
























General Neurology
Renal failure: neurologic complications
Jan. 28, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author explains the clinical presentation and pathophysiology of cerebral gas emboli. Cerebral gas emboli may originate from venous or arterial circulations, and the causes, pathophysiology, clinical manifestations, and prognosis differ depending on the circumstances. Iatrogenic instances from diagnostic and chest procedures were reported during the late 1800s and early 1900s, but the frequency of recognized traumatic and iatrogenic cerebral gas embolism increased dramatically after the 1970s. Iatrogenic gas embolism is associated with high mortality: one in five is dead at 1 year following the event. Independent predictors of mortality at 1 year include cardiac arrest at the time of the accidental gas embolism and admission to an intensive care unit (ICU). Among ICU survivors, independent predictors of survival at 1 year include age, Babinski sign, and acute renal failure.
|
• Neurologic manifestations are much more common with arterial than venous air emboli, and onset is immediate in the majority. With arterial air emboli, less than 1 cubic centimeter of injected air is sufficient to cause significant central nervous system or cardiac damage or even death. | |
|
• Findings may include a change in sensorium including coma; seizures or status epilepticus; focal motor (eg, hemiparesis), sensory (eg, paresthesias), or visual findings (eg, visual field deficits); dizziness; or headache. Motor focal findings are by far the most common and the most readily recognized focal neurologic manifestations of air emboli. | |
|
• Neurologic manifestations of venous air emboli may occur due to cardiovascular compromise or paradoxical embolism via a right-to-left cardiac shunt, pulmonary arteriovenous fistulas, or “overloading” of pulmonary filtering capacities. | |
|
• Air emboli are usually diagnosed clinically, rather than with diagnostic testing. Although various imaging modalities may show evidence of air or gas emboli, they may also be entirely normal in the face of severe neurologic compromise. | |
|
• Initially following cerebral gas embolism, 100% oxygen should be administered, with institution of hyperbaric oxygen as soon as possible. Clinical results can be dramatic with hyperbaric oxygen therapy especially if instituted early, but clinically evident benefits have been demonstrated in individual cases even if institution of hyperbaric oxygen therapy was delayed for several hours or even 1 to 2 days. | |
|
• Iatrogenic gas embolism is associated with high mortality: one in five is dead at 1 year following the event. Independent predictors of mortality at 1 year include cardiac arrest at the time of the accidental gas embolism and admission to an intensive care unit (ICU). Among ICU survivors, independent predictors of survival at 1 year include age, Babinski sign, and acute renal failure. | |
|
• Independent predictors of long-term sequelae include focal motor deficit and Babinski sign on ICU admission and duration of mechanical ventilation of at least 5 days. |
Human arterial air embolism was recognized as early as 1769 by Italian anatomist Giovanni Battista Morgagni (1682 to 1771), and experimental work on dogs was performed in 1878 by French zoologist and physiologist Paul Bert (1833 to 1886) (167). Iatrogenic instances from diagnostic and chest procedures were reported in the late 1800s and early 1900s (187; 167), but the frequency of recognized traumatic and iatrogenic cerebral gas embolism increased dramatically after the 1970s in large part due to the advent of computed tomography and magnetic resonance imaging (100).
Cerebral air emboli may originate from venous or arterial circulations, and the causes, pathophysiology, clinical manifestations, and prognosis differ depending on the circumstances. Other types of cerebral gas emboli are also possible but are generally rare and occur under unusual circumstances, such as inhalation of high-pressure helium from unregulated pressurized cylinders (165; 151; 216) or laparoscopic or angiographic use of carbon dioxide (186; 118; 95).
Air and gaseous embolism are becoming more common with increased use of interventional medical procedures and increased popularity of sport diving (117).
|
• Systemic manifestations with venous air emboli are primarily cardiac and respiratory. | |
|
• Cardiac manifestations include decreased cardiac output, hypotension, a so-called “mill-wheel” murmur, cardiac arrhythmias, and cardiac arrest. | |
|
• Respiratory manifestations include dyspnea, cyanosis and tachypnea, irregular gasping respirations, or apnea. | |
|
• Systemic manifestations with arterial air emboli may include sudden death, coronary ischemia, chest pain, hemoptysis, a marbled appearance to the skin, mottling of the tongue (Liebermeister sign), air in arterial aspirations, frothy blood from bleeding vessels, air in retinal arterioles, pain, and avascular necrosis. | |
|
• Neurologic manifestations are much more common with arterial air emboli and onset is immediate in the majority. | |
|
• Motor focal findings are by far the most common and the most readily recognized focal neurologic manifestations of air emboli. |
Systemic manifestations with venous air emboli are primarily cardiac and respiratory (61; 159; 250). Cardiac manifestations include decreased cardiac output; hypotension; a so-called “mill-wheel” murmur, which is a loud “splashing” murmur, secondary to outflow obstruction from the right ventricle by air with resulting hypotension and a thready pulse; cardiac arrhythmias; and cardiac arrest (61; 82; 159; 37; 250). Respiratory manifestations include dyspnea, cyanosis and tachypnea, irregular gasping respirations, or apnea (61; 250). Rarely, there may be heard a hissing sound initially as air is sucked into a vein (61).
Systemic manifestations with arterial air emboli may include sudden death, coronary ischemia with heart failure and hypotension, chest pain, hemoptysis, a marbled appearance to the skin, mottling of the tongue (Liebermeister sign), air in arterial aspirations, frothy blood from bleeding vessels, air in retinal arterioles (eg, streaming bubbles or pale silvery sections), pain, and avascular necrosis (237; 167; 121; 100; 30).
Neurologic manifestations are much more common with arterial air emboli, and onset is immediate in the majority. Neurologic findings associated with arterial or venous air emboli may include a change in sensorium, including coma, seizures, status epilepticus, syncope, focal motor (eg, hemiparesis, ataxia), sensory (eg, paresthesias) or visual findings (eg, visual field deficits), dizziness, or headache (147; 167; 01; 42; 53; 233; 200; 138; 250; 157; 218). Motor focal findings are by far the most common and the most readily recognized focal neurologic manifestations of air emboli.
In one series, among 15 patients with iatrogenic cerebral arterial gas emboli, 11 (73%) developed seizures: five prior to hyperbaric oxygen therapy, three during hyperbaric oxygen therapy, and three after hyperbaric oxygen therapy (157). With a median follow-up of 5 months, five individuals had complete neurologic recovery, five had minor neurologic deficits, two had moderate-to-severe neurologic deficits, and three had died. No patients had recurrent seizures after hospital discharge, although four still used antiepileptic drugs at last follow-up.
The prognosis depends heavily on the amount of air that enters vessels, whether the air emboli are venous or arterial, the rapidity of air injection, posture of the patient, venous pressure, and the rapidity and thoroughness of appropriate treatment.
Cerebral arterial air emboli are found frequently on postendovascular treatment CT imaging. In one retrospective study, 65 of 402 patients (16%) had at least one linear cerebral arterial air embolus in the affected MCA-territory after endovascular treatment (102). Seventeen patients (4%) showed isolated circular cerebral arterial air emboli. Multivariate models showed an association between both the presence and the number of linear cerebral arterial air emboli and the modified Rankin Scale score at 90 days. Isolated circular cerebral arterial air emboli were not significantly associated with any outcome measure.
In patients with venous catheter-related cerebral air embolism, unfavorable prognostic indicators may include the presence of gyriform air on brain CT imaging, old age, initial disturbance of consciousness, and hemiparesis (40).
Both venous and arterial cerebral air emboli may produce transient or permanent neurologic dysfunction and may be fatal (250; 15).
