









Peripheral Neuropathies
Neuropathic pain: treatment
Jan. 19, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The author describes the fundamentals of the diagnosis and treatment of cervical disc disease. A historical overview is provided as well as some of the newest concepts in diagnostic imaging and surgical repair. Case studies with imaging and intraoperative photographs are reviewed.
|
• Neck pain, with or without radiating arm pain and associated root distribution paresthesias, numbness, and motor deficit, is the classic presenting feature of cervical disc disease. | |
|
• Degenerative changes in the cervical disc are an inevitable result of aging, and rupture of disc material through the annulus frequently presents as an irritative mass against the centrally positioned spinal cord or laterally positioned root. | |
|
• Along with historical features, physical exam findings help to establish the diagnosis of cervical disc rupture and to distinguish between other causes of pain in the upper extremity, such as shoulder impingement or myofascial pain syndromes. | |
|
• Cervical MRI has become the standard imaging test to confirm the diagnosis of cervical disc disease and rupture; other diagnostic tools such as EMG, CT, or CT-myelography and motion (flexion-extension) x-rays assist in confirmation of diagnosis and in treatment planning. | |
|
• Conservative, nonsurgical treatment is effective and recommended for the majority of cervical disc ruptures, and includes nonsteroidal anti-inflammatory medications, analgesics and muscle relaxants, physical therapy, and traction, as well as epidural steroid injections in selected cases. | |
|
• Surgical treatment consists of nerve or spinal cord decompression, with or without fusion of the disc space segment; there are various time-honored approaches as well as newer techniques and advances, including artificial disc replacement (disc arthroplasty). |
Neck pain, with or without neurologic signs or symptoms, is virtually ubiquitous in modern adult society and represents one of the more common reasons for missed work or visits to the general practitioner, physical therapist, chiropractor, orthopedist, neurologist, or neurosurgeon. Pathological changes in the intervertebral disc and their presumed relationship to neck pain were not well described until the 19th century by such pioneers as Key, Gowers, and von Bechterew (135), and surgical treatment was not attempted until Sir Victor Horsley performed a posterior cervical decompression for spondylotic myelopathy in 1892 (127). Osteoarthritic compression syndromes of the cervical cord and roots were increasingly reported by the turn of the 20th century (08); in 1928, Stookey described a surgical treatment for "ventral extradural cervical chondroma" (122). Walter Dandy recognized the "chondroma" removed from a patient's lumbar spinal canal as displaced cartilaginous disc material (30), and in the 1934 landmark report of surgical treatment for ruptured intervertebral disc, Mixter and Barr described four cervical cases among a larger group of lumbar disc ruptures (87). Gradually the characteristic "soft disc" and "hard disc" compression syndromes were recognized and distinguished from other ailments involving the cervical roots and cord, such as amyotrophic lateral sclerosis, the spastic paraparesis of pernicious anemia ("combined-system disease"), brachial neuralgia or neuritis, and scalenus anticus or thoracic outlet syndrome (35). Spurling further classified the various cervical root compression syndromes and popularized the posterior surgical approach (120; 121), and Lord Brain provided a definitive patient assessment for eliciting history and signs of cervical myelopathy, radiculopathy, and myeloradiculopathy (15). The introduction of positive contrast imaging of the spinal cord and nerve roots in 1944, myelography, raised diagnostic confidence and clinical awareness, which has been further enhanced with CT scanning and the advent of noninvasive MRI.
Degenerative changes in the cervical intervertebral disc are an inevitable result of aging and are influenced by major and minor mechanical stresses to the cervical spine. Dehydration of the disc occurs naturally, allowing shrinkage, cracking, and protrusion of nuclear material through weakening support elements, the annulus and posterior longitudinal ligament. Clinically, this process yields a continuum from the "soft disc" rupture in the earlier phase to the "hard disc," "spur," or osteophyte in the later phase, and often both elements are found to some degree in those cases that come to surgery. Nomenclature varies, and (depending on context, degree of protrusion, and imaging findings) cervical disc herniation may be referred to as "annular bulge," "subligamentous rupture," "extradural rupture" or "free fragment rupture." Ideally, the imaging or surgical description of the abnormality should be based on anatomical compartment (annular, subligamentous, extradural), site of compression (central or ventral, centrolateral, foraminal), and tissue quality (soft disc, ridge, or spur). Cervical spondylosis at an isolated site may be referred to as "osteophyte" or "spur," whereas the unmodified term "spondylosis" refers to a more generalized, frequently multilevel condition. Degenerative changes in the disc may be associated with sclerotic changes in the uncovertebral "joint" (joint of Luschka) or uncinate process located just anterior to the intervertebral foramen, further narrowing the root's bony passage, hence, the term "uncovertebral spur."
Symptoms. Classically, the patient with cervical disc rupture complains of neck, shoulder, and arm pain, with or without distal radiating paresthesias. This symptom complex is typical for acute disc syndromes involving the root, whether from soft disc rupture or acute mechanical root irritation by long-standing foraminal spur. Radicular pain is described as "aching" or "stabbing" in the medial scapular musculature and radiates across the trapezius or shoulder blade down the arm in a partial dermatomal pattern, depending on the root involved, rarely reaching the hand; pain tails off into paresthesias by the mid-forearm, so a dysesthetic tingling or pins-and-needles sensation is described in the hand and fingers. An inciting injury may be cited, ranging in violence from an "innocent sneeze" to a whiplash or rollover car accident, but just as often patients cannot recall a specific moment of injury, and report simply "I woke up with it." Usually, a history of one or more remote injuries will be elicited, as well as a history of repeating minor stresses, particularly at the workplace. Acute radicular pain is more often than not preceded by neck spasm by hours or even days, and the complete resolution of neck pain with persistent severe shoulder, interscapular, and arm pain may indicate a freely ruptured, extradural fragment; as the annular tear allows nuclear material to escape, the disc has spontaneously decompressed.
Pain is usually triggered or intensified with neck extension, particularly with lateral rotation (Spurling maneuver), which further closes the already narrowed foramen. Neck flexion and particularly flexion with lateral bend and rotation away from the involved root affords relief in many cases. Not infrequently, on first sight of the patient in the exam room, he or she is sitting with head tilted forward and to the side, leaning back against the wall, holding the involved arm up and resting the wrist on top of the head, mimicking the position he or she has used for attempted upright sleep in a lounge chair at home. This neck position opens the foramen and alleviates the additional stretch to a compressed root by supporting the arm's weight. This clinical correlation of neck position, foraminal size, and provocation of pain was confirmed by a kinematic MRI study of 25 patients with cervical spondylosis or cervical disc rupture (89). The pain may be constant or intermittent, aggravated by maneuvers that secondarily increase intradiscal pressure, such as coughing, Valsalva maneuver, or strained lifting. Upper cervical root compression, C3, C4, may radiate anteriorly toward the clavicle and predominantly feature neck and shoulder pain rather than extremity pain. Lower root syndromes may also present with shoulder and chest wall pain, indicating an inflamed pectoralis innervation; at times, if left-sided and associated with arm paresthesias, the patient and physician will confuse this for angina and proceed with cardiac workup. Painless syndromes presenting with weakness and numbness or tingling generally are not root in origin but may be due to compressive or irritative lesions of the spinal cord or brachial plexus. Disc or spur compression of C5 produces pain down through the deltoid and biceps toward the elbow, but rarely more distal. Painful paresthesias from C6 compression travel beyond the elbow and down along the radial forearm and brachioradialis, with tingling in the "trigger fingers" (thumb and index). The middle three fingers are involved with C7 compression, along with interscapular pain and a deep aching in the triceps and posterolateral upper arm. Paresthesias more ulnar in distribution may indicate C8 or even t1 involvement, but more commonly represent cord compression or anatomical variation of C7 innervation.
When acute or subacute spinal cord compression occurs, the patient may describe urinary urgency and frequency. Recent onset impotence may be noted. Other more subtle complaints of chest, truncal, or lower limb numbness may indicate early development of an anterior spinal artery syndrome, or partial Brown-Sequard syndrome. Difficulty climbing stairs, getting up, and getting out of chairs is reported, raising the concern for lower extremity spasticity with proximal weakness. Radiating pain in the legs is not seen with cervical cord compressive syndromes, and this confounding history may or may not point to a separate lumbar root problem.
