


Epilepsy & Seizures
Tonic status epilepticus
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Cerebral cavernous malformations are vascular lesions that may cause hemorrhage, seizures, headaches, cranial neuropathies, or neurologic manifestations reflecting lesion location. Sporadic and familial forms of this disorder are increasingly recognized with the advent of gradient-echo MRI. Genetic studies have elucidated at least 3 genes associated with familial forms of this disorder, suggesting abnormal angiogenic stimuli as an important etiopathogenic factor. In this article, the author summarizes the clinical features and data related to this syndrome.
• Cerebral cavernous malformations are an increasingly recognized cause of intracranial hemorrhage that can be detected with MRI. | |
• Recurrent bleeds may occur, causing symptoms due to tissue injury and edema. | |
• Medical therapy primarily focuses on seizure control, and surgery is possible in selected cases. |
The existence of vascular anomalies of the brain has been known for over 100 years. The first reported case dates to 1895, in the works of Steinheil (93), whereas the classic study of "angiomatous angiomas" by Virchow constitutes the first comprehensive work on cerebral vascular malformations (36). Over the past century, the elucidation of these anomalies has challenged the most illustrious minds in neurosurgery and neuropathology. In 1928 Cushing and Bailey, through meticulous observation and documentation of autopsy and surgical specimens, made the critical distinction between true vascular tumors and congenital malformation of blood vessels (36). Subsequently, Olivecrona devised a classification system for the latter based on etiology and pathology. He classified cavernous malformations as distinct from the racemose lesions, which included arteriovenous, venous, and capillary malformations (93). In their landmark reports, Russel and Rubenstein, as well as McCormick proposed more stringent classification systems for cerebral vascular malformations. They recognized 4 discrete entities: (1) arteriovenous malformation, (2) capillary telangiectasias, (3) venous malformations, and (4) cavernous malformations (84; 109). This categorization forms the basis of our current classification of these lesions. The evolution of the nomenclature of intracranial vascular malformations (from the original, vague and all-encompassing term "angiomatous arteriovenous aneurysms," to the nondescript "angioma," to the currently accepted "cavernous malformation") reflects the evolution of consensus regarding their pathophysiology. Collaborative efforts have delineated the key research priorities on cavernous malformations (14).
Cavernous malformations are well circumscribed lesions that consist of closely packed, enlarged, capillary-like vessels without intervening brain parenchyma (29). They create a spectrum of presentations, ranging from the asymptomatic lesion, discovered incidentally at autopsy or on neuroimaging, to the rare reported cases of fatal hemorrhage. The clinical course is highly variable. Patients present with acute or chronic neurologic deficits, periods of remission and exacerbation, or a progressive, insidious deterioration (128; 119; 20; 21; 62).
Patients with headache or nonspecific symptoms generally are categorized as asymptomatic. Headache has been associated as the only complaint in up to 30% of cases (119; 107; 62). In other studies, up to 44% of patients harboring single or multiple lesions had no symptoms. On rare occasions, presenting symptoms may include trigeminal neuralgia (05). One case described migraine as the presenting feature of a cavernoma (06). It has been estimated that less than half of those will develop new neurologic symptoms within 5 years (57; 107).
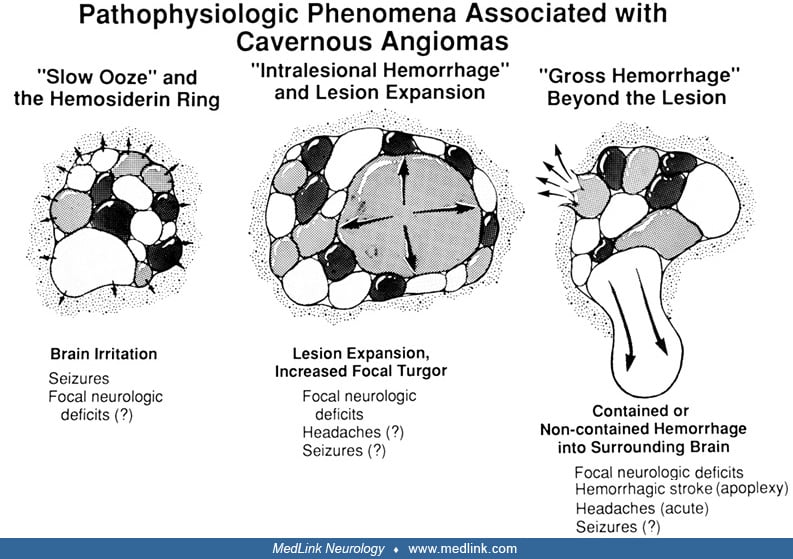
Epilepsy is the most common clinical presentation of cavernous malformations (119; 103; 40; 16; 18; 62; 16; 105). All seizure types have been observed, with generalized tonic-clonic seizures being the most common, followed by complex partial seizures and simple seizures (16; 18; 16). In some cases, the disorder is longstanding and controlled on medication, whereas in other cases seizures are of sudden onset. Seizures can herald acute intracranial hemorrhage. The pathophysiological features of seizures among patients with cavernous malformations are related to the size of the lesion and the iron deposits in the surrounding brain tissue after repeat microhemorrhages (09).
