
Epilepsy & Seizures
Tonic status epilepticus
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Toxoplasma gondii is an important cause of congenital infections. When the infection occurs during pregnancy, the parasite can cross the placenta and severely damage the fetus, where the fetal brain and retina are particularly vulnerable. Microencephaly, intellectual disability, vision impairment, hydrocephalus, and epilepsy are common outcomes. In this updated article, the authors discuss the differential diagnosis of congenital toxoplasmosis, the ways in which infection with this parasite can be differentiated from other congenital infections, and management strategies for treatment before and after birth of an affected infant.
|
• Toxoplasma gondii is an intracellular parasite that can gravely damage the human brain and retina when infection occurs during pregnancy. | |
|
• The severity of fetal pathology is greatest when maternal infection occurs early in pregnancy, but likelihood of transmission to the fetus is greatest when maternal infection occurs in later pregnancy. | |
|
• Classic signs of congenital toxoplasmosis infection include intrauterine growth retardation, liver dysfunction, rash, chorioretinitis, and intracranial calcifications. | |
|
• Congenital toxoplasmosis is most commonly diagnosed serologically, but can also be diagnosed by real-time PCR or by the detection of parasites in fetal tissues. | |
|
• Newborns with suspected or confirmed congenital toxoplasmosis should be treated with a combination of pyrimethamine, sulfadiazine, and folinic acid for one year. |
Toxoplasma gondii, an obligate intracellular parasite of the phylum Apicomplexa and subclass coccidia, was first observed in 1908 in cells from the spleen and liver of the gondii, a North African rodent, from which the parasite derives its name. Twenty years later, chorioretinitis was recognized as a complication of human infection with T gondii. In 1939, observations linked congenital toxoplasmosis to intrauterine transmission of the parasite. The first serologic tests for toxoplasmosis were developed in 1948. It was not until the 1960s that cats were identified as the principal host of T gondii and the vector through which the pathogen most commonly reaches humans. In the mid-1970s, it became recognized that past infection with toxoplasmosis could reactivate in immunocompromised patients. Today, toxoplasmosis is recognized as one of the most common and important of the prenatal infections and accounts for the TO in the TORCH acronym guiding physicians in the workup of suspected congenital infections.
|
• Congenital toxoplasmosis can result in varying degrees of chorioretinitis, structural brain abnormalities, hydrocephalus, and developmental delay. | |
|
• When vertical transmission from mother to fetus occurs during the first trimester of pregnancy, the manifestations on the fetus will be the most severe. | |
|
• Maternal to fetal transmission is most likely to occur when the mother is infected in the third trimester. |
Congenital infection with T gondii occurs during infection of the mother. Risk to the fetus is greatest during primary maternal infection (38). The risk of primary infection during pregnancy is related to the mother's antibody status and to the intensity of exposure to T gondii oocysts. The parasite disseminates hematogenously to the placenta, where it may cross to the fetus.
The period of gestation during which the maternal infection occurs is critical to the risk of mother-to-fetus transmission and to the severity of the fetal infection. Studies have shown substantial variability in vertical transmission rates, but all have found that the rate increases with gestational age (83; 55; 32). Across all studies, transmission of the parasite to the fetus most readily occurs during the third trimester (Table 1). In contrast, the likelihood of severe disease is greatest when the infection occurs during the first trimester. Although many fetuses infected with T gondii during the first trimester will have substantial neurologic disease as newborns, most fetuses infected during the third trimester will be asymptomatic as neonates. If left untreated, however, as many as 85% of these children may develop chorioretinitis or developmental delay during childhood (61).
|
Trimester |
Risk of infection |
With treatment |
|
1st |
25% |
8% |
Congenital toxoplasmosis typically results from acquired infection in nonimmune women. However, infants with congenital toxoplasmosis have been born to immunocompetent women with prior histories of toxoplasmosis infection and with evidence of prior immunity (46). This can occur when a previously-infected pregnant mother is reinfected with a new and more virulent strain. Most commonly, this happens when a woman travels internationally or when she eats undercooked meat from regions in which more virulent strains of toxoplasmosis predominate (52). In addition, intrauterine transmission of the parasite can occur during reactivated T gondii infections in HIV-infected women. Toxoplasmic reactivation in HIV-infected women who are immunosuppressed can result in severe congenital toxoplasmosis (04).
Although congenital toxoplasmosis most commonly results from primary maternal infections during the first trimester, resulting in seropositivity during the pregnancy, important exceptions to this pattern can occur. Congenital toxoplasmosis can result from maternal infections during the several weeks or months immediately preceding pregnancy. This is especially true if the mother still has signs of acute infection, such as cervical adenopathy, at the time of conception. Conversely, maternal toxoplasmosis infections may occur very late in pregnancy, so that a mother has not yet seroconverted by the time of delivery. Thus, toxoplasmosis may pose a risk to the fetus even if the infection precedes the onset of pregnancy or if the mother remains seronegative at parturition. These possibilities illustrate the importance of routine risk assessment for toxoplasmosis during pregnancy and the requirement to adapt screening strategies to special situations (17).
There is evidence in murine models and early support in human populations that a more robust maternal immune response, as exhibited by higher antibody levels and lymphocytic proliferation, was positively associated with a greater chance of vertical transmission of toxoplasmosis from mother to fetus. Thus, although elevated maternal antibody levels likely prevent a more severe presentation of acquired toxoplasmosis, their presence just before or during pregnancy may actually signal an increased risk that the fetus will acquire disease (30).
A review of infants born to mothers with primary infection who were not treated with antibiotics indicated that 6% of infants were stillborn, 39% were not infected, and 55% were infected (74). Among infected infants, 75% were asymptomatic, 16% had mild infections, and 8% had severe disease.
Maternal toxoplasmosis increases the risk of premature birth. One study showed that premature delivery occurred in 25% of infected mothers, compared to 9% in uninfected mothers (26).
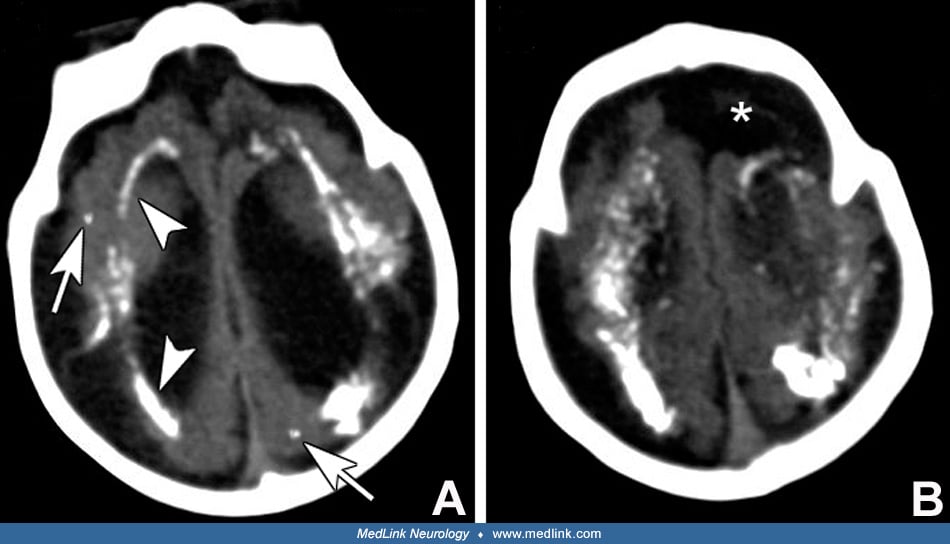
Infants with congenital toxoplasmosis display a spectrum of signs and symptoms that resemble congenital cytomegalovirus infection. Common manifestations of congenital toxoplasmosis include intrauterine growth retardation, jaundice, hepatosplenomegaly, petechial skin rash, chorioretinitis, microcephaly, and macrocrania (due to hydrocephalus). Compared to infants with congenital cytomegalovirus infections, infants with congenital toxoplasmosis more often have chorioretinitis and hydrocephalus. Cranial CT often reveals intracranial calcifications, hydrocephalus, or cystic changes.