With time, symptoms of root compression tend to be blurred with those of myofascial irritation, a diffuse burning and aching in the musculature of the neck and shoulder girdle, with palpable trigger points. Headache is variable, may be suboccipital and myofascial, and is more difficult to treat in the context of chronic disc syndromes than the root pain itself. Headache with posterior neck pain may be the only presenting symptom of upper cervical disc ruptures, C2-3 or C3-4, because of the proximal and restricted axial innervation by C3 and C4 nerve roots. Chronic disc syndromes produce adaptive or maladaptive behaviors and personalities that can be difficult to separate from the underlying neuromuscular problem.
One important distinction for the examiner to make is between C5 root compression and shoulder impingement syndrome, such as may occur with variable degrees of rotator cuff tear. Both pain syndromes produce severe arm pain that may radiate down from the shoulder and result in weakness and shoulder girdle atrophy. Typically, shoulder impingement pain will be reported as pain and a sense of weakness when extending the arm forward or rotating the arm externally, such as when putting the arm into a coat sleeve, and not be provoked by head turning or head position, as will cervical root pain. The patient with shoulder impingement will awaken with shoulder ache when sleeping on the affected side, whereas the patient who awakens with arm pain from cervical radiculopathy will usually have radiating hand paresthesias. Signs of shoulder impingement syndrome are characteristic and not seen with isolated cervical root compression: pain and weakness with external rotation of the bent arm on manual testing, and pain and weakness with the supraspinatus tests, “full-can” (thumb up) and “empty-can” (thumb down) signs. The latter signs are elicited by having the patient extend the arm 30 to 45 degrees forward with the hand turned thumb up or thumb down, and then having the patient raise the arm to parallel with the floor against resistance. Pain and pain-inhibited weakness indicate a supraspinatus tear with impingement and is much more characteristic of rotator cuff tear than C5 root irritation or deficit, which may simply exhibit painless weakness on this test (91). Diagnosis is further confirmed by shoulder MRI, looking for specific rotator cuff tear and associated pathology. It is fairly common for the clinician managing cervical disc disease to encounter patients with imaging evidence for both cervical root compression and rotator cuff tear, making the physical examination even more crucial in determining which problem needs immediate attention.
Cervical disc rupture presenting with symptoms and signs of spinal cord compression without upper extremity symptoms or neurologic findings is rare but may occur in up to 1% of patients, as documented by a study of 982 surgical patients, 12 of whom presented with truncal, perineum, or lower extremity numbness with gait impairment but without arm or hand symptoms (54).
Signs. Reproduction of the patient's pain on extension and ipsilateral rotation of the head (Spurling maneuver) is pathognomonic for cervical root irritation, analogous to sciatica produced by straight leg raising in the patient with herniated lumbar disc. Variations in pain with mechanical maneuvers likely indicate the peculiar nature of the rupture, or spur, and individual variances of spinal anatomy. Lhermitte sign, a neck flexion-induced electrical shock down the chest, and frequently into the arms, indicates worrisome cord compression and the patient's high vulnerability to further injury with motion.
Sensory loss to light touch or pin below the shoulder is unusual in lesions involving C5 or higher, due to overlapped dermatomal innervation with roots above and below. Occasionally ipsilateral facial numbness is reported in the patient with cord compression, and suspicion of a brainstem or supratentorial demyelinating lesion is raised. However, the cervical cord does carry the trigeminal tract for some distance below the medulla, probably accounting in some instances for the resolution of facial numbness after cord decompression. Sensory loss involving the radial forearm, thumb, and index finger typifies C6 compression. Relative sensory change noted in the middle three fingers is compatible with C7 compression. Fourth and fifth fingers and ulnar forearm are more common with C8 involvement, and T1 ulnar hand and forearm to the elbow. Both ulnar neuropathy from cubital tunnel syndrome and proximal radiation of pain to the neck must be distinguished from lower cervical radiculopathy. Painless loss of sensation is more characteristic of some brachial plexopathies or neuropathies, but also may be seen in the context of chronic spinal cord compression from medial disc or spur. The degree of sensory loss correlates well with the severity of nerve root compression, and the chance of permanent loss despite treatment.
Muscle examination includes inspection for signs of lower motor neuron dysfunction, such as atrophy and fasciculations of the shoulder girdle, or signs of upper motor neuron dysfunction, such as spastic gait. The C5 root independently feeds supraspinatus, infraspinatus, and deltoid muscles and to a much lesser extent the biceps, so profound proximal arm weakness may be detected early with an acute C4-C5 disc rupture. The hallmark findings for C6 root involvement with C5-C6 disc are weakness of biceps and brachioradialis in elbow flexion and forearm supination. Triceps weakness in attempting elbow extension and forearm pronation coupled with finger extension weakness is seen in C7 root syndromes, typically a C6-C7 disc rupture. Syndromes overlap for C8 and T1, although finger flexion weakness is more characteristic of C8, whereas loss of intrinsics with weak finger abduction and adduction is seen with T1 root compression at T1-T2. However, intrinsic hand weakness is far more commonly seen due to compressive cervical myelopathy and injury to anterior horn cells, or to ulnar neuropathy, than to these unusual cervicothoracic root syndromes.
Deep tendon reflexes are diminished or absent at the biceps with either C5 or C6 root compression, depending on individual variation. Brachioradialis reflex is usually somewhat diminished with C6 compression, and often goes with the biceps reflex. Triceps reflex loss typifies C7 deficit. With pure cord compression from medial disc or spur, all reflexes may be increased, along with increased tone and positive Hoffmann sign. Alternatively, a combination of lost biceps-brachioradialis reflexes with increased triceps and lower extremity reflexes may be seen in large C5-C6 disc ruptures as a "central cord syndrome" or "anterior spinal artery syndrome," in which the spasticity of corticospinal tract compression may yield to the overriding lower motor neuron compression of anterior horn cells and C6 root. Increased quadriceps and Achilles deep tendon reflexes, with or without ankle clonus or Babinski, may be seen with cord compressive lesions long before the patient complains of myelopathic symptoms. Loss of superficial abdominal reflexes or anal sphincter tone occurs only in severe compressive cervical myelopathy and is seen with more obvious quadriparesis.
|
Cervical roots |
Reflex Deficit |
Sensory deficit and pain |
Motor deficit |
|
C3 |
---- |
No deficit; pain in paraspinals, scalenes and trapezius, clavicular region |
---- |
|
C4 |
---- |
No deficit; pain in paraspinals, trapezius, scalenes out to shoulder |
None, or rhomboids |
|
C5 |
+/- biceps |
No deficit; pain in paraspinals, shoulder girdle, pectoralis, deltoid, and biceps |
Rhomboids, deltoid, supraspinatus, infraspinatus, some biceps |
|
C6 |
Biceps, radialis |
Radial forearm, thumb, and index finger; pain in paraspinals, shoulder girdle, pectoralis, biceps, and volar forearm |
Biceps, brachioradialis, extensor carpi radialis |
|
C7 |
Triceps |
2nd, 3rd, 4th fingers; pain from paraspinals, medial scapula, pectoralis, and down posterolateral arm |
Triceps, finger extensors |
|
C8 |
+/- triceps |
4th, 5th fingers, ulnar hand; pain in medial scapula, posterolateral arm, medial elbow |
Hand grip, finger flexors, and interossei |
The majority of acute cervical disc herniations will respond to conservative management and resolve spontaneously over the course of weeks and months. Similarly, acute radiculopathy related to spondylosis will also resolve, given time to allow the inflamed nerve root to heal. Spontaneous resolution of herniated cervical disc material has been well documented and is thought to be achieved through inflammatory cell chemotaxis, neovascularization, and phagocytosis (131). Root pain that heralds profound sensorimotor deficit is more likely to be associated with large, free fragment disc rupture, and more likely to require surgical intervention to prevent permanent loss of function. For the more centrally located rupture or spondylotic ridge that presents with myelopathic symptoms or signs, surgical decompression is more likely required to prevent permanent injury, but long-term prognosis is still excellent in this context as well. Acute quadriparesis carries a grave prognosis, whether from soft or hard disc compression, as the cord may have sustained permanent damage regardless of subsequent decompression. Chronic pain that originates from constant and recurrent root compression is more difficult to treat as well as more likely to be refractory to treatment, regardless of modality, as the cycle of root inflammation, myofascial irritability, and postural guarding have already been established. Habitual reliance on narcotic analgesics and muscle relaxants, alterations of personality with onset of dependent and depressive features, and interest in secondary gain from injury all worsen the long-term prognosis for recovery of function and return to gainful employment and satisfactory lifestyle. In a retrospective study of 67 consecutive patients with cervical disc rupture who underwent anterior discectomy, 38% had not returned to work at 1 year after surgery, and length of preoperative sick leave negatively influenced the rate of return to work; disability claim also prolonged return to work, but such factors as gender, smoking history, levels of disc disease, and type of work had no association with rate of return to employment following surgery (10).
