





General Neurology
Use of focused ultrasound in neurologic disorders
Jan. 13, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Cortical blindness refers to visual loss due to bilateral lesions of the geniculocalcarine pathways in the brain. The term “cortical blindness” is used interchangeably with “cerebral blindness,” as will be the case in this discussion. Patients with cortical blindness may not be aware of their visual deficits. When they are unaware of the extent of visual loss (often confabulating their responses), the clinical presentation is termed “Anton syndrome.” Etiologies of cortical blindness are numerous and diverse.
|
• Cortical blindness can be confused with nonorganic visual loss because the eye examination, including pupillary responses, is normal. Nonorganic (ie, psychogenic, functional) visual loss should be considered as a diagnosis of exclusion but can be suggested by examination findings that violate physiological patterns of visual loss. | |
|
• Cortical blindness may be overlooked because symptoms of visual loss may not be expressed or may even be denied by the patient. | |
|
• Brain MRI is an important diagnostic test to determine the cause of cortical blindness, but not all causes produce MRI abnormalities. |
"Cortical blindness" refers to visual loss due to bilateral dysfunction of the occipital visual cortex (“striate cortex” or V1). Some patients will exhibit unawareness of the extent of visual loss. This remarkable clinical state is termed "Anton syndrome" in reference to Gabriel Anton, who described this phenomenon in 1899. Anosognosia, coined by Babinski in 1914, defines a lack of knowledge of disease. Anton syndrome (sometimes referred to as Anton-Babinski syndrome) is a form of visual anosognosia. For lesions not isolated to the cortex, including the subcortical visual pathways, the term "cerebral blindness" may be more appropriate. In strictest terms, cortical blindness is a specific subtype of cerebral blindness. The term "cortical visual impairment" has been applied in the pediatric population when visual deficits are incomplete. Nevertheless, because the term "cortical blindness" continues to be in common use, it will be retained in this article.
|
• Patients with cortical blindness will have normal pupillary constriction to light despite severely reduced vision. Pupillary responses are spared because they rely on synaptic reflexes through the brainstem and do not require cortical inputs. | |
|
• Patients with cortical blindness may be unaware of their visual deficits and may confabulate (Anton syndrome). |
Patients often present with bilateral symmetric vision loss that may extend to no light perception. In bilateral posterior cerebral artery infarctions that spare the occipital poles, the visual acuity may remain normal within the small area of preserved central vision. Visual fields show constriction due to bilateral homonymous hemianopias with central sparing. One characteristic of this type of visual field constriction is that the spared central portion resembles a “keyhole,” with two semicircles of different diameters each respecting the vertical midline and joining together.
This unique pattern distinguishes visual field constriction caused by bilateral occipital strokes from such causes as glaucoma or retinitis pigmentosa.
In cortical blindness, pupillary reflexes and ophthalmoscopy are normal. Hence, these patients may be misdiagnosed as having non-organic vision loss. Here, response to movement of checkered black and white rectangles on a rotating drum or strip, or to a shifting mirror, can be helpful. Optokinetic nystagmus is normally evoked by the movement of checkered strips. That form of nystagmus is consistently absent in patients with cortical blindness. But because nystagmus evoked by such a stimulus is difficult to suppress when vision is intact, it will be preserved in non-organic vision loss. The shifting-mirror test, in which a large mirror is rocked back and forth in front of the patient to evoke pursuit eye movements in a normally-sighted individual, can also be used to rule out non-organic visual loss.
Awareness of the visual deficit varies across patients with cortical blindness. Some patients will exhibit unawareness of the extent of visual loss, a phenomenon called "Anton syndrome," also known as “visual anosognosia.” In 1899, Gabriel Anton published a paper titled “On the Self-Awareness of Neurologic Deficits in Patients with Cortical Blindness and Cortical Deafness” (02). He described a patient as follows:
|
A 56-year-old needlewoman…Her condition was characterized by complete blindness although the pupils and fundi remained normal. The patient could not distinguish light and darkness. She could not perceive objects… It was very striking that the patient did not take any notice of extreme and later on complete loss of vision. The patient, who was otherwise complaining a lot, was almost unaffected by this loss (13). |
At autopsy, the patient was found to have “cystic necrosis primarily affecting the white matter of the left and right occipital lobes.” Anton offered the interpretation that this “is a breakdown of the functional relationships with other cortical areas. It is undoubtedly possible that the function of one part of the brain, which is not damaged itself, can be altered through other parts.”
