















General Neurology
Use of focused ultrasound in neurologic disorders
Jan. 13, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author explains the clinical presentation, pathophysiology, diagnostic work-up, and management of disequilibrium. Vestibular vertigo is a common problem, particularly in the elderly. Careful history and detailed examination, including focused evaluation of proprioception, vestibular function, directional bias of postural sway, ability to maintain stance with eyes open and closed (Romberg test), ability to maintain stance despite perturbations (eg, pull test), and gait will allow distinction of the major categories of disequilibrium in most cases and will often allow a specific etiologic diagnosis as well.
|
• Postural control is not simply a collection of righting and equilibrium reflexes but is instead a complex motor skill derived from the interaction of multiple sensorimotor processes. | |
|
• Postural control can be divided into two component abilities or subgoals: postural orientation and postural equilibrium (ie, balance). | |
|
• Disequilibrium is a state of nonvertiginous altered static (eg, standing) or dynamic (eg, walking) postural balance. | |
|
• Patients with disequilibrium often complain of unsteadiness, imbalance, and falls. | |
|
• Except in cases of visual-vestibular mismatch, patients with sensory disequilibrium generally do worse in the dark and frequently have a Romberg sign on examination, whereas motor disequilibrium caused by impaired motor performance is generally not exacerbated in the dark or by closing the eyes. |
Postural control is not simply a collection of righting and equilibrium reflexes but is instead a complex motor skill derived from the interaction of multiple sensorimotor processes (292; 166; 324; 174). Postural control can be divided into two component abilities or subgoals: postural orientation and postural equilibrium (ie, balance). Maintaining postural orientation requires active control of body alignment and tone with respect to the visual environment, gravity (ie, components of the vestibular system), the support surface (ie, mediated by cutaneous mechanoreceptors), and internal cues that provide awareness of the position and movement of the body (ie, proprioception); thus, spatial orientation requires the interpretation of convergent sensory information from the visual, vestibular, and somatosensory systems. Postural equilibrium requires the coordination of multiple sensorimotor strategies to stabilize the body’s center of mass over the base of support (ie, the area beneath an object or person that includes every point of contact that the object or person makes with the supporting surface), during both self-initiated and externally triggered disturbances in postural stability (273; 166).
Disequilibrium is a state of nonvertiginous altered static (eg, standing) or dynamic (eg, walking) postural balance (189; 207). This framework for disequilibrium derives in part from an influential paper by Drachman in 1972 that employed a 4-fold categorization of dizziness: vertigo, disequilibrium (with sensory and motor subcategories), presyncope, and psychophysiological (psychogenic) dizziness (113); disequilibrium was further divided into sensory and motor subtypes to reflect the predominant clinical dysfunction responsible. However, an alternative approach might have been to consider vertiginous disequilibrium as an additional subcategory of disequilibrium.
The clinical literature contains many articles that use “disequilibrium” (or “dysequilibrium”) as a synonym or umbrella term for dizziness, often encompassing vertigo, orthostatic hypotension, and psychogenic conditions as well as motor and sensory disequilibrium. However, in this article, disequilibrium is to be understood as distinct from these other disorders, recognizing of course that patients can be imprecise in describing the sensations of dizziness that they experience. Although the imprecision of a patient’s report can complicate clinical assessment, it doesn’t change the task of sorting out the underlying process that is responsible for the patient’s complaints. Therefore, these terms should be used to indicate the underlying pathophysiology and not some label that the patient gives to his or her complaints.
Disequilibrium has been labeled as “unsteadiness” in the International Classification of Vestibular Disorders I (ICVD-I), the first consensus document of the Committee for the Classification of Vestibular Disorders of the Bárány Society (39).
Romberg sign. In the first half of the 19th century, European physicians described loss of postural control in darkness in patients with severely compromised proprioception, a phenomenon that became known as the “Romberg sign” (217). Early in its history, the sign was linked to tabes dorsalis (locomotor ataxia), later known to be a tertiary stage of syphilis. By the end of the 19th century, the Romberg sign had developed from a patient-reported symptom of a specific disease (ie, tabes dorsalis) into a bedside-elicited sign of deafferentation (217; 205; 206; 205).
In his Lectures on the Nervous System and its Diseases (1836), English physician Marshall Hall (1790 to 1857) described the loss of postural control in darkness among patients with severely compromised proprioception (154; 217):
|
I have this day seen a patient with a slight degree of paralysis of feeling and of voluntary motion of the lower limbs. He walks safely while his eyes are fixed upon the ground, but stumbles immediately if he attempts to walk in the dark. His own words are “my feet are numb; I cannot tell in the dark where they are, and I cannot poise myself.” The voluntary motions are regulated by the sense of touch, when this is unimpaired; or by that of sight, when touch is paralyzed (154). |
Hall recognized that: (1) proprioception and vision were important for postural control; (2) vision could at least partially compensate for defective proprioception; and (3) in the absence of vision (eg, in darkness) proprioceptive deficits can produce overt impairment of postural control.
Several years after Hall’s initial description, in the second edition of Lehrbook der Nervenkrankheiten des Menschen in 1851, and in a subsequent English translation in 1853, German neurologist Moritz Romberg (1795 to 1873) described the loss of postural control in patients with tabes dorsalis on closing their eyes or in darkness (300; 301). Romberg devised a bedside clinical test to demonstrate the phenomenon, although Romberg’s approach was simply to observe a change in postural control when patients were asked to close their eyes (without any stated preferred position of the feet).
|
If the patient [with tabes dorsalis] is told to shut his eyes while in the erect posture, he immediately begins to move from side to side, and the oscillations soon attain such a pitch that unless supported, he falls to the ground . . . The eyes of such patients are their regulators, or feelers; consequently in the dark, and when amaurosis supervenes, as is not unfrequently [sic] the case, their helplessness is extreme . . . The feet feel numbed [sic] in standing, walking, or lying down, and the patient has the sensation as if they were covered with a fur . . . The gait begins to be insecure, and the patient attempts to improve it by making a greater effort of the will; as he does not feel the tread to be firm, he puts down his heels with greater force. From the commencement of the disease, the individual keeps his eyes on his feet to prevent his movements from becoming still more unsteady. If he is ordered to close his eyes while in the erect posture, he at once commences to totter and swing from side to side; the insecurity of his gait also exhibits itself more in the dark. It is now ten years since I pointed out this pathognomonic sign [ie, c. 1840] (301). |
German physician Bernardus Brach (1799-?) described similar symptoms around the time that Romberg claimed to have recognized them, and he published them more than a decade before Romberg:
|
It is known that people with tabes dorsalis have an unusual gait . . . While other paralytics drag their legs, a patient with tabes dorsalis lifts his leg with a straight knee and with difficulties. When he steps with his feet hard and taps on the floor, his whole body is stiff and strained. With fearful eyes he watches his every step. He is dependent upon his cane for support . . . He doesn’t feel the movement he makes with his legs . . . Because of this, he raises his legs slowly to maintain balance . . . He has no sensation [proprioception] in his lower limbs, so he relies upon his other senses. When walking, he is very fearful of falling and uses his body and arms for counter-balance. He finds it nearly impossible to walk on a level walkway in conversation with others, or in the dark. With two patients I observed these symptoms. With tests such as cold and warm, pressure, pinching, scratching with a needle tip, or a hair, the patients responded just like a healthy person. Thus, one cannot say that they don’t have any sensation (52). |
Despite their inability to stand or walk in the dark, Brach noted that such patients were not weak; indeed, in the fall of 1838, a 36-year-old educated man made a 5-hour journey on foot to visit Brach and reported his symptoms in a letter to him (52):
|
I must watch carefully every step and stone. I must use my eyes to guide me. In the dark I have no sense of balance, and even though familiar with the area, I will certainly fall. When walking, I must fully concentrate on the task of walking and not on conversation with people . . . I step so hard on my feet that my soles are sore and inflamed after a short distance. My self-confidence is low when walking up steps, over crooked paths, strange places, or with many people (52). |
In A Manual of Diseases of the Nervous System (1888), British neurologist William Gowers (1845 to 1915) presented a clear account of how to optimally perform the Romberg test, adding instructions that the patient should assume a narrow base as part of the test (143):
|
The characteristic incoordination of movement [in tabes dorsalis] develops gradually. It is always increased (as Romberg first pointed out) by closure of the eyes and at first may only exist when the guiding influence of vision is, thus, withdrawn. Before it causes ataxy of movement, it may render difficult the maintenance of equilibrium when the base of support is narrowed by the feet being placed close together, toes and heels. If then the eyes are closed, the patient sways, and may even tend to fall. In health slight unsteadiness is thus produced, varying in degree in different persons, but never amounting to even a suggestion of a fall . . . The early defect in coordination may be discovered by the patient when he walks in the dark, or, not uncommonly, when he shuts his eyes in the process of washing the face. In a further degree of incoordination there is inability to stand with the feet together even when the eyes are open, and the patient is only steady when the feet are wide apart. If the feet are bare, the difficulty is greater, because muscular action has to replace the rigid base of the boot (143). |
Although some felt or implied that the Romberg phenomenon was a specific sign of tabes dorsalis, others soon recognized that it was a more general sign of deafferentation. Later authors recognized that the sign was not specific even to deafferentation, noting that it may be present in some patients with vestibular or even cerebellar lesions.
Station and postural sway. As noted in 1886 by Philadelphia neurologist Silas Weir Mitchell (1829 to 1914) and his trainee Morris Lewis (1852 to 1928):
|
[Station is] the relative power to stand steady, with eyes open or shut. This symptom can be made numerically accurate by standing the patient in front of a bar marked in inches and placed on a level with the ears. The extent of lateral sway of the head may thus be easily observed; a like observation records the anterior tendency. The first is rarely over half an inch in health; the second does not usually exceed an inch, even with closed eyes. Any large increase is suspicious (248). |
Mitchell developed a simple sway meter to measure postural sway as part of the clinical examination (247).
Mitchell’s sway meter consisted of two rulers, graduated in inches, placed perpendicular to each other on a stand. Applying the sway meter in patients with tabes dorsalis, Mitchell and Lewis found that impairment of station progressively worsened over the course of the disease and was associated with both progressive loss of muscle stretch reflexes and loss of the ability to augment these with reinforcement (248). Muscle stretch reflexes were lost early in the legs, even with reinforcement, while station (with eyes open) remained normal; by the time station became severely impaired, muscle stretch reflexes were also lost in the arms.