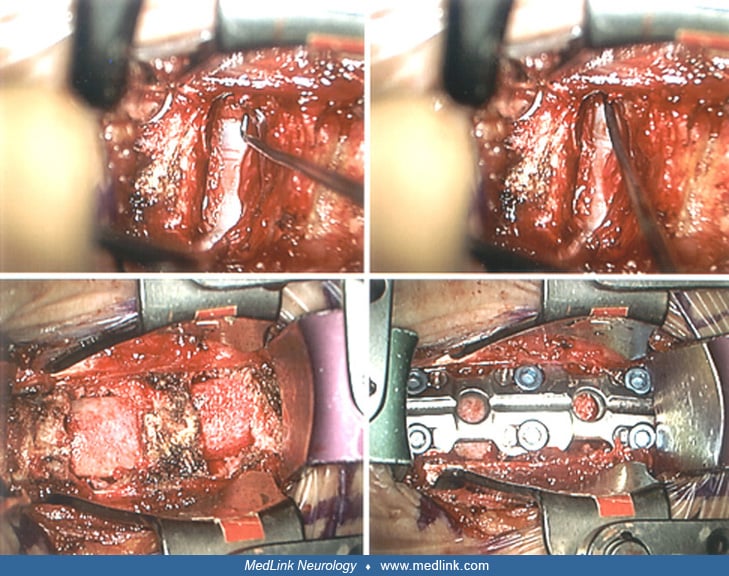
Patient A. A healthy 37-year-old man sustained a flexion-rotation injury during a karate exhibition that rendered him immediately but transiently quadriplegic. He rapidly regained movement in all extremities, but with persistent weakness in the hands and a dysesthetic burning and numbness in the fingers and palms. He was transported with neck immobilization on a spine board to a referral center, where lateral cervical spine x-ray demonstrated disc space narrowing and straightening at C5-C6, but no fracture or subluxation. Examination revealed findings of central cord syndrome, with some features of Brown-Sequard: 4/5 strength in biceps, brachioradialis, and triceps, 4-/5 in finger flexors and 3+/5 intrinsics, all findings slightly better on the right than left. Leg power was intact, but tone was increased bilaterally; sensation to light touch and position change was slightly diminished in the entire left arm, hand, and leg, as compared with right side, but pin-temperature on the left more acute on the left, also more dysesthetic. Deep tendon reflexes were 3+/4 on the right and 4/4 on the left, with sustained left ankle clonus and bilateral upgoing toes to Babinski testing. Sphincter function was spared. Cervical MRI was obtained. Sagittal view demonstrated C5-C6 herniated disc, with protrusion of disc fragments centrally against the cord and elevation of the posterior longitudinal ligament from its attachments on C5 and C6. Axial view reveals ventral compression and flattening of the cord with loss of CSF signal circumferentially. He was treated with intravenous methylprednisolone 30 mg/kg bolus, then with a 23-hour infusion of methylprednisolone 5.4 mg/kg per hour. Gradual recovery of sensorimotor function with limited activity, including ambulation in a Philadelphia collar, allowed resolution of spinal cord edema and delayed surgical treatment at 3 weeks. The patient underwent C5-C6 anterior microdiscectomy, allograft fusion, and plate fixation. Neutral neck position was maintained through intubation and surgery. Findings at surgery were disrupted interspace with hypermobile ligaments, loose cartilaginous endplate, and tear of the posterior longitudinal ligament, with disc fragments protruding and impacting against the ventral dura-covered cord. The patient awoke with resolution of his arm and hand weakness and sensory deficit; there was persistent but improved lower extremity hyperreflexia, and milder transient burning in the fingertips. Postoperative lateral C-spine x-ray confirmed good alignment and position of plate, screws, and graft with restoration of disc space height.
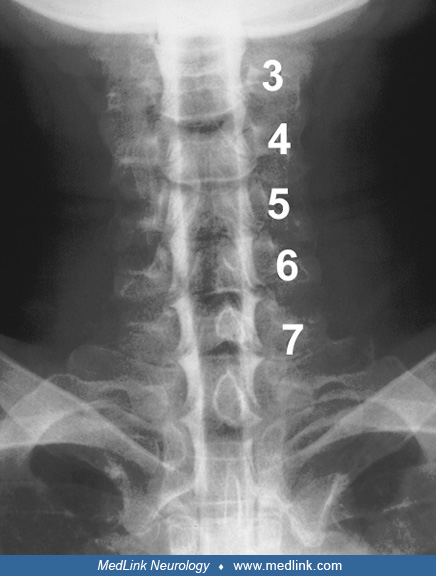
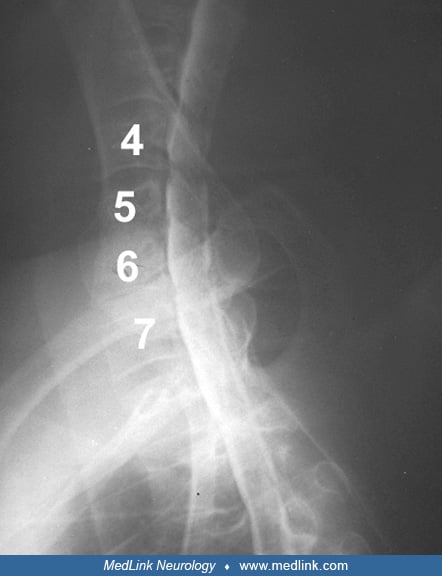
Patient B. A healthy 41-year-old man developed recurrent stiff neck, left shoulder, and arm pain, which were refractory to physical therapy, anti-inflammatory medications, and reduced workload. He had successfully recovered from C5-C6 anterior microdiscectomy, allograft fusion 2 years earlier. This time, however, paresthesias were noted in the middle fingers of the left hand, rather than in the "trigger fingers," and examination revealed mild motor deficit in left triceps and forearm pronation; triceps reflex was absent. Strength and reflex of biceps and brachioradialis were normal, and there were no myelopathic findings. Spurling maneuver reproduced his pain pattern along the medial scapula and posterolateral arm. Initial workup included a C-spine x-ray series with flexion-extension views, showing a solid fusion at C5-C6 with good alignment, and mild degenerative changes at the C6-C7 interspace. Sagittal view MRI revealed minor annular bulges at multiple levels, with no evidence of recurrent disc or spur compression at the operative C5-C6 site axial views suggested foraminal disc herniation left C6-C7 but were inconclusive. Cervical myelography was, therefore, obtained. Anteroposterior view demonstrated good root filling bilaterally at all levels. Contrast filled the subarachnoid space around the cord at all levels on lateral view. However, the axial CT-myelogram view at the C6-C7 showed a moderate sized disc herniation that extended to the left C7 foramen, confirming the axial MRI finding. The patient underwent successful C6-C7 anterior microdiscectomy, allograft fusion, and returned to work following 4 weeks of recovery and an additional 4 weeks of a work conditioning program.
Symptomatic disc disease is multifactorial. Disc degeneration occurs with the dehydrating process of aging, subjected to repeated mechanical stresses or injuries. There may be hereditary and dietary factors at play that are not well understood. Neurologic findings are related to the developmental size of the spinal canal and these superimposed pathological encroachments of thickened ligament, cartilage, and bony spur. Generally, a normal disc will not rupture when subjected to a violent force, as the surrounding bony structures are likely to fracture first; virtually all disc ruptures represent some interplay of degenerative change and injury.