Patients with Anton syndrome typically confabulate responses when asked about their visual environment. Patients may be asked, for instance, about the color of the examiner’s tie or whether she is wearing glasses or has a beard. Although patients will not have sufficient vision to know the answers to these questions, patients will essentially guess answers that seem reasonable (or make excuses for an inability to give the correct answer). The mechanism of anosognosia remains unknown. It typically persists for 1 to 2 weeks after the inciting event, after which patients begin to be aware of their visual deficit.
Some patients with cortical blindness may demonstrate the opposite dissociation between visual function and awareness, in which they claim no conscious awareness of a visual percept yet retain a primitive ability to distinguish visual features when asked to guess. For example, a patient may claim not to see a visually presented object but may accurately guess its color when forced to choose. Termed "blindsight," this phenomenon is a rare occurrence. Investigations of a patient with bilateral striate cortex lesions showed that despite the patient’s assertion of being blind, fMRI responses were intact in the amygdala, superior temporal sulcus, extrastriate body area, insula, and orbitofrontal cortex while the patient passively viewed images of faces and bodies (37). Scrambled stimuli did not elicit these responses. The authors suggested that these findings indicated the presence of V1-independent inputs to cerebral areas along the ventral visual processing stream. Another phenomenon described in patients with lesions of occipital lobes is statokinetic dissociation, also called the Riddoch syndrome. This phenomenon refers to the perception of moving but not static stimuli in the affected field. The pathophysiology of Riddoch syndrome due to occipital lobe disease is thought to involve visual inputs reaching the V5 (motion processing cortex) and bypassing the V1 area.
In a patient with suspected cortical blindness, portions of the examination must be modified to determine the extent of residual visual function. It can be helpful to use a stimulus with high limbic valence, such as the examiner’s face, to assess the patient’s ability to track a moving target. In addition, one may hold a mirror in front of the patient to observe whether small shifts in gaze accompany movements of the mirror. In cases of complete blindness, no reliable pursuit eye movements will be observed, regardless of the test stimulus.
A patient’s ability to blink to visual threat is often assessed in the setting of severe visual loss. Most patients with complete cortical blindness will demonstrate reduced blink to visual threat, although extrageniculate visual mechanisms may preserve this reflex in some cases. When testing the blink to threat, care should be taken to avoid stimulating the cornea by moving air toward it.
Lesions causing bilateral dysfunction of the retrogeniculate visual pathways may occur either simultaneously or sequentially. If they occur sequentially, a patient will demonstrate the findings of a contralateral homonymous field deficit when the first lesion occurs. Complete cortical blindness would result after a second lesion occurred in the visual cortex of the opposite hemisphere.
The prognosis of cortical blindness depends on its cause, severity, and age of onset. The outcome is particularly poor for ischemic injuries, where visual recovery is minimal. Neurodegenerative disorders may have a fluctuating course with a generally downward trend. Infectious and toxic insults may have variable recovery depending on the severity. The visual loss of posterior reversible encephalopathy syndrome is rapidly reversible if acute hypertension is the cause, there is no restricted diffusion on MRI, and the blood pressure is promptly controlled.
In general, children are believed to have a better prognosis than adults.
Formed and grotesque visual hallucinations may occasionally occur during recovery from cortical blindness. They are attributed to deafferentation and inappropriate activation of damaged cortex. The positive visual phenomena typically resolve within weeks after stroke but may persist if the lesion has other causes. Persistent seizures should be ruled out, although the hallucinations due to seizures are typically geometric patterns rather than fully formed images.
