








Stroke & Vascular Disorders
Neoplastic and infectious aneurysms
Dec. 29, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Cerebrovascular insufficiency, typically caused by extra- or intracranial steno-occlusive disease, remains the leading cause of ischemic stroke. The management of various types of stenosis varies according to the chronicity and symptomatic presentation of the patient. Mechanical thrombectomy has emerged as the standard of care for treating acute occlusions of the carotid or large intracranial vessels. For chronic extracranial occlusion, surgical options can range from carotid endarterectomy to transfemoral or transcarotid stent placement. Intracranial steno-occlusive disease due to intracranial atherosclerosis is often addressed through antiplatelet therapy. Surgical interventions are reserved for cases where initial medical management proves ineffective. These options may include extracranial-to-intracranial (EC-IC) bypass and endovascular angioplasty with or without intracranial vessel stenting. This updated article delves into the etiologies of various cerebrovascular insufficiencies and provides insights into surgical options and techniques.
|
• Cerebrovascular insufficiency is a leading cause of ischemic stroke. | |
|
• Management of cerebrovascular insufficiency depends on the chronicity and symptomatology of the patient. | |
|
• Mechanical thrombectomy has become the standard of care for acute carotid and intracranial large artery occlusion. | |
|
• Chronic or asymptomatic cerebrovascular insufficiency may be managed medically, but symptomatic lesions or lesions refractory to medical management may require surgical or endovascular revascularization. |
Descriptions of early attempts at surgical embolectomy for the treatment of brain ischemia appeared in the literature in the 1950s (117; 27). Microsurgical reconstruction of brain arteries, ie, cerebral bypass surgery, became available following the introduction of the operating microscope in the 1960s (122). Indications for intracranial revascularization procedures have subsequently been refined, and surgical techniques have considerably evolved over the following decades.
The association between extracranial carotid pathology and ipsilateral ischemic stroke was recognized in the early 1900s (24; 66), and carotid endarterectomy for stroke prevention was introduced only in the second half of the 20th century (38; 48). There was an exponential growth in the application of carotid endarterectomy for treating carotid atherosclerotic disease, with more than 30,000 carotid endarterectomies being carried out annually in the United States by the 1980s.
Endovascular cerebral revascularization began with the introduction of percutaneous dilating angioplasty in the 1960s (41). A decade later, percutaneous transluminal angioplasty was adopted (57). Carotid artery stenting became available in the mid-1990s (40). Stents have since been used in nearly every segment of the cerebral circulation and for various indications.
Intraarterial installation of thrombolytic drugs directly into the occluding thrombus for the urgent revascularization of patients suffering from cerebral artery occlusions became available in the 1980s (125; 126). However, intra-arterial thrombolysis remained limited by its comparatively low ability to re-establish flow, which contributed to the development of endovascular mechanical thrombectomy. Initially, the occluding particle was retrieved using various types of snares. However, snares were technically challenging to use and were, therefore, progressively replaced by more trackable and more efficient devices, so-called stent retrievers (49). Although first-generation stent retrievers allowed an increase in recanalization rates, their ability to improve functional outcomes in patients suffering from large cerebral artery occlusions remains unproven (109; 14; 15). The turning point for mechanical thrombectomy occurred in 2015 when five multicenter, open-label randomized controlled trials (MR CLEAN, ESCAPE, SWIFT PRIME, EXTEND-IA, and REVASCAT) unequivocally demonstrated that mechanical thrombectomy with second-generation stent retriever devices was superior to standard treatment with intravenous thrombolysis alone for large-vessel, anterior circulation occlusions (10; 18; 53; 70; 104). Since then, indications for mechanical thrombectomy have continued to expand, and clot retrieval techniques, as well as devices, continue to be refined.
General concepts. Atherosclerosis is the primary cause of cerebrovascular insufficiency. Nonatherosclerotic etiologies include various types of inflammatory disease as well as trauma. Generally, any lesion capable of producing cerebrovascular insufficiency, with or without ischemia or infarction, does so by a combination of distinct attributes, each with its own pathogenic implications (Table 1).
|
Attribute |
Defining criterion |
Influencing variables |
|
Hemodynamic impact |
Degree of bulk flow alteration downstream from the lesion |
Degree of stenosis |
|
Emboligenicity |
Propensity of the lesion to generate thromboembolism |
Endothelial integrity |
|
Branch involvement |
Involvement of arterial branches by the lesion, through extension or embedment |
Competing target tissues |
Hemodynamic impact. The hemodynamic impact of a stenotic lesion depends on the reduction of bulk flow in the affected artery and, consequently, the reduction of perfusion in its vascular bed. From a clinical point of view, the patient may remain asymptomatic, may suffer from hypoperfusion symptoms, or may develop ischemic stroke. The appearance of clinical manifestations depends on factors such as metabolic needs of the concerned territory or competence of collateral circulation.
The flow of fluids through a tubular entity such as a cerebral artery can be approximated by Poiseuille’s Law, which states that the flow depends on the viscosity of the fluid, the pressure gradient along the tube, the length of the tube, and the diameter of the tube. It is important to remember the strong impact of caliber variations, meaning, for instance, that reducing the tube’s diameter by half (50% stenosis) decreases the flow rate by 16-fold (r4). Quantifying bulk arterial flow with sufficient accuracy for clinical application is challenging despite the introduction of techniques like quantitative magnetic resonance angiography (35). Novel imaging techniques, such as 4D flow MR imaging, are being developed to evaluate flow patterns and circulation but are not routinely used in clinical practice. Therefore, surrogate measurements, such as “degree of stenosis” (ie, the maximal reduction in vascular cross-sectional diameter caused by a lesion, typically expressed as a percentage), are used in clinical practice to estimate the severity of a stenotic lesion and to determine whether or not a revascularization procedure is indicated.
Perfusion imaging is now used routinely to evaluate for occlusive lesions as a surrogate for adequate blood flow to areas of the brain. The hemodynamic impact of a stenotic cerebrovascular lesion (as well as the effects of revascularization) can be estimated quantitatively or semi-quantitatively by a range of advanced imaging techniques that include computed tomography perfusion imaging, magnetic resonance perfusion imaging, and positron emission tomography (121; 78; 23).