A Japanese prospective study of over 200 asymptomatic volunteers showed significant degenerative “modic” changes in the cervical discs and endplates by analyzing MRI scans done 10 years apart on each individual; the changes were most common in males over 40 whose initial study revealed asymptomatic degenerative disc disease (82). Another group of Japanese researchers found age-related progression of disc disease and canal narrowing in over 1200 asymptomatic individuals, particularly at the C5-6 level (64; 139). Large retrospective studies confirm that the majority of the population develops degenerative disc space changes with age (endplate sclerosis, loss of disc space height, calcifications), most commonly at C5-6, with a lesser degree of slight slip or spondylolisthesis, particularly at C4-5 (126).
Anatomical considerations. Note the following relationships between the vertebral bodies, the intervertebral discs, spinal cord, the exiting nerve roots, and the vertebral artery as seen from a lateral viewpoint. For clarity, the anterior longitudinal ligament running the ventral surface of the vertebral bodies has been omitted. Posteriorly, the ligamentum flavum and dura have been omitted, and the laminar arches of C2 through C6 have been spread to allow a view of the dorsolateral spinal cord.
(1) There is no intervertebral disc between C1 and C2 vertebrae. The ring of C1 articulates with the dens, or odontoid process, of C2 as a rotatory joint supported by the atlantoaxial ligament (anterior limit of the spinal canal), and cruciform, accessory and lateral alar ligaments that form an occipitoatlantoaxial complex. The C1 nerve root (not depicted) is purely motor and exits the spinal canal over the atlas and adjacent to the vertebral artery to innervate the rectus capitis muscles; sectioning C1 along with other upper ventral roots and the accessory nerve is performed in treatment for spasmodic torticollis.
(2) The mixed motor-sensory root C2 exits the canal between the laminar arches of C1 and C2, which articulate anteriorly at the lateral mass. Below this point, from C2 down, posterior articulation is at the facet joint, which lies posterior to the neural foramen and the exiting nerve root.
(3) The C3 root emerges horizontally from the cord and exits under the pedicle of C2 through the C2-C3 intervertebral foramen, posterior to the vertebral artery as it climbs through its vascular foramen in the transverse process. A lateral disc herniation, or spur, at the level of C2-C3 is, therefore, in a position to "catch" the C3 root before it leaves the canal, or within the neural foramen. Because of this horizontal course and numbering of the cervical roots, the cervical intervertebral disc syndromes produce root effects corresponding to the lower numbered vertebra. Thus, a C3-C4 disc rupture typically produces a C4 root syndrome; a C4-C5 rupture produces a C5 syndrome, etc. The C8 root (not depicted) exits through the C7-T1 foramen, and so is vulnerable to compressive lesions at that level. However, the T1 root exits through the T1-T2 foramen, so thoracic disc syndromes have a radicular component corresponding to the upper numbered vertebra. (Because of the descending course of lumbar roots, and the altered relationship between pedicle and intervertebral disc in the lumbar spine, the guideline for "numbering" lumbar disc syndromes shifts again.)
(4) The vertebral artery typically enters its vascular bony channel, or foramen, at C6, and lies in close proximity to the uncinate process and exiting nerve until it enters C2, making it vulnerable to spondylotic compression and to surgical decompression of the root.
From a mid-cervical oblique "front face" or cross-sectional viewpoint, the posterior longitudinal ligament and dura have been omitted, and the tilted surface of the facet joint may be seen. Also depicted is the central nuclear gray of the anterior and posterior horns of the cord.
(5) The nerve root exits the cord (a) through a bony foramen bounded anteriorly by the lateral margin of the disc and the uncinate process and (b) posteriorly by the articulating process of the facet joint.
(6) Small sensorimotor branches are given off as the root exits, innervating periosteum, ligaments, joint capsule, and paraspinal musculature.
(7) A lateral disc herniation or uncinate spur may "catch" just the root, or both at the anterolateral cord and root. A medial disc rupture or calcification of the posterior longitudinal ligament directly impacts the spinal cord.
(8) Lower motor neuron symptoms (eg, weakness, diminished muscular tone, atrophy, diminished or lost deep tendon reflex, fasciculations, and fibrillations) may be due to lateral compression of the exiting root, or to medial compression of the central gray.
Biological changes in the annulus and nucleus pulposus may allow disc rupture in the face of trivial trauma, or with the simple daily stresses of passive and active head and neck motion. Discs are composed of hyaline cartilage end plates attached to the vertebral bodies above and below, a nuclear or central core of mucopolysaccharide gel, and a surrounding layered collagen annulus. The gel is virtually incompressible, making the disc resistant to compression forces, and the annular fibers are arranged to render it relatively resistant to tension, bending, and shear forces. Torsion, as with sudden or repeated neck turning in flexion or extension, puts the annular fibers under the greatest stress, allowing annular fissures and acute protrusion of dehydrated nuclear material (35). Dehydration and fragmentation of the nucleus is a natural process of aging; the nucleus, approximately 88% water in infancy, is reduced to 65% in the elderly (53). The disc loses height and elasticity, transferring some of the stress to the surrounding annulus, and anterior and posterior longitudinal ligaments. As the annular ligaments tear from their bony attachments, bony repair is initiated along the vertebral end plate margins, particularly at the uncinate process laterally; over time a spur is formed. The posterior longitudinal ligament is strongest medially, and tapers out laterally toward the foramen, thus, accounting for the predominance of lateral soft disc protrusion and root compression, over medial rupture with cord compression. The posterior ligament tends to thicken and calcify as well. Chronically, osteophyte formation and vertebral bridging will compensate for the increased motion of the degenerated disc, leading to spontaneous fusion. This ridge will protrude from the vertebral endplates into the spinal canal anteriorly, compressing the spinal cord gradually with or without subtle neurologic change. A critical narrowing occurs when the thickened ligamentum flavum infolds in sudden extension, as seen when an elderly person falls forward; the spinal cord is traumatically pinned between the two unyielding structures. Vascular elements are also compressed in the compromised canal, and venous engorgement and stasis may produce further nerve root and spinal cord edema and injury. Long standing compression of the cord leads to demyelination in corticospinal tracts and loss of anterior horn cells, and cord atrophy may be noted on imaging studies. The compressed nerve root may suffer mild axonal changes of ischemia, producing transient paresthesias, weakness, and loss of reflex, or progress to axonal death and Wallerian degeneration with partial or complete sensorimotor deficit (95).
An extreme form of posterior ligament calcification is now recognized, extending over multiple levels of the cervical spine and not confined to the disc space level, termed "ossification of the posterior longitudinal ligament." Although originally described in the Asian population, and studied and treated extensively by the Japanese, ossification of the posterior longitudinal ligament is reported in other racial groups and presents as a multilevel spondylotic myelopathy (107; 49).
Lumbar disc disease most commonly affects those in the 20- to 39-year-old age group, and cervical disc disease slightly later, perhaps the 30- to 49-year-old age group, and continues into the 50s and 60s and beyond in the form of cervical spondylosis. Next to lumbar disc disease, cervical disc disease is the most frequent cause of missed work in industrial occupations. The prevalence rate for osteoarthrosis of the cervical spine increases with age and may be associated with generalized osteoarthrosis. Note that these degenerative changes do not always lead to symptoms; an MRI study in Japan of 497 asymptomatic subjects found degenerative changes in 17% of discs in men in their 20s and 12% of discs in women in their 20s, and 86% and 89% of discs in men and women over 60 years of age (81). Physically stressful employment tends to increase incidence of the ruptured cervical disc, but the condition is also frequently seen in the sedentary population, and repeated minor stresses may contribute more than single isolated injuries. Generally, reviews of the literature fail to provide more specific etiology and natural history details (66).
However, some researchers are finding a higher incidence of symptomatic degenerative disc disease among populations with congenitally smaller canals; one study found significantly smaller midsagittal and transverse diameters among South African black cadavers than among white cadavers (125).