In one study of 18 children with congenital toxoplasmosis, 11 patients were symptomatic at birth (32). Eight of the newborns had chorioretinitis, and six of these had active disease. An additional seven infants had retinal scarring, five of which involved the macula. Six of the patients had hydrocephalus diagnosed via cranial ultrasound, and five had intracranial calcifications on CT imaging. Of these 18 infants, 38.8% were born prematurely.
Sometimes, congenital toxoplasmosis presents in the newborn with a sepsis-like picture, including hypotension, acidosis, and multiorgan system failure. Because this scenario so closely resembles classic bacterial neonatal sepsis, diagnosis of toxoplasmosis is often delayed until negative blood and CSF cultures for bacteria trigger suspicion that a different type of pathogen may be responsible (02).
Sequelae of untreated, symptomatic congenital toxoplasmosis include vision loss (75%), hearing loss (27%), intellectual disability (60%), cerebral palsy (70%), epilepsy (80%), and hydrocephalus or microcephaly (30%) (74; 84; 80; 32). However, aggressive anti-toxoplasma therapy and neurosurgical intervention reduce the likelihood of permanent neurodevelopmental sequelae from intrauterine toxoplasmosis. In one trial, 79% of treated infants had mental development within the normal range, and children with hydrocephalus responded favorably to shunt placement (80). Visual loss commonly occurred despite treatment. Infants with high cerebrospinal fluid (CSF) protein and passive ventriculomegaly (“hydrocephalus ex vacuo”) have a less favorable prognosis (56; 80). Infants with subclinical congenital infection may develop manifestations of toxoplasmosis, especially chorioretinitis, later in childhood.
In the majority of immunocompetent children and adults, including greater than 50% of pregnant women, acquired infections are asymptomatic (32). However, approximately 10% of immunocompetent individuals experience lymphadenopathy, malaise, and fever. Toxoplasma infection can cause disseminated, life-threatening disease in immunocompromised persons. CNS toxoplasmosis in CD4-deficient AIDS patients occurs at rates of 1 to 3 per 100 person years (01). Toxoplasma infections in such individuals can be the result of primary or reactivated latent infections.
Classic complications of congenital toxoplasmosis include chorioretinitis, cerebral calcifications, and hydrocephalus. Microcephaly, seizures, hearing loss, strabismus, hepatomegaly, splenomegaly, pneumonia, thrombocytopenia, and anemia are also commonly observed.
Outcomes vary considerably, but children with microencephaly and cerebral calcifications are almost always severely affected with spastic quadriplegic cerebral palsy, cognitive impairment, and epilepsy (03).
Each year, congenital toxoplasmosis is responsible for approximately 1.9 million disability-adjusted life years, which the World Health Organization defines as years of complete health lost to premature death, disability, or poor health status (25). In children with congenital toxoplasmosis, the most frequently involved organ is the eye. Fifteen-year follow-up of infants in the United States who were diagnosed with congenital toxoplasmosis showed that 92% of them developed chorioretinitis. In untreated children, the development of new ocular lesions occurred in 90% (32).
The patient was a male infant born to a gravida 3 para 2 (now 3) married Caucasian woman. The woman had delivered two children previously, both of whom were healthy. The baby was born at 39 weeks’ gestation following a pregnancy complicated only by a mild “flu-like” maternal illness of 1 week’s duration during the first trimester. In retrospect, it was noted that this illness began 10 days after the family had purchased a domestic kitten. The mother’s symptoms had included malaise, low-grade fever, sore throat, and myalgia. The maternal illness was self-limited and she did not seek medical care for it. The mother received routine prenatal care but elected not to receive any prenatal ultrasound testing.
The infant was born by normal spontaneous vaginal delivery, which was complicated by late decelerations in the late stages of labor. The newborn’s birth weight was 2450 grams (small for gestational age), and he was depressed at birth. APGAR scores were 3 at 1 minute, 5 at 5 minutes, and 7 at 10 minutes. On delivery, he appeared moderately cyanotic and had poor muscle tone. Heart rate was initially 40 to 60 beats per minute, and he initially made poor respiratory efforts. He required vigorous resuscitation with chest compressions and bag-valve-mask ventilatory assistance. After several minutes of resuscitation, his clinical condition improved. The heart rate rose to 110 to 130, and spontaneous respirations became adequate.
The baby was admitted to the Newborn Intensive Care Unit (NICU) for suspected sepsis. In the NICU, the general physical examination revealed hepatomegaly, splenomegaly, generalized lymphadenopathy, and a maculopapular rash over the trunk and extremities. On neurologic examination, he was lethargic, generated few spontaneous movements, and was hyporesponsive to tactile stimuli. His pupils were round and equal but minimally responsive to light. He had a generalized hypotonia. His head circumference was 32 cm, which was small for gestational age but proportional to body weight. The anterior fontanelle was open but less than 1 cm in diameter.
Laboratory testing revealed anemia (hemoglobin = 11.5 g/dl), thrombocytopenia (platelet count = 96,000/ml of blood), and elevated liver enzymes (lactic acid dehydrogenase = 226 mU/mL, serum glutamic oxaloacetic transaminase = 450mU/mL). CSF examination revealed a pleocytosis (56 white blood cells per ml), two red blood cells per ml, elevated protein content (186 mg/dl), and normal glucose content.
The head CT scan was markedly abnormal. It revealed ventriculomegaly of the lateral ventricles as well as periventricular and multifocal parenchymal calcifications.
Diagnostic workup included blood, urine, and CSF cultures, a urine culture for cytomegalovirus, a PCR of CSF for herpes simplex virus, a rapid plasma reagin test for syphilis, and a rubella serology study. All of these studies were negative.
Serologic tests for toxoplasmosis were positive. On the second day of life, the infant had T gondii-specific IgM antibodies (1:400) and IgG antibodies (1:800). The mother also had positive T gondii-specific IgG antibodies (1:400) but not IgM antibodies.
The ophthalmology service was consulted. Examination of the eye structures with an indirect ophthalmoscope revealed bilateral chorioretinitis.
The infant was diagnosed with congenital toxoplasmosis. He was treated with a combination of pyrimethamine and sulfadiazine for four weeks.
The NICU course was complicated by multiple medical issues, including feeding problems, liver dysfunction, thrombocytopenia, anemia, and seizures. Hyperbilirubinemia emerged on the second day of life and required phototherapy. Seizures began on the third day of life and consisted of multifocal clonic activity. The seizures were well controlled with phenobarbital. Due to poor feeding, a gastrostomy tube was placed. Because of the ventriculomegaly, serial head ultrasound examinations were performed. The size of the ventricles did not increase over time. It was determined that the ventriculomegaly was chiefly due to hydrocephalus ex vacuo. Thus, placement of a ventriculoperitoneal shunt was not required. He was discharged to go home on the 28th day of life. Follow-up titers on the infant at two months of life revealed negative IgM antibodies, whereas IgG antibodies had risen to 1:3200.
