







Infectious Disorders
Creutzfeldt-Jakob disease
Dec. 27, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
CNS infections affect populations worldwide. Although relatively rare compared to other sites of infection, high morbidity, mortality, and long-term sequelae make many CNS infections a neurologic emergency requiring prompt diagnosis and rapid initiation of targeted antimicrobial treatment. The widespread use of molecular diagnostics incorporating multiplex nucleic acid amplification of common CNS pathogens, such as the FilmArray Meningitis/Encephalitis Panel (BioFire Diagnostics, Salt Lake City, UT), combined with emerging unbiased metagenomic sequencing, has immensely shortened the turnaround time for identification of the culprit organism and detection of rare or unexpected pathogens. Despite the promise these novel techniques offer, diagnosing CNS infections remains a challenge. A comprehensive approach should incorporate thorough history-taking, neurologic examination, knowledge of pathogens endemic to the area of interest, and formulation of a differential diagnosis supported by imaging studies, serology, and CSF analysis when feasible.
• CNS infections have high morbidity and mortality, which highlights the importance of an accurate and timely diagnosis. | |
• Diagnosing CNS infection requires a comprehensive approach that includes a detailed history and physical examination, CSF analysis when feasible, neuroimaging, and targeted microbial testing. | |
• It is important to recognize the strengths and weaknesses of available tests for CNS infections as well as the chosen source of specimen (CSF vs. serum vs. others) in order to choose the method most likely to yield an accurate result. |
James Leonard Corning first performed CSF analysis in 1885, which led to the performance of the first lumbar puncture by Heinrich Quincke a few years later. Robust identification and description of microorganisms followed at the turn of the 20th century and led to the description of the most common bacteria isolated from the CSF as a cause of meningitis (49). Viruses were harder to identify; the earliest reports suggesting herpes simplex virus as a causative agent of encephalitis in humans appeared in the 1920s (07), and for the better part of the 20th century, histopathological diagnosis by visualizing the necrotizing characteristics of the virus on biopsy or autopsy remained the gold standard for diagnosis (53). The development of PCR in 1983 revolutionized the field of molecular diagnostics and was the cornerstone that led to the creation of monoplex real-time PCR assays, followed by multiplex PCR meningitis/encephalitis panels, which are instrumental in rapidly diagnosing the most common CNS infections (see Molecular diagnosis of CNS infections).
The approach to a patient with suspected CNS infection begins with an attempt to identify the anatomical location of the inflammation, which may allow a targeted approach to determine the causative organism. CNS infections can be approached based on the presenting clinical syndrome, including meningitis, encephalitis, meningoencephalitis, space-occupying rim enhancing lesions in the brain or spine, cerebrovascular involvement, myelitis, and myeloradiculitis. Certain microorganisms have specific tropism in the CNS, for example, the mesiotemporal lobes and insula in Herpes simplex virus (01), rhombencephalitis in Listeria monocytogenes (06), and deep brain lesions as seen with West Nile virus, Japanese encephalitis virus (01), and toxoplasmosis (14).
Occasionally, some CNS infections are associated with pathognomonic clinical presentations that would facilitate, when present, the diagnostic process, such as the oculomasticatory myorrhythmias seen in CNS Whipple disease caused by Tropheryma whipplei (02).
Establishing the etiology of neuroinflammatory diseases, whether infectious or autoimmune, is particularly challenging given the significant overlapping clinical and radiographic manifestations, which necessitate consideration of multiple tests and hypotheses simultaneously. History should include onset, course of illness, travel and exposures, drug use, sexual and dietary habits, immune status (competent vs. compromised), recent vaccinations, animal contact, sick contact, seasonality, and geographic exposures to endemic diseases.
The acuity and severity of CNS infections depend on the type of the organism and the part of the CNS involved. Bacterial meningitis is uniformly fatal if untreated. Even with treatment it may cause acute hydrocephalus in 5% of patients (mainly communicating, but rarely obstructive) and seizures in 17% to 50% (especially in children with pneumococcal meningitis). Both of these complications are poor prognostic factors and increase the risk of death. Other complications include cerebral edema, increased intracranial pressure, cerebral venous thrombosis, ischemic and hemorrhagic strokes, and subdural empyema. Long-term sequelae involve hearing loss, residual focal deficits, cognitive impairment, and epilepsy (24).
Although viral meningitis is a much more benign process that is self-limited and seldom requires any antiviral treatment, viral encephalitis can lead to devastating consequences if not treated promptly and, even with appropriate interventions, can leave permanent deficits (26). Age above 65 years, a compromised immune system, a Glasgow Coma Scale of 8 or less and a need for intensive care unit admission, and delay in initiating acyclovir are all poor prognostic factors for Herpes simplex virus encephalitis (50). Among those who recover from Herpes simplex virus encephalitis, up to 20% develop postherpetic autoimmune encephalitis with antibodies to the N-methyl-D-aspartate receptor [NMDAR] that can mimic Herpes simplex virus encephalitis relapse, typically between 2 to 6 weeks after initial diagnosis (11).
CNS fungal infections are challenging to diagnose due to their rarity and can be life-threatening and have a fulminant course if not rapidly diagnosed. Cryptococcal meningoencephalitis is the most common fungal CNS infection and is fatal without treatment. Even with optimal care, the 3-month mortality approaches 20% in persons living with HIV (PLWH) and 20% to 30% of non-HIV nontransplant patients (15).
