






Epilepsy & Seizures
Tonic status epilepticus
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Cerebral venous thrombosis is a rare but important cause of stroke that is often missed or delayed in diagnosis. The author of this article provides literature on the topic. The clinical manifestations are myriad, and a high level of suspicion must be maintained in order to effectively and expeditiously identify this disorder. Infectious and noninfectious processes may cause cerebral venous thrombosis. In the last several years, there has been increased presentation of cerebral venous thrombosis in patients with coronavirus disease 2019 (COVID-19), or after immunization against COVID-19 (02; 09). In adults, about half of cases are associated with pregnancy and the puerperium, but numerous unusual etiologies must be considered in the remainder of patients. Anticoagulation is the mainstay of therapy in the presence of either ischemic or hemorrhagic stroke; in some dire cases, more aggressive approaches such as thrombolysis or mechanical clot disruption may be undertaken.
• Cerebral venous thrombosis is associated with an extensive range of medical disorders. | |
• Treatment is primarily focused on thrombus resolution, with either anticoagulation or endovascular approaches in cases with rapid neurologic deterioration. | |
• Intracerebral hemorrhage due to cerebral venous thrombosis is not necessarily a cause to withhold anticoagulation. |
Ribes made the first clinical description of cerebral venous thrombosis in 1825. In the preangiography era, the clinical presentation of progressive headache, papilledema, seizures, focal deficits, and coma led to the diagnosis of cerebral venous thrombosis, which was usually confirmed by the pathological findings of thrombosis of the major venous sinuses accompanied by hemorrhagic infarction. Cerebral angiography, CT, and MRI (28; 164) have facilitated the diagnosis of this entity and a wide range of clinical presentations has been depicted. Rigorous study of cerebral venous thrombosis has been limited due to its low incidence, and information has come mostly in the form of relatively small case series. However, in 2001, the International Study of Cerebral Vein Thrombosis completed prospective enrollment of 624 patients with this disorder and has provided a wealth of clinical data (62; 64). The overall incidence is estimated at 1.32 per 100,000 person-years (95% CI, 1.06-1.61), and among women between the ages of 31 and 50 years, the incidence is 2.78 (95% CI, 1.98-3.82) (46).
The clinical manifestations are dependent on the venous anatomy. However, involvement of multiple sinuses occurs in about half of cases.
Venous sinuses
Superior sagittal sinus. The superior sagittal sinus drains the major part of the cerebral cortices and plays a major role in the reabsorption of cerebrospinal fluid. It is involved in 70% of cases, and obstruction is manifested by increased intravenous and intracranial pressure. Patients usually present with headache, focal neurologic symptoms, seizures, and papilledema.
Lateral sinus. The lateral sinus, also called the transverse sinus, is involved in 60% to 70% of cases. It drains blood from the sagittal sinus, cerebellum (96), brainstem, and posterior part of the cerebral hemispheres. Isolated occlusion is rare; patients usually have thrombosis of multiple sinuses or cerebral veins. Patients usually present with headache, focal neurologic symptoms, seizures, and papilledema.
Cavernous sinus. The cavernous sinuses are located on each side of the sella turcica superolaterally to the sphenoid air sinuses. Cranial nerves III, IV, and V (V1 and V2 branches) course along the lateral wall of the cavernous sinuses; cranial nerve VI and the carotid artery run in the center. They drain blood from the orbits through the ophthalmic veins and from the anterior part of the base of the brain by the sphenoparietal sinus and middle cerebral veins. Because of their location, cavernous sinuses are often thrombosed in relation to infections of the face or sphenoid sinusitis. Cavernous sinus thrombosis comprises about 5% of all cerebral venous thrombosis cases. Patients usually present with headache, chemosis, proptosis, and painful ophthalmoplegia. Presentation can be more insidious, with only sixth nerve palsy, mild chemosis, and proptosis.
Cerebral veins
Superficial cerebral veins. Some of the cortical veins (frontal, parietal, and occipital) drain by ascending into the superior sagittal sinus, whereas the middle cerebral veins drain by descending toward the cavernous sinuses. Dilation and reversal of flow can occur when the sinus into which the veins drain is occluded due to thin walls and the absence of muscle fibers and valves in these veins. There is also anatomical variation in these veins, making it difficult to define a clinical syndrome of cortical vein thrombosis.
Deep cerebral veins. The deep cerebral veins, including the internal cerebral veins and the basal vein of Rosenthal, drain the deep white matter of the cerebral hemispheres and the basal ganglia. They are affected in 10% of cerebral venous thrombosis cases. Headache and changes in level of consciousness are seen with extensive involvement of this system (156). Severe presentations include focal findings, such as hemiparesis or aphasia, due to bilateral or unilateral edema and hemorrhagic infarction of the basal ganglia and thalami on brain imaging, particularly in young women (151; 37).
Veins of the posterior fossa. Venous drainage of the posterior fossa is divided into superior, anterior, and posterior veins that drain into the vein of Galen, petrosal sinus, and the torcular herophili, as well as the adjacent sagittal sinus and lateral sinus, respectively.
