Sleep Disorders
Sleeptalking
Jan. 18, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Circadian rhythm issues are common and can impact health and quality of life. Delayed sleep-wake phase disorder (DSWPD) is characterized by late bedtime and wake times and an inherent delay of biological rhythms compared to the natural daylight. This pattern is frequently observed in adolescents and young adults and may cause chronic sleep deprivation, leading to compromise in school and work performance (40). Some investigators have considered delayed sleep-wake phase disorder as a marker or precursor for psychiatric and possibly neurologic issues. Delayed sleep-wake phase disorder may disguise itself as insomnia, attention deficit disorder, emotional or affective disorder, or maladjustment, and it can be somewhat similar to the schedule seen in restless legs syndrome. The delay in the body clock can be treated with a combination of lifestyle modifications, appropriately timed exposure to light, and melatonin.
|
• Delayed sleep-wake phase disorder is a relatively common circadian rhythm sleep disorder; it usually begins in adolescence and is manifested as habitually delayed time of sleep onset and waking. | |
|
• Delayed sleep-wake phase disorder may significantly impede academic and occupational achievements. | |
|
• Delayed sleep-wake phase disorder must be distinguished from other sleep disorders as the treatment approach is different. | |
|
• Treatment with appropriately timed melatonin and bright light, augmented with behavior and lifestyle modifications, may be effective. | |
|
• Relapses after cessation of treatment are common. |
Delayed sleep-wake phase disorder was first described in 1979 by a group of researchers and clinicians from Montefiore Medical Center in New York and Stanford University School of Medicine (61). The current formal name established in the third edition of the International Classification of Sleep Disorders (ICSD-3tr) is delayed sleep-wake phase disorder (01). Prior names include delayed sleep phase syndrome and circadian rhythm sleep disorder, delayed sleep phase type.
|
• The circadian rhythm influences many aspects of physiology. | |
|
• The circadian rhythm in delayed sleep-wake phase disorder is shifted later when compared to the social norms. Thus, patients have trouble falling asleep at night and trouble waking in the morning. | |
|
• Patients with delayed sleep-wake phase disorder have otherwise normal sleep except that the sleep occurs later in the night and waking occurs later in the morning or early afternoon. | |
|
• Many patients have more delay in their schedule over the weekends, making Sunday night and Monday morning symptoms worse. | |
|
• Individuals with delayed sleep phase disorder are more likely to have affective disorders and other detrimental health and behavioral effects. |
The circadian rhythm is an intrinsic body clock that modulates a variety of physiologic processes to anticipate upcoming events and physiologically prepares for those events. Although every system in the body has a circadian rhythm, one manifestation is the sleep-wake cycle, and it is estimated that between 10% and 20% of genes oscillate in a circadian fashion. The circadian rhythm provides a stimulus for alerting. Typically, this alerting signal from the circadian rhythm increases throughout the morning, decreases between 2:00 PM and 4:00 PM (associated with an “afternoon dip” in alertness), and increases through late afternoon to peak later in the evening. The alerting drive then decreases through the night to reach a low in the early morning before a slow rise prior to the morning awakening. In patients with delayed sleep-wake phase disorder, the circadian rhythm is delayed when compared to the typical day-night schedule, and therefore, sleep onset and the natural wake time is delayed, usually by more than 2 hours, in relation to conventional or socially acceptable time. This results in difficulty with sleep-initiation and difficulty awakening at the desired time for societal activities. When able to sleep and wake unrestricted, these patients will fall asleep very late at night and then sleep until late morning or early afternoon. The quality and quantity of their sleep is otherwise normal; however, it occurs at a time that is delayed when compared to the societal norms. These patients will frequently suffer from difficulty falling asleep, excessive morning sleepiness, and chronic sleep deprivation while trying to adhere to typical school or work schedules. This may result in disrupted vocational or social functioning. The complaint of daytime sleepiness depends partially on sleep deprivation resulting from an attempt to get up at conventional hours. Adolescents with delayed sleep-wake phase disorder commonly fall asleep during morning classes. Morning sleepiness in delayed sleep-wake phase disorder is also attributable to the delayed position of the "sleepy" phase of the circadian sleep-wake rhythm. Those who do manage to arise on time for school or a daytime job are awakening in the middle of their endogenous "night."