In space-occupying lesions, such as abscesses and toxoplasmosis, increased intracranial pressure, midline shift, and herniation are the most feared complications. Spinal canal abscesses are also emergent as they can cause spinal cord compression, blood supply compromise, and septic thrombophlebitis (24).
Infectious invasion of the cerebrovascular system can also be difficult to identify given the similarities in presentation to other noninfectious causes of stroke and requires a high margin of suspicion. Varicella-zoster virus, syphilis, tuberculosis, aspergillosis, and acute bacterial meningitis can all cause ischemic or hemorrhagic stroke and aneurysm formation (44).
Prion diseases, also referred to as “transmissible spongiform encephalopathies,” are a group of fatal neurodegenerative diseases caused by conversion of the normal prion related-protein (PrPC, “C” for cellular), which is predominantly alpha-helical, into an abnormal beta-pleated form called the prion (PrPSc, “Sc” for scrapie), meaning proteinaceous infectious particle (13). Most cases are sporadic, such as Creutzfeldt-Jakob disease, but there are transmissible forms, such as Kuru due to human cannibalism and bovine spongiform encephalopathy or “mad cow disease” due to consumption of meat from affected cattle, hence, the classification with other CNS infections. Clinically, patients with Creutzfeldt-Jakob disease present with rapidly progressive dementia with cortical dysfunction (eg, aphasia, apraxic and neglect), personality changes, ataxia, extrapyramidal features, exaggerated startle response, myoclonus, and eventual akinetic mutism. Creutzfeldt-Jakob disease is universally fatal, with a median of 5 months from diagnosis to death and 90% of patients dead within 1 year (13).
Initial screening laboratory studies should assess electrolytes, renal and liver function abnormalities, presence of leukocytosis, and markers of inflammation (eg, sedimentation rate, C-reactive protein, and procalcitonin). HIV status should be assessed in all patients for whom it is unknown as this can widely alter the differential diagnosis and management. Microbiological testing should start with the most likely or “can’t miss” pathogens. Because of the urgency of both diagnosis and treatment, testing for multiple possible diseases and simultaneous empiric treatment are often necessary. Blood cultures should be drawn immediately. Interferon-gamma release assays and serum serological testing for microbial pathogens may be done less urgently in appropriate situations. Although nonspecific, some electrolyte abnormalities can add helpful data to the diagnostic algorithm; for example, hyponatremia can be seen in up to 45% of patients with tuberculous meningitis, mainly due to cerebral salt-wasting syndrome (29).
Timely CSF analysis is crucial to the diagnosis of most CNS infections, but in the presence of intracranial mass lesions, lumbar puncture can theoretically lead to downward herniation. Although guidelines vary slightly, there is general agreement that CT should be performed prior to lumbar puncture in a patient with any of the following: severely altered mental status (GCS< 10), new-onset seizures, focal neurologic deficits (other than cranial nerve palsies), or a severely immunocompromised state. Otherwise, lumbar puncture should be obtained immediately (before CT) to avoid delays in management (51). In addition to the studies detailed below, storing extra CSF and sera is advised as it allows for subsequent testing without the need to repeat lumbar puncture and also allows interpretation of results without the confounding effects of antimicrobials, steroids, and the occasional immunotherapy, such as intravenous immunoglobins (IVIg) in more diagnostically challenging cases. In such situations, testing CSF and sera in parallel for antibodies and autoantibodies can be performed.
Ancillary testing, such as EEG, should be performed for patients with unexplained or persistent altered mental status or high suspicion of seizure activity. The EEG pattern itself, in the absence of active seizures, is usually nonspecific with diffuse slowing. Nonetheless, it can help recognize certain cases by demonstrating characteristic interictal patterns, such as the lateralized periodic discharges seen with Herpes simplex virus encephalitis, or the classic 1- to 2-Hz periodic sharp-wave (often biphasic or triphasic) complexes seen in late Creutzfeldt-Jakob disease (13). It may also help identify noninfectious etiologies of encephalitis, such as the presence of extreme delta brush, which is characteristic for anti-NMDAR encephalitis and heralds a poorer prognosis (30).
The specificity of neuroimaging in the workup of CNS infection is on a spectrum from normal or nonspecific in cases of mild meningitis to highly diagnostic when paired with the appropriate clinical manifestation and knowledge of pathogens’ neurotropism, such as Herpes simplex virus encephalitis. Head CT without contrast can be a helpful first step in the presence of focal neurologic deficits and altered mental status. Hydrocephalus, subdural effusions, and mass effect can be easily identified on CT. MRI with intravenous gadolinium allows for better characterization of such CT findings and may detect more subtle changes not visible on CT. Brain CT with contrast can be used in cases where MRI is not available or its use is contraindicated (43).
Neuroimaging can help differentiate CNS infectious syndromes (see Table 1). In cases of severe purulent meningitis, findings can include leptomeningeal and cisternal enhancement, hydrocephalus, ependymal enhancement (indicating ventriculitis), ischemic infarction, and subdural empyema.