A 59-year-old woman was admitted for altered sensorium, vision loss, headaches, and seizures. Admitting blood pressure was 203/180. Visual acuity was 20/400 in the right eye and 20/800 in the left. Pupils were normal in size and constricted normally to light. The anterior ocular segment and fundus examinations were normal in both eyes. MRI revealed bilateral parieto-occipital areas of edema without infarction consistent with posterior reversible encephalopathic syndrome. Visual acuity improved to 20/70 in both eyes three days after inpatient blood pressure control.
A 59-year-old woman had severe bilateral vision loss as well as altered sensorium, headaches, and seizures. The blood pressure was 203/180 mmHg. MRI revealed signal abnormality in the bilateral parieto-occipital areas, predomin...
Because "cortical blindness" is a general term referring to dysfunction of the retrogeniculate visual pathway, etiologies are numerous and diverse (01). Table 1 lists several conditions associated with cortical blindness.
|
Vascular | |
|
• Bilateral occipital infarction (07) | |
|
Infectious | |
|
• Meningitis (25) | |
|
Metabolic disturbances | |
• Hypoglycemia (39) | |
|
Mitochondrial | |
|
• Mitochondrial encephalopathy (MELAS syndrome) (26) | |
|
Neurodegenerative | |
|
• Leukodystrophy (21) | |
|
Other | |
|
• Seizures and postictal state (10) | |
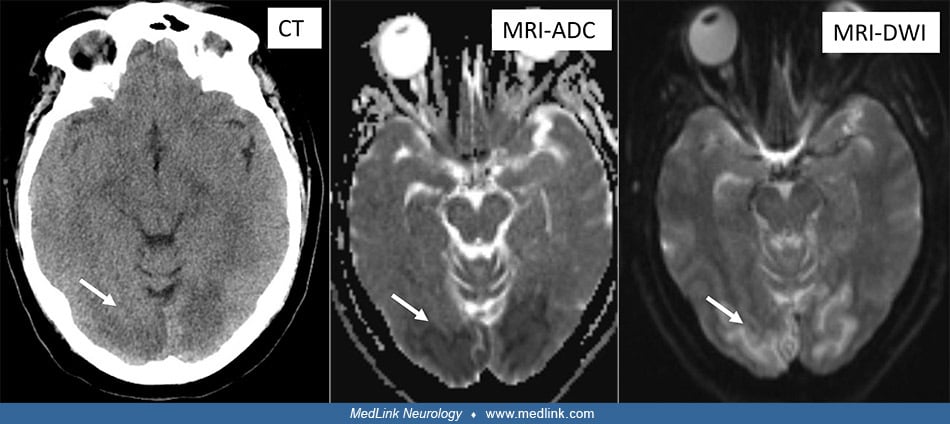
Posterior cerebral artery strokes. Bilateral simultaneous or sequential posterior cerebral artery occlusions may cause cortical blindness (07). Posterior cerebral artery infarction leads to homonymous hemianopia, often in isolation without other neurologic deficits.
Patients may be unaware of the field defect until the contralateral posterior cerebral artery infarction leads to profound vision loss when the contralateral hemifield is affected. Ischemic infarction is diagnosed in the acute phase by reduced diffusivity on diffusion-weighted MRI. Basilar artery thrombosis or embolism is an important consideration in the setting of acute bilateral posterior cerebral artery strokes. Diagnostic studies should assess for a proximal embolic source or vertebrobasilar arterial dissection.
Venous infarction of the occipital lobes resulting from venous sinus thrombosis has also been reported as a cause of cortical blindness (38).
Cortical blindness is a well-recognized complication of hypoxic-ischemic encephalopathy following cardiac arrest. The gray matter (cortex, thalami, basal ganglia, and the watershed vascular zones) are relatively susceptible to systemic hypotension.