The child has remained neurologically and developmentally abnormal throughout life. At age 6 years, he has intellectual disability, spastic quadriparesis, and epilepsy. He is microcephalic, and he remains feeding tube-dependent. He has some receptive language skills but no expressive language. Due to shortened heel cords, he became unable to ambulate at age 5 years. He required bilateral heel cord lengthening and can now ambulate for short distances. He has multiple seizure types, including atypical absence seizures, myoclonic seizures, and generalized tonic-clonic seizures (Lennox-Gastaut syndrome). The seizure disorder is partially controlled by topiramate.
|
• Congenital toxoplasmosis is due to infection of the fetus with Toxoplasma gondii, an obligate intracellular parasite. | |
|
• Humans can become infected by ingesting oocysts in unclean food or water, by ingesting undercooked meat, by organ transplantation, or by vertical transmission from mother to fetus. |
Toxoplasmosis, in all of its forms, is due to infection with Toxoplasma gondii, an obligate intracellular parasite that can infect all warm-blooded animals, including mammals and birds. The parasite has three infective stages, only the first two of which are found in humans and other intermediate hosts (23). The first stage is the rapidly dividing tachyzoite stage. This stage differentiates from the oocyte following ingestion, at which time it invades the host’s intestinal cells to reproduce asexually. Once the parasite overwhelms the host cell, necrosis occurs, leading to cell rupture and release of the tachyzoites to infect other cells and to enter the bloodstream (55). Therefore, the tachyzoite stage is the disseminating form that can invade all nucleated cells and cause the most tissue damage. Because it can target virtually all cells, the pathogen can infect all organs of a host.
The second stage is the quiescent bradyzoite stage. This is the stage in which the pathogen reverts to a chronic infection. In this stage, the parasites reside by the hundreds or thousands within tissue cysts, which can persist for the life of the host. Tissue cysts are generally confined to muscle, retina, and brain.
The third and final stage, which is the sporozoite-containing oocyst, is generated in the intestinal tract. Each oocyst contains two sporocysts, which in turn hold four sporozoites. This stage, however, occurs only in cats. It is for this reason that cats are considered the definitive host of the parasite (55). Infected felines shed enormous quantities of oocysts, as many as 1 million per day. The oocysts become infectious approximately 48 hours after excretion and can remain viable in warm, moist soils for a year or more.
All three infective stages are eliminated by heating above 65º C and are killed by cooking. However, the three stages are differentially vulnerable to freezing. Although tachyzoites and bradyzoites are typically killed by freezing for several weeks, oocysts can survive freezing for months (78).
Humans can become infected with T gondii in four ways. First, and probably most commonly, humans can become infected by directly ingesting oocysts, via the consumption of unwashed raw vegetables or contaminated water, or through unwashed hands after gardening or other outdoor activities, or by contact with infected cats (79). Second, because infectious T gondii resides as tissue cysts within muscle tissue of many animals and birds, carnivorous humans can become infected via ingestion of undercooked meat. Third, because T gondii can reside within multiple human organs, uninfected people can become infected when they receive an organ transplant or blood transfusion from an infected donor. Fourth, vertical infection can occur when a maternal primary infection occurs during pregnancy, and tachyzoites are transferred across the placenta during maternal blood stream dissemination.
There is possibly a fifth way in which humans can become infected with T gondii, and that is by sexual transmission. In particular, male to female transmission of T gondii infection is known to occur in several nonhuman mammalian species, including rats, dogs, and goats. A study has found that toxoplasma tissue cysts are present within the semen of infected human males, thus strengthening the notion that toxoplasmosis may be a venereal disease. However, it has not yet been proven that these cysts are viable or that they can successfully initiate and establish infection in sexual partners. If this infection can be successfully transmitted sexually from males to females, then this may explain the poor efficacy of educational campaigns that strive to reduce risk of congenital toxoplasmosis. Further research may lead to the addition of T gondii to the list of sexually transmitted diseases (87).
A risk factor analysis demonstrated that highest risk behaviors include eating raw ground beef, rare lamb, or locally produced cured, dried, or smoked meat; working with meat; or drinking unpasteurized goat milk. Possessing three or more kittens also carries a high risk of infection (37); however, the majority of women with primary gestational infections have no identifiable risk factors and remain asymptomatic (73). The lack of evident risk factors in these women may be due to sexual transmission from their male partners.
The trophozoite (also called a tachyzoite or proliferative form) can invade nearly all mammalian cells. Trophozoites reside in the cytoplasm of infected cells, releasing progeny parasites or pseudocysts. Tissue cysts can persist for the duration of the infected host's life. Each cyst may contain up to 3000 bradyzoites. The parasites are phagocytized in the ileum, multiply, and rupture from host cells. The organisms can be killed by neutrophils. However, tachyzoites remain viable in macrophages and spread hematogenously to many organs, including the placenta, where congenital transmission occurs (83). In congenital toxoplasmosis, infection of the brain and retina are particularly prominent. This pattern of infection leads to periaqueductal inflammation, aqueductal obstruction, hydrocephalus, tissue necrosis, parenchymal calcifications, and chorioretinal scars.
Among fetal tissues, the brain and retina may be particularly vulnerable because they are immunologically protected. An evaluation of infected fetuses, who were electively aborted during the second trimester after the mothers had developed IgG antibodies against T gondii, found that the stage of the parasite and its potential for further tissue damage were different in the fetal brain and retina than in all other fetal tissues. In particular, the placenta, fetal adrenal, and fetal heart possessed tissue cysts, but few or no tachyzoites. Thus, in these tissues, there was evidence only of a chronic infection. In contrast, the fetal brain and retina still possessed large numbers of actively dividing, tissue-destructive tachyzoites. Because the brain and retina are immunologically protected, maternal (and fetal) immune mechanisms are likely impaired in those regions, thus, allowing the parasite to proliferate and damage tissues for a longer period and to a greater extent than in other fetal organs (24).
The precise mechanisms by which toxoplasmosis disturbs brain development are unclear. However, the presence of microcephaly, focal cortical dysplasia, and generalized brain dysfunction suggests that the infection disturbs multiple facets of brain development. Indeed, a study examining the effects of Toxoplasma gondii on cultured neural progenitor cells in vitro has shown that the intracellular parasite reduces neuronal proliferation and disturbs neuronal migration and differentiation. Thus, it is likely that the infection damages the developing brain, not just through immune-mediated mechanisms, but also by directly disturbing developing brain cell function and maturational processes (70).
Some of the damage to infected CNS tissues may be due to the glial scars that form in response to the infection. A mouse model of congenital ocular toxoplasmosis showed that GFAP and vimentin protein levels increased significantly in Muller cells, along with photoreceptor depletion, suggesting that infection-induced reactive gliosis may be responsible for retinal damage and loss of vision in human ocular toxoplasmosis cases (45).
|
• Cats are a major reservoir of Toxoplasma gondii. | |
|
• The disease is found throughout the world, but infection rates are typically higher in areas with limited access to healthcare. |
One third of the global population is infected with Toxoplasma gondii, with variation among individual regions and countries. Toxoplasmosis is especially prevalent in Europe, Central America, Brazil, and Central Africa (32). The prevalence of this disease is tied to the dietary and hygiene habits of the population as well as exposure to cats. Prevalence is more common in rural areas, areas of low income, and those with more limited access to health care resources. Developing countries with higher seroprevalence rates (up to 80%) of Toxoplasma gondii were also found to have a higher frequency of congenital toxoplasmosis when compared to more developed regions, where seroprevalence ranges from 10% to 50% (09; 55).