Another common presenting complaint is inability to fall asleep at the desired time at night. Patients typically do not feel sleepy until well past the desired bedtime. It may be difficult to clinically distinguish delayed sleep-wake phase disorder from insomnia. Insomnia patients tend to complain of fatigue and sleepiness while trying to go to bed but may feel more awake once in bed. Those with delayed sleep-wake phase disorder do not notice this evening sleepiness nor do they note feeling sleepy until late into the night or morning. Some patients may suffer from both delayed sleep-wake phase disorder and insomnia.
Patients with delayed sleep-wake phase disorder often have worsening delay on weekends when there is less constraint on the sleep-wake schedule. Patients may sleep until late morning or early afternoon in an attempt to “catch up.” Falling asleep on Sunday night tends to be very difficult due to progressive delay in circadian rhythm during the weekend. In adolescents, the battle over bedtime often becomes a major source of conflict between children and parents.
Some patients may have the presenting symptoms of depression or anxiety. The delay in their bedtime and wake time may be perceived as a mechanism of avoidance and not a circadian rhythm disorder. In addition, the delayed schedule may be a contributing factor to the mood issues (20).
|
• Patients with delayed sleep-wake phase disorder have a high rate of school and work tardiness and can frequently be labelled as lazy or depressed. |
Even in the absence of major psychopathology, serious occupational, school, and social dysfunction are complications of delayed sleep-wake phase disorder, occurring in 4% of adolescent and young adults (15). The disorder appears slightly more prevalent in male (4.7%) than female (2.7) Norwegian adults ages 18 to 35 years (53). Tardiness at school or work, absenteeism, and daytime sleepiness are the common precipitants for evaluation (44). Delayed sleep-wake phase disorder can be mistaken for school refusal. Difficulty waking in the morning has resulted in job loss and disciplinary measures in the military. Patients with delayed sleep-wake phase disorder may be labeled as lazy or mentally ill by their families, peers, or superiors in the business or school environment, solely on the basis of their inability to awaken in the morning. Sleepiness due to chronic sleep deprivation may make driving dangerous.
Prognosis of delayed sleep-wake phase disorder depends on a variety of factors, including how much sleep the patient needs (short sleepers tend to do better), family support, and most of all, the motivation of the patient to change the timing of sleep. Waking a sleeping teenager can be an unpleasant or even violent experience for the parents of a delayed sleep-wake phase disorder patient. If the parent-teen relationship is a difficult one, the control of bedtime and waking can become a major battleground. For most people who develop a mild delay (1 to 2 hours) in their sleep phase, simple behavioral measures can help with resetting their body clocks. However, for many patients with more significant delayed sleep phase syndrome, long-term management with multiple strategies is needed to help keep their circadian rhythm in synchronization with society.
Emerging evidence suggests that appropriately functioning circadian rhythms contribute to wellbeing, health, and cognitive performance (46). Studies indicate that delayed sleep-wake phase tendencies are linked to multiple psychiatric and medical health risks, especially in adolescents and young adults (04). Children aged 11 to 13 years who sleep less than 9 hours had an adjusted odds ratio of over 3.3 for developing delayed sleep phase syndrome. This risk seemed primarily related to early mental health issues (25). Individuals with a preference for the evening are more prone to depression (03). Adults with attention deficit hyperactivity disorder tend to show a delay in melatonin secretion and circadian timing, and a subgroup of patients with bipolar disorder appear to present with delayed sleep phase (56; 11; 58). A delayed sleep tendency may predispose individuals to type 2 diabetes and metabolic syndrome (63). Understanding the role of the circadian rhythm in psychiatric and medical conditions may serve an important role in evaluating risk and treatment strategies for such disorders.
A 16-year-old patient presents to clinic with a chief complaint of difficulty falling asleep, inability to wake in time for school, and excessive daytime sleepiness. Over the past 2 years, the patient describes an inability to go to sleep at a normal time. He characterizes himself as a “night owl.” He will fall asleep around 2:00 AM each night. He reports that he does not feel sleepy until that time. If he lies in bed, he will not feel tired or sleepy until he falls asleep around 2:00 AM and he will struggle to wake up at 7:00 AM for school. To occupy his time at night, he will play video games or use his computer until he feels sleepy. On weekends, he will routinely go to bed between 2:00 AM and 4:00 AM and wake between noon and 2:00 PM. He reports feeling less sleepy on weekends. Due to his late bedtime, he has been unable to wake up in time for school on multiple occasions and is now receiving homebound education due to numerous missed days.
