As early as 1873, Thomson published a paper on the inhalation of nitrous oxide, nitrogen, hydrogen, and other gases and gaseous mixtures (126), and in 1927, he specifically proposed the use of helium in deep diving and caisson work (127; 128).
Dysbarism. Dysbarism is a general term that encompasses disturbances in the human body resulting from a change in atmospheric pressure. Dysbarism encompasses five subentities: decompression sickness, barotrauma, gas embolism, inert gas narcosis, and oxygen toxicity.
Decompression sickness. Decompression sickness is one of several forms of dysbarism, ie, disturbances in the human body resulting from a change in atmospheric pressure. Divers, miners, tunnel workers, and caisson workers will experience decompression sickness if they progress too quickly to a lower environmental pressure. Rapid ascent to high altitudes in an aircraft with an uncompressed cabin can also produce decompression sickness. The first and least severe symptoms are characterized by limb and joint pain. In more severe cases, with ascent from greater depths, after longer bottom times, or with more rapid ascent or decompression, other nervous system, cardiac, or pulmonary symptoms may occur.
The condition was well known among caisson workers, and it was, therefore, called "caisson disease." Other terms used to describe the condition are "the bends" (limb and joint pain), "the chokes," and "hits."
Clinical manifestations
Presentation and course
| |
• Dysbarism encompasses five subentities: decompression sickness, barotrauma, gas embolism, inert gas narcosis, and oxygen toxicity. |
| |
• Neurologic manifestations of decompression sickness while diving appear during or immediately after ascent. |
| |
• A common neurologic manifestation of decompression sickness is myelopathy. |
| |
• Livedo racemosa (often incorrectly labeled "cutis marmorata"), due to gas emboli in the cutaneous circulation, precedes neurologic symptoms and almost always indicates a right-to-left shunt. |
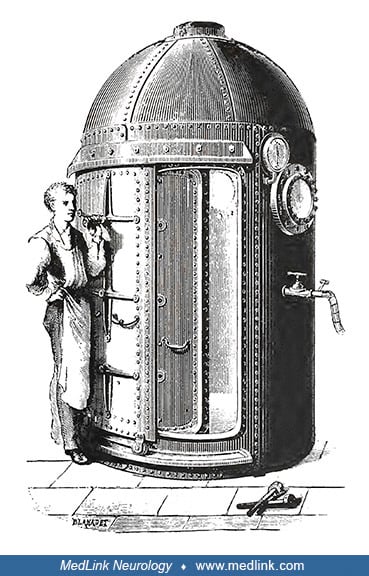
Dysbarism. Dysbarism is a general term that encompasses various pathologies that result when the body experiences an increase or decrease in atmospheric pressure at a rate or duration that exceeds the capacity of the body to safely adapt (109). Although the most common cause of dysbarism is underwater diving, it can also occur with aviation and space exploration as well as compressed air tunnel and caisson work ("caisson's disease" --a caisson is a large watertight chamber, open at the bottom, from which the water is kept out by air pressure and in which construction work may be carried out underwater) (129; 52).
-
Caisson schematic
(Illustration by Yk Times in February 2007. Creative Commons Attribution-Share Alike 3.0 Unported License, https://creativecommons.org/licenses/by-sa/3.0/deed.en.)
-
New caisson at Norfolk Naval Shipyard
This is the Navy's only East Coast dry dock capable of docking any diesel or nuclear-powered ship. (Photo taken on June 7, 2012 by Norfolk Naval Shipyard Public Affairs. Creative Commons Attribution 2.0 Generic License [CC BY 2...
Dysbarism encompasses five subentities: decompression sickness, barotrauma, gas embolism, inert gas narcosis, and oxygen toxicity.
Decompression sickness. Symptoms of decompression sickness develop rapidly and appear during or immediately after ascent. They usually occur within 3 hours of surfacing but may sometimes take as long as 24 to 36 hours to manifest. They are mainly seen in persons who have experienced pressures greater than two atmospheres absolute.
Aviation decompression sickness can also occur, for example, with rapid decompression of cabin pressures (87), or with military parachutist dispatchers exposed repeatedly to high altitude (25,000 feet) (32). However, events that occur at flight altitudes below 17,000 feet (5182 meters) or with rapid decompression pressure changes under 0.3 atm, decompression sickness is less likely to be the etiology of the presenting symptoms.
Golding and colleagues proposed a dichotomous classification of decompression sickness: a minor form (Type I) affecting the musculoskeletal system and characterized by limb and joint pain ("the bends"), and a major form (Type II) involving the neurologic ("hits"), pulmonary ("the chokes"), and cardiac systems (52). Neurologic manifestations are present in 10% to 15% of decompression sickness cases. Isolated cutaneous manifestations (ie, livedo racemosa) are generally considered to be type I decompression sickness. Circulator shock is considered to be type II decompression sickness.
Neurologic manifestations of decompression sickness. A common neurologic manifestation of decompression sickness is myelopathy (134; 95; 92; 132; 37). Symptoms of spinal cord involvement usually appear early, typically within 3 minutes of surfacing. They are characterized by leg weakness with walking difficulties, leg numbness and paresthesia, and bladder dysfunction. Other reported symptoms include intense nausea, localized back pain, penile erection, and fecal incontinence (37). The severity varies from mild sensory symptoms to paraplegia or even tetraplegia. In most cases, the segmental level of the responsible lesion is around the sixth to eighth thoracic segment, which is the area most susceptible to ischemia. Decompression sickness may, however, involve any part of the spinal cord. Fortunately, in many cases of spinal decompression sickness, the symptoms gradually disappear, leaving the patient asymptomatic, although slight reflex abnormalities may persist as evidence of earlier damage.
Spinal cord decompression sickness presenting as Brown-Sequard syndrome, with MRI abnormalities corresponding to infarction in the territory of a posterior spinal artery, may improve considerably following hyperbaric oxygen therapy (95; 132); the diagnosis is mainly based on clinical findings rather than MRI (132). Gas bubbles may also block the anterior spinal artery, causing weakness in both lower extremities (134).
Some divers develop decompression sickness with acute cerebral hemispheric dysfunction, manifesting variously as hemiparesis, aphasia, hemianopsia, Anton syndrome (ie, visual anosognosia due to cortical blindness) (08), memory loss, convulsions, and coma.
Inner ear decompression sickness may manifest as vertigo and hearing loss, but so may inner ear barotrauma (84; 91; 110). Development of post-dive benign paroxysmal positional vertigo may occur due to nitrogen bubble formation within the semicircular ducts (35; 36).
Livedo racemosa (often mislabeled "cutis marmorata"). Cutis marmorata, livedo reticularis, and livedo racemosa have been improperly considered synonyms when, in fact, they refer to phenomena with different appearances and pathophysiology (59). Cutis marmorata is the most commonly used term in the context of decompression sickness and is a form of livedo reticularis; however, this is "a physiological and benign, livid circular discoloration with a net-like, symmetric, reversible, and uniform pattern" (59).