Three clonal lineages of Toxoplasma gondii– types I, II, and III–have been genetically characterized and may contribute to regional discrepancies in disease severity. Type I strains display higher virulence and are related to more severe clinical manifestations, such as ocular disease and acute inflammatory response. This lineage is most prevalent in Central and South America, where severe presentations of toxoplasmosis are found. Types II and III, although less virulent, more readily differentiate into bradyzoites, allowing the formation of tissue cysts and transition to the latent phase of toxoplasmosis. Type II parasites are more prevalent in North America and Europe, whereas type III strains are more commonly found in North and South America (22).
In the United States, the seroprevalence of Toxoplasma gondii is lower in females than in males. In addition, in the United States, it is more prevalent in those of low income, low education, and older age (68). This information may help direct future programs for prevention of vertical transmission of Toxoplasma gondii from mother to fetus.
Data regarding temporal trends in toxoplasmosis infections worldwide are scarce. Nevertheless, studies suggest that the seroprevalence of toxoplasmosis is slowly declining in many countries. The factors driving this reduction in seroprevalence are not known for certain but are probably multiple and involve reductions in the ways in which humans are exposed to the bradyzoite, oocyst, and tachyzoite stages of the parasite. For example, farming practices that lower the risk of livestock infections likely reduce human exposure to T gondii bradyzoites in their food. Sufficient cooking and freezing of meat prior to consumption and sheep vaccination in some countries would similarly reduce this exposure. Improvements in water, sanitation, and hygiene, along with culling of stray cat populations and keeping pet cats indoors reduces human exposure to oocysts. Reduction in tachyzoite exposure could be occurring through safe needle use and milk pasteurization. Whatever the cause or causes underlying reductions in toxoplasmosis seroprevalence, this trend will likely also lead to reductions in congenital toxoplasmosis (57).
Felines, especially domestic cats, serve as the major reservoir of infection in most regions of the world. Approximately 20% of cats possess serologic evidence of toxoplasma infection, but only 1% actively shed oocysts. Toxoplasma tissue cysts can be found in the skeletal muscle of 20% to 30% of pigs, sheep, and cattle worldwide.
Until recently, it was assumed that all domestic cats were equally prone to infection with toxoplasmosis. However, studies have shown that domestic cat breeds differ substantially in their seroprevalence for Toxoplasma gondii. Long-haired cats have much greater seroprevalence than short-haired cats. Among the tested breeds, Persian cats had the highest seroprevalence (60%), which was greater than three times the rate seen in Burmese cats, which had the lowest seroprevalence (18.8%). Studies have also revealed that seroprevalence varies with age, as older cats are more likely to be seropositive than younger ones. The “lifestyle” of the cat also influences its likelihood of infection. Cats that consume raw meat are much more likely to be seropositive than those that don’t. However, although seroprevalence varies with cat breed, age, and lifestyle, all domestic cats are susceptible to toxoplasma infection and can serve as a source of infection to humans (62).
Although cats are the only species that can shed toxoplasma, many other species can be infected. Consumption of those species by humans and other animals can lead to infection. Toxoplasma tissue cysts can be found in the skeletal muscle of 20% to 30% of pigs, sheep, and cattle worldwide (52).
The global incidence of congenital toxoplasmosis is estimated at 190,100 cases per year, or about 1.5 cases per 1000 live births (83). Four hundred to 4000 cases of human congenital toxoplasmosis occur each year in the United States. About 750 deaths are attributed to toxoplasmosis each year (50).
The parasite is widely distributed and may infect as many as one third of all persons worldwide (27). The prevalence of antibodies to T gondii in women of child-bearing age varies according to age, geographic location, and dietary practices. Approximately 12.5% of the population in Norway, 25% in Finland and Sweden, 27% in New York, and 84% in Paris exhibit serologic evidence of previous infection with T gondii (42). Annual rates of acquired T gondii infection range from less than 1% to 3% or higher per year. Infection rates among pregnant women range from approximately 1 per 10,000 in certain areas of the United States to as high as 1 per 100 in France (74; 05; 36). A study of 1037 pregnant women in Benin showed a seroprevalence of T gondii of 52.6%, with a seroconversion rate of 3.4% and a 0.2% rate of congenital infection (32). Comprehensive serologic screening of newborns in Massachusetts detected a rate of congenital toxoplasmosis of approximately 1 per 12,000 live births (36). The overall incidence of maternal toxoplasma infection and, hence, congenital infection, depends on the prevalence of the organism in the environment.
In addition to environmental factors and gestational timing of infection, genetic factors of the fetus and mother may also play important roles in determining the incidence and severity of congenital toxoplasmosis. Polymorphisms in two fetal genes, COL2A1 and ABCA4, are associated with ocular and brain disease in congenital toxoplasmosis. These two genes play roles in brain and eye development. Thus, isotypes of these genes may influence the way in which toxoplasmosis disrupts brain and eye development or may affect the ways in which the toxoplasma parasite replicates or disseminates within developing tissues (35).
Genes affecting the immune response–whether maternally derived or fetally derived–may also influence the clinical outcome of congenital toxoplasmosis (51). For example, the NALP1 gene encodes a protein that forms inflammasomes, an important component of the innate immune response that triggers proinflammatory cytokines on cellular infection. Susceptibility for human congenital toxoplasmosis has been linked to allelic differences in NALP1 (91). A study has yielded further evidence regarding the importance of the innate immune response. Numbers of CD11b(+) Gr-1(+) cells in the placenta were found to increase significantly on T. gondii infection, thus, suggesting that the innate immune responses is an important part of the immunity against T. gondii infection via the feto-maternal interface (85). Furthermore, TLR4 and TLR9 SNPs may protect fetuses against congenital toxoplasmosis, according to a small study (93).
Controversy has arisen as to whether congenital toxoplasmosis should be included universally in newborn screening. Proponents argue that congenital toxoplasmosis should be included in newborn screening because the disorder is (a) relatively common (more common than phenyl ketone urea), (b) easily missed at birth if laboratory testing is not conducted, (c) effectively detected by newborn screening techniques, (d) damaging to the child if the disorder is undetected, and (e) effectively treated by medical therapies (41; 82). Others have argued that the incidence of congenital toxoplasmosis is too low to warrant routine surveillance and that there is lack of clear evidence that the benefits of treating asymptomatic infected infants outweigh the risk of harm (28). Further studies designed to assess the disease burden of congenital toxoplasmosis and the efficacy of treatment will likely be needed before newborn screening for congenital toxoplasmosis becomes universal. In some European countries (Austria and France for example) with higher incidence of toxoplasma infections, surveillance programs to monitor for and treat primary gestational infection with toxoplasma gondii are part of mandatory prenatal care. Results from the Austrian toxoplasmosis register from 1992 to 2008 revealed a decreased incidence of congenital toxoplasmosis since the implementation of mandatory prenatal screening compared to historical data (reduced from 78 per 10 000 live births to 1 per 10 000 live births) (73).