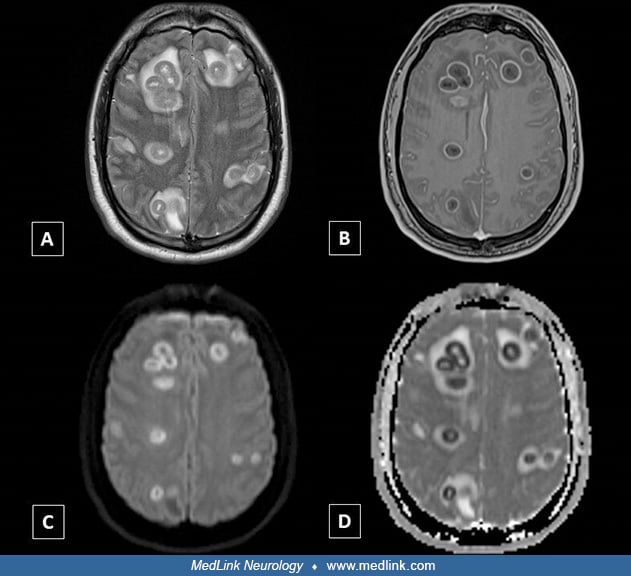
Purulent debris in the brain or extra-axial spaces may be identified as hyperintensities on diffusion-weighted imaging. Pyogenic brain abscesses characteristically demonstrate ring enhancement of the capsule with intravenous contrast and surrounding edema (hypodensity on CT or T2 hyperintensity on MRI). The abscess central cavity is typically CSF isointense on MRI, with a T1 hyperintense and T2 hypointense rim. Diffusion-weighted imaging sequences can be helpful in differentiating abscesses from tumors and other cystic masses as abscesses may demonstrate strong diffusion restriction secondary to the pus within the cavity.
The differential diagnosis of ring-enhancing lesions should be broadened in immunocompromised patients to include nonpyogenic abscesses, such as tuberculoma, toxoplasmosis, and aspergilloma (14; 15).
Cerebrovascular imaging involves multiple techniques, such as MR or CT angiography, digitally subtracted angiography, and high-resolution MRI with contrast-enhanced vessel wall imaging. Vessel imaging may be helpful for demonstrating parainfectious vasculopathy with the characteristic findings of segmental constriction and occlusion with poststenotic dilatation, creating the classic “beading” appearance typically seen with vasculitis of different etiologies (44).
Aside from CNS imaging, body imaging can be considered; for example, a CT of the chest may be considered when there is high suspicion of disseminated infections with hematogenous spread (such as tuberculosis and fungal infections). Transthoracic or transesophageal echocardiogram should be performed in cases of suspected endocarditis with septic emboli.
Syndrome | Most commonly associated pathogens | Differential diagnosis |
Meningitis | Multiple; severe acute meningitis usually points to bacterial etiology | |
- Basal enhancement: tuberculosis or fungal meningitis | - Neurosarcoidosis can cause basal meningitis | |
Encephalitis | - Limbic (temporal, insular, cingulate gyrus): Herpes simplex virus, cytomegalovirus, adenovirus, syphilis | - Autoimmune limbic encephalitis (anti-NMDA, LGI-1, AMPA) |
- Deep brain, bithalamic, basal ganglia (46): rabies, West Nile virus, Japanese encephalitis virus, eastern equine virus, Powassan virus, Cryptococcus, mucormycosis, toxoplasmosis, Creutzfeldt-Jakob disease (hockey sign: involvement of the head of the caudate with the ipsilateral thalamus) | - Deep venous sinus thrombosis and top of the basilar syndrome - Acute necrotizing encephalopathy (eg, secondary to COVID-19) - Metabolic causes (eg, Wernicke encephalopathy and osmotic myelinolysis) | |
- Brainstem: listeria, rabies, brucella, enteroviruses A71 and D68, Herpes simplex virus1, Eastern equine virus, Powassan virus, Japanese encephalitis virus, Whipple disease | - Autoimmune encephalitis (anti- IgLON5, DPPX) - Behçet disease | |
- Hemispheric, cortical: Creutzfeldt-Jakob disease (cortical ribboning) | - Acute disseminated encephalomyelitis | |
- Subcortical white matter: JC virus leading to progressive multifocal leukoencephalopathy | - Other inherited leukodystrophies | |
- Cerebellar: varicella-zoster virus, Epstein-Barr virus, mumps, listeria, brucella, Powassan virus, St. Louis encephalitis virus | ||
Space-occupying, rim enhancing lesions | Pyogenic abscesses, toxoplasmosis, many fungal infections, some parasitic infections, such as neurocysticercosis and trichinellosis (48) | - Neoplasm due to primary brain tumor or metastatic disease - Tumefactive demyelination - Subacute stroke |
Cerebrovascular involvement | Severe purulent meningitis, tuberculosis, syphilis, invasive aspergillosis, endocarditis - Signs of vasculitis: varicella-zoster virus, tuberculosis, syphilis | - Noninfectious etiology of stroke - Primary CNS angiitis |
Myelitis | HIV, HTLV-1, and HTLV-2, cytomegalovirus, varicella-zoster virus, polioviruses and nonpolio enteroviruses (acute flaccid myelitis), rabies, and tabes dorsalis in syphilis. Varicella-zoster virus and Lyme may cause focal myeloradiculitis. | Inflammatory myelopathies (multiple sclerosis, neuromyelitis optica spectrum disorders, neurosarcoidosis); toxic metabolic (Vitamin B12 deficiency), vascular, and compressive myelopathies |
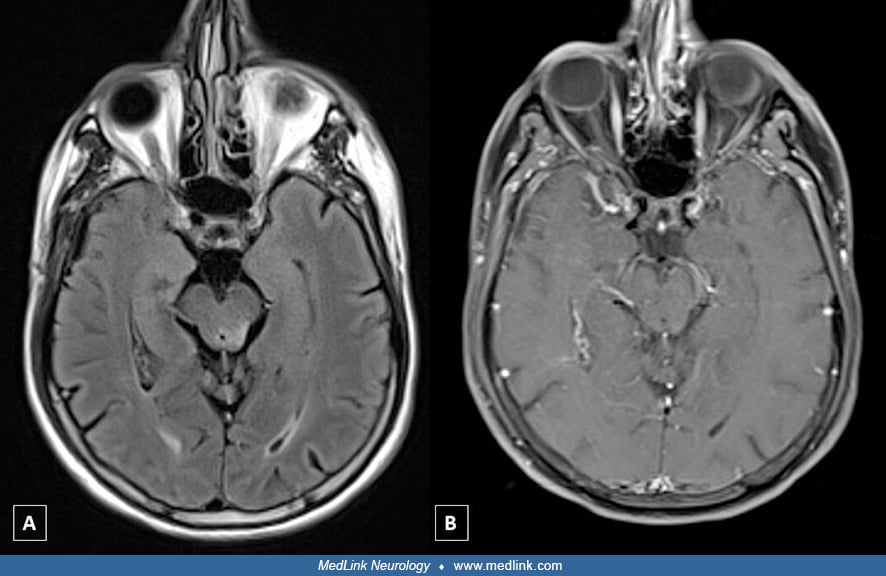