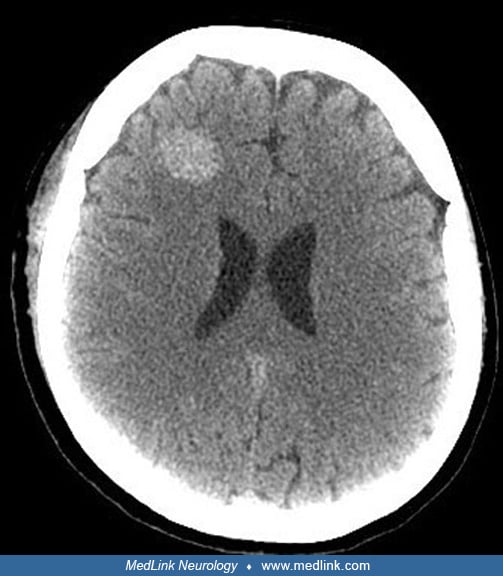
Hemorrhage is the second most common clinical presentation of cavernous malformations (119; 103; 40; 107; 105; 16; 18; 20; 21). A critical distinction is made between gross intracranial hemorrhage and ongoing repeated microhemorrhages. The latter is universally present in cavernous malformations, and usually clinically silent. Gross hemorrhage is less common, but more significant. Such hemorrhages may be more common in lesions with associated venous malformations (67). Hemorrhages are usually intraparenchymal. One paper described perimesencephalic hemorrhage into the subarachnoid space from a cavernoma (136). The clinical findings depend on the location of the lesion. Typically, the patient has acute onset of headache, followed by the development of new neurologic deficits and depression of the level of consciousness. Hemorrhages in the posterior fossa result in neurologic sequelae more frequently, due to the clustering of nuclei, vital tracts, and the possibility of obstructing CSF pathways in this location. Characteristic symptoms include headache, emesis, ataxia, nystagmus for lesions in the cerebellum and diplopia, hemiparesis, sensory changes, and change in mental status for brainstem cavernous malformations (107; 20; 21).
An exhaustive review of 1426 publications about cavernomas in humans formed the basis for a uniform definition and reporting standards. They defined a cavernoma-related hemorrhage as requiring acute or subacute onset symptoms (headache, epileptic seizure, impaired consciousness, or new/worsened focal neurologic deficit referable to the anatomic location of the cavernous malformation) accompanied by radiological, pathological, surgical, or rarely only cerebrospinal fluid evidence of recent extra- or intralesional hemorrhage. The definition includes neither an increase in cavernous malformation diameter without other evidence of recent hemorrhage nor the existence of a hemosiderin halo (12).
Individual hemorrhages are self-limited, and patients generally achieve a good recovery (107; 148; 20; 21; 08; 70). However, recurrent clinically overt hemorrhages are associated with progressive neurologic decline and severe residual deficits. In the brainstem, there may be periods of exacerbation followed by remission, mimicking demyelinating disease (107; 148; 20; 21). Regardless of the presentation, data from several studies suggest that the risk of recurrent hemorrhage is increased after an initial bleed (57; 107; 80; 20; 21; 08; 88; 89; 13; 50).
The third common clinical presentation of cavernous malformations is an acute, or progressive, neurologic deficit. This is usually associated with intralesional or perilesional hemorrhage documentable by MRI. The frequency in clinical series ranges from 15.4% to 46.6% (57; 119; 103; 40; 107; 105a; 105b; 80; 110; 141). The precise syndrome depends on the lesion location and size. The deficit may be transient, progressive, recurrent, or fixed. Aggressive and recurrent hemorrhagic episodes leave heightened degrees of disability, often resulting in severe fixed impairments (107; 105; 148; 80; 20; 21; 110; 38). The cumulative morbidity from repeated bleeds of angiography occult vascular malformations (usually a cavernous malformation) is greater than that from arteriovenous malformations (80; 21).
Other neurologic manifestations or presenting features may be dependent on the location of the cavernous malformation. For instance, hemichorea may result from a cavernoma in the putamen (45).
The prognosis of patients presenting with cavernous malformations has been calculated in a large series of 326 patients (65). The data suggest that the annual risk of hemorrhage is 4.46% per lesion-year. In another large series of 331 cases, the annual hemorrhage rate was 8.7% in patients initially presenting without hemorrhage (n = 82) (77). The risk factors for hemorrhage were female sex (hazard ratio [HR] 1.445, p = 0.041), prior hemorrhage (HR 1.277, p = 0.029), and perilesional edema (HR 1.830, p = 0.002). It has been estimated that improved/unchanged outcomes occurs in most patients (85.4%) with incidental brainstem cavernomas (145).