Multicenter international data collections are ongoing, with early reports of a possible bacterial origin for disc degeneration. Propionibacterium acnes (P acnes) has been cultured from a significant portion of operated discs as reported from each institution, both cervical and lumbar. A bacterial biofilm distribution within the disc matrix has been demonstrated, and meticulously prepared anaerobic cultures of harvested disc material from patients undergoing routine discectomy for degenerative rupture have yielded positive results for P acnes alone, or P acnes mixed with coagulase-negative Staphylococcus species in 44% (162 of 368) of patients' discs (28; 17). In a study, seven of 32 patients demonstrated positive disc material cultures for coagulase-negative staphylococci and two for P acnes, a 25% incidence of disc infection present at surgery (20). Further studies are needed to confirm a causal relationship between anaerobic bacteria and disc degeneration given the ubiquitous presence of the skin flora of P acnes and coagulase-negative staphylococci and the possibility of laboratory contamination during sample collection.
Increased awareness of the relationship between posture, workplace body mechanics, and the development of neck and back pain has led to the developing field of ergonomics. Large series of occupational types have been reported, linking increased incidence of disc disease with repetitive traumatic movements dubbed "repetitive strain injury" (45). Modification of the work environment is recommended to prevent the onset of strain as well as the associated losses in work and compensation. Examples of groups studied include dentists (103), urban transit operators (71), and medical secretaries (63). Most studies stress the value of postural education, range of motion and isometric muscular toning, and adaptation of the workstation to allow a neutral, unstressed posture.
Laboratory testing indicates a metabolic pathway for prevention and treatment of the inflammatory component of disc degeneration; cells from the nucleus pulposis taken at surgery from patients with cervical disc herniation were cultured in the laboratory and found to have accumulations of selective catabolic and inflammatory cytokines, compared with controls (85).
Radiating neck pain with arm and hand numbness may be seen in nondiscogenic disorders, and the myelopathic symptoms of cervical spondylosis are seen in a variety of other disorders as well (Table 2).
|
Degenerative, spinal, or skeletal | ||
|
• Discogenic disease, soft disc, or spondylosis | ||
|
Degenerative, neurologic | ||
|
• Amyotrophic lateral sclerosis (motor neuron disease) | ||
|
Neoplastic | ||
|
• Intradural, intramedullary | ||
|
- Glioma (ependymoma, astrocytoma, ganglioglioma) | ||
|
• Intradural, extramedullary | ||
|
- Schwannoma, neurofibroma | ||
|
• Extradural | ||
|
- Schwannoma, neurofibroma | ||
|
• Brachial plexus | ||
|
- Pancoast tumor | ||
|
Traumatic | ||
|
• Vertebral or posterior element fracture | ||
|
Brachial plexus stretch injury (Erb-Duchenne or Klumpke) | ||
|
Peripheral neuropathy, compressive | ||
|
• Suprascapular | ||
|
Radial | ||
|
• Ulnar (cubital tunnel syndrome, Guyon canal syndrome) | ||
|
Inflammatory | ||
|
• Arteritis | ||
|
Demyelinating | ||
|
• Multiple sclerosis | ||
|
Infectious | ||
|
• Vertebral osteomyelitis | ||
|
Metabolic | ||
|
• Diabetic radiculopathy, plexopathy | ||
|
Vascular | ||
|
• Thoracic outlet syndrome | ||
|
Congenital | ||
|
• Syringomyelia | ||
|
Referred pain | ||
|
• Cardiac ischemia | ||
Plain films. X-rays of the cervical spine in the patient with acute soft disc rupture may be normal or may show straightening of the usual lordosis as a result of paraspinal spasm; the disc space may, occasionally, be narrowed, in association with a significant volume disc rupture. Flexion-extension lateral views allow determination of alignment and stability and may reveal occult fracture or subluxation. A lateral view of the cervical spine with canal narrowed to 13 mm or less indicates significant stenosis, either congenital or acquired (53). More advanced endplate changes or anterior and posterior spondylotic ridges are generally seen with pre-existing disc disease, but do not preclude superimposed soft disc rupture. Oblique views allow inspection of the neural foramina for osteophytic narrowing. Spontaneous fusion by bridging osteophytes may be seen. Postoperative findings of previous laminectomy or fusion are best seen on plain radiographic studies. Differential diagnostic clues may be discovered, such as the erosive lesions of the dens or articular surfaces in rheumatoid arthritis, or of the pedicles and cortical margins in metastatic tumors.
MRI. If initial treatment warrants further workup for neck and arm pain, cervical magnetic resonance imaging is currently the standard evaluation for diagnosing and localizing disc disease. Because of the excellent imaging of soft tissue variations, the study will discriminate between a desiccated (dehydrated) disc, a protruded disc fragment, a posterior disc margin osteophyte, foraminal stenosis, and the calcified posterior longitudinal ligament seen in extensive spondylosis and ossification of the posterior longitudinal ligament. Subtle features of cord or root displacement may be detected, and details of cord atrophy, edema, demyelination, or cystic cavitation are usually evident. Advances in surface coils and imaging software has led to sagittal and axial T2 images that rival CT-myelography. Intravenous Gd-DTPA contrast-enhanced MRI may help to distinguish between postoperative epidural fibrosis and recurrent disc herniation. Nondiscogenic diagnoses such as epidural abscess or metastatic tumor are readily apparent. Advances include direct multiplanar imaging, soft tissue detail, and absence of ionizing radiation. Disadvantages include expense, patient claustrophobia, degradation of signal in the obese patient or patient with fusion hardware, poor bony detail as compared with computerized tomography, and incompatibility with pacemakers or ferromagnetic implanted or imbedded material. MRI is also a sensitive study and will detect disc space changes and spondylosis in asymptomatic patients. One advantage of the lower field strength MRI generally used in open-magnet MRI is the reduced artifact generated by metals in the disc arthroplasty; Antosh and colleagues have shown that the 0.2T magnet actually provides clearer imaging of the patient with artificial disc than does the standard closed 1.5T unit (07).
CT. Occasionally, thin-section CT will visualize the cord and disc anatomy to sufficiently diagnose herniated disc or spur. Additionally, it may be appropriate for the patient for whom MRI or CT-myelography is not tolerated or indicated.
These invasive procedures offer a great deal of detail, particularly the bony foraminal margins not seen well on MRI, but entail the discomfort and risks of lumbar puncture and intrathecal contrast, including allergic reaction and post-puncture headache. Currently, they offer complementary views when MRI has not established the diagnosis or are performed when MRI is not compatible or tolerated. The interrupted flow of intrathecal contrast on prone flexion-extension lateral myelography provides a functional assessment not obtained on static supine MRI, particularly in the context of subluxation or infolded ligamentum flavum. Anatomical detail of the cord, anterior and posterior rootlets, and foraminal contrast filling on axial CT-myelography is exquisite and usually exceeds that seen on axial MRI. Osseous detail of spur, fracture, or calcified posterior ligament is far superior to that seen on MRI. One of the serious concerns regarding the new surgical implants available in treatment of ruptured cervical disc--cervical disc arthroplasty, or “artificial disc”--is the obscuring artifact on MRI and CT produced by the stainless steel (Prestige®, Medtronics Sofamor Danek) or titanium (Bryan® Disc, Medtronics Sofamor Danek) used in these devices. At this point, plain cervical spine x-ray and plain cervical myelography (without CT) are the only satisfactory methods of imaging patients with these implants in evaluation for nerve root or cord compression (124; 37).
Electromyography is valuable in differentiating cervical root disease from lesions involving the brachial plexus and peripheral nerves as well as in providing objective evidence of root irritation in patients whose workup has been otherwise confusing or negative. An abnormal upper extremity EMG sparing the paraspinals may indicate a peripheral lesion in the plexus or peripheral nerves, whereas abnormalities restricted to the paraspinal muscles may be the only electrical finding of a cervical radiculopathy (29). EMG may not isolate root involvement more specifically than two adjacent root levels, especially at C6 (76). As a simple confirmatory test beyond the history, physical exam, imaging studies, and EMG are unnecessary.
Diagnostic root block performed with local anesthetic, such as lidocaine, using fluoroscopic or CT guidance may help distinguish which cervical root is symptomatic in the patient with ambiguous clinical findings and multilevel disc disease or spondylosis, thus, directing surgical treatment (04). A temporary alleviation of symptoms would indicate potential benefit of focal root decompression, and certainly, failure to achieve relief might be a negative predictor for surgical outcome. In addition, acute root compression syndromes occasionally benefit from therapeutic root block in which a combination of steroid and local anesthetic is given, particularly in patients with atraumatic foraminal spondylosis or soft disc herniations at the foramen (117; 116; 123; 24).