(A) T2 FLAIR hyperintense lesion in the right caudate nucleus with (B) associated punctate enhancement on contrast T1-weighted image. (C and D) images demonstrate similar FLAIR lesions with associated enhancement in the midbrai...
Routine CSF analysis includes measurements of protein and glucose, red blood cell count, and white blood cell count with differential. In an adult patient, the recommended amount to be collected is around 20 mL divided over 4 tubes with the last tube saved for storage. The pattern of abnormalities may give clues regarding the etiology of CNS inflammation or infection. These results need to be interpreted with caution in immunocompromised patients who may be unable to mount an inflammatory response. Classically, the combination of low CSF glucose (hypoglycorrhachia), high protein, and neutrophilic pleocytosis of several thousand white blood cells points toward bacterial meningitis until proven otherwise, whereas a lymphocyte-predominant pleocytosis is a hallmark of viral meningoencephalitis or an atypical infection (fungal, mycobacterial). These patterns are not reliable, though, as some viruses can have an early neutrophilic response (eg, West Nile virus and cytomegalovirus). Eosinophilic pleocytosis is rare but can be a sign of a helminthic or Coccidioides infection (20). In infections due to certain atypical bacteria, such as Treponema pallidum, lymphocytic pleocytosis can last up to 2 years with treatment and up to decades without (40).
High CSF protein, although sensitive for inflammation in the CNS, is nonspecific and can be falsely elevated by the presence of red blood cells in a traumatic puncture. Spontaneous formation of a fine fibrin clot after CSF removal may occur in highly proteinaceous CSF with presence of fibrinogen and should raise concern for tuberculous meningitis (see Tuberculosis of the CNS). Low CSF glucose (hypoglycorrhachia) can occur with bacterial or fungal meningitis, malignancy, neurosarcoidosis, neurosyphilis, cerebral toxoplasmosis, and stroke or hemorrhage, among other causes, even rarely with some viral infections like mumps and lymphocytic choriomeningitis virus (05; 20). Glucose tends to be lowest (at times undetectable) with bacterial meningitis and neoplasm. In general, CSF glucose needs to be adjusted for simultaneous serum glucose for accurate interpretation.
Opening pressure is an important investigation when CNS infection is suspected, although it is nonspecific. High pressure is especially common in bacterial and cryptococcal meningitis (15), neurocysticercosis (48), and primary amebic meningoencephalitis (08).
Timing of CSF evaluation in relation to symptom onset and antimicrobial initiation may impact CSF values. Early encephalitis may be associated with normal CSF, but repeat testing often shows abnormal findings more typical of encephalitis, such as pleocytosis and elevated protein. Antibiotics may affect the CSF profile in bacterial meningitis. In a study of 245 children with bacterial meningitis, 85 patients who were pretreated with antibiotics showed higher CSF glucose levels and lower CSF protein levels; these changes happened as early as 4 hours posttreatment but became more prominent after 12 hours. White blood cell count and absolute neutrophil count were found to be unaffected when the lumbar puncture was done fewer than 12 hours after administration of antibiotics (32).
Routine microbial studies of CSF include Gram stain and cultures, both of which should be performed on every patient in whom CNS infection is suspected whether or not they show pleocytosis. Gram stain has a sensitivity of 60% to 90%, but this is dependent on the burden of bacteria present in the CSF. Sensitivity is highest in untreated S. pneumoniae meningitis, whereas L. monocytogenes has one of the lowest sensitivities at around 25%. The specificity of Gram stain, on the other hand, is as high as 97% (20; 31). The specificity of bacterial cultures is near 100%, but results can take a long time to finalize, which is not ideal in situations where rapid identification of the causative bacteria is key and may lead to longer hospitalization and lengthier time on empiric antibiotics. An advantage for conventional cultures over molecular diagnostic techniques is the ability to perform a sensitivity analysis, which helps in accurately narrowing the antibiotic spectrum.
