






Neuro-Ophthalmology & Neuro-Otology
Diplopia
Jan. 08, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The macula is the portion of the retina surrounding the foveal region. It is vital in discriminating high-contrast achromatic vision (visual acuity) and chromatic (color) vision. Macular pathology often leads to loss of these functions and image distortion, known as metamorphopsia.
Many disease processes affect the macula. The most prevalent is age-related macular degeneration, a leading cause of global blindness. Central serous chorioretinopathy results from changes in vascular permeability, characterized by the accumulation of subretinal fluid in the macular region. A third maculopathy results from the toxicity of hydroxychloroquine.
The diagnosis of macular diseases can sometimes be challenging. Patients often present with very subtle ophthalmoscopic abnormalities or features that mimic the clinical presentation of optic neuropathy. Optical coherence tomography, fundus autofluorescence, and retinal fluorescein angiography have been deployed as adjuncts to ophthalmoscopy.
|
• The macula is the retinal region responsible for visual acuity and color vision. | |
|
• Age-related macular degeneration is the most common maculopathy in adults, characterized by bilateral degeneration of the outer retina and choriocapillaris. | |
|
• Central serous chorioretinopathy typically presents with unilateral clear subretinal fluid in the macula and typically occurs in young to middle-aged men. | |
|
• Hydroxychloroquine toxic maculopathy can cause irreversible vision loss. Routine screening with multimodal imaging for early detection is crucial. | |
|
• Ocular imaging techniques such as optical coherence tomography, fundus autofluorescence, and fluorescein angiography can help diagnose and monitor macular diseases. |
The macula, also known as the macula lutea (macula = spot, lutea = yellow), refers to the area of the retina surrounding the fovea between the temporal vascular arcades. The retinal pigmented epithelium in the fovea is enriched with high concentrations of lutein and zeaxanthin, which give it the faint yellow (“luteal”) coloration.
The overlying ganglion cell layer of the macula is relatively thick because of the high concentration of photoreceptors and their retinal connections.
The outermost retinal layer adjacent to the choroid is the retinal pigmented epithelium. It plays a vital role in supporting the function and survival of photoreceptors by recycling visual pigments, removing waste products, protecting against phototoxicity and oxidative stress, and constituting the blood-retina barrier.
The inner side of the retinal pigmented epithelium lies in close contact with the retinal photoreceptors, the rods and cones whose nuclei form the outer nuclear layer.
The photoreceptors synapse with bipolar cells, whose nuclei comprise the inner nuclear layer. The bipolar cells synapse with ganglion cells, whose axons run parallel to the retinal surface and ultimately assemble into axon bundles that enter and travel in the optic nerve to the lateral geniculate nucleus.
The retinal arterial circulation comprises two systems: the central retinal artery and the choroidal arteries. The central retinal artery supplies the inner two-thirds of the retina. The capillary network of the choroidal vascular system, called the choriocapillaris, resides on the outer side of Bruch’s membrane and provides oxygen and nutrients to the outer one-third of the retina.
A slight surface depression in the center of the macula is called the fovea. The inner retinal tissue surrounding the fovea bends outward to allow light to reach the photoreceptors without being blocked, enhancing image resolution.
The radial organization of the outer plexiform layer is responsible for the “macular star,” a collection of lipid exudates that results from capillary serum leakage in optic disc inflammation, diabetic retinopathy, and hypertensive retinopathy. These exudates give rise to the ophthalmoscopic appearance of straight yellow lines radiating from the foveal center, in contrast to the irregular yellow patches seen in other retinal regions.
Maculopathies often display subtle ophthalmoscopic abnormalities, making them difficult to detect and differentiate from optic neuropathies.
A patient report of seeing flashes of light (photopsia) suggests a diagnosis of retinopathy (including maculopathy) rather than optic neuropathy. Another clue to retinopathy is visual difficulty in low light settings (night blindness, nyctalopia) or bright light settings (day blindness, hemeralopia). These symptoms suggest pathology of photoreceptors, as in hereditary (dystrophic) retinopathy, often known colloquially as “retinitis pigmentosa.”