In several series of cerebral sinus thrombosis, the reported mortality was between 6% and 30% (36; 50; 29). In the International Study of Cerebral Vein Thrombosis (ISCVT), mortality was only 4%, which was better than previously reported (64), and recent work suggests that mortality has been progressively declining over the last decade (48). Factors related to poor prognosis include involvement of deep cerebral sinuses, coma, hemiparesis, a large intracerebral hemorrhage or cerebral infarction, age of the patients (infants and the elderly), and the underlying cause (such as cancer or a concurrent neurologic disorder) (64; 73; 54). The presence of cortical venous involvement and parenchymal lesions has also been linked with worse outcomes (106). Overall, 39% of cases in the ISCVT had an intracranial hemorrhage at presentation. Older cases, men, those with thrombosis of the deep cerebral venous system or the right lateral sinus, and those with presence of a motor deficit were at higher risk for death or dependency at 6 months (72). A prognostic score has been developed based on the findings of the ISCVT (61; 94). For those patients who do survive, the outcome is usually good, with full recovery in about two thirds of patients (64). Persistent deficits in some patients can include optic nerve atrophy, hemiparesis, or epilepsy. Residual symptoms, albeit relatively minor, may affect the majority of individuals (83). Recurrence is relatively infrequent, yet repeated episodes may occur (15; 73). Age at cerebral venous thrombosis onset, nonadministration of anticoagulation, persistent venous occlusion, and presence of G20210A mutation in factor II predict recurrence in children (90). The risk of recurrent cerebral sinovenous thrombosis is low and is higher in the first year after discontinuation of anticoagulant treatment and among men (114).
Increasing attention has been devoted to the detection of patent foramen ovale as a cause for ischemic stroke due to paradoxical embolization from systemic veins. An extremely unusual case of paradoxical embolization following cerebral venous thrombosis has also been described (53).
A 22-year-old woman with a prior normal MR scan presented with sagittal and lateral sinus occlusion. Sagittal T1-weighted MR images 4 years earlier showed a normal sagittal sinus, whereas images taken later showed a clot within the sagittal sinus. Despite heparin therapy, the patient had a marked and progressive increase in intracranial pressure with loss of vision and was subsequently treated with multiple doses of intravenous tissue plasminogen activator. The patient's condition and thrombus formation stabilized, but the thrombus did not resolve despite thrombolytic therapy. Optic nerve fenestrations and finally a lumbar-peritoneal shunt successfully relieved the patient's symptoms of increased intracranial pressure.
Numerous predisposing factors for cerebral venous thrombosis have been reported and are present in the vast majority of cases; however, direct causal mechanisms are usually not identified.
Infectious causes. Bacterial sepsis or localized infection was formerly a common cause of cerebral venous thrombosis but has been remarkably reduced since the introduction of antibiotics. In a study published in 1985 by Bousser and colleagues, in a series of 38 patients, only 4 patients had cerebral venous thrombosis secondary to infection. In subsequent series of 135 patients collected by the same authors, only 9 cases were septic. Cavernous sinus thrombosis is the most common form of septic cerebral venous thrombosis, as a consequence of staphylococcus aureus infection of the middle third of the face. Other infection sources include sphenoid or ethmoid sinusitis, dental abscess, and otitis media. Cerebral venous thrombosis may also occur secondary to mastoiditis (91). Herpes zoster has also been associated with cerebral venous thrombosis (127; 167). Thrombosis has been described as a complication of coronavirus disease 2019 (COVID-19) (141; 146; 148; 166).
Hypercoagulability
Hormone-related hypercoagulability. The most common cause of cerebral venous thrombosis in women of childbearing age is hypercoagulability associated with the postpartum period, pregnancy, or oral contraceptive pills. In Bousser and colleagues’ series of 135 patients, the use of oral contraceptives was the only etiologic factor in 14 patients (10%). In the International Study on Cerebral Vein Thrombosis, oral contraceptives were used by 46% of the 464 women with this disorder (34). In a metaanalysis of the effect of oral contraceptive pills on stroke, current oral contraceptive pill users had a 16-fold increased risk of cerebral venous thrombosis compared to nonusers. Emergency contraception has also been associated with cerebral venous thrombosis (85). However, in developing countries, the puerperium is most frequently associated with this entity in young women. Cantu and Barinagarrementeria’s series of 113 hospitalized patients with cerebral venous thrombosis from Mexico City revealed that 57 cases (50%) occurred during the first 3 weeks postpartum.
Genetic prothrombotic disorders. Several genetic thrombophilias predispose to cerebral venous thrombosis (113). The hereditary resistance to activated protein C (also called APC-R) caused by the mutation in factor V (known as factor V Leiden) is the most common. The abnormally formed factor V is unable to be cleaved by activated protein C. This mutation is present in approximately 5% of Caucasians. A single gene defect confers increased risk, but this may not necessarily lead to thrombosis, unless an interaction with an environmental factor (eg, oral contraceptives or pregnancy) or another genetic risk factor is present. Deschiens and associates performed systematic coagulation studies in 40 patients with cerebral venous thrombosis and found that 4 cases (10%) had APC-R with heterozygous factor V Leiden; all of those cases were associated with other risk factors, including systemic lupus, antiphospholipid antibody syndrome, nephrotic syndrome (160), and cervical myelitis (55). TAFI gene polymorphisms have also been described in association with cerebral venous thrombosis (149).