It is not presently known what triggers the development or the rate of growth of cavernous malformations. The classic work of Russel and Rubenstein best characterizes our current understanding: "by definition these hamartomas are conceived as congenital anomalies (usually arising between 3 and 8 weeks of gestation) that, though not true neoplasms, somewhat resemble tumors in their clinical and macroscopic features. And in common with the true neoplasms, it is clear that some at least are not static but grow and inflict progressive destruction on the adjacent brain" (109).
The existence of familial forms of cavernous malformation lends further support to the premise that these are congenital lesions. Linkage studies of families of Hispanic and non-Hispanic origin have localized the gene for cavernous malformations to the proximal segment of chromosome 7q (58; 83; 92; 98). Kindred analysis supports an autosomal dominant pattern of inheritance with variable penetrance (60; 103; 58; 83; 92; 98).
Several published and anecdotal reports also raise the possibility of the development of lesions de novo (07; 68; 33). Such reports were initially ascribed to MRI limitations, but further reports have surfaced (102; 26). Some occur spontaneously without apparent antecedent pathology. Others have been documented after stereotactic or standard radiation (68; 19; 37), after viral infection, or after reactive angiogenesis from microhemorrhage (140). Reports of de novo formation in moyamoya disease also implicate upregulated angiogenesis (72; 117; 64).
There is greater certainty regarding the etiology of the clinical manifestations of cavernous malformation. Cavernous malformations appear to be more frequently associated with intractable epilepsy than other vascular malformations (16; 18). The epileptogenic potential of cavernous malformations is ascribed to the destruction of red blood cells from repeated microhemorrhages. The subsequent deposition of heme breakdown products, particularly iron, in the surrounding brain tissue leads to a gliotic reaction; brain irritation and mass effect are believed to trigger the cellular cascades, leading to seizures (16; 18). Hemorrhage and lesion growth lead to mass effect and focal damage, which account for focal neurologic deficits consistent with the clinical spectrum of cavernous malformations.
Little is understood of the specific factors that determine the hemorrhagic behavior of cavernous malformations. Histoimmunological and histochemical studies have identified several angiogenic proteins present in these lesions. Vascular endothelial growth factor, basic fibroblast growth factor, fibronectin, collagen type 4, and alpha smooth muscle actin are expressed by cavernous malformations. The presence of these compounds is felt to be indicative of enhanced angiogenic activity (66). It is, though, nonspecific, as these same compounds are found in arteriovenous malformations and dural arteriovenous malformations (108). Tissue plasminogen activator has also been identified in cavernous malformations, particularly in those presenting with hemorrhage (52). It has, therefore, been suggested that local thrombolytic activity of tissue plasminogen activator may play a role in initial and recurrent hemorrhages (52). The role of angiogenic and thrombolytic factors needs further investigation to better characterize their precise role in the biological behavior of cavernous malformations.
The cavernous malformations are grossly discrete, well-circumscribed lesions with a reddish-purple, multiloculated appearance that has often been likened to a cluster of mulberries. In contrast to arteriovenous malformations, these lesions lack features of high flow, or the enlarged arterial feeders or draining veins, that are associated with arteriovenous shunting (84; 109; 107). On electron microscopic evaluation, cavernous malformations are composed of caverns of varying size, filled with resorbing intracavernous blood, whose thin walls are lined by endothelial cells (126). Pathology studies have revealed that sinusoidal venules may be admixed with thrombus and granulation tissue (02). A progressive process of thrombosis within cerebral venules associated capillary bleeding and hematoma expansion has been postulated as a potential pathophysiologic mechanism for the development of cavernous malformations (02; 17). Uniformly, the basal laminae are intact (134). The lack of intervening brain parenchyma is one of the characteristic pathologic markers of cavernous malformations (84; 109). Frischer and colleagues have proposed revision in lesion definition, as the absence of intervening brain parenchyma does not represent an essential histopathological criterion, and the diameter of the vessel lumina and the thickness of vessel walls may widely vary (53). The lesion is not always racemose and may include satellite-like projections into the adjacent brain. Rare reports show disorganized, scattered elastic fibers in lesions, with morphological features consistent with cavernous malformations (119). The surrounding parenchyma often has evidence of prior microhemorrhage, hemosiderin discoloration, and hemosiderin-filled macrophages. Within the lesion, hyalinization, thrombosis with varying degrees of organization, calcification, cysts, and cholesterol crystals are common (84; 128; 109; 119; 103; 97). A gliotic reaction of the surrounding parenchyma is characteristic and may form a capsule around the lesion.