Pretreatment with antibiotics causes a drop of sensitivity by 50% for CSF Gram stain and sterilization of CSF cultures as fast as 2 hours after treatment for N. meningitidis and up to 8 hours for S. pneumoniae. Therefore, it is essential to acquire peripheral blood cultures before initiating empiric treatment, even if CSF studies are delayed (20). It should be noted that blood cultures’ rate of positivity is different based on the causative bacteria, ranging from 40% in children with meningococcal meningitis and up to 90% in some patients with H. influenzae meningitis; however, the yield is decreased by 20% in those pretreated with antibiotics (03).
Other stains include India ink for cryptococcal infection, especially in resource-limited settings; these stains are positive in 50% to 70% of patients with cryptococcal meningitis, and the yield is up to 90% in patients with AIDS (31). CSF culture is positive in 90% of patients with cryptococcal meningitis after 48 to 72 hours of incubation (15).
The most common neuroinvasive fungi, including Cryptococcus, Candida, and Aspergillus, can be cultured on standard bacterial media with variable sensitivity, but specific culture media should be used when rarer fungi are considered (38).
As far as staining and cultures for viral pathogens, enteroviruses are the easiest to culture, but sensitivity is only 75% at best, and the turnaround may be up to a week, so CSF viral culture has largely fallen out of practice, especially following the introduction of molecular diagnostics (31).
In tuberculous meningitis, CSF acid-fast bacilli culture and Ziehl-Neelsen staining are the traditional and most widely available testing methods. The culture specifically is limited by a lengthy growth period of up to multiple weeks and a low rate of positive samples (5% to 58% of patients); although larger CSF volumes improve the culture sensitivity, it is still an unreliable test for timely and critical intervention (42).
Giemsa stain and a CSF wet mount are both useful for protozoal infections, such as demonstration of motile trophozoites of Naegleria fowleri (Cope and Ali 2021). Parasitic infection (protozoal or helminthic) sometimes can also be diagnosed by direct visualization of the adult parasite, larvae, or eggs in either CSF or other affected tissues or in body secretions, including stool, urine, and sputum (48).
Brain biopsy is a last-resort method reserved for the most challenging cases. It can be considered when there is a question about the etiology (infectious, autoimmune, neoplastic) and when other methods have failed to detect the causative pathogen, especially when the microorganism is sequestered in a confined area in the CNS, such as an abscess.
Antigen detection involves the identification of microbial proteins and glycoproteins by immunologic methods, such as latex particle agglutination, coagglutination, and enzyme-linked immunosorbent assay (ELISA) (38). Detection of bacterial antigens in the CSF was used in the past for rapid diagnosis of bacterial meningitis, especially when delays in lumbar puncture led to sterile CSF, but it fell out of common practice due to low sensitivity and the widespread availability of multiplex PCR assays. Detection of antigens in the CSF (eg, lipoarabinomannan, early secreted antigen target or ESAT, Ag 85 complex, and the 65-kDa antigens) has shown more promise in some atypical bacteria like mycobacterium tuberculosis, with potential correlation between the concentration and clinical severity (31).
The cryptococcal antigen (CrAg) assay directed at the polysaccharide capsule remains a key test for cryptococcal meningitis. It can detect both Cryptococcus neoformans in the immunocompromised and its counterpart Cryptococcus gattii in the immunocompetent host (20). Both serum and CSF CrAg are highly specific and sensitive (93% to 98% and 93% to 100%, respectively) (27), and the introduction of the lateral flow assay has allowed rapid diagnosis from serum, plasma, and CSF (38). The most recent World Health Organization guidelines for diagnosing cryptococcal meningitis recommend testing of CSF CrAg, and if CSF is not immediately accessible or lumbar puncture is contraindicated, rapid serum, plasma, or whole-blood antigen assays are acceptable alternatives. Screening with serum CrAg is also recommended for people living with HIV who have CD4 count lower than 100 (54). It is worth mentioning that although the initial CSF titer can be prognostic, it should not be used as a marker of treatment response (38).
Other commonly used fungal antigen tests include serum and urine histoplasma antigen to assess for disseminated disease and CSF coccidioidal antigen, which is highly sensitive and specific though not widely available (47). Galactomannan, a cell wall polysaccharide present in the Aspergillus species, can be detected in invasive infections in either serum (sensitivity of 60% to 80% and specificity of 80% to 95%) or CSF (sensitivity of 85% to 90% and specificity of 95% to 100%) (22). Another cell wall component common to many fungal species, 1,3 beta-D-glucan (BDG) antigen testing in the serum or CSF, can be used as a sensitive marker for invasive fungal infection, such as candidiasis and aspergillosis. Effective antifungal therapy causes reduction in CSF BDG titers, which makes it a useful biomarker to monitor treatment response (38; 31).
Antigen assays can be used to rapidly diagnose parasitic infections with variable sensitivity and specificity (eg, the bedside rapid antigen detection of Plasmodium falciparum histidine rich protein 2 and lactate dehydrogenase) (45). CSF cysticercal antigen assays can be helpful to detect live parasites and to monitor therapy response in subarachnoid and other extraparenchymal forms of neurocysticercosis, although this is not available commercially in the United States (12).
