cavernous fistulas.
Because direct carotid-cavernous fistulas typically present with prominent orbital or ocular congestion, the main differential diagnoses include orbital processes such as thyroid eye (Graves) disease, idiopathic orbital inflammation (inflammatory orbital pseudotumor), orbital cellulitis, intraorbital tumor (eg, meningioma), or the various other causes of cavernous sinus syndrome (eg, carotid-cavernous thrombosis or Tolosa-Hunt syndrome). The main distinguishing aspect is the association of direct carotid-cavernous fistulas with recent, severe head trauma.
Thyroid eye disease. Exophthalmos and limitation of eye movement present subacutely and without trauma. Typically, both eyes are involved with the characteristic retraction of the upper eyelid. Chemosis and conjunctival injection are less severe than in direct carotid-cavernous sinus fistulas (12).
Idiopathic orbital inflammation. This entity encompasses nonspecific orbital inflammation that cannot be attributed to infection, tumor, or another identifiable cause. The signs and symptoms range from mild myositis to severe orbital apex syndrome. By presenting acutely, subacutely, or chronically, it may mimic both direct and indirect carotid-cavernous sinus fistulas. Like a direct carotid-cavernous sinus fistula, it usually presents unilaterally with severe scleral injection. However, it is not typically associated with trauma or an orbital bruit. Idiopathic orbital inflammation is sensitive to corticosteroids (44).
Orbital cellulitis. This condition presents with severe proptosis, eyelid edema, pain with extraocular eye movements, and vision loss. However, infection occurs over several days and is often preceded by upper respiratory infection, nasal congestion, or sinusitis. The constitutional symptoms include fever, decreased appetite, or malaise. Cellulitis responds to antibiotics (97).
Intraorbital tumor. Slowly progressive proptosis, paralytic or restrictive eye movements, and vision loss suggest an intraorbital tumor. Corkscrew conjunctival vessels are not seen with intraorbital tumors.
Vertebral-venous fistula. A case of vertebral-venous fistula resembling a carotid cavernous fistula was diagnosed by angiography. Although extremely rare, it should be suspected if carotid angiography is normal in a patient with symptoms suggestive of carotid-cavernous sinus fistulas (34).
Indirect (“dural”) carotid-cavernous fistulas.
Indirect carotid-cavernous sinus fistulas are insidious and should be distinguished from conjunctivitis, blepharitis, episcleritis, or scleritis. However, carotid-cavernous sinus fistulas typically exhibit a radial, corkscrew pattern of the conjunctival or scleral injection. Moreover, carotid-cavernous sinus fistulas do not cause discharge and are refractory to topical antibiotics or anti-inflammatory medications. Lastly, cranial nerve palsies and other intracranial manifestations (eg, headache or transient ischemic attacks) occur frequently in indirect carotid-cavernous fistulas but not in these ocular inflammatory conditions.
The differential diagnosis of vision loss includes posterior ischemic optic neuropathy, proliferative retinopathy, choroidal detachment, and effusion (37).
|
• History of trauma and acute presentation suggest direct carotid-cavernous fistulas. | |
|
• High ocular pulse amplitude measured by tonometry is consistent with either direct or indirect carotid-cavernous fistulas. | |
|
• CT or MRI of the head and CT or MR angiography are sensitive to structural changes and blood flow abnormalities, respectively. | |
|
• Transcranial and carotid Doppler may detect carotid-cavernous fistulas missed by CT or MR angiography. | |
|
• Digital angiography is the gold standard for carotid-cavernous fistula imaging. |
Direct carotid-cavernous fistulas present with dramatic orbital signs after severe head trauma and basal skull fractures. The patients describe a whooshing noise or a heartbeat bruit in their head. The bruit can be auscultated with a stethoscope placed over the closed eye or at the temple. Arterialization of the conjunctival vessels occurs more frequently in carotid-cavernous fistulas than in other orbital diseases. Indirect carotid-cavernous fistulas, especially those draining posteriorly, are more difficult to diagnose by history and physical examination alone. One should still suspect them in any middle-aged to elderly woman presenting with a spontaneous red eye, chemosis, isolated or multiple cranial nerve palsy, and mild orbital congestion (63). Misdiagnosis is common. A retrospective series of 24 patients with carotid cavernous fistulas identified two patients who were diagnosed with cluster headaches: one with an orbital fracture and one with thyroid eye disease (08).
Ocular pulse amplitude. Tonometry helps diagnose a carotid-cavernous sinus fistula by measuring the ocular pulse amplitude, which is the difference between the maximum and minimum intraocular pressure during the cardiac cycle. In one study, an ocular pulse amplitude larger than 1.6 mmHg was 100% sensitive and 93% specific in distinguishing carotid-cavernous sinus fistulas from other orbital diseases. However, this method cannot distinguish the direct from indirect carotid-cavernous sinus fistula (32). The ocular pulse amplitude usually normalizes after endovascular embolization (32; 48).