Mixed or transitional lesions containing features common to more than 1 class of vascular malformation have been described (109; 103; 80; 16; 18; 21; 105). A cavernous malformation may be associated with capillary telangiectasias that are adjacent or remote from the lesion. Other cavernous malformations are identified with neighboring medullary venous structures, which are akin to venous malformations (135; 03). In rare cases, cavernous malformations may be associated with features of venous occlusive disease (43). The role of the venous system has been further explored as a possible factor in lesion development as well (04). In some lesions with predominant cavernous malformation histology, there are regions with more mature vessels suggestive of arteriovenous malformations. Culture of endothelial cells from cavernous malformations has revealed the increased angiogenic activity within these lesions and relative sensitivity to vascular endothelial growth factor (143). Cerebral cavernous malformations also have been shown to increase the endothelial expression of MMP-2, MMP-9, and TIMP-2, promoting hemorrhage (54).
Estimates of the prevalence of cavernous malformations vary considerably. Older studies relied on large autopsy specimens, whereas more recent studies examined angiograms, CT, and MRI. In some cases, the prevalence has been projected from relative frequency ratio between arteriovenous malformations, aneurysms, and cavernous malformations with questionable validity (23). The major autopsy data documented a calculated prevalence of 0.02% to 0.53% (95; 62), whereas other serial MRI studies examining lesions with imaging characteristics typical of cavernous malformations calculate a prevalence rate of 0.39% to 0.9% (40; 62; 16; 110).
The existence of a familial form, characterized by multiple lesions and an autosomal dominant inheritance pattern, is well documented (57; 60; 103; 141; 58; 83). The prevalence is notably higher than suggested in earlier scattered clinical reports. Multiplicity in familial lesions is as high as 73%, compared to less than 33% for sporadic lesions (57; 103; 141). It has been suggested that Hispanic patients may have a higher predilection for familial cavernous malformations (60; 103). Several genes and specific mutations causing cerebral cavernous malformations in families with the disease have been identified. In the last few years, many advances have culminated in elucidating the genetics of these vascular lesions (74). Linkage analyses using autosomal dominant families manifesting CCMs have identified 3 different causative loci on chromosomes 7q21.2 (CCM1), 7p13 (CCM2), and 3q25.2-q27 (CCM3) (130). CCM1 encodes the ankyrin containing protein Krit1, which binds a putative tumor suppressor protein in vitro (144). Phosphatase and tension homolog deleted on chromosome 10 (PTEN), a tumor suppressor, has been associated (146; 147). This may, in turn, participate in angiogenesis (39). Mutations in the gene MGC4607, or Malcavernin, are responsible for CCM2 (116). A study established Programmed Cell Death 10 (PDCD10) as the gene responsible for CCM3 (22). PDCD10/CCM3 is highly expressed in the neurovascular unit and in the arterial endothelium of the brain (124). The potential for a fourth locus has also been suggested (78). Incomplete penetrance, isolated cavernous malformations, and lesions that evade accurate gradient-echo MRI detection may limit the distinction of familial from sporadic forms of cavernous malformations (42; 56; 76). The phenotypic manifestations of cerebral cavernous malformation genetic mutations may also be highly variable (41; 55; 115).
Intracranial cavernous malformations affect both sexes with equal frequency, except in the middle cranial fossa, where there is a female preponderance. It affects all ages, with a majority of patients presenting in the second to fourth decade. Data from virtually all clinical series demonstrate that symptomatic lesions are rare in the elderly. It has been suggested that there is a male predominance in patients presenting at less than 30 years of age, a female preponderance in patients aged 30 to 60 years, and a more equal ratio thereafter (107). It is not known why cavernous malformations manifest so rarely later in life. It is possible that lesions invariably become symptomatic early in life or not at all, or that senescence may be associated with lesion regression or quiescent behavior (11).