Case 1. Iatrogenic arterial air embolism due to management of mediatinal shift after pneumonectomy. A 69-year-old man underwent a right pneumonectomy for a right lower lobe non-small cell bronchogenic carcinoma with metastatic involvement of the mediastinal lymph nodes. Subsequently, he developed a shift of the mediastinum into the evacuated pleural cavity with decreased venous return and decreased cardiac output. A surgical resident injected air into the evacuated pleural cavity, which resulted in the return of the mediastinum toward the midline and associated clinical improvement. However, 3 hours later the procedure had to be repeated because of recurrent mediastinal shift. The resident again injected air into the right thorax, but this time the patient immediately became unresponsive, his eyes rolled upward, and he began a generalized convulsion. The resident gave several bolus injections of intravenous diazepam, but the convulsions continued for over 30 minutes. A neurology consult was called, and appropriate treatment with intravenous diazepam and phenytoin converted the generalized convulsions initially to persistent left-sided convulsions, then to intermittent seizures, and finally to no further seizures. However, the patient remained unresponsive. The neurologist diagnosed a cerebral air embolism. A CT scan of the head was obtained and showed swelling of the right hemisphere but no visible air. Hyperbaric oxygen was begun at 3 atmospheres absolute. In the hyperbaric chamber, status epilepticus returned and did not stop with a further 500 mg of intravenous phenytoin. The patient was removed from the hyperbaric chamber and had a cardiorespiratory arrest. He was revived and the status epilepticus resumed. Status epilepticus was subsequently controlled with anesthetic doses of phenobarbital. Further attempts at hyperbaric oxygen therapy were unsuccessful because of the patient’s marginal cardiovascular status. He had another cardiac arrest and died two days after the initial event.
This patient had an iatrogenic arterial air embolism with immediate and profound neurologic consequences, including coma and status epilepticus. Brain imaging showed acute structural damage with swelling of the right cerebral hemisphere. Hyperbaric oxygen therapy was instituted without apparent benefit and, in fact, was complicated by recurrent seizures, which may have been in part related to oxygen toxicity.
Case 2. Massive cerebral air embolism following percutaneous transhepatic biliary drainage. A 50-year-old woman was evaluated in the emergency room for altered mental status one week after percutaneous transhepatic biliary drainage (PTBD) (133). She had a history of gallbladder cancer (pathologic stage T2N0M0), which required cholecystectomy, liver wedge resection, and hepaticojejunostomy. Despite three courses of postoperative chemotherapy, endoscopic biopsy 8 months after the operation confirmed local recurrence in the intrahepatic duct. Follow-up abdominopelvic CT showed multiple metastases in the liver with seeding in the right subphrenic and subhepatic spaces. Because of strictures at the anastomotic site and in the biliary duct from local tumor recurrence and multiple hepatic metastases, PTBD was performed three times with biliary tract dilatation and stent placement.
On neurologic examination she was stuporous and quadriplegic. Brain CT angiography revealed extensive pneumocephali in the sulci of the right cerebral hemisphere, with air densities in the superior frontal sulcus of the left frontal lobe. Pulmonary CT angiography showed a large pulmonary thromboembolism in the left main pulmonary trunk and branches of the left pulmonary arteries. She was treated with hyperbaric oxygen therapy without evident benefit.
Initial noncontrast brain CT in a in a 50-year-old woman with recurrent gall bladder cancer shows extensive pneumocephali in the sulci of the right cerebral hemisphere with air densities in the superior frontal sulcus of the le...
Pulmonary CT angiography reveals large filling defects in the left main and left lobar (upper and lower) pulmonary arteries (arrows), consistent with pulmonary thromboembolism. (Source: Lee JH, Lee HY, Lim MK, Kang YH. Massive ...
Abdominopelvic CT showed a large necrotic mass containing air bubbles in the right hepatic lobe as well as free air and fluid in the right perihepatic and subphrenic spaces suggestive of metastatic hepatic tumor rupture. Additional findings included right portal vein thrombosis and multiple metastatic masses in the subcutaneous and muscle layers of the abdomen.
Coronal abdominopelvic CT shows a ruptured hepatic mass with free air and fluid in the perihepatic space (white arrow in upper left). (Source: Lee JH, Lee HY, Lim MK, Kang YH. Massive cerebral air embolism following percutaneou...
Axial abdominopelvic CT shows air bubbles around the biliary stent and percutaneous transhepatic biliary drainage tube (small white arrows). (Source: Lee JH, Lee HY, Lim MK, Kang YH. Massive cerebral air embolism following perc...
Diffusion-weighted brain MRI revealed multiple high-signal intensities in the right frontal, right parietal, and left frontal (superior and medial gyri) lobes, mainly in the cortex, with low-signal intensities on the corresponding apparent diffusion coefficient map. Fluid-attenuated inversion recovery (FLAIR) showed increased signal intensities with cortical swelling. Gradient-echo sequence revealed multifocal hypointense "blooming dots" in the right frontal and temporal lobes that were interpreted as probable residual air bubbles. Arterial spin-labeling perfusion imaging showed decreased blood flow in the right cerebral hemisphere and left frontal lobe. Collectively, these MRI findings were suggestive of acute infarction in the right cerebral hemisphere and left superior frontal lobe, probably due to cerebral air embolism. Magnetic resonance angiography showed no significant vascular abnormalities.
Brain diffusion-weighted MRI revealed multiple high signal intensities in the right frontal, right parietal, and left frontal (ie, superior frontal gyrus) lobes. (Source: Lee JH, Lee HY, Lim MK, Kang YH. Massive cerebral air em...
Apparent diffusion coefficient map shows the corresponding low-signal-intensity areas. (Source: Lee JH, Lee HY, Lim MK, Kang YH. Massive cerebral air embolism following percutaneous transhepatic biliary drainage: a case report....
Fluid-attenuated inversion recovery shows areas of increased signal intensity and cortical swelling, suggestive of acute infarctions. (Source: Lee JH, Lee HY, Lim MK, Kang YH. Massive cerebral air embolism following percutaneou...
Gradient-echo sequence shows multifocal hypointense "blooming dots" (arrows) in the right frontal and temporal lobes, consistent with residual air bubbles. (Source: Lee JH, Lee HY, Lim MK, Kang YH. Massive cerebral air embolism...
Arterial spin-labeling perfusion imaging shows that the cerebral blood flow is markedly decreased in the right cerebral hemisphere and mildly decreased in the left frontal lobe. (Source: Lee JH, Lee HY, Lim MK, Kang YH. Massive...
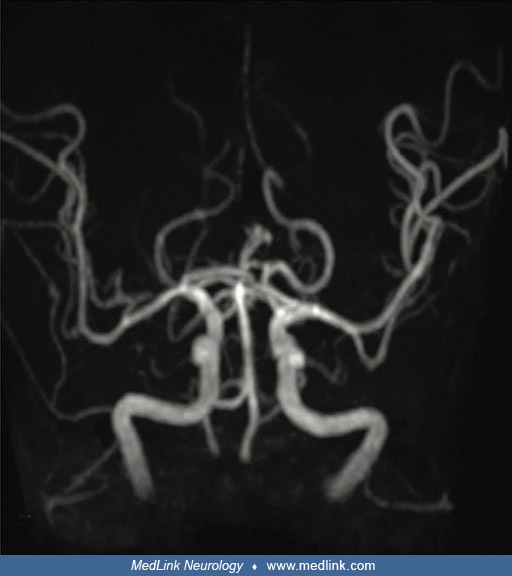
Magnetic resonance angiography shows no demonstrable steno-occlusive lesions. (Source: Lee JH, Lee HY, Lim MK, Kang YH. Massive cerebral air embolism following percutaneous transhepatic biliary drainage: a case report. Medicine...
Follow-up brain CT 12 hours later showed worsening of the right cerebral hemisphere edema with a midline shift to the left. Asymmetric enlargement of the left lateral ventricle was also observed, which was consistent with obstructive hydrocephalus. Despite vasopressor administration, her blood pressure progressively dropped. She developed progressive oliguria, metabolic acidosis, and hyperkalemia. She died 12 days after admission.
Follow-up brain CT 2 days after percutaneous transhepatic biliary drainage shows a marked increase in the extent of cerebral edema in the right cerebral hemisphere with a midline shift to the left. (Source: Lee JH, Lee HY, Lim ...