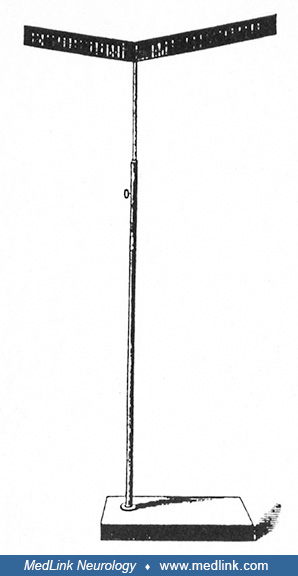
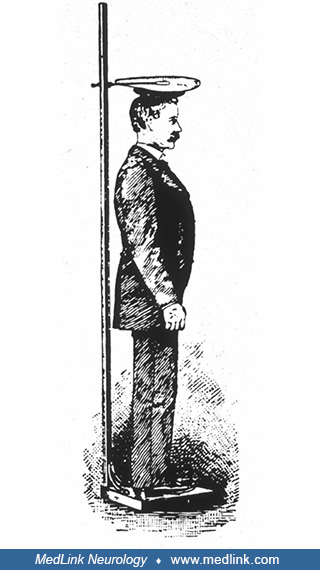
Philadelphia neurologist Guy Hinsdale (1858 to 1948), who served as an assistant to both Mitchell (in the mid-1880s) and William Osler (c. 1888 to 1889), published two studies of postural sway in the late 19th century using Mitchell’s sway meter and more refined graphical methods (162; 163). One graphical method employed a simple recording apparatus in practical use in Mitchell’s clinic contemporaneously with the sway meter:
|
Tracings were taken by attaching to the top of a man’s head a flat piece of cardboard, upon which was stretched some smoked paper. The subject was then placed under an index, free to move up and down, in a fixed line, and which traced curves on the paper as the subject who stood beneath swayed in any direction (162). |
Hinsdale measured postural sway using his apparatus in several groups of people, including normal adults and children, inmates of the Institution for the Blind, and individuals with various neurologic disorders (including tabes dorsalis). In normal individuals, Hinsdale observed postural sway that increased with the eyes closed. In experiments on themselves, Hinsdale and fellow Philadelphia physician William C. Lott found that the postural sway of normal individuals was exaggerated with ether. Blind individuals tended to sway about as much as healthy individuals with their eyes closed, whereas the sway of persons with tabes dorsalis was decidedly greater.
Other American neurologists developed similar devices, including an instrument developed by New York neurologist Charles Loomis Dana (1852 to 1935) around the turn of the century--the “ataxiagraph” (98).
Such nineteenth-century efforts to record and quantitate postural sway under various circumstances and in various pathologic conditions anticipated later physiologic studies as well as the introduction of computerized dynamic platform posturography in the 1970s and 1980s and, later, the less sophisticated but more easily applied technique of foam posturography.
The “dynamic Romberg sign.” In the late 1870s and 1880s, prior to the development of movie cameras or projectors, English-American photographer Eadweard Muybridge (1830-1904) photographed sequential images of people and animals in motion, using arrays of sequentially triggered single-image cameras (257; 210; 212; 216).
In 1885, Philadelphia neurologist Francis Dercum (1856-1931) collaborated with Muybridge at the University of Pennsylvania to photograph sequential images of patients with various neurologic disorders involving abnormal movements and, particularly, various gait disorders, including the sensory ataxic gait of tabes dorsalis (257; 106; 107; 217; 210; 216).
The Dercum-Muybridge collaboration produced the first motion-picture sequences of neurologic gait disorders ever filmed. In particular, Muybridge’s Plate 550 is remarkably informative in demonstrating the clinical features of the sensory ataxic gait, with fairly normal gait while walking with eyes open but with marked decompensation and evident ataxia while trying to walk with eyes closed, a phenomenon I have previously labeled the “dynamic Romberg sign” (217).
Internist William Osler (1849-1919), who had been appointed Chair of Clinical Medicine at the University of Pennsylvania in Philadelphia in 1884, was present there during the Dercum-Muybridge collaboration in 1885. One of Osler’s later aphorisms succinctly expressed the dynamic Romberg phenomenon in such patients: “The normal man walks by faith, the tabetic by sight” (274; 211; 216).
Postural instability in Parkinson disease. Postural instability was first described as a feature of Parkinson disease by Romberg in 1853 (301; 170). In the 1880s, French neurologist Jean-Martin Charcot (1825-1893) recognized a tendency to propulsion and retropulsion in patients with Parkinson disease and then began attempts to evaluate postural instability by pulling the clothes of patients (75; 170; 255).
Several clinicians noted postural instability, and some offered simple clinical assessments or tests that can, in retrospect, be seen as precursors of the modern pull test (143; 241; 53; 245; 250; 103; 236). In the 1960s, neurologists Margaret Hoehn (1930-2005) and Melvin Yahr (1917-2004) assessed postural instability in patients with Parkinson disease using a push on the sternum (164). The modern form of the pull test was proposed by neurologist Stanley Fahn in the 1980s; in 1987, the pull test was incorporated into the Unified Parkinson's Disease Rating Scale (UPDRS) (123).
Postural instability in bilateral vestibulopathy. In the late 19th century, several investigators, including American psychologist and philosopher William James (1842-1910), studied the manifestations of absent labyrinthine function in deaf-mute patients.
James found that manifestations included dysequilibrium, ataxia, absence of vertigo during or after rotation, reduced caloric and rotation-induced nystagmus, and resistance to seasickness (176; 214).
In 1941, neurosurgeon Walter Dandy at Johns Hopkins reported disequilibrium (especially in the dark) and oscillopsia in patients with Meniere disease who underwent bilateral vestibular nerve section (99; 208).
|
Division of both vestibular nerves is attended by one rather surprising after effect, jumbling of objects (visual) when the patient is motion. As soon as the patient is at rest, the objects are again perfectly clear. The other disturbance is uncertainty when the patient is walking in the dark. Both of these effects persist, though with gradual lessening in severity (99). |
Although these manifestations of bilateral vestibulopathy were later called “Dandy syndrome,” similar observations following bilateral vestibular nerve section had been reported earlier by neurologist Frank R Ford (1892-1970) and neuro-ophthalmologist Frank B Walsh (1895-1978) in a surgical patient of Dandy’s (130; 208; 213):
|
During convalescence [following bilateral vestibular nerve section], it became evident that a new series of symptoms had developed. Objects seemed to move before his eyes unless his head was kept perfectly still. Walking caused objects to “jump” before his eyes to some extent . . . He was also very unsteady in the dark. (130). |
In 1950, Ford summarized the observations he made with Walsh in the 1930s:
|
Destruction of the vestibular apparatus on both sides in man produces a constant unsteadiness of station and gait, which is exaggerated in the dark and also by sudden movements of the head. There is also a striking inability to fix objects with the eyes when the head is in movement so that the patients complain of objects seeming to dance or oscillate before their eyes when they are walking or riding in a car. This oscillation ceases as soon as the head is held still (129). |
Similar observations in nonsurgical patients were also made by neurologist Paul M Levin (1906-1978) before Dandy's report (226). Levin had also been at Johns Hopkins at the time of Ford and Walsh’s initial report.
With the widespread use of streptomycin in the late 1940s, clinicians began to recognize the full clinical syndrome of acquired bilateral vestibulopathy. Some patients treated with streptomycin for tuberculosis developed disabling disequilibrium, ataxia, and oscillopsia, and the clinical features of these patients resembled those described earlier by Dandy (87; 88; 89; 215). The most important report from that period was a case of “JC,” anonymously reported by a 30-year-old physician in 1952 (87). “JC” was John “Jack” Douglas Crawford II (1920-2005), an identity that Crawford acknowledged in a separate publication the same year as his original report (88).
Postural instability and sensory ataxia in neuronopathies. Postural instability and sensory ataxia were recognized sporadically with multiple disorders that produced neuronopathies. Initially, in the mid-19th century, tabes dorsalis (“locomotor ataxia”) was most closely linked with this type of disequilibrium.
The sensory ataxic gait results from loss of proprioceptive input. Key clinical features of the sensory ataxic gait include: (1) relatively normal gait with eyes open but gait ataxia with eyes closed, (2) Romberg sign, (3) impaired joint-position sense, (4) pseudoathetosis, and (5) sensory drift (as distinct from pronator drift).
The sensory ataxic gait is sometimes called a “stomping gait” because patients learn to compensate for their proprioceptive deficits by using an auditory cue (ie, the sound from forcefully striking the ground). To accomplish this some may, with eyes open, lift their legs higher than normal to strike the ground with sufficient force. Consequently, from continued excessive joint trauma, their joints may be damaged over time, producing what has been variously labeled “Charcot joints” or neuropathic arthropathy.
In the 1980s, multiple investigators reported that pyridoxine overdose causes a pure sensory neuronopathy with sensory ataxia, poor coordination, numbness, and decreased sensation to touch, temperature, and vibration. Sensory neuronopathy from pyridoxine abuse was first recognized by neurologist Herbert H Schaumburg and colleagues at Albert Einstein College of Medicine in 1983 (304). Subsequently, multiple authors described sensory neuronopathy (and less commonly a sensorimotor neuropathy) in patients who consumed high doses of pyridoxine (ie, most consumed greater than 2 g/day) (321; 282; 95; 04; 97; 03; 242; 203; 101; 137; 71; 138; 202; 118). Some of these cases were iatrogenic, resulting from pyridoxine treatment of pyridoxine-dependent epilepsy, homocystinuria, mushroom poisoning, and premenstrual syndrome (04; 97; 03; 242; 118). The pyridoxine dose varied from 200 mg to 10 grams per day for periods of up to 20 years (308). Symptoms began one month to several years after starting pyridoxine. Duration of consumption prior to symptom onset was inversely proportional to dose. In many cases, symptoms partially improved following discontinuation of pyridoxine, but many were still left with severe disability. The relationship between pyridoxine overdose levels and histological damage has now been well characterized in both humans and animals. Pyridoxine given in large doses selectively destroys large-diameter peripheral sensory nerve fibers, leaving motor fibers intact.
Cerebral balance disorders. Over the past century, there have been significant advances in the classification of balance disorders, although significant gaps in our understanding remain. For example, late in the 19th century, Bruns coined the term frontal ataxia to describe cerebral-related (mainly frontal lobe) balance and gait disorders, but his term fell out of favor; the concept of frontal gait apraxia began to be used during the first quarter of the 20th century and continues to be used, with some controversy, into the 21st century. In 1926, Gerstmann and Schilder described two patients with frontal lesions and what they labeled as “gait apraxia”; the patients were unable to lift their feet to walk and could not stand or sit without falling backward (330). Despite the confusing terminology surrounding cerebral balance disorders and despite our limited understanding of their pathophysiology, historical cases show that cerebral balance disorders are caused by mainly subcortical, frontal, and occasionally parietal lesions (337; 133; 104) and that cerebral balance disorders are characterized by varying combinations of parkinsonian, ataxic, spastic, “magnetic” (feet stuck to ground), and “apractic” qualities. For simplification, this article adopts a generic term, cerebral balance disorders, to refer to balance disorders due to cortical or subcortical lesions.
Psychiatric, psychogenic, and somatoform disorders. In 1860, Swiss physician Sigismond Jaccoud (1830-1913) described the inability to stand (ie, “astasia”) in the face of normal limb movement (188; 329).