Cutis marmorata is a physiologic form of livedo reticularis observed commonly on the legs on exposure to cold, with gradual resolution on rewarming; it occurs primarily in cold children and slim young women (eg, after being in cool water) (59). It is a physiological vasospastic response to coldness or systemic disease with a consequent decline of tissue oxygen saturation, particularly in the periphery of the vascular distribution of small cutaneous arterioles (59). The characteristic symmetric and uniform cyanotic mottling pattern is related to the vascular anatomy of normal skin. The microanatomical structure of the cutaneous blood supply is arranged in a series of 1 to 3 cm cones at the margins of which the zone of arterial predominance wanes, while the superficial venous plexus becomes more prominent.
Anatomical structure of the cutaneous blood supply
The microanatomical structure of the cutaneous blood supply is arranged in a series of 1 to 3 cm cones, with the apex of each cone deep in the dermis at the site of an ascending arteriole. At the margins of each cone, the densi...
Therefore, physiologic or pathologic processes, like livedo reticularis, that impede cutaneous blood flow may produce a regular, net-like coloration pattern of closed rings in the predominantly venous areas at the margins of the cones.
-
Skin pattern of livedo reticularis and livedo racemosa
If the blood flow in cutaneous arteries and veins is reduced, the erythrocytes become more deoxygenated than usual, so the draining veins become visible as a regular network. Therefore, any physiological or pathological process...
-
Skin pattern of livedo reticularis and urticaria compared with livedo racemosa
Skin pattern of livedo reticularis (top and bottom left) and urticaria (bottom right) for comparison with livedo racemosa. (Source: Hartig F, Reider N, Sojer M, et al. Right/left shunt. Front Physiol 2020;11:994. Copyright © 20...
In contrast, decompression-associated skin discolorations correspond to the "pathological, irregular, broken netlike pattern" of livedo racemosa, a pathologic and painful disorder typically found on the limbs, trunk, and buttocks, which intensifies with higher ambient temperature (59). Livedo racemosa is caused by thrombotic or embolic vascular occlusion of arterioles with resultant local perfusion deficits and hypo-oxygenation, causing an irregular reddish-blue or violaceous net-like mottling of the skin.
-
Skin pattern of livedo racemosa (not related to decompression sickness)
The pattern of livedo racemosa is caused by vascular occlusion of arterioles with irregular, local perfusion deficiency leading to a reddish blue, irregular mottling of the skin. The cases shown in this figure were not related ...
-
Skin pattern of livedo racemosa due to decompression sickness
The pattern of livedo racemosa is caused by vascular occlusion of arterioles with irregular, local perfusion deficiency leading to a reddish blue, irregular mottling of the skin. The cases shown in this figure were due to decom...
-
Livedo racemosa in a 35-year-old man with decompression sickness
A 35-year-old man, supine with livedo racemosa (mislabeled cutis marmorata) secondary to type I decompression sickness after diving in Notre Dame Bay on the north side of Newfoundland, Canada. The skin marbling can be seen outl...
With decompression sickness, the embolic obstructions of the ascending or feeding arterioles consist of gas bubbles, whereas in other settings, the emboli may consist of fibrin, cholesterol, or calcium phosphate.
Several hypotheses have been proposed to explain livedo racemosa (51; 79; 46): (1) local formation of bubbles in cutaneous blood vessels; (2) arterialization of venous bubbles across a right-to-left shunt augmented by local amplification of bubble size on reaching supersaturated skin via the arterial circulation; and (3) arterialized venous gas bubbles embolizing the brainstem, where the autonomic nervous system regulates skin blood vessel dilation and constriction (51; 79). Of these, the most likely is that livedo racemosa results from arterialized venous bubbles that pass to the cutaneous circulation via a right-to-left shunt (hypothesis 2), possibly with bubble augmentation on reaching supersaturated skin.
Livedo racemosa is generally caused by thrombotic or embolic occlusion of cutaneous arteries, which suggests that decompression-associated livedo racemosa is caused by arterial gas emboli (hypothesis 2) (59). Moreover, when proper techniques are used, investigators have uniformly identified significant right-to-left shunts in patients with decompression-associated livedo racemosa (81; 46; 59; 09). In one study of four divers with livedo racemosa (albeit mislabeled cutis marmorata), all four had the following: (1) large right-to-left shunts, (2) numerous small bubbles visibly moving within the skin microvasculature, and (3) no bubbles visible in adjacent areas of normal skin (46). In another case of livedo racemosa (also mislabeled cutis marmorata), the presence of intravascular air was confirmed by CT (76). These findings discount hypotheses 1 and 3 and confirm the validity of hypothesis 2.
Decompression sickness-related circulatory shock. A patient who presented with neurologic symptoms and hypovolemic shock after two risky dives had multiple cerebral and pulmonary thromboembolisms on MRI (83)
Another recreational diver dove to a depth of 218 feet for 43 minutes while breathing air and developed nitrogen narcosis. He ascended from depth slowly according to the staged decompression recommendations of his dive computer, but ultimately he exhausted his air supply and was forced to surface, having omitted 6.5 hours of required air decompression (06). After requesting emergency medical services, he lost consciousness on the surface and was rescued from the water; he was then intubated and mechanically ventilated. The clinical presentation was remarkable for loss of consciousness, hypotension, livedo racemosa, peripheral edema, and severe hypoxia requiring mechanical ventilation. Shock worsened during hyperbaric oxygen therapy, requiring aggressive volume resuscitation with crystalloid plus albumin in addition to multiple vasopressors. After 37 hours of hospitalization, blood pressure normalized, and vasopressors were tapered and discontinued. He ultimately required 10 days of mechanical ventilation and was discharged on day 21 with mild decompression sickness-related neurologic deficits.
Early hyperbaric oxygen therapy can reduce the neurologic deficits associated with decompression sickness plus shock, and cardiopulmonary and renal functions can normalize with aggressive volume expansion and pressors to counteract refractory hypotension (83; 06).
Decompression sickness-related damage to other organs. Rarely, decompression sickness can present with other organ damage, such as severe acute kidney injury (27).
Barotrauma. Barotrauma is physical tissue damage caused by a pressure difference, usually between an unvented space inside the body and surrounding gas or fluid, but it can occur superficially as well; for example, mask squeeze barotrauma results from failure to equalize the air space created between the face mask and the face.
Mask squeeze barotrauma
Note the periorbital ecchymoses and the bilateral subconjunctival hemorrhages. (Source: Wikimedia Commons user:prilfish, 2003. Creative Commons Attribution 2.0 Generic [CC BY] license, creativecommons.org/licenses/by/2.0/deed.e...
The damage is due to shear or overstretching of tissues. As a gas-filled space expands or contracts, it can cause damage to the local tissue. This is a phenomenon well-known to deep-sea fishermen who pull up deep-dwelling fish that have experienced barotrauma by rapid ascent in the nets.
Fish with distended swim bladder prolapsed, everted, and projecting from its mouth
A fish brought up from a considerable depth with a distended swim bladder prolapsed, everted, and projecting from its mouth (after Regnard). (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London...