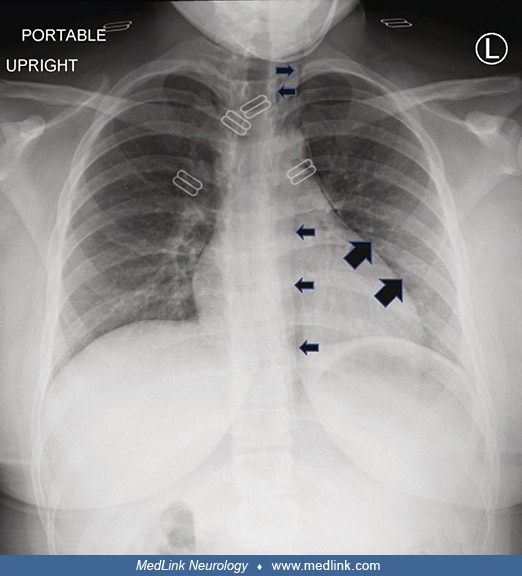
Case 3. Cerebral air embolism after pigtail catheter drainage for pneumothorax. A 50-year-old man presented with a 2-month history of productive cough and a 1-month history of blood-stained sputum (39). The patient had a history of cigarette smoking and no history of tuberculosis. A chest CT scan showed a mass in the right lower lung. Based on the history and imaging examination, lung abscess was considered, and he was treated with antibiotics for two months without a change in the size of the mass and without improvement in the right pneumonic infiltration. A right lower lobectomy was performed. The chest tube was removed on postoperative day 4, but he developed a pneumothorax. A pigtail catheter (small-bore chest tube) was inserted through a guide wire after thoracentesis to help relieve the pneumothorax. As soon as the guide wire was inserted, the man lost consciousness and developed convulsions and limb stiffness. CT scan of the brain showed multiple low densities in the right occipital lobe, indicative of cerebral gas embolism. He was not treated with hyperbaric oxygen but gradually improved and was discharged with a left hemiparesis after 27 days of treatment. At follow-up 3 months later, his left hemiparesis persisted.
Chest x-ray shows evidence of a pneumothorax after removal of a chest tube (red arrows). (Source: Chen Y, Zheng C, Zeng Q, Zhang F, Tu S, Wu Z. Cerebral air embolism after pigtail catheter drainage for pneumothorax: a case repo...
Case 4. Paradoxical and retrograde air emboli from a pressurized peripheral intravenous bolus. A 32-year-old woman was admitted to a medical intensive care unit for respiratory failure (184). Her relevant medical history included (1) intravenous heroin and cocaine abuse; (2) infective endocarditis of the tricuspid valve due to methicillin-sensitive Staphylococcus aureus on vancomycin; (3) patent foramen ovale; (4) septic pulmonary embolism with cavitation; (5) chronic ventilator dependence s/p tracheostomy; and (6) multifocal cerebral infarction. She required 100% oxygen with high positive end-expiratory pressure (PEEP 20 mmHg). Her Glasgow Coma Scale was 15 on admission. Sputum cultures and blood cultures were obtained, and she was started on broad-spectrum antibiotics. Chest CT was unremarkable for pulmonary embolism, left lower lobe collapse, and improving lung cavitation. She was evaluated for tricuspid valve and patent foramen ovale repair. Transthoracic echocardiogram showed normal ejection fraction, a dilated right ventricle, and elevated right ventricular systolic (45 mmHg) and right atrial (15 mmHg) pressures, along with severe tricuspid regurgitation with a highly mobile tricuspid valve vegetation. There was a large right-to-left shunt through the patent foramen ovale on the bubble study, with spontaneous opacification of the left atrium and ventricle. Her ventilator requirements improved on decreased PEEP at 10 mmHg, and her oxygen requirement improved to 60% as her right-to-left shunting improved.
Transthoracic echocardiography showing tricuspid valve vegetation (left, white arrow) and location of interatrial septum and patent foramen ovale (right, white arrowhead). There was a large right-to-left shunt through the paten...
On day four, she developed hypotension (78/43 mmHg). She was resuscitated with 1 liter of intravenous lactated ringers with a pressure bag into a midline peripheral access. She became unresponsive 25 minutes after the bolus, with decerebrate posturing, roving gaze, sluggishly reactive pupils, cyanosis, and persistent hypotension requiring vasopressors. After stabilization, brain CT showed diffuse arterial and venous cerebral air emboli, which were attributed to accidental administration of air with the fluid bolus. She was laid flat, and 100% oxygen was administered. She did not receive hyperbaric oxygen. Evidence of air embolism resolved by the next day on a follow-up CT scan of the brain, but her neurologic exam did not improve. On day six, her pupils were fixed and nonreactive. She was managed with hyperventilation, hyperosmolar therapy, and head elevation. Brain MRI showed findings consistent with global anoxic injury, and flattening of the globe of the eye at the optic nerve insertion was suggestive of intracranial hypertension. Given her poor prognosis, the family opted for comfort measures, and she died on the eighth day.
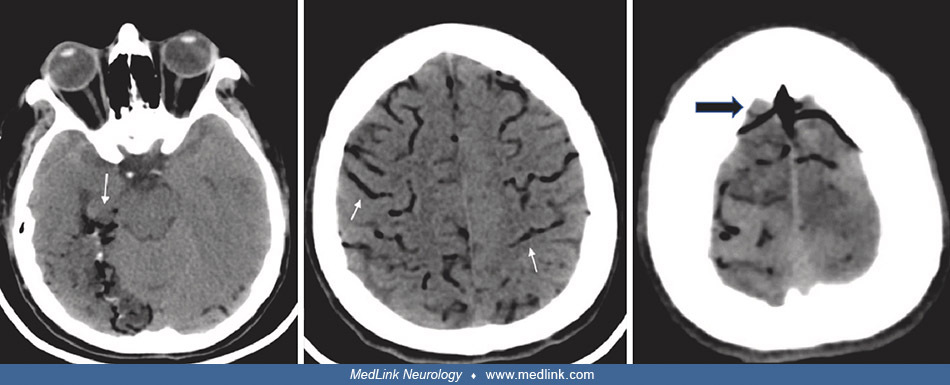
Axial brain CT showing air emboli in the cortical branches of the posterior cerebral, middle, and anterior cerebral arteries (left and center, white arrows), and air in the superior sagittal sinus and cortical veins (right, bla...
Case 5. Spontaneous (not iatrogenic) cerebral arterial air embolism due to lung cancer. A 55-year-old man underwent radiotherapy and chemotherapy for cancer in the hilum of the left lung that had come to attention because of hemoptysis (107). Although a biopsy could not be safely performed because of the cancer location, the cancer was suspected to be squamous cell carcinoma based on sputum cytology results and tumor marker levels. Six months later, he developed a severe cough, and chest CT revealed tumor growth and metastases to the left upper lobe and lymph nodes. One year after diagnosis, he was admitted with fever, chest pain, shock, and altered mental status. Chest and abdominal CT revealed that the cancer had invaded the left atrium and left main bronchus. Small low-density areas were evident on CT within the tumor and around the intestinal membrane, which were interpreted as the presence of air due to invasion of the lung cancer. Echocardiography revealed tumor invasion into the left atrium but no evidence of infective endocarditis. Staphylococcus aureus was detected in blood cultures. Septic shock was treated with a vasopressor (norepinephrine) and broad-spectrum antibiotics (meropenem and vancomycin).
The following day (day 2), he complained of difficulty in speaking and weakness in the left side of his body. Neurologic examination revealed normal alertness, left spatial neglect, left hemiparesis, and mild right leg weakness. Head CT revealed multiple small, low-density areas in the right cortex and bilateral subcortex, which were interpreted as air emboli. Head MRI revealed faint hyperintensity along the right parietal cortex, subcortex, and left frontal cortex on diffusion-weighted images and a small dot-like low signal in the right frontal cortex and left parietal subcortex on susceptibility-weighted images. These abnormalities were interpreted as cerebral air emboli associated with the invasion of lung cancer into the left atrium, causing ischemic stroke (although brain metastases associated with cancer progression were also considered).