Emboligenicity. Stenotic lesions can also produce downstream ischemia by embolus formation. This phenomenon can occur even at non-flow-limiting degrees of stenosis. From a clinical point of view, the patient may remain asymptomatic (“silent emboli” but with radiographic evidence) or develop neurologic impairment, depending on the location and size of the thromboembolic stroke.
As the vessel lumen decreases, there is a shift from laminar to turbulent flow. Turbulent flow is associated with disturbed hemostasis caused by increased platelet aggregation (ie, "white clot" formation), resulting in thromboemboli formation. As flow compromise progresses, turbulence intensifies, and downstream perfusion is reduced. This adds another dimension to the disturbance of hemostasis, hence, the risk for stroke: sluggish flow as a prethrombotic state (ie, "red clot" formation). Finally, occlusion is followed by the appearance of a stagnant column of flow distal to the lesion, with its consequent downstream hemodynamic compromise.
The propensity of a stenotic lesion to generate thromboembolism also depends on its endothelial surface integrity, morphology (ie, composition), and stability. Lesions with a smooth surface and endothelial integrity have comparatively little emboligenic potential. Disruption of endothelial continuity results in exposure of the subendothelial thrombogenic surfaces, thereby, increasing the likelihood of thromboembolism. The major sources of emboli are secondary to carotid stenosis or from cardiac origin.
Branch involvement. Cerebrovascular lesions often involve branching arterial segments. Carotid artery stenosis and occlusion typically occur at or immediately distal to the carotid bifurcation. It is critical to evaluate all branching arteries for treatment decision-making. In certain arterial segments, occlusion of certain branching arteries (eg, external carotid artery) is of no clinical consequence and generally well tolerated, whereas occlusion of other branching arteries (eg, middle cerebral artery or anterior cerebral artery) is critical. Similarly, collateral branches embedded into the lesion itself represent a challenge from diagnostic and therapeutic points of view.
Extracranial carotid atherosclerosis accounts for up to 15% of ischemic strokes in the United States (47). The disease is more prevalent in men, and its prevalence steadily increases with age (44; 37). The management of extracranial carotid atherosclerosis depends on a combination of factors that include the symptomatic nature of the patient, the anatomy of the carotid, and the patient’s comorbidities. Treatment options include maximal medical therapy, carotid endarterectomy, and peripheral or transcarotid stent placement with or without balloon angioplasty. Although carotid endarterectomy remains a standard of care for treating carotid stenosis, research has demonstrated equipoise, efficacy, and safety of carotid artery stenting in carefully selected patients. Currently, the Society for Vascular Surgery guidelines recommend carotid revascularization for symptomatic patients with recent stroke and greater than 50% stenosis and for asymptomatic patients with stenosis of 70% to 99% (02).
Symptomatic carotid stenosis. NASCET remains the most important North American trial to guide decision-making (93). When the trial was terminated during interim analysis, 659 symptomatic patients with more than 70% stenosis had been randomized to either a combination of medial management and carotid endarterectomy or to medical management alone. With 24 months of mean follow-up, ipsilateral strokes had occurred in 26% of the nonsurgical cohort, compared to 9% of patients who had undergone carotid endarterectomy. Patients who underwent carotid endarterectomy had a lower occurrence of stroke in any territory and major stroke or death from any cause, with perioperative morbidity and mortality of under 6%. Subsequent meta-analyses of major symptomatic carotid stenosis trials (NASCET, ECST, and Veterans Affairs Cooperative Studies Program Trial) demonstrated marginal stroke prevention benefit of carotid endarterectomy for patients with 50% to 69% stenosis, equivalent outcomes compared to medical management for patients with mild stenosis (30% to 49%), and worse outcomes with surgery for patients with minimal stenosis (less than 30%) (93; 84; 08; 101).
Asymptomatic carotid stenosis. In the ACAS and the ACST trials, asymptomatic patients with more than 60% carotid stenosis were randomized either to medical management combined with carotid endarterectomy or to medical management alone (07; 62). The ACAS investigators found a 5.9% absolute risk reduction in patients undergoing carotid endarterectomy (11% vs. 5.1%), and the ACST investigators similarly found a 5.4% absolute risk reduction in patients treated by carotid endarterectomy (11.8% vs. 6.4%). Of note, the benefits of surgery over medical management depend on a combined morbidity and mortality rate below 3% for carotid endarterectomy.
Treatment options for carotid artery stenosis.
Medical management. With the advent of statins, aggressive dyslipidemia treatment, and modern antiplatelet agents, there is ongoing debate about whether the results of these pivotal trials remain valid. CREST-2 is currently enrolling asymptomatic patients with more than 70% stenosis to separately compare carotid endarterectomy to modern medical management alone and carotid artery balloon-dilatation in combination with stent placement to modern medical management alone (estimated study completion, February 2026) (65).
Carotid endarterectomy. Carotid endarterectomy remains a valid standard of care for managing carotid artery stenosis. This procedure involves making a surgical incision, identifying the carotid artery, and removing the plaque, thereby restoring normal blood flow. This procedure may be performed under general anesthesia or local anesthesia. Carotid endarterectomy is beneficial for patients with low surgical risks, favorable surgical anatomy, and those who may not tolerate antiplatelets.
Peripheral (transfemoral or transradial) carotid artery stenting. Carotid artery stenting has emerged as an alternative revascularization technique for carotid artery stenosis. This endovascular approach involves inserting a catheter into the radial artery or the femoral artery and placing a self-expanding stent at the stenotic segment.
The CREST investigators demonstrated that carotid artery angioplasty with stent placement is at least equally effective as carotid endarterectomy, except in patients 70 years of age or older, who had a lower incidence of perioperative strokes with carotid endarterectomy when compared to angioplasty with stent placement (16).
Carotid artery angioplasty with stent placement carried a perioperative stroke and death rate of 7% to 9% in early experience. However, following the introduction of embolic protection devices, registries and clinical trials demonstrated a progressive decline in complication rates (60; 29), which paved the way to a more rigorous comparison of carotid artery angioplasty with stent placement and carotid endarterectomy (16; 11; 69; 103).
The 30-day major adverse cardiovascular event rates reported by the various registries and studies of carotid artery stenting, organized chronologically by the year of publication, illustrate the continued decremental trend obs...