In 1888, French neuropathologist Paul Blocq (1860-1896) first used the term “astasia-abasia,” which came to refer to any “nonorganic” gait (272); such use, however, is not precise and should be discouraged. Instead, either the term “psychiatric balance disorder” (ie, referring to balance disorders attributable to psychiatric ailments, such as schizophrenia or depression) or “psychogenic balance disorder” (ie, referring to balance disorders due to a somatoform disorder when a known stress is present) or “somatoform disorder not otherwise specified” (when no known stressful event is present) should be used (08).
|
• Disequilibrium is a state of nonvertiginous altered static (eg, standing) or dynamic (eg, walking) postural balance. | |
|
• Patients with disequilibrium often complain of unsteadiness, imbalance, and falls. | |
|
• Sensory disequilibrium is caused by altered spatial orientation. | |
|
• Except in cases of visual-vestibular mismatch, patients with sensory disequilibrium generally do worse in the dark and frequently have a Romberg sign on examination. | |
|
• Motor disequilibrium is caused by impaired motor performance, which may be due to either mechanical factors or dysfunction of central and peripheral nervous system motor pathways. | |
|
• Motor disequilibrium, including that due to cerebellar dysfunction, is generally not exacerbated in the dark or by closing the eyes. | |
|
• Disequilibrium can be a feature of an evolving vestibular disorder that presents as acute vertigo and evolves into a state of chronic disequilibrium. | |
|
• Lateropulsion is a subjective sensation of being pulled to one side or an active tilt of the body to one side, which serves to adjust the body orientation in the roll plane to an incorrect reference of verticality. | |
|
• Lateropulsion is an important driver of disability in subacute stroke because it limits a person’s ability to sit, stand, and walk and consequently delays or interferes with functional recovery. | |
|
• "Pusher syndrome" or “pusher behavior” is a clinical disorder following cerebral hemispheric damage in which some patients with lateropulsion actively push toward the hemiparetic side (contraversive pushing) and resist any attempt to correct their posture, leading to a loss of postural balance. | |
|
• Romberg sign is not specific for any particular cause of disequilibrium, but it is most closely associated with proprioceptive sensory loss (eg, in tabes dorsalis as described by Romberg). | |
|
• Patients with hemispheric lesions frequently suffer from disequilibrium that may be prolonged and may interfere with rehabilitation; at least in part, the disequilibrium in such cases may be related to an impairment of the corticovestibular modulation of the vestibular function (ie, manifest in an association between post-lesion vestibulo-ocular reflex gain and disequilibrium). | |
|
• Disequilibrium is a common and often disabling problem in the elderly, leading to unsteadiness, falls, falls with injury, and fear of falling. | |
|
• Sensory neuronopathies and peripheral neuropathies can impair proprioception, causing impaired postural control (especially with eyes closed or in darkness), gait difficulties, and a higher risk of falling. |
Disequilibrium is a state of nonvertiginous altered static (eg, standing) or dynamic (eg, walking) postural balance (189; 207). Patients with disequilibrium often complain of unsteadiness, imbalance, and falls (87; 88; 89; 113; 83; 84; 207; 215).
Sensory disequilibrium is caused by altered spatial orientation. Except in cases of visual-vestibular mismatch, patients with sensory disequilibrium generally do worse in the dark and frequently have a Romberg sign on examination (87; 88; 89; 217; 207; 210; 209; 215; 216; 253).
Motor disequilibrium is caused by impaired motor performance, which may be due to either mechanical factors or dysfunction of central and peripheral nervous system motor pathways. Motor disequilibrium, including that due to cerebellar dysfunction, is generally not exacerbated in the dark or by closing the eyes.
Disequilibrium is significantly associated with increasing age, diabetes, arthritis, impaired vision, and decreased grip strength (322).
With (nonvertiginous) disequilibrium, there is no sensation of active turning or movement of the subject or the environment when the subject is at rest; in other words, vertigo is not present. Disequilibrium can, however, be a feature of an evolving vestibular disorder that presents at times as acute vertigo and evolves into a state of chronic disequilibrium (331; 156). Many patients who develop sequential bilateral vestibulopathy (ie, first one side and then the other) can develop vertigo whenever there is asymmetric vestibular function but then ultimately be left with the chronic disequilibrium syndrome seen with bilateral vestibulopathy. Some patients may develop chronic disequilibrium after acute vertigo with unilateral vestibular lesions, potentially as a result of incomplete peripheral recovery or partial or inadequate central compensation (156), as seen in approximately one third of patients after surgery for acoustic neuroma (114; 230). Similarly, patients who are treated with particle repositioning maneuvers for benign paroxysmal positioning vertigo may develop (nonvertiginous) disequilibrium for several days or sometimes longer, presumably resulting from utricular dysfunction associated with changes in hair cell function; this may occur when otoliths are first released from the matrix and then again when they are returned to the matrix in potentially a somewhat different spatial arrangement after some compensatory adjustments had already been made.
Acute transient monocular disequilibrium (Halpern syndrome) is a rare syndrome that has been claimed to be an impairment of oculovestibulocerebellar integration, manifest by misjudgment of verticality and motion-induced by looking with one eye and alleviated by use of the fellow eye (157; 158; 125; 34). This may instead be a nonorganic disorder.
Medical history and examination. The medical history should characterize subjective sensations of imbalance or “dizziness,” onset and temporal pattern (acute or chronic, static or episodic), precipitating circumstances for such sensations if episodic, associated symptoms, course (ie, whether symptoms are static, worsening, or improving over time), and consequences (eg, frequency, circumstances, direction, and resulting injuries from falls; fear of falling; negative impact on activity levels and quality of life). During the examination, the clinician should inquire about falls (ie, frequency and precipitating circumstances as well as occurrence of fall-associated injuries), ability to dual task (ie, can the patient still maintain balance if carrying a tray or if walking and talking), medications (and particularly any temporally associated medication changes), comorbid psychiatric issues (eg, depression, anxiety, psychosis), and other comorbid neurologic or systemic symptoms or disorders (including cognitive difficulties, aural or vestibular disorders, peripheral neuropathy, urinary symptoms, etc.).
A careful general and neurologic examination is indicated in such cases, including particular attention to the assessment of mental status (including screening for depression and anxiety and assessment of frontal-executive abilities), audiovestibular function, gait, and sensation, especially proprioception in the legs. Although the details of the general neurologic examination are beyond the scope of this article, the examiner should at least address the following as part of the motor or gait examination: observation of gait initiation and execution; step length (eg, normal or short; constant or variable), height (eg, increased, normal, or reduced/magnetic), and rhythmicity or prosody; arm swing (eg, normal or reduced, symmetrical or asymmetrical); walking speed (eg, normal or reduced); presence of hesitancy, freezing, or festination; ability to manage environmental features, such as doorways and physical obstructions to the intended path; turning ability (eg, number of steps needed to turn 360 degrees, which in the normal elderly is typically six to eight steps; noting any hesitancy or stuttering, freezing, loss of balance, or tendency to move the inside foot backward during the turn); observation of “dual-task” performance (eg, noting if the patient stops walking while talking); walking on toes and then heels (mostly an assessment of distal limb strength); if able, hopping on either foot (a test of distal limb strength, balance, and coordination); tandem gait; and limb apraxia (eg, waving goodbye; pretending to brush teeth, comb hair, or use a screwdriver; demonstrating how to kick an imaginary ball). In carefully selected patients, gait and tandem gait can be assessed both with eyes open and with eyes closed, assuming adequate assistance and appropriate precautions can be taken to protect the patient from falling. The Fukuda test is optional but can be helpful in selected cases: the patient is instructed to march in place for 50 steps; if the patient deviates approximately 90 degrees or more to the left or right, the test is considered “abnormal” and is supportive of an ipsilesional peripheral vestibular disorder.
Observations of standing equilibrium from examination should include the following: (1) assessment of the patient’s ability to stand up with or without using arms or examiner’s assistance and the degree of difficulty if successful as well as the fluidity of truncal and limb movements in transitioning between sitting and standing; (2) standing posture (eg, upright, stooped); (3) stance (eg, narrow or wide base; can measure in inches or fractions of a floor tile); (4) Romberg test, noting the amount of sway with eyes open and then closed, whether the sway is generated at the ankles of hips, and whether the patient takes a step for stabilization or requires the examiner’s assistance to prevent a fall; and (5) the pull test.
The collection of clinical assessments encompasses (1) normal stance with eyes open, noting the width of the stance and any directional bias; (2) a comparison of sway with a narrow base and eyes open and then closed (ie, the Romberg test); and (3) an assessment of ability to maintain equilibrium following an unexpected perturbation (ie, the pull test).
Directional bias of postural sway. The loci of lesions causing disequilibrium are shown as a function of the directional bias of postural sway in Table 1. A directional bias of postural sway has been called “directional pulsion” in the International Classification of Vestibular Disorders I (ICVD-I), the first consensus document of the Committee for the Classification of Vestibular Disorders of the Bárány Society (39).
|
None | ||
|
• Proprioceptive impairment (diffuse or generalized) | ||
|
Lateropulsion | ||
|
• Ipsipulsion (lateropulsion ipsilateral to lesion) | ||
|
- Labyrinth | ||
|
• Contrapulsion (lateropulsion contralateral to lesion) | ||
|
- Vermis | ||
|
Fore-aft sway | ||
|
• Upbeat or downbeat nystagmus (brainstem or cerebellum) | ||
|
Retropulsion | ||
|
• Vermis | ||
Lateropulsion. Lateropulsion is a subjective sensation of being pulled to one side or an active tilt of the body to one side (291). It serves to adjust the body orientation in the roll plane to an incorrect reference of verticality (94). Lateropulsion is an important driver of disability in subacute stroke because it limits a person’s ability to sit, stand, and walk, and consequently delays or interferes with functional recovery (93; 94; 139).
Axial lateropulsion may occur with or without signs of vestibular dysfunction (eg, vertigo) and without vestibular nucleus involvement. It is typically evident only when standing, although a minority of patients may have a visible tilt while sitting (196).
Severity of lateropulsion can be graded as mild (ie, postural imbalance during tandem gait), moderate (ie, postural imbalance on standing and tandem gait), and severe (ie, inability to stand or sit without support) (358).
With non-irritative lesions (eg, infarction), lateropulsion is usually ipsilesional in caudal brainstem lesions and contralesional in rostral brainstem, thalamic, and hemispheric lesions. Irritative lesions can produce the opposite pattern (eg, otolith Tullio phenomenon) (111; 60).
Ipsilesional axial lateropulsion and ipsiversive falls have been reported in vestibular neuritis, lateral medullary syndrome (especially with rostral-dorsolateral lesions), infarcts in the territory of the medial branch of the posterior inferior cerebellar artery (without Wallenberg syndrome), infarction of the anterior rostral cerebellum (in the territory of the lateral branch of the superior cerebellar artery), and transient ischemic attacks referable to the vertebral artery and due to subclavian steal syndrome (41; 33; 07; 06; 05; 109; 109; 323; 222; 11; 231; 268; 02; 82; 194; 119; 156; 235; 362; 291; 288; 80; 286).
Contralesional axial lateropulsion and contraversive falls are reported with the otolith Tullio phenomenon (ie, sound-induced vertigo); some patients with medial medullary, pontine, or rostral midbrain tegmentum (near the red nucleus) infarction; infarction of the cerebellar nodulus or tonsil; thalamic astasia; rare isolated lesions of vestibular pathways in the internal capsule; vestibular epilepsy, and with parietal strokes (59; 27; 223; 181; 221; 360; 18; 220; 259; 271; 280; 169; 269; 72). One case has been reported with contralesion axial lateropulsion with lesions of the lateral medulla, inferior cerebellum, and rostral postero-lateral cervical spinal cord (307).
Isolated lateropulsion has been rarely reported: specific loci of isolated ipsilesional lateropulsion have included the flocculonodular lobe, the rostral cerebellar vermis, the superior and inferior cerebellar peduncles, the reticular formation of the medulla, and the dorsal spinocerebellar tract, whereas loci of isolated contralesional lateropulsion have included the midbrain tegmentum near the red nucleus and the paramedian pontine tegmentum (47; 165; 126; 36; 196; 251; 219; 360).