Pulmonary compression barotrauma may occur during very deep descents during breath-hold diving. As lung volume decreases to or below residual volume, mucosal edema, vascular engorgement, pulmonary edema, and hemorrhage may occur as nonventilated areas fill with liquid to counteract the negative pressure. Affected individuals may experience chest pain, dyspnea, and hemoptysis on ascent.
Ear barotrauma may affect the external, middle, and inner ear. This may occur on descent (compression) or ascent (decompression), depending on the circumstances that cause pressures to be unbalanced across the tympanic membrane or the round and oval windows. For example, if the external auditory canal is blocked by cerumen, the higher air pressure from the tank regulator with pass through the Eustachian tube, causing the affected tympanic membrane to bulge outward and possibly to rupture with resultant severe pain and bloody otorrhea. If, instead, the Eustachian tube is blocked, and the diver is unable to "clear" the passage and balance the pressures with a Valsalva maneuver, middle ear pressure will be less than the pressure of the water against the tympanic membrane, causing the affected tympanic membrane to bulge inward and possibly to rupture with (again) resultant severe pain and bloody otorrhea. Less commonly, the round or oval window may rupture with Eustachian tube dysfunction, causing severe, acute vertigo, a potentially life-threatening situation at depth.
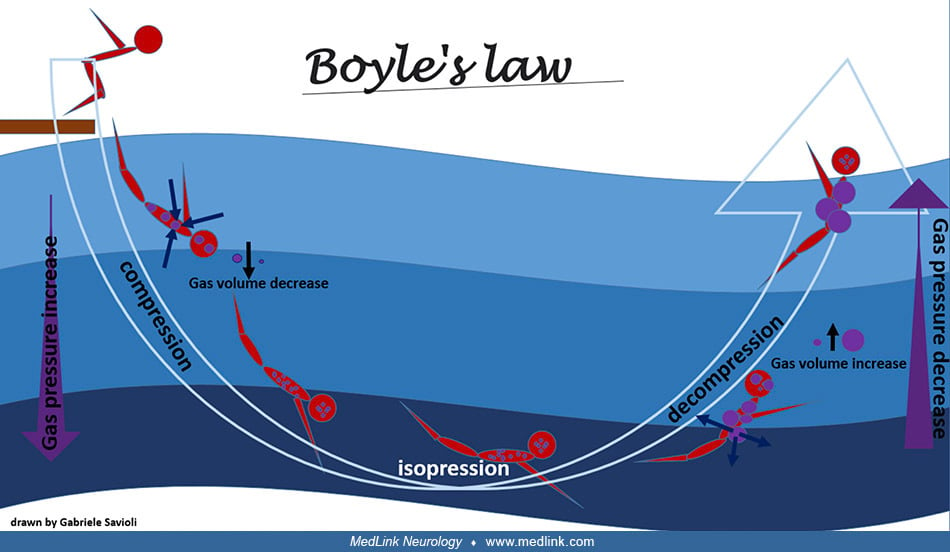
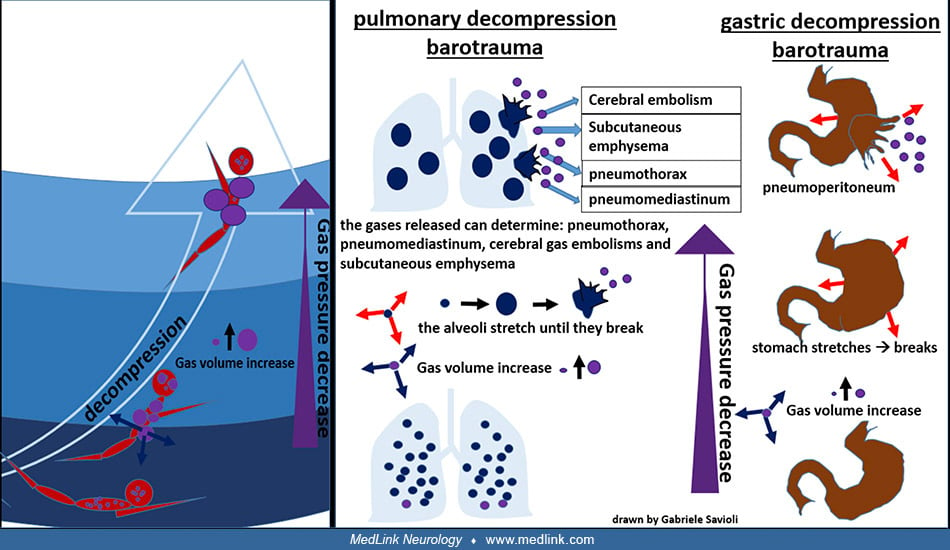
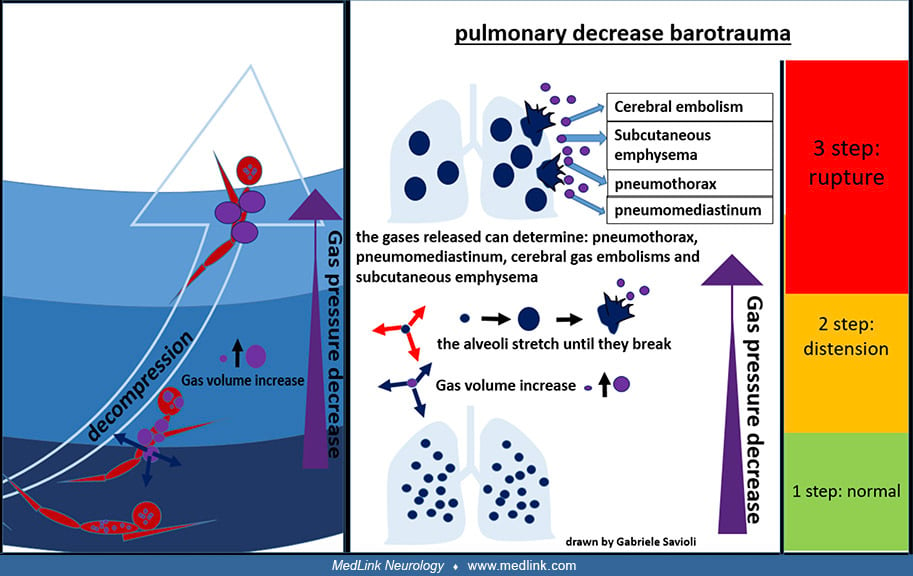
Decompression barotraumas can damage the lungs and gastrointestinal tract. As the pressure decreases with ascent, the volume occupied by the gases increases (Boyle’s law), and the excess gas (ie, excess for the available volume of the organ that contains it) is exhaled from the lungs and expands within the gastrointestinal tract to be expelled, if possible, from the mouth or anus. If the surplus is retained, the tissues that contain the gas are stretched and damaged. Pulmonary decompression barotraumas may cause cerebral arterial gas embolism, subcutaneous emphysema, pneumothorax, and pneumomediastinum. Gastrointestinal decompression barotraumas may cause gastrointestinal rupture and pneumoperitoneum.