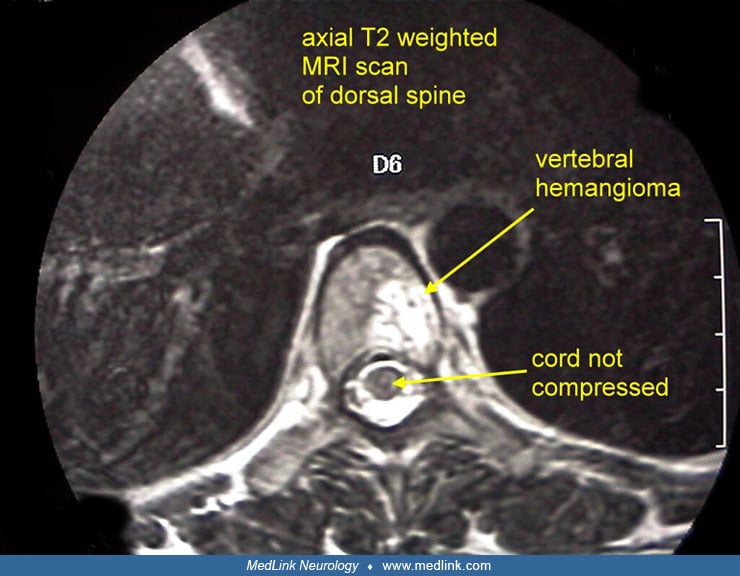
Cavernous malformations have been reported to range in size from less than 0.1 cm to as large as 9 cm (109; 119; 40; 62). The majority of intracranial cavernous malformations are supratentorial, whereas approximately 15% are infratentorial, and 5% are located in the spine (140). Less common intracranial locations include the cerebellopontine angle, the pineal gland, the middle fossa, the cavernous sinus, the optic nerve and chiasm, and dural based lesions. Cavernous malformations have been reported in association with other vascular lesions, such as capillary telangiectasias, arteriovenous malformations, and venous malformations, with a frequency of 8% to 44% (128; 109; 119; 107; 16; 18; 21; 105; 106). Initial studies suggest that cavernous malformations are more likely to be part of a mixed lesion than other vascular malformations, the most common association being between cavernous malformations and venous malformations. As the latter does not usually present with hemorrhage, any hemorrhage in a patient with a known venous malformation should be evaluated to rule out cavernous malformation. In a study by Abdulrauf and colleagues, 24% of patients with cavernous malformations had associated venous malformations (01). Patients in this group were more likely to present with symptomatic hemorrhage and more likely to have infratentorial lesions than in the group of patients with cavernous malformation only. Also observed was the fact that cavernous malformations associated with venous malformations were more likely to occur in females and less likely to present with seizures or family history of vascular malformation. Intracranial cavernous malformations may rarely be found in conjunction with intraspinal, extracerebral soft tissue, and visceral hamartomas (109; 62; 125), and other central nervous system tumors such as meningiomas and astrocytomas (62). A seasonal predilection for bleeding of cavernous malformations has been disclosed (49).
There are scant data for identifying specific host and lesion factors that determine the biological behavior of cavernous malformations. Pediatric and pregnant patients may have a greater risk for hemorrhage, and this possibly supports a more aggressive surgical approach, although a series during pregnancy suggests a more indolent course (75; 120; 85). In addition, a bleed predicts a greater risk of subsequent hemorrhages. In contrast, lesion size, association with other vascular malformations, and location do not appear to significantly affect the risk of hemorrhage, although infratentorial bleeds tend to manifest neurologic sequelae more frequently.
There are no known modifiable risk factors of clinical sequelae in cavernous malformations.
Cavernous malformations are a distinct entity within the category of vascular malformations of the central nervous system, which also include arteriovenous malformations, capillary malformations (telangiectasias), and venous malformations. They have traditionally been considered congenital hamartomas distinct from true vascular neoplasms, each possessing characteristic gross and microscopic morphology (84; 109).
Arteriovenous malformations are the most commonly recognized and clinically well-documented of the cerebrovascular malformations. They appear as a tangled, serpiginous mass of abnormally dilated vessels of variable caliber, with intervening and surrounding parenchymal gliosis. On microscopic evaluation, the arterial walls often display abnormalities of the internal elastic lamella, the elastic and muscle fibers, as well as the media, which may be thickened or thinned with aneurysmal dilatation. The arteries are directly connected to abnormal veins without an intervening capillary network. The veins are classically "arterialized" with secondary collagenous hyalinization. Signs of fibrosis and atheroma, particularly in the arteries and varicose dilatation in the veins, are among the more common degenerative changes demonstrated in the walls of these vessels. There is intervening gliotic brain parenchyma within the interstices of the nidus. Arteriovenous malformations are rarely multiple or familial, except in cases of hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu disease). Lesions may be associated with adjacent ischemic parenchymal changes, resulting in seizures or focal neurologic deficits, or may cause apoplectic hemorrhage from rupture of the arteriovenous malformation nidus or associated aneurysm (84; 109).
Capillary malformations are often incidental findings at autopsy. Macroscopically, they appear as a poorly demarcated pink or reddish discolored region with dilated capillaries, occasionally having a petechial hemorrhage appearance. The capillaries are lined by a layer of endothelium, and lack muscle or elastin fibers. The vessels are of differing calibers, occasionally with fusiform and saccular dilations. The presence of intervening normal parenchymal tissue between the vessels, and the absence of surrounding gliosis and microhemorrhages, distinguishes these capillary telangiectasias from other vascular malformations (109). Capillary malformations can be found in the same host harboring cavernous malformations, and as satellite lesions beyond the cavernous malformation.
