










General Neurology
Renal failure: neurologic complications
Jan. 28, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Ciguatoxin, which was first isolated from a dinoflagellate from the Gambier Islands (a small group of islands, remnants of a caldera, in French Polynesia in the Pacific Ocean) and termed Gambierdiscus toxicus, is the most common nonbacterial food toxin related to seafood ingestion in the United States, Canada, and more recently, Europe. Ciguatoxin represents various lipid-soluble polyethers that are acid and heat stable; tasteless, colorless, and odorless; and have a number of pharmacologic effects. The clinical syndrome, termed “ciguatera,” is a serious, although rarely lethal, human food toxicity related to the consumption of tropical reef fish. Because fish is eaten in such abundance and distributed throughout the world, ciguatera can occur most anywhere and should be familiar to treating physicians. Clinicians may soon be able to directly test for ciguatoxins in patients to verify that they have been exposed to ciguatoxin, as opposed to relying solely on the clinical presentation.
|
• Ciguatera fish poisoning is a prevalent environmental toxic exposure found, for the most part, in tropical areas. | |
|
• Patients may be diagnosed in non-tropical areas if there is a history of travel in endemic areas or of eating tropical reef fish shipped to nonendemic areas. | |
|
• Chronic ciguatera symptoms are prevalent after acute exposure and can be exacerbated by foods containing alcohol and serotonin. | |
|
• Inverted sensory symptoms ("hot-cold") are common in ciguatera fish poisoning. |
Ciguatera poisoning is a serious, though rarely fatal, condition related to consuming tropical reef fish. Ciguatoxins are odorless, tasteless, and colorless neurotoxins that accumulate in many fish tissues, including the muscles, head, viscera, and roe. Ciguatoxins retain toxicity despite cooking and freezing (94).
A naming system has been proposed for the various ciguatoxins. CTX is used to indicate toxins that accumulate in fish to levels likely to cause ciguatera poisoning in humans. A letter code indicates the ocean or sea of origin of toxic fish (eg, Pacific Ocean is P-CTX), and a number code indicates the chronological order of reporting of the specific toxin (eg, P-CTX-1) (173).
Fish poisonings appear in translated writings of early Spanish and Portuguese explorers in the 1500s, the writings of Captain James Cook’s voyages to the South Pacific, and in Captain William Bligh’s fateful voyage after the Mutiny on the Bounty (120). A credible description of ciguatera fish poisoning was provided by an author in the Spanish colony of Cuba in the late 1700s.
One of the first recorded outbreaks of ciguatera poisoning occurred in 1774 on His Majesty’s Ship Resolution during Captain James Cook’s (1728–1779) second voyage to the Pacific (44). On July 23, 1774, off Malicolo island in the New Hebrides island group in the South Pacific (now the nation of Vanuatu), the ship’s surgeon William Anderson (1750–1778) recorded a clear account of ciguatera poisoning (02).
• Ciguatera affects multiple organ systems and may have gastrointestinal, neurologic, cardiovascular, dermatological, genitourinary, and emotional components. | |
• Neurologic manifestations affect more than 75% of cases. | |
• Neurologic manifestations usually follow the development of gastrointestinal symptoms. | |
• Neurologic symptoms can be protracted, sometimes lasting many months. | |
• Neurologic symptoms can include various sensory complaints, including numbness and dysesthesias of the extremities; pruritus; temperature reversal; cold allodynia; toothache; circumoral paresthesia; and burning mouth syndrome. | |
• Headaches, dizziness or vertigo, malaise or profound fatigue, circumoral tingling, dysgeusia (eg, metallic taste), dry mouth, pain or tingling in the extremities, and a "loose" sensation of the teeth are common complaints. |
Ciguatera affects multiple organ systems and may have gastrointestinal, neurologic, cardiovascular, dermatological, genitourinary, and emotional components (45; 75; 23). Onset of symptoms is usually within 15 minutes to 72 hours (most within 12 hours) of the ingestion of contaminated fish (08). Acute illness can be prolonged, and the resulting neurologic symptoms can last months, with variable asymptomatic and symptomatic periods (32; 36; 37; 45; 34).
The initial gastrointestinal phase may be the only manifestation, and similarly isolated neurologic involvement may occur. Occasionally, a patient may present with only the inverted sensory phenomenon or with pruritus after alcohol and have no other symptoms. Re-exposure may cause a significant worsening of symptoms (71).
Gastrointestinal. Gastrointestinal symptoms are often the most frequent and earliest manifestations, affecting more than 90% of cases (23; 151). Gastrointestinal symptoms include hypersalivation, abdominal cramps and pain, nausea, intense vomiting, and watery diarrhea (151). The symptoms generally resolve within 1 to 2 days (37).
Neurologic. Neurologic manifestations affect more than 70% of cases (23; 151). Neurologic manifestations usually follow the development of gastrointestinal symptoms, suggesting that the neurologic manifestations may be due to a different physiologic process, such as neuronal or Schwann cell swelling through prolonged activation of sodium channels (03). Neurologic symptoms can be protracted, sometimes lasting many months (37).
Neurologic symptoms can include various sensory complaints, including numbness and dysesthesias (eg, prickling and burning sensations) of the extremities; pruritus (either generalized or affecting preferentially the palms and soles); temperature reversal (eg, where cold objects feel hot, or occasionally vice versa: "hot-cold inversion," "temperature reversal," "sensory inversion"); cold allodynia (ie, pain from mildly cold skin temperatures that would not generally be considered painful); toothache; circumoral paresthesia; dysguesia; and burning mouth syndrome (79; 08; 185; 12; 58; 23; 91; 151). The inverted sensory phenomenon is considered by some to be pathognomonic of involvement with marine toxins (10), although it has also been reported rarely in diabetic and uremic polyneuropathies (184). The Lhermitte phenomenon can occur with ciguatera poisoning (90), and hyperintense signal on T2-weighted sequences in the cervical cord has been reported with ciguatera poisoning (177).