Pulmonary barotrauma is a significant reason (15%) for emergency calls to the Divers Alert Network (DAN) involving diving minors, likely because of psychological immaturity, suboptimal management of adverse situations, and inadequate supervision (61).
Sinus barotrauma may result from blocked or intermittently blocked sinuses. The inability to maintain a balance between the air pressure within the sinuses and the ambient pressure (which is matched by the regulator for the inspired air or gas mixture) causes the pressure inside the sinuses to become lower than the ambient pressure during descent; if some high-pressure gas enters the sinus during the dive and partially compensates for the higher ambient pressure at depth, a reverse situation may occur on ascent. The pressure differences alone can cause intense sinus pain, vascular engorgement, and epistaxis. In addition, during ascent, compression of the maxillary branch of the trigeminal nerve in the maxillary sinuses can cause infraorbital paresthesia that usually resolves within several hours without treatment.
Gas embolism. Gas embolism can occur when a pressure gradient allows air to enter the bloodstream or when bubbles form within the bloodstream. The bubbles then obstruct blood flow in distal vessels. Gas emboli may complicate barotrauma, decompression sickness, and mixed forms. Arterial gas embolism is usually precipitated by rapid ascent, breath holding, or preexisting lung disease.
Inert gas narcosis. Inert gas narcosis (also known as nitrogen narcosis, "rapture of the deep," the "Martini effect," and the "narcs") is a reversible alteration in consciousness that occurs while diving at depth (82). It is caused by the anesthetic effect of certain inert gases at high pressure. Narcosis produces a state similar to drunkenness (alcohol intoxication), so the relation of depth to narcosis has been referred to informally as "Martini's law.” Inert gas narcosis results in the feeling of one martini for every 10 meters (33 ft) below 20 meters (66 ft) depth, so the effect starts at 30 meters or 100 feet, with a pressure of approximately four atmospheres absolute.
Narcosis may be completely reversed in a few minutes by ascending to a shallower depth, with no long-term effects. Nitrogen narcosis rarely develops into a serious problem if the divers are aware of its symptoms and ascend to manage it. Diving much beyond 40 meters (130 feet) is outside the scope of recreational diving. Special training in the use of various helium-containing gas mixtures (eg, heliox or trimix) is required to dive at greater depths for military or commercial purposes and minimizes the risks of narcosis and oxygen toxicity. These mixtures prevent narcosis by replacing some or all of the nitrogen fraction of the breathing gas with non-narcotic helium.
Manifestations of inert gas narcosis may include: (1) feelings of tranquility, exhilaration, giddiness, anxiety, depression, or paranoia; (2) impaired concentration and multi-tasking ability; (3) impaired judgment and decision-making ability; (4) increased reaction time and impaired coordination; (5) vertigo and visual or auditory disturbances; and (6) reduced perception of cold discomfort and impaired shivering (with a consequent faster decline in core body temperature, aggravating many of the problems of inert gas narcosis) (57; 65).
Oxygen toxicity. Oxygen toxicity (or oxygen poisoning) results from breathing oxygen at higher-than-normal partial pressures (33). In particular, breathing oxygen at partial pressures above 1.4 atmospheres absolute (ie, a partial pressure of more than approximately 220 mm Hg) can produce acute neurotoxicity. Activities and situations associated with increased risk of oxygen toxicity include underwater diving breathing air, hyperbaric oxygen therapy, exposure to prolonged high oxygen levels, and prematurity. Acute oxygen toxicity typically manifests with CNS effects ("the Bert effect"), whereas chronic toxicity presents with mainly pulmonary effects ("the Smith effect"). CNS effects can include fasciculations and myoclonus, nausea, tinnitus, dysphoria, and generalized convulsions; pulmonary effects can include pleuritic chest pain, substernal heaviness, coughing, dyspnea, damage to the pulmonary epithelium, pulmonary (intra-alveolar) edema, inactivation of surfactant, interstitial thickening and fibrosis, and atelectasis.
-
Oxygen poisoning damage to the lung (1)
Oxygen poisoning damage to the lung, showing exudation in a bronchiolar tube and the alveoli of the lung. (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domai...
-
Oxygen poisoning damage to the lung (2)
Oxygen poisoning damage to the lung, showing an alveolus of the lung (high power), exudation of leucocytes, and congestion of capillaries (high power). (Source: Hill L. Caisson sickness and the physiology of work in compressed ...
Deep diving. Diving at depths of more than 50 meters of seawater is designated deep diving. Breathing air is not advised at those depths due to the risk of nitrogen narcosis, a toxic effect of the high partial pressure of nitrogen. Therefore, other gas mixtures are used (eg, heliox, a mixture of helium and oxygen, or triox, a mixture of oxygen, helium, and nitrogen).
Diving with heliox to depths greater than 150 meters produces signs and symptoms of high-pressure neurologic syndrome. The syndrome includes tremor in the upper extremities, impaired memory, dizziness, nausea, and in severe cases, myoclonic jerks and even unconsciousness. High-pressure neurologic syndrome in a dive chamber is accompanied by EEG changes with increased theta (72).
Deep diving requires a prolonged period of compression and a decompression period that may extend over several days. Even after uncomplicated deep dives, transitory focal neurologic changes have been reported, although it is unclear whether these represent an unmasking of otherwise asymptomatic lesions from prior decompression sickness or are instead evidence of new lesions.
Prognosis and complications
Long-term neurologic sequelae of decompression sickness are common among professional offshore divers (123). Among 208 retired Norwegian offshore divers, 163 (78%) reported episodes of decompression sickness, with neurologic decompression sickness in 41 (20%) (123). Divers with a history of neurologic decompression sickness had significantly more neurologic findings on tests of motility, coordination, and sensation (123).
Long-term follow-up of 30 divers treated with hyperbaric oxygen for decompression sickness in 2009 and 2010 revealed that a quarter had long-term residual symptoms (125). More severe presentations of decompression sickness are more likely to have severe long-term sequelae (eg, gait disorders and sphincter incontinence) (18). In decompression sickness with myelopathy, the improvement in MRI findings is not necessarily associated with improved clinical status. Initial motor impairment, further aggravation during transfer to the hyperbaric facility, and development of sphincter dysfunction are indicators of poor prognosis, regardless of the treatment.
In a population-based study, those with decompression sickness had a 3.8-fold increased risk of developing psychiatric disorders and a 5.7-fold increased risk of developing sleep disorders (131).
In a study of 59 military divers with decompression sickness, the main independent risk factor for poor outcome (ie, sensory and motor deficits or bladder dysfunction) was the severity of neurologic manifestations at onset, and recovery was not significantly improved by prompt administration of recompression treatment (17).
In a prospective study of 28 divers with neurologic decompression sickness at a hyperbaric facility, those who presented more than 17 hours after surfacing were likely to have more intense symptoms than those who presented earlier (99). However, delayed initiation of hyperbaric oxygen therapy was not associated with a need for more hyperbaric treatment or worse outcomes.