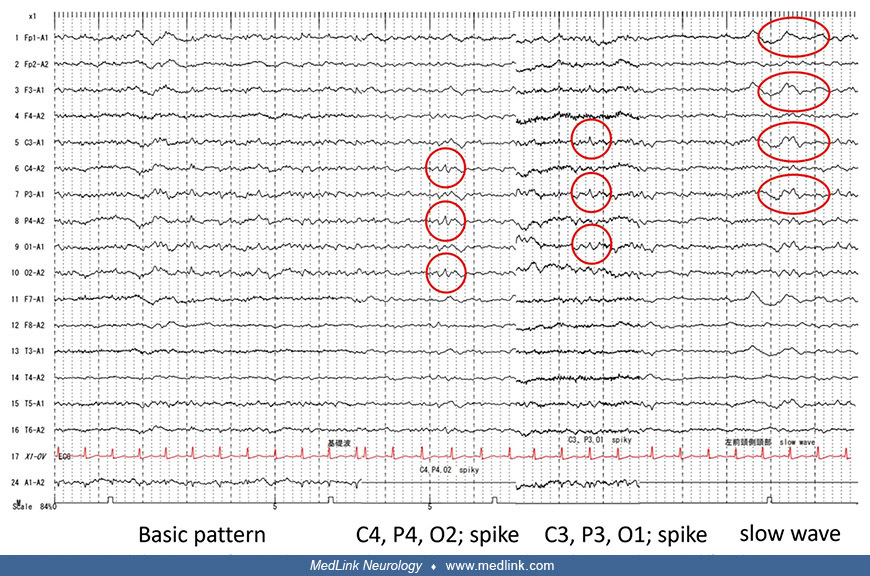
On day 3, a generalized tonic-clonic seizure occurred, lasting approximately 1 minute, and was followed by left leg twitching and right gaze deviation (gaze deviation was not likely ictal but was probably related to his large right-hemisphere lesion). Subsequent interictal EEG partial epilepsy-like waves with intermittent spikes corresponded to the bilateral central, parietal, and occipital regions and a diffuse slow-wave for the left frontal lobe. Levetiracetam was begun intravenously and followed by oral administration. He recovered from sepsis and had no further seizures. He was discharged on day 28 with residual weakness and died of hemoptysis 50 days after discharge.
Case 6. Helium emboli due to breathing from unregulated high-pressure cylinder. A 12-year-old girl inhaled helium from a high-pressure gas cylinder (155). Within a few seconds, she began coughing and quickly lost consciousness for less than 1 minute. On awakening, she was disoriented and complained of headache, chest pain, visual deficits, and weakness. She could not walk due to right-sided weakness. In the emergency room, she had sinus bradycardia and right hemiparesis as well as better than antigravity in her arm but less than antigravity in her leg. ECG showed sinus rhythm. Chest x-ray revealed pneumomediastinum and subcutaneous emphysema of the neck. CT of the brain without contrast was reportedly normal. CT angiogram of the head and neck showed a small right apical pneumothorax and subcutaneous emphysema but no abnormalities within the vasculature or brain parenchyma. She was placed on 100% oxygen via a nonrebreather mask and positioned supine. A right-sided chest tube was placed prior to transport given the concern for expansion of the pneumothorax during hyperbaric oxygen. She was flown by fixed-wing airplane to the regional pediatric tertiary center, utilizing sea level cabin pressure, and was subsequently transferred to the nearby hyperbaric center by ambulance. Hyperbaric oxygen began 6 hours and 45 minutes following helium inhalation. She received a total of 6 hours and 10 minutes of hyperbaric oxygen according to U.S. Navy Treatment Table 6, the standard protocol for arterial gas embolism. Complete resolution of neurologic deficits was noted after 90 minutes of hyperbaric oxygen. An MRI and MRA of the brain and a transthoracic echocardiogram with bubble study were normal on hospital day 3.
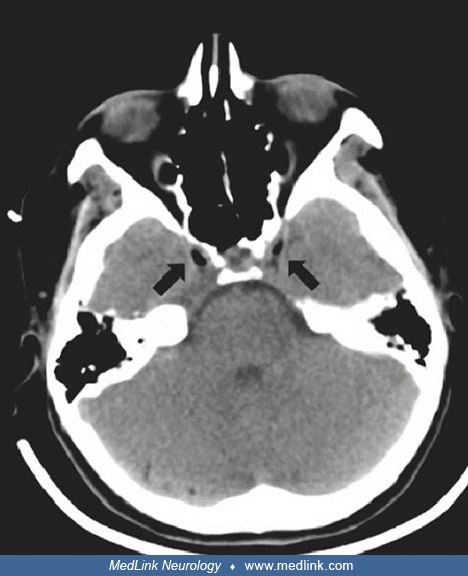
CT angiography of the head and neck shows a small right apical pneumothorax (solid arrow) and pneumomediastinum (nonsolid arrows). (Source: Morales G, Fiero M, Albert J, Di Gennaro J, Gerbino A. Cerebral arterial gas embolism d...
Case 7. Helium emboli from single breath from unregulated high-pressure cylinder. A 27-year-old male polysubstance abuser inhaled a single breath of helium from an unregulated high-pressure cylinder while intoxicated to experience the voice-altering effects of helium (151). Within seconds he became rigid and collapsed unconscious. Within about 15 minutes of the event, he was transported to a nearby emergency room. His Glasgow Coma Scale score improved from 10 to 15 over 10 minutes of treatment with oxygen through a nonrebreather mask. Once conscious, the patient complained of total blindness and central pleuritic chest pain. He had only equivocal perception of bright light, although pupils were equal and reactive and funduscopy was unremarkable (ie, no gas bubbles were observed in retinal vessels). An EKG showed tachycardia but no other abnormalities. Chest x-ray showed pneumomediastinum and right pneumothorax. He was treated with lidocaine and a series of hyperbaric oxygen treatments 6, 20, 36, and 54 hours after the accident. Diffusion-weighted MRI images obtained 17 hours after the accident (and about 3.5 hours after the first hyperbaric oxygen treatment) showed increased signal in the left temporo-occipital cortex, and smaller foci of increased signal in the right occipital cortex, considered to be consistent with patchy areas of cerebral infarction, but a second MRI 3 days after the accident showed almost complete resolution of the previous areas of increased signal intensity. When evaluated by ophthalmology 7 days after the accident, his visual acuity, color vision, visual fields, and funduscopy were all normal.
Case 8. Helium emboli from single breath from unregulated high-pressure cylinder. A 13-year-old boy inhaled helium from the nozzle of a pressurized tank at a party (165). He immediately lost consciousness and had a 10-minute generalized tonic-clonic seizure. Paramedics administered oxygen and the boy regained consciousness but was disoriented and complained of blurred vision, neck pain, and headache. Initial examination showed a spastic right hemiparesis with clonus and a Babinski sign, which improved somewhat over the 4 hours it took to transport him to a facility with hyperbaric oxygen therapy capabilities. Chest x-ray showed subcutaneous emphysema and pneumomediastinum. CT of the head was unremarkable. His deficits improved substantially after the first hyperbaric oxygen therapy, but he still had mild right arm dysmetria, right pronator drift, and impaired tandem gait. Further hyperbaric oxygen treatments 20 hours later and again 6 hours after that produced minimal further improvement, but on follow-up two weeks later, his neurologic examination was normal.
Case 9. Helium emboli due to breathing from unregulated high-pressure cylinder. A 23-year-old male singer inhaled helium from a high-pressure tank to produce a change in his voice (216). The last of eight inspirations was accidentally done without pressure reduction, and within seconds he collapsed unconscious. Within about 15 minutes of the event, he was transported to a nearby emergency room. He was drowsy and had pleuritic chest pain with deep inspiration. EKG showed ST elevations in I, AVL, and V4-V6. Chest x-ray showed pneumomediastinum and pulmonary congestion. No right-to-left shunt was evident on color Doppler echocardiography. He was treated with oxygen, aspirin, low-molecular weight heparin, and infusions of crystalloids and colloids. His EKG normalized over 30 minutes, and his CPK remained normal, but his troponin was elevated within 6 hours, indicating myocardial injury. His drowsiness gradually resolved over 10 hours.