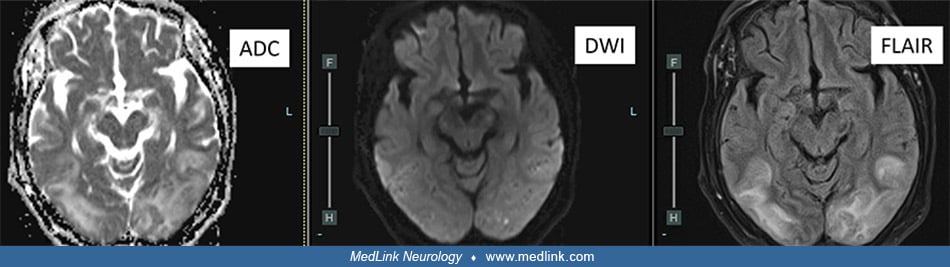
Posterior reversible encephalopathy syndrome. Posterior reversible encephalopathy syndrome describes cerebral edema that typically has a posterior distribution; its causes include severe hypertension, eclampsia or pre-eclampsia, and exposure to drugs including tacrolimus and cyclosporine as well as selenium (17; 06). Hypomagnesemia may be contributing factor. The underlying mechanism relates to endothelial dysfunction and a disturbance of normal cerebral vascular autoregulation. Patients present with visual deficits often associated with headaches, confusion, and, occasionally, seizures. MRI is more sensitive than CT and will demonstrate cerebral edema in affected areas. Cortical and subcortical T2- and FLAIR signal hyperintensities are common findings on MRI studies. The presence of restricted diffusion would be more characteristic of ischemic infarction.
Angiographic contrast dye-induced encephalopathy. Contrast-induced encephalopathy is a rare complication following the use of iodinated intravascular contrast agents. Transient cortical blindness is the most common manifestation. Noncontrast CT may be normal. MRI typically shows high T2/FLAIR signal predominant in the occipital lobes, as in posterior reversible encephalopathy syndrome. Patients with hypertension and end-stage renal disease and those with high-dose injections into the aortic arch or cranial vessels are at highest risk (35).
Tumor and tumor-related edema. Neoplastic lesions and associated edema can disrupt the bilateral geniculocalcarine pathways. In adults, causes include astrocytoma, lymphoma, or metastatic tumors. Extra-axial lesions, such as meningiomas, may cause compression and edema within the underlying brain. Visual deficits, including complete cortical blindness, may result when these lesions are situated in the occipital lobes.
Additionally, acute obstructive hydrocephalus can lead to posterior cerebral artery compression and ischemia causing cortical blindness (08).
Radiation necrosis. The side effects associated with radiation treatment can be considerable. When used in combination with systemic chemotherapy, there is a significant risk of radiation necrosis. In addition, radiation treatment produces accelerated atherosclerosis and vascular endothelial dysfunction, increasing the risk of cerebral ischemia. When posterior areas of the brain are within the field of radiation treatment, these untoward effects can produce bilateral occipital dysfunction (19).
Progressive multifocal leukoencephalopathy. Progressive multifocal leukoencephalopathy is a degenerative condition produced by reactivation of the JC virus. It occurs more commonly in immunocompromised patients, such as those with acquired immunodeficiency syndrome (AIDS) or those receiving immunosuppressive chemotherapeutic agents. JC virus reactivation often affects astrocytes and oligodendrocytes, resulting in perturbation of the myelin with associated inflammation and secondary axonal loss. The infection has a predilection for the posterior hemispheres and cerebellum and can cause cortical blindness (36).
Creutzfeldt-Jakob disease. The Heidenhain variant of Creutzfeldt-Jakob disease is a rapid neurodegenerative condition caused by abnormal prion proteins (23). In this form of prion disease, spongiform changes occur with an early predilection for the occipital lobes. Patients present with prominent visual dysfunction, often progressing to cortical blindness.
Seizures. Occipital seizures may result from various causes, including developmental cortical dysplasia, gliosis following stroke or hemorrhage, neoplastic disease, and infections. When seizures propagate to involve both occipital lobes, transient cortical blindness can result (10). Other manifestations of seizures, such as involuntary motor activity, may not be present. Occipital seizures of long duration often cause prolonged postictal visual loss, although the deficits typically recover once the seizures stop.
