





Neuromuscular Disorders
Neurogenetics and genetic and genomic testing
Dec. 09, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author discusses the EEG findings in encephalopathic states, both acute and chronic. Encephalopathy is characterized clinically by a generalized alteration of attention, consciousness, or cognition. Acute encephalopathies range from delirium to coma. In the chronic, static, or slowly progressive encephalopathies there may be maintenance of attention initially, but there is loss of cognitive functions as seen in dementia. Electroencephalography (EEG) plays a significant role in the evaluation of patients with acute encephalopathy. Most importantly, EEG can differentiate between a true acute encephalopathy and epileptic states or psychiatric conditions. Although EEG is very sensitive in detecting an acute encephalopathy, it is not usually etiologically specific. The usefulness of EEG in chronic encephalopathy is less clear. Studies are beginning to appear about inter-rater reliability in the EEG literature and have bearing on one of the patterns often seen in encephalopathic states.
|
• The EEG hallmark of most acute encephalopathies is background slowing. | |
|
• The severity of slowing typically corresponds to the degree of impairment. | |
|
• EEG findings of encephalopathies are typically of nonspecific etiology. |
Electroencephalography (EEG) has been used to assess cerebral dysfunction for more than 70 years. The EEG is very sensitive to changes in the function of the cerebral cortex. Encephalopathy refers to global cerebral dysfunction, which manifests itself as slowing of activity in the cortex. This slowing may be due to dysfunction of the cortical neurons themselves or a reflection of abnormalities in the subcortical gray matter or white matter. EEG has long been used as an objective means of assessing the degree of cerebral dysfunction. In general, it does not help to reveal the etiology of the encephalopathy.
The first reference to the diffuse slowing seen in encephalopathic states appears to have been in a paper by Gibbs and colleagues published in 1935 (24). In 1936, an article by Davis was published and included mention of this issue (13). An article was published in 1937 that looked at encephalopathy caused by medication (23). Hoagland published another article on this topic in 1937 (27). Over the years since then, numerous articles have been published looking at EEG changes in a variety of encephalopathies of different etiologies.
There has been a lot of interest in the current version of Critical Care EEG terminology, and it is being used in many institutions (26). When discussing some of the EEG terms, I will also include the description in terms of how it would look like in the EEG terminology, when applicable.
The EEG is performed using metallic disk electrodes affixed to the scalp in a standard arrangement called the International 10-20 system. Electrodes cover the superficial regions of the frontal, temporal, parietal, and occipital lobes. Current recordings are obtained using digital systems that allow post hoc change for the gain and filter settings and the electrode chain montages. The montages are different ways of connecting the electrodes so that different spatial characteristics can be seen. There are bipolar montages, such as the longitudinal (double banana), the transverse, and referential montages in which the scalp electrodes are connected to a reference point, such as the ipsilateral ear.
The normal frequencies seen in an EEG vary with age. In children older than 8 years of age and in adults, there should be a posterior dominant rhythm (alpha rhythm) of at least 8.5 Hz. During wakefulness, small of amounts of theta (4 to 8 Hz) and beta (above 13 Hz) activity are seen more anteriorly. Drowsiness may produce slowing or loss of the posterior dominant rhythm as well as increasingly greater amounts of theta activity. It is important to differentiate between drowsiness and pathological slowing. This can be accomplished by using alerting stimuli such as asking the patient to count or, if necessary, using noxious stimuli. Children younger than 8 years of age may have significantly lower background frequencies and still be completely normal. Greater than anticipated amounts of theta or beta activity, or any delta activity (below 4 Hz), in a fully alert patient indicates an encephalopathy.
The purpose of obtaining an EEG is to assess cerebral function. Although EEG does not have the spatial resolution of an MRI, it has the advantage of being able to capture brain function with temporal resolution in the millisecond range. It can also assess changes in brain function over time and in response to stimuli. In encephalopathy, the EEG is used to assess the severity of the condition and the distribution of the functional abnormality and to differentiate it from status epilepticus or a psychiatric disorder.
The evaluation of altered mental status and of seizures is the main indication for an EEG.
There are no contraindications for EEG.