The pivotal studies, including CREST, demonstrated clinical equipoise between carotid artery angioplasty with stent placement and carotid endarterectomy in symptomatic patients, both in the short and long term (ie, 10-year follow-up) (16; 17). Additionally, these trials suggested that:
|
1. Carotid endarterectomy is more likely to be complicated by myocardial infarction, whereas carotid artery angioplasty with stent placement has a higher risk for perioperative stroke. | |
|
2. Carotid artery stenting has possibly a greater benefit in younger patients, whereas carotid endarterectomy is probably superior in patients older than 70 years. | |
|
3. Carotid endarterectomy may be associated with fewer complications than carotid artery angioplasty with stent placement in women. | |
|
4. Cranial nerve palsies were 15 times more frequent in patients undergoing carotid endarterectomy (ie, 4.7%). | |
|
5. Maximal medical therapy can be aggressively implemented, leading to a significant reduction in risk factors. | |
|
6. Early revascularization, either surgically or endovascularly, is not associated with increased risk of complications. | |
|
7. There is no difference in cost between carotid endarterectomy and angioplasty with stent placement. |
Surgical or endovascular treatment of asymptomatic patients remains controversial. CREST-2 is an ongoing trial to determine the benefits of endovascular and surgical management for asymptomatic patients.
Transcarotid artery revascularization. This newer procedure combines percutaneous common carotid artery puncture, proximal reverse flow embolic protection, and balloon dilatation with stent placement. Conceptually, this strategy addresses several key shortcomings of both endovascular and surgical carotid revascularization. In the absence of randomized trials, there have been promising initial results with this technique, for instance, regarding the reduction of the 1-year risk for ipsilateral stroke and death (75; 71). Transcarotid artery revascularization was initially approved for treating carotid artery stenosis with high physiologic or anatomic risks but has rapidly been adopted in the United States. In 2022, the US Food and Drug Administration expanded the indications for transcarotid artery revascularization to include patients with standard risk profiles.
Practice guidelines for extracranial circulation (carotid artery disease). The Society for Vascular Surgery clinical practice guidelines published in 2022 recommend carotid endarterectomy as the first-line treatment for patients with symptomatic carotid stenosis of 50% to 99% and for patients with asymptomatic carotid stenosis of 70% to 99% (02).
For patients with symptomatic carotid artery disease with greater than 50% stenosis and with stable stroke, carotid revascularization should be considered as soon as the patient is neurologically stable, after 48 hours from symptom onset and within 14 days from symptom onset.
Screening for asymptomatic carotid artery stenosis in patients without symptoms or risk factors for carotid artery disease is not recommended. In selected patients with asymptomatic carotid artery disease and increased risk factors, screening can be considered if the patient is a candidate for carotid intervention on the discovery of stenosis.
Regarding nonatherosclerotic lesions, such as traumatic injuries (eg, dissections), congenital vasculopathies (eg, fibromuscular dysplasia), and proliferative stenoses (eg, radiation), there remains a lack of large prospective clinical trials. A systematic review regarding the use of stents in many of these conditions suggests that complication rates may be favorable when medical therapy has failed but perhaps not in the case of primary stenting (12). Therefore, it seems reasonable to have an individualized therapeutic strategy for these patients as it remains difficult to make general recommendations.
Vertebral pathology causing brain ischemia is associated with a 90-day risk of stroke of 25% to 30% following any index event (90; 58; 59), and approximately 15% to 50% of patients who present with vertebrobasilar insufficiency have either an underlying hemodynamically significant lesion or artery-to-artery embolisms (19). Treatment options for vertebrobasilar insufficiency have not been studied as extensively as those for carotid artery stenosis. In general, these lesions are often challenging to access by means of open surgery; therefore, endovascular techniques are often preferred for revascularization of lesions that involve the subclavian or the extracranial portion of the vertebral arteries.
Subclavian and vertebral bypass. Bypass surgery for vertebrobasilar insufficiency has become exceptional, given the advancements in endovascular technology. Still, bypass procedures remain a proven treatment option for vertebrobasilar insufficiency, as seen with vertebral artery occlusion or subclavian steal syndrome.
“Subclavian steal” is defined as a reversal of vertebral arterial flow. Duplex ultrasound is the first noninvasive test of choice for evaluating subclavian steal syndrome. Additional noninvasive tests, including MR angiography and CT angiography, can be used to diagnose an abnormality found on duplex ultrasound.
For patients with symptomatic subclavian steal syndrome, digital subtraction angiography with endovascular balloon dilatation with or without stent placement has become the first-line treatment because of its minimally invasive nature. Subclavian artery-to-carotid artery transposition or carotid artery-to-subclavian artery bypass remain proven alternatives, particularly in cases where the lesion cannot be crossed endovascularly (30). Subclavian and vertebral bypass surgical procedures commonly utilize the occipital artery, which is anastomosed to the extradural vertebral artery, the posterior inferior cerebellar artery, or the posterior cerebral artery branch, depending on the patient’s site of steno-occlusive disease (61; 63; 111). Endarterectomy of the vertebral artery has also been described, but this procedure is no longer used in routine practice, given the availability of endovascular angioplasty and stenting options.
Subclavian and vertebral artery angioplasty and stenting. Although the application of percutaneous transluminal angioplasty for the management of subclavian artery steno-occlusive lesions dates back to the 1980s (09; 83; 114), there remains an ongoing debate in the literature regarding angioplasty alone versus angioplasty with stenting, without any clear settlement based on the existing information (68; 03). Overall, there are probably lesions that can effectively be treated by angioplasty alone, but maintaining patency in more complex or resilient lesions likely requires stent placement. This seems particularly true in patients with occluded subclavian arteries, many of whom present with symptoms of neurologic (ie, vertebrobasilar) or cardiac (ie, internal mammary artery-coronary) steal (82; 51; 102).