Case 10. Cerebral oxygen gas emboli after ingesting concentrated hydrogen peroxide. A 2-year-old boy drank 4 to 6 oz of 35% hydrogen peroxide stored in the family refrigerator (which had been used to extend the shelf life of raw milk) (41). He rapidly became unresponsive and cyanotic with ineffective respiratory efforts and stiffening of the left arm. He was transported to an emergency room within 10 minutes but had a junctional rhythm on EKG with a heart rate of 35 bpm and without palpable pulses. He received appropriate cardiopulmonary support, including CPR, endotracheal intubation, and pressors. Chest x-ray showed gas in the right ventricle, mediastinum, and portal venous system. His heart rate increased to 100 bpm, pulses were detected by Doppler, and made spontaneous respiratory efforts. He was transferred by helicopter to a tertiary medical center, where he had evidence of poor tissue perfusion and his abdomen was found to be markedly distended without bowel sounds. Abdominal x-rays showed resolution of the air in the portal venous circulation, but dilated loops of small bowel. Esophagogastroduodenoscopy showed apparently normal esophagus and duodenum, but severe hemorrhagic gastritis without evident gastric perforation. The following day he developed decorticate posturing and right focal seizures. A CT scan showed a low-density lesion in the left cerebral hemisphere. Hyperbaric oxygen therapy was apparently neither considered nor attempted. He deteriorated further over the next 3 days to the point of brain death on post-procedure day 4. Autopsy showed diffuse cerebral edema with evidence of uncal and cerebellar tonsillar herniation, and superficial gastritis, but no other abnormality of the gastrointestinal system.
Case 11. Cerebral oxygen gas emboli after ingesting concentrated hydrogen peroxide. A 33-year-old female postal courier stopped at a lapidary shop on her route to obtain a drink of water (77). She mistakenly consumed the residual volume (amount unknown) in a well-marked 1-pint bottle of 35% hydrogen peroxide. Within minutes, she vomited, collapsed, and had a brief tonic-clonic seizure. She was taken to an emergency room where she was markedly cyanotic, had white foam coming from her mouth, was intermittently seizing, and had a slightly distended abdomen. Treatment included diazepam, dextrose, mechanical ventilation, gastric lavage, and activated charcoal. EKG showed sinus tachycardia. Chest x-ray showed free air below the left hemidiaphragm and a right lower lobe infiltrate consistent with aspiration pneumonitis. EGD showed mild erythema of the distal esophagus, and extensive edema and hemorrhages of the stomach mucosa. Laparotomy disclosed air bubbles in the lesser sac and along the lesser curvature of the stomach with no visible perforation or extravasation of methylene blue dye instilled in the stomach. Postoperative seizures were ultimately controlled with phenytoin. Postoperative CT of the head without contrast demonstrated bilateral cerebral edema. A pressure monitor showed an initial intracranial pressure of 30 cm of CSF, which reportedly responded to hyperventilation. The patient gradually regained alertness but had residual asymmetric quadriparesis and truncal ataxia. Hyperbaric oxygen therapy was apparently neither considered nor attempted. She was transferred ultimately to a rehabilitation facility.
Case 12. Cerebral oxygen gas emboli after ingesting concentrated hydrogen peroxide. A 64-year-old man accidentally drank a “large gulp” of 35% hydrogen peroxide that he assumed was water because it was in the refrigerator (158). He vomited “white foam,” complained of nausea and headache, began staggering, and acted confused. He was evaluated in an emergency room and was felt to be stable after two hours of observation and then discharged home. Two hours after that he developed increasing confusion and impairment of basic activities, difficulty speaking, and clumsiness in his right arm. On return to the emergency room 14 hours after ingestion, he was found to be confused and to have ataxia, as well as dysmetria and incoordination of the right arm. A diagnosis of acute cerebral gas embolism was entertained at this point and the patient was transferred to another hospital for hyperbaric oxygen therapy. With institution of hyperbaric oxygen therapy, he had rapid and complete resolution of his neurologic symptoms even though his severe claustrophobia resulted in termination of the therapy after about 50 minutes.
Case 13. Cerebral oxygen gas emboli after irrigating surgical field with hydrogen peroxide. A 54-year-old man underwent anterior cervical fusion for radicular sensory symptoms due to a herniated C5-6 cervical disc (156). After inserting an apatite dowel into the drilled hole in the vertebrae, the surgeon irrigated the surgical field with 30 ml of 3% hydrogen peroxide with resulting (and expected) formation of profuse oxygen bubbles. However, 30 seconds later, the patient’s systolic blood pressure suddenly dropped to 70 mm Hg and his oxygen saturation dropped from 99% to 90%. The patient was swiftly ventilated with 100% oxygen and placed in the Trendelenburg position. The remaining oxygen bubbles were aspirated, and the surgical field was flooded with normal saline. Systolic blood pressure increased to over 100 mm Hg and oxygen saturation increased to 99% within 1 minute. Following the procedure, the patient had no neurologic sequelae.
|
• The vast majority of air emboli occur in-hospital, of which a large proportion occur during an operation or invasive procedure. | |
|
• Vascular access procedures are most commonly associated with air embolism, with clinical signs and symptoms related to the location of the air emboli. | |
|
• Possible etiologies of air emboli include trauma, various diagnostic and therapeutic procedures (cardiovascular, vascular and endovascular, pulmonary, and gastrointestinal), other activities (eg, rapid decompression or barotraumas in flying or diving and some forms of orogenital sex), and angioinvasive cavitary aspergillosis infections. |
The vast majority of air emboli occur in-hospital (94%), of which a large proportion (78%) occur during an operation or invasive procedure (142). Vascular access procedures are most commonly associated with air embolism, with clinical signs and symptoms related to the location of the air emboli (eg, right heart/pulmonary artery, cerebrum).
The possible etiologies of air emboli are varied and include the following (not all mutually exclusive categories) (226; 250; 10; 63; 64; 85; 122; 242; 150; 67; 02; 21; 128; 130; 220; 13; 75; 79; 111; 231; 05; 47; 88; 95; 135; 96; 133; 184; 206; 06; 23; 107; 109; 110; 154; 183; 188; 196; 207; 247; 190; 194; 196; 205; 30; 45; 222; 248):
|
Trauma | ||
|
• Trauma or blunt injury (especially with the heart gravitationally below an injured great vessel) (230) | ||
|
Cardiovascular, vascular, and endovascular procedures | ||
|
• Carotid endarterectomy | ||
|
Pulmonary procedures | ||
|
• Thoracentesis or chest tube placement | ||
|
Gastrointestinal procedures | ||
|
• Complication of esophagogastroscopy or esophagogastroduodenoscopy (190) | ||
|
Other surgical operations and medical procedures | ||
|
• Various obstetric and gynecologic procedures, including cesarean section, especially when done in Trendelenburg position (as a result of air intravasation through uterine veins) | ||
|
Other | ||
|
• Pressurized peripheral intravenous bolus when the line is inadequately primed | ||
|
- Angioinvasive cavitary aspergillosis | ||
|
• Rapid decompression or barotraumas in flying or diving (12; 153) | ||
Following cardiopulmonary resuscitation for nontraumatic cardiopulmonary arrest, cerebral gas embolism is demonstrated in about 8% of cases on postmortem computed tomography, with cerebral arterial emboli evident in approximately 10% of these, presumably due to pulmonary barotrauma and/or paradoxical embolism (195).
A variety of cases of non-air gas emboli have been reported with serious sequelae with such gases as helium, oxygen, and carbon dioxide. For example, helium emboli may occur from ruptured helium-filled intra-aortic balloon pumps used for counterpulsation (71; 227; 69), and cerebral carbon dioxide emboli may occur during laparoscopic cholecystectomy (81; 186), hysteroscopy (81; 76; 161; 118; 135), carbon dioxide pneumoperitoneum in laparoscopic surgery (249), or carbon dioxide angiography (95).
Carbon dioxide has been used as a contrast agent since the 1920s for visualization of retroperitoneal structures (95). In the 1980s carbon dioxide was applied as a contrast agent for digital subtraction angiography (95). Carbon dioxide angiography is still used as an alternative contrast agent in patients with chronic kidney disease and those at risk of developing contrast-induced nephropathy (95). However, inadvertent carbon dioxide entry into cerebrovascular circulation during angiography can cause fatal brain injury (95). Therefore, CO2 angiography in blood vessels above the diaphragm is best avoided.