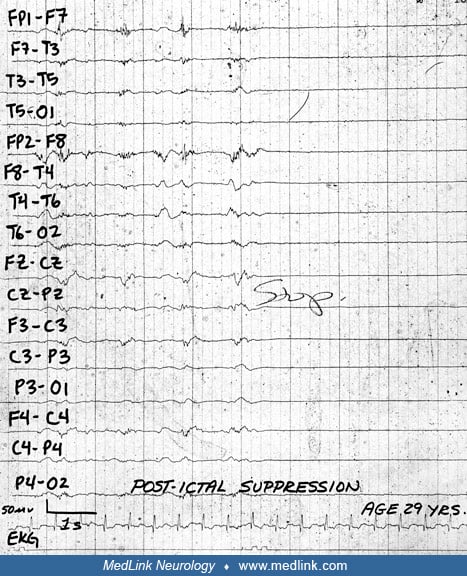
The EEG hallmark of acute encephalopathy is slowing of the background frequencies. The severity of the slowing correlates with the degree of impairment of attention (52). Mild confusion may be accompanied only by slowing of the posterior dominant rhythm and decreased amounts of beta activity. Typical examples of patients with acute encephalopathies but normal EEGs include patients with mild systemic infections (particularly seen in the elderly), patients experiencing medication or illicit drug side effects, post-concussion patients, patients in the postictal state, younger patients with meningoencephalitis, and patients with psychogenic disease (34). As the encephalopathy worsens, theta activity progressively increases as does the amount of delta activity. The theta and delta activity may be continuous or intermittent. Predominantly delta activity is seen in patients who are unresponsive (comatose).
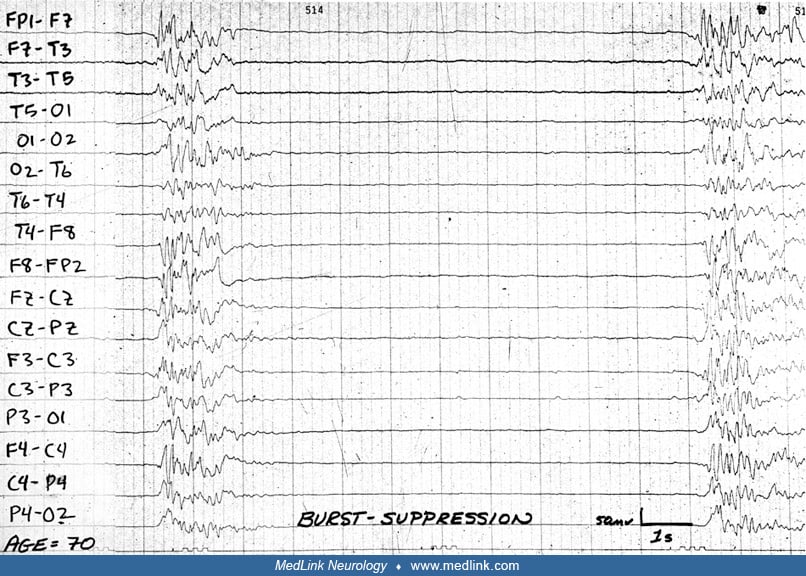
The frequencies continue to slow as the coma deepens. Spontaneous changes in the EEG background and EEG reactivity are lost in deep coma. As the severity increases, the EEG becomes discontinuous (burst-suppression pattern) and then flat (electrocerebral silence or inactivity).
The exception to the slowing would be in cases of mild intoxication with a sedative-hypnotic, such as a barbiturate or benzodiazepine where an increased amount of beta activity is seen before any slowing is noted.
Chronic encephalopathies, such as dementias, often are associated with normal EEGs until relatively late in the course of the disease. The loss of ability to attend seems to correlate best with the degree of slowing. There is some debate as to how much slowing can be considered normal in the elderly with no signs of dementia.
Unfortunately, EEG patterns rarely are truly pathognomonic for any specific cause of encephalopathy, but some may be suggestive of an etiology. One exception is the chronic encephalopathy of subacute sclerosing panencephalitis (see below).
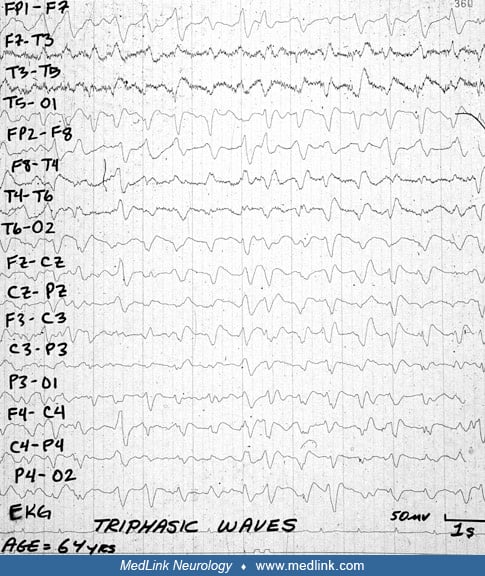
Triphasic waves. Triphasic waves were first described in 1950 as blunted spike and wave (19). They were later described as a main deflection downward preceded and followed by a lower amplitude upward deflection giving rise to a triphasic contour (04).