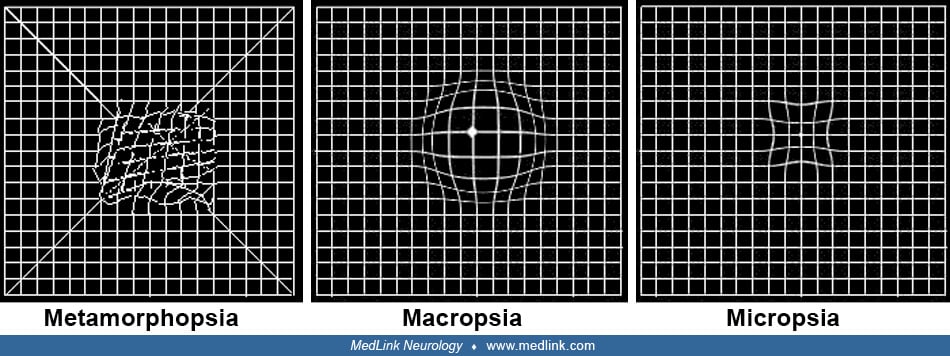
A report of seeing distorted imagery (metamorphopsia), minified imagery (micropsia), or magnified imagery (macropsia) favors maculopathy, especially when it occurs with viewing by just one eye. These image distortions result from disorders in photoreceptor arrangement. Metamorphopsia owes to irregular displacement, micropsia to spreading out, and macropsia to crowding of photoreceptors. These common disturbances in photoreceptor distribution result from foveal edema or scarring, as occurs in central serous chorioretinopathy, cystoid macular edema, and epiretinal membrane.
Symptoms of distorted imagery can be brought out on examination by having the patient view a grid of straight lines (“Amsler grid”). The patient will report that the lines are curved or that the boxes created by the grid appear focally larger or smaller.
The presence of a relative afferent pupillary defect favors the diagnosis of optic neuropathy rather than retinopathy (maculopathy). Only the most severe maculopathies will demonstrate a relative afferent pupillary defect, always subtle and only apparent if the pathology is asymmetric between the two eyes.
Color vision testing can help to differentiate maculopathy from optic neuropathy. In maculopathy, color vision loss occurs only when visual acuity is markedly depressed. By contrast, color deficiency may be present in optic neuropathy even when visual acuity is minimally depressed. In a special color test called the Farnsworth D100, the color deficiency in optic neuropathy is usually along a red-green axis, whereas in maculopathy, it is along a blue-yellow axis (Kollner’s Rule) (13).
The photostress (light bleaching) test can also be used to differentiate maculopathy from optic neuropathy. The patient’s visual acuity is tested using the standard method. The patient then views the bright light of a direct ophthalmoscope for 10 seconds. Immediately after that, the patient is instructed to read Snellen letters slightly larger than those previously correctly identified. If the patient requires more than 60 seconds to identify the larger letters, the test is “positive” and suggests a maculopathy. The explanation for a positive test result is that normal recovery of visual acuity after light-exposed bleaching of visual pigments requires intact photoreceptors. A delay of over 30 seconds suggests photoreceptor malfunction (07).
Optical coherence tomography and fundus autofluorescence have emerged as useful adjuncts to fluorescein angiography in diagnosing and monitoring macular diseases. OCT is a noninvasive imaging technique used to provide cross-sectional images of the macula. It readily detects structural defects within the substance of the retina.
Fundus autofluorescence is an imaging technique that relies on the natural fluorescence emitted by lipofuscin in the retinal pigmented epithelium. On fundus autofluorescence, areas of dysfunctional retinal pigmented epithelium appear exceptionally bright, and areas of retinal pigmented epithelium atrophy appear exceptionally dark. Fluorescein angiography is a test in which fluorescein dye is injected into an antecubital or forearm vein to highlight blood flow in the retina. It helps detect leakage and new blood vessels (neovascularization).
Epidemiology. Age-related macular degeneration is characterized by degeneration of the retinal pigmented epithelium, photoreceptors, and choriocapillaris in the macular area. It is the most common maculopathy in adults. A 2019 study estimated that 19.8 million Americans older than 40 years of age had age-related macular degeneration (18). Caucasians are at higher risk.
Manifestations. Patients with age-related macular degeneration commonly present with gradual binocular painless visual acuity loss. An early structural abnormality is drusen, a collection of lipofuscin deposits, which are waste products generated by retinal pigmented epithelium metabolic dysfunction. Appearing ophthalmoscopically as scattered yellow subretinal spots, drusen may be located between the retinal pigmented epithelium and Bruch’s membrane (basal laminar deposit) or inside the Bruch’s membrane (basal linear deposit).