Metabolic derangements. Severe metabolic derangements, such as extreme hypoglycemia, can cause injury to metabolically active regions, including the primary visual cortex (39). Neonates are particularly vulnerable to this type of brain injury and can develop permanent neurologic deficits, including visual loss.
Mitochondrial disorders. Mitochondrial disorders may produce deficits relating to impaired cerebral energy metabolism. The syndrome of mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS) typically produces neurologic deficits with lesions that do not conform to vascular boundaries (26). Bilateral retrogeniculate lesions may produce profound visual deficits. Mitochondrial cortical blindness eventually leads to visual recovery more than in ischemic stroke but less often than in posterior reversible encephalopathy syndrome.
Alzheimer disease. In a subset of patients with Alzheimer disease, visual symptoms, including homonymous hemianopia and cortical blindness, may occur before dementia (24). MRI shows posterior cortical atrophy.
Leukodystrophies. Some inherited leukodystrophies with adult onset have a predilection for the posterior cerebral hemispheres. Adult-onset X-linked adrenoleukodystrophy characteristically causes bilateral occipital lesions with a leading edge of enhancement visible at their anterior border (21). In this disorder, impaired peroxisomal beta-oxidation of fatty acids leads to the accumulation of very long chain fatty acids and abnormal myelin. There is phenotypic variability, but visual deficits are common.
Pediatric considerations. There are special considerations in the pediatric population regarding cortical blindness. Structural lesions of the visual cortex are evident in most cases. A review of patients with children evaluated in a tertiary referral facility revealed that major risk factors for so-called “cortical visual impairment” were perinatal hypoxia and premature birth (22). In these cases, MRI may demonstrate ischemic lesions of the occipital cortex and white matter. Findings relating to periventricular leukomalacia or intraventricular hemorrhage are also common in this population. It is often difficult to predict the ultimate visual outcome in these children. Early intervention with physical and occupational therapy can be helpful to improve their development.
A separate population of neonates presents with early visual impairment in isolation, without other neurologic deficits or imaging abnormalities. This presentation is attributed to delayed maturation of visual cortical neurons, and the prognosis for development of normal sight is generally good. Often normal fixation and tracking develop by the age of 5 to 6 months (03). The mechanism underlying delayed visual maturation is poorly understood.
Cortical blindness is relatively uncommon, and its exact incidence in the general population has not been well studied.
Because the causes of cortical blindness are diverse, there is no single preventive therapy. Because stroke is a leading cause, risk may be reduced by the management of risk factors, including hypertension, hyperlipidemia, diabetes, and cardiac arrhythmias. Antiplatelet agents such as aspirin may be beneficial. Early identification and treatment of the underlying cause may reduce the likelihood of permanent cortical blindness. When infarction is suggested by MRI, the diagnostic workup should be aimed at identifying cardioembolism and other causes of stroke.
Ocular disorders that may cause symmetrically decreased vision in both eyes with reactive pupils and normal-appearing fundi should be considered in the differential diagnosis of cortical blindness. Leber hereditary optic neuropathy often presents with simultaneous or rapidly sequential visual loss in both eyes, and pupillary responses may be paradoxically preserved in the acute stage, even when only one optic nerve appears to be damaged. Paraneoplastic retinopathies, such as cancer-associated retinopathy, may cause only a mild reduction in the pupillary light reflex and produce no fundus abnormalities. Genetically determined retinal photoreceptor degenerations, such as foveal cone dystrophy, may have minimal ophthalmoscopic findings. Bilateral retrobulbar optic neuritis can present with symmetrically reduced vision in both eyes and normal fundus, but pupils would be expected to be sluggish.
Young children with ocular motor apraxia who have impaired volitional gaze may appear to be blind because they do not orient normally to visual targets. Therefore, they may be misdiagnosed as having cortical blindness if head thrusting is not present. Infants with retinal degenerations, such as Leber congenital amaurosis and achromatopsia, whose pupils and retinas appear normal, may also be misdiagnosed as having cortical blindness.