|
• Because congenital toxoplasmosis has the most severe effects on the fetus when the mother is infected early in pregnancy, adequate prevention measures must attempt to educate on exposures even before conception. | |
|
• Effective preventative education measures have focused on proper cooking of meat, safe food preparation, and avoidance of cat feces. | |
|
• Preventative education reduces the rates of seroconversion during pregnancy. | |
|
• Prenatal identification followed by treatment of pregnant women who are infected with Toxoplasmosis gondii reduces the rate of transmission to the fetus. |
Before they conceive, pregnant women and those attempting to conceive need to be educated about the risk of congenital toxoplasmosis and the means to reduce the likelihood of infection. These include: (1) cooking meat to a safe temperature (ie, one sufficient to kill toxoplasma) or freezing meat planned for raw or undercooked consumption; (2) peeling or thoroughly washing fruits and vegetables before eating; (3) cleaning cooking surfaces and utensils after contact with raw meat, poultry, seafood, or unwashed fruits or vegetables; (4) avoiding contact with cat feces or cat litter; and (5) not feeding raw or undercooked meat to cats and keeping cats inside to prevent acquisition of toxoplasma by eating infected prey (50; 67). Preventive educational interventions that target pregnant women can greatly reduce seroconversion rates during pregnancy (52).
Only about 50% of mothers of congenitally infected infants identified known risk factors (14; 13). Furthermore, acute toxoplasma infections in mothers are unlikely to be diagnosed, as most infections are asymptomatic, and, even when symptomatic, the symptoms are nonspecific. It is for these reasons that some advocate universal screening (13). Universal screening is mandated by law in some European countries, including France and Italy, where the incidence of toxoplasma infections is higher than in the United States. If a pregnant woman is suspected to have acquired toxoplasma during gestation, then treatment should be initiated to prevent vertical transmission of the pathogen or to decrease disease severity. One study found that untreated mothers had a transmission rate of 50%, compared to only 8.3% in their treated counterparts, making infants born to untreated mothers 6.5 times more likely to be infected with toxoplasmosis (83). Less severe disease, as well as decreased rate of vertical transmission, have been reported in countries where systematic screening and treatment have been implemented (64; 73).
Congenital toxoplasmosis is associated with more severe complications when the mother is untreated (63). Ideally, treatment should be initiated prenatally. Prenatal screening and treatment protocols have been found to be more cost-effective than programs that screen and treat after birth. Cost reductions from prenatal screening programs are attributable to fewer long-term medical complications from congenital toxoplasmosis (10).
Because exposure to infected cats is a major conduit through which humans acquire toxoplasmosis, another approach to prevention could be to minimize the infection of cats. For long-term prevention, development and use of a cat vaccine can be very effective in reducing T gondii disease burden (67).
Effective vaccines for the prevention of toxoplasmosis in humans do not yet exist. Live-attenuated vaccines have been the most studied in animal models and have shown some efficacy. However, a major concern is the possibility that the attenuated state of the parasite could inadvertently reverse, transforming the attenuated parasite into a virulent state, thus, causing infection. It is principally for this reason that live-attenuated vaccines for toxoplasmosis are not being pursued for human use. Other forms of vaccines, including those using recombinant proteins, DNA, and exosomes are also being investigated (06).
One line of research that is particularly promising, but still in its infancy, is the use of nanoparticles in T gondii vaccines. By virtue of their small size and specific structure, nanoparticles can direct toxoplasma antigens to specific cells of the immune system. The nanoparticles can also maintain antigen in a tissue area and allow gradual release of the antigen, thereby increasing exposure time and enhancing immune response. Early studies suggest that the use of nanoparticles may be especially useful for development of a T gondii vaccine (15).
The development of a human vaccine against Toxoplasmosis gondii could potentially prevent vertical transmission if it were given prior to or during pregnancy. However, no vaccine trials have been shown to prevent effectively vertical transmission in animal models. The problem is exacerbated by the lack of knowledge regarding the elicited immune protection at the maternal-fetal interface. A greater understanding of the pathophysiology of transmission at the placental level could prove helpful in developing an effective vaccine to prevent congenital infection (06).
Congenital toxoplasmosis resembles other TORCH infections, an acronym incorporating toxoplasmosis, rubella, cytomegalovirus, and herpes simplex virus, all potential causes of intrauterine infection. Each of these agents can produce intrauterine growth retardation, jaundice, hepatosplenomegaly, skin rash, intracranial calcifications, and chorioretinitis. These other infections can typically be distinguished from toxoplasmosis on the basis of laboratory testing ("TORCH titers").
Lymphocytic choriomeningitis virus (LCMV) is another prominent human pathogen that can induce congenital infections. A rodent-borne arenavirus, lymphocytic choriomeningitis virus mimics congenital toxoplasmosis by producing microencephaly, chorioretinitis, and progressive hydrocephalus. However, unlike toxoplasmosis, which can infect virtually all fetal tissues, lymphocytic choriomeningitis virus has a strong tropism for the brain and tends not to infect other fetal tissues. Thus, newborns with congenital lymphocytic choriomeningitis virus infection may have substantial brain disease but will typically not have hepatosplenomegaly, thrombocytopenia, rash, or somatic growth failure (92; 12; 11). Congenital lymphocytic choriomeningitis virus infection is diagnosed serologically by identifying lymphocytic choriomeningitis virus-specific IgM and IgG antibodies.
Zika virus has emerged as a major pathogen worldwide, especially in the Americas. An arbovirus that is spread by the bite of mosquitoes, Zika, can cause congenital infections that, like toxoplasmosis, can induce severe brain and retinal injuries. An intensely neurotropic virus, Zika targets neuroprogenitor cells and tends to spare other fetal organs. Congenital Zika infection leads to microencephaly, which is often even more severe than that observed with toxoplasmosis. The most severe form of microencephaly is referred to as fetal brain disruption sequence, in which the sutures overlap and there are scalp rugae. This condition is commonly induced by Zika but rarely occurs with toxoplasmosis. Both Zika and toxoplasmosis can induce cerebral calcifications. However, in congenital Zika virus infection, the calcifications tend to occur at the gray-white matter junction, whereas in toxoplasmosis, they are more diffuse (47).
Intrauterine varicella virus (chickenpox) infection also deserves consideration. However, unlike toxoplasmosis, varicella infection of the fetus often produces cicatricial skin lesions with underlying tissue hypoplasia and skeletal anomalies, including limb hypoplasia, equinovarus, and calcaneovalgus (39).
Noninfectious disorders that potentially mimic congenital toxoplasmosis include Aicardi syndrome (a genetic disorder causing chorioretinal lacunae and agenesis of the corpus callosum) and developmental CNS disorders (ie, hydranencephaly, severe schizencephaly, and aqueductal stenosis). Careful analysis of neuroimaging studies usually allows clinicians to distinguish the latter disorders from intrauterine infections, including congenital toxoplasmosis.
Several additional genetic disorders have been described that closely resemble congenital toxoplasmosis (81). Aicardi-Goutieres syndrome (AGS) is an autosomal recessive disease that presents with signs similar to those of congenital toxoplasmosis, including microencephaly, intracranial calcifications, encephalopathy, and cerebrospinal fluid lymphocytosis. Furthermore, like congenital toxoplasmosis, the neurologic status of patients with AGS may decline over months and years. Aicardi-Goutieres syndrome can be distinguished from congenital toxoplasmosis by lack of serologic evidence of infection and by detection of the mutant genes responsible for Aicardi-Goutieres syndrome, AGS1, AGS2, or TREX (77).