Cerebral arterial gas embolism can occur from inhalation of pressurized helium (165; 151; 216; 155; 219). Adolescents, young adults, and some singers may intentionally inhale high-pressure helium for entertainment or to produce a change in their voice. Inhaled high-pressure gas can produce high transpulmonary pressure sufficient to rupture alveoli and surrounding blood vessels, introducing gas into the pulmonary veins and allowing systemic embolization through the left heart. Secondary cardiac and brain ischemia are common in such circumstances; particularly in an upright person (eg, inhaling gas from a high-pressure cylinder), pulmonary venous gas is likely to enter the cerebral circulation as it is transported through the left heart and across the aorta.
Hydrogen peroxide is an oxidizing agent, which in the most common household form (ie, 3% concentration) is variously used to bleach hair and as an antiseptic for minor skin lesions. Industrial-strength hydrogen peroxide is sold at 35% concentration and is highly toxic when ingested (134). Hydrogen peroxide is a fairly common cause of exposures reported to poison control centers, with 325 such exposures reported to a single poison control center over a 3-year period (50). Ingestion of hydrogen peroxide is particularly common in children, and with hydrogen peroxide left in easily accessible locations (eg, a refrigerator) or stored in improperly labeled containers (eg, a water bottle or a wine bottle). More than two thirds of such exposures occur in the pediatric population (< 18 years of age) and most are due to ingestion. Less common routes of exposure are ocular or dermal, and rarely parenteral (as in intravenous administration in attempted suicides or inadvertent use by intravenous drug users). Exposures to household concentrations (ie, 3%-5%) are usually benign, with nausea, vomiting, and mild abdominal bloating the most common symptoms with ingestion (103; 50; 21). More severe outcomes (including severe burns of the oropharynx and gastrointestinal tract, central nervous system dysfunction, and death) are increasingly likely with ingestion of hydrogen peroxide at concentrations greater than 10% (78; 103; 170; 224; 233; 174). Ingestion of concentrated hydrogen peroxide causes severe gastric irritation and produces large volumes of oxygen gas, which can result in venous oxygen embolization and even rupture of a portion of the alimentary tract (34). Because each 1% hydrogen peroxide is equivalent to 3.3% oxygen by volume, 1 ml of 3% hydrogen peroxide will release 10 ml of oxygen gas in a tissue reaction, whereas 1 ml of 35% hydrogen peroxide will release almost 120 ml of oxygen gas.
Because hydrogen peroxide decomposes immediately into water and oxygen on contact with organic tissue containing the enzyme catalase, it has been considered a safe agent for cleaning and irrigating wounds. However, serious complications can occur, including massive cerebral gas embolism (192; 191; 17; 189; 198; 217; 156; 233; 163; 166; 253; 254; 245). When hydrogen peroxide is ingested, or when it is used therapeutically in closed or semi-closed body cavities or areas of abnormal tissue breakdown, oxygen emboli can form in surrounding vessels and disrupt blood flow to tissues, causing serious neurologic sequelae (eg, seizures, cerebral ischemia) and death (166; 199; 115).
Venous air emboli can produce a variety of systemic manifestations, for example by obstruction of blood flow through the heart (“air lock”), acute pulmonary hypertension, and pulmonary edema. Neurologic manifestations of venous air emboli usually require at least 2 cubic centimeters of air and perhaps 30 to 100 cubic centimeters, depending on the rate of injection and other factors (61; 100).
In animal experiments (using pigs), an open chest and pericardium facilitated the transpulmonary passage of venous air emboli (204).
Neurologic manifestations of venous air emboli may occur due to cardiovascular compromise or paradoxical embolism via a right-to-left cardiac shunt, pulmonary arteriovenous fistulas, or “overloading” of pulmonary filtering capacities (201; 167; 141; 01; 241; 18; 212; 214; 252; 100; 93; 101; 159; 209; 246; 04; 127; 229; 168; 48; 62; 10; 64; 242; 06).
Right-to-left cardiac shunts occur with patent foramen ovale or congenital heart disease (84; 241; 127; 229; 70). Patent foramen ovale is reported in 17% to 35% of the population and ranges in size from 1 to 19 mm with a mean of 5 mm (three fourths are between 2 and 6 mm, and the vast majority are between 1 and 10 mm) (84; 100). A paradoxical embolus through a patent foramen ovale requires that right atrial pressure is greater than left atrial pressure (at least intermittently). Venous air emboli may increase right atrial pressure up to 10-fold. Other factors that may increase right atrial pressure include pulmonary embolus secondary to deep venous thrombosis, positive end expiratory pressure, coughing, Valsalva maneuver or crying in the neonate, pulmonary hypertension, chronic obstructive pulmonary disease, and congestive heart failure (100).
Pathway of air emboli paradoxically traveling from the right atrium across an intracardiac shunt (eg, patent foramen ovale) into the left atrium and subsequently into the left ventricle and aorta before entering the carotid and...
Pulmonary arterioles and capillaries are generally considered an effective filter for thrombi, platelet aggregates, and fat emboli, but they may be less effective for trapping air, especially with bolus injections (60; 33). Furthermore, pulmonary arteriovenous fistulas are not uncommon and may be up to 300 microns in size, and some medications (eg, aminophylline, vasodilators, and anesthetic agents) may act to “open up” latent pulmonary arteriovenous fistulas, providing a noncardiac shunt and, thus, an alternate route for paradoxical emboli (61; 167; 159). Patients with cirrhosis may have multiple small pulmonary arteriovenous fistulas (167).
It is also possible for cerebral venous air emboli to ascend directly through the right atrium to the superior vena cava and then to the jugular vein, against the opposing blood flow in an upright patient. This may be facilitated by the lack of valves in the jugular veins and small bubble size relative to the jugular veins as well as in situations of increased intrathoracic pressure. Alternatively, the gas may take a more circuitous route when there is significant tricuspid regurgitation. Severe tricuspid regurgitation may drive retrograde pressure into the superior vena cava and then the jugular veins (184).
Air travels in a retrograde fashion due to severe tricuspid regurgitation forcing air back into the superior vena cava where it ascends into the jugular veins and intracranial venous structures. (Source: Santucci J, Mullaguri N...
With arterial air emboli, less than 1 cubic centimeter of injected air is sufficient to cause significant central nervous system or cardiac damage or even death (61; 01; 100).
Several pathophysiologic mechanisms contribute to cerebral damage in patients with air emboli: mechanical blockage of blood flow in the heart secondary to air lock or cardiac ischemia, mechanical blockage of blood flow in cerebral vessels (particularly the smaller 30 to 60 μm end arteries at the cortical-white matter junction), vasospasm, development of platelet thrombi as a result of activation of platelets by the blood-gas interface, damage to the endothelium with secondary margination and activation of monocytes, activation of inflammatory reactions, hemoconcentration, abnormal vascular permeability and development of cytotoxic and vasogenic edema, small hemorrhages, and loss of vascular autoregulation (167; 01; 94; 152; 210).
Very limited information is available on the epidemiology of cerebral arterial gas embolism, most of which is anecdotal and from case series of particular procedures.
The diagnosis is often straightforward if there is a reasonable degree of clinical awareness, particularly during certain invasive vascular procedures or neurosurgical procedures done in the sitting position (129). At a head elevation angle of 36 degrees, the probability of venous air embolism is 50% (129). In some cases, though, clinicians may attribute manifestations to other factors such as thromboemboli or metabolic derangements. Failure to recognize the manifestations of air emboli delays appropriate therapy and may adversely affect the prognosis.
|
• Air emboli are usually diagnosed clinically rather than with diagnostic testing. | |
|
• Several diagnostic tools can detect intracardiac or cerebral air, including plain x-rays, transesophageal echocardiography, chest CT angiography, transcranial Doppler, CT, or MRI. | |
|
• With cerebral gas emboli, CT may be normal or may show multiple small areas with air density in the cerebral hemispheres, air within cerebral vessels (eg, as negative density serpiginous streaks producing casts of cerebral arteries), multiple enhancing low-density areas consistent with infarction, watershed infarctions, and cerebral edema. | |
|
• Ingestion of hydrogen peroxide should be strongly considered in patients presenting to an emergency room with white foam on the lips and abdominal distention, particularly in young patients with sudden cardiac failure or arrest or acute neurologic symptoms. |
Air emboli are usually diagnosed clinically, rather than with diagnostic testing. Several diagnostic tools can detect intracardiac or cerebral air, but they may not be necessary to confirm systemic air embolism. These diagnostic technologies include plain x-rays, transesophageal echocardiography, chest CT angiography, transcranial Doppler, CT or MRI (237; 105; 228; 92; 113; 42; 11; 99; 197; 193; 178; 03; 08; 119; 171; 239; 123; 93; 127; 182; 59; 44; 223; 37).