Imaging. The radiographic evaluation of a carotid-cavernous sinus fistula begins noninvasively with CT, CT angiography, MRI, MR angiography, or transcranial Doppler ultrasound. A CT scan is initially used after head trauma. Direct carotid-cavernous sinus fistulas are characterized on CT by ipsilateral proptosis, cavernous sinus and superior ophthalmic vein expansion, enlargement of the extraocular muscles, and possible skull fractures (83).
Magnetic resonance imaging (MRI) has a similar diagnostic utility to CT but is less sensitive in detecting bone fractures. An abnormal cavernous sinus flow void suggests the presence of a carotid-cavernous fistula. In one study of indirect carotid-cavernous fistulas, CT detected a dilated superior ophthalmic vein more often than MRI. MRI also found an abnormal flow void in the cavernous sinus in 11 of 12 patients with indirect carotid-cavernous fistulas (100).
CT angiography allows direct visualization of the carotid-cavernous fistula (23). In one study, CT angiography matched the catheter angiography and was superior to MRA. This advantage was even greater in diagnosing direct carotid-cavernous fistulas involving the C4 segment of the internal carotid artery (16). A review of 18 consecutive patients with a carotid-cavernous fistula analyzed the most sensitive and specific imaging features diagnosed by CTA. Early enhancement and dilatation of the superior ophthalmic vein had 100% sensitivity. Arterial-phase contrast in the cavernous sinus had 88.9% sensitivity (10). 4D CT angiography is increasingly used for diagnosis (101; 60).
MR angiography directly visualizes carotid-cavernous sinus fistulas. However, traditional angiography is superior for delineating the small arterial feeder vessels or cortical venous drainage (87). 4D flow MRI allows a preoperative quantitative analysis of blood flow velocity and volume in direct carotid cavernous fistula (70).
Ultrasound. Other imaging modalities are transcranial, transorbital color Doppler, and carotid duplex ultrasonography (18; 19). Vascular ultrasound facilitates the diagnosis of indirect carotid-cavernous sinus fistulas not seen by CT or MRI and helps assess blood flow. Color Doppler ultrasound may indicate the need for invasive conventional angiography, assess the collateral capacity of the circle of Willis, and judge the outcome of the intervention (49). Orbital color Doppler ultrasound (OCDUS) can rule out an anterior-draining carotid-cavernous fistula (102).
Digital subtraction angiography. The gold standard for diagnosis of direct and indirect carotid-cavernous fistulas is catheter angiography. Cerebral angiography can localize the carotid-cavernous fistula, delineate the feeder vessels, and assess the drainage pattern. If the cavernous sinus is draining superiorly into the cortical veins, intracerebral hemorrhage, and possible hemiparesis may be prevented by emergency treatment. Angiography can map the optimal route of approach, transarterial or transvenous, whether the carotid-cavernous fistula is being fed bilaterally, and the capacity of the circle of Willis (25). A common regimen that answers these questions includes selective injections of both internal carotid arteries and external carotid arteries, the ipsilateral vertebral artery, the ipsilateral ascending pharyngeal artery, middle and accessory meningeal arteries, and proximal and distal internal maxillary arteries (61). In a retrospective study of only eight patients, using the DSA-Dynavision in treatment planning allowed more precision in their treatment and reduced the time of treatment (11).
|
• There are no randomized clinical trials of the treatment of carotid-cavernous sinus fistulas. | |
|
• Indirect carotid-cavernous fistulas may improve or heal spontaneously with conservative management. | |
|
• However, retrograde venous drainage is associated with higher mortality and requires urgent treatment. | |
|
• Direct carotid-cavernous fistulas are treated mostly with endovascular therapy. | |
|
• Endovascular treatment includes coiling, embolization, covered stents, flow diverters, and micro-plug or arterial sacrifice. | |
|
• Surgical approach is reserved for failure of endovascular therapy. |
The definitive treatment of any arterial-venous fistula is the obliteration of the abnormal connection. There are four methods of treatment: conservative, endovascular, stereotactic radiation, and surgical. The type of carotid-cavernous sinus fistulas often guides the chosen treatment, but the optimal approach is still unknown.
Conservative treatment. Indirect carotid-cavernous fistulas may close spontaneously or after diagnostic angiography alone in as many as 60% of patients (80; 83). Another conservative approach is a trial of carotid compression causing thrombosis (40; 36; 46). Initially, the ipsilateral carotid artery is compressed with the opposite hand for 10 seconds thrice hourly while awake. The compression duration is gradually increased until complete occlusion is achieved. Direct carotid-cavernous sinus fistulas respond less to this method due to the high flow. Complete resolution of symptoms was reported in 21% to 34% of patients with indirect carotid-cavernous fistulas (40; 36; 46).
Conservative management alone may succeed even without thrombosis or closure of the indirect carotid-cavernous fistula. For example, one series found that 82% of patients (39 of 48) recovered or significantly improved with conservative treatment (27). However, closure delay of a retrograde venous drainage pattern increases the risk of intracerebral hemorrhage and mortality by 30% (36).