Less common are deficiencies in protein C, protein S, and ATIII (approximately 1 person in 1000 to 5000 people). People with these congenital thrombophilias have a higher incidence of thrombosis than those with factor V Leiden. Cerebral venous thrombosis is the most common neurologic event in patients with these conditions (including factor V Leiden) and can occur in 1% to 3% of affected individuals. Deficiencies of protein C and protein S may also be acquired, particularly by protein wasting in the nephrotic syndrome.
Prothrombin gene variant (substitution of G to A in the prothrombin gene at nucleotide 20210 allele) has been associated with an increased risk for venous thrombosis, including cerebral venous thrombosis, in the setting of other risk factors (factor V Leiden or use of oral contraceptives). This condition is associated with elevated prothrombin levels and its prevalence in the Caucasian population is 2% (115; 100).
Voetsch and colleagues have also identified promoter polymorphisms in the plasma glutathione peroxidase (GPx-3) gene that may predispose to cerebral venous thrombosis (153). Factor XII C46T gene polymorphisms may also increase the risk of cerebral venous thrombosis (130).
Factor VIII elevations may also be associated with cerebral venous thrombosis (32; 89; 129).
Interestingly, the specific thrombophilias involved in cerebral venous thrombosis may differ with respect to disorders associated with deep venous thrombosis (159). A study protocol has been established by the Biorepository to Establish the Aetiology of Sinovenous Thrombosis (BEAST) that aims to recruit highly phenotyped cases to discern genetic links (42).
Acquired hypercoagulable disorders. Other coagulation disorders that are recognized as a cause or predisposing condition for cerebral venous thrombosis include disseminated intravascular coagulation, heparin-induced thrombocytopenia (65), plasminogen deficiency, epsilon aminocaproic acid treatment, sickle cell disease, polycythemia vera, paroxysmal nocturnal hemoglobinuria, thrombocythemia, antiphospholipid antibody syndrome (122), nephrotic syndrome, thyrotoxicosis (144; 23; 68), and hypercoagulability associated with malignancy. Anemia due to iron deficiency and other causes has also been associated with cerebral venous thrombosis (17; 143; 126; 78; 87; 125; 47; 25). Anemia has been confirmed as an overt risk factor for cerebral venous thrombosis (47). Elevated red cell distribution width has been associated with cerebral venous thrombosis (112).
Inflammatory disorders. Conditions such as lupus erythematosus, Behçet disease, sarcoidosis, ulcerative colitis, Crohn disease, and Wegener granulomatosis are associated with cerebral venous thrombosis (59; 157; 50; 07; 20; 41; 10). Cerebral venous thrombosis may be the first manifestation of an inflammatory systemic disease.
Structural damage to venous sinuses. Head trauma and intracranial surgeries are among the most common structural etiologies of cerebral venous thrombosis (57; 74; 11). Cutaneous infections or contusions can injure the diploic veins that connect to the scalp via emissary veins and drain in the superior sagittal sinus.
Miscellaneous causes. Arteriovenous malformations, tumors, carcinomatous meningitis, arachnoid cysts, local or surgical trauma to the jugular vein, high altitude exposure (40; 92), and electrical injury have also been associated with cerebral venous thrombosis (134). Intracranial hypotension and low CSF pressure syndromes have been associated with cerebral venous thrombosis, although the pathophysiologic links require further elucidation (97; 99; 131; 154; 124; 162). Thrombosis has also been noted as a complication of ventriculoperitoneal shunting (140; 12). Systemic venous thrombosis may also be associated.
Idiopathic causes. The proportion of cases of unknown etiology remains high, between 20% and 35% (34). In these cases, even after an extensive initial evaluation is performed, repeated investigations are advisable.
Multiple causes. Multiple predisposing factors were identified in 38% of the International Study of Cerebral Vein Thrombosis population.
The balance between procoagulant (clot-promoting) and anticoagulant (clot-preventing) mechanisms serves to prevent an excessive generation of thrombin when coagulation is triggered. This balance is determined by the levels of all coagulation factors (functional status) and fibrinolytic factors; its disturbance can result in thrombotic events, such as cerebral venous thrombosis. Damage in the endothelium of the vessel wall can also result in cerebral venous thrombosis. Other conditions such as dehydration, particularly in neonates, peripartum women, and elderly individuals can contribute to the development of cerebral venous thrombosis.
Venous occlusion can increase the venous pressure enough to lower the cerebral perfusion pressure, decreasing blood flow and, thus, leading to an area of infarction. Not every venous occlusion is followed by a venous infarction. Perfusion imaging techniques have demonstrated this effect of venous compromise on cerebral perfusion (51; 77).