Headaches, dizziness or vertigo, malaise or profound fatigue, circumoral tingling, dysgeusia (eg, metallic taste), dry mouth, pain or tingling in the extremities, and a "loose" sensation of the teeth are common complaints. Cranial nerve abnormalities may also include ptosis, miosis, trismus, various oculomotor and lower cranial nerve palsies, spontaneous downbeat and perverted head-shaking nystagmus, impaired smooth pursuit, visual fixation suppression failure during the bithermal caloric test, and aphonia (124). Other central nervous system manifestations may include opisthotonus, meningismus (ie, signs of meningeal irritation without meningitis), ataxia, and rarely intractable seizures (54). Neuromuscular abnormalities may include hyporeflexia/areflexia, stocking-glove hypesthesia or numbness, carpopedal spasm, myalgias, low back pain, muscle stiffness or spasm, fasciculations, and elevated CPK levels (177). Rarely, the patient may proceed to develop peripheral flaccid paralysis, respiratory muscle paralysis with respiratory failure, generalized seizures, stupor, and death.
Cardiovascular. Cardiovascular manifestations are noted in 20% to 40% of cases (23; 151). Cardiovascular manifestations most often involve bradycardia or hypotension but can include hypotension, hypertension, bradycardia, tachycardia, other arrhythmias, heart block, pulmonary edema, and congestive heart failure (08; 38; 36; 04; 23; 151). In a study of 124 cases of ciguatera intoxication from French Polynesia, cardiovascular symptoms were the primary criteria of severity, with bradycardia and hypotension documented in 75% and 43%, respectively (69).
Dermatologic. The patient may rarely develop a pruritic rash, which, if present, is usually diffuse, nonraised, confluent, and erythematous (109). Loss of hair and nails has been reported.
Genitourinary. Genitourinary signs include the following: painful urination; pain in the perineum, penis, or vagina; and pain in the penis during erection, which may be intensified during ejaculation (158). Cases have been reported of dyspareunia in unaffected women following ejaculation by their male partners, suggesting the possibility of sexual transfer of the toxin, although this has not been proven (101; 99; 31). The toxin can cross the placental barrier causing hypoactivity or shivering movements of the fetus that can be detected by sonography, and also similarly causing transient hypoactivity of the newborn. Ciguatoxin can be secreted in the breast milk causing hypersensitivity of the nipples that interferes with breastfeeding, as well as diarrhea in the infant (19).
Emotional. The patient may be emotionally depressed, hyperexcitable, anxious, nervous, giddy, apprehensive, restless, and agitated. Hysteria, delirium, hallucinations, and irrational behavior may occur (65). The varied and often inexplicable symptoms of ciguatera have been postulated in some cases to be related to somatization (178), but this is unlikely to explain many cases, even with unusual complaints, given the consistency of many of the reports of the affected individuals in different times and locales.
Hypothermia. A high frequency (approximately 60%) of hypothermia (ie, body temperature lower than 36.5 °C) was reported in one study (23).
The prognosis of ciguatera poisoning is generally good, with symptoms typically subsiding within 3 to 6 weeks. However, the outcome apparently depends on the dose of toxin or toxins initially ingested, individual susceptibility, and whether sensitization has occurred. Once intoxication has occurred, consuming fish and alcohol may aggravate the condition and should be eliminated from the diet, at least initially.
Ciguatera-related mortality is rare (less than 0.1% of reported cases) (41).
Chronic ciguatera. Some patients with ciguatera toxicity may develop chronic symptoms (92). Chronic ciguatera is marked by disproportionate disability and nonspecific refractory symptoms such as fatigue, cognitive deficits, and pain and has many similarities to chronic Lyme disease. After the acute phase of ciguatera, many bothersome symptoms may linger for months to years, including pruritus after alcohol consumption, dysesthesias, myalgias, arthralgias, sensitivity to cold, marked fatigue, malaise, and depression (10; 116; 77; 160; 136; 57; 108; 39; 92). Common signs and symptoms of chronic ciguatera can include fatigue, myalgias, headache, diarrhea, cold allodynia, pruritus, and fluctuating paresthesias (92). Symptoms may be exacerbated by consumption of alcohol, fish, nuts, and chocolate. Putative predictors of having symptoms lasting 3 months or longer include age, tobacco consumption, acute bradycardia, laboratory measures of urea, and neutrophils (68).
Case 1. An 18-year-old man suddenly developed painful dysesthesias while living in Hong Kong. He recalled no prior illnesses besides some gastrointestinal distress and abdominal pain. The dysesthesias in his hands and feet waxed and waned but were exacerbated by eating certain foods (eg, chicken, fish, and bouillabaisse) and drinking alcohol. He had no weakness. The patient’s neurologic exam was normal, except for some minimal sensory loss to vibration in his feet.
Nerve conduction velocity studies demonstrated a polyneuropathy involving both the hands and feet. The F waves were mildly delayed in his lower extremities, and his distal sensory and motor latencies were mildly delayed with relatively intact amplitudes. EMG showed some chronic denervation, suggesting some prior axonal involvement.
The patient's syndrome was compatible with a CTX-induced neuropathy. The ingestion of fish and alcohol is well known to exacerbate CTX neuropathy.
Texas 1998 outbreak. Two cases of ciguatera fish poisoning were identified in attendees of a 1998 dinner party in Houston, Texas, where guests were served snapper and barracuda fillets caught from an oil-rig platform off the Texas Gulf Coast (30). None of the fish were saved for laboratory testing. Within 4 hours of the meal, a 50-year-old woman developed generalized pruritus and severe gastrointestinal symptoms, including diarrhea, abdominal pain, nausea, and vomiting. One day after the meal, she began experiencing arm and leg weakness. Two days after the meal, she developed tingling acral and perioral paresthesias and had hot-cold temperature sensation reversal. She recovered after several days. She reported no long-term effects. A 56-year-old man attended the same dinner party and became ill within 12 hours of eating the fish. He experienced myalgias and muscle stiffness, dysuria, a metallic taste in his mouth, and hot-cold temperature sensation reversal. As a fisherman, he knew the symptoms of ciguatera, assumed that he had the condition, and did not seek any medical treatment. He reported no long-term effects.