Pusher behavior. "Pusher syndrome" or “pusher behavior” is a clinical disorder following cerebral hemispheric damage in which some patients with lateropulsion actively push toward the hemiparetic side (contraversive pushing) and resist any attempt to correct their posture, leading to a loss of postural balance (327; 48; 283; 284; 290; 289; 287; 291; 182; 100; 265). If not assisted, patients push themselves into a lateral inclination until they fall toward the hemiparetic side. Patients with pusher syndrome show normal perception of the visual vertical, but they exhibit a severe tilt of perceived body posture in relation to gravity (183; 182). The responsible brain lesions may involve large areas of cortex (causing neglect with right hemisphere strokes or aphasia with left hemisphere strokes), but the area that appears to underly the observed syndrome is the posterolateral thalamus (183; 182). Lesions of the posterolateral thalamus cause contraversive pushing but not a tilt of the perceived visual vertical whereas, in contrast, lesions of the human "vestibular cortex" result in the opposite pattern (64). Pusher syndrome has rarely been reported with cerebellar strokes (277).
Fore-aft instability. Predominant fore-aft instability can be seen in vestibular disorders (eg, bilateral vestibulopathy and benign paroxysmal positioning vertigo as well as in conjunction with disorders causing downbeat or upbeat nystagmus) and basal ganglia disorders.
Vestibular falls can be diagonally forward or backward and toward or away from the side of the lesion, depending on the site of the lesion and on whether vestibular structures are excited or inhibited.
Backward disequilibrium. “Backward disequilibrium” (retropulsion) is an abnormal postural behavior that has been defined as a posterior position of the center of mass relative to the base of support (234; 233; 305). It is characterized by a posterior trunk tilt in standing and sitting positions, which predisposes subjects to backward falls. This can result in falls, escalating fear of falling, and loss of autonomy.
The Romberg test. Romberg sign is not specific for any particular cause of disequilibrium, but it is most closely associated with proprioceptive sensory loss (eg, in tabes dorsalis as described by Romberg). The Romberg test is relatively insensitive to compensated unilateral vestibular or cerebellar dysfunction, but it may be present in bilateral vestibular loss, acute unilateral vestibular loss, sometimes with pathology of the spinocerebellum (ie, the anterior vermis and paravermis of the anterior lobe), and less often with other cerebellar dysfunction. Sensitivity in routine clinical settings can be increased by narrowing the patient’s base of support (eg, with a “sharpened Romberg test” with feet in a heel-to-toe position) or by standing on foam rubber to distort proprioceptive input from the feet (“foam posturography”).
Although the Romberg sign is now fairly standardized, there is still some variability in examination technique and interpretation across expert neurologic examiners. In particular, there is variability in how much postural instability is required for a positive test (eg, increased sway only, a step to the side, or a fall); whether sway at the ankles is critical, or whether sway from the hips can be accepted; whether the feet should be positioned together, as close together as possible to maintain stance with eyes open, or in tandem position; whether footwear should be worn or removed; whether hands should be held at the side or extended forward or laterally; whether the examiner should gently pull or push the patient to one side; and so on. Such variability may affect both the sensitivity and specificity of the test.
In examining a patient for the presence of the Romberg sign, the examiner typically observes the patient’s postural stability with the patient’s feet together, initially with eyes open and then with the eyes closed. The Romberg sign is present when a patient is able to stand with feet together and eyes open but sways or falls with eyes closed.
The pull test. To properly perform the pull test (254), the patient should be informed that he or she will be pulled forcefully backward to test balance and that the patient must prevent himself or herself from falling, if necessary, by taking a step backward after he or she is pulled. At least one practice session is carried out before the final test. The patient must be upright with feet comfortably apart and must not lean forward unless axial flexion prevents upright posture. The pull test should be performed with a wall or door behind the examiner to allow the use of an appropriately forceful pull and to avoid injuries to the patient and examiner from a fall; this is especially important if the patient weighs near the same weight or significantly more than the examiner, but really it is good practice to perform the test this way on all patients. The patient should be pulled briskly and forcefully without any hint of the exact timing of the pull (ie, so nothing like “1, 2, 3, pull” or “here we go”), but must not be pulled while off balance from a previous pull.
The most common errors in performing the pull test are (1) the patient is tapped or pulled too lightly; (2) the examiner does not allow sufficient recovery space for the patient; (3) the patient stands with feet held together or too far apart; (4) the patient is pulled with a steady, continuous pull; (5) the examiner pulls the arms rather than the shoulders; (6) the patient braces by shifting his or center of gravity forward; and (7) the pull test is performed without support, especially when the patient weighs much more than the examiner (254).
Cerebral balance disorders. Patients with hemispheric lesions frequently suffer from disequilibrium that may be prolonged and may interfere with rehabilitation; at least in part, the disequilibrium in such cases may be related to an impairment of the corticovestibular modulation of the vestibular function (ie, manifest in an association between post-lesion vestibulo-ocular reflex gain and disequilibrium) (73).
“Frontal disequilibrium,” dysfunction of fronto-subcortical (mainly fronto-basal) pathways, is manifest by an inability to organize trunk and leg movements to rise or stand unsupported. Frontal disequilibrium can be seen in normal pressure hydrocephalus, Binswanger disease, anti-Hu encephalomyelitis (86), demyelinating disease, etc. Diurnally fluctuating frontal dysequilibrium has been reported secondary to a pineal pilocytic astrocytoma with the fluctuating symptoms of hydrocephalus possibly caused by a check-valve mechanism in a pineal-region tumor with transient or variable compression of the basal ganglia and frontal lobes (197).
Disequilibrium in the elderly. Disequilibrium is a common and often disabling problem in the elderly, leading to unsteadiness, falls, falls with injury, and fear of falling (344; 20; Fife and 20; 193; 339). Although the Romberg sign is often absent in such patients, they tend to sway more and do poorer on semiquantitative gait and balance testing than similarly aged peers (Fife and 20). Several studies suggest that multifocal subcortical disruption of association fibers is a significant contributing factor to age-associated disequilibrium (23; 22; 193; 350; 256), or what has been called “presbyastasis” (30). Subcortical white matter lesions identified on MRI are associated with disequilibrium in elderly people; these lesions probably interfere with central processing of sensorimotor signals leading to impaired postural responses and gait and balance difficulties (23; 22; 193). In a prospective, longitudinal study of elderly subjects (aged 75 to 92 years) with disequilibrium with age- and sex-matched controls, patients were four times more likely to fall than control subjects over five years of follow-up (193). The frequency of falls was strongly correlated with measures of balance. Cases had significantly worse subcortical white matter lesions and frontal atrophy and a higher ventricle-to-brain ratio (Evans ratio) than controls (193). In pathologic studies, disequilibrium in elderly individuals was associated with frontal atrophy and ventriculomegaly, reactive astrocytes in the frontal periventricular white matter, and increased arteriolar wall thickness (ie, as measured by a “sclerotic index”) (350); these findings support an association between subcortical leukoencephalopathy and disequilibrium in older patients, even in the absence of hypertension. Other studies of elderly patients with disequilibrium symptoms found evidence for contributions to disequilibrium from age-associated involvement of central vestibular pathways; in particular, (1) fixation suppression of vestibular nystagmus was associated with T2 hyperintensities in the basal ganglia (256); and (2) previous vascular disorders of the central nervous system were a predictor of decreased vestibulo-ocular reflex gain (325).
Proprioception also declines significantly with aging, and consequently, aged individuals rely less on proprioception for postural control (28); not surprisingly, then, disrupting proprioceptive inputs by prolonged Achilles tendon vibrations produces a greater postural perturbation in young adults compared with older adults (28).
Postural instability (disequilibrium) in Parkinsonism. People in the early stages of Parkinson disease are able to intentionally reweight the influence of disorienting visual information for postural control (91). As the disease advances, postural control in patients with Parkinson disease becomes particularly impaired during forward and backward leaning, whereas postural control in patients with idiopathic normal pressure hydrocephalus is impaired in all directions (264).
Postural instability is intertwined with freezing of gait in Parkinson disease, and the two can influence each other behaviorally and may coincide neurologically (29), whereas in contrast postural instability is not linked to REM sleep behavior disorder (32).
The ability to recover balance after a sudden shoulder pull is used as a clinical measure of postural instability in Parkinson disease. There are, in fact, several common variants of this test being used in clinical practice: (1) the “pull test” or “retropulsion test” as described in the MDS-UPDRS scale; (2) using an unexpected shoulder pull, without prior warning; and (3) the push-and-release test (123; 46; 336; 255; 267). In a comparison with several variants, the most valid test for postural stability in Parkinson disease was an unexpected shoulder pull, executed once, with taking more than two steps backward considered abnormal (342). However, another study concluded that both the pull test and the push-and-release test are valid and relatively equivalent when assessing patients in their “off” medication state; however, the push-and-release test is more accurate than the pull test in the “on” state (336). In any case, the utility of such tests to detect postural instability is related to the subject's behavioral response, not the force needed to pull them off balance—they are simply unable to compensate for the perturbations: indeed, if patients with Parkinson disease need assistance to prevent a fall on the first pull, they do not generally show a learning effect when pulled multiple times in the same direction (198). Unfortunately, variability in pull test performance and interpretation by examiners can lead to inadequate evaluation of postural instability in patients with Parkinson disease (254; 267). In addition, there is only a moderate correlation between the retropulsion test and body sway after platform rotations with dynamic posturography during the “off” phase, but no correlation during the “on” phase (46).
Various standardized quantitative clinical balance measures and functional gait scales have also been developed, including Tandem And Unipedal Stance, Functional Reach (assessed while standing), Modified Functional Reach (assessed while sitting for individuals unable to stand), Lateral Reach, Timed Up-and-Go, Balance Master, Dynamic Balance, Clinical Test Of Sensory Interaction And Balance, Berg Balance Scale, Tinetti Performance-Oriented Mobility Assessment, Activities-Specific Balance Confidence Scale, Sensory Organization Test, Self-Selected Gait Velocity, and Dynamic Gait Index. Reaching tasks particularly challenge postural stability in patients with severe Parkinson disease (320). The Functional Reach Test is (1) simple and easy to use, (2) useful for detecting balance impairment and monitoring change in balance performance over time, (3) predictive of falls in the elderly and in patients with Parkinson disease or stroke, and (4) a marker of physical frailty (116; 115; 345; 148; 173; 187; 49); however, (1) whether the Functional Reach Test actually measures dynamic balance has been questioned because healthy elders and balance-impaired individuals with vestibular hypofunction attained the same functional reach distance (348); (2) the test is not as easy to use in clinical neurologic practice as some other measures. In the Functional Reach Test, (1) the patient is instructed to stand next to, but not touching, a wall and position the arm that is closer to the wall at 90 degrees of shoulder flexion with a closed fist; (2) the assessor records the starting position at the third metacarpal head; (3) the patient is instructed to “reach as far as you can forward without taking a step”; (4) the location of the third metacarpal is again recorded; (5) scores are determined by assessing the difference between the start and end position (ie, the “reach distance,” usually measured in inches); (6) three trials are done, and the average of the last two is used as the final reach distance.