Gross pathological examination usually reveals pallor and edema of the cortex in the area drained by the thrombosed vein. Multiple petechial hemorrhages can be observed. Thrombosed and dilated sinuses and cortical veins are seen on the brain surface, often accompanied by subarachnoid hemorrhage (22) or subdural hematoma (08; 18). Cerebral edema leads to flattened gyri. Microscopic changes reflect ischemic damage. There is loss of staining in the neuronal cytoplasm, nuclei are pyknotic, and the number is greatly reduced. Reactive gliosis can be seen (30).
The incidence of cerebral venous thrombosis in the general population is unknown. However, several investigators have reported 3 to 5 new cases per year at a single busy general hospital (36; 29). The increased use of neuroimaging has likely led to higher incidence than previously estimated (56). The population subgroup with the highest risk appears to be women of childbearing age, particularly in the postpartum period. The incidence of cerebral venous thrombosis in the peripartum period in India is about 4.5 cases per 1000 obstetric admissions, compared to an incidence of less than 1 case in 3000 obstetric admissions in Western countries.
The International Study on Cerebral Vein and Sinus Dural Thrombosis collected prospective data regarding the clinical presentation, causes, risk factors, prognostic factors, currently applied treatments, complications, and outcomes of patients with cerebral sinus thrombosis. The study recruited 624 patients from 100 centers around the world.
Another high-risk group appears to be neonates or young infants in the setting of severe dehydration (21; 132; 31; 155; 121). In a community-based study of childhood stroke, Broderick and colleagues reported that 3 strokes of all 29 documented strokes were due to cerebral venous thrombosis (31). The cerebral vein thromboses occurred at 6 weeks (dehydration and postviral infection were the causes), 3 months (sagittal sinus thrombosis associated with acute lymphocytic leukemia was the cause), and 15 months (severe dehydration was the cause). Barron and colleagues reported 10 cases of cerebral venous thrombosis in neonates during a 10-year period (21). Thrombosis in these cases was usually associated with an acute systemic illness, such as shock or dehydration. Neonatal thrombosis may also reflect an underlying hematologic disorder (165). These data suggest that cerebral venous thrombosis is proportionally a more common cause of stroke in neonates and infants than in older children and adults. Mortality may be particularly high in this cohort (155).
Specific physiologic states, such as the postpartum period, are important causes of cerebral venous thrombosis. Proper hydration in the postpartum period for ill infants and for neonates is important in preventing cerebral venous thrombosis. Individuals with a known inherited thrombophilia should be treated prophylactically with warfarin to prevent sinus or cerebral vein thrombosis.
Air travel has been associated with cerebral venous thrombosis. Five patients with cerebral venous thrombosis were described who had been traveling on long-distance flights. Diarrhea, dehydration or fasting (133), oral contraceptives, and recent high-altitude mountaineering were associated factors (76). Maintaining good hydration during prolonged travel and treating exacerbating conditions such as diarrhea may help prevent cerebral venous thrombosis. Cerebral venous thrombosis should be suspected in individuals exposed to prolonged air travel who present with symptoms consistent with increased intracranial pressure.
Isolated increased intracranial pressure is one of the most common clinical syndromes associated with cerebral venous thrombosis (29; 79). Benign intracranial hypertension or pseudotumor cerebri is frequently diagnosed in many of these patients, but this entity should be diagnosed only after excluding cerebral venous thrombosis by an appropriate imaging study. Severe elevations of intracranial pressure can mimic encephalitis or meningitis. Appropriate cerebrospinal fluid and radiological studies help to differentiate between these conditions.
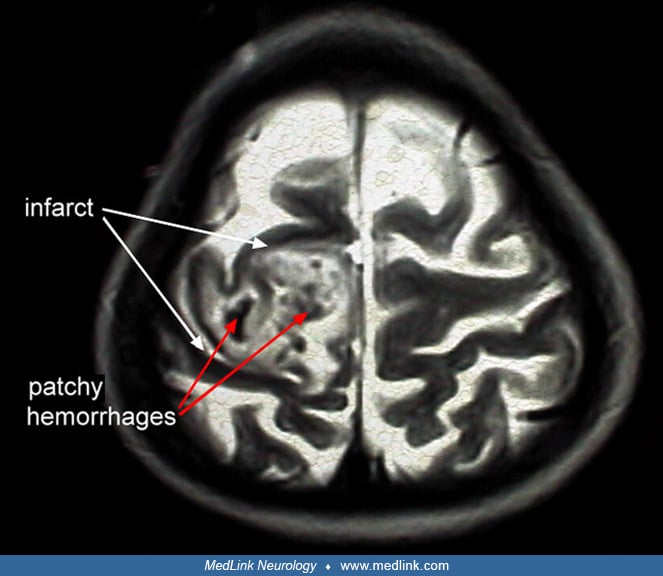
Focal presentations such as stroke syndromes, seizures (focal or generalized), a combination of focal deficits, or a change in the level of consciousness are common. Determining whether the focal findings are due to a venous or arterial occlusion may be difficult. Infarct in an atypical arterial distribution with hemorrhage or surrounding “feathered” edema is characteristic of venous infarction.