The therapeutic response in patients with inner ear decompression sickness remains poor. Treatment with 100% oxygen followed by recompression in a hyperbaric chamber will improve the condition of most patients, but two thirds have incomplete recovery (50). Time to recompression does not clearly influence clinical outcome. Vestibular symptoms are more prevalent in retired off-shore divers than in age-matched controls, presumably because of prior decompression sickness: among retired divers, 28% reported dizziness, 14% had vertigo, and 25% had an unsteady gait (53).
Dysbaric osteonecrosis (aseptic bone necrosis) most commonly involves the femoral head but may involve other joints, including the humeral head (24). Symptoms may appear months after diving (24). It is an occupational hazard for commercial and navy divers but is also seen in sport divers.
Clinical vignette
A 31-year-old man working as an underwater fisherman presented with a 1-day history of paresthesia and difficulty writing (108). While spearfishing, he developed fatigue and headache as well as paresthesia and weakness of the right hemibody. He also reported feeling “confused” and “disoriented” and had difficulty getting out of the water. The patient’s dive profile consisted of a 3-hour dive at a maximum depth of 30 meters, with inter-immersion periods of less than 2 minutes on the surface and breath-hold times longer than 2 minutes. Two days earlier, he had made another dive of 4 to 5 hours at a similar maximum depth and with a similar dive profile. CT scan of the brain showed a hypodense lesion in the medial left frontal lobe due to decompression sickness.
Hypodense lesion in the medial left frontal lobe due to decompression sickness (CT)
CT scan of the brain in a 31-year-old man working as an underwater fisherman showing a hypodense lesion in the medial left frontal lobe due to decompression sickness. The patient presented with symptoms of paresthesia and diffi...
Neurosonological studies (ie, carotid and vertebral ultrasound and transcranial Doppler studies) of supra-aortic and intracranial arteries showed no atheromatosis or significant hemodynamic alterations. Transthoracic echocardiography was normal, including a negative agitated saline contrast study to assess for a right-to-left shunt. Total-body CT scan showed no evidence of a neoplastic process.
Given the patient's history of breath-hold diving and the clinical and neuroimaging findings, the patient was transferred to a hyperbaric chamber. Recompression was carried out in the hyperbaric chamber at 2.8 atmospheres absolute. With a progressive resolution of symptoms, treatment was completed using United States Navy Table 6. Total elapsed time is 285 minutes, ascent time between stops (18 to 9 meters and 9 to 0 meters) is 30 minutes (3 meters per 10 minutes), and maximum pressure is 18 meters of seawater.
Treatment for decompression sickness using US Navy Treatment Table 6
Given the patient's history of breath-hold diving with a risk profile for decompression sickness, as well as the clinical and neuroimaging findings, the patient was transferred to a hyperbaric chamber. Recompression was carried...
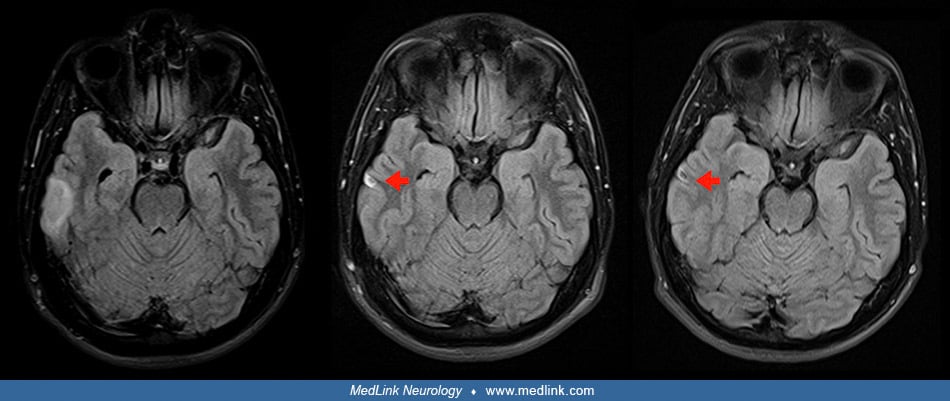
MRI studies done 4 and 5 days after clinical onset showed a left frontal cortico-subcortical hyperintense lesion on FLAIR images due to decompression sickness. Axial diffusion-weighted imaging (DWI b1000) sequences did not show high-signal-intensity lesions.
-
Left frontal cortico-subcortical hyperintense lesion on FLAIR in decompression sickness
FLAIR images 4 and 5 days after onset due to decompression sickness. MRI done 4 days after clinical onset (left and center) and 5 days after clinical onset (right) show a left frontal cortico-subcortical hyperintense lesion (re...
-
Axial diffusion-weighted imaging sequences in decompression sickness
Axial diffusion-weighted imaging (DWI b1000) sequences did not show high-signal-intensity lesions. MRI done 4 days after clinical onset (left and center) and 5 days after clinical onset (right). (Source: Sánchez-Villalobos JM, ...
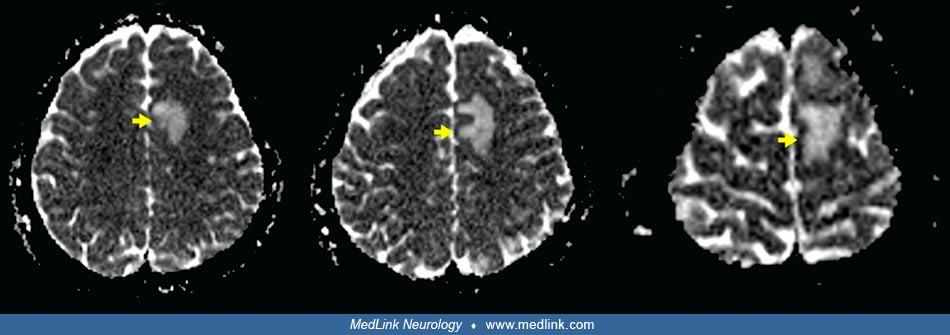
Axial apparent diffusion coefficient maps showed a hyperintense lesion in the left frontal lobe. Axial gadolinium-enhanced 3D T1-weighted imaging (Gd T1WI) showed the presence of different areas of enhancement with irregular morphology in the left frontal area, not suggestive of tumor enhancement. Over a 4-month period, the left frontal lesion gradually evolved with lessoning hyperintensity on axial FLAIR images, ultimately leaving a small area of encephalomalacia.
-
Axial apparent diffusion coefficient maps show a hyperintense lesion in decompression sickness
Axial apparent diffusion coefficient maps show a hyperintense lesion in the left frontal lobe (yellow arrows). MRI done 4 days after clinical onset (left and center) and 5 days after clinical onset (right). (Source: Sánchez-Vil...
-
Axial Gd T1WI showing areas of enhancement with irregular morphology in decompression sickness
Axial gadolinium-enhanced 3D T1-weighted imaging (Gd T1WI) shows the presence of different areas of enhancement with irregular morphology in the left frontal area (blue arrow), not suggestive of tumor enhancement. MRI done 4 da...