Genetic disorders. Several similar genetic conditions have been reported under the rubric of “disequilibrium syndrome.” Cerebellar ataxia, mental retardation, and dysequilibrium syndrome (CAMRQ), often more simply referred to as “disequilibrium syndrome,” is a rare genetically heterogeneous disorder characterized by congenital cerebellar ataxia and mental retardation and transmitted as an autosomal recessive trait. Affected family members may have severe truncal ataxia with or without a quadrupedal gait. CAMRQ1 (OMIM #224050) is an autosomal recessive condition caused by homozygous mutation in the VLDLR gene (OMIM #192977), which encodes the very-low-density-lipoprotein receptor, on chromosome 9p24 (278; 51; 246). CAMRQ2 (OMIM #610185) is an autosomal recessive condition caused by homozygous mutation in the WDR81 gene (OMIM 614218) on chromosome 17p. CAMRQ3 (OMIM # 613227) is an autosomal recessive condition caused by homozygous mutation in the CA8 gene (114815) on chromosome 8q12. CAMRQ4 (OMIM #615268) is an autosomal recessive condition caused by homozygous mutation in the ATP8A2 gene (OMIM 605870) on chromosome 13q12. Other disorders overlap with CAMRQ4, including congenital disorder of glycosylation, type Ia (OMIM #212065), which is an autosomal recessive condition caused by homozygous or compound heterozygous mutation in the gene encoding phosphomannomutase-2 (OMIM 601785) on chromosome 16p13 (243).
Episodic ataxia is a genetically heterogeneous disorder that is characterized by spells of disequilibrium and incoordination and is often associated with progressive ataxia. Episodic ataxia type 1 (OMIM #160120), with myokymia and periodic ataxia, is transmitted as an autosomal dominant trait and is caused by a heterozygous mutation in the potassium channel gene KCNA1 (OMIM 176260) on chromosome 12p13. Episodic ataxia type 2 (OMIM #108500), with nystagmus and periodic ataxia, is transmitted as an autosomal dominant trait caused by heterozygous mutation in the calcium ion channel gene CACNA1A (OMIM 601011) on chromosome 19p13. Episodic ataxia type 6 (OMIM #612656) is caused by a heterozygous mutation in the SLC1A3 gene (OMIM 600111) on chromosome 5p13. Other forms of episodic ataxia are associated with vertigo rather than disequilibrium.
Disequilibrium with spastic diplegia and immunodeficiency and intracytoplasmic neutrophil inclusion bodies has been reported in children with purine nucleoside phosphorylase deficiency (OMIM #613179), a rare autosomal recessive immunodeficiency caused by mutation in the PNP gene (OMIM 164050) (319). Clinical improvement in neutropenia has been anecdotally reported after intravenous immunoglobulin (144; 319; 14).
Sensory neuronopathies and peripheral neuropathies. Chemotherapy-induced peripheral neuropathy can impair proprioception, causing impaired postural control (especially with eyes closed or in darkness), gait difficulties, and a higher risk of falling (253). The situation is similar for other neuropathies (eg, diabetes), and sensory neuronopathies (eg, tabes dorsalis, pyridoxine toxicity).
Postural instability is a major factor predisposing affected individuals to balance-related falls and subsequent medical complications (eg, fractures), fear of falling, decreased mobility, self-restricted physical activity, social isolation, depression, apathy, loss of autonomy, and decreased quality of life (39; 195; 159; 90). Postural instability is one of the most disabling features of aging and of age-related diseases (eg, Parkinson disease, stroke).
Patients with bilateral vestibulopathy generally do not recover; only 20% of patients rate their illness as improved over time, yet more than half feel they are mildly to not at all affected by their illness (363). Sensory neuronopathy also has a poor prognosis for recovery, but in the absence of additional morbidity or mortality related to the underlying disease, many continue to manage by learning various coping strategies, and rare patients improve modestly (95; 147; 351; 96; 145; 146; 84; 69; 190; 298; 311; 186; 308).
Most elderly patients with nonspecific disequilibrium progress slowly (193), although occasional patients worsen over a short time (Fife and 20; 22). Severe white matter disease, with its associated gait disturbance, is associated with greater morbidity and mortality in the elderly (66) and predicts worse outcome after balance and gait rehabilitation (151).
Patients with vascular parkinsonism typically progress faster than those with Parkinson disease (297). In Parkinson disease and various Parkinson-plus syndromes, there may be retropulsion with standing leading to falls backward, festination leading to falls forward, or stuttering and freezing while turning leading to falls to the side. Overall, though, backward falls are most common with these disorders.
In contrast, patients with stroke are most likely to have lateropulsion and falls to one side. Lateropulsion in the brainstem or with thalamic or basal ganglia lesions generally lasts days to weeks (238; 126), with one systematic review finding a median time to resolution of 14 days (296). Lateropulsion is commonly seen after medullary infarction and is an isolated finding in one third of such patients; large vessel atherosclerosis and large-vessel occulsion are the most common etiologies (296).
Lateropulsion delays recovery from stroke and increases dependency, particularly with right-hemisphere strokes (17; 15; 16; 265). The rate of recovery from lateropulsion after stroke depends on the side of the lesion and the number of key motor, proprioceptive, or hemianopic or visual-spatial deficits; the more postural control systems affected, the slower the recovery (15). In addition, older age and severe impairments are associated with delayed recovery from lateropulsion in a side-specific manner (17; 16). Predictors of persistent lateropulsion at discharge among patients with a left-hemisphere stroke include older age and worse admission motor status, whereas predictors for patients with a right-hemisphere stroke include older age, greater admission limb placement error, and lower cognitive Functional Independence Measure scores. Visuospatial neglect does not influence recovery from lateropulsion.
Psychogenic balance and gait disorders is potentially reversible, especially if the symptoms have been sudden in onset and are less than a few weeks to months in duration (121).
Case 1. 52-year-old man with tabes dorsalis from the Dercum-Muybridge collaboration (257; 106; 107; 217; 210; 216):
A 52-year-old Danish man with advanced tabes dorsalis developed marked difficulty walking in the dark or with eyes closed. Philadelphia neurologist Francis Dercum arranged to have him photographed by pioneering photography Eadweard Muybridge at the University of Pennsylvania in 1885, using Muybridge’s arrays of sequentially triggered single-image cameras. The resulting images are the first example of motion-picture sequences of a sensory ataxic gait. The images obtained were composited onto a global plate.
The man was first photographed while walking with eyes open. As Dercum summarized, “[Owing] to the guidance afforded by his eyes and to the evident effort he is making, as shown in the throwing back of the shoulders and the fixation of the trunk, his walk is tolerably good” (106; 107). The footfalls are close to the centerline along the direction of ambulation. In contrast, his gait severely deteriorated when he closed his eyes:
|
A remarkable change is at once observed, and it needs no elaborate study of the trajectories to show what the chief elements of the change are. It is seen at once that the foot is raised much higher from the ground, and that the lateral sway is enormously increased; also, that the successive steps are more irregular . . . [The foot strikes the ground abruptly], the entire sole impinging or flopping, as it were, on the ground at once (106; 107). |
With eyes closed, the feet were spread widely apart for balance, often farther apart than the spread of the shoulders. The feet were lifted high but were appropriately dorsiflexed at the ankle. Muybridge had clearly not understood the significance of these sequences because he simply indicated “arms down” and “arms up” in the captions he included in Animal Locomotion (1887). In contrast, Dercum clearly understood their significance and considered that this set of photographic sequences “is one of the most instructive in the collection” (106; 107).
Case 2. John “Jack” Douglas Crawford II (87; 88; 89; 215):
In 1948, shortly after streptomycin became available as a drug, John “Jack” Douglas Crawford II (1920-2005), then a 30-year-old pediatric endocrinologist, was misdiagnosed with tuberculous arthritis of the knee and was treated with intramuscular and intra-articular streptomycin. After 2.5 months of treatment with streptomycin, Crawford experienced the dramatic onset and rapid progression of bilateral vestibular dysfunction, evolving over several days. Manifestations included postural instability in darkness (Romberg symptom), gait ataxia, motion-induced vertigo and nausea, and oscillopsia. Initially, he had to hold onto objects and rely on tactile cues to ambulate, but later he was able to walk by focusing his gaze on distant objects. After four years, he had learned to walk fairly well in the light and had resumed most of his former recreational activities, despite continued vestibular dysfunction. One partial benefit was a newly acquired resistance to seasickness. However, he continued to have severe disequilibrium in the dark and sometimes had to get about on hands and knees. Forty years after his loss of vestibular function, Crawford was still very active physically and with little evident disability. However, he acknowledged continued disequilibrium with particular difficulty on uneven or unstable surfaces and in the dark.
|
• The “limits of stability” (ie, the area over which an individual can move their center of mass and maintain equilibrium without changing the base of support) are determined by the size of the support base (eg, stance width), which strategies (eg, hip flexion) are adopted to maintain stability, and limitations on joint flexibility, muscle strength, and available sensory information to detect the limit. | |
|
• Although the 3-dimensional locus of stability has been likened to an inverted cone, this is really a crude approximation given that the actual shape depends on the base of support and what “strategy” is adopted (eg, whether motion is constrained to the ankles or whether motion at multiple joints is allowed). | |
|
• The “cone” of stability is typically quite distorted, for example, being wider with forward perturbations than with backward perturbations. | |
|
• Small limits of stability will increase the risk of falls. | |
|
• Common movement strategies to maintain balance include: (1) the “ankle strategy,” in which the body moves at the ankle as an “inverted pendulum,” is appropriate for small amounts of sway when standing on a firm surface; (2) the “hip strategy,” in which the body exerts a torque at the hips, is appropriate when the center of mass must be moved quickly for rapid large perturbations, especially when standing on a narrow or compliant surface (for which ankle torque is insufficient); (3) the “stepping strategy,” (ie, taking a step to regain equilibrium); and (4) the “reaching strategy” (ie, using arm reactions to regain equilibrium). | |
|
• Elderly individuals at risk of falling tend to use hip, stepping, and arm strategies more than those with a low risk of falling who preferentially use the ankle strategy to maintain postural stability. | |
|
• Control of postural sway (equilibrium) develops during childhood to reach an optimum during early adult life and stays fairly constant for several decades before progressively declining after age 50. | |
|
• In a process of “sensory reweighting,” the nervous system adjusts the relative contribution of sensory information to maintain balance with changing environmental circumstances. | |
|
• Optimal balance requires continuous monitoring of body sway and other orientation information provided by the somatosensory, vestibular, and visual systems; the functional ranges of these systems overlap, allowing partial compensation for deficits or distortions. | |
|
• Sensory disequilibrium is caused by altered spatial orientation, which may be due to proprioceptive impairment, balanced bilateral or compensated unilateral vestibular dysfunction, visual-vestibular mismatch, or multisensory impairment. | |
|
• The ability to compensate for small irregularities in the ground surface relies on automatic sensory-feedback regulation mediated through afferent neurons subserving proprioception. | |
|
• Vestibular dysfunction in the roll plane of the vestibulo-ocular reflex is responsible for body lateropulsion in most cases. | |
|
• Motor disequilibrium is caused by impaired motor performance, which may be due either to mechanical factors or to dysfunction of central and peripheral nervous system motor pathways: the central motor pathways that may be affected in patients with motor disequilibrium include the pyramidal, extrapyramidal, and cerebellar systems, whereas the peripheral motor pathways include the peripheral nerves, neuromuscular junctions, and muscles. |
The “limits of stability” (ie, the area over which an individual can move their center of mass and maintain equilibrium without changing the base of support) are determined by the size of the support base (eg, stance width), which strategies (eg, hip flexion) are adopted to maintain stability, and limitations on joint flexibility, muscle strength, and available sensory information to detect the limit (166). Although the 3-dimensional locus of stability has been likened to an inverted cone, this is really a crude approximation given that the actual shape depends on the base of support and what “strategy” is adopted (eg, whether motion is constrained to the ankles or whether motion at multiple joints is allowed). Furthermore, the “cone” of stability is typically quite distorted, for example, being wider with forward perturbations than with backward perturbations. Small limits of stability will increase the risk of falls (116; 166).