South Carolina 2004 outbreak. Two cases of ciguatera fish poisoning in a husband and wife were reported on August 10, 2004, after they ate fillets from a barracuda caught approximately 60 miles southeast of Charleston, South Carolina. Caribbean ciguatoxin was identified by high-performance liquid chromatography and mass spectrometry in a remaining portion of the barracuda fillet (30). The husband (age not reported) had diarrhea and abdominal cramping approximately 5 hours after eating the fish, followed by weakness, tooth pain, and the feeling that his teeth were loose, but he recovered within a few days with no long-term effects. The 36-year-old wife had nausea, vomiting, severe abdominal pain, and diarrhea 2 hours after eating the fish, followed by bradycardia; hypotension; dizziness; severe, generalized pruritus; reversal of hot and cold temperature sensations; and the sensation that the tops of her hands and feet were burning. She was hospitalized for 13 days and received intravenous fluids, promethazine for nausea, and low-dose dopamine. Eighteen months later, the patient still occasionally experienced slight tingling in her hands.
Shipboard outbreak. On December 9, 2021, a bulk carrier sailing from Higashiharima, Japan, to Gladstone, Australia, reported an outbreak of sudden illness, with 19 of 20 sailors on board reporting gastrointestinal and neurologic symptoms (96). On the previous day, all of the sailors consumed a self-caught barracuda and squid, which were prepared by the ship’s cook. Unconsumed samples of the fish and squid were sent for testing: the barracuda sample contained multiple ciguatoxins (P-CTX-1, P-CTX-2, P-CTX-3) with a total count of 3.40 ug/kg confirming the diagnosis of ciguatera poisoning. Five of the sailors (25%) were hospitalized. Symptoms included diarrhea (85%), abdominal pain (70%), myalgias (70%), vomiting (60%), paresthesias (40%), and a metallic taste in the mouth (5%); none had evident cardiac involvement.
|
• Ciguatera poisoning is contracted by eating any of a large number of species of fish that have been reported to contain ciguatoxins, including most of the common shallow-water oceanic game fish and many of the smaller colorful reef dwellers. | |
|
• Although it has long been assumed that larger fish within a given species are more likely to contain a significant amount of toxin, empirical studies have not supported this. | |
|
• Ciguatoxins generally produce channelopathies affecting particularly voltage-sensitive sodium channels and calcium and potassium channels in some cases. | |
|
• Significant slowing of sensory and motor nerve conduction velocities and F-wave latencies with prolongation of the absolute refractory and supernormal periods has been demonstrated in ciguatera poisoning. | |
|
• Ciguatera sensitization occurs when people previously intoxicated with ciguatoxin suffer a recurrence of typical ciguatera symptoms after ingesting fish that do not cause symptoms in ciguatoxin-naive individuals. |
The disease is contracted by eating any of the many species of fish that have been reported to contain ciguatoxins. These include most of the common shallow-water oceanic game fish and many of the smaller colorful reef dwellers. Common offenders include barracuda, snapper, jacks, grouper, Humphead wrasse, lionfish (including invasive Indo-Pacific lionfish in the western Atlantic Ocean), hogfish, kingfish, parrotfish, surgeonfish, rock hind, triggerfish, bigeye trevally, moray eel, and certain sharks (76; 08; 155; 32; 33; 152; 36; 37; 62; 35; 94; 164; 41).
Toxin-bearing fish appear healthy and are apparently not adversely affected by the toxin. The toxic substance, a lipid-soluble polyether, is acid and heat stable, tasteless, colorless, odorless, and not removed by any known cleaning method; nor is it inactivated by storage conditions, cooking, freezing, salting, drying, smoking, marinating, or gastric juices.
Although it has long been assumed that larger fish within a given species are more likely to contain a significant amount of toxin, empiric studies have not supported this (67); because no relationship between the proportion of toxic fish within a family and the relative total length of individual fish was observed, fish size cannot be used as a reliable predictor of fish toxicity (67). Deep-water fish (especially below 50 fathoms) tend to be safer, but exceptions have occurred (48). Cold water fish outside of the tropical areas are generally free of the problem (eg, flounder, cod, haddock, halibut, perch, scrod, sole, salmon), as are shellfish, including lobster and crab, although a case was reported from eating farm-raised salmon (56). The latter may be related to toxin-laden fishmeal, as even livestock have been contaminated through exposure to fishmeal.