Other features that are typical of venous thrombosis are papilledema, bilateral edema, infarction, or hemorrhage in the upper part of the cerebral hemispheres or thalami. Cerebral venous thrombosis should be suspected in patients presenting with prominent and persistent seizure activity, prominent headache several days prior to the stroke, or symptoms in the setting of predisposing conditions such as puerperium or dehydration. Changes in headache characteristics, including exacerbation in head down position, may also herald cerebral venous thrombosis (147). Cerebral venous thrombosis typically manifests with holocranial and bifrontal headache of increasing severity (27). Use of an epidural blood patch for headache has also been implicated in cerebral venous thrombosis (95).
Cerebral venous thrombosis has many potential clinical manifestations and, therefore, diagnosis may be challenging. Ultimately, neuroimaging is needed to detect this disorder. As an initial screening test for patients with suspected cerebral venous sinus thrombosis, D-dimer levels appear to be of value. Prior reports suggested that patients with D-dimer levels below 500 ng/mL are unlikely to have a cerebral venous sinus thrombosis (98), yet a negative D-dimer defined as lower than this threshold does not rule out the diagnosis (49). In the presence of isolated headache, such lower or negative values on D-dimer assays may provide a misleading diagnosis (49).
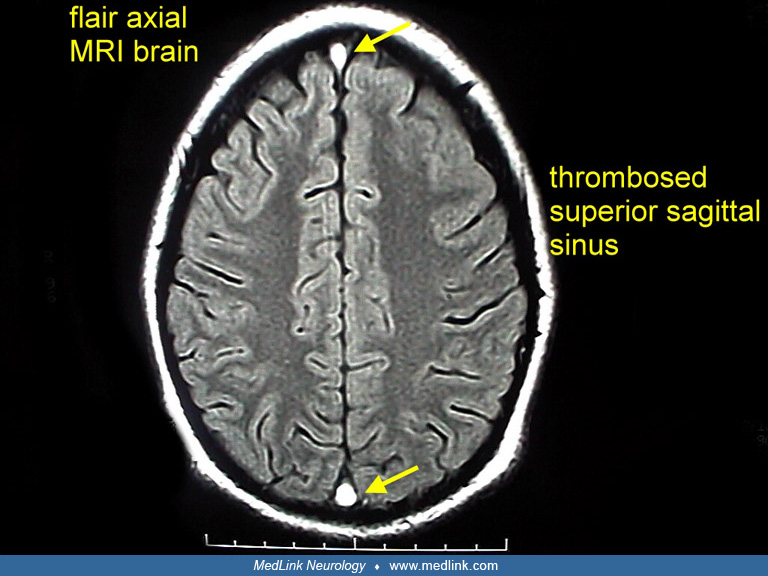
High-quality MRI is the initial procedure of choice for a patient suspected of suffering from cerebral venous thrombosis.
MRI noninvasively detects absence of blood flow in cerebral venous sinuses, images the thrombus itself, demonstrates associated brain infarction, edema, or hemorrhage, detects structural causes of the thrombosed sinus (such as tumor), and rules out other conditions (such as arterial stroke or abscess).
Most importantly, it can be repeated to evaluate resolution or progression of thrombosis.
Selection of the correct MRI protocol is critical, and images in multiple planes and sequences must be evaluated by an experienced physician. For example, on some conventional T1- and T2-weighted MR images, flowing blood can be of high or low signal intensity, as well as isointense. In addition, the appearance of the thrombus itself changes over the first 3 weeks to 4 weeks (88). In the acute phase (day 1 to day 5), the thrombus usually appears strongly hypointense on T2-weighted images, and isointense on T1-weighted images. Magnetic resonance black-blood thrombus imaging may help localize the exact site of thrombosis and aid planning of endovascular treatment (164). Gradient echo imaging may be useful in detecting thrombus in this stage, when it is difficult to detect on other pulse sequences (103; 14). These signal changes correspond to the presence of deoxyhemoglobin and may mimic the appearance of a flow void in some cases. In the subacute stage (up to day 15), the thrombus signal is often strongly hyperintense on both T1-weighted and T2-weighted images as the release of extracellular methemoglobin develops.
In the third stage (after week 3), the thrombus signal is decreased in all sequences and shows increasing inhomogeneity. Finally, the fourth (late or chronic) stage is characterized by either the restitution of blood flow or the persistence of a residual thrombus.
Advances in flow-sensitive 2-dimensional time-of-flight MR, phase-contrast MR, or contrast-enhanced 3-dimensional time-of-flight MR angiography can provide an accurate picture of the presence or absence of flow within the major venous sinuses (88; 29; 117; 118).