Common movement strategies to maintain balance include: (1) the “ankle strategy,” in which the body moves at the ankle as an “inverted pendulum,” is appropriate for small amounts of sway when standing on a firm surface; (2) the “hip strategy,” in which the body exerts a torque at the hips, is appropriate when the center of mass must be moved quickly for rapid large perturbations, especially when standing on a narrow or compliant surface (for which ankle torque is insufficient); (3) the “stepping strategy,” (ie, taking a step to regain equilibrium); and (4) the “reaching strategy” (ie, using arm reactions to regain equilibrium) (302; 166; 174); the latter might be labeled better as the “arm counterbalance strategy” or more simply and broadly as the “arm strategy.” Postural strategies are employed for both spontaneous (ie, unexpected) perturbations and anticipated perturbations (eg, with self-initiated movement). To some degree, individuals can influence which strategies are selected in a particular circumstance, and then weigh their responses based on intention, experience, and expectations (68; 166).
Elderly individuals at risk of falling tend to use hip, stepping, and arm strategies more than those with a low risk of falling who preferentially use the ankle strategy to maintain postural stability (232; 166). Use of the hip strategy is also augmented when an individual has developed a fear of falling (01; 166). In Parkinson disease, rigidity results in biomechanical impairments (eg, stooped posture), and bradykinesia impairs both reactionary and anticipatory postural adjustments (279); in addition, later in the course, patients with Parkinson disease also may develop freezing of gait, decline of executive functions, inflexibility in adapting motor set to changing circumstances, and difficulty perceiving small changes in surface inclination (ie, impaired kinesthesia) that individually and collectively contribute to balance and mobility dysfunction (354; 279).
Control of postural sway (equilibrium) develops during childhood to reach an optimum during early adult life and stays fairly constant for several decades before progressively declining after age 50 (310).
In a process of “sensory reweighting,” the nervous system adjusts the relative contribution of sensory information to maintain balance with changing environmental circumstances (244; 292; 293; 294; 74; 141; 142; 140). For example, in a well-lit environment with a firm support base, healthy individuals rely primarily on somatosensory (approximately 70%) inputs, with some relatively minor contributions from vision (approximately 10%) and vestibular information (approximately 20%) (292); however, on an unstable surface, vestibular and visual information are weighted much more heavily for postural orientation, and dependence on surface somatosensory inputs is markedly decreased.
The perception of verticality (ie, the direction at right angles to the horizon, or “upright”) has multiple neural representations (183). The perception of visual verticality is independent of the perception of postural (or proprioceptive) verticality (40); consequently, in disease, the different systems can be differentially affected. For example, the internal representation of visual, but not postural, verticality is tilted in persons with unilateral vestibular loss, while the internal representation of postural, but not visual, verticality is tilted in persons with hemineglect due to stroke (185). Such inaccurate (ie, tilted) internal representations of verticality result in automatic but counterproductive postural adjustments that are not aligned with gravity, resulting in postural instability (166).
Optimal balance requires continuous monitoring of body sway and other orientation information provided by the somatosensory, vestibular, and visual systems. The functional ranges of these systems overlap, allowing partial compensation for deficits or distortions (260; 261). For example, a normal subject can maintain an upright stance either with vision eliminated (eg, with eye closure), with proprioception disrupted (eg, standing on a moving or tilting surface), or with vestibular function distorted (eg, as a result of rotationally induced vertigo). However, loss or distortion of inputs from two or more of these systems is associated with disequilibrium and falls. Thus, a patient with profound loss of proprioception or with uncompensated unilateral or bilateral vestibular dysfunction may fall if vision is eliminated (eg, with eyes closed); this is the basis of the Romberg sign (217). The intensity of imbalance is a function of the mismatch between the sensory systems that results from deficient or distorted input from one or more components (57).
Sensory disequilibrium is caused by altered spatial orientation, which may be due to proprioceptive impairment, balanced bilateral or compensated unilateral vestibular dysfunction, visual-vestibular mismatch, or multisensory impairment.
The ability to compensate for small irregularities in the ground surface relies on automatic sensory-feedback regulation mediated through afferent neurons subserving proprioception. Intact proprioception is necessary for the rapid processing of visual feedback during movements (24). Although visuospatial abilities can influence the capacity to form accurate spatial representations, proprioception can influence the time and effort necessary to use spatial representations, which in time-dependent situations (eg, ambulation on uneven group or in complex environments) can increase the risk of falls (299). Proprioception also contributes to the visual identification of ownership during active movements (25). In the absence of proprioception, limited motor memory may allow maintenance of posture or continuation of a simple repetitive movement, but no novel movements are possible without visual feedback (85).
Vestibular dysfunction in the roll plane of the vestibulo-ocular reflex is responsible for body lateropulsion in most cases (54; 55; 59; 63; 65). Graviceptive inputs from the otoliths and the vertical semicircular ducts converge at the level of the vestibular nuclei in the lateral pontomedullary junction and then cross the midline in the pons, just rostral to the vestibular nuclei (61; 65; 360). After crossing, the graviceptive pathways ascend the brainstem through the paramedian tegmentum in ascending fiber bundles such as the medial longitudinal fasciculus, then through the vestibular thalamus, to reach the multisensory parieto-insular “vestibular” cortex (56; 64; 65). Consequently, brainstem lesions caudal to or involving the vestibular nuclei generally cause ipsiversive tilts and falls, whereas lesions just rostral to the vestibular nuclei generally cause contraversive tilts and falls.
Neural afferent fibers from the otoliths and the vertical semicircular ducts mediating vestibular function in the roll plane also project to the ocular motor nuclei, the supranuclear centers of the interstitial nucleus of Cajal, and the rostral interstitial nucleus of the medial longitudinal fasciculus, crossing the midline just rostral to the sixth nerve and vestibular nuclei; lesions in this pathway produce the ocular tilt reaction (349; 58; 63; 155; 54; 55; 228; 59; 65).
Lesion mapping studies have demonstrated that ipsilesional axial lateropulsion results from lesions of the dorsal spinocerebellar tract, the inferior cerebellar peduncle, the inferior vestibular nucleus, or the lower cerebellar hemisphere involving the territory of the lateral branch of the posterior inferior cerebellar artery (309; 231; 328; 119). Axial lateropulsion without limb ataxia results from an impairment of vestibulospinal postural control caused by a lesion of the descending lateral vestibulospinal tract, whereas axial lateropulsion with limb ataxia likely results from impaired or absent proprioceptive information caused by a lesion of the ascending dorsal spinocerebellar tract (328). It is possible that ascending graviceptive information from the spinal cord may run adjacent to the dorsal spinocerebellar tract or perception of the visual vertical can be influenced by ascending spinal proprioception (194). In the pons, axial lateropulsion probably results from damage to the graviceptive pathway ascending through the paramedian pontine tegmentum (360).
The location of the vestibular cortex in humans has been investigated in various lesion and stimulation studies, but there continues to be disagreement about its precise location and functions and about even the existence of a unimodal vestibular cortex (61; 56; 64; 152; 56; 43; 200; 124; 50; 180; 117; 227; 364; 239; Dieterich and Brandt 2015; 359). Suggested loci of the human vestibular cortex have included the multisensory parieto-insular cortex (61; 56; 120; 352), the posterior insular cortex (352), the cytoarchitectonic area OP 2 in the parietal operculum (364), the superior temporal region (134), the lateral cortical temporoparietal area (the “temporo-peri-Sylvian vestibular cortex”) (180), and the anterior portion or superior lip of the intraparietal sulcus (128; 43).
Although the parieto-insular cortex has been postulated to be the core region within the vestibular cortical system (56; 227; 239; 359), the vestibular cortical system is likely distributed among several multisensory areas in the parietal and temporal cortex, which are part of a larger network for spatial attention and sensory-motor control (124; 50; 364; 131). This extended cortical network of vestibular cortex areas may have right hemispheric dominance, consistent with the rightward asymmetrical cortical network for spatial orientation (124). Nevertheless, although animal and human studies demonstrate several multisensory areas that process vestibular information, rather than a single primary vestibular cortex (64), the parieto-insular vestibular cortex is apparently an integration center of the multisensory vestibular cortex areas within the parietal lobe (64; 227). A coordinate-based meta-analysis of neuroimaging studies using caloric vestibular stimulation, galvanic vestibular stimulation, and auditory stimulation (clicks and short-tone bursts) to activate the vestibular receptors and, thereby, stimulate the vestibular cortex found that the retroinsular cortex, parietal operculum, and posterior insula are vestibular regions where afferents converge from otoliths and semicircular canals (227). The parieto-insular vestibular cortex may not be a single functional area but instead may consist of multiple areas with different anatomical correlates and different functional specializations (132).
Motor disequilibrium is caused by impaired motor performance, which may be due either to mechanical factors or to dysfunction of central and peripheral nervous system motor pathways. The central motor pathways that may be affected in patients with motor disequilibrium include the pyramidal, extrapyramidal, and cerebellar systems, whereas the peripheral motor pathways include the peripheral nerves, neuromuscular junctions, and muscles.
Cerebellar diseases. A PET study using a mobile gantry PET system, confirmed the distributed neural network involved in standing equilibrium, found that the cerebellar vermis efferent system plays an important role in maintaining standing posture, and suggested that visual association cortex may help regulate postural equilibrium while standing (275). Compared with the supine position, (1) standing with feet together activated the anterior lobe of the cerebellum and the right visual cortex (Brodmann area 18/19); (2) standing on one foot activated the anterior vermis of the cerebellum and the lateral cortex of the posterior lobe ipsilateral to the weight-bearing side; (3) tandem stance activated the visual association cortex, the anterior and posterior vermis, and the midbrain; and (4) standing with eyes closed activated the prefrontal cortex (Brodmann area 8/9) (275).
Nevertheless, in patients with cerebellar disease, the vestibulopostural loop remains largely unaffected, and patients generally retain the ability to use vision to control much of their unsteadiness, despite unsteadiness due to muscle incoordination and disordered regulation of vestibuloproprioceptive reflexes. Postural sway with eyes closed is increased both clinically and with more sophisticated measurement and recording techniques in patients with cerebellar disease, particularly in patients with disease of the vestibulocerebellum or spinocerebellum.