In addition to reviewing good sleep hygiene practices and taking the cell phone out of the bedroom at night, the patient was prescribed 0.5 mg of synthetic melatonin at 8:00 PM each night along with lifestyle modification to avoid late night light exposure by wearing blue-blocking sunglasses after 8:00 PM. He was instructed to move his bedtime and wake time earlier by 15 minutes each day. He was also instructed to get as much light exposure as possible upon awakening in the morning initially after 10:00 AM. Over the course of 3 weeks, his sleep cycle eventually began to shift, and the patient was instructed to advance the morning light in 15-minute increments. Over the next 6 weeks the patient was able to go to bed at 10:00 PM and wake at 7:00 AM. He was able to successfully transition back to school. He was instructed to maintain the same sleep-wake schedule on both weekdays and weekends and continue wearing the nighttime blue light blocking sunglasses and use of melatonin.
|
• The circadian rhythm is inherent in every tissue of the body and influences many physiological processes to promote readiness of each organ system when typically needed. | |
|
• This rhythm can be influenced by specific stimuli, such as bright light, activity, food, and social interactions. | |
|
• The rhythm can become out of phase with the environment, especially if specific stimuli are present at times that can shift the circadian rhythm. |
The circadian rhythm is based on a genetic feedback loop that approximates 24 hours. Due to being genetically based, this rhythm is ubiquitous in every tissue, and thus, it relies on a complex system to synchronize the rhythm in every cell. Although most synchronization is primarily achieved through the suprachiasmatic nucleus, the suprachiasmatic nucleus relies on several environmental clues to synchronize the body’s overall clock with the natural world. These clues are primarily related to bright light, activity, food, and social interaction, with the strongest being bright light influence. Timed delivery of these stimuli will change the circadian rhythm. Thus, delivery of these stimuli in the evening will delay the clock, whereas delivery of these stimuli in a typical morning advances the clock. In our adolescent years, our response to bright light in the evening appears to be more intense and even low levels of light may delay our ability to fall asleep. Some individuals may maintain this increased sensitivity, whereas others may have the genetic predisposition for their body clocks to be delayed when compared to the rest of the society.
Delayed sleep-wake phase disorder is due to a misalignment between the body’s endogenous circadian rhythm and the social environment. The alerting signal from the circadian rhythm persists past the time in which the patient should be sleeping, and likewise, there is a delay in the rise of the alerting signal in the morning, leading to delay in awakening. The mechanism underlying delayed sleep-wake phase disorder involves a delay in the timing of the circadian pacemaker. Proposed causes for this delay include decreased response to the phase-advancing effect of morning light, an increased responsiveness to the delaying effects of evening light, and a longer than average circadian cycle. Although the etiology is unknown in most cases, studies show a genetic predisposition in familial cases due to polymorphisms in circadian clock genes. Patients may also have increased light exposure and increased activities at night that likely play a role (27; 39). In addition, some evidence of increased susceptibility to evening environmental clues, either by age or genetics, may play a significant role for some patients (27). This may be exacerbated by the patient’s activity pattern.
In order to understand how this misalignment occurs, it is important to understand the mechanisms that establish and modulate the circadian rhythm.
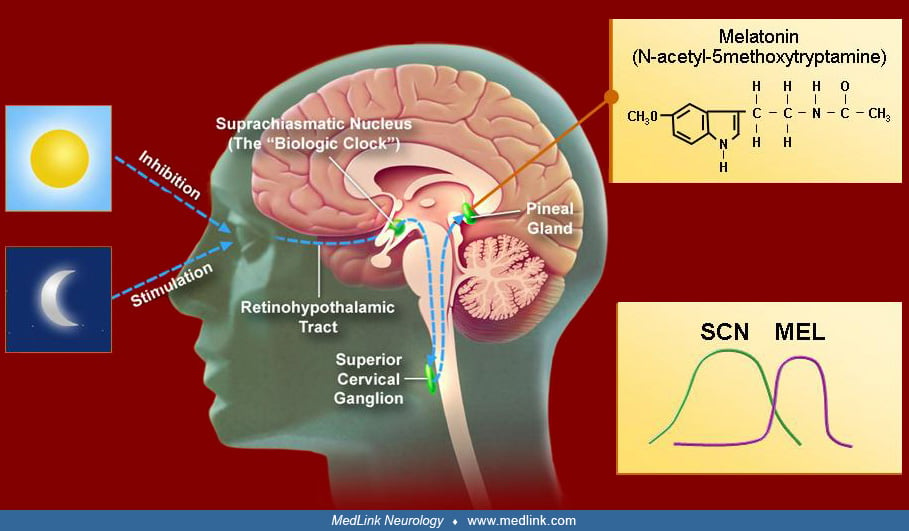
All living organisms possess an inherent circadian rhythm. This near 24-hour cycle modulates a variety of physiologic and behavioral processes, such as sleep-wake cycle, body temperature, mood, hormone secretion, and many others. The paired suprachiasmatic nuclei (SCN) of the hypothalamus have been established as the “master clock” that sets the timing of the mammalian circadian system. The SCN is composed of 10,000 anterior ventromedial hypothalamic neurons that maintain a self-sustaining daily rhythm. This cycle is achieved through a complex system of timed gene expression that creates an autoregulatory feedback loop. A variety of genes are involved in this cycle, including Clock, Per, Bmal1, and Cry.