Venous malformations are relatively common, usually asymptomatic lesions characterized by a single dilated vein or a cluster of abnormally large veins, and drained by a single large vein appearing as the classic caput medusa pattern. They are rarely associated with hemorrhage. There is regional venous dysmorphism, with the venous malformation typically solely responsible for competent venous drainage, with paucity of other regional venous structures. Intervening parenchyma is typically normal, although the venous malformation has been shown in association with cavernous malformations (109; 16; 105; 106).
At present, no clinical syndrome or diagnostic test establishes the diagnosis of cavernous malformations. A combination of clinical presentation and neuroimaging can suggest the presence of this lesion, which ultimately can only be proven with certainty by pathological specimen.
MRI is the most sensitive diagnostic tool (27). The appearance is sufficiently characteristic to allow confident preoperative evaluation of symptomatic lesions, identification, screening, and follow-up of incidental lesions, and depiction of lesion behavior including expansion, hemorrhage, and thrombosis (103; 107; 97; 110). Cavernous malformations typically appear as well-defined, lobulated lesions on MRI with a classic T2-weighted image of a central core of reticulated mixed density surrounded by a rim of signal hypointensity (107; 97; 110). A T1-weighted hyperintensity may also be found at the periphery of these lesions (139). For several years, gradient-recalled echo MRI sequences have been used to illustrate these lesions, but dedicated susceptibility-weighted imaging may be superior (34; 44). The use of diffusion-tensor imaging or DTI may be helpful in surgical resection of brainstem cavernomas (51; 112). Pathologically confirmed lesions have an 80% to 100% radiographic correlation. High-field MRI has characterized lesions to an extent near histologic definition, detailing the unique angioarchitecture (118; 113). Dynamic contrast-enhanced perfusion MRI has been used to illustrate additional features of cavernomas such as quantitative susceptibility and permeability mapping, previously unnoted on standard MRI (59; 87; 123). The enhanced permeability may be apparent in areas remote from the cavernoma (86).
Mixed signal intensities reflect chronic lesion behavior and the hemodynamics of cavernous malformations. The spectrum of behavior of cavernous malformations ranges from quiescence to gross hemorrhage. Repeated subclinical intralesional hemorrhages lead to hemosiderin deposition secondary to erythrocyte breakdown. The reticulated low T2 signal also reflects speckled intralesional calcification. There is infiltration of macrophages laden with ferritin. The paramagnetic effects of iron appear to account for the characteristic rim of low signal intensity seen on T2 images (107; 105; 106; 97; 110). Areas of hyperintensity correspond to focal hemorrhages and different stages of thrombus organization. Associated cysts most likely represent residua of previously expanded hemorrhagic caverns, which have since involuted with thrombus organization and resolution (119).
The classic T2-weighted MR image, although characteristic, is not pathognomonic. Other lesions may manifest an indistinguishable appearance (35). The differential diagnosis should include arteriovenous malformations, mixed vascular lesions, thrombosed arteriovenous malformations, primary hemorrhagic and metastatic tumors, infectious and granulomatous diseases, and inflammatory lesions (97). Hemorrhagic primary or metastatic tumors and nonhemorrhagic tumors with melanin and fat may also confound the diagnosis. The absence of signs of a systemic neoplasm and surrounding edema, and the presence of multiple lesions, calcifications, and ossification offer clues distinguishing neoplasms from cavernous malformations and substantially increase diagnostic accuracy. Most arteriovenous malformations, with the notable exception of small thrombosed arteriovenous malformations, are readily distinguished from cavernous malformations by the presence of serpiginous signal void abnormalities, dilated arteries, and draining veins.
When epilepsy is the clinical presentation, it is critical to localize the epileptogenic zone before ascribing a cavernous malformation as the cause of seizures, particularly in patients with multiple lesions. The diagnostic workup should begin with EEG. Unfortunately, in up to 57% of cases, the study is normal or indeterminate. In order to localize the seizure foci, prolonged EEG monitoring with video monitoring should be used. Interictal and ictal SPECT or PET may be necessary to yield convergent data and enhance the accuracy and validity of the data (16; 18).
No known chemical or hematological abnormalities are associated with cavernous malformations.
Patients with cavernous malformations may be considered in distinct clinical categories that correlate with their risk of hemorrhage and neurologic disability. Each clinical scenario proposes a distinct management approach aimed at weighing treatment risk against the best estimate of the cumulative natural risk.