A second syndrome that mimics congenital toxoplasmosis is pseudo-TORCH syndrome, a disorder that gained its name by its close resemblance to the TORCH infections. Infants with pseudo-TORCH syndrome typically have microencephaly, cerebral calcifications, spasticity, and seizures. They may also have extracerebral signs suggestive of a TORCH infection, including neonatal icterus, hyperbilirubinemia, thrombocytopenia, and hepatomegaly. The serologic evidence of toxoplasmosis will not be present in cases of pseudo-TORCH syndrome. In addition, although chorioretinitis is common in symptomatic congenital toxoplasmosis, it is absent in pseudo-TORCH syndrome (89).
Acquired toxoplasmosis can mimic malignancies (ie, lymphoma) or other infectious disorders (ie, hepatitis and the infectious mononucleosis syndromes caused by Epstein-Barr virus or cytomegalovirus). These disorders can usually be distinguished from toxoplasmosis by microbiological and histopathological studies.
|
• Prenatal testing for toxoplasmosis infection in the pregnant woman consists of serum anti-toxoplasma IgG and IgM titers. | |
|
• If maternal antibodies or fetal ultrasound are highly suggestive of congenital toxoplasmosis, then amniotic fluid PCR testing can be done at 18 weeks’ gestation or later to confirm the diagnosis. | |
|
• Because some infants with congenital toxoplasmosis are asymptomatic in the neonatal period, evaluation for this diagnosis must be pursued whenever the history is concerning for prenatal exposure. |
For decades, serologic testing was the only practical diagnostic test for toxoplasmosis. Molecular techniques have arisen, which allow testing to be done on amniotic fluid, umbilical cord blood, maternal blood, newborn blood, placental fragments, and colostrum. This testing greatly augments serology as an approach to diagnosing remote, recent, and ongoing toxoplasmosis infections. However, there is variability in the guidelines utilized by each country or society regarding the procedures to diagnose toxoplasmosis, and many countries have developed congenital toxoplasmosis surveillance programs (25).
Diagnosis during pregnancy. Serologic testing for anti-toxoplasma IgG and IgM titers is usually the first step. However, a positive IgG antibody titer does not necessarily indicate a recent infection (49). Likewise, IgM antibodies may persist for over 1 year following an acute infection. For this reason, a positive IgM result should be followed up with further testing at a reference laboratory (such as Palo Alto Medical Foundation Toxoplasma Serology Laboratory [PAMF-TSL]; Palo Alto, CA; http://www.pamf.org/serology) (48; 60).
During pregnancy, molecular diagnostic tests can be conducted most usefully on amniotic fluid samples. One study examined the performance of four molecular methods for the laboratory diagnosis of congenital toxoplasmosis in amniotic fluid samples (86). The study found that real-time PCR assay had somewhat greater sensitivity and specificity than conventional PCR, nested PCR, and multiplex-nested PCR. However, all four of these molecular techniques performed well and were capable of contributing to the laboratory diagnosis of toxoplasmosis.
Different parts of the T gondii genome have been targeted in these assays, and studies have demonstrated that some genes may be much better candidates than others. For example, targeting the REP-529 gene in quantitative PCR assays for the diagnosis of T gondii provided a higher sensitivity and, hence, better performance than targeting the B1 gene. Targeting B1 not only failed to detect several positive samples but also yielded a higher number of false positives (07). However, one meta-analysis showed that the B1 gene remained the most commonly targeted gene in PCR testing, and, although some studies in this analysis supported the higher sensitivity of the REP-529 gene, others showed no significant difference between the two gene targets (25).
An ongoing challenge in the diagnosis of toxoplasmosis is differentiating between acute and chronic infection. One possible innovation is the use of stage-specific parasite antigens to determine the phase of the infection. For example, the SAG1 protein is characteristic of the tachyzoite stage and could identify acute infections, whereas the BAG1 protein is characteristic of the bradyzoite stage and could identify chronic infections (55).
Amniotic fluid PCR at 18 weeks of gestation (the optimal time) or later can be used for prenatal diagnosis of congenital toxoplasmosis. The value of amniotic fluid PCR testing before 18 weeks of gestation has not been studied. Amniotic fluid PCR should be considered for pregnant women with (1) diagnostic or highly suggestive serologic test results, (2) fetal ultrasound abnormalities suggestive of congenital toxoplasmosis, or (3) immunosuppressed status, which increases the risk of reactivation of a latent infection (60). A systematic review and meta-analysis of performance of amniotic fluid PCR in the diagnosis of congenital toxoplasmosis revealed a sensitivity of 87% and a specificity of 99% when PCR was performed up to five weeks after maternal diagnosis (21). Furthermore, determining the parasite burden in the amniotic fluid can aid in predicting the severity of symptoms in neonates with congenital infection (25).
A standardized clinical approach is important to avoid unnecessary amniocenteses. A retrospective study among the birth cohort of 1992-2008 conducted in Austria--where a mandatory screening for toxoplasma-specific antibodies exists--indicated that half of the amniocenteses were performed without clinical justification. Although most infants with congenital toxoplasmosis were accurately identified, serological confirmation at 1 year of age was important. In addition, serological and clinical follow-up of infants from mothers with acute infection was important for final diagnosis and timely identification of the infants at risk of congenital toxoplasmosis (73).
When amniotic fluid testing is not available or is not positive, placental analysis can aid in the diagnosis of congenital infection and in the isolation and genotyping of the parasite. However, if the mother was treated for toxoplasma infection during pregnancy, then placental analysis may be less effective, as the parasite is less frequently isolated in the placenta following treatment (25).
In case of HIV-positive pregnancy, an undetectable viral load using antiretroviral therapy should be achieved before conducting an amniocentesis in order to avoid inadvertent transmission of the HIV virus during the procedure (53).
Monthly ultrasound is recommended for women with suspected or diagnosed acute toxoplasma infection shortly before conception (within 3 months of conception) or during gestation. Ultrasound may reveal fetal abnormalities suggestive of toxoplasmosis, such as cerebral calcifications, hydrocephalus, hepatosplenomegaly, and ascites (75).
Diagnosis in the newborn. Many infected newborns do not exhibit any clinical signs. Therefore, a thorough evaluation is mandatory for any newborn with suspected congenital toxoplasmosis. The workup includes serologic testing (toxoplasma-specific IgG, IgM, and IgA), PCR of peripheral blood, urine and CSF, brain imaging, complete neurologic evaluation, ophthalmological evaluation, and hearing screen. Serological testing should be conducted in the mother after birth as well, in consultation with a reference laboratory (71). Other diagnostic strategies, including colostrum (66), saliva (16), and Guthrie card (54) serology, are under investigation.
Because IgM does not cross the placenta, Toxo-IgM in a newborn must be derived from the newborn itself and strongly suggests the diagnosis of congenital toxoplasmosis. However, a significant portion of congenitally infected infants do not have Toxo-IgM on the first day of life. Some of these IgM-negative newborns will become positive after the first or second weeks of life, but 20% to 50% never become positive. Negative IgM is also more frequent in neonates whose mothers received prenatal treatment (32). In addition, among the infants who do have IgM antibodies on the first day of life, 20% will be negative by 1 month, and more than 50% will be negative by 3 months. Thus, although the detection of Toxo-IgM antibodies can be highly valuable in diagnosing congenital toxoplasmosis, these antibodies can come and go rapidly and unpredictably. As a result, absence of Toxo-IgM is by no means equivalent to absence of congenital toxoplasmosis (44).