However, flow phenomena are not always straightforward and must be interpreted in light of the other standard MR sequences. In a prospective MRI study of cerebral venous thrombosis, Isensee and colleagues recommend the combined use of T1-weighted, spin-density, and single-slice, 2-dimensional, flow-sensitive sequences for the accurate diagnosis of an acute dural sinus thrombosis. However, accurate diagnosis and evaluation of third-stage and fourth-stage cerebral venous thrombosis may be difficult because of the evolution of the thrombus and partial recanalization of the venous sinus. MR venography is a readily available technique that may be more sensitive than MRI in diagnosing cerebral venous thrombosis. If the analysis of the magnetic resonance images is indeterminate and an older thrombosis is suspected clinically, conventional angiography should be performed (88). Artifacts on MRI may also occur, and conventional angiography should be considered when clinical suspicion remains (158).
MRI is not available in some institutions and is unobtainable in many patients who are intubated or uncooperative. Until the recent developments in MRI, CT of the brain was the initial test of choice in the diagnosis of cerebral venous thrombosis. Like MRI, it may rule out other conditions such as arterial strokes or tumors and visualizes cerebral edema, infarction, or hemorrhage associated with cerebral venous thrombosis (168).
With contrast administration, an "empty delta sign" may be seen, representing the opacification of collateral veins in the wall of the sagittal sinus surrounding the nonenhancing clot within the sinus (84; 29).
However, the usefulness of this sign is limited because it is present in only 30% of reported cases. In addition, the posterior sagittal sinus divides into 2 channels in nearly a quarter of normal persons; the 2 channels can appear as a delta sign on CT imaging. Other CT findings include contrast enhancement of the falx and tentorium as well as small cerebral ventricles. The advent of multimodal CT, including noncontrast CT, CT angiography, and CT perfusion may provide a wealth of data for cerebral venous thrombosis, analogous to detailed MRI studies (77). CTA may reveal abnormalities even when symptoms are minimal in the presence of headache and when examination is normal (13). Although parenchymal definition of specific tissue changes may not be as detailed, CT venography can provide exquisite anatomic detail of thrombosed venous sinuses (107; 75). Cerebral venous collaterals are often noted; however, their presence does not seem to relate to clinical outcomes (19).
Cerebral angiography has been the gold standard in the diagnosis of cerebral venous thrombosis for many years. Four-vessel digital or conventional angiography, with visualization of the entire venous phase on at least 2 projections, is necessary. Partial or complete lack of filling of a sinus is the classic angiographic sign of cerebral venous thrombosis.
However, the anterior part of the sagittal sinus may be absent in normal persons, and nearly one fifth of normal persons have partial or total agenesis of 1 lateral sinus. Nonfilling of the posterior portion of the sagittal sinus, the deep venous sinuses, or multiple sinus occlusions is the most specific radiographic marker of thrombosis. MRI is superior to cerebral angiography in that it not only visualizes the absence of blood flow but also the clot itself. Black-blood thrombus imaging has been demonstrated as a promising noninvasive diagnostic strategy (163). Angiography also carries some risk that the dehydrating effects of the contrast agent may result in progression of the thrombosis. In summary, multiple MR and MR angiographic sequences interpreted by an experienced neuroradiologist are the test of choice for suspected cerebral venous thrombosis. CT, followed by cerebral angiography, is another excellent diagnostic option. If MRI is inconclusive, cerebral angiography should be performed.
Cerebrospinal fluid examination is a useful diagnostic, and sometimes therapeutic, procedure. Evaluation of the cerebrospinal fluid can exclude infection or leptomeningeal cancer as a cause of the sinus thrombosis. Repeated lumbar drainage of cerebrospinal fluid may also relieve the symptoms of increased intracranial pressure (150). Some patients, however, may worsen with cerebrospinal fluid drainage in the setting of superior sagittal sinus thrombosis (128). It has been suggested that alleviating cerebrospinal fluid drainage may further decrease flow in these already thrombosed venous structures (128). Cerebrospinal fluid examination should be avoided, if possible, in the setting of an intracranial mass lesion such as a large cerebral infarction or hemorrhage. Cerebrospinal fluid findings in cerebral venous thrombosis include mild to moderate elevation of cerebrospinal fluid protein in two thirds of patients, greater than 20 red cells in two thirds of patients, and a mild pleocytosis in one third of patients (29). Increased cerebrospinal fluid pressure is seen in almost all patients with signs and symptoms of increased pressure.
EEG should be obtained in patients with cerebral venous thrombosis who are comatose or have had recurrent seizures. Seizures are common with cerebral venous sinus thrombosis (111), though it is not certain whether the occurrence of seizures impacts clinical outcome (63; 116). Nonconvulsive status epilepticus, periodic epileptiform discharges, or frequent electrographic seizures on an EEG may point to causes of unresponsiveness other than increased intracranial pressure or stroke that may respond to changes in anticonvulsant therapy. Other investigations include complete blood count, sedimentation rate, renal and liver panels, protime, partial thromboplastin time, antinuclear antibody, rheumatoid factor, serum protein electrophoresis, antiphospholipid antibodies, and chest x-ray. If an obvious cause of venous thrombosis is not found initially, a more extensive evaluation of the hemostatic and thrombolytic systems should be performed, such as protein C, protein S, antithrombin III, circulating lupus anticoagulant, and Leiden factor. If hemostatic abnormalities are detected, long-term anticoagulation will likely be needed.