The biological clocks of normal humans of all ages have a natural endogenous circadian cycle of slightly more than 24 hours, generally about 24.2 hours. Therefore, the internal body clock must be adjusted on a daily basis to align with the 24-hour day, a process called entrainment. Entrainment involves using zeitgebers (German for “time givers”) to reset the internal clock slightly each day. Common zeitgebers include light, melatonin, food intake, social interaction, and exercise. Each of these factors can independently change the timing of the circadian pacemaker, thereby altering the time of all physiologic processes that are regulated on a circadian basis.
Light is the main zeitgeber for endogenous clocks in humans. The human circadian system is more sensitive to short-wave blue-green light than to long-wave red-spectrum light. The major afferent input to the SCN consists of a melanopsin-containing subset of photosensitive retinal ganglion cells whose axons synapse on SCN cells.
This retinohypothalamic tract transmits nonvisual, light-dark information to the SCN, which is mediated through glutamate and pituitary cyclase-activating peptide (PACAP). In addition to a direct pathway, retinal ganglion cells also project to the intergeniculate leaflet of the lateral geniculate body, which in turn projects to the SCN. Neuropeptide Y and GABA are the main neurotransmitters. Other time clues appear to influence the SCN through serotonergic input from the brainstem raphe nuclei.
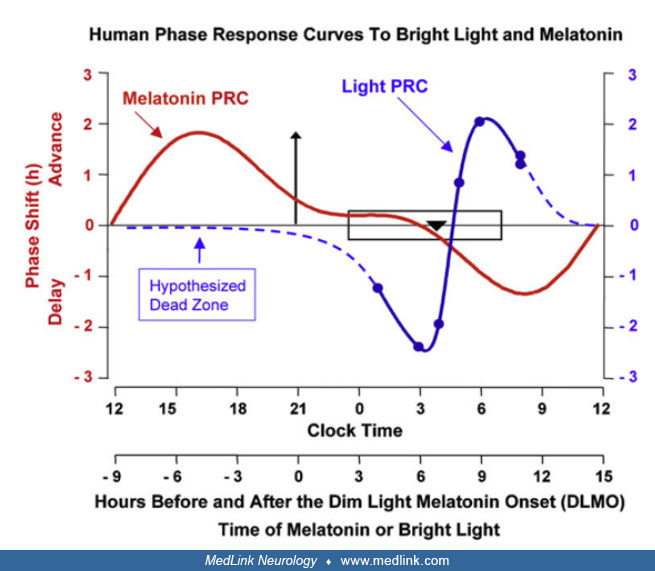
Key to understanding the zeitgebers is that the response of the circadian rhythm depends on when the stimulus is delivered. For example, light delivered prior to the temperature nadir (typically 4:00 AM in normal phase individuals) will cause a delay in the body clock. Light delivered after the body temperature nadir will advance the clock. Thus, for light therapy to be appropriately used, understanding the true timing of the circadian rhythm is essential. The temperature nadir is typically 1.5 to 2 hours before the undisturbed natural wake up time. Therefore, if a person is naturally waking at 11 AM without an alarm, the temperature nadir would most likely be between 9:00 and 9:30 AM.
Similar to light, melatonin also has a time-dependent effect on the phase of the circadian rhythm. However, melatonin has the opposite effect of light, such that melatonin delivered in the evening causes a phase advance whereas morning use may cause a mild phase delay. The SCN exhibit dense melatonin receptors, probably establishing a feedback mechanism for the sleep-wake cycle. Melatonin and potentially other factors such as light help synchronize the multitude of endogenous rhythms in the brain and other organs. Synchronization of these endogenous rhythms is important to optimal body function. Isolated delay in an endogenous rhythm has been implicated in individuals with nocturnal eating syndrome, which appears to be a delay in the feeding rhythm. Although appearing benign, in this disorder the timing of food intake can impact insulin sensitivity and metabolism (19).