Lesions of the vertebral artery are prevalent, and a vertebral artery stenosis that causes 50% or more diameter reduction carries a stroke risk similar to that for carotid pathology (90; 34). Stroke risk is highest during the weeks that follow the index event (ie, acute ischemic stroke or transient ischemic attack) (59). Reports on vertebral artery angioplasty and stenting date back to the late 1990s (21; 80). Despite multiple reports of low rates of periprocedural complications and high efficiency in addressing refractory vertebrobasilar insufficiency in particular (112), there remains ongoing skepticism about the effectiveness of the technique and lack of randomized clinical trials to demonstrate improved outcomes compared to medical therapy alone (33; 81; 120). Also, in-stent restenosis remains definitively a risk, even if the severity of restenosis is often not sufficient to require additional intervention, and technological advances (eg, drug-eluting stents and balloons) are likely to continue to lower its incidence (94; 20). A case series from our center outlines the safe use of a drug-eluting, balloon-expandable Resolute Onyx™ coronary stent (Medtronic) as a unique technique to address vertebral artery ostial stenosis in both symptomatic and asymptomatic patients (77).
Nonatherosclerotic lesions of the extracranial vertebral artery are less frequent, the most pervasive being traumatic dissection, typically at the interface of the V1-V2 or V2-V3 segments. As in the carotid territory, most dissections heal spontaneously without the need for intervention. However, there remains a subset of patients whose symptoms prove refractory to medical treatment or whose lesions cause flow compromise in the context of suboptimal contralateral collateral support, and these patients should definitively be considered for intervention. Stenting of extracranial vertebral artery dissections has been shown to be safe and effective, although the existing literature remains scarce (97; 31; 32; 28; 50).
Intracranial atherosclerotic disease is the most common cause of acute ischemic stroke worldwide, and approximately 50,000 to 100,000 patients per year in the United States suffer from acute ischemic stroke due to intracranial atherosclerotic lesions (67). Its prevalence approximates 13% to 15% in the overall population and is even higher in African-Americans, Japanese, Chinese, and Hispanics, possibly due to a disproportionate prevalence of uncontrolled risk factors, such as arterial hypertension, in these populations (73; 110; 43; 118). Intracranial atherosclerosis carries considerable risk for acute ischemic stroke following any index event, irrespective of any chosen medical therapy. In fact, in two prospective randomized studies of stenting versus aggressive medical therapy (ie, SAMMPRIS and VISSIT), the patients in the medical groups still accrued acute ischemic stroke rates of approximately 5% to 9% during the first 30 days following randomization, and rates of 9% to 12% during the first year of follow-up (26; 25; 39; 123).
Unlike internal carotid artery or vertebral artery lesions, there is considerable variability among intracranial atherosclerotic lesions, particularly in relation to their location and relationship to other intracranial arteries.
Intracranial atherosclerosis lesions can be differentiated based on three attributes:
|
Arterial wall morphology and its microenvironment. The wall of the first-order cerebral arteries (ie, internal carotid artery and vertebral artery) undergoes physical changes as the vessel traverses different spaces: progressive loss of the external lamina elastica, thinning of the tunica media, and variation in transmural pressures due to different surrounding tissues. As the vessel courses through the subarachnoid space, its wall continues to change, becoming increasingly thin and, hence, vulnerable to rupture (eg, iatrogenic subarachnoid hemorrhage from wire perforation during endovascular catheterization maneuvers). | |
|
Relationship to major collateral vessels. Lesions located in arterial segments proximal to the Circle of Willis (eg, carotid bifurcation stenosis or occlusions) are not as likely to produce downstream hemodynamic compromise as those located distal to the communicating arteries (eg, thromboembolic occlusion of the middle cerebral artery). Although arterial territories distal to the Circle of Willis can still receive collateral support from leptomeningeal arterioles, this system is somewhat less predictable, particularly in the elderly with long-standing arterial hypertension. | |
|
Presence of in situ collateral branches. The presence of collateral branches lends itself to these small vessels becoming embedded by the intracranial atherosclerosis lesion and, therefore, vulnerable to acute closure with subsequent ischemic stroke (eg, perforator occlusion due to either progression of an atherosclerotic lesion or during angioplasty or stenting). |
Accordingly, not all intracranial atherosclerosis lesions are equivalent in terms of risk (both natural and procedural) and optimal therapeutic approach (ie, either medical or interventional).
Lack of discrimination between different types of intracranial atherosclerosis lesions potentially explains unsuccessful outcomes of certain clinical trials (ie, SAMMPRIS and VISSIT) (26; 39; 123), and granular differences in the morphology of intracranial atherosclerosis lesions have been shown to considerably influence the outcomes of percutaneous transluminal angioplasty and stenting (Table 2) (87; 88; 89).
Before 2011, more than 80 reports in the literature suggested that percutaneous transluminal angioplasty and stenting could be applied to the treatment of intracranial atherosclerosis lesions with reasonable safety, although there were concerns about high restenosis rates and uncertainty about efficacy (87; 88; 89; 36; 45; 46; 124; 108; 119). The results of two pivotal subsequent studies, SAMMPRIS and VISSIT, changed the prevailing enthusiasm for stenting of intracranial atherosclerosis lesions almost overnight (26; 39; 123). Both studies were stopped prematurely due to the results of interim analyses that uncovered 30-day stroke and death rates that were significantly higher in the patients treated endovascularly (ie, 14.7% and 29.3%, respectively) than in the medical treatment groups (ie, 5.8% and 9.4%, respectively). Interestingly, the stroke rates for the medically treated patients at 1-year follow-up were 12.2% and 15.1%, respectively, underscoring the seriousness of this condition. Both studies have been the subject of criticism, discussions, and controversy, with additional series continuing to appear in the literature in an attempt to elucidate select patient populations who may be considered for this therapy (107; 98; 22; Derdeyn 2015; 64). Despite these criticisms, the current American Heart Association guidelines for secondary stroke prevention due to a recent stroke or transient ischemic attack secondary to severe stenosis (70% to 99%) of an intracranial artery, 90-day dual antiplatelet therapy is the first-line treatment (72). However, the management guidelines for patients who have recurrent transient ischemic attacks or strokes despite dual antiplatelet therapy are less clear. Endovascular treatment may be considered in these patients or in select patients with hemodynamic compromise who suffer from recurrent stroke. Future studies are needed to determine the management of patients with recurrent stroke due to intracranial atherosclerotic disease and which patient population would maximally benefit from endovascular or surgical revascularization of intracranial atherosclerotic disease (42).