-
Radiological evolution of left frontal cortico-subcortical hyperintense lesion from decompression sickness
Axial FLAIR images initially (left), at 1 month (center), and 4 months (right). By 1 month, the lesion is minimally hyperintense (yellow arrow). By 4 months, there is a small area of encephalomalacia (yellow arrow). (Source: Sá...
MRI studies done 4 and 5 days after clinical onset also showed a right temporal cortico-subcortical hyperintense lesion with slight mass effect due to decompression sickness. Over a 4-month period, the right temporal lesion gradually evolved with lessoning hyperintensity on axial FLAIR images, ultimately leaving a small area of encephalomalacia.
-
Right temporal cortico-subcortical hyperintense lesion with slight mass effect due to decompression sickness
MRI done 4 days after clinical onset (left, left center, and right center columns) and 5 days after clinical onset (right) column. Axial fluid-attenuated inversion recovery (FLAIR) images (left column) show a right temporal cor...
-
Radiological evolution over 4 months of hyperintense lesion in the right temporal lobe from decompression sickness
Axial FLAIR images initially (left), at 1 month (center) and 4 months (right). By 1 month the lesion is minimally hyperintense (red arrow). By 4 months, there is a small area of encephalomalacia (red arrow). (Source: Sánchez-Vi...
Biological basis
Etiology and pathogenesis
| |
• Breathing air or gas mixtures under increased pressure leads to increased nitrogen saturation of tissues. |
| |
• On decompression (eg, on ascent from diving or with rapid gain in altitude during flying), gas bubbles may form in the blood and embolize to the CNS and other organs. |
| |
• Embolic lesions in the CNS are facilitated by a right-to-left shunt (eg, patent foramen ovale). |
Decompression sickness. Decompression sickness is caused by the formation of gas bubbles in the blood and tissues during or after a decrease in environmental pressure (decompression).
-
Bubbles in the upper cervical spinal cord of a goat
(Boycott and Damant) (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
-
Bubbles in the spinal cord of a goat at the level of the 2nd cervical, 5th dorsal (thoracic), and 2nd lumbar roots
(Boycott and Damant) (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
-
Bubbles of oxygen in the brain of a mouse
(Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
-
Effect of decompression sickness on the liver
(1) Normal cat liver. (2) Cat liver after decompression from 8 atmospheres in 5 seconds. Bubbles have formed in the fat within the hepatocytes and also are present within the lumens of capillaries. (Source: Hill L. Caisson sick...
-
Decompressed cat's liver (1)
Low-power photomicrograph. (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
-
Decompressed cat's liver (2)
High-power photomicrograph. The hepatocytes are honeycombed with bubbles. (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
-
Effect of decompression sickness on the kidney
(1) Normal cat kidney. (2) Cat kidney after decompression from 8 atmospheres in 5 seconds. (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
-
Decompressed cat's kidney
Low-power photomicrograph. (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
As ambient pressure increases, the inspired pressure of the inert gas (most often diatomic nitrogen, N2) is greater than its arterial partial pressure, which causes the tissues to absorb the gas until the two pressures are balanced. A rapid decrease in pressure (eg, with ascent while diving) causes the dissolved nitrogen to return to its gas form while it is still in the blood or tissues, creating intravascular "bubbles."
Physiopathology of decompression sickness
(Source: Savioli G, Alfano C, Zanza C, et al. Dysbarism: an overview of an unusual medical emergency. Medicina [Kaunas] 2022;58[1]:104. Illustration by Gabriele Savioli. Creative Commons Attribution License [CC BY], https://cre...
These bubbles can cause mechanical obstruction of a vein or an artery (ie, venous or arterial gas embolism) and can also produce an inflammatory response with activation of complement, coagulation factors, and platelets.
-
Spinal cord of a goat with necrotic areas in the 11th dorsal (thoracic) and 2nd lumbar roots
Ascending and descending degeneration is shown in the sections above and below these levels (Boycott and Damant). (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Publ...
-
Necrotic areas in the posterior columns of the spinal cord in a fatal case of decompression sickness
(von Schrötter) (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
-
Gas in the heart and coronary vessels of a dog killed by rapid decompression
(von Schrötter) (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
-
Gas bubbles in the arteries and veins of the omentum and small intestines
(von Schrötter) (Source: Hill L. Caisson sickness and the physiology of work in compressed air. London: Edward Arnold, 1912. Public domain.)
This can lead to the formation of thrombi, an increase in vascular permeability and interstitial edema, and stasis of the microcirculation with tissue hypoperfusion and ischemia. Divers, aviators, and astronauts are at risk of decompression sickness when ambient pressure reductions exceed a critical threshold.
Gas bubbles are present in venous blood after ascent from water depths as shallow as 3 meters. Free venous gas does not invariably lead to decompression sickness because most bubbles are filtered out by the pulmonary capillaries and do not enter the arterial circulation. However, the foramen ovale remains open, or patent, in 25% to 34% of the adult population, with detectable shunting in 8% to 10% (63), and divers with a patent foramen ovale have a significantly increased risk of developing decompression sickness (22; 116); the risk increases with increasing grade of the right-to-left shunt (116). Large right-to-left shunts due to a patent foramen ovale are associated with an increased risk of spinal cord decompression sickness with thoracolumbar involvement (48). In addition, filtration is size-dependent, as small bubbles may escape entrapment. Small emboli do not necessarily cause infarction but may disturb the blood-brain barrier, inducing what has been termed the "perivenous syndrome" (73).
There is a high prevalence of patent foramen ovale in divers suffering from inner ear decompression sickness manifested by vestibular and cochlear symptoms following dives while breathing helium-based mixtures (55).
In a few reported autopsies of apparently unaffected divers, CNS degeneration and vasculopathy have resembled the abnormalities found after decompression sickness. Subclinical damage associated with small emboli is common, especially in the midbrain, as demonstrated by MRI (73).
Predisposing factors for decompression sickness. Risk factors for decompression sickness include strenuous activity during the dive, dehydration, and dive depths exceeding 30 meters of seawater (124). Exercise-induced muscle damage from eccentric work that is characterized by reduced strength and delayed-onset muscle soreness leads to increased formation of venous gas emboli during subsequent hypobaric exposure (ie, acute decompression) (54). Persons with right-to-left shunt (eg, patent foramen ovale) have an increased risk of developing neurologic complications even after recreational scuba diving. Whether cigarette smoking increases the risk of developing decompression sickness is unclear but has been debated.
Yo-yo diving (ie, a series of short-duration dives alternating with similar periods on the surface) was previously considered to reduce bubble formation and risk of decompression sickness based on studies in rats. Subsequently, concern was raised that yo-yo divers may have an increased risk of neurologic decompression sickness, which has been supported by detection of gas bubbles in the left ventricle and neuronal injury in the spinal cord in a study using pigs (100).
A patent foramen ovale or other left-to-right shunt patent foramen ovale can lower the threshold for venous gas embolism tolerance with a tendency for earlier and more abundant arterialization during decompression (103; 104).
An experimental study in rats has shown that pretreatment with sildenafil, a phosphodiesterase-5 blocker used for the treatment of erectile dysfunction, promotes the onset and severity of neurologic decompression sickness, possibly related to vasodilation with increased cerebral blood flow (16).