Serological testing relies on detecting antibodies against pathogenic antigens and can be helpful in the diagnosis of CNS pathogens that are present at low titers, for brief amounts of time, or for when the manifestations of the infection are largely due to the host immune response. Some infections, including arboviruses and certain spirochetes and rickettsia, can only be diagnosed by serological methods. However, serology has drawbacks in terms of variable “window” periods until seroconversion happens and a positive result is detected, which can lead to either a false-negative result or delayed diagnosis. Additionally, immunocompromised hosts, such as people living with HIV or those treated with a B-cell-depleting agent, may have false-negative serologies due to their inability to mount an appropriate immune response against the pathogens. In these situations, PCR assays may sometimes be used in place of serology. False-positive CSF serology results can be seen when there is blood contamination in traumatic lumbar punctures as well as in certain cases of cross-reactivity, such as the finding of positive Zika virus serology in those given vaccines against the Japanese encephalitis virus or Yellow fever virus, both in the Flaviviridae family (20; 31). Finally, because some IgG responses are long-lasting, serological results can sometimes represent true positive prior exposure but not indicate the cause of the current syndrome. Another serum assay is IgG avidity, in which low avidities point to a more recent infection. For all serological assays, testing is typically done in 2 steps: (1) screening, such as with an enzyme immunoassay or immunofluorescence assay, and then (2) confirmatory testing with a technique like plaque reduction neutralization test (PRNT). Most tertiary labs have these tests paired where a positive screening would reflex into confirmatory testing (20).
Identification of IgM antibodies in the CSF is particularly helpful. As IgM is a large molecule and has poor ability to cross the blood-CSF barrier, its presence in CSF generally confirms intrathecal production. On the other hand, IgG readily crosses the blood-CSF barrier, so the ratio of specific IgG in CSF and serum is then normalized to the CSF:serum ratio of albumin (IgG index).
Certain infections are diagnosed based on clinical and epidemiological factors in the presence of compatible serology. For example, many arboviruses cause a brief viremia early in illness but are not detectable by standard PCR assays at the time of neurologic symptoms. West Nile virus IgM detection in the CSF in the absence of IgM specific to other endemic viruses is diagnostic of West Nile virus neuroinvasive infection. Both serum and CSF West Nile virus IgM can turn positive as soon as 3 days after systemic symptom onset and persist for 3 months or longer, making serum and CSF IgM the preferred diagnostic test. If IgM is negative, but there is high clinical suspicion, a second sample should be obtained after day 5 and before day 15 of symptom onset. The presence of seroconversion in blood confirms infection, especially when there is a 4-fold or greater increase in virus-specific antibody titers in the paired acute and convalescent sera, but this generally takes several weeks and provides a retrospective diagnosis (35).
Most varicella-zoster virus-related neurologic disease in adults is due to reactivation of latent infection. Varicella-zoster virus PCR of CSF is useful if positive but has poor sensitivity at 60% in meningoencephalitis and as low as 30% in vasculopathy. In these cases, CSF varicella-zoster virus IgG can be helpful, especially when the CSF:serum ratio of immunoglobulins is elevated, indicating intrathecal production. A drawback is that the assay usually takes 1 to 2 weeks to result (44; 20).
Serum antibody index for JC virus helps stratify the risk of developing progressive multifocal leukoencephalopathy in patients with multiple sclerosis who are treated with natalizumab (36). Because there is a high seroprevalence in the general population, however, the actual diagnosis of progressive multifocal leukoencephalopathy requires CSF PCR, which has a specificity of 100% but variable sensitivity from 58% to 92%. Sensitivity is particularly low in people living with HIV who are on antiretroviral therapy; brain biopsy may rarely be needed when suspicion is high, but PCR is negative (20).
Neurologic involvement of syphilis can occur at any stage of infection. Diagnosis of neurosyphilis begins with confirmation of syphilis in serum by treponemal antibody reactivity. Serum nontreponemal tests, such as the venereal disease research laboratory (VDRL) or rapid plasma reagin (RPR) tests, are almost universally reactive in neurosyphilis during and after the second stage of syphilis and are useful for monitoring treatment response but can revert to nonreactive in late neurosyphilis due to decrement in titers over time. For patients with reactive serum treponemal antibody, CSF VDRL is highly specific for neurologic involvement but has low sensitivity (30% to 70%), so a negative result does not rule out neurosyphilis. If suspicion is high, CSF treponemal testing with fluorescent treponemal-antibody absorption (FTA-ABS) has high sensitivity but can give false-positive results when CSF is contaminated by blood. Nonreactive treponemal testing in the CSF rules out asymptomatic neurosyphilis and makes symptomatic infection unlikely, especially when the syndrome does not fit with the neurosyphilis spectrum (40).