Intracranial artery lesion | Attribute | Finding | Success | Restenosis |
Type A | Extension | Discrete | 90% | 0% |
Length | < 5 mm | |||
Stenosis (ø) | 70% to 90% | |||
Occlusion | ||||
Accessibility | Not readily accessible. Straight | |||
Contour | Smooth | |||
Calcification | None | |||
Branch involvement | None | |||
Thrombus | None | |||
Type B | Extension | Tubular | 77% | 31% |
Length | 5 to 10 mm | |||
Stenosis | 90% or greater | |||
Occlusion | Near | |||
Accessibility | Tortuous and | |||
Contour | Irregular | |||
Calcification | Moderate | |||
Branch involvement | Yes. Protectable | |||
Thrombus | Possible | |||
Type C | Extension | Diffuse | 67% | 67% |
Length | Greater than 10 mm | |||
Stenosis | Occlusion | |||
Occlusion | Yes | |||
Accessibility | Tortuous and | |||
Contour | None | |||
Calcification | Severe | |||
Branch involvement | Yes. Not protectable | |||
Thrombus | Yes | |||
| ||||
Practice guidelines for intracranial atherosclerosis. The American Academy of Neurology Practice Advisory for preventing stroke in patients with symptomatic large-artery intracranial atherosclerosis recommends medical management to reduce the risk of recurrent stroke or death (115). Effective management options include antithrombotics, dyslipidemic agents, and lifestyle modification. Angioplasty or stenting and surgical bypass are not recommended as the first-line treatment for symptomatic intracranial atherosclerotic disease. The optimal stroke prevention for patients with recurrent strokes despite maximal medical therapy remains unknown.
Moyamoya disease is a rare, progressive cerebrovascular disease defined by a progressive steno-occlusion of unknown etiology that affects the bilateral supraclinoid internal carotid artery and often involves the proximal anterior and middle cerebral arteries as well. The name “moyamoya” means “puff of smoke” in Japanese and describes the look of the tangle of tiny vessels formed in the basal ganglia to compensate for the blockage. Moyamoya disease was first described in Japan and is found in individuals worldwide; its incidence is higher in Asian countries than in Europe or North America. The disease primarily affects children, but it can also occur in adults. In children, the first symptom of moyamoya disease is often stroke or recurrent transient ischemic attacks (commonly referred to as “mini-strokes”), frequently accompanied by muscular weakness or paralysis affecting one side of the body. Adults may also experience these symptoms that arise from blocked arteries but more often experience a hemorrhagic stroke due to bleeding into the brain. Other symptoms of moyamoya disease include headaches, seizures, disturbed consciousness, involuntary movements, and vision problems, as well as cognitive or sensory impairment. Although most patients with moyamoya disease experience recurrent ischemic or hemorrhagic stroke, a subpopulation may also suffer from chronic hypoperfusion syndromes.
Moyamoya disease is a progressive cerebrovascular disorder that can be classified into six stages, each with typical angiographic findings, according to the Suzuki classification (113).
|
Stage 1: Narrowing of the carotid arteries. | |
|
Stage 2: Initial appearance of basal moyamoya with dilatation of all main cerebral arteries. | |
|
Stage 3: Intensification of moyamoya vessels together with a reduction of flow in the middle and anterior cerebral arteries. | |
|
Stage 4: Minimization of moyamoya vessels; the proximal portions of the posterior cerebral arteries become involved. | |
|
Stage 5: Reduction of moyamoya vessels and absence of all main cerebral arteries. | |
|
Stage 6: Disappearance of moyamoya vessels; the cerebral circulation is supplied only by the external carotid system. |
In addition to moyamoya disease, moyamoya-like vascular changes are seen in association with radiotherapy to the head or neck (particularly radiotherapy for optic gliomas, craniopharyngiomas, and pituitary tumors) as well as with other conditions that include Down syndrome, neurofibromatosis type 1 (with or without tumors of the hypothalamic-optic pathway), and sickle cell disease.
Medical therapy for moyamoya disease includes single antiplatelet medication; the most often used is aspirin, 81 to 325 mg daily. Still, many patients will experience mental decline and multiple strokes because of the progressive narrowing of arteries. Therefore, cerebral blood flow augmentation surgery is often performed. Options for cerebral revascularization include direct EC-IC bypass (eg, superficial temporal artery-to-middle cerebral artery [STA-MCA] bypass) as well as indirect bypass techniques (eg, encephaloduroarteriosynangiosis, encephalomyosynangiosis, or omental transposition). Although many surgeons prefer direct bypass techniques in adult patients (to afford immediate improvement in cerebral hemodynamics), indirect methods remain popular, particularly in children and juvenile patients in whom they promote a robust extracranial-intracranial collateralization over a period of months to years.
Cerebrovascular bypass (ie, cerebral blood flow augmentation surgery). Cerebrovascular or intracerebral bypass collectively refers to a wide range of microsurgical techniques used to improve blood flow and oxygenation to the distal cerebral vasculature. These methods include direct (eg, anastomosis of an extracerebral artery to an intracerebral artery) and indirect (eg, apposition of an extracranial artery or vascularized tissue onto the pial surface) techniques. The former method affords immediate augmentation of hemodynamic flow; the latter method requires months to years for collateral vascular connections to develop. Various indirect bypass procedures include encephaloduroarteriosynangiosis (donor = superficial temporal artery), encephalomyosynangiosis (donor = temporalis muscle), and omental transposition (donor = vascularized abdominal tissue). In situ bypass involves an anastomosis between two intracerebral arteries; this is an uncommon procedure and is outside the scope of this article. Direct cerebral bypass can be further dichotomized into high-flow (eg, anastomosis of external carotid artery to an intracerebral artery using an interposition graft) and low-flow (eg, anastomosis of superficial temporal artery or occipital artery to middle cerebral artery). The superficial temporal artery-middle cerebral artery arterial graft is the most common of the direct procedures and is the focus of this article.
Direct superficial temporal artery to middle cerebral artery (STA-MCA) bypass surgery is typically performed under single antiplatelet therapy, the most often aspirin, 81 to 325 mg daily. Angiography provides information about the course and size of the donor (superficial temporal artery or occipital artery) and recipient (middle cerebral artery) arteries; the recipient artery should be at least 1 mm in diameter. Through the procedure, mean arterial pressure is maintained approximately 10% to 15% above baseline, and osmodiuresis is not used to avoid hypotension. Following exposure, under microscopic visualization, the recipient middle cerebral artery branch on the pial surface is dissected from its arachnoid attachments. Temporary clips are placed on the proximal and distal ends of the recipient artery, and the artery is opened sharply.