Decompression sickness-related circulatory shock. Decompression sickness-related shock results from bubble-endothelial interactions, which cause a transient capillary leak syndrome associated with plasma extravasation, hemoconcentration, and hypovolemia (06).
Altitude-related decompression sickness. Cases of altitude-related decompression sickness, some with CNS manifestations, were reported in an Air Force training facility during pressure reduction in a chamber to simulate altitudes between 25,000 and 35,000 feet (7,500 and 10,668 meters) (23). The number of altitude-related decompression sickness incidents with CNS manifestations among United States Air Force U-2 pilots in the period from 2002 to 2009 was greater than experienced by United States military aviators in the preceding 47 years due in large part to longer, more frequent high-altitude exposure (74). The U-2 can climb to 60,000 feet in less than 45 minutes, which far exceeds the altitude and rate of ascent of a passenger airliner, which might take 30 to 40 minutes to reach a cruising altitude of only 35,000 feet. A review of decompression sickness cases associated with the NASA altitude physiological training program at Johnson Space Center indicated an incidence of 1.16 cases per 1000 exposures with significant heterogeneity across studies (31); denitrogenation time, exposure pressure, and exposure time were associated with the probability of decompression sickness.
Because decompression sickness is one of the most likely adverse effects among pilots of supersonic, high-altitude aircraft, they may require hyperbaric oxygen treatment before resuming active duty (107). An F/A-18D pilot, who presented with neurologic symptoms following a loss of cabin pressure at altitude, required multiple hyperbaric oxygen therapy sessions over several days due to the recurrence of symptoms on resumption of flying.
Neurologic decompression sickness in 50 high-altitude pilots was associated with a significant increase in the volume of hyperintense white matter lesions on MRI, especially in the insula; this was attributed to hypobaric exposure rather than hypoxia because all pilots were maintained on 100% oxygen throughout their flights (98).
Among United States military personnel exposed to extreme altitude-chamber exposures (from 29 tests comprising 708 altitude chamber exposures), important contributors to hypobaric decompression sickness included decompression "dose" (based on higher tissue ratio or bubble growth index), male gender, and high-intensity exercise at altitude (30).
Most cases of altitude-related decompression sickness occur among individuals exposed to altitudes of 25,000 feet or higher (103; 104).
Barotrauma. Barotrauma occurs when gas pressures across a membrane or surface differ sufficiently to cause damage.
Greater than 90% of the human body is either water or bone, which are effectively incompressible, leaving those structures that are filled with air or gas to be most directly affected by pressure changes: the middle ear, the Eustachian tube, the sinuses, the lungs, and the gastrointestinal tract.
-
Pulmonary compression barotrauma
(Source: Savioli G, Alfano C, Zanza C, et al. Dysbarism: an overview of an unusual medical emergency. Medicina [Kaunas] 2022;58[1]:104. Illustration by Gabriele Savioli. Creative Commons Attribution License [CC BY], https://cre...
-
Barotitis: external, middle, and inner
(Source: Savioli G, Alfano C, Zanza C, et al. Dysbarism: an overview of an unusual medical emergency. Medicina [Kaunas] 2022;58[1]:104. Illustration by Gabriele Savioli. Creative Commons Attribution License [CC BY], https://cre...
-
Decompression barotraumas
(Source: Savioli G, Alfano C, Zanza C, et al. Dysbarism: an overview of an unusual medical emergency. Medicina [Kaunas] 2022;58[1]:104. Illustration by Gabriele Savioli. Creative Commons Attribution License [CC BY], https://cre...
-
Pulmonary decompression barotrauma
(Source: Savioli G, Alfano C, Zanza C, et al. Dysbarism: an overview of an unusual medical emergency. Medicina [Kaunas] 2022;58[1]:104. Illustration by Gabriele Savioli. Creative Commons Attribution License [CC BY], https://cre...
-
Gastric decompression barotrauma
(Source: Savioli G, Alfano C, Zanza C, et al. Dysbarism: an overview of an unusual medical emergency. Medicina [Kaunas] 2022;58[1]:104. Illustration by Gabriele Savioli. Creative Commons Attribution License [CC BY], https://cre...
Barotrauma can occur either with an increase (eg, on descent while diving) or with a decrease (eg, on ascent while diving) of the ambient pressure. Under Boyle's Law, described by Anglo-Irish natural philosopher Robert Boyle (1627-1691), as external pressure increases, the gas volume in the body cavities containing air or other gas decreases (eg, lungs, middle ear, sinuses, gastrointestinal tract, etc.), as it will also in a face mask in which the pressure is not equalized with the ambient pressure. The opposite occurs when external pressure decreases. Iatrogenic barotrauma may, of course, also occur during intubation and mechanical ventilation (ie, “ventilator-associated lung injury” or “ventilator-induced lung injury”).
Inert gas narcosis. The mechanism of inert gas narcosis is not well understood, but it may result from gas dissolving into nerve membranes and causing a temporary disruption in nerve transmissions (82). Although the effect was first observed with air (due to the nitrogen content), other gases, including argon, krypton and hydrogen, cause very similar effects at higher than atmospheric pressure. Although some of these effects may be due to antagonism at NMDA receptors and potentiation of GABAA receptors, this is not likely to be the result of chemical bonding to receptors because these manifestations can be produced by breathing the very chemically inactive gas argon at high pressure.
Table: Signs and Symptoms of Nitrogen Narcosis, Breathing Air
|
Pressure (bar) |
Depth (m) |
Depth (ft) |
Symptoms |
|
1 to 2 |
0 to 10 |
0 to 33 |
Minor or none |
|
2 to 4 |
10 to 30 |
33 to 100 |
Mildly impaired reasoning
• Mild euphoria possible |
|
4 to 6 |
30 to 50 |
100 to 165 |
Sense of well-being
• Laughter and loquacity (in chambers)
• Over-confidence
• Anxiety (especially in cold, murky water)
• Delayed response to visual and auditory stimuli
• Reasoning and immediate memory affected more than motor coordination
• Calculation errors
• Idea fixation |
|
6 to 8 |
50 to 70 |
165 to 230 |
Sleepiness
• Impaired judgment
• Confusion
• Uncontrolled laughter, hysteria (in chamber)
• Terror in some
• Hallucinations
• Severe delay in response to signals, instructions, and other stimuli
• Occasional dizziness |
|
8 to 10 |
70 to 90 |
230 to 300 |
Stupefaction
• Poor concentration and mental confusion
• Decreased judgment
• Increased excitability
• Hallucinations
• Loss of memory
• Decreased dexterity |
|
10+ |
90+ |
300+ |
Euphoria, mania, or depressive states
• Disorganized time sense
• Hallucinations
• Dizziness
• Sense of impending blackout or of levitation
• Unconsciousness
• Death |
|
Note: a bar is defined as 100,000 Pa (100 kPa) or slightly less than the current average atmospheric pressure on Earth at sea level (1 atm, approx. 1.013 bar). Within a few percent, 1 bar = 100 kPa, approx. 1 at (or atmospheres absolute), approx. 1 atm, approx. 750 Torr, approx. 14.5 psi. |
Oxygen toxicity. Oxygen toxicity is caused by oxygen-derived free radicals generated by mitochondrial oxidoreductive processes, certain extra-mitochondrial enzymes (eg, xanthine/urate oxidase), auto-oxidative reactions, and phagocytes during bacterial killing. These free radicals create lipid peroxidations, especially in cell membranes, and disrupt nucleic acids and protein synthesis, leading to membrane rupture and cell death.