Parkinson disease. Many factors contribute to balance impairment in patients with Parkinson disease, including disturbed postural reflexes, poor control of voluntary movement, worse trunk mobility, abnormalities in programming preparatory postural adjustments, an ineffective stiffening response, inability to modify postural responses for changing postural demands, difficulties in scaling postural responses in accordance with the need of the balance task at hand, and abnormal vertical perception and disturbed processing of graviceptive pathways (225; 167; 266; 285; 198; 340; 13). Defective cue production may be the basic deficit in parkinsonian hypokinesia (237); defective cues lead to problems synchronizing preparatory activity, which in turn produce abnormalities in movement forces that are characterized by unpredictable and inaccurate movement endpoints, ultimately producing postural and gait instability (237).
Individuals with Parkinson disease have smaller than normal postural stability margins in all directions, especially for backwards sway and for lateral sway with a narrow stance width: backwards postural stability is compromised by lack of knee flexion and lateral postural stability is compromised by lack of trunk flexibility (167). Even among patients with Parkinson disease and a normal pull test, there is a subclinical direction-specific balance impairment that is more apparent in forward-right and backward-left directions on dynamic posturography (136). An increased mediolateral sway and sway area while standing with eyes closed are characteristic of parkinsonian postural instability (44); these sway indices are significantly associated with disease severity, rated both by the Hoehn and Yahr scale as well as by the Motor Section of the Uniform Parkinson’s Disease Rating Scale (UPDRS) (44). Although the stooped posture contributes to destabilization in patients with Parkinson disease, it does not account for the abnormal postural responses (175).
Postural instability or gait difficulty (PIGD), akinetic-rigid, and tremor-dominant subtypes of Parkinson disease have been proposed (77; 160). PIGD and tremor-dominant subtypes show different clinical manifestations and different patterns of spontaneous neural activity in the cerebellum and putamen (77). Compared with non-PIGD Parkinson disease, the PIGD subtype has (1) markedly greater cortical thinning of the bilateral frontal-temporal and posterior cortical regions (cuneus or precuneus) (160); (2) increased neocortical beta-amyloid deposition (252; 365); (3) a greater frequency of cerebral microbleeds (79); (4) more white matter lesions and greater loss of white matter integrity (150) although an association of PIGD Parkinson disease with white matter hyperintensities on brain MRI has not been consistently demonstrated (161); (5) a particular pattern of brain hypometabolism (compared to tremor-dominant Parkinson disease in the caudate and inferior parietal lobule) with particular metabolic reductions in the inferior parietal lobule, middle frontal gyrus, and fusiform gyrus, and decreased functional connectivity within the prefrontal-parietal network, associated with severe PIGD symptoms (361); (6) a stronger association with cognitive dysfunction, particularly impairments in global cognition and aspects of executive functioning (357; 295; 224; 252; 191); (7) a stronger association with nonmotor symptoms (356); (8) a stronger association with sexual dysfunction (105; 177); and (9) different associations to alcohol and smoking (315). The PIGD subtype of Parkinson disease itself may have distinct subtypes because those with postural instability with falling (PIF) and those with freezing of gait (FOG) have different demographic, nonmotor, and genetic predictors (122) and possibly different patterns of cortical atrophy (160). In addition, specific cognitive domains are differentially related to distinct PIGD components, suggesting that multiple neural pathways contribute to the relationship of cognition and PIGD symptoms in persons with Parkinson disease: deficits in executive function are associated with impairments in gait, freezing, and postural stability, whereas visuospatial impairments are associated only with more severe freezing, and poorer memory function is associated only with greater postural instability (191).
The lack of benefit from dopaminergic medication contrasted with the apparent success of extrastriatal deep-brain stimulation suggests that postural instability in Parkinson disease involves neurotransmitter systems other than dopamine and brain regions extending beyond the basal ganglia (149; 90). The PIGD subtype is consistently associated with greater severity of nondopaminergic symptoms (338). Indeed, patients with severe PIGD, but not those with tremor-dominant Parkinson disease, appear to have a derangement in indoleamine metabolism at the reaction step catalyzed by aromatic amino acid decarboxylase (AADC), suggesting that postural instability in advanced Parkinson disease may be related in part to impaired serotonergic transmission secondary to inhibition or down-regulation of AADC (171).
Small vessel cerebrovascular disease. Small vessel disease can also cause disequilibrium (23; 22; 193; 204; 350; 256). For example, isolated pontine hyperintense lesions on MRI are associated with disequilibrium in patients with atherosclerosis (204). In addition, subcortical white matter lesions identified on MRI are associated with disequilibrium in elderly people; these lesions probably interfere with central processing of sensorimotor signals leading to impaired postural responses and gait and balance difficulties (23; 22; 193).
|
• Dysequilibrium is a major category of dizziness in the elderly but can affect individuals of any age. | |
|
• The increased risk of disequilibrium and falls associated with aging is not due to aging of “the balance system” per se but to an increased likelihood of impairment or pathology in the various physiological subsystems underlying the complex skill of balancing. |
Dysequilibrium is a major category of dizziness in the elderly but can affect individuals of any age (346; 353). In a study of a community in Poland, the prevalence of dizziness was 16%, with dizziness being more common in the elderly and in women (353); among young people, dizziness was typically due to vertigo or presyncope, whereas among people aged 50 or older, dizziness was often due to disequilibrium.
Lateropulsion occurs in approximately one third of patients with peripheral vestibular disorders (332). It can be induced by rotation, and postrotatory lateropulsion occurs in every instance when postrotatory nystagmus is detectable (333).
In a study of 66 patients with isolated cerebellar infarctions, axial lateropulsion occurred in 82%, and isolated lateropulsion occurred in 8% (358). Patients with lesions in the caudal vermis (ie, folium-tuber, uvula, tonsil, and nodulus) and posterior paravermis were more likely to have lateropulsion than those without lesions in these locations, and all patients with lesions in the folium-tuber or nodulus showed lateropulsion (358). Lesions in the nodulus were strongly associated with contralateral pulsion, and involvement of the culmen (ie, the portion of the anterior vermis adjacent to the primary fissure of cerebellum) was associated with ipsilateral pulsion and isolated lateropulsion without vertigo (358). Severe lateropulsion was seen significantly more commonly among patients with lesions in the uvula (41%), nodulus (44%), and tonsil (38%) than those with cerebellar infarctions in other areas (358). Nearly one third (30%) of patients with a lesion of the culmen showed lateropulsion without vertigo, whereas only 7% without this lesion showed lateropulsion without vertigo (358).
In a study of 134 patients with isolated pontine infarctions, axial lateropulsion was the main presenting symptom in eight (6%) (360). All of the lesions in cases with lateropulsion were localized to the paramedian tegmentum just ventral to the fourth ventricle. All except one had contralesional lateropulsion. In two patients, axial lateropulsion was the sole clinical manifestation. The results suggest that axial lateropulsion probably results from damage to the graviceptive pathway ascending through the paramedian pontine tegmentum.
In a study of eight patients with isolated unilateral inferior cerebellar peduncular lesion at the pontine level, five patients had ipsiversive lateropulsion, and lateropulsion was not observed in three (81).
In a study of 220 patients consecutively admitted to a neurorehabilitation ward after a first hemisphere stroke, lateropulsion was frequent, especially after right hemisphere stroke, and it was almost always in right-handers; it affected about half on admission and a quarter on discharge (93).
The increased risk of disequilibrium and falls associated with aging is not due to aging of “the balance system” per se but to an increased likelihood of impairment or pathology in the various physiological subsystems underlying the complex skill of balancing (168; 166).
A systematic review of 22 studies comprising a total of 5125 patients found the prevalence of lateropulsion to be 41% after supratentorial stroke, although only 13% had severe lateropulsion ("pushers"), whereas the prevalence of lateropulsion was 83% after infratentorial stroke (92).
|
• There is no general approach to prevention of disequilibrium as it is a varied and multifactorial problem, and in particular there is no general means of primary prevention. | |
|
• Primary and secondary prevention do apply to specific circumstances of iatrogenic illness, which would encompass avoidance of vestibulotoxic drugs, and (when absolutely necessary) using them at appropriate dosages adjusted for renal function and with drug-level and neuro-otological monitoring. |
There are three levels of disease prevention: (1) primary prevention--trying to prevent the occurrence of disease; (2) secondary prevention--trying to detect disease early and prevent it from getting worse; and (3) tertiary prevention--trying to improve quality of life and reduce the symptoms and progression of extant disease. There is no general approach to prevention of disequilibrium as it is a varied and multifactorial problem, and in particular, there is no general means of primary prevention. Primary and secondary prevention do apply to specific circumstances of iatrogenic illness, which would encompass avoidance of vestibulotoxic drugs (eg, aminoglycosides) and, when absolutely necessary, using them at appropriate dosages adjusted for renal function and with drug-level and neuro-otological monitoring (21). Such considerations also apply to multiple drugs and drug combinations that can cause or exacerbate disequilibrium when used in the elderly or those with existing balance disorders. Tertiary prevention includes measures to minimize balance-related falls and falls with injury.
Except in cases of visual-vestibular mismatch, patients with sensory disequilibrium generally do worse in the dark and frequently have a Romberg sign on examination (217). Motor disequilibrium, as from cerebellar dysfunction, is generally not exacerbated in the dark or with the eyes closed.
Sensory disequilibrium may be due to proprioceptive impairment, balanced bilateral or compensated unilateral vestibular dysfunction, visual-vestibular mismatch (eg, due to impaired vision, ocular misalignment, or use of optic devices [ie, lens implants or new glasses]), or multisensory impairment (57). Both proprioceptive loss and bilateral vestibulopathy typically have a nondirectionally positive Romberg sign, but the two can be readily distinguished at the bedside. Proprioceptive impairment has impaired joint position sense and may have pseudoathetosis and a sensory drift but no oscillopsia or bilaterally positive head impulse test. In contrast, bilateral vestibulopathy has oscillopsia and a bilaterally positive head impulse test with preserved joint position sense and no pseudoathetosis or sensory drift. In addition, other bedside tests can be used to demonstrate an impaired vestibulo-ocular reflex in bilateral vestibulopathy (eg, impaired dynamic visual acuity with low-frequency head oscillations).
The differential diagnosis can also be approached by considering the direction bias of postural imbalance (eg, none, laterally, or backward). The absence of a direction bias is typical of sensory disequilibrium due to bilateral vestibular or proprioceptive impairment. Lateropulsion is typically seen with acute or subacute lateralizing disorders affecting the brainstem, cerebellum, or thalamus. Many afflictions can cause “backward disequilibrium” (retropulsion), including somatic conditions (eg, degenerative, ischemic, and traumatic brain lesions), psychosomatic conditions, and psychiatric disorders (eg, depression).
Another approach is to consider associated symptoms, although this gets complicated by an impossible-to-manage complexity of possible combinations and associations. Nevertheless, some combinations are worth remembering. For example, the triad of opsoclonus, myoclonus, and ataxia, mainly in a form of disequilibrium, is usually associated with infectious, postinfectious immune-mediated, or paraneoplastic processes (26).
Proprioceptive disequilibrium and a sensory ataxic gait can occur with sensory neuronopathy (ganglionopathy) or peripheral neuropathy (eg, diabetes). Causes of sensory neuronopathy are varied and include (1) tabes dorsalis (“locomotor ataxia”); (2) viral infections; (3) subacute combined degeneration (vitamin B12 deficiency) or copper deficiency; (4) paraneoplastic subacute sensory neuronopathy (eg, anti-Hu antibodies); (5) medication toxicity (cis-platinum, pyridoxine); (6) dysimmune disorders (eg, Sjögren syndrome, Miller Fisher syndrome, and Bickerstaff brainstem encephalitis); (7) celiac syndrome; (8) cerebellar ataxia, neuronopathy, and vestibular areflexia syndrome (CANVAS) (321; 95; 203).