In addition to IgM, Toxo-IgA can also be used for the diagnosis of acute infection. The IgA is detectable when performed after the neonate is 10 days old (55).
Toxoplasma IgG in a newborn could be derived from an infected fetus. Alternatively, because IgG can cross the placenta, Toxo-IgG antibodies may be derived from the mother, and the infant may have been spared infection. If the infant was not infected, then the passively transferred IgG titers will progressively decrease and disappear before 1 year of age (58). In contrast, if the infant was infected, then that infant will continue to produce IgG antibodies. A positive IgG in an infant at 1 year of age is often considered the gold standard for diagnosis of congenital toxoplasmosis (59).
As is the case for IgM antibodies, IgG antibodies may or may not be detectable in an infected newborn. For this reason, molecular diagnostic tests can be useful. In particular, PCR for toxoplasmosis on cerebrospinal fluid (CSF) samples can sometimes be positive in infants in whom the serology was negative. The use of serologic studies and PCR, when combined, provides a greater sensitivity for the diagnosis of congenital toxoplasmosis than does either test alone (65).
Further diagnostic options include indirect methods, such as immunosorbent agglutination assays (ISAGA), western blot (WB), enzyme-linked immunosorbent assay (ELISA), and IgG avidity. ISAGA is a rapid test using IgM and IgA to immunocapture the tachyzoite phase of toxoplasma. ISAGA is more sensitive than ELISA testing, though ELISA is the most used method for serological testing. Western blot can be used to confirm congenital toxoplasmosis by comparing maternal and neonate samples, though this method is expensive and unsuitable for screening. IgG avidity, a variant of ELISA, determines the affinity of IgG to bind parasitic antigens. As low-affinity antigens are produced in acute infection and high-affinity antigens are produced in chronic infection, this method can be used to differentiate between the two phases of infection (55).
Brain imaging may reveal abnormalities, such as intracranial calcifications, hydrocephalus, and encephalomalacia. Intracranial calcifications can be detected most readily by CT. In practice, ultrasound is often performed prior to CT, and the intracranial calcifications are often evident on ultrasound, as well (43). Calcifications usually involve the basal ganglia, periventricular regions, cerebral cortex, and subcortical white matter (34). Hydrocephalus is frequently observed, most often caused by an ependymitis occluding the aqueduct, thus, leading to enlarged third and lateral ventricles. In contrast to congenital cytomegalovirus, malformations of cortical development, such as polymicrogyria, are not typical in congenital toxoplasmosis (34). An eye examination, ideally performed by an ophthalmologist familiar with the disease, may reveal chorioretinitis. Hearing should also be tested during the neonatal period.
|
• Management of congenital toxoplasmosis varies based on the timing of exposure and gestational or postnatal age at the time of diagnosis. | |
|
• Pyrimethamine is the principal agent used in the treatment of congenital toxoplasmosis. |
The management of congenital toxoplasmosis depends on the clinical situation. In particular, specific treatment recommendations depend on (1) when, in the course of pregnancy, the infection occurs, (2) whether there is evidence of fetal infection or not, and (3) whether the infant has yet been born or not. A summary of the recommended treatments for the various clinical scenarios is provided in Table 2.
Prevention of vertical transmission before 14 weeks of gestation. Spiramycin is recommended for pregnant women with suspected or confirmed acute infection during the first 14 weeks of gestation or shortly before conception. It is recommended to transition to pyrimethamine-sulfadiazine and folinic acid after the first 14 weeks until the result of the amniotic fluid PCR is available at 18 weeks (32). The goal of the treatment at this time is to prevent fetal infection with toxoplasma. In studies using historical controls, treatment with spiramycin decreased the incidence of congenital infection by approximately 60% (19). Because spiramycin concentrates in the placenta to prevent vertical transmission but does not readily cross the placenta, it cannot be relied on to treat the infected fetus. Thus, spiramycin is used exclusively to treat the infected mother. There is no evidence that spiramycin is teratogenic. Spiramycin is not commercially available in the Unites States, but it can be obtained at no cost after consultation with one of the reference laboratories (Palo Alto Medical Foundation Toxoplasma Serology Laboratory, Palo Alto, CA, Phone # 650-853-4828; or US National Collaborative Treatment Trial Study, Chicago, IL, Phone # 773-834-4152).
For many years, Sanofi-Aventis has been providing spiramycin to pregnant women in the United States at no cost (60).
Once initiated, spiramycin is administered until delivery, even in pregnant women with negative amniotic fluid PCR, because of the possibility that fetal infection can still occur later in pregnancy from a placenta that was infected earlier (19). If the fetus develops ultrasonographic signs suggestive of congenital infection, or if the amniotic fluid PCR turns positive, then treatment should be switched from spiramycin to pyrimethamine, sulfadiazine, and folinic acid.
Although spiramycin is generally considered the treatment of choice for prevention of vertical transmission before 18 weeks of gestation, the approach is not standardized. Some authors advocate the use of pyrimethamine/sulfadiazine in this clinical situation, based on the lower incidence of maternal adverse effects, especially acral paresthesia, accompanying this approach (72).
Prevention of vertical transmission after 14 weeks of gestation. If the infection is acquired after 14 weeks of gestation, then the combination of pyrimethamine, sulfadiazine, and folinic acid is recommended. Pyrimethamine is potentially teratogenic, as it inhibits the folate metabolic pathway. For this reason, it should not be used in the first trimester (69). Folinic acid (NOT folic acid) is added to prevent or reduce bone marrow suppression. CBC and LFTs need to be monitored. An ultrasound should be done at least monthly until term. If congenital infection is not likely, such as in the setting of a negative amniotic fluid PCR and normal ultrasounds, then switching to spiramycin should be considered.
In a study that included 120 mothers and 123 newborns, comparison among three treatment methods (spiramycin/bactrim vs. pyrimethamine/sulfonamide vs. spiramycin alone) demonstrated that the spiramycin/bactrim combination has a significant efficacy advantage in reducing mother-to child transmission of T. gondii infection (88).
Treatment of the infected fetus. If the amniotic fluid PCR is positive or if the fetal ultrasound suggests congenital toxoplasmosis, then the combination of pyrimethamine, sulfadiazine, and folinic acid should be administered to the pregnant woman to initiate early treatment of the infected fetus. Effective prenatal treatment decreases the rate of severe neurologic sequelae by 75% in neonates with congenital toxoplasmosis (29). CBC and LFTs need to be monitored throughout the treatment. A fetal ultrasound should be obtained at least monthly until term.
Treatment of the newborn with confirmed congenital toxoplasmosis. All infected children need to be treated, regardless of their clinical presentation. Infected children who are not treated are at particular risk for developing new chorioretinal lesions later in life and other sequelae. Treatment should be given to newborns diagnosed prenatally, regardless of whether or not the mother received treatment. Treatment should also be given to newborns with clinical signs suggestive of congenital toxoplasmosis, pending results of confirmatory tests. For newborns without clinical signs and with equivocal serology results, treatment can be withheld pending a definitive diagnosis (58). Treatment consists of the combination of pyrimethamine, sulfadiazine, and folinic acid for 1 year. Administration of pyrimethamine and sulfadiazine for 1 year to infants with congenital toxoplasmosis resulted in normal neurologic and cognitive outcome in the great majority of patients. This favorable outcome was achieved even among most patients who had moderate or severe neurologic disease during the newborn period. This outcome following a year of therapy was better than outcomes reported for children who were treated for only 1 month in previous studies. Currently, the 1-year treatment regimen is the standard of care in the United States for congenital toxoplasmosis. Longer treatment courses may be necessary as the medications are ineffective against bradyzoites and tissue cysts (22).