In Lyme disease, the causative agent, Borrelia burgdorferi, is transmitted by the bite of the Ixodes tick. Neurologic involvement (neuroborreliosis) happens in 10% to 15% of patients and, by definition, involves disseminated infection. Neuroborreliosis most commonly manifests as lymphocytic meningitis, cranial neuritis, or painful radiculoneuritis. Per guidelines from the Infectious Diseases Society of America (IDSA) and the American Academy of Neurology (AAN), the diagnostic algorithm starts with serum antibody assay testing as almost all patients with neuroborreliosis have reactive serum serology; if negative, alternative etiologies should be considered. Antibody reactivity is usually tested via a first-tier test (enzyme immunoassay or immunofluorescence assay) and then confirmed with second-tier testing with Western blot. Serum serology is superior to PCR and culture of serum or CSF. Testing may be negative early in infection at the time of erythema migrans and, rarely, in early-onset neurologic symptoms, so if clinical suspicion is high, this can be repeated. In a patient with positive serum antibody, the preferred method to detect intrathecal production of antibodies to B. burgdorferi is the antibody index, which measures the ratio of simultaneously collected CSF and serum antibody concentration. Frequent Lyme serology testing in patients without one of the neurologic syndromes typical for Lyme disease may lead to false-positive results, especially if the IgM is positive with a negative IgG. Furthermore, up to 20% of the population in certain endemic areas can be positive for Borrelia-specific antibodies due to an infection that happened months or years prior, leading to true positives that would be irrelevant to the current symptoms. (19; 23).
For certain fungal CNS infections, such as those caused by dimorphic fungi like Histoplasma capsulatum, CSF serologies are key in making the diagnosis as culture and antigen testing are not adequately sensitive. The yield can be low in immunocompromised patients, however, and fungal culture is the preferred method in these patients (39). In coccidioidal meningitis, CSF antibody assays have a sensitivity of 70% and a specificity near 100% (47).
Most parasitic infections manifest clinically after the humoral immune response has led to IgG production. Serum antibody testing can establish infection in most cases and in some circumstances is even more sensitive than the CSF. For example, in neurocysticercosis the test of choice for antibody detection is serum enzyme-linked immunoelectrotransfer blot (EITB), which has a sensitivity up to 98% in the presence of 2 or more viable CNS parasites. An exception is toxocariasis (visceral larva migrans), where detection of CSF antibodies, especially IgG, is more sensitive than serum for CNS disease (55).
Toxoplasmosis is one of the most common protozoal infections, causing clinical neurologic disease mainly in immunocompromised hosts such as people living with HIV. Although CSF PCR can confirm diagnosis, sensitivity is low and lumbar puncture is sometimes contraindicated in these patients due to mass effect. Serum toxoplasma IgG will almost always be positive (rarely, profoundly immunocompromised patients may lose seropositivity) and in the context of appropriate clinical and radiographic presentation can confirm a high probability of toxoplasma encephalitis. To avoid the potential morbidity of brain biopsy, empiric treatment with an appropriate clinical and radiographic response can be used to confirm the diagnosis. If serum toxoplasma IgG is negative or the clinical course continues to worsen despite appropriate empiric treatment, further diagnoses should be considered, and biopsy may be necessary to differentiate toxoplasmosis from other space-occupying lesions in AIDS, such as primary CNS lymphoma or tuberculoma (20).
In the parasitic infection schistosomiasis, positive serology results should be interpreted carefully in endemic areas with high prevalence, as sometimes the disease can be asymptomatic, and these antibodies persist for years. Other methods should be employed to confirm the diagnosis, such as egg identification in the stool or urine or a punch biopsy from the rectal mucosa (55; 04).
Molecular diagnostic techniques are now among the most valuable tools and have revolutionized the way we detect CSF infections. Most have excellent sensitivity and specificity, can identify infections with low organism burden and those organisms that cannot be cultured, can obviate the need for serological testing in immunocompromised hosts who are unable to mount a measurable immune response--all with a short turnaround allowing for prompt intervention and management. These assays typically rely on nucleic acid. One of the earliest monoplex assays was successfully used for the detection of Herpes simplex virus in the CSF in the 1990s and paved the way for more pathogen-specific assays that would limit the need for invasive procedures such as brain biopsy (41). Traditional PCR assays are usually qualitative, providing a binary result (positive or negative), whereas quantitative methods can provide concentrations or “copy numbers” (17).
As mentioned above, HSV1-2 PCR in the CSF is now the gold standard in diagnosing Herpes simplex virus encephalitis with a sensitivity of 98% and specificity of 94% but can be falsely negative if the sample is taken too early in the course of the disease (21). In cases of high clinical suspicion, CSF testing should be repeated 3 to 7 days following the initial tap. Herpes simplex virus PCR in CSF usually remains positive up to 7 days after initiating treatment with acyclovir.
CSF PCR for Mycobacterium tuberculosis has a sensitivity of 50% and a specificity close to 100%. These numbers are highly dependent on the diagnostic criteria used, the amount of CSF sampled, and whether antituberculous therapy was administered before collection of CSF. These assays are also limited to some reference laboratories, require high expertise, and are expensive (57). More recently, the Xpert MTB/RIF assay, and the Xpert Ultra assay, have been used as a nucleic acid amplification test on CSF with results available in less than 2 hours. In a study of 235 patients in South Africa with suspected meningitis, the Xpert MTB/RIF assay is likely a good “rule-in” test for tuberculosis meningitis with a sensitivity up to 80% when centrifugation is used; performance was even higher in people living with HIV (34). This was corroborated in a meta-analysis of 13 studies where the pooled sensitivity was up to 80.5% (09). Of note, a prospective, randomized, diagnostic accuracy study aimed to compare Xpert Ultra vs Xpert in 205 adults with suspected tuberculous meningitis from a single center in Vietnam. The subjects were randomly assigned, and the results showed that Xpert Ultra was not statistically superior to Xpert for the diagnosis of tuberculous meningitis in HIV-uninfected and HIV-infected adults (10).