A temporary clip is placed on the proximal superficial temporal artery branch, the artery is transected distally and "fish-mouthed" to widen the orifice, and an end-to-side arterial anastomosis is completed. Micro-Doppler and indocyanine green videoangiography are used to verify patency of the graft. Postoperatively, the mean arterial pressure is maintained at baseline or slightly elevated, and aspirin is continued for life. Catheter angiography is performed at 6 to 12 months to verify graft patency.
Direct and indirect bypasses are currently standard for managing moyamoya disease that has failed conservative management. In the past, surgical revascularizations were often routinely performed for ischemic and atherosclerotic diseases. In 1985, the Extracranial/Intracranial Bypass Study Group published a prospective, international, randomized clinical trial to address the question of whether extracranial-to-intracranial (EC-IC) bypass in addition to optimal medical therapy was superior to best medical therapy alone in patients with recently-symptomatic extra- or intracranial athero-occlusive disease (Group EIBS 1985). After an average follow-up period of 55.8 months (and despite an excellent graft patency rate of 96%), the investigators found no surgical benefit for bypass surgery as compared to medical management alone (14% increase in relative risk of fatal and nonfatal stroke in the surgical group as compared to the medical group). Further, higher rates of major perioperative ischemic strokes were seen in the surgical group (4.5% vs 1.3%). Outcomes were particularly poor in patients with middle cerebral artery stenosis or occlusion and those with ongoing symptoms. This study was criticized for the lack of hemodynamic criteria used to select patients at particularly high risk of stroke and, therefore, likely to derive the most benefit from surgery. This critical issue was subsequently addressed in the Carotid Occlusion Surgery Study (COSS) (95). The COSS was a prospective, randomized, blinded-adjudicated trial designed to address the question of whether STA-MCA bypass (in addition to best medical therapy) reduced the 2-year risk of ipsilateral ischemic stroke as compared to optimal medical therapy alone. The trial enrolled patients who had recently suffered from symptomatic extracranial internal carotid artery occlusion and who had documented hemodynamic cerebral ischemia (ie, increased oxygen extraction fraction on positron emission tomography). Despite high graft patency rates (98%), the authors found no benefit for surgery (2-year ipsilateral stroke risk = 21% in the surgical group vs. 22.7% in the medical group; p = 0.8) and a higher rate of perioperative stroke in the surgical group (14.4% vs. 2%, respectively; 95% CI 4.9% to 19.9%). However, a follow-up report detailing the surgical results of COSS and excluding the patients who experienced perioperative strokes (within 30 days of surgery) revealed improved cerebral hemodynamics and lower rates of recurrent ipsilateral ischemic strokes in the surgical group as compared to the medical group (9% vs. 22.7%, respectively, at 2 years) (56). These findings suggest that factors unrelated to the surgery (eg, hemodynamic fragility of the patients involved) were likely responsible for the high perioperative stroke rate in the surgical group (100; 99). The more recent Chinese Carotid and Middle Cerebral Artery Occlusion Surgery Study (CMOSS) again confirmed no benefit of direct bypass in patients with symptomatic internal carotid artery or middle cerebral artery occlusion with hemodynamic insufficiency on CT perfusion imaging (79). Taken together, the EC-IC bypass, COSS, and CMOSS trials ultimately provided Level I evidence for the lack of benefit of STA-MCA bypass in patients with recently symptomatic extra- or intracranial athero-occlusive disease.
Current practice guidelines for Moyamoya disease. The American Heart Association/American Stroke Association current (2023) guidelines recommend that in patients with moyamoya disease and a history of ischemic stroke or TIA, the use of antiplatelet therapy for the prevention of ischemic stroke or TIA may be reasonable (52). There are class 2a recommendations for surgical revascularization in adult patients with symptomatic moyamoya disease. Endovascular or surgical treatment should be considered for hemorrhagic aneurysms of moyamoya vessels.
Intravenous thrombolysis using alteplase remains the first-line therapy for eligible patients with acute ischemic stroke, provided that treatment is initiated within 4.5 hours of clearly defined symptom onset. For the time being, eligible patients should receive intravenous alteplase without delay, even if subsequent mechanical thrombectomy is being considered.
Indications and evidence. The purpose of mechanical thrombectomy is to restore cerebral blood flow in an attempt to salvage ischemic brain tissue that is not already infarcted. Mechanical thrombectomy is indicated for selected patients with acute ischemic stroke due to large artery occlusion, regardless of whether they have received intravenous thrombolysis for the same ischemic stroke event.
There was a turning point for mechanical thrombectomy in 2015 when the aforementioned five multicenter, open-label randomized controlled trials (MR CLEAN, ESCAPE, SWIFT PRIME, EXTEND-IA, and REVASCAT) unequivocally demonstrated that early intra-arterial treatment with second-generation mechanical thrombectomy devices in early time windows (defined as 6 hours from last seen well) is superior (defined as a significant difference in the 90-day modified Rankin Scale score) to standard treatment with intravenous thrombolysis alone for ischemic stroke caused by a documented proximal anterior circulation artery occlusion (10; 18; 53; 70; 104). The number needed to treat for one additional person to achieve functional independence in these trials ranged from 3 to 7.5, and mechanical thrombectomy was beneficial across a wide range of patient subgroups, including patients older than 80 years, patients with high initial stroke severity, and patients not receiving intravenous thrombolysis (54).
Mechanical thrombectomy has also been shown safe and effective in the later time windows (6 to 24 hours) and for “wake-up” stroke patients who have a clinical deficit that is disproportionately severe compared with the volume of infarction on advanced imaging studies (for details, see DAWN and DEFUSE 3 trial eligibility criteria) (04; 91). The evidence for the benefit of mechanical thrombectomy in large core infarcts remains unclear. In a meta-analysis of four randomized controlled trials, endovascular therapy had better functional outcomes measured by mRS score and a higher probability of survival than medical therapy in patients with large ischemic core volume; however, the endovascular intervention group also had higher rates of symptomatic hemorrhage (74).