Delayed sleep-wake phase disorder is theorized to develop due to multiple possible factors, including decreased response to the phase-advancing effect of morning light, an increased responsiveness to the delaying effects of evening light, and a longer than average circadian cycle. However, work shows that the magnitude of circadian shift with light exposure may be similar in adults regardless of age (28). This work, however, did not examine the potential influence of genetics. There are familial cases, indicating a genetic basis for delayed sleep-wake phase disorder. Susceptibility to delayed sleep-wake phase disorder may involve polymorphisms of the circadian gene Per3 and its promoter region (32). Variations in the Per2 gene, including the missense variant gene Rs35333999 commonly found in Europe and the missense variant p.Val1205Met found in a Japan population, are associated with later chronotypes (07; 38). Also, mutations in the Cyr gene have been implicated in one family with delayed sleep phase (42). Behavioral factors such as late-night light exposure through television, computer screens, and smartphones also play an important role.
Unfortunately, the other time clues of activity, social interaction, and food have not been studied. These may also have specific effects in particular ages, especially recognizing the synchronizing effects of stimuli such as food on the brain and other organ systems (10). Individuals with the majority of their calorie intake later in evening, known as nocturnal eating syndrome, frequently have features similar to delayed sleep phase syndrome (36).
Delayed sleep-wake phase disorder is more common in adolescents and young adults. Several studies show the incidence of delayed sleep phase disorder range from 4% to 14% in the population of adolescents compared to 1.5% of all adults (41; 15). Patients with delayed sleep-wake phase disorder comprise 7% to 10% of the patients with insomnia referred to sleep clinics. The duration of delayed sleep-wake phase disorder symptoms preceding diagnosis varies from months to decades. The syndrome onset has been reported as early as prepubertal childhood and as late as the sixth decade (01). Adolescence, however, appears to be a particularly vulnerable life stage for the development of the syndrome. Both genders are equally affected. Newer work suggests that phase changes may also be influenced by genetic predisposition and ethnicity (17).
|
• Avoidance of light emitting devices and maintaining the same sleep-wake schedule can help prevent delaying the inherent sleep phase. |
The incidence of the delayed sleep-wake phase disorder and its severity of symptoms may be modified by better education of parents, students, and health care workers. Emphasis on good sleep hygiene, with a particular focus on maintaining the same sleep schedule on weekends and weekdays, is important. Elimination of late night light exposure, such as computers and cell phone, may also help preclude delayed sleep-wake phase disorder. Individuals with delayed sleep phase had less light in the early portion of their day, thus not advancing their body clock (62). Similarly, using a light emitting tablet compared to reading printed material in the evening, the tablet delayed bedtime by a half hour and delayed the melatonin secretion onset by 50 minutes (09). Light in the evening also has an effect in children. Children appear to be sensitive to evening light in suppressing their melatonin secretion and causing delay in the sleep phase (23; 24). Therefore, evening light exposure should be limited for this age group to prevent the development of delayed sleep phase.
Delayed sleep-wake phase disorder must be distinguished from other common issues that cause insomnia or hypersomnia. Many individuals without delayed sleep phase, particularly adolescents, adopt late bedtime and awakening hours. They adjust promptly to temporary periods of sleep-onset delay due to late-night studying or work followed by oversleeping to recover (eg, on weekends) and do not develop chronically delayed sleep onset nor oversleep when they resume a more conventional schedule. Additionally, some individuals adopt a social jetlag that is exacerbated by late night screen time (65). The patient who can adapt to a strictly imposed schedule and sleep normally within 7 to 10 days probably does not have true delayed sleep phase. The chronic inability to advance the schedule is the hallmark of delayed sleep-wake phase disorder.
Chronic insomnia disorders, such as idiopathic insomnia and psychophysiological insomnia, will also have delayed sleep onset. These patients are typically tired and sleepy but are unable to fall asleep, unlike patients with delayed sleep-wake phase disorder, who typically report not feeling sleepy until late at night. Restless legs syndrome may cause delayed sleep but is easily distinguished clinically from delayed sleep-wake phase disorder based on clinical complaints of the need to move to improve the symptoms. The two disorders may often occur together. Late sleep onset may also occur in association with the onset of a major psychiatric illness, particularly the manic phase of bipolar disorder and in schizophrenic decompensation. A chronic pattern of sleep phase delay is sometimes seen in individuals avoiding social interaction (eg, personality disorders); a response to a rigidly imposed schedule may help narrow the differential diagnosis.