An additional ophthalmoscopic sign of age-related macular degeneration is atrophy of the retinal pigmented epithelium and choriocapillaris in the macular region, which appears ophthalmoscopically as hypopigmented spots. Dysfunctional retinal pigmented epithelium may also disgorge melanin, visible as brown or black patches.
These signs characterize the “dry” form of age-related macular degeneration. If choroidal neovascular membranes appear, age-related macular degeneration is designated as “wet” because the choroidal neovascular membranes typically exude serum and leak blood.
Choroidal neovascular membranes are the primary cause of permanent vision loss in patients with wet age-related macular degeneration, who often present with acute vision loss from bleeding from these newly formed vessels. Bleeding induces subretinal fibrosis (macular disciform scar). This process is ruinous to vision.
Pathophysiology. Genetic studies have identified mutations in the complement factor H locus, which contributes significantly to age-related macular degeneration risks among Caucasians (19). Dysregulation of the complement system may lead to inflammation, lipofuscin accumulation, and oxidative stress, which result in drusen formation and retinal pigmented epithelium degeneration (09). In both forms of age-related macular degeneration, histopathology discloses macular loss of retinal pigmented epithelium, photoreceptors, and choriocapillaris with sparing of the inner retina. In wet age-related macular degeneration, there are areas of subretinal fibrosis and breaks in Bruch’s membrane.
Management. The Age-Related Eye Disease Study 2 (AREDS2) showed retardation in the progression of intermediate-stage dry age-related macular degeneration to advanced-stage age-related macular degeneration with the use of oral multivitamin supplements, including vitamin C 500 mg, vitamin E 400 IU, copper 2 mg, zinc 80 mg, lutein 10 mg, and zeaxanthin 2 mg (02).
The main treatment of wet age-related macular degeneration, with its choroidal neovascular membranes, is the intravitreal injection of anti-vascular endothelial growth factor, such as bevacizumab or ranibizumab (01). Anti-vascular endothelial growth factor therapy promotes regression of choroidal neovascular membrane and may even improve visual acuity. Photodynamic therapy and focal laser photocoagulation are alternative treatments. Advances in retinal stem cell transplantation have provided new--but unproven--hope for patients with age-related macular degeneration (14).
Epidemiology. Central serous chorioretinopathy is characterized by the pathologic presence of clear subretinal fluid in the macula. It typically occurs in men between the ages of 20 and 50 years. Corticosteroids delivered exogenously or endogenously have a strong association with the development of central serous chorioretinopathy (04; 08). Patients with extroverted personality types are said to be at increased risk (20).
Manifestations. Patients usually present with acute or subacute, mild to moderate, monocular visual acuity loss. The cause is an accumulation of macular subretinal fluid and a hyperopic shift from edematous, anteriorly displaced photoreceptors (15). Metamorphopsia, micropsia, or macropsia are common accompanying symptoms.
Examination shows subretinal fluid over the macular area, seen ophthalmoscopically as dullness of the foveal light reflex and mild elevation of the retina. Patients with central serous chorioretinopathy occasionally develop a relative afferent pupillary defect, which leads to a misdiagnosis of optic neuropathy. This feature emphasizes the importance of thorough macular examination in patients with suspected optic neuropathy.
OCT commonly shows a hyporeflective area of subretinal fluid in the macula.
Other OCT abnormalities include retinal pigmented epithelium detachment and an increase in subfoveal choroidal thickness, known as “pachychoroid.”
Fluorescein angiography may show leakage points at the interface between the choroid and outer retina. The leaking dye often begins as a small point that expands with hazy margins (“smoke-stack”).
In some cases, fluorescein angiography discloses new blood vessels that penetrate the Bruch’s membrane to enter the subretinal area (choroidal neovascularization). Bleeding from choroidal neovascularization can lead to subretinal or subretinal pigmented epithelium hemorrhage, a potential source of severe vision loss. Recurrent hemorrhage may eventually lead to atrophy of the retinal pigmented epithelium.