Chest x-ray, chest CT, or chest CT angiography may show air in the heart or great vessels, as well as pneumohemothorax, pneumatocele, interstitial emphysema, infiltrates, or contusion (100). Similarly, skull x-ray may show air in the cerebral circulation or brain (237). Transesophageal echocardiography can detect gas bubbles as small as 2 micrometers in diameter (100).
Immediate head CT is the imaging technique of choice for suspected cerebral gas embolism. With cerebral gas emboli, CT may be normal or may show multiple small areas with air density in the cerebral hemispheres, air within cerebral vessels (eg, as negative density serpiginous streaks producing casts of cerebral arteries), multiple enhancing low-density areas consistent with infarction, watershed infarctions, and cerebral edema (105; 228; 92; 113; 42; 11; 99; 197; 80; 03; 08; 171; 236; 239; 123; 93; 127; 182; 59; 223; 124; 114; 32; 68). The use of thin-slice (thickness of 5 mm or smaller) CT and the measurement of air attenuation coefficient can reduce false-negative studies (29).
CT perfusion may show specific perfusion defects in patients with a clinical diagnosis of cerebral artery gas embolism, which suggests that CT perfusion may be supportive in diagnosing cerebral artery gas embolism in cases where no intracerebral gas is seen on noncontrast CT (66).
MRI may also be normal or may show focal or patchy hyperintensities and other evidence of ischemic cerebrovascular lesions (106; 173; 236; 185; 37; 114; 174). Air can sometimes be visualized on T2-weighted gradient echo images as multiple hypointense lesions in the bihemispheric corticomedullary junction (114). Multiple, bihemispheric cortical areas of restricted diffusion in a gyriform pattern on diffusion-weighted magnetic resonance imaging can occur with venous gas emboli that are small enough to be filtered through the lungs (37). Normal initial brain imaging does not exclude a diagnosis of cerebral air embolism, and if cerebral air embolism is clinically suspected, brain imaging should be repeated in 48 to 72 hours (197; 239; 162; 249).
Transcranial Doppler ultrasonography is a noninvasive technique that can detect minute cerebral air emboli, particularly during procedures, including cardiac procedures and carotid endarterectomy (164; 202; 225; 52; 73; 139; 31; 72; 132). Typically, the right middle cerebral artery is monitored as it supplies approximately 80% of the hemisphere, and during open heart surgery air emboli are more likely on the right than the left.
Imaging workup of a patient with symptoms of paradoxical emboli usually starts with CT and MRI to identify the cause of the symptoms and any thromboembolic complications in target organs (eg, stroke, peripheral arterial occlusion, visceral organ ischemia). Echocardiography is necessary to identify cardiac shunts, and additional techniques (eg, transcranial Doppler ultrasonography, CT angiography, MR angiography) are necessary to identify extracardiac shunts (eg, pulmonary arteriovenous malformations). Acutely, hemodynamic evaluation with point-of-care ultrasound (POCUS) may show bubbles in both right and left heart cavities in cases of paradoxical emboli (179).
In cases with seizures, electroencephalography may show focal spike activity and diffuse slow waves (107).
Ingestion of hydrogen peroxide should be strongly considered in patients presenting to an emergency room with white foam on the lips and abdominal distention, particularly in young patients with sudden cardiac failure or arrest or acute neurologic symptoms.
In fatal diving accidents, postmortem computed tomography studies can easily detect intra- and extra-vascular gas collections (47). Postmortem computed tomography is very useful in the detection of macroscopic gas collections in the body whereas microscopic gas collections identified at autopsy can aid in the differentiation between decompression sickness and pulmonary barotrauma followed by vascular gas embolism. These results may have wider application in in assessing the cause of death in fatalities when gas embolism is a possible cause or contributor to death.
|
• Supportive therapy is critical following an air embolism and may include positioning, administration of 100% oxygen, initial manual and then mechanical ventilation, cardiopulmonary resuscitation or cardiac massage if necessary, aspiration of air from the right heart, intraoperative retrograde cerebral perfusion if feasible, deep barbiturate anesthesia, surface hypothermia, enhanced cardiac output, administration of vasopressors if blood pressure remains low, and aggressive management of cerebral edema. | |
|
• Seizures should be treated with diazepam or lorazepam in addition to phenytoin. | |
|
• Clinical results can be dramatic with hyperbaric oxygen therapy especially if instituted early. | |
|
• Complications of hyperbaric oxygen therapy include complications related to oxygen toxicity, which may include seizures, pulmonary problems, and bradycardia. |
Supportive therapy is critical following an air embolism and may include positioning to minimize dissemination of air and facilitate its removal, administration of 100% oxygen until hyperbaric oxygen can be arranged, initial manual and then mechanical ventilation (preferably with high-frequency ventilation and small ventilatory volume), cardiopulmonary resuscitation or cardiac massage if necessary, aspiration of air from the right heart, intraoperative retrograde cerebral perfusion if feasible, deep barbiturate anesthesia, surface hypothermia, enhanced cardiac output, administration of vasopressors if blood pressure remains low (and even in consideration of supranormal blood pressure), and aggressive management of cerebral edema (61; 149; 42; 177; 197; 148; 07; 215; 100; 101). Seizures should be treated with diazepam or lorazepam in addition to phenytoin (167; 234; 215). Phenobarbital or thiopental are effective in treating intractable seizures or status epilepticus in such cases (215). Antiplatelet agents (especially aspirin), anticoagulation, mannitol, and steroids have also been recommended by some authors (232; 167; 215), but all are of unproven benefit and, in some cases (eg, anticoagulation, prophylactic mannitol, and administration of high-dose steroids), controversial (159). Some animal studies support the use of heparin (180; 159), lidocaine (143; 57; 159), and doxycycline (172) but not dexamethasone (58).
The optimal positioning of the patient depends somewhat on clinical circumstances and remains controversial (43; 159). Positioning the patient with the head down and in the left decubitus position keeps venous air from proceeding across a patent foramen ovale or into the pulmonary vasculature (61; 82; 43) and may help in removing the obstruction to blood flow in the heart by positioning the right ventricular outflow tract inferior to the right ventricular cavity (so that air migrating superiorly will not block outflow) (56; 43). It can also be helpful in patients with inadvertent injection of air into the aorta during angiography (126). Such positioning also increases venous return, increases central venous pressure, distends subclavian veins to facilitate insertion of a subclavian line for aspiration of air from the right ventricle, and enhances retrograde flow of bubbles from cerebral arteries (61; 82; 43). However, in some studies, hemodynamic responses were not improved by the use of left lateral decubitus position with the head tilted downward (145; 74; 159). Furthermore, Trendelenburg head positioning in conjunction with cardiac de-airing showed no greater decrease in cerebral microemboli than horizontal head positioning (159; 176).
Initially, 100% oxygen should be administered, with institution of hyperbaric oxygen as soon as possible (208; 35; 243; 89; 16; 137; 160; 27; 108; 90; 42; 46; 55; 83; 09; 36; 131; 136; 24; 125; 240; 49; 175; 158; 100; 159; 98; 25; 238; 20; 146; 116; 174; 213; 26; 112; 34; 199). If transport is necessary for hyperbaric oxygen therapy, it is preferable that this be done via ground transportation or low-flying helicopter rather than via an unpressurized plane. Although animal studies have suggested that hyperbaric oxygen therapy must be administered within two hours of cerebral gas embolism in order to have a positive impact on cerebral function (235), hyperbaric oxygen may be useful in affected people even if delayed for more than 24 hours and sometimes as much as 72 hours (86; 42; 55; 09; 181; 24; 49; 100; 238; 199).