Morning sleepiness and hypersomnia are seen in a variety of disorders with inadequate or disrupted sleep. Insufficient sleep syndrome and those with long sleep time will often have morning sleepiness. Patients with insufficient sleep have less trouble falling asleep earlier and improve with the extension of the time dedicated to sleep. Similarly, disorders that can disrupt sleep, such as sleep-related breathing disorders and periodic limb movement disorder, can present with morning sleepiness and be confused with delayed sleep-wake phase disorder. Central causes of hypersomnolence, including narcolepsy, should be considered. Narcolepsy patients often describe difficulty with sleep initiation.
Some patients may present with the most pressing feature of delay in eating the majority of the calories. This disorder is called nocturnal eating syndrome and may occur with delayed sleep-wake phase disorder or have very similar features of a delay in sleep wake phase (36). The key distinction would be if the major symptom is related to the late eating, then the diagnosis would be nocturnal eating syndrome. Because patients with nocturnal eating syndrome may have a similar delay in the circadian rhythm, similar treatment may coincide.
Patients with delayed sleep-wake phase disorder may present with features of insomnia and excessive daytime sleepiness. Commonly, the patients focus on one of these issues, and the other issue is not felt to be as concerning, thus it is typically not mentioned. Because patients with circadian rhythm disorder can present with either insomnia or hypersomnia as a major complaint, patients with insomnia or hypersomnia need thorough questioning and possibly a sleep diary or actigraphy to determine the possible role the circadian rhythm may play.
Other circadian rhythm disorders can be confused with delayed sleep-wake phase disorder. Advanced sleep-wake phase disorder is associated with individuals falling asleep early in the evening and waking typically prior to 4:00 AM. Non-24-hour sleep wake disorder can commonly be confused with delayed sleep-wake phase disorder, but in patients with non-24-hour sleep wake disorder, their circadian rhythm continues to gradually move later each day, causing a cycling of symptoms across the day night period (see non-24-hour sleep wake disorder). Irregular sleep wake disorder is characterized by three major bouts of sleep across the 24-hour period. All of these may have features in common with delayed sleep-wake phase disorder and can become more obvious with the actigraphy or sleep logs.
Affective disorders are frequently associated with circadian rhythm disorders. In adolescents and young adults, depression is associated with delayed sleep-wake phase disorder. These disorders appear to have a bidirectional interaction whereby delayed sleep phase increases the risk of developing affective disorder, and the affective disorder increases the risk of development of the delayed sleep phase (26). Other affective issues such as bipolar disorder and schizophrenia have been associated with delayed sleep-wake phase disorder (29; 30). Similarly, borderline personality disorder and those with obsessive compulsive disorder appear to have a preponderance of comorbid circadian issues including delayed sleep phase disorder (37; 12). Also, adults with attention deficit and hyperactivity disorder have a higher likelihood of delayed sleep phase (59). Thus, individuals with mood issues and learning difficulties should be asked about their sleep pattern, and those with delayed sleep phase should be asked about possible underlying mood issues. Those with mental disorders such as depression appear to have worse outcomes in relationship to cognitive functioning, social interactions, and quality of life (57). This may highlight the need for questioning and possible correction of the sleep phase to improve outcomes.
Another concern is overall healthy habits and cardiovascular health. Individuals with delayed sleep phase are more likely to smoke and to have less healthy habits, and they are less likely to engage and gain from healthy habits, such as exercise (21; 16). Individuals who are more likely to be sleep deprived because of their delayed schedule appear to also carry a higher risk of dyslipidemia and downstream arteriosclerotic issues (14).
|
• Actigraphy or a sleep diary tracking the patient’s sleep wake pattern for at least 7 and preferably 14 days is essential to making the diagnosis of delayed sleep wake phase disorder. |
In an otherwise healthy patient with a normal neurologic examination, the diagnosis of delayed sleep-wake phase disorder only requires obtaining the characteristic history and confirming it with a sleep log or actigraphy. The ICSD-3 established five diagnostic criteria that must be met for the diagnosis of delayed sleep-wake phase disorder: (1) there is a significant delay in the major sleep episode compared to the desired or required wake time and sleep time; (2) symptoms last for at least 3 months; (3) when patients are free to choose their own sleep schedule, they show improved sleep quality and duration. They maintain a delayed phase in their sleep-wake pattern; (4) sleep logs and, if possible actigraphy, for at least 7 and preferably 14 days show delay in timing of the sleep period; (5) the sleep disturbance is not better explained by another etiology (55; 01).