These waves can also be characterized as sharpest, deepest, and longest. They most commonly occur at 1.5 to 2.5 Hz, and a frontal-occipital lag can sometimes be present. Triphasic waves are suggestive, but not diagnostic, of a metabolic cause of an encephalopathy (17). They were initially thought to be indicative of hepatic failure, but this is no longer believed to be true (18). A study of 50 patients with triphasic waves (half retrospective and half prospective) showed etiologies as follows: hepatic (56%), renal failure (20%), anoxia (18%), hyper-/hypoglycemia (4%), hyperosmolality due to respiratory failure (2%). A more comprehensive differential might include electrolyte abnormalities, baclofen, lithium, pregabalin, cefepime, aztreonam, ifosfamide toxicities, CNS infection, or even mild infections of the upper respiratory or urinary tract (33). The anoxic cases included cardiac arrest (including arrest after stroke) and respiratory failure (35). Almost any cause of stupor or coma can be associated with triphasic waves, including structural lesions. Nonetheless, triphasic waves are most commonly seen in metabolic encephalopathies. This pattern can sometimes be confusing, because it can respond to benzodiazepines or antiseizure medications in about one third of cases (46). Data suggest that there is substantial disagreement as to the EEG appearance of triphasic waves (20). Given this disagreement, it may be prudent to both name and describe the pattern seen on the EEG. In the critical care ICU terminology, there are different descriptions possible for triphasic waves. When the triphasic waves are separated by relative or diffuse attenuation, as they most commonly occur, it would be described as generalized periodic discharges (GPDs) with triphasic morphology. Less frequently, triphasic waves appear as one wave immediately following another. In this case, they would be described as generalized rhythmic delta activity (GRDA). GRDA is not allowed to include a triphasic morphology as a descriptor, so would include anterior-posterior lag descriptor (if it were present).
Rhythmic Delta Activity (RDA). RDA is high amplitude, intermittent, 2 to 3 Hz semirhythmic activity that often has anterior prominence, and is qualified as such when this occurs.
In one study of 36 cases of RDA, there was only a single case of metabolic encephalopathy; there were seven infectious encephalopathies, six drug related encephalopathies, and four tumors, four cerebral lesions, and four epileptic cases (01). In a cohort of 154 hospitalized patients with acute encephalopathy, the presence of FIRDA may be associated with a Glasgow outcome score of one to three in patients after stroke, and liver failure, but may be associated with worse prognosis with renal insufficiency (statistical significance not sustained after Bonferonni correction of multiple comparisons) (62). In children, RDA with a posterior predominance is more frequently seen.
OIRDA is most frequently seen in children with absence epilepsy. Using critical care terminology, these would be described as rhythmic delta activity with frontal predominance (for FIRDA) and occipital predominance (for OIRDA).
Alpha coma and spindle coma. Alpha coma and spindle coma are characterized by nonreactive diffuse alpha or sleep spindle-like activity (approximately 14 Hz) (37; 08; 49). These patterns are most commonly seen in severe encephalopathies after an anoxic injury or severe poisoning.
The prognostic significance seems to be related to etiology. In one report that combined many studies, there were 10 survivors of 86 patients after cardiopulmonary arrest, but seven of eight survivors after respiratory arrest (29).
Lateralized periodic discharges (LPDs). Previously termed periodic lateralized epileptiform discharges (PLEDs), lateralized periodic discharges usually indicate a subacute structural lesion (28). The most common cause is stroke, which in one series occurred in 53% of patients with lateralized periodic discharges (47). Lateralized periodic discharges are indicated by semirhythmic epileptiform patterns (spikes or sharp waves or complexes) that usually occur at a frequency between 1 and 3 Hz.
Whether lateralized periodic discharges are an ictal rhythm is debated, but their greater prevalence in patients who have seizures reactive to a subacute cerebral injury is more universally accepted. There is a retrospective series of 90 patients with lateralized periodic discharges, in 10 of whom lateralized periodic discharges represented an ictal rhythm (56). There is another case series of 10 patients, which correctly identified those who had seizures and those who did not by the finding of restricted diffusion on brain MRI (43).
Bilateral independent periodic discharges (BIPDs). Bilateral independent periodic discharges are simply lateralized periodic discharges that occur independently in each cerebral hemisphere. Eighteen patients with bilateral independent periodic discharges were compared to 45 patients with lateralized periodic discharges, and there was higher mortality in the bilateral independent periodic discharge group (61% vs. 29%) (14).