Asymptomatic patients with single or multiple lesions and only vague complaints, such as headache or dizziness in the absence of neurologic deficits, have a low annual risk of a first debilitating hemorrhage. There are no current data to support an aggressive approach in this group, nor in purely incidental lesions, in either sporadic or familial cases. Yet, surgical intervention for solitary lesions carries a small risk and virtually eliminates all subsequent bleeding risk from the lesions (20). It appears reasonable to follow these patients with sequential MRI. Alternatively, elective excision of readily accessible lesions may be considered in younger patients whose cumulative risk over time may not be negligible. Young patients with mild or nondisabling symptoms and solitary, accessible (usually supratentorial or cerebellar) lesions should be followed closely, with consideration of lesion excision at the first manifestation of lesion growth or an exacerbation of symptoms. Cases with less accessible lesions dictate a correspondingly higher threshold for lesion excision.
The major role of medical management in cavernous malformations is in the control of epilepsy (15). Often, the epileptogenicity may be localized to a single lesion. The clinical spectrum ranges from those patients who respond well to anticonvulsant medication, to patients with medically intractable and functionally debilitating seizures. Several studies have shown that patients with severe epilepsy given only anticonvulsant treatment had their symptoms persist unabated, with significant clinical and social disability from seizures (107; 16). It has been suggested that statins be studied for the treatment of cavernous malformation pathology (47).
It is currently agreed that accessible symptomatic cavernous malformations should be resected. The firmly established indications for surgical management are overt hemorrhage, focal neurologic symptoms, or medically intractable epilepsy. The overall results are generally favorable (Table 2). Data suggest, however, that patient-reported outcomes underscore the important role of conservative management (25).
Patients presenting with an initial bleed are at greater risk for recurrent hemorrhage. Recombinant factor VIIa has been used to stop the initial bleeding event (48). Resection of symptomatic supratentorial accessible lesions has been accompanied by a low rate of morbidity (128; 119; 107; 18; 16; 20; 21; 105; 106; 129). Favorable results have also been reported in resection of lesions, which present to a pial or ventricular surface (40; 148; 20; 90). There is no consensus whether these lesions should be excised after a first bleed or whether they should await symptom recurrence or progression (24). In a series by Kupersmith and colleagues, cavernomas of the brainstem of at least 10 mm were associated with a higher risk of bleeding episodes. Thirty-one bleeding episodes occurred in 31 patients, yielding a bleeding rate of 2.46% per year for the brainstem lesions. There were 8 re-bleeding episodes, which yielded a rate of 5.1% per year (73). Lesion accessibility clearly reflects on surgical risk (40; 20; 101; 96). Mortality risk with surgery for brainstem cavernous malformations has ranged from 0% to 20%, with transient neurologic worsening in 20% to 40%, and permanent worsening in less than 20% of cases (119; 40; 148; 20). In a series of brainstem lesions presenting with neurologic deficits that were misdiagnosed, mistreated, and not surgically treated, 70% of patients had an unremitting or fatal outcome (119). In patients with multiple lesions, only the offending lesion should be resected, and the others may be followed expectantly as with asymptomatic lesions. Hypertrophic olivary degeneration has been noted after brainstem cavernoma excision (61). Recurrences have been reported with subtotal removal and are found more commonly in less accessible and infratentorial locations. There is evidence to suggest de novo lesion genesis in certain cases (20). Advances in microsurgical anatomy have disclosed relatively safer access routes to decompress brainstem hemorrhages due to cavernomas (30).
Although much focus is placed on hemorrhagic complications, it has been demonstrated that long-term antithrombotic treatment by antiplatelet drugs or warfarin does not increase the frequency of CCM-related hemorrhage (114).
Patients with debilitating epilepsy are candidates for surgical excision of the lesion. Overall analysis of the data demonstrates improvement of symptoms in the majority of patients (57; 107; 16; 32; 142). Of groups treated with surgical resection of the offending lesion, 50% to 91% were reportedly seizure-free with or without anticonvulsant therapy (57; 40; 107; 32). Persistent seizures are reported with incomplete lesion resection. Excision of cavernous malformations should be accompanied by resection of grossly abnormal surrounding brain parenchyma, whenever possible, to enhance seizure outcome (40; 18; 16). The risk of persistent postoperative epilepsy is associated with the duration and frequency of the patient's preoperative seizures (32). In this subgroup of patients with severe intractable epilepsy, or in those where prior lesion surgery was unsuccessful, a more extensive excision of additional epileptogenic brain is recommended (18; 16; 20; 21; 32; 138).