Treatment of cerebral venous thrombosis has 4 major components: (1) limitation or elimination of the thrombus, (2) treatment of the underlying cause of thrombus formation (if one is found), (3) treatment of seizures, and (4) management of increased intracranial pressure. However, treatment varies dramatically among centers (62). The efficacy of heparin in cerebral venous thrombosis has been demonstrated in a small randomized, placebo-controlled trial and in several large retrospective case series (58; 29; 104). Almost all patients with cerebral venous thrombosis should initially receive full-dose heparin (1.5 times to 2.0 times normal partial thromboplastin time). Studies suggest that even intracerebral hemorrhage is not necessarily a contraindication for anticoagulation in patients with severe and extensive cerebral venous thrombosis (58; 29).
Current recommendations include full-dose heparin (partial thromboplastin time 2.0 times to 2.5 times normal) in all patients without hemorrhage. A similar approach can be considered in patients with cerebral venous thrombosis and hemorrhagic infarction, but alternatively lower levels of anticoagulation with heparin (partial thromboplastin time 1.25 times to 1.5 times normal) can also be considered. Low molecular weight heparin and heparinoids could also be considered for use in patients with cerebral venous thrombosis. However, the single randomized trial of the low molecular weight heparin, nadroparin, showed only a trend (but not a definite pattern) toward more favorable outcomes than patients treated with placebo (52). In the International Study of Cerebral Vein Thrombosis, the vast majority (86%) of patients were treated with heparin or low molecular weight heparins, suggesting a consensus of opinion on its utility in this disease (62; 43). The introduction of novel anticoagulants, including factor Xa inhibitors, provides an alternative form of anticoagulation (71; 120; 123; 60; 38; 66). A systematic review of direct anticoagulants has also been undertaken (26; 136; 161).
Patients must be watched carefully for signs of clinical deterioration or marked increases in intracranial pressure. Duration of subsequent oral anticoagulation depends in part on the clinical picture and followup brain imaging (39). Warfarin (International Normalized Ratio 2.0 times to 3.0 times normal) is generally used for 6 months in stable patients without a defined cause and in whom the thrombus has remained stable or resolved at 6 months. Intervening clinical symptoms should be evaluated by followup MRI. If a persistent abnormality in the hemostatic or thrombolytic systems is discovered during laboratory testing, lifelong anticoagulation treatment may be considered.
Sources of systemic and local infection should be sought carefully for and treated with appropriate antibiotics. In particular, cavernous sinus thrombosis should be assumed to be due to infection until proven otherwise and should be treated with a combination of intravenous antibiotics and heparin. Intravenous steroids may be appropriate in patients with known lupus or Behçet disease (157; 20). Intravenous phenytoin or phenobarbital should be used to control seizures, but prophylactic antiepileptic treatment in a patient without seizures is not necessary.
One of the most difficult treatment issues is the control of increased intracranial pressure. Ideally, one should try initially to avoid dehydrating treatments such as mannitol and furosemide because they may lead to further clot extension. Acetazolamide may be associated with less dramatic fluid shifts and has been used by some investigators. Cerebrospinal fluid drainage by repeated lumbar punctures is a useful treatment option, but it is made more difficult by the frequent use of heparin. Steroids may be helpful if the elevation of pressure does not respond to drainage of cerebrospinal fluid, but this is controversial. Nevertheless, steroids are used in many centers and were administered to one quarter of the 624 patients in the International Study of Cerebral Vein Thrombosis (62). Steroids in the acute phase of cerebral venous thrombosis were not useful and were detrimental in patients without parenchymal cerebral lesions (35). If markedly elevated pressures persist and are accompanied by changes in the level of consciousness, an intracranial pressure monitor can guide therapy to decrease intracranial pressure. In extremely severe cases with progressive deterioration, pentobarbital-induced coma can effectively treat the pressure until the clot begins to lyse or collateral drainage develops (81). In patients with persistently increased intracranial pressure who have progressive visual loss due to optic nerve involvement, optic nerve fenestration can prevent loss of vision. Lumbar-peritoneal shunting should be reserved for patients with chronic symptomatic intracranial hypertension that is unresponsive to other therapies, as systematic review has questioned the overall benefit of shunting in this disorder (108). Decompressive hemicraniectomy may be considered in exceptional cases where mass effect is excessive (45; 101) as this procedure may be lifesaving, and authors suggest relatively good outcomes (01).