Finally, mechanical thrombectomy may be a reasonable treatment option for patients with acute large artery occlusion in the posterior circulation, such as the basilar artery, the vertebral artery, or the posterior cerebral artery. Recent meta-analyses of four randomized controlled trials demonstrated that patients with basilar artery occlusion who underwent thrombectomy had an improved mortality rate and better functional status at 3 months than patients treated with medical management alone. However, the risk of symptomatic intracranial hemorrhage was also higher in the intervention group (01; 13).
Technique. First-generation stent retrievers, such as the Merci® Retriever (Concentric Medical) or the Penumbra System® devices (Penumbra, Inc.), may increase recanalization rates in selected patients, but their ability to improve functional outcomes in patients with acute large artery occlusion remains unproven (109; 14; 15). With second-generation stent retrievers, such as the Solitaire™ Flow Restoration Device (Medtronic) and the Trevo® Retriever (Stryker), significantly higher reperfusion rates and better patient outcomes were achieved (92; 106). These second-generation devices were used in the positive thrombectomy trials, MR CLEAN, ESCAPE, SWIFT PRIME, EXTEND-IA, and REVASCAT (10; 18; 53; 70; 104). Catheter aspiration techniques, such as A Direct Aspiration First Pass Technique (ADAPT), employ a catheter to aspirate the thrombus as the first approach. ADAPT has revascularization rates and functional outcome benefits comparable to those of second-generation stent retrievers (85; 76; 116). The continued refinement of devices, such as third-generation stent retrievers (Solitaire X™ [Medtronic]) and catheters (Red® 72 [Penumbra] and Zoom Stroke Solution™ [Imperative Care]), allows for increased vessel navigability and clot retrieval.
The technical advancement that made this possible was the introduction of "stent retrievers," which are devices that can be deployed just like a self-expandable stent across the occluding particle but remain attached to a wire that allows the operator to pull them back into a guide catheter, thereby retrieving the embolic material.
These devices, now in their third generation of design, introduced elements of efficiency and speed to urgent revascularization (ie, rescue) and changed the landscape of care for acute ischemic stroke. The impact of thrombectomy is supported by the remarkable consistency and reproducibility of the results of the different studies, several of which were stopped following interim analyses due to the loss of equipoise derived from the magnitude of benefit observed in their endovascular treatment arms. There are obvious differences and similarities in the design of these studies, yet the weight of their results has shaped our current approach to these patients. In addition, more recent publications have continued to confirm the data outlined in Table 3, including the HERMES metanalysis, which consolidated the experience derived from the five studies considered pivotal (105).
Side effects and complications. Mechanical thrombectomy is not associated with increased rates of symptomatic intracranial hemorrhage or mortality. Reported complications include failure to achieve complete revascularization, new ischemic stroke in a different vascular territory (10), and access site hematoma and pseudoaneurysm formation (18; 53).
MRCLEAN | SWIFT PRIME | EXTEND-IA | ESCAPE | REVASCAT | HERMES | |
Population selection | ||||||
Patients (endo only) | 233 | 98 | 35 | 165 | 103 | 634 |
Stroke severity (NIHSS) | ≥ 2 | ≥ 8 & < 30 | None | > 5 | ≥ 6 | N/A |
Last seen well (hours) | ≤ 6 | ≤ 6 | ≤ 6 | < 12 | 8 | |
Collaterals (ASPECTS) | No | No | No | ≥ 5 | ≥ 7 | |
Penumbra imaging | No | Yes | Yes | Yes (") | No | |
Pre-stroke function (mRS) | ≤ 2 | ≤ 1 | < 2 | ≤ 2 | ≤ 1 | |
Preceding intravenous-TPA | 203 (87.1%) | 98 (100%) | 35 (100%) | 120 (72.7%) | 70 (68%) | 526 (83%) |
Procedural metrics | ||||||
Door to puncture time (min) (*) | 260 | 224 | 210 | 185 | 269 | 238 |
Groin – flow (min) (*) | NR | 28 | 38 | 56 | NR | 48 |
TICI 2b+3 | 115 (58.7%) | 73 (88%) | 25 (86%) | 113 (72.4%) | 67 (66%) | 390 (71%) |
Outcome metrics | ||||||
90-day mRS 0-2 (%) | 32.6 | 60 | 71 | 53 | 43.7 | |
Mortality | 27 (11.6) | 12 (12%) | 3 (9%) | 17 (10.4%) | 19 (18.4%) | 97 (15.3%) |
Infarct volume (ml) (*) | 49 | 32 | 105 | NR | 16.3 | NR |
Trial stopped early | No | Yes | Yes | Yes | Yes | N/A |
Safety metrics | ||||||
Remote embolism | 20 (8.6%) | NR | 2 (6%) | NR | 5 (4.9%) | NR |
Dissection | 4 (1.7%) | NR | NR | 1 (0.6%) | 4 (3.9%) | NR |
Wire perforation | 2 (0.9%) | NR | 1 (2.8%) | 1 (0.6%) | 5 (4.9%) | NR |
Totals hemorrhages | NR | 9 (9.1%) | NR | NR | 29 (28%) | NR |
Sx hemorrhages | 18 (7.7%) | 0 (0%) | 0 (0%) | 6 (3.5%) | 7 (6.7%) | 28 (4.4%) |
HI1 | 1 (0.4%) | NR | NR | 27 (16.4%) | NR | NR |
HI2 | 1 (0.4%) | NR | NR | 25 (15.2%) | NR | NR |
PH1 | 0 (0%) | 4 (4%) | 4 (11%) | 5 (3%) | NR | NR |
PH2 | 14 (6.0%) | 1 (1%) | NR | 4 (2.4%) | NR | 32 (5.1%) |
SAH | 2 (0.9%) | 4 (4%) | NR | 5 (3%) | 5 (4.8%) | NR |
| ||||||
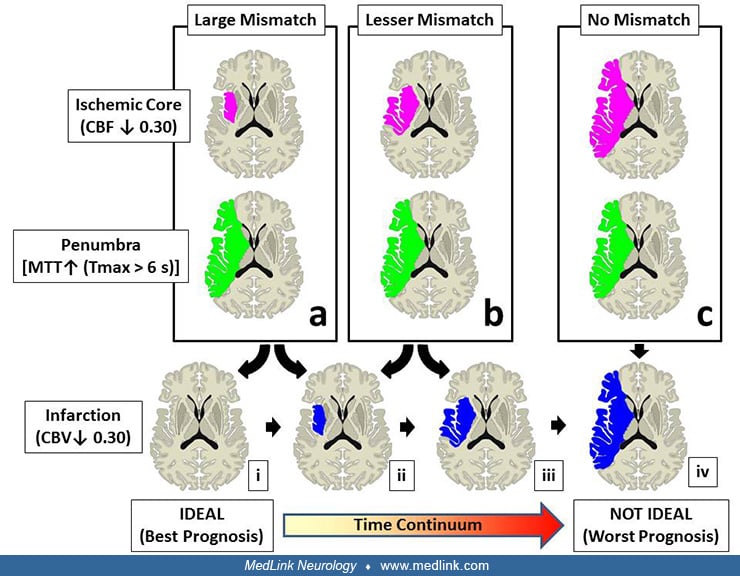
The shift from a strict "therapeutic time window" to a more individualized approach obeys the successful introduction of imaging techniques capable of identifying potentially salvageable (ie, ischemic but not infarcted, or "ischemic penumbra") brain tissue along the time continuum (06). Data from the studies that included CT or MR perfusion as intrinsic steps in their protocols (ie, SWIFT PRIME and EXTEND-IA) demonstrated that certain imaging patterns are associated with a greater chance of improvement following thrombectomy or to predict futility of intervention (18; 104; 86).