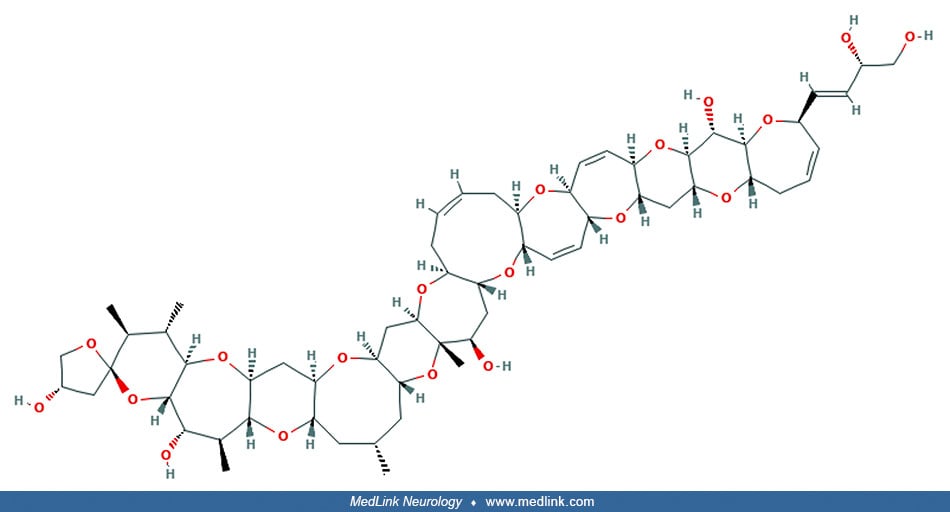
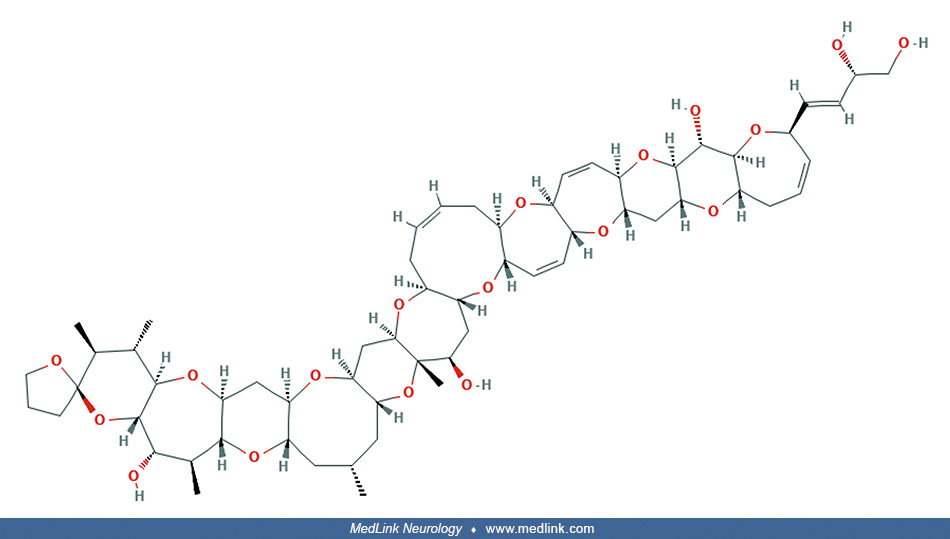
Ciguatera can be the clinical consequence of ingesting multiple toxins found in flagellate protists, in particular benthic dinoflagellates (ie, dinoflagellates occupying the ecological region at the lowest level of a body of water). Ciguatoxins are a class of toxic, high-molecular-weight, polycyclic polyethers. Several have been identified, including CTX-1, CTX-2, CTX-3, CTX4, scaritoxin (a mixture of CTX-4A and CTX-4B), maitotoxin (named from the ciguateric fish Ctenochaetus striatus—called "maito" in Tahiti), palytoxin, and okadaic acid (which can be involved in both diarrheic shellfish poisoning and ciguatera) (95; 168; 182).
A ciguatoxin was first isolated from Gambierdiscus toxicus, a dinoflagellate from the Gambier Islands (a small group of islands, remnants of a caldera, in French Polynesia in the Pacific Ocean) (09). Several additional dinoflagellates have since been demonstrated to harbor the toxins, some more toxic than G toxicus (169). These unicellular flagellated organisms can be found on bottom algae in tropical areas where herbivorous bottom-feeding fish scavenge for food. The same fish are later ingested by carnivorous fish, which may acquire high concentrations of ciguatoxin. Ciguatoxins can also accumulate in sea urchins and gastropods, which can produce ciguatera poisoning when they are eaten by indigenous populations of Pacific islands (50; 49; 70).
Initially considered to be anticholinesterases, ciguatoxins instead generally produce channelopathies affecting particularly voltage-sensitive sodium channels, but also in some cases calcium (eg, maitotoxin) and potassium channels (52; 153; 88; 175). In addition, some ciguatoxins interfere with enzyme systems or have hemolytic effects (125; 180), and others have both cholinergic and adrenergic effects, including inhibitory effects on nicotinic receptors or stimulant effects on muscarinic receptors (63; 115; 123). The order of potency of various ciguatoxins is (from most potent to least) CTX1B, CTX3B, CTX4A, gambierol, gambierone, and MTX3 (150).
CTXs are produced by dinoflagellates of the genera Gambierdiscus and Fukuyoa (163; 01; 43; 143). Field collections of Pacific reef fish showed that consumed CTXs undergo oxidative biotransformations, resulting in numerous toxic analogs (43; 131). CTX activity is present in all tissues of exposed fish, with the highest concentrations in the spleen (43). Muscle tissue retains the largest proportion of CTXs, with nearly half (44%) of the total tissue burden. Larger fish with slower growth rates assimilated a more than 6-fold higher proportion of ingested toxin in their flesh (13% vs. 2%).
A novel C-CTX analogue, C-CTX5, has been isolated from Gambierdiscus silvae and Gambierdiscus caribaeus strains from the Caribbean (118; 119). C-CTX5 from G silvae was confirmed to have voltage-gated sodium-channel-specific activity (118). Metabolism in vitro by fish liver microsomes converts algal C-CTX5 into C-CTX1/2, the dominant CTX in ciguatoxic fish from the Caribbean. There is variability in the enzymatic reduction at C-3 and C-56 of C-CTXs in reef fish, leading to variations in the ratios of CTX stereoisomers: in naturally contaminated fish tissues, C-CTX1/2 is a mixture of two diastereoisomers at C-3, whereas C-CTX3/4 is a mixture of two pairs of diastereoisomers at C-3 and C-56 (119).
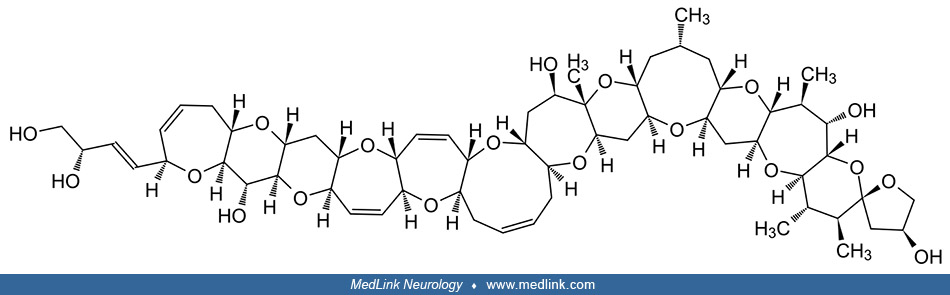
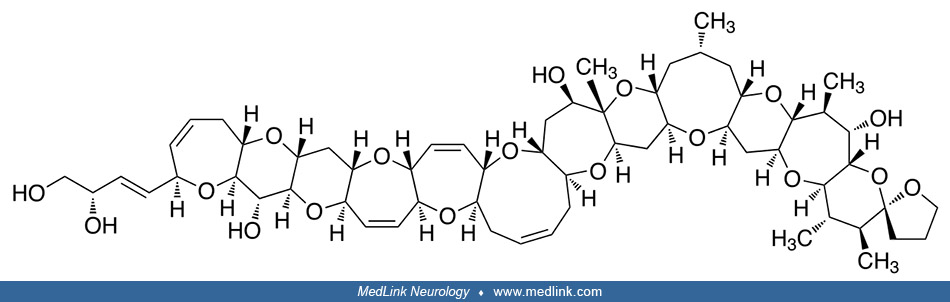
CTX-group toxins are structurally related to the brevetoxins (PbTx), another family of lipid-soluble polyether toxins, produced by the marine dinoflagellate Karenia brevis (01). K brevis is a microscopic, single-celled, photosynthetic organism commonly found in the waters of the Gulf of Mexico (110). It is responsible for the "red tides" that affect the Gulf coasts of Florida and Texas in the United States and the nearby coasts of Mexico.