Conservative treatment. Most soft disc ruptures are partially contained by layers of the annular and posterior longitudinal ligaments, and occur laterally, where the posterior ligament is attenuated. In time, these ruptures will internally scar and contract, pulling away from the root, alleviating pain, paresthesias, and early motor deficits; sensory deficits will usually resolve later, over weeks and months, but may shrink down to the involved fingertip and persist, indicating permanent root injury. A short course of tapered oral steroid (eg, a 6-day course of prednisone 30 mg in divided doses, reduced to 5 mg) will often speed resolution of root edema, as will a course of nonsteroidal anti-inflammatory drugs. Physical therapy modalities of heat, ultrasound, and electrical stimulation have been shown to reduce discomfort and out-of-work time, and neck immobilization in a soft collar may prevent recurrent mechanical root irritation (61; 109). Chiropractic manipulation of the cervical spine in the context of nerve root or spinal cord compression is potentially dangerous and should be discouraged. Manual manipulation of far lateral disc herniation has been shown to cause vertebral artery occlusion and stroke; spontaneous occlusion and stroke have also been known to occur (96). However, gentle in-line cervical traction of 7 to 10 lbs may reduce the soft disc bulge by exerting tension on the posterior longitudinal ligament; it may also reduce root irritation by transiently widening the neural foramen. Results of traction are less positive in spondylosis, and traction should be discontinued if symptoms worsen. It should not be initiated if the patient is myelopathic. Patients with examination and imaging evidence of spinal cord compression should be referred early for surgical intervention. Most spine centers advocate at least 3 weeks to 6 weeks of nonoperative treatment for nerve root compression syndromes, although patients with profound or progressive sensorimotor deficit may benefit from earlier intervention.
Linear MRI scanning of patients with soft disc herniations shows a high incidence of resorption of disc material extruded laterally into the foramen, thus, supporting nonsurgical treatment in these patients (88).
Conservative management of soft disc rupture is likely to result in resolution of the majority of pain within 6 to 12 months in three quarters of patients and in roughly two thirds of patients with disc osteophytes, arguing against early surgery in patients without neurologic deficit who show early response to nonsurgical therapy (09).
As noted in the diagnostic section, selective cervical root block may play both a diagnostic and therapeutic role in the care of the patient with cervical disc herniation or foraminal spondylosis. Local anesthetic and steroid are injected transforaminally under fluoroscopic or CT guidance; less precision is achieved when injections are done interlaminar into the epidural space, with or without x-ray guidance (14; 116; 24). Technically proficient clinicians using fluoroscopic guidance have shown that in patients selected for isolated root without cord compression, epidural steroid injections can be performed safely and can bring significant symptomatic relief in a majority of patients, thus, avoiding surgery (62). The typical course for epidural injection would include initiation after failed conservative treatment for 2 to 4 weeks, an injection that yields at least 50% pain relief, followed as needed by one or two additional injections over the next months providing intervals of 3 to 4 weeks between injections. Failure to achieve pain relief, exacerbation of symptoms, or onset of neurologic deficit with injection therapy would all indicate possible need for surgical intervention (34).
Over the past several years there has been an increasing interest in treating discogenic pain by blocking or reversing disc degeneration with intradiscal stem cell transplantation, or with intradiscal injection of regenerative factors. The theory is that implanting mesenchymal stem cells into the disc space might reverse attenuation of proteoglycans and type II collagen synthesis, which is the cellular basis of disc deterioration (44). However, these efforts are still in an investigational phase with animal models, and intradiscal stem cell implantation is not FDA approved. The disc space represents a hostile environment to transplanted tissue or injected factors, and current investigations are looking at ways to control for disc space hypoxia, absence of blood supply, and endogenous proteinases and cytokines (56; 104). Percutaneous intradiscal injection of gel ethanol has been reported in investigational mode with positive results in preliminary studies of patients treated for “contained” (bulging) cervical disc herniation (72).
Surgical treatment. Patients referred for surgery have either failed conservative measures of treatment and exhibit refractory pain or progressive sensorimotor deficit, or they demonstrate significant root or cord compression by MRI or CT myelography. Operative procedures vary, but contemporary techniques are divided into anterior and posterior approaches selected and tailored to accommodate the patient's specific problem. Prognosis with surgery is excellent, and patients generally return to work within 3 to 12 weeks from the day of surgery, depending on severity of preoperative deficit and the job requirement for postoperative rehabilitation or work conditioning program. As with all surgeries performed on patients typically presenting in pain, patient selection is critical to outcome. One multivariate analysis study from the University of Wisconsin found that gainful employment and minimal preoperative disability were positive predictors for good surgical outcome, whereas preoperative involvement in worker's compensation claims and personal injury litigation were negative predictors for outcome (06). A 2019 Norwegian single-center retrospective study of 1300 consecutive outpatient microsurgical cases showed significant benefit as well as safety and cost savings; in this mix of anterior cervical fusions and posterior microforaminotomies there were no fatalities, rare readmissions, and a 1.2% complication rate that included hematoma, CSF leak, dysphagia or hoarseness and infection (50).
Anterior discectomy, with or without fusion. The anterior approach to the spine allows complete emptying of the disc space of disc material and cartilaginous endplate, and with the use of the microscope, safe opening and removal of the annulus and posterior longitudinal ligament. The anterior wall of the neural foramen may be widened. This approach affords excellent visualization of the pathological tear and ruptured fragments or uncinate spur, and confirmation of a completely decompressed dura covering the spinal cord and proximal roots. To address the more extensive longitudinal cord compression seen in multilevel spondylosis and ossification of the posterior longitudinal ligament medial corpectomy may be accomplished. The approach lends itself to fusion, with restoration of alignment and disc space height using allograft or autologous bone graft, thereby eliminating pathological motion of the disc space and recurrence of the spur, as well as some of the myofascial neck pain seen with chronic degenerative subluxation (84). Historically, techniques have evolved since the original descriptions by Cloward (26) and Smith (118), and have been supplemented by the operating microscope, allograft bone availability, and instrumentation for internal fixation. Disadvantages of the technique include the small operative risks of root or cord injury, hoarseness from recurrent laryngeal nerve injury, esophageal perforation or vertebral artery injury, graft displacement, nonunion or plate-screw failure where those modifications are used, and the need for prolonged external immobilization when internal fixation is not elected. Another theoretical disadvantage of fusion is the potential for accelerated degeneration at adjacent nonfused segments (transitional disease), due to translation of motion above and below from the fused level. This concern has provided some of the incentive for developing disc arthroplasty, “the artificial disc,” which attempts to restore motion, although there are anatomic studies suggesting that transitional disease is simply incidental progression of the patient’s spondylosis (101).