Special consideration should be given to CSF analysis in prion diseases as it requires special handling for the specimen and equipment. Basic CSF studies are usually normal with occasional mildly elevated protein (less than 100 mg/dL) (13). The most specific CSF diagnostic marker is real-time quaking-induced conversion (RT-QuIC), which has higher specificity and sensitivity than total Tau and 14-3-3 protein. The RT-QuIC method monitors the formation of PrPSc aggregates in real time. Its interpretation can be influenced by the presence of blood contamination in the CSF or the presence of more than 10 white blood cells in CSF. Application of the RT-QuIC assay to olfactory mucosa and skin biopsy may have better sensitivity than CSF (18). In the United States, the National Prion Disease Pathology Surveillance Center offers a “CJD panel” that includes RT-QuIC in addition to t-Tau and 14-3-3 protein.
Multiplex PCR assays can identify several causes of meningitis and encephalitis simultaneously in one CSF sample. An example of this technology is the FilmArray BioFire meningitis/encephalitis panel, approved by the United States Food and Drug Administration in 2015. Reportable within 1 hour, it assesses 14 common CNS pathogens. The sample required is only 200 µl of CSF. The organisms assayed include:
• 6 bacteria: Escherichia coli K1, Haemophilus influenzae, Listeria monocytogenes, Neisseria meningitidis (encapsulated), Streptococcus agalactiae, Streptococcus pneumoniae. | |
• 7 viruses: Cytomegalovirus, enterovirus, herpes simplex virus 1, herpes simplex virus 2, human herpesvirus 6, human parechovirus, varicella-zoster virus. | |
• 1 yeast: Cryptococcus neoformans or gattii. |
This method has some limitations: it lacks testing for organisms that affect the neurosurgical and immunocompromised populations as well as regional infections, such as arboviruses. False positives and negatives can also occur, such as with Cryptococcus; this may require other ancillary workups to confirm the diagnosis, such as CrAg (25; 33).
It is worth mentioning that human herpesvirus 6 (HHV-6), which is ubiquitous and usually causes asymptomatic infection, has been a frequently encountered positive target on the panel. In a study of 793 patients (including adults and children), 60 were positive for 1 or more target, 15 of which were HHV-6. Only one individual likely had HHV-6 encephalitis--a woman with signs of limbic encephalitis 3 weeks following hematopoietic stem cell transplant, which is the classical association for HHV-6. Hence, caution is advised when interpreting positive HHV-6 PCR on the meningitis/encephalitis panel (16).
Despite introduction of PCR monoplex and multiplex assays into the diagnostic workup of meningitis and encephalitis, in as many as 50% of individuals a causative pathogen is not identified. Primer-independent next-generation sequencing is a technique that extracts total DNA and RNA CSF or tissue, and both host and nonhost nucleic acid is amplified and sequenced. Human and environmental contaminant sequences are excluded through a combination of appropriate controls and post-processing computational methods. Subsequently, all remaining sequences are matched against publicly available databases to identify the infectious pathogens (except for prions). This has allowed testing for rare and even novel pathogens. In one study, a causative pathogen was identified in 22% (13 of 57 patients) of previously undiagnosed cases by conventional methods; 8 of these results had an impact on the clinical course (Precision Diagnosis of Acute Infectious Diseases [PDAID] study) (56).
Commercial NGS is limited to only a few reference labs in the United States. Other limitations include high expense and delay in reporting of more than a week in most cases. Moreover, a pathogen’s sequence may not exist in available databases. Currently, this new technology is still best when paired with the standard conventional methods to maximize the diagnostic yield (38; 56). Next-generation sequencing is particularly useful in suspected recurrent or chronic infections, especially in immunocompromised hosts susceptible to less common or more fastidious pathogens.
Evidence has been limited to case reports and case series. SARS-CoV-2 RNA is rarely detected in CSF, and the test itself is not commercially available (37). The pathophysiology remains unclear. In a post-mortem study of 43 patients who died from Covid-19 infection, inflammation was observed in the brainstem with microglia activation and cytotoxic T cell infiltration (28). However, SARS-CoV-2 RNA was detected by RT-PCR in only 21 individuals, which raised the possibility of parainfectious, rather than infectious etiologies, similar to acute necrotizing encephalopathy seen in children with influenza (52).
CNS listeriosis has a predilection toward affecting pregnant woman and other vulnerable populations, such as elderly, neonatal, diabetic, and immunocompromised hosts. This gram-positive intracellular rod is commonly found in the soil but can also be foodborne. It can cause abscesses and cerebritis and is the primary bacterial cause of rhombencephalitis.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Lama Abdel Wahed MD
Dr. Abdel Wahed of University of Iowa Hospitals and Clinics has no relevant financial relationships to disclose.
See Profile
Tracey A Cho MD
Dr. Cho of University of Iowa Carver College of Medicine has no relevant financial relationships to disclose.
See Profile
Christina M Marra MD
Dr. Marra of the University of Washington School of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Infectious Disorders
Dec. 27, 2024
Infectious Disorders
Dec. 12, 2024
Infectious Disorders
Dec. 10, 2024
Infectious Disorders
Dec. 10, 2024
Peripheral Neuropathies
Nov. 16, 2024
Infectious Disorders
Nov. 15, 2024
Infectious Disorders
Nov. 12, 2024
Infectious Disorders
Nov. 12, 2024