Brevetoxin A, a group of neurotoxins isolated from the marine dinoflagellate Karenia brevis (formerly Gymnodinium breve).
Brevetoxin-1 (PbTx-1) R = -CH2C(=CH2)CHO
Brevetoxin-7 (PbTx-7) R = -CH2C(=CH2)CH2OH
CTX-1. Patch-clamping experiments demonstrated that CTX-1 increases neuronal excitability by shifting the voltage of activation of tetrodotoxin-sensitive Na+ channels to more negative potentials (81).
Pacific-CTX-1. Pacific-CTX-1 (P-CTX-1) is the most potent known ciguatoxin (150). It acts on tetrodotoxin-resistant Na+ channels by increasing the rate of recovery from Na+ channel inactivation in dorsal root ganglion neurons, suggesting a mechanism for the sensory symptoms associated with the toxin (165).
In animal experiments, P-CTX-1 can be detected in peripheral nerves within hours of exposure and persists for months; during this period, P-CTX-1 reduces the intrinsic growth capacity of peripheral neurons, which contributes to the delay in functional recovery (07).
Carribean-CTX-1. Carribean-CTX-1 (C-CTX-1) affects nerve excitability and neurotransmitter release at nerve terminals by inducing upregulation of Na+ channels and inhibition of K+ channels, at low nanomolar concentrations (113).
CTX-1 is particularly effective at releasing calcitonin-gene-related peptide (CGRP) from nerve terminals (170). In experimental animal studies, P-CTX-1 reduced delta and theta electroencephalogram activity and disrupted the balance of excitatory and inhibitory neurotransmitters in the motor cortex (97). In a mouse model, persistence of P-CTX-1 in the nervous system induced an irreversible motor deficit that correlated with excitotoxicity and neurodegeneration detected in the motor cortical neurons (06). In the Caribbean Sea and Atlantic Ocean, ciguatera arises from a multiplicity of CTXs, although one major form (C-CTX-1) is dominant (143).
Maitotoxins. Maitotoxins act on the calcium channel (74), likely leading to a harmful calcium-dependent generation of intracellular reactive oxygen species (183). Maitotoxins activate extracellular calcium channels, leading to an increase in levels of cytosolic Ca2+ ions (126). Although the exact molecular target of maitotoxins is unknown, maitotoxin may bind to the plasma membrane Ca2+ ATPase, turning it into an ion channel, similar to how palytoxin turns the Na+/K+-ATPase into an ion channel (161). A necroptosis cascade is ultimately activated, resulting in membrane blebbing and eventually cell lysis (Estacion 2001 Schilling 2001). In addition, maitotoxins can indirectly activate calcium-binding proteases calpain-1 and calpain-2, contributing to necrosis (176).
Gambierol. Gambierol blocks voltage-gated potassium channels (46).
Significant slowing of sensory and motor nerve conduction velocities and F-wave latencies with prolongation of the absolute refractory and supernormal periods has been demonstrated in ciguatera poisoning (26; 27). This nerve conduction slowing could be a consequence of nodal swelling, increased internodal length, and increased nodal volume, all of which have been demonstrated with in vitro ciguatoxins (16; 111; 112).
The multiplicity of toxins and their varied actions on nerve, muscle, and the neuromuscular junction, with accompanying presynaptic and postsynaptic effects, account for the diverse clinical manifestations related to the intoxication. The toxins cross the blood-brain and placental barriers and can be secreted in breast milk and semen.
Ciguatoxins produce cold allodynia, without producing heat or mechanical allodynia, by activating sodium channels and producing a large peripheral sensitization to dynamic cold stimuli in thinly myelinated A delta (Aδ) fibers (58). In human experiments using intracutaneous injection of low millimolar concentrations of CTX, brain responses are much less to constant cooling than with dynamic temperature changes cerebellum. Brain areas that respond to dynamic cold stimuli during cold allodynia are located bilaterally and include the medial insula, medial cingulate cortex, secondary somatosensory cortex, frontal areas, and cerebellum. The same brain areas also responded to a dynamic warming stimulus on the control site but remained silent to a dynamic warming stimulus on the injected site.
Ciguatera sensitization occurs when people previously intoxicated with ciguatoxin suffer a recurrence of typical ciguatera symptoms after ingesting fish that do not cause symptoms in ciguatoxin-naive individuals (20). The mechanisms underlying ciguatera sensitization remain undefined but apparently are not mediated by a channelopathy. Axonal excitability studies in patients with ciguatera sensitization found excitability parameters all within normal limits, arguing against dysfunction of axonal membrane ion channels in large-diameter fibers in ciguatera sensitization (174). Chronic ciguatera may involve serotonin metabolism with immune sensitization and delayed-type hypersensitivity (160). Inflammatory factors may also be important in chronic ciguatera. Pathologic activity of the complement/coagulation cascade has been demonstrated in patients with chronic ciguatera poisoning. In addition, gene expression profiling in brain, whole blood, and liver of mice exposed to CTX showed an acute anti-inflammatory response in the brain, blood, and liver that was postulated to represent a systemic antiinflammatory environment to protect against cellular damage caused by the toxin (154).
Most commonly, ciguatera results from a single exposure to ciguatoxin-contaminated fish, but continuous consumption of toxic fish over time may also produce ciguatera poisoning, even when the toxin concentration in the fish consumed is low (47).
Ciguatera fish poisoning affects an estimated 50,000 persons per year in tropical and subtropical latitudes (163). The risk uncertainty and the spread of Gambierdiscus have serious consequences for fisheries and food safety, particularly as most of the more than 400 fish species recognized as potential vectors of CTXs are high-valued commercial species. Ciguatera fish poisoning cases in Europe led to implementation of monitoring programs and fisheries restrictions with considerable negative impact on local economies.