Although grafting the disc space has become the norm, there are still advocates for anterior discectomy without graft, particularly for the patient who has single level lateral disc rupture with root compression (108). Generally, those patients not grafted will go on to interspace fusion, but most surgeons argue for the restoration of normal spinal alignment and foraminal size, as well as reduced postoperative interscapular pain when intervertebral grafting is performed. For a select group of patients with acute small lateral disc ruptures, the concept of anterior discectomy without graft has been reintroduced using a minimally invasive approach (57). There has also been interest in a minimally invasive approach for patients with smaller acute soft disc rupture predominantly presenting with neck pain: percutaneous cervical nucleoplasty. A preliminary 4-year study of 118 patients in the Netherlands undergoing this minimally invasive approach showed similar outcomes to a comparable demographic undergoing the more standard anterior cervical discectomy with fusion (31). Ongoing studies investigate synthetic graft materials for fusion, thus, avoiding the risks associated with standard use of autologous iliac crest or allograft bone. Hydroxyapatite appears to be the most promising substitute, with one investigation of 70 patients demonstrating solid radiographic fusion at 1 year (68; 128). One possible disadvantage of anterior fusion is the increased strain transmitted to the unfused segments above and below the fusion. One report found a 20% increase in shear strain in the adjacent unfused segments 1 year after 2-level and 3-level fusion surgeries. Some of these led to new disc ruptures (83). Substitution of bioabsorbable polymers for the currently popular titanium plate, which would allow slow resorption while maintaining alignment, is currently in the investigational phase (97). Another solution relies on a titanium cage, which can be threaded into the intervertebral disc space and filled with a small volume of in situ autograft bone chips. This eliminates the risk and expense of using allograft bone as well as the morbidity of the iliac crest donor site incision. Preliminary reports demonstrate high fusion rate for one or two levels, with restoration of disc space height and alleviation of symptoms (48). PEEK (polyetheretherketone) cages filled with autologous bone chips, with or without bone morphogenic protein and other “osteostimulation” fusion enhancers, are also approved for use in the United States and have been shown to be adequate substitutes for cadaver grafts, and when used in conjunction with anterior plating, result in a comparable 90% to 95% rate of fusion and prevent subsidence and restenosis of the cervical foramina (12; 73; 129). Synthetic bone graft substitutes, such as beta tricalcium phosphate, are now available (Chronos: Synthes Spine; Signify: Globus Medical) and provide a scaffolding for bony ingrowth across the disc space as well as stimulate osteoblast migration and growth within the PEEK cage, promoting solid fusion (111). A Chinese study of 60 consecutive patients undergoing either autologous iliac crest graft anterior cervical fusion or PEEK cage filled with locally derived bone demonstrated the same high fusion rate (90.3% vs. 93.1%) at 2 years for the PEEK cage group, with the lower morbidity expected by avoiding use of autologous iliac crest graft (78). However, all forms of fusion following disc removal, at least in theory, stress the adjacent motion segments and may cause or accelerate adjacent disc deterioration. Adjacent level disc osteophyte formation with increased adjacent level disc space motion has been well documented (75). The cages may well reduce adjacent segment degeneration as compared with plating procedures because the risk of adjacent level annular ossification has been shown to increase as the edge of the anterior plates come closer to the next disc space (67; 01). The cages are currently being used successfully as a stand-alone device without plate fixation, are effective in restoring disc space height and alignment without complications of subsidence seen with plate fixation, and reduced dysphagia is reported (132; 77). Although critics of stand-alone cage implants were concerned about increased subsidence or loss of lordosis compared with plate fixation implants, several studies have shown no correlation between those postoperative radiological findings and clinical outcome (112; 119). Despite the strong push to consider cervical disc arthroplasty in order to avoid adjacent disc space degeneration seen with fusion, a 22-year follow-up study of 65 patients undergoing single level or multilevel anterior discectomy with plated fusion discovered only two patients (4.5%) who went on to additional surgery for adjacent level disease (16).
Cervical disc arthroplasty. After trials in Europe and an investigational period in the United States, the FDA approved for implantation the 1-level cervical disc arthroplasty (artificial disc), designed to allow continued motion at the intervertebral space, therefore, putting less strain on the adjacent segments (134). The Prestige® (steel, metal on metal; Medtronics Sofamor Danek) and the ProDisc-C (2 cobalt chrome alloy endplates and an ultra-high molecular weight polyethylene inlay; Synthes Spine) are approved by the FDA for implantation, with ongoing trials to determine efficacy and for outcome comparison with fusion surgery. Bryan® was approved by the FDA in 2009; by design (composite polyurethane and titanium, Medtronics Sofamor Danek) it ultimately may be more appropriate for multilevel arthroplasty in addition to its role in 1-level disc replacement. One Belgian study comparing the clinical outcomes of grafting versus disc restoration using the Bryan artificial disc show equivalent relief of neurologic signs and symptoms after 1 year, with restoration of physiological motion at the operative site (41). Similar support for this device is emerging from a North American multicenter prospective randomized controlled trial (27). European and American prospective trials are ongoing using the Prestige II cervical disc replacement with preliminary results that are promising (100; 130; 90; 92). Similar promising results were reported for the Mobi-C disc prosthesis in a 5-year prospective trial compared against 1-level discectomy fusion, with similar outcome data and lower adjacent segment degeneration; this device is approved for 2-level disc replacement as well (52). Five-year follow-up has been recommended before accepting disc replacement surgery as a routine procedure, and currently, 10-year reviews are available from disc arthroplasty centers that establish a safety record, with minimal device failure or device migration noted. Still, it is not clear whether a single level fusion truly leads to increased stress or breakdown, “transitional disease,” at the adjacent motion segment (70). Certainly, the patient who develops a C6-7 disc herniation with or without surgical treatment is at greater risk to go on to a C5-6 disc rupture as well, than is the patient who never develops cervical disc disease. Cadaver studies show increased range of motion at the arthroplasty level compared with either a fused level or natural disc level, indicating that the device reduces stress at the adjacent segments and will hopefully prevent transitional disc-level degeneration and future surgeries (18). At this point, most studies show that 1-level disc replacement compares favorably with anterior cervical fusion in reducing neck pain and radiating nerve root symptoms, but long-term analyses are required before any conclusions can be drawn about the touted reduction in “transitional disease” in the adjacent discs in these patients (105; 140).
One of the first long-term studies of single level disc arthroplasty found that 18 years after Bryan implant surgery only 32 of 57 patients (56%) had preserved motion at the arthroplasty level and 77% of patients had adjacent segment degeneration despite the arthroplasty surgery, comparable to results seen with long-term single-level fusion surgery (39). Adjacent segment ossification is typically reported as less with arthroplasty than with fusion, although the clinical significance may be negligible for most patients (13).
Of note, despite the claim that preserving motion with disc arthroplasty will prevent adjacent segment degeneration, one study analyzing three prospective trials of 93 patients undergoing either total disc arthroplasty or anterior cervical fusion found that after 3 years 16% of the arthroplasty patients and 18% of the fusion patients developed symptomatic adjacent segment disc degeneration, leading to additional surgeries (59). In agreement, additional studies looking at the combined reported series of patients undergoing disc arthroplasty or anterior instrumented fusion show no significant difference in global cervical motion (“cervical kinematics”) (05) or in the rate of development of adjacent segment degeneration by radiological criteria (102; 21; 133). Similarly, Maldonado and colleagues in a prospective study comparing 105 single-level anterior cervical fusion patients with 85 cohort matched single-level cervical disc replacement patients for a minimum of 3 years found no difference in progression in adjacent segment disc disease--10.5% versus 8.8% (80). Several studies have now shown a reduced ability of the artificial disc to sustain range of motion as intended; in a British study, only 17 of 80 artificial discs implanted (21%) showed adequate range of motion after 2 years, and 15 of the discs (18.8%) had gone on to completely fuse by flexion extension x-ray criteria (23). Several authors attribute these adverse outcomes of reduced motion or fusion of the disc replacement to heterotopic bone formation, noted to be more common in patients with preoperative uncinate spurring and spondylotic disease than in those with simple soft disc rupture (25; 137) or in patients undergoing 2-level cervical disc replacement (136). One study of 32 patients studied from 36 months of cervical disc arthroplasty found that most patients developed some degree of heterotopic ossification, as high as 56% with clinical significance (22). A meta-analysis of 230 published papers over 38 years of cervical disc replacement surgeries found a likely underreporting of heterotopic bone formation as a complication, with only 19 papers directly addressing this issue; among these papers that included at least 5-year follow-up, severe heterotopic bone formation occurred at a rate of 22.8% (33). These patients have typically fused across the disc replacement space, raising the concern that for many disc arthroplasty is just a more expensive fusion surgery. A better match between implant surface area and endplate surface area may reduce exposed endplate, thereby reducing postoperative heterotopic bone formation (138). Long-term studies of disc replacement surgery from more than 4 years of research are reporting migration of the implant as well as progressive bone loss around the implant (47). Although rare, migration of a metal-polymer implant forward into the esophagus or posteriorly into the canal can be disastrous and has to be considered in any surgery in which the goal is preservation of motion rather than fusion (98). Case reports elaborating on the details of implant migration emphasize the need for long-term case follow-up (99). A further caution to artificial disc enthusiasts is raised by Guyer and colleagues, who report a debilitating lymphocytic reaction known as “metalosis” in four spinal disc arthroplasty patients, three lumbar and one cervical, comparable to the inflammatory response previously reported with metal-on-metal hip arthroplasties; each of the patients ultimately underwent removal of the devices, and histological analysis showed delayed-type hypersensitivity reaction as a cause for prosthetic failure (46). Revision surgery for complications related to cervical disc implant was initially shown to be more costly and to have a higher morbidity than cervical fusion surgery (93). A 10-year study of 835 cervical disc arthroplasty patients with at least a 2-year follow-up on each patient revealed an overall incidence of 7.5% reoperation, with 4.4% reoperation at the 2-year follow-up point; the majority (76%) of those patients were young women, and their second surgery was revision with anterior cervical fusion (106).