Polysomnography is not indicated in typical cases of delayed sleep-wake phase disorder. However, if the patient has symptoms of sleep apnea or sleepiness throughout the 24-hour period despite adequate time to rest, a sleep study would be indicated.
Demonstration of delayed DLMO may serve in the future as a laboratory confirmation for delayed sleep onset syndrome (06). Samples are easily obtained through salivary sampling.
|
• Timing of melatonin 4 to 6 hours in advance of bedtime is key to advancing the circadian rhythm. | |
|
• Blue light blocking sunglasses used in the evening until bedtime may help in advancing the circadian rhythm. | |
|
• Light therapy should be delivered after the temperature nadir, thus approximately around the undisturbed wake up time of the patient. Light therapy delivered prior to the temperature nadir will cause further delay of the circadian rhythm. |
Treatments for delayed sleep-wake phase disorder aim to achieve sustained phase shift to synchronize the circadian sleep-wake signals to the desired sleep-wake schedule. This is achieved through a combination of behavioral modification and pharmacologic interventions. The main treatment approach involves timing of light exposure, exogenous melatonin, and chronotherapy. Although slow advancement of the bedtime and wake time can help advance the body clock, taking melatonin in the early evening and having exposure to bright light in the morning after the temperature nadir maintains the phase advancement better than providing a strict wake-time schedule (50; 02). General measures to improve sleep hygiene may help to consolidate and maintain the new schedule.
Timing of light exposure is a vital part of treatment. Light is the most important zeitgeber to the circadian oscillator. Bright light exposure has phase-shifting effects, with phase delay or advance following late evening or early morning exposure, respectively. In the first controlled human study, enhancement of the morning time cue with bright light (2500 lux full spectrum light between 7:00 AM and 9:00 AM) was helpful in 20 patients with delayed sleep-wake phase disorder (02). More studies followed that employed different protocols of light intensity and timing, including the use of blue light emitting glasses that appear to be helpful (31). Daily light exposure sessions are probably needed to maintain phase shift. However, two long-term studies showed that benefits did not persist (22). Because phase-response curves for melatonin and light are at nearly 180° phase angle difference to each other, it is possible to use combined light-melatonin treatment with proper timing of each in order to increase the success rate of the treatment of circadian rhythm disorders (43). An additional consideration is daylight savings time. The condition of sunlight exposure later in the evening may exacerbate the delay in the sleep-wake schedule. Reis and colleagues found that patients did better on standard time, compared to having daylight “later” in the schedule as in daylight savings time (47). Patients may need to wear blue light–blocking sunglasses when outside in the evening.
Many commercial light boxes are available, varying in design and light intensity. Longer periods of moderate intensity light may be more effective than a shorter exposure period of high intensity light.
Physiological doses of exogenous melatonin (less than 1 mg) were found to shift circadian phase and advance the time of sleep onset in as few as 5 days (54). A modest phase advancing effect of doses up to 5 mg of melatonin given in the evening was shown in patients with delayed sleep-wake phase disorder (02). Controlled-release melatonin was also effective in improving sleep in children with delayed sleep-wake phase disorder and neurodevelopmental disability (05). In one of the largest series reported to date (61 patients), evening melatonin was effective in 96.7%; however, the vast majority relapsed after melatonin was discontinued. Many patients relapsed a long time after melatonin wash out (2 months or more), and these patients tended to have milder delayed sleep-wake phase disorder than patients with immediate relapse (up to 1 week after discontinuing melatonin). The timing of melatonin administration seems to be more important than the dose (02); the largest phase advance is achieved when melatonin is administered 5 to 6 hours before the individual’s DLMO. The review and practice parameters of the American Academy of Sleep Medicine state that melatonin is indicated as a therapy for patients with delayed sleep-wake phase disorder (02). Similarly, a review of the use of melatonin for delayed sleep-wake phase disorder in children and adolescents showed relatively consistent results in reducing sleep latency by 22 to 60 minutes, with no relevant adverse effects (35). This response is also noted in children with some neurodevelopmental disorders (49). Some of the melatonin effect may be related to the underlying genetics. Magee and colleagues examined the response to melatonin 1 hour before the desired bedtime in individuals with delayed sleep phase disorder and subdivided the groups based on the Period 3 gene polymorphism (34). These investigators found those with PER 3 4/4 had greater subjective improvement in sleep latency. However, there were no significant differences when compared to