In some cases, the standard treatments may be unsuccessful, and the patient may develop worsening levels of consciousness or extension of the thrombus by brain imaging. In these settings, thrombolytic therapy may be considered. Smith and colleagues reported 7 patients who were successfully treated with heparinization and direct installation of a thrombolytic agent into the cerebral venous system via a catheter (139). All of these patients had clinical signs and symptoms of increased intracranial pressure (duration of symptoms 1 week to 6 months) that had not improved or had worsened with heparinization and standard medical therapy. None had evidence of hemorrhage on CT or MRI. Patients received urokinase doses ranging from 20,000 units per hour to 150,000 units per hour, with a mean infusion time to lysis of thrombus of 163 hours (range 88 hours to 244 hours). All patients with headache, papilledema, or focal neurologic findings improved. An infected access site and hematuria were the only complications. Horowitz and colleagues reported treatment of 13 patients with urokinase instilled in the intradural veins via a transfemoral catheter (86). Despite the presence of preinfusion infarcts in 5 patients, 4 of which were hemorrhagic, no major therapeutic morbidity occurred. Functional patency was achieved in 11 of 12 patients, and good to excellent clinical outcome was achieved in 10 of 11 patients with recanalization. The total dose of urokinase ranged from 1.5 million to 7 million units and the duration of treatment varied from 12 hours to 84 hours. The reason for the long infusion times is due to some organization of a large amount of longstanding thrombus. Others have reported effective thrombolytic treatment of superior sagittal sinus thrombosis and venous hemorrhagic infarction with an infusion of low-dose urokinase or tPA directly into the thrombus for up to several days via selective venous catheterization; all of them also received intravenous heparin for 36 hours to 84 hours (69). Angiographic patency was restored, and patients had dramatic clinical improvement. Shorter duration thrombolytic therapy may not result in recanalization. Several mechanical clot disruption techniques may be used as well, including use of the angiojet, stenting (67; 03), and other devices (04). Endovascular thrombectomy may now be performed with a variety of mechanical techniques and devices (145; 33), including direct aspiration (24; 80; 70; 105; 135; 93; 110; 164). Interestingly, the need for complete endovascular recanalization has been questioned (109). The design of a study comparing endovascular thrombolysis with anticoagulation has been detailed (44). A systematic review of 185 cases suggests reasonable safety, although a prospective randomized study is warranted (137; 138). The effect of systemic thrombolysis remains unknown due to lack of a controlled study (152). Spontaneous recanalization during anticoagulation may occur up to 1 year after onset (16; 82).
At present, thrombolytic therapy in patients with venous thrombosis should be considered experimental but worthy of consideration in dire circumstances (142). Unfortunately, the relatively small number of cases of cerebral venous thrombosis at a given institution and the lack of experience with thrombolytic infusion make a randomized trial comparing thrombolytic agents and heparin difficult. The TO-ACT trial, however, is now directly ascertaining this management question, comparing endovascular thrombectomy with anticoagulation (44). In practice, this option appears to be infrequently considered, as it was used in only 2% of the 624 patients in the International Study of Cerebral Vein Thrombosis (62).
Operative thrombectomy of the sagittal sinus, heparin, and pentobarbital coma have been used successfully in the treatment of a 16-year-old boy with extensive sagittal and lateral sinus thrombosis who was comatose with focal neurologic signs and had bilateral white matter ischemia or edema and markedly increased intracranial pressure.
In summary, almost all patients with cerebral venous thrombosis should receive intravenous heparin, treatment for the underlying cause (if known), and nondehydrating treatment for increased intracranial pressure. Patients with cerebral venous thrombosis who have parenchymal blood on brain imaging may still be candidates for heparin therapy, but only with close monitoring of the clinical state and brain images. Those patients who clinically worsen or who show clear evidence of clot extension on MR imaging, despite the best standard therapy including heparin, may be candidates for thrombolytic therapy. Use of thrombolytic therapy as an initial, first-line therapy requires further study.
Pregnancy and the peripartum period are associated with a higher risk of cerebral venous thrombosis. Data suggest that the absolute risk of pregnancy-related venous thrombosis is low in women with previous cerebral vein thrombosis, but the relative risk of noncerebral venous thromboembolism is 16-fold higher, and the recurrence of cerebral vein thrombosis is 80-fold higher (06). In Cantu and Barinagarrementeria’s series of 113 cases of aseptic cerebral venous thrombosis, 57 cases occurred in the postpartum period and 5 cases occurred during pregnancy (1 case in the first trimester, 2 cases in the second trimester, and 2 cases in the third trimester) (36). Seventeen percent of the female patients in the International Study of Cerebral Vein Thrombosis had their thrombosis during pregnancy or the puerperium (34). The risk of recurrent cerebral venous thrombosis with subsequent pregnancies seems to be low; however, many women are treated with anticoagulation during the periods that they are at risk (119). Prenatal diagnosis of fetal cerebral venous thrombosis has also been documented with ultrasonography, allowing for prompt treatment (102). Despite concerns regarding cerebral venous thrombosis and pregnancy, a systematic study demonstrated that recurrent thrombosis with subsequent pregnancies is infrequent (05).
No clinical data are available concerning the use of general anesthesia in the setting of cerebral venous thrombosis. However, in extreme cases of increased intracranial pressure, pentobarbital coma may be used to lower intracranial pressure.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
David S Liebeskind MD
Dr. Liebeskind of the University of California, Los Angeles, received consulting fees for core lab activities from Cerenovus, Genentech, Medtronic, Rapid Medical, and Stryker.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jan. 20, 2025
Sleep Disorders
Jan. 18, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
General Neurology
Jan. 13, 2025