Ciguatera is endemic in a band-like area extending around the globe, generally from 35° North to 35° South latitude (114). The highest incidence rates are consistently reported from two historical endemic areas, ie, the Pacific and Caribbean regions, a situation partly due to the strong reliance of local communities on marine resources (41). Ciguatera poisoning is particularly common in certain areas of the Caribbean (especially the Virgin Islands, Puerto Rico), parts of southern Florida, and certain Pacific regions (eg, Hawaii, Australia, and several of the islands of the South Pacific, including the Marshalls, French Polynesia, American Samoa, Guam, and New Guinea) (106). Cases have been reported from several states in the United States, the Mexican Pacific coast, Baja California, Canada, Japan, and, more recently, the Mediterranean. Some of this spread is due to the consumption of fish shipped in from endemic areas (142) or from travelers arriving home from endemic areas (135; 149; 93; 53; 122), whereas some of it is due to range expansion of ciguatera to subtropical regions because of climate change (40).
The incidence of ciguatera fish poisoning in endemic areas is estimated to be between 500 and 600 cases per 10,000 people (99; 42). Outbreaks of ciguatera fish poisoning have been associated with ingestion of warm water, reef-dwelling fish caught between latitudes +35° and -35°. In addition, flash freezing and shipping fish around the world has caused cases of ciguatera in nonendemic areas (80). Ciguatera poisoning has also been reported after the ingestion of farm-raised salmon (56).
Ciguatera toxin is the most common cause of neurotoxic foodborne outbreaks in the United States: a foodborne disease outbreak is defined as an incident in which two or more persons experience a similar illness after ingesting a common food, which is supported by laboratory or epidemiologic analysis (85). Most cases in the United States occur in Hawaii, Southern California, and Florida, with the incidence in Florida estimated to be five cases per 10,000 people (61; 14; 73).
Since the 1970s, nearly half of foodborne disease outbreaks of chemical origin have been caused by toxic fish or shellfish (with most of the remainder caused by poisonous mushrooms, heavy metal poisoning, excessive use in food of monosodium glutamate, and miscellaneous chemicals) (86); practices that contributed to the occurrence of ciguatera outbreaks included the inadvertent selection for consumption of toxic fish. Ciguatera toxin continues to be responsible for 40% of all foodborne disease outbreaks in Florida, and only 28% of these outbreaks are detected through complaints (106).
Ciguatera tends to be prevalent where recent algae blooms harbor the toxic dinoflagellates, which depend on a complex interaction of water temperature, disruption of underwater surfaces, and availability of nutrients. The highest rates of ciguatera fish poisoning in the Caribbean Sea and the West Indies between 1996 and 2006 were in the eastern Caribbean, where the water temperatures were highest and least variable (166). There also appears to be a temporal relationship in Hong Kong between the peak incidence of cholera outbreaks and ciguatera, which may be related to a common environmental trigger (98). Algae blooms may result from the availability of new surfaces produced by underwater explosions or recent construction of dams and seawalls. With the advent of dock construction, tourism, sewage outfall, global warming, and consequent coral bleaching, conditions favorable to G toxicus proliferation are increasing (102; 84). The eutrophication of marine environments (ie, excessive richness of nutrients in bodies of water, frequently due to runoff from the land) has also contributed to increasing levels of ciguatera; a study in Cuba found the level of organization of the local sport-fishing community and the degree of degradation of the local near-shore marine ecosystem to be key etiologic factors for the ciguatera outbreaks recorded in the 1990s (117).
Global warming has contributed to the emergence of dinoflagellate species in subtropical and temperate regions that had been limited to tropical areas (114; 40; 167). This may lead to increased ciguatera prevalence and an expanded range of high-risk endemic areas, although there is little evidence this has occurred (148; 167).
Globalization of the fishing industry and tourism have led to a progressive increase in ciguatera cases (114; 53). Ciguatera is the most common nonbacterial form of food poisoning related to seafood ingestion in the United States, Canada, and more recently, Europe (29; 100; 162). Annually, between 50,000 and 500,000 people develop acute ciguatera poisoning from consuming toxic fish, and approximately 5% of these individuals develop chronic ciguatera, a multisystem, chronic illness that can last for decades (159; 114).
The incidence of ciguatera poisoning was 0.67 cases per 10,000 patient-years in Martinique over the 6-year period from October 2012 to September 2018 (151). No patient died, but symptoms persisted in 40% of the 77 patients with follow-up at day 15.
Risk factors for ciguatera toxicity include alcohol consumption at least weekly, a history of previous ciguatera episodes, lower levels of education, and frequent fish consumption (147). Risk factors for severe ciguatera include ingestion of reef fishes and CTX-rich fish parts, ingestion of high-risk fish (eg, barracuda), as well as concomitant alcohol consumption (146; 35; 148). Concomitant alcohol consumption is associated with a much higher risk of developing bradycardia, hypotension, and neuropathic sensory changes (37).
Asian ciguatera outbreaks often present as large disease clusters due to group consumption of a single contaminated fish (41).
Ciguatera toxicity is underrecognized by medical providers, especially when patients present with ciguatera toxicity outside of endemic areas (140; 114; 94; 148).
|
• Ciguatera can be prevented by not eating fish from tropical waters, specifically tropical reef fish. | |
|
• The main species responsible for poisoning include jack, snapper, grouper, barracuda, and goatfish. | |
|
• Ciguatera cannot be prevented by cooking or freezing contaminated fish. |
Ciguatera can be prevented by not eating fish from tropical waters, specifically, tropical reef fish. The main species responsible for poisoning include jack, snapper, grouper, barracuda, and goatfish (23). Certain fish (including barracuda, grouper, hogfish, lionfish, and eels, among others) should never be eaten in endemic areas, and sale of these is often prohibited by law because of the recognized risk of toxicity (08; 32; 33; 36; 37; 62; 35; 55). The liver, other viscera, and roe of tropical fish may harbor high concentrations of ciguatoxins (78) and should be avoided in endemic areas. Because of the increased risk of severe symptoms, ingestion of CTX-rich fish parts with alcohol should be avoided (35). To prevent large outbreaks and severe illness, large apex predators from coral reefs should never be served at banquets (32; 37; 35).