Radiosurgery has been established as an alternative, effective treatment option for small arteriovenous malformations in eloquent and inaccessible areas (71; 69; 132). With standard dosages as used for arteriovenous malformations, cavernous malformations exhibit a poor clinical response and a high complication rate (57; 119). In a series of 16 patients (13 with a cavernous malformation alone, and 3 with a cavernous malformation associated with a venous malformation), there was no radiographic change in 80%, but 37.4% eventually developed radiation induced changes, 1 re-bled, and 12.5% had persistent neurologic deficits (121). When lower margin doses are utilized, the results may be more promising (81; 82; 31; 79; 69). One such report used doses of 12 to 16 gray for 39 deep-seated cavernous malformations, with an average follow-up of 23 months. The authors reported temporary neurologic sequelae with MR changes secondary to radiation in 10 patients (25.4%). There were 4 deaths, 2 reportedly unrelated to radiosurgery and 2 after "delayed microneurosurgery." After 15 months there were no cases of delayed hemorrhage (81; 82; 31). Even when hemorrhages occur early, recurrence markedly decreases after the first couple of years (69). These data correlate with published data on angiographically occult vascular malformations in general; clearly, the use of radiosurgery needs further investigation. In rare cases, de novo cavernous malformations have formed in response to radiation exposure (91). Radiation-induced cavernous malformations may develop within the radiation port within 12 years of initial treatment, and these lesions may be multiple with similar hemorrhagic risk (37). In particular, issues of patient selection, follow-up, long-term risks, and safe dose levels must be addressed (63). Endpoints of therapeutic success or failure have been difficult to establish in view of the variability of natural behavior of the lesions.
The results of treatment of cavernous malformations must be judged against the known natural history of the disease. We have formulated an outcome scale based on known disease-specific relevant parameters for cavernous malformations. Treatment modalities may yield an excellent, good, fair, poor, or fatal outcome (Table 1). When the outcomes of several surgical series are compared, the overall results reveal excellent to fair surgical outcomes in 83% to 100% of patients (Table 2) (46). As these are selected series with small sample sizes, heterogeneous patient populations, variable surgical intervention criteria, distinct surgical techniques, and different follow-up timeframes, there is much potential for bias in such data. Prospective, stratified, and hypothesis-driven clinical research studies are needed to objectively compare the relative outcomes of different treatments, and to better define host and lesion factors impacting on natural and treatment outcome of cavernous malformations. The BLED2 scoring system reported on multivariable analysis that yielded 4 risk factors: bleeding at presentation (HR 1.92, p = 0.048), large size >/= 12 mm (HR 2.06, p = 0.016), eloquent location (HR 3.01, p = 0.013), and duration </= 1 year since last event (HR 9.28, p = 0.002) as a prediction instrument for subsequent neurologic events (94). The 1-, 2-, and 5-year risks of a recurrent neurologic event ranged from 0.6%, 1.2%, and 2.3%, respectively, for patients with a BLED2 score of 0, to 48%, 74%, and 93%, respectively, for patients with a BLED2 score of 5. Such studies would ideally follow treated and untreated lesions, and preferably incorporate rigorous case-control or randomization methodologies. External validation of such a grading system for microsurgical treatment of cavernomas has been conducted, providing evidence for such classification schema (28).
Clinical status | |
• Excellent: no symptoms | |
Seizures or epilepsy | |
• Excellent: Seizure-free or no anticonvulsants | |
Lesion behavior or hemorrhage | |
• Excellent: Regression | |
Author and Year | Clinical outcome (% cases in reported series) | ||
Excellent | Good or fair | Poor or dismal | |
(128) | 0 | 100 | 0 |
(57) | 64.3 | 28.6 | 7.1 |
(119) | 52.2 | 39.1 | 8.7 |
(122) | 33.3 | 50 | 16.7 |
(137) | 58.8 | 29.4 | 11.8 |
(127) | 76 | 8 | 16 |
(131) | 20 | 79 | 1 |
(Includes multiple series) | 11.1 | 72.2 | 16.7 |
(107) | 57 | 33 | 10 |
(111) | 60 | 40 | 0 |
(148) |
|
|
|
• Pediatric only | 28.7 | 64.3 | 9.0 |
• Infratentorial | 77 | 23 | 0 |
| |||
Information relating to cavernous malformations and pregnancy is exceedingly scant, yet a systematic review provides some perspective (85). Case reports and clinical series document rapid growth and hemorrhage of intracranial and systemic lesions in pregnancy (107; 105; 16; 110; 99; 100; 10). The apparent propensity of women to display multiple cavernous malformations, present with gross hemorrhage, exhibit lesion predilection for certain sites, and have exacerbations of symptoms during pregnancy, as well as a reported increased prevalence of mixed and multiple lesions, suggest a dynamic hemorrhagic risk modulated by hormonal factors (10). The risk of intracranial hemorrhage from cerebral cavernous malformations is likely not changed during pregnancy, delivery, or postpartum, however (133; 120).
No published data are available, although anecdotal data suggest that patients with these lesions are at no greater risk than other patients with intracranial lesions undergoing anesthesia.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
David S Liebeskind MD
Dr. Liebeskind of the University of California, Los Angeles, received consulting fees for core lab activities from Cerenovus, Genentech, Medtronic, Rapid Medical, and Stryker.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jan. 20, 2025
Sleep Disorders
Jan. 18, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Stroke & Vascular Disorders
Dec. 29, 2024