A wide variety of disorders can produce bilateral vestibulopathy, including (1) viral infections (bilateral viral neurolabyrinthitis or “vestibular neuritis”); bilateral Meniere disease; (3) meningitis; (4) neurosypihilis; (5) superficial siderosis; (6) postinfectious and autoimmune disorders; (7) vestibulotoxic effects of pharmaceuticals (eg, aminoglycosides); (8) toxins (including lead); and (9) head injury (which can cause loss of vestibular sensory epithelium) (31; 153). Lead poisoning can worsen postural stability, by affecting both vestibular and proprioceptive inputs (37; 38).
Motor disequilibrium may be due either to mechanical factors (eg, severe arthritis or prosthetic limbs) or to dysfunction of central and peripheral nervous system motor pathways. The central motor pathways that may be affected in patients with motor disequilibrium include the pyramidal, extrapyramidal, and cerebellar systems whereas the peripheral motor pathways include the peripheral nerves, neuromuscular junctions, and muscles. Mass lesions, particularly involving the posterior fossa (eg, epidermoid tumor of the foramen magnum, posterior fossa arachnoid cysts) have been associated with disequilibrium, which is typically motor and may be fluctuating or static (102; 335).
The differential diagnosis can also be categorized by disease course. Acute disequilibrium may be caused by a wide range of conditions, including toxic or metabolic disorders (eg, alcohol intoxication, phenytoin toxicity, aminoglycoside toxicity, pyridoxine toxicity, idiosyncratic reactions to medications) (108), and central nervous system lesions (eg, thalamic or brainstem infarction). Chronic disequilibrium may also be caused by a wide range of conditions, including bilateral vestibulopathy, mal de debarquement syndrome, proprioceptive impairment, subcortical lesions involving motor pathways or association fibers, and various movement disorders (eg, spinocerebellar ataxias, progressive supranuclear palsy, Parkinson disease, etc.) (78). Episodic or waxing-and-waning disequilibrium in adults may be caused by episodic ataxia, toxic or metabolic disorders (eg, alcohol intoxication, phenytoin toxicity), and psychogenic disorders including phobic postural “vertigo” (316; 281; 78; 112).
|
• Diagnostic studies that may be helpful in patients with dysequilibrium vary greatly depending on the identified neurologic or mechanical deficits. | |
|
• The clinical value of neuroimaging for patients presenting to emergency rooms with disequilibrium-related dizziness is very low and appears to have declined over time. | |
|
• Posturography has been advocated as a potentially useful tool for evaluating the severity and nature of postural instability as well as the effects of pharmacologic and rehabilitative treatment. | |
|
• The utility of posturography lies in quantifying balance and in functionally defining different types of sensory deficits for use either in guiding rehabilitation or in monitoring recovery from a disease process. |
Diagnostic studies that may be helpful in patients with dysequilibrium vary greatly depending on the identified neurologic or mechanical deficits but may include electromyography and nerve conduction studies, cranial or spinal imaging, joint x-rays, somatosensory evoked potentials, and specific laboratory studies.
The clinical value of neuroimaging for patients presenting to emergency rooms with disequilibrium-related dizziness is very low and appears to have declined over time. Patients who are more likely to have abnormal findings on CT are those with severe headaches or some neurologic deficits in addition to disequilibrium-related dizziness, particularly among individuals over 60 years of age presenting with new-onset imbalance or disequilibrium or a history of recent head trauma, whereas those with isolated disequilibrium-related dizziness are very unlikely to have acute, life-threatening abnormalities (10; 76; 192; 262; 263; 306; 249; 09).
Posturography has been advocated as a potentially useful tool for evaluating the severity and nature of postural instability as well as the effects of pharmacologic and rehabilitative treatment (35). Modern posturography techniques allow assessment of vestibular contributions to postural stabilization by systematically eliminating or disrupting visual and proprioceptive inputs. The contribution of vision to postural stabilization can be quantified with posturography as the ratio of standing performance with eyes open and eyes closed, the so-called Romberg quotient. Unfortunately, modern forms of posturography have not been demonstrated to be particularly useful in distinguishing among different causes of imbalance or in localizing lesions. The utility of posturography lies in quantifying balance and in functionally defining different types of sensory deficits for use either in guiding rehabilitation or in monitoring recovery from a disease process.
|
• The treatment of disequilibrium varies by type and cause, but in general it is symptomatic and directed at the underlying cause. | |
|
• A major focus should be on fall and injury prevention, and maintenance of activity (especially walking) with appropriate assistance and precautions. | |
|
• Vestibular sedatives (ie, including antihistamine-anticholinergic such as meclizine and dimenhydrinate and benzodiazepines such as lorazepam and diazepam) are commonly used indiscriminately as purported treatments for “dizziness” and “vertigo,” without characterizing the dizziness carefully; these agents may alleviate true vertigo (especially acute persistent vertigo), but these agents may exacerbate disequilibrium and presyncope. | |
|
• Drugs should be reviewed in all patients with dizziness, including those presenting with disequilibrium. | |
|
• Some authors have reported that “vestibular rehabilitation is an effective method of therapy for many patients with disequilibrium and balance disorders and that for some patients it is the best therapy available,” but evidence supporting this statement is weak. |
The treatment of disequilibrium varies by type and cause. In general, it is symptomatic and directed at the underlying cause. A major focus should be on fall and injury prevention, including appropriate footwear (tie- or Velcro-closure flat-soled walking shoes, not slip-ons, sandals, cowboy boots, etc.), use of hip protectors (if tolerated; some find these cumbersome to put on and take off especially with urinary urgency), assistive devices (eg, cane, walker, wheelchair), modification of the home environment (lighting, handrails, grab bars, no-slip surfaces for bath and shower, shower chair, night lights en route to the bathroom, and removal of throw rugs, clutter, and other trip hazards), and maintenance of activity (especially walking) with appropriate assistance and precautions. In many institutions, physical therapists can help patients and caregivers learn to perform safe transfers and can make additional recommendations regarding gait training, and occupational therapists can perform an in-home safety evaluation.
Vestibular sedatives (ie, including antihistamine-anticholinergic such as meclizine and dimenhydrinate and benzodiazepines such as lorazepam and diazepam) are commonly used indiscriminately as purported treatments for “dizziness” and “vertigo,” without characterizing the dizziness carefully. These agents may alleviate true vertigo (especially acute persistent vertigo), but these agents may exacerbate disequilibrium and presyncope (207).
Drugs should be reviewed in all patients with dizziness, including those presenting with disequilibrium. Drugs associated with disequilibrium include alcohol and other central nervous system depressant medications (eg, benzodiazepines, barbiturates, phenothiazines), aminoglycoside antibiotics, anticonvulsants, antidepressant medications, antihypertensive medications (eg, angiotensin-converting enzyme inhibitors), chemotherapeutic agents, loop diuretics (eg, furosemide), and salicylates (42). Abrupt withdrawal of selective serotonin reuptake inhibitors may cause a sudden drop in serotonin in the vestibular nucleus complex bilaterally, causing a motor disequilibrium without vertigo (318). The elderly are particularly susceptible to drug ototoxicity because (1) they are more likely to receive ototoxic drugs; (2) they have less reserve (due to age-associated vestibular end-organ changes, preexisting sensorineural hearing loss, and previous treatment with ototoxic drugs); and (3) they are more likely to have impaired renal function.
Some authors have reported that “vestibular rehabilitation is an effective method of therapy for many patients with disequilibrium and balance disorders and that for some patients it is the best therapy available” (201), but evidence supporting this statement is weak. Patients with disequilibrium may benefit modestly from physical therapy (particularly for fall prevention and use of walking aids) but are unlikely to have significant benefit from typical “vestibular rehabilitation” exercises (207).
Other have advocated that poststroke balance and gait rehabilitation should incorporate techniques devoted to misorientation with respect to gravity given the prevalence of lateropulsion as an important contribution to altering poststroke balance and gait at the subacute stage (93). Most therapeutic studies of pusher syndrome have been anecdotal case reports (276).
Anecdotally, in a patient with pontine hemorrhage-associated sensory impairment of the extremities, standing and sit-to-stand or stand-to-sit training aimed at shifting the center of gravity and subjective postural vertical in the anterior direction may improve backward disequilibrium and correct tilt to the anterior direction (135). Case series and controlled trials will be needed before this can be accepted.
Patients with Parkinson disease may complain of unsteadiness and impaired balance not only when “off,” but also while “on,” even with levodopa-induced dyskinesia (12). Although postural instability responds poorly to dopaminergic medications (45; 67; 149; 252), it may respond to physical therapy approaches (312; 314; 313; 178; 70; 317; 195; 199; 303; 334), and also to unilateral pallidotomy (67) or deep-brain stimulation (19; 179; 195; 347). Exercise programs using incremental speed-dependent treadmill training can reduce postural instability and fear of falling and can also improve mobility (70). Rivastigmine may also improve certain elements of postural control in patients with Parkinson disease (240). In a meta-analysis, bilateral stimulation of the internal globus pallidus, bilateral stimulation of the subthalamic nucleus, and to a lesser extent, unilateral pallidotomy significantly improved postural instability and gait disability, more so during the “on” phase than during the “off” phase, though the overall effects are at best modest (19). Later trials cast doubt on the utility of subthalamic nucleus deep-brain stimulation for postural instability in patients with Parkinson disease, finding that subthalamic nucleus stimulation does not alleviate levodopa-resistant postural instability in Parkinson disease (341). A small trial found that low-frequency stimulation of the pedunculopontine nucleus area helped alleviate step length, speed of walking, and quality of life (347; 343).
Sensory disequilibrium (eg, bilateral vestibulopathy or sensory neuronopathy) may recover to some extent in mild cases but is usually chronic and persists indefinitely (87; 88; 89; 83; 84; 215). Nevertheless, affected patients may learn to make compensatory changes in behavior that allow them to continue in many activities. For example, with neuropathy associated with pyridoxine toxicity, complete recovery may occur in patients with a mild involvement who have been taking only low doses of the vitamin (186); the sensory neuronopathy caused by pyridoxine overdose shows little improvement.
Outcomes for motor disequilibrium vary considerably as a function of the underlying etiology.
The general pattern of balance in healthy pregnant women is similar to nulligravidae (355). Moreover, the base width is wider in late pregnancy, and the center of pressure moves more medially and less interiorly to maximize stability (229). During the third trimester, anteroposterior and mediolateral sway is significantly higher than in nonpregnant women (172).
Pregnant women are susceptible to a wide range of potential illnesses that can cause balance disorders. Sometimes prolonged bed rest is needed for a pregnant woman, and this can result in significant deconditioning and nonspecific lightheadedness and disequilibrium that can last into the postpartum period if the patient is not educated to start walking and exercising again. This is transient and resolves with vestibular and regular physical therapy. This has been replicated in normal patients in whom three weeks of bed rest resulted in postural sway (270).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
General Neurology
Dec. 30, 2024
Neuro-Oncology
Dec. 13, 2024
General Neurology
Dec. 13, 2024
General Neurology
Dec. 13, 2024