other polymorphisms on objective sleep latency from actigraphy. The key to this work suggests that responses may be different based on the underlying genetic polymorphism, and further investigation of the relationship of polymorphisms and circadian responses is needed. The response may also vary depending on other underlying disorders. In patients with bipolar disorder and treatment with timed melatonin, one single-arm study found improvement in sleep time and efficiency in those with self-reported delayed sleep phase (13). Overall, melatonin seems promising in the treatment of delayed sleep-wake phase disorder, although its effect seems to last only as long as it is administered. Major issues such as the optimal timing and dose remain to be evaluated; the doses employed in various studies range from 0.3 to 5 mg. Long-term safety of melatonin also needs to be determined, although up to 1000 mg per day have been administered for 30 days without major side effects except drowsiness. This hormone is not currently approved in the United States, except as an investigational agent; it is available, however, as a nonprescription supplement, raising questions as to the standardization and purity of various preparations. The U.S. FDA approved ramelteon, a highly selective melatonin agonist with high affinity to melatonin MT1 and MT2 receptors, as a medication for insomnia. In preliminary studies ramelteon was shown to shift circadian phase in both animals and humans (02). This shift was also seen with low dose ramelteon in the 0.14 to 1.2 mg range and appears to shift individuals as much as 3 hours over 2 weeks (52). Another melatonin agonist, tasimelteon, was found to effectively shift a circadian phase and improve sleep in simulated jet lag as well as helping the free running circadian rhythm in non-24-hour sleep-wake rhythm disorder (45; 33). These may start an era of standardized melatonin agonist preparations with selective activity at various receptors, thus, enabling specific therapeutic effects. The dopamine blocking agent, agomelatine, also has demonstrated some benefit in advancing sleep phase in young adults. This compound is not approved in the United States but is available in Europe and Australia (64).
One approach is to combine melatonin therapy in the evening and providing light therapy in the morning. This approach was successful in advancing the DLMO in healthy subjects. Unfortunately, Cheng and colleagues showed in a systematic review of studies utilizing this combined therapy that in subjects with delayed sleep phase it produced no clear benefit (08). Thus, combining therapy may not be as beneficial as once thought.
Alternatively blocking blue light in the evening may be beneficial for advancing sleep phase in this population. In this small open label study, eight subjects with delayed sleep wake phase disorder wore blue light blocking glasses in the evening for 2 weeks and showed an average of 78 minutes of phase advance in DLMO and over 2 hour advance in their sleep onset time (18). In two other studies using morning exercise as the stimulus, subjects with delayed sleep phase also appeared to advance their phase with as little as 4 days of morning exercise (48).
Slowly advancing a patient’s circadian rhythm is most effective with a combination of avoiding late night light exposure, low-dose melatonin, and early morning light exposure, along with slowly moving bedtime and wake time by 10 to 15 minutes each day. Once the patient arrives at the appropriate sleep timing, it is imperative to maintain this schedule by avoiding bright light prior to bed and exposing themselves to bright morning light. Low-dose melatonin may be necessary to maintain the circadian phase.
Long-term success in the treatment of delayed sleep-wake phase disorder is probably difficult to achieve because it is unclear whether chronobiological interventions change the inherent tendency to relapse. To maintain a “normal” sleep-wake pattern, improving the sleep hygiene and adhering to a strict schedule are no less important than various interventions; these may prove difficult in the long run because lifestyle changes need to be maintained.
Pregnancy is frequently a time of disturbed sleep. Although little is known about the circadian rhythm during pregnancy, some animal models suggest that maternal chronodisruption may have effects on the offspring (60). The sleep phase may also have a resulting effect for women during and after pregnancy. Delayed sleep phase appears to be a clue as to the possible development of depression. Postpartum women with delayed sleep phase appear to have more weight retention (51). Each of these demonstrate clues how the circadian rhythm may hallmark and impact maternal health.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Bradley V Vaughn MD
Dr. Vaughn of UNC Hospital Chapel Hill and University of North Carolina School of Medicine has no relevant financial relationships to disclose.
See Profile
Antonio Culebras MD FAAN FAHA FAASM
Dr. Culebras of SUNY Upstate Medical University at Syracuse has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jan. 18, 2025
Sleep Disorders
Dec. 03, 2024
Sleep Disorders
Dec. 01, 2024
General Neurology
Nov. 09, 2024
Sleep Disorders
Nov. 04, 2024
Sleep Disorders
Oct. 31, 2024
Sleep Disorders
Oct. 27, 2024
Sleep Disorders
Oct. 14, 2024