Non-organic visual loss may mimic cortical blindness. To decide whether a constricted visual field is of non-organic origin, the examiner should assess the extent of the spared central field and then assess it again after doubling the testing distance. With organic visual field constriction, the preserved field will double in diameter as the testing distance is doubled. A patient with non-organic visual loss will demonstrate “tubular” fields that do not expand as the testing distance is increased.
Patients with nonorganic visual loss may also demonstrate preservation of optokinetic nystagmus or eye movements during the “mirror test.” However, the diagnosis of non-organic visual loss cannot rest on these findings as they may also occur with organic visual loss that is not complete.
|
• Manual or automated perimetry establishes the homonymous nature of the visual loss in patients whose field defects are patchy and incomplete. Brain MRI is an essential diagnostic test to determine cerebral infarction, meningitis, encephalitis, and neurodegenerative disorders. Diffusion-weighted MRI images help to identify areas of acute infarction. In patients who are unable to undergo MRI, CT may be utilized but is insensitive to many causes of cortical blindness, including the acute stage of infarction. | |
|
• Additionally, MRI may be insensitive, and the lesion may be subtle or even inapparent in some conditions typically: recent severe systemic hypotension causing hypoxic-ischemic brain injury, acute migraine, status epilepticus, posterior cortical atrophy, nonketotic hypoglycemia, CJD, focal encephalitis. |
In some patients with cortical blindness caused by the Heidenhain variant of Creutzfeldt-Jakob disease, a SPECT or PET scan will be necessary to identify cortical dysfunction (23). Spinal tap and targeted laboratory studies may detect infectious and metabolic etiologies.
Electroretinography is a useful method of establishing a diagnosis of paraneoplastic retinopathy, prior retinal vascular occlusion, and retinal dystrophy, including Leber congenital amaurosis and congenital stationary night blindness.
The role of visual-evoked potentials in evaluating cortical blindness remains ill-defined. The correlation between visual acuity and the visual evoked potential is inaccurate because well-developed visual-evoked potentials may be present in complete cortical blindness. In addition, up to 20% of normal subjects can, by conscious maneuvers, attenuate or even extinguish visual-evoked potentials (27). Therefore, a diminished visual-evoked potential neither excludes non-organic visual loss nor provides objective evidence for cortical blindness.
In patients with cerebral infarction, antiplatelet therapy is recommended to reduce platelet aggregation and the risk for future ischemic events. Evaluation of a proximal embolic source is warranted and may alter recommendations for secondary stroke prevention. For example, patients with atrial fibrillation are likely to benefit from anticoagulation. Patients with meningitis and encephalitis should be treated with appropriate intravenous antimicrobial agents. Metabolic disorders should be corrected, and toxic exposures should be eliminated and treated.
There are currently no validated vision restoration treatments for cortically blind patients (30). Therapies typically focus on occupational therapy that involve teaching compensatory strategies to maximize the use of their remaining vision. Visual restoration therapies including visual transcranial magnetic stimulation are being proposed by some researchers and yet have to be validated (32). Additionally, social service consultation can provide the patient with valuable information about federal and community benefits. Many patients gradually learn to compensate for the loss of vision.
Cortical blindness may occur in severe preeclampsia or eclampsia as part of posterior reversible encephalopathy syndrome (12; 17) or due to ischemic injury from reversible cerebral vasoconstriction syndrome. In posterior reversible encephalopathy syndrome, visual recovery typically occurs within days of restoration of normal blood pressure and is usually complete. In cases associated with preeclampsia or eclampsia, delivery of the fetus may be necessary to reverse the underlying cause.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Sangeeta Khanna MD
Dr. Khanna of University of Michigan has no relevant financial relationships to disclose.
See Profile
Jonathan D Trobe MD
Dr. Trobe of the University of Michigan has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
General Neurology
Dec. 30, 2024
Neurogenetic Disorders
Dec. 26, 2024
Neurogenetic Disorders
Dec. 13, 2024
Neuro-Oncology
Dec. 13, 2024