Management
On-site first aid. First aid of decompression sickness consists of on-site 100% oxygen, immobilization (ie, no unnecessary movement), and fluid administration; telephone consultation with a diving medicine specialist is recommended (78). Unfortunately, on-site first aid administration of oxygen is frequently omitted (26).
Medical transport. Rapid movement of a patient with decompression sickness may present difficulties when the site of the hyperbaric treatment facility is a considerable distance away. Fortunately, the movement of patients with decompression sickness by low-level helicopter flight is both safe and effective, especially when a pressurized aircraft is neither available nor practical. In one study, patients were transferred by low-level helicopter flight without evident complications when the helicopter stayed within 200 feet (61 meters) above ground level of the take-off point, but symptoms of decompression sickness did worsen when this altitude was exceeded (105). A more recent study found that subjective symptoms or oxygen levels of patients with decompression sickness may improve when the patient is transported in physician-staffed emergency helicopter flights less than 300 meters in height with the administration of oxygen and fluids (101).
Recompression and hyperbaric oxygen. The treatment of decompression sickness is, first and foremost, recompression. Treatment aims to reduce bubble growth, promote gas clearance, and counteract ischemia and hypoxia in the affected tissues. Therefore, if possible, treatment should be initiated before pathologic changes become irreversible.
Treatment is performed in a hyperbaric chamber following various hyperbaric oxygen protocols (11; 12; 05; 10; 71).
-
NASA decompression chamber at the Neutral Buoyancy Lab
(Source: Mike Renlund at https://www.flickr.com/photos/86078640@N00/2342068692. Creative Commons Attribution 2.0 Generic License [CC BY 2.0].)
-
Deck decompression chamber
(Photograph by Peter Southwood, taken on October 19, 2021. Creative Commons Attribution-Share Alike 3.0 Unported License, https://creativecommons.org/licenses/by-sa/3.0/deed.en.)
-
Decompression chamber training
Seaman Ethan Cypher gives the thumbs up to instructors as he and Seaman Jeff Finkel prepare to undergo decompression chamber training. Students at the Naval Diving and Salvage Training Center undergo various training scenarios ...
US Navy Treatment Table 6 has been used widely for mild decompression sickness, but shorter treatment schedules may be better, requiring fewer treatments until symptom resolution and more often accomplishing complete symptom resolution after the initial treatment (10). Hyperbaric oxygen therapy is effective in restoring and preserving neurologic function in the “perivenous syndrome” associated with decompression sickness in both animal and clinical studies (73).
In a retrospective study, hyperbaric oxygen therapy administered within 24 hours of the onset of type 1 decompression sickness was associated with rapid relief of symptoms after a single treatment (89). Seasoned military divers showed a faster response after recompression with fewer residual symptoms than commercial or recreational divers.
A patient with high-altitude decompression sickness recovered completely following hyperbaric oxygen therapy, recompression, and extracorporeal oxygenation (114). In another case, an unconscious stowaway was discovered in a wheel well of a Boeing 747-400F but recovered completely with hyperbaric oxygen therapy (111).
Despite oxygen first aid being given infrequently and long delays before definitive treatment, treatment outcome following decompression and hyperbaric oxygen therapy is generally satisfactory; at the end of hyperbaric oxygen treatment, most divers (65%) recover completely but many have significant residua (26).
In-water recompression. In-water recompression involves placing the affected diver back in the water at a depth of 9 meters with a prolonged pure oxygen-breathing period followed by gradual ascent to the surface (43; 136). In-water recompression has been used by several navies and in remote areas where local recompression chambers are not available. In-water recompression is not without risk and should only be carried out by divers with suitable equipment and practical training.
Decompression sickness-related circulatory shock. The pathophysiology and typical clinical course of decompression sickness-related shock support the use of aggressive but time-limited volume expansion and pressors to counteract hypovolemia (06). Hyperbaric oxygen therapy should be strongly considered for decompression sickness even in the face of extreme critical illness with refractory shock and respiratory failure (06).
Drug therapy. No drugs have been clearly demonstrated to benefit human decompression sickness. Aspirin is used frequently for the treatment of decompression sickness, but its efficacy has not been established by controlled studies. Fluoxetine, an antidepressant with anti-inflammatory properties, decreases the incidence of experimental decompression sickness in mice (15). Statin-mediated lipid reduction may reduce bubble generation via alterations in plasma rheology and surface tension. The use of high-dose steroids in decompression sickness is controversial.
Patent foramen ovale management. In divers with a history of major neurologic decompression symptoms, transesophageal echocardiography should be performed to exclude a right-to-left shunt (eg, patent foramen ovale, atrial septal defect, etc.). Divers with a history of decompression sickness and a cardiac right-to-left shunt should stop diving until the shunt has been corrected. Patent foramen ovale closure may reduce the risk of decompression sickness among divers, but adverse events may occur in up to 8% of those undergoing surgical correction (67; 41; 01). No difference is observed in the occurrence of venous bubbles between patent foramen ovale and patent foramen ovale closure groups, but catheter-based patent foramen ovale closure eliminates arterial bubbles after simulated dives (69). Divers with a history of decompression sickness may resume diving after patent foramen ovale closure with reasonable safety, but a conservative diving profile is recommended when there is a residual shunt after patent foramen ovale closure to minimize the risk of recurrent decompression sickness events (41). The subgroup of divers with an unclosed patent foramen ovale and a previous episode of serious decompression sickness may not be safe to dive, even within conservative limits (22).
In a meta-analysis of four observational studies with a total of 309 divers (141 with PFO closure and 168 without PFO closure), patent foramen ovale closure was associated with a significantly lower incidence of decompression sickness (PFO closure 2.8% versus no closure 11%; relative risk 0.29; 95% CI: 0.10 to 0.89; number needed to treat for an additional beneficial outcome = 11) (01). Adverse events occurred in 7.6% of patent foramen ovale closures, including tachyarrhythmias and bleeding.
In a study of a graded-strategy approach, divers with a high-grade patent foramen ovale were offered either catheter-based patent foramen ovale closure (the closure group) or advised conservative diving (high grades), whereas divers with a low-grade shunt were advised conservative diving (low grades), and those with no patent foramen ovale continued unrestricted diving (controls) (68). Among 702 divers who continued diving, decompression sickness incidence decreased significantly in all groups except the controls. During follow-up, there were no decompression sickness events in the closure group; decompression sickness incidence was similar to the controls in the low-grade group but remained higher in the high-grade group.