Ciguatera cannot be prevented by cooking or freezing contaminated fish (94).
Several novel folkloric methods for detecting affected fish have been described.
In the Grand Caymans, local fishermen reportedly lay a fish down on the sand, and if ants are attracted, the fish is considered safe to eat (89). Experienced fishermen from tropical areas reportedly rub their gums with fish organs, and if their gums tingle afterward, the fish is not safe to eat (28).
Many other forms of food poisoning can mimic the initial gastrointestinal presentation of ciguatera, but most do not progress to involve other organ systems. In general, three classes of diseases can result from seafood consumption: allergies, infections, and intoxications (13). An allergic reaction, anisakiasis, results when people become sensitized to Anisakis (a genus of parasitic nematodes of fish and marine mammals) and then have an immunoglobulin E-mediated allergic reaction, potentially including anaphylaxis, after again eating fish infected with the organism (13). Scombroid is an intoxication due to ingestion of histamine that is formed when fish begins to decay; because histamine is also involved in allergic reactions, scombroid food poisoning resembles an allergic reaction and is often misidentified as a food allergy (13). Infections are usually self-limited and respond to supportive care, except for certain Vibrio species (57). The classic marine neurotoxic syndromes include shellfish poisoning, puffer fish ("fugu") poisoning (due to tetrodotoxin-induced inhibition of voltage-gated sodium channels in nerve cell membranes), and ciguatera (05). The symptoms of ciguatera and neurotoxic shellfish poisoning are often similar. Ciguatera, and particularly chronic ciguatera, is a consideration in the differential diagnosis of chronic fatigue syndrome (138).
|
• The diagnosis of ciguatera is based on appropriate clinical manifestations, a high index of suspicion, and a specific history of reef fish ingestion. | |
|
• A case definition of ciguatera fish poisoning has been proposed. | |
|
• There are no specific laboratory abnormalities in humans related to ciguatera, and there is no clinically available test for detecting ciguatoxins in human body fluids. |
The disease is vastly underdiagnosed; diagnosis is made almost entirely by history and usually in retrospect. There are few physical findings, none of which are diagnostic. Any combination of gastrointestinal, neurologic, cardiovascular, dermatological, genitourinary, and emotional symptoms should arouse clinical suspicion to inquire whether fish has been ingested.
Ciguatera can be confused with many other illnesses (159). The diagnosis of ciguatera is based on appropriate clinical manifestations, a high index of suspicion, and a specific history of reef fish ingestion (12). Note that ciguatera poisoning can present anywhere in the world, from eating fish shipped from affected areas or from travelers returning from trips to affected areas (133).
The combination of gastrointestinal symptoms and paresthesias, in combination with a likely source, can be used for early detection of ciguatera poisoning (96).
A case definition of ciguatera fish poisoning has been proposed (Table 1) (66). This case definition requires the presence of neurologic symptoms, but in documented outbreaks of ciguatera poisoning, patients may have gastrointestinal or cardiac symptoms without neurologic symptoms, leading to misdiagnosis or delayed diagnosis (15).
|
Critical criteria: | ||||
|
Required features: | ||||
|
1. Patient consumed a saltwater (marine) fish that has been previously associated with ciguatera fish poisoning.* | ||||
|
2. Patient reports neurologic symptoms, which may include any combination and sequence of paresthesia, dysesthesia, pruritus, allodynia, myalgia, and dizziness. | ||||
|
3. Symptoms onset within 48 hours after eating the fish. | ||||
|
Consistent features: | ||||
|
1. Gastrointestinal symptoms (eg, nausea, vomiting, diarrhea) may precede or accompany the neurologic symptoms. | ||||
|
2. Gastrointestinal symptom onset is usually within minutes to 12 hours after fish consumption. | ||||
|
3. Cardiovascular symptoms and signs (eg, hypotension, bradycardia) may be present. | ||||
|
Laboratory criteria: Confirmation of ciguatoxin(s) in a remnant of the implicated raw or cooked fish meal. | ||||
|
Epidemiological criteria: Exposure to the same fish source as a confirmed ciguatera fish poisoning case. | ||||
|
Case classification: | ||||
|
1. Confirmed case: Any patient meeting the clinical and laboratory criteria. | ||||
|
2. Probable case: Any patient meeting the clinical and epidemiological criteria. | ||||
|
3. Possible case: | ||||
|
a. Any patient meeting the clinical criteria after consuming a saltwater (marine) fish that is either not previously associated with ciguatera fish poisoning or is of an unknown species. | ||||
|
b. Any patient with an illness presentation that differs slightly from the clinical criteria or is an unusual presentation that, in the judgment of the healthcare provider, merits consideration for a ciguatera fish poisoning diagnosis. | ||||
|
c. Any patient who meets the clinical criteria, but other etiologies have not been ruled out. | ||||
|
Outbreak definition: Two or more cases that are epidemiologically related. | ||||
|
| ||||
There are also no specific laboratory abnormalities in humans related to ciguatera, and there is no clinically available test for the detection of ciguatoxins in human body fluids, although the situation is under intense study (22; 21; 127; 72).
Multiple bioassay methods and several sophisticated immunochemical methods for detection of ciguatoxins in fish have been devised for research studies but have not been widely employed in clinical medicine (82; 130; 182; 83; 104; 134; 144; 172; 59; 60; 105; 171; 132).
Reports of brain or spinal cord MRI findings in patients with ciguatera poisoning are limited (177; 107; 181). Wasay and colleagues reported a T2-hyperintense lesion in the cervical spinal cord (177), and Liang and colleagues reported similar MRI changes within the corpus callosum (107). Yalachkov and colleagues reported reversible intramyelinic cytotoxic edema symmetrically affecting distinct fiber tracts in two patients; in the more severely affected patient, there were marked diffusion-weighted imaging hyperintensities and apparent diffusion coefficient reductions throughout the corpus callosum, most pronounced in the splenium, as well as bilaterally in the pyramidal tract, ranging from the posterior portion of the internal capsule to the cerebral crus, and in the middle cerebellar peduncles (181).