Multiple trials, such as MR CLEAN, ESCAPE, SWIFT PRIME, EXTEND-IA, and REVASCAT, demonstrated the superiority of mechanical thrombectomy over intravenous thrombectomy alone among patients with acute stroke when performed within 6 hours of symptom onset (10; 18; 53; 70; 104). Even if benefits of the intervention decline as the time since onset increases, a subset of patients remains in whom ischemic brain tissue remains salvageable in case of reperfusion. Herein, the DAWN and DEFUSE 3 trials demonstrated a 90-day functional outcome benefit of mechanical thrombectomy over standard therapy alone in patients with anterior circulation large artery occlusion and favorable perfusion imaging pattern in the 6- to 24-hour window after initial onset of symptoms (04; 05; 91).
The "ideal" imaging profile of a patient who is likely to benefit from thrombectomy for large artery occlusion is one with: (a) a much larger area of penumbra than ischemic "core" (ie, large mismatch), (b) a small area of ischemic "core," and (c) normal cerebral blood volume. The specifics of how this has translated into the clinical trials are displayed in Table 4.
|
Study |
Core threshold |
Core volume |
Penumbra threshold |
Penumbra volume |
Mismatch ratio |
Mismatch volume |
|
SWIFT PRIME |
NS |
< 50 ml < 80 y |
Tmax > 10 sec |
≥ 15 ml |
> 1.8 |
NS |
|
< 20 ml ≥ 80 y | ||||||
|
EXTEND-IA |
< 30% |
< 70 ml |
Tmax > 6 sec |
NS |
> 1.2 |
> 10 ml |
|
| ||||||
Practice guidelines for mechanical thrombectomy. The American Heart Association/American Stroke Guidelines 2019 Update recommends consideration of mechanical thrombectomy for patients within 0 to 6 hours from symptom onset if they meet the following criteria: pre-stroke mRS score of 0-1, large vessel occlusion of the internal carotid artery or M1 segment of the middle cerebral artery, age older than 18 years, NIHSS score greater than 6, ASPECTS score greater than 6, and treatment can be initiated (groin puncture) within 6 hours from symptom onset (96). Mechanical thrombectomy in the M2 or M3 portion of the middle cerebral artery may be considered in carefully selected patients.
For patients 6 to 24 hours from onset and those who have large vessel occlusion in the anterior circulation and meet other DAWN and DEFUSE 3 eligibility criteria (04; 91) (Table 5), mechanical thrombectomy should be considered.
|
DAWN |
DEFUSE-3 | |
|
Eligibility |
6 to 24 hours |
6 to 16 hours |
|
Location of large vessel occlusion |
Intracranial ICA or proximal MCA |
Extra- or intracranial ICA or proximal MCA |
|
Infarct volume |
≤20 mL if age>80 |
≤70 mL |
|
Mismatch volume |
Not required |
≥15 mL and a mismatch ratio of ≥1.8 |
|
| ||
Although endovascular mechanical thrombectomy has emerged as the standard of care for acute ischemic large vessel occlusions, ongoing investigations are performed to further elucidate which additional subsets of patients may benefit from intervention. It remains unclear whether mechanical thrombectomy may benefit mild symptomatic patients. Current trials, such as Endovascular Therapy for Low NIHSS Ischemic Strokes (ENDOLOW), assess whether patients with low NIHSS scores may have improved 90-day outcomes with endovascular therapy compared with medical management alone. With technological advancements, devices can now be delivered and retrieve clots in distal vessels, but it remains unclear whether this confers clinical benefits in these medium- or small-sized intracranial vessel strokes. ESCAPE-MeVO (Endovascular Treatment to Improve Outcomes for Medium Vessel Occlusions) is a multicenter randomized clinical trial currently enrolling patients with symptomatic acute ischemic stroke in medium-sized vessels to include M2 or M3 segments, A2 or A3 segments, and P2 or P3 segments to investigate 90-day clinical outcome defined by mRS scores. Similarly, DISTALS (Distal Ischemic Stroke Treatment with Adjustable Low-profile stent retrievers) aims to evaluate the use of the Tigertriever 13 revascularization device (Rapid Medical) in patients with smaller vessel acute ischemic stroke to include nondominant or codominant M2 segments, M3 segments, and posterior cerebral artery or anterior cerebral artery segments. These trials will expand our current guidelines for mechanical thrombectomy to benefit patients with acute carotid and cerebral artery occlusions.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Pui Man Rosalind Lai MD
Dr. Lai of Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, has no relevant financial relationships to disclose.
See ProfileTanya Singh MD
Dr. Singh of University at Buffalo has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
Dec. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Sleep Disorders
Oct. 14, 2024
Developmental Malformations
Sep. 22, 2024