Even with clinical improvement or resolution of symptoms following oxygen treatment and positioning, patients may secondarily deteriorate, necessitating emergent hyperbaric oxygen therapy (218).
For treatment to be maximally successful, appropriate treatment measures must be initiated almost immediately, requiring a medical team that is well-prepared to recognize and manage such incidents. Prompt appropriate management of venous gas emboli can avert or minimize complications (19). The factor that is most clearly associated with good neurologic outcome is time to first hyperbaric oxygen therapy: better neurologic outcome is associated with hyperbaric oxygen therapy within 8 hours of cerebral gas embolism (19; 221). Unfortunately, appropriate treatment of cerebral gas emboli with hyperbaric oxygen is often impeded by delays in diagnosis and subsequent transfer of patients to a hyperbaric unit (19).
Hyperbaric oxygen has several mechanisms of potential benefit for treating air emboli (100; 97; 211). First, it helps decrease tissue hypoxia; because hemoglobin is largely saturated while breathing room air, the excess oxygen is carried mainly as dissolved oxygen in plasma. Second, hyperbaric oxygen increases the diffusion gradient of nitrogen out of the body (air bubbles in emboli are approximately 80% nitrogen). Third, hyperbaric oxygen decreases the size of the air bubbles in vessels, which reduces their mechanical obstructive effect and facilitates their reabsorption. By Boyle’s law, the volume of a gas is inversely proportional to pressure (at constant temperature). Thus, at 3 atmospheres of pressure, the relative volume of a bubble will be only a third of its volume at 1 atmosphere, and its surface area will be only half of its surface area at 1 atmosphere. Advantages of decreased air bubble size include faster resorption, decreased area of obstruction within blood vessels, decreased turbulence, decreased surface area, decreased acute inflammation, and decreased platelet aggregation caused by blood-bubble interaction (28). Fourth, hyperbaric oxygen helps to decrease cerebral edema and associated increased intracranial pressure, in part through vasoconstriction.
Clinical results can be dramatic with hyperbaric oxygen therapy especially if instituted early (221), but clinically evident benefits have been demonstrated in individual cases even if institution of hyperbaric oxygen therapy was delayed for several hours or even 1 to 2 days. For hyperbaric oxygen therapy to be useful, however, the clinical manifestations of cerebral arterial gas emboli have to be recognized and dealt with appropriately by clinicians. Even in iatrogenic cases where cerebral arterial gas embolism is or should be suspected early, hyperbaric oxygen therapy is not consistently applied and unfortunately many such cases die or are left with severe neurologic residua.
Monoplace hyperbaric chambers require fewer medical personnel to operate them than do multiplace chambers. They also present no significant hazard to medical personnel; they allow rapid access to the patient and removal of the patient if necessary; they are more widely available; and with 100% oxygen, they probably can administer a greater partial pressure of oxygen. Multiplace chambers allow administration of greater pressures, which help to maximally decrease the volume and surface area of bubbles. However, there is no significant increased benefit after 6 atmospheres of air (corresponding to 1.2 atmospheres of oxygen), and there are more frequent complications of treatment (144).
Complications of hyperbaric oxygen therapy include complications related to oxygen toxicity, which may include seizures, pulmonary problems, and bradycardia (203; 51). Generalized tonic-clonic seizures develop in normal individuals exposed to 4 atmospheres of oxygen for more than 45 minutes. Acute neurologic insults and steroids further lower the seizure threshold for oxygen toxicity. If oxygen-toxicity-related seizures develop during hyperbaric oxygen therapy for air emboli, hyperbaric oxygen can be discontinued, or the partial pressure of oxygen can be decreased, and anticonvulsants should be administered. Diazepam may provide some prophylactic benefit. Hyperbaric oxygen therapy rarely may also cause barotrauma and resulting air embolism (244).
With hyperbaric oxygen therapy administered promptly following iatrogenic cerebral gas embolism, 80% to 90% get full or partial relief, and the remaining individuals get no relief or die (19). Prognostic factors include the time delay to initiation of hyperbaric oxygen treatment, the amount of air injected, and the presence of hemiplegia as the first presenting sign (211; 19; 65): delays of 8 hours or more before the first hyperbaric oxygen therapy, larger volumes of air injected, and presence of hemiplegia on presentation are associated with poor outcomes (211; 19). A meta-analysis of studies of hyperbaric oxygen therapy for cerebral arterial gas embolism (10 studies, 263 patients) showed that patients with favorable outcomes were treated with hyperbaric oxygen therapy on average 2.4 hours earlier than patients with unfavorable outcomes (65). In the same study, a multivariate model (eight studies, 126 patients) showed a significant relationship between time to hyperbaric oxygen therapy and the probability of a favorable outcome that remained significant after correcting for the severity of adverse manifestations of cerebral arterial gas embolism (65). Probability of favorable outcome decreased from approximately 65% when hyperbaric oxygen therapy was started immediately, to 30% when hyperbaric oxygen therapy was delayed for 15 hours (65). Cardiopulmonary symptoms are significantly more common in association with a venous rather than arterial source of gas but do not influence the rate of favorable outcomes of hyperbaric oxygen therapy (211).
Several factors affect the risk of complications of air emboli, particularly with venous air embolism. First is the amount of injected air and the speed of injection. Small amounts of air injected slowly into the venous system may be adequately filtered by the lungs, but larger amounts injected rapidly may produce a deficit. Even a small amount of air (ie, less than 1 cubic centimeter) injected into the arterial system may cause clinical deficits.
The second factor to be considered is venous pressure and the effects of posture during surgical procedures. Right atrial pressure is approximately zero in the erect posture. Veins above the right atrium generally collapse because of negative pressure and thin walls. However, negative pressure also develops in noncollapsible venous channels, especially the diploic veins in the skull and the cerebral venous sinuses (61). As a result, there is considerable risk of performing neurosurgical procedures in the sitting position, as with surgery for acoustic neuromas, for example (87; 61; 104; 251; 240; 91; 214; 54; 169). Preoperative contrast echocardiography should be performed to exclude a patent foramen ovale, which increases the risk of paradoxical embolism and should be considered a contraindication to surgery in the sitting position (169). Several techniques during surgery help to avoid or minimize the risk of venous air emboli under such circumstances, including waxing bone edges, cauterizing visible veins, flooding the surgical field with saline, increasing venous return (for example, with pressure stockings), and avoiding spontaneous respirations (as there is increased negative venous pressure with inspiration) (61). A similar situation occurs with Trendelenburg positioning of patients undergoing pelvic surgery.
The third factor that can help reduce the risk of complications of air emboli is close attention to proper technique with invasive vascular or pulmonary invasive diagnostic or therapeutic procedures. For example, the patient should be in the head-down position prior to venipuncture for a central line (and also supine or in slight Trendelenburg position prior to removal); the needle should always be kept closed with the stylet or the operator’s gloved finger; connections on all tubing should be maintained; and the entry (or exit) site should be covered with an air occlusive dressing (82; 167; 148; 38; 159). To minimize air emboli during angiography, contrast media should be allowed to stand prior to injection, and catheters should be flushed slowly with saline (140).
And finally, prophylactic treatment with hyperbaric oxygen therapy can be considered in certain situations, for example when there was inappropriately rapid decompression, or when there was an indication of air embolism during open heart surgery (even before neurologic manifestations of cerebral ischemia occur) (125).
Iatrogenic gas embolism complicates approximately 3 per 100,000 hospitalizations and is associated with high mortality (one in five are dead at 1 year following the event) and high morbidity (22; 150). Independent predictors of mortality at 1 year include cardiac arrest at the time of the accidental gas embolism and admission to an intensive care unit (ICU) (22). Among ICU survivors, independent predictors of survival at 1 year include age, Babinski sign, and acute renal failure (22). Independent predictors of long-term sequelae include focal motor deficit and Babinski sign on ICU admission and duration of mechanical ventilation of at least 5 days (22).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
General Neurology
Jan. 28, 2025
General Neurology
Jan. 23, 2025
General Neurology
Jan. 20, 2025
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025