However, 5- and 10-year follow-ups for 1-level and 2-level anterior cervical fusion versus total disc replacement in the published literature have been analyzed for cost, complication rate, severity, surgical revision rate, and symptom resolution, and these metaanalysis studies conclude that either the two procedures are comparable or that cervical disc arthroplasty has become the preferred procedure with slightly lower complication and revision rate (19; 42; 86; 114). Given that spine instrumentation is a lucrative field and a significant medical cost, one metastudy out of a Cleveland clinic looked at the impact of conflict of interest on reported data for these implants using 74 studies divided between authors who reported affiliation with the device instrumentation company and authors did not report affiliation. Although surgical outcome reporting was the same in both groups of publications, studies published by affiliated authors reported a significantly lower and more favorable complication rate for implant surgery than did the nonaffiliated authors (03). A 2018 metanalysis of the American College of Surgeon's National Surgical Quality Improvement Program (NSQIP) database indicated comparable outcomes for single level anterior cervical fusion patients and single level cervical arthroplasty patients, with a slightly higher hospital readmission rate and a 1 day longer length of hospital stay noted in the fusion cohort (113).
One report based on FDA data looking at device failure found that implant migration, neck pain, and heterotopic ossification were the leading indications for device removal in 678 patients over 18 years, subdivided by nine different devices studied (02).
Five-year and 10-year analyses continue to be published looking at outcomes from cervical disc arthroplasty compared with anterior cervical fusion in comparable cohort groups, and these either confirm long-term safety and clinical benefit of cervical arthroplasty without statistically significant reduction in subsequent adjacent level surgeries (40; 43; 65; 79; 74), or indicate small but statistically significant reduction in the need for surgery at the adjacent level in the arthroplasty group (142). There is growing evidence with longer follow-up of cervical disc arthroplasty that implants of various types lead to heterotopic ossification in 33.3% to 46.7% of cases at 5 years (38; 141), but of questionable clinical significance. There are reports, however, of symptomatic heterotopic bone formation producing spinal cord compression much later in follow-up, as in the case of a 46-year-old man requiring a second surgery 10 years after 3-level disc arthroplasty for decompression of a heterotopic spur (55). Despite these concerns, cervical disc arthroplasty has become an accepted and “equal” surgical alternative to anterior cervical discectomy with fusion for most cases of either cervical radiculopathy or cervical myelopathy. A fair comparison of the two techniques was reported in a military study looking at a demographically similar cohort of 45 patients undergoing surgery overseas, with surgical success measured as recovery and return to active duty; 25 patients with anterior cervical fusion and 22 patients with cervical disc arthroplasty underwent surgery with an average follow-up of approximately 6 months (32). There was no statistically significant difference between the two groups regarding outcome or complications or self-assessment. Forty-one (87.2%) patients were able to return to duty without restrictions.
One of the initial concerns was about possible spinal cord, vascular, or esophageal injury due to device dislodgement. Also, the feasibility of revision surgery: can the device be removed and replaced with a more conventional fusion construct, or can the failed device be successfully replaced with another arthroplasty? One group in Texas that performs a high volume of disc arthroplasties studied 53 consecutive total disc replacement revisions and found that the mean postoperative timing for revision was at 40 months. The most common reason for removal was severe osteolysis, often involving C acnes infection; device removal and fusion were performed for subsidence, device migration, treatment of symptoms arising from posterior anatomy (facet joints, etc.), approach-related complications, and pain. Rather than fusion after device removal, device replacement was feasible for hypermobility, metal allergy, implant locked in kyphosis, and oversized implant use (11).
Posterior approaches. Posterior decompression of the cervical nerve root by foraminotomy is achieved with removal of the overlying medial facet and lamina. Small disc fragments and spurs may be removed safely by dissecting ventral to the exposed root sleeve, lateral to the cord (36). Decompression adds little instability, as the facet joints, disc, and supporting ligaments are left intact; fusion of the involved segment and postoperative immobilization are generally unnecessary. Complete laminectomy with foraminotomies will achieve a wider decompression of the spinal cord by removal of compressive posterior elements, such as thickened ligamentum flavum and overhanging facet joints. As compared with the anterior approach, which (except in unusual circumstances) can be safely performed from C3 down to C7 only, posterior decompression may be easily performed from the suboccipital area down through and past the cervicothoracic junction. (Anterior approaches attending to lesions at C1-C3 are taken trans-orally and are rarely indicated for disc disease). Multilevel laminectomy is required to achieve decompression from a single level anterior spondylotic ridge to allow ample room for the cord to "ride away" from the offending ridge. Instability may be treated with bone grafting and instrumentation, as indicated. Disadvantages include the low operative risks of nerve or spinal cord injury, inability to visualize or remove central disc ruptures or spur, extensive paraspinal muscle dissection, and the risk of recurrent disc rupture; unless fusion is performed, the issues of myofascial pain from segmental degenerative motion are left unanswered. Extensive laminectomies carry the additional late risk of reversed lordosis, or "swan neck deformity," due to laxity of the posterior supporting elements. Chronic pain with or without myelopathy may result, leading to further surgery for reduction and fusion (51). In general, simple posterior decompression for discogenic cervical pain is discouraged in the patient with straight or kyphotic cervical alignment due to the increased pressure and abnormal mobility transferred to adjacent segments, which leads to adjacent level deterioration as well as the need for future instrumented fusion and extensive realignment (94). Nevertheless, studies have shown continued utility of the posterior approach for disc or spur in achieving early and longstanding relief from cervical root compression, particularly in patients with unilateral single level involvement (58; 115). For simple nerve root decompression (foraminotomy), it is generally accepted that anterior discectomy with fusion is a better long-term solution than posterior foraminotomy. A large national cohort of 31,953 patients treated by anterior cervical discectomy with fusion (29,958; 93.76%) or posterior cervical foraminotomy (1995; 6.24%) was analyzed and controlled for age, sex, and comorbidities and demonstrated that posterior cervical foraminotomy was associated with a significantly greater rate of wound dehiscence, surgical site infection, and pulmonary embolism; however, it was associated with significantly lower odds of readmission, dysphagia, and pneumonia (60). At 5 years, posterior cervical foraminotomy cases had a significantly higher cumulative revision rate compared to anterior cervical fusion cases.
Although joint injection therapies using cell transplantation or platelet-rich plasma have been in use for years in extra-spinal joint degeneration, the safety and efficacy of such injections for herniated discs in the cervical and lumbar region has not been well studied and established. A group in Tokyo conducted a metaanalysis of the existing literature and concluded that the benefit of this minimally invasive treatment—injecting into the degenerative disc or into the vertebral body above and below—shows promise, but the group is critical of the overall study designs: general lack of comparative before-and-after imaging, and the lack of distinction between patients presenting with discogenic pain versus radicular pain or even set inclusion/exclusion criteria established for this injection therapy. Recommendations were made for more informative study designs (110).
The incidence of ruptured cervical disc in pregnancy is not greater than at other times, and a large series by King found it to be a rare condition (69).
General anesthesia is required for surgical procedures of the cervical disc. Specific considerations include avoidance of neck extension during intubation in those patients with compressive myelopathy, and the maintenance of adequate spinal cord perfusion during positioning and surgical decompression, particularly in elderly patients who undergo a posterior approach. Prone rather than sitting position for posterior decompression may be required to provide adequate blood flow to the cord.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Saul S Schwarz MD
Dr. Schwarz of the University of Colorado Health Sciences has no relevant financial relationships to disclose.
See Profile
Randolph W Evans MD
Dr. Evans of Baylor College of Medicine received honorariums from Abbvie, Amgen, Biohaven, Impel, Lilly, and Teva for speaking engagements.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Jan. 19, 2025
Peripheral Neuropathies
Jan. 19, 2025
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
Peripheral Neuropathies
Dec. 30, 2024
Peripheral Neuropathies
Dec. 30, 2024