Pathophysiology. The pathophysiology of central serous chorioretinopathy is not fully understood. One theory is that upregulation of adrenergic receptors leads to increased sympathetic activity, choriocapillaris vasospasm, and ischemia-induced increases in choriocapillaris permeability (10). An alternative hypothesis is that activation of mineralocorticoid receptors causes the permeability change (03).
Management. In 80% of instances, the leakage resolves without treatment, but visual acuity may not return to normal. Metamorphopsia may also persist, with further episodes in about 30% of patients (06). Refractory central serous chorioretinopathy may be treated with a short course of corticosteroids or leakage point photocoagulation.
Epidemiology. Hydroxychloroquine was formerly an anti-malarial medication but is now prescribed mostly for patients with rheumatoid arthritis, systemic lupus erythematosus, and other autoimmune diseases. The risk of developing hydroxychloroquine maculopathy depends on the dose and duration of the medication. The estimated prevalence for patients who take the medication for more than 5 years is 7.5% (17). The ocular complication of hydroxychloroquine usually affects the macular after 5 years of consuming a daily dose exceeding 5 mg/kg or a cumulative dose of more than 1,000 gm. Patients with liver or kidney disease and who are taking tamoxifen concurrently are at increased risk of developing hydroxychloroquine maculopathy (11).
Chloroquine, which is used less commonly in clinical practice, is associated with a higher risk of developing maculopathy and with a more rapid progression of disease (05).
Manifestations. Patients with hydroxychloroquine maculopathy usually present with painless, slowly progressive, binocularly symmetrical vision loss. The primary site of pathology is the retinal pigmented epithelium, and secondarily the photoreceptors. The disease typically first affects the parafoveal region. At that stage, patients may be visually asymptomatic. But the damage spreads inward to involve the fovea and causes visual acuity loss in the late stage.
Subtle atrophy of the parafoveal retinal pigmented epithelium is the first observable change. Ancillary studies are more sensitive. For example, fundus autofluorescence highlights the retinal pigmented epithelium alterations. OCT demonstrates signal alterations in the photoreceptor layer (ellipsoid band) in the parafoveal and perifoveal zones. The remaining ellipsoid band at the foveal center resembles a saucer (“flying saucer sign”). Static perimetry reveals small scotomas within 10 degrees of fixation in the parafoveal area. The Humphrey 10-2 protocol is more sensitive than the more commonly used Humphrey 24-2 protocol in detecting these small defects close to fixation (21). Multifocal electroretinography shows reduced wave amplitude in the foveal region (12).
Ophthalmoscopy and fundus photography are not sensitive enough tests for hydroxychloroquine maculopathy. They are no longer recommended as screening tools for hydroxychloroquine maculopathy.
In the advanced stage of hydroxychloroquine toxicity, a ring of retinal pigmented epithelium atrophy around the fovea will be evident in ophthalmoscopy. This sign is known as “bull’s eye maculopathy.” At this stage, vision loss is usually irreversible and may worsen despite discontinuation of the medication.
Management. Once hydroxychloroquine maculopathy is diagnosed, the only approach to reduce the risk of further vision loss is to stop the medication. The retinal pigmented epithelium and photoreceptor loss is irreversible. Despite medication cessation, it is not uncommon for the vision loss to progress. This emphasizes the importance of routine screening and early detection.
The recommended screening protocol is to initiate examination 5 years after starting treatment with hydroxychloroquine. Patients with high-risk factors, including those with renal impairment, concurrent tamoxifen use, or are consuming more than 5 mg/day of hydroxychloroquine, should undergo annual screening starting after the first year of the treatment (16; 21). Due to their high sensitivity, OCT and fundus autofluorescence should be the screening methods. Visual field testing with Humphrey 10-2 should be added in patients with an abnormal OCT or fundus autofluorescence. Multifocal electroretinogram is adjunctive in patients with OCT or fundus autofluorescence abnormalities who do not have visual field defects.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Chaow Charoenkijkajorn MD
Dr. Charoenkijkajorn of Methodist Eye Associates in Houston, Texas, has no relevant financial relationships to disclose.
See Profile
Jonathan D Trobe MD
Dr. Trobe of the University of Michigan has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
Neuro-Oncology
Dec. 13, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 24, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuromuscular Disorders
Oct. 29, 2024
Developmental Malformations
Sep. 28, 2024