Some patients with ciguatera toxicity may develop chronic symptoms (92). Chronic ciguatera is a clinical diagnosis. Common signs and symptoms of chronic ciguatera can include fatigue, myalgias, headache, diarrhea, cold allodynia, pruritus, and fluctuating paresthesias.
|
• Treatment is symptomatic and supportive. | |
|
• No known antidote exists. | |
|
• If vomiting has not occurred within 3 to 4 hours after ingestion, emetics or gastric lavage may be utilized to promote elimination of any remaining fish products and their associated toxins, though some discourage the use of emetics because they may exacerbate fluid losses. | |
|
• Activated charcoal combined with a nonmagnesium-containing cathartic in a slush can be administered to promote elimination of the toxin. | |
|
• Intravenous mannitol is considered the drug of choice for severe acute toxicity, especially within the first 24 hours, though this conclusion is not based on well-controlled studies. | |
|
• In severe poisoning, intravenous calcium gluconate (15 g/kg over 15 minutes, followed by a continuous infusion of 45 to 70 mg/kg until serum calcium is in midnormal range) has been recommended to counteract competitive inhibition of calcium by ciguatoxins. |
Treatment is symptomatic and supportive; no known antidote exists (72). In severe intoxication, basic support measures should be initiated with monitoring of fluid and electrolytes, cardiac function, and blood gases, with awareness that severe bradycardia and respiratory paralysis may occur and that complications stemming from severe dehydration may rarely become life-threatening.
If vomiting has not occurred within 3 to 4 hours after ingestion, emetics or gastric lavage may be utilized to promote elimination of any remaining fish products and their associated toxins, though some discourage use of emetics because they may exacerbate fluid losses. Activated charcoal combined with a nonmagnesium-containing cathartic in a slush can be administered to promote elimination of the toxin.
Intravenous mannitol is considered the drug of choice for severe acute toxicity, especially within the first 24 hours, though this conclusion is not based on well-controlled studies (121). Nevertheless, dramatic effects have been reported when given early, rapidly, and in adequate quantities (1 g/kg of a 20% solution intravenously over 1 to 2 hours). Mannitol has been used effectively in both children and adults with severe initial presenting symptoms, including coma (129; 139; 179). Care must be taken to adequately hydrate the patient, who may have had severe diarrhea and vomiting, and to attend to fluid deficits before and during mannitol use because of its potent osmotic diuretic action. Normal saline or Ringer lactate with additional electrolyte solutions should be used depending on vital signs, urine output, the amount of vomitus and diarrhea, and the results of laboratory studies.
Treatment with mannitol after the first 24 hours has had less dramatic results, and a double-blind study suggests that mannitol is not superior to normal saline in relieving symptoms and signs of ciguatoxin exposure at 24 hours and that mannitol has more side effects than normal saline (156). Nevertheless, one anecdotal report suggests potential benefit of mannitol treatment even a month after ciguatoxin exposure (157). Also, although the neuroprotective effect of mannitol in reducing the neurologic disturbances in ciguatera poisoning in people remains disputed, mannitol can reverse some toxic effects of ciguatoxin in vitro and in animal models (103; 145; 18).
Hypotension can usually be managed with volume replacement; pressor agents are rarely needed, but dopamine infusion (5 mg/kg per minute to 20 mg/kg per minute) can be used for severe and prolonged hypotension (38). Bradyarrhythmias usually respond well to atropine (0.01 to 0.02 mg/kg intravenously every 10 minutes for symptomatic heart rate less than 50 per minute), but transvenous cardiac pacing may be required in the presence of refractory bradycardia or heart block (38). Mechanical ventilatory support and oxygen may be needed in the event of respiratory failure.
In severe poisoning, intravenous calcium gluconate (15 g/kg over 15 minutes, followed by a continuous infusion of 45 to 70 mg/kg until serum calcium is in midnormal range) has been recommended to counteract competitive inhibition of calcium by ciguatoxins.
Certain additional medications may provide relief for individual symptoms. Benzodiazepines (eg, diazepam or lorazepam) and phenytoin have been helpful in treating associated convulsions. Indomethacin, ketorolac, and other nonsteroidal anti-inflammatory agents are useful for dysesthesias, myalgias, arthralgias, and pruritus. Acetaminophen may be more effective than other analgesics for associated headaches. Corticosteroids are reportedly useful for arthralgias not responsive to other anti-inflammatory compounds. Gabapentin and lamotrigine may be helpful in patients with shooting pains, pruritus, dysesthesias, and cold allodynia (141; 185; 58). Amitriptyline may help ameliorate some ciguatera symptoms, including pruritus (24; 51; 25; 108). Fluoxetine may help treat associated chronic fatigue symptoms (17).
There are also anecdotal reports of the use of multiple other medications for symptom relief, including calcium-channel blockers, chlorpromazine, diphenhydramine, H2-receptor blockers, mexiletine, neostigmine, tramadol, vitamin B complex, vitamin B12, tocainide, and procaine, among others.
A “serotonin-sparing” diet eliminating fish or fish products, shellfish or shellfish products, nuts, coconuts, nut products, seeds, seed products (including oils), alcoholic beverages or ethanol-containing products, mayonnaise, chocolate, and mushrooms has also been recommended while a patient remains acutely intoxicated and for 3 to 6 months after symptoms resolve (160).
Anti-ciguatoxin monoclonal antibodies have been developed that exhibit neutralizing activity against ciguatoxins in vitro and in vivo (87). Such work is a first step toward a safe and rational method for in vivo detoxification of ciguatoxins.
Treatment of chronic ciguatera toxicity involves supportive care and avoidance of food and environmental factors that exacerbate symptoms (92).
Although most pregnant women diagnosed as having ciguatera have been delivered at term with no apparent sequelae to the fetus, ciguatoxin apparently does cross the placental barrier and may cause premature labor and spontaneous abortion (137; 11). Transmission of ciguatoxin from mother to infant via breast milk has also been reported, producing diarrheal illness in the infant (11; 19).
An anecdotal report discusses implications in one case of uneventful anesthetic use without complications in a patient intoxicated 6 months previously who had residual muscle pains and weakness before surgery (128).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileMedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125