Endovascular treatment. Endovascular treatment is the primary means of treating carotid-cavernous sinus fistulas. The surgical intervention is reserved for endovascular failure. Direct and indirect carotid-cavernous sinus fistulas can be closed by transarterial or transvenous routes, or a combination. The endovascular modalities include coils, stents, flow diverters, liquid embolic material, carotid sacrifice, detachable balloons, a vascular micro-plug, or combinations of these (09).
Direct carotid-cavernous sinus fistulas are usually closed by transarterial coiling, with or without a supportive stent (68). In a series of 172 patients with direct carotid-cavernous sinus fistulas, the endovascular occlusion rate was 94%, with a 70% rate of sparing the carotid artery (20). Mortality and morbidity were 0.6% and 2.4%, respectively.
Covered stents and flow diverters allow vascular reconstruction without occluding the sinus (103; 95; 50; 56; 74; 82). A systematic review showed that flow diverters used alone, or as adjunct treatment may be useful. However, long-term data are unavailable (90).
Indirect carotid-cavernous sinus fistulas are challenging to treat because the feeding vessels may be multiple, small, tortuous, or difficult to reach. The transvenous approach via the inferior petrosal sinus is the preferred route. Other options include the superior petrosal sinus, basilar plexus, pterygoid plexus, the facial vein, or even a direct puncture of the dilated superior ophthalmic vein or percutaneous access to the facial vein with ultrasound guidance (65; 61; 62; 106; 71; 24; 105; 58; 03). Coils or liquid agents are used for embolization. Robotic surgery can facilitate the embolization of indirect carotid-cavernous sinus fistulas (47).
In a retrospective analysis of 267 patients, obliteration was accomplished in 86.5% (04). In another retrospective analysis of 98 patients, the transvenous approach had a higher obliteration rate than the transarterial approach (94.3% vs. 75%, respectively). The complication rate of coiling is lower when compared to liquid embolic agents (05).
Occasionally, a tortuous carotid artery limits the endovascular access to the fistula. Another approach to indirect carotid-cavernous sinus fistulas, when the endovascular treatment is contraindicated, is the endoscopic endonasal orbital apex decompression (88).
A direct carotid-cavernous sinus fistula can be closed by sacrificing the carotid artery. The feasibility of this procedure is tested preoperatively by transient balloon occlusion of the carotid artery followed by a nuclear perfusion study to determine the robustness of the collaterals.
Surgical treatment. Access to the cavernous sinus involves posterior orbitotomy or craniotomy (79; 83; 69; 89). In a series of 19 patients who failed endovascular treatment, direct surgery closed 100% of the carotid-cavernous sinus fistulas. However, three patients (16%) required a graft to bypass the trapped intracavernous carotid artery, and in approximately 26% of procedures, the internal carotid artery or bypass graft was sacrificed (99).
Radiotherapy. Targeted radiotherapy with gamma knife or X-Knife® triggers thrombosis and occlusion of the carotid-cavernous sinus fistulas. The closure rate for 22 indirect carotid-cavernous fistulas was 90.9%, with no recurrences during follow-up up to 14 years. However, improvement may take an average of 2.4 months, and complete occlusion takes approximately 7.5 months (06). This latency is similar to other studies (81; 75; 21).
Complication rates depend on the radiotherapeutic modality. In one study, X-Knife® delivered higher radiation doses to the lens, optic nerve, optic chiasm, and brainstem than gamma knife (76). Stereotactic radiotherapy closed only a third of posttraumatic direct carotid-cavernous fistulas (06). In a retrospective study of 18 cases, stereotactic radiosurgery achieved total obliteration of direct carotid-cavernous sinus fistulas in 83% of patients at 2 years (77).
The ocular compartment syndrome requires urgent canthotomy/cantholysis performed by an ophthalmologist to decrease the intraocular pressure and prevent vision loss (59).
Angiographic occlusion of the carotid-cavernous sinus fistulas predicts a good outcome (45). Of 34 patients with direct and indirect carotid-cavernous sinus fistulas, all showed complete recovery, and only one patient (3%) had a complication. Possible complications after endovascular treatment include groin hematoma, infection, intracranial hemorrhage, new neurologic deficit, endocrine dysfunction, or recurrence (38). The syndrome of inappropriate antidiuretic hormone secretion after Onyx embolization has been described (17).
Patients with impaired renal function. Renal dysfunction may aggravate due to contrast use during an endovascular procedure. The risks and benefits must be weighed carefully and discussed with the patient and family. Radiotherapy may be an option.
Women may develop indirect carotid-cavernous sinus fistulas during pregnancy or postpartum due to cavernous sinus thrombosis (98). Additionally, the hemodynamic changes during pregnancy may explain the reopening of a previously resolved direct carotid-cavernous sinus fistula. Backflow to the cortical veins may lead to intracerebral hemorrhage and hemiplegia (57).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Adrian Marchidann MD
Dr. Marchidann of Kings County Hospital has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
Dec. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Sleep Disorders
Oct. 14, 2024
Developmental Malformations
Sep. 22, 2024