Pyrimethamine is a cornerstone in the treatment of congenital toxoplasmosis. This medication inhibits T gondii proliferation and survival through inhibition of the folate metabolic pathway. In particular, pyrimethamine blocks the synthesis of tetrahydrofolate, which the parasite requires for DNA synthesis. This interference with tetrahydrofolate, however, can also adversely affect human tissues, especially those with high metabolic activities, including the epithelium and bone marrow. As a result, skin rashes and bone marrow suppression are adverse events that are commonly observed in infants treated with pyrimethamine for congenital toxoplasmosis. The neutropenia, thrombocytopenia, and anemia induced by pyrimethamine can be particularly troublesome and, if not monitored and corrected, often force a change in treatment, which can adversely affect outcome. Thus, infants treated with pyrimethamine should undergo periodic blood counts with dosage adjustments and transfusions as necessary (08).
However, the observed neutropenia might not always be due to the pyrimethamine and could, instead, be due to the proliferative action of tachyzoites, which induce cell lysis. One study showed a 2.7 times higher risk of developing neutropenia in infected patients receiving treatment compared to uninfected patients also undergoing treatment (83).
New studies have suggested that protein kinases (PKs) exclusive to Toxoplasma gondii could become targets for therapeutic medications, especially as these kinases do not have homologs in human cells. Knock out of specific protein kinases involved in parasite metabolism impairs parasite development and survival. For example, inhibiting phosphofructokinase-2 in T gondii increases pyrophosphate concentrations to toxic levels in the parasite, leading to its death. Similarly, blocking pyruvate kinase-1 and pyruvate kinase-2 suppresses glycolysis, leading to energy deprivation in the parasite. Therefore, inhibitors of toxoplasma-specific protein kinases could be utilized to further advance toxoplasma treatment options (22).
Congenital toxoplasmosis often induces ventriculitis and inflammation of the ventricular ependymal lining. This inflammatory effect often leads to stenosis or obliteration of the cerebral aqueduct and a subsequent noncommunicating hydrocephalus. Consequently, many children with congenital toxoplasmosis require placement of a ventricular shunt for alleviation of hydrocephalus.
Because toxoplasmosis can induce retinitis, which may or may not be evident in the neonatal period, all children with congenital toxoplasmosis should be treated postnatally and followed with routine ophthalmologic examinations throughout childhood. In addition, hearing should be tested during infancy, and the patient should have ongoing developmentally appropriate hearing screening and at least one diagnostic audiologic assessment by 24 to 30 months of age, even if the child passed the newborn hearing screening (33).
Indication | Therapy |
Prenatal Infection | |
Maternal infection is suspected or documented to have occurred 3 months before conception or during pregnancy, but before 18 weeks of gestation. | Spiramycin: 1 g (3 million U) every 8 hours |
Immunocompromised pregnant women suspected of having a reactivated latent infection. | Spiramycin: 1 g (3 million U) every 8 hours |
Maternal infection is suspected or documented to have occurred during pregnancy, but after 18 weeks of gestation. | Pyrimethamine: 50 mg every 12 hours for 2 days, followed by 50 mg daily, and Sulfadiazine: Initial dose 75 mg/kg, followed by 50 mg/kg every 12 hours (maximum 4 g per day) and Folinic acid: 10-20 mg daily, until 1 week following cessation of pyrimethamine treatment. |
Maternal infection is suspected, but congenital infection is not likely, such as negative amniotic fluid PCR and normal ultrasounds. | Consider switching to Spiramycin 1 g (3 million U) every 8 hours |
Congenital infection is highly suspected or documented by abnormal ultrasound and/or positive amniotic fluid PCR. | Pyrimethamine: 50 mg every 12 hours for 2 days, followed by 50 mg daily, and Sulfadiazine: Initial dose 75 mg/kg, followed by 50 mg/kg every 12 hours (maximum 4 g per day) and Folinic acid: 10-20 mg daily, until 1 week following cessation of pyrimethamine treatment. |
Postnatal infection | |
Congenital infection in the newborn is highly suspected or congenital toxoplasmosis has been confirmed in the infant. | Pyrimethamine: 1 mg/kg every 12 hours for 2 days, followed by 1 mg/kg daily for 6 months, followed by the same dose 3 times per week, and Sulfadiazine: 50 mg/kg every 12 hours, and Folinic acid: 10 mg 3 times per week until 1 week following cessation of pyrimethamine treatment. |
Mortality rates for untreated infants with congenital toxoplasmosis range from 1% to 5% (42). Of 300 infected, untreated infants studied by Couvreur and Desmonts in the 1950s, only 14% had normal intelligence (18). However, aggressive treatment of congenital toxoplasmosis reduces the likelihood of permanent neurologic sequelae (20; 31; 56; 80). In a therapeutic trial, nearly 80% of the infants receiving early neurosurgical intervention and prolonged treatment with antitoxoplasma chemotherapy, as described below, had favorable neurodevelopmental outcomes (56).
The most common complication of congenital toxoplasmosis is chorioretinitis. One study examined the risk factors for development of chorioretinitis among children who were treated with pyrimethamine and sulfonamide for congenital toxoplasmosis (40). The study found that the two greatest risk factors for chorioretinitis were the presence of intracranial calcifications and a delay of 8 weeks or greater between maternal seroconversion and first treatment of the infection. These findings suggest that brain involvement predisposes to retinal involvement and underlines the importance of prompt treatment.
Even if a newborn receives prompt and standard pre and postnatal treatment for congenital toxoplasmosis, new or recurrent ocular lesions can continue to arise in that patient for many years. Indeed, one study examined the long-term ocular prognosis of a cohort of congenitally infected children who were treated according to a standardized protocol and monitored for up to 22 years (90). The investigators found that recurrences of new ocular lesions occurred up to 12 years after the appearance of the first lesion. This finding suggested that annual postnatal checkups should be continued throughout puberty to identify new ocular lesions. Additionally, there is evidence that patients with macular scarring from congenital toxoplasmosis could show improvement in visual acuity with occlusion therapy guided by an ophthalmologist (76).
The risk of primary infection during pregnancy depends on the mother's antibody status and the degree of exposure to toxoplasma oocysts. Fetal infection occurs more commonly during third trimester maternal infections.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Daniel J Bonthius MD PhD
Dr. Bonthius of Atrium Health/Levine Children's Hospital has no relevant financial relationships to disclose.
See Profile
Marissa Balkcom MD
Dr. Balkcom of Atrium Health Levine Children’s Hospital has no relevant financial relationships to disclose.
See ProfileRyan M Bonthius BS
Mr. Bonthius of University of Iowa Carver College of Medicine has no relevant financial relationships to disclose.
See ProfileCrystal L Walker MSN CPNP
Crystal Walker of Atrium Health - Levine Children’s Hospital has no relevant financial relationships to disclose.
See ProfileNina F. Schor MD PhD
Dr. Schor of the National Institutes of Health has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jan. 20, 2025
Sleep Disorders
Jan. 18, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Developmental Malformations
Dec. 26, 2024