Generalized periodic discharges (GPDs). Generalized periodic discharges are indicative of a severe, diffuse cerebral dysfunction such as that which may be seen after an anoxic brain injury. Although there is a need for replication, it may be that generalized periodic discharges consistent with electrographic status epilepticus evolving out of a discontinuous background are a poor prognostic sign in patients with post anoxic encephalopathy (0 out of 14 patients had good outcome in one study) (50).
Burst suppression. Burst suppression is a pattern consisting of periods (bursts) of activity and periods of suppression or inactivity. The periods of activity may or may not have epileptiform discharges in them. As the situation worsens, the bursts of activity shorten and the intervals of suppression lengthen (10).
Electrocerebral inactivity (silence). Electrocerebral inactivity (silence) is defined as the lack of any cerebral electrical potentials that are greater than 2 mcV in amplitude. In the presence of a known, irreversible cause, this is the EEG pattern associated with brain death. When diagnosing brain death, the EEG needs to be recorded according to specific guidelines (02) The ACNS criteria include double-distance electrode placement, checking each electrode during the recording, sensitivity set to 2mcV, and at least 30 minutes recording duration.
COVID-19. There were three meta-analyses of EEG abnormalities of generalized patients withs with COVID-19 infection (03; 51; 36). Each found a high rate of diffuse slowing. One found that the slowing affected the posterior dominant rhythm (51), and two meta-analyses found that about 10% did not have a discernible posterior dominion rhythm (03; 51). The rate of status epileptics was less than 6% in all three meta-analyses. This contrasts with a case series of critically ill patients, which found two of five had status epilepticus, and one of five had status myoclonus. A cohort of patents, half of which were in the ICU, were followed (54). In this cohort, more than 90% of acute EEG had low amplitude background. More than half had intermittent focal, rhythmic activity. Follow-up recordings only infrequently were suppressed (about 20%). These data need to be replicated, as this was not described in any of the three preceding metaanalyses.
CNS infections. Infections of the CNS, such as meningitis, encephalitis, or meningoencephalitis, may also cause both diffuse and focal EEG abnormalities. The abnormalities may consist of diffuse or focal slowing, focal or generalized epileptiform discharged, or both. Classically, herpes simplex encephalitis is associated with lateralized periodic discharges at a frequency of 1 to 2 Hz (65).
Hepatic encephalopathy. Hepatic encephalopathy is seen in liver insufficiency or failure from any cause. Regardless of the cause, the EEG initially shows slowing and later may show triphasic waves. Triphasic waves were originally thought to be specific for hepatic encephalopathy, but this is not the case (04; 18). The Triphasic Wave pattern is now subsumed into the generalized periodic discharge category. The triphasic waves occur at a relatively deep stage of obtundation. In deep coma, the triphasic waves disappear and are replaced by diffuse delta slowing.
Hypercalcemia. Hypercalcemia causes slowing and can cause spikes and biphasic waves (32).
Hyperglycemia. Hyperglycemia, like hypoglycemia, produces diffuse slowing. At extreme levels, it may cause epileptiform discharges and seizures.
Hypernatremia. Hypernatremia is associated with generalized high voltage slow activity (22).
Hypocalcemia. Hypocalcemia produces progressive slowing of the EEG and at very low levels may produce generalized bursts of spike activity (44). Hypocalcemia produces progressive slowing of the EEG and at very low levels may produce generalized bursts of spike activity (44). There is a case report of exaggerated photomyoclonic response associated with hypocalcemia (40).
Hypercalcemia. Hypercalcemia also causes slowing and can cause spikes as well as triphasic waves (32).
Hypoglycemia. Hypoglycemia causes progressive slowing of the background as well as loss of faster frequencies (57), and at extreme levels or after a rapid fall may produce seizures.
Hyponatremia. Hyponatremia is characterized on EEG by progressive slowing of the background from theta to delta frequencies as the sodium concentration decreases (67). However, the sodium concentration does not cause slowing as much as the rate of its decrease.
Hypothyroidism. Hypothyroidism is associated with progressive slowing of the background and a low-amplitude record. Triphasic waves and periodic complexes have been reported.
Hypoxic (anoxic)-ischemic injury. Hypoxic (anoxic)-ischemic injury manifests across a spectrum from mild slowing to an isoelectric EEG, depending on the severity of the brain injury. Severe slowing and a lack of reactivity are often signs of a poor prognosis in this setting. Theta, unreactive alpha, or spindle comas are, likewise, typically indicators of a poor prognosis for recovery of meaningful consciousness. Burst suppression, alternating periods of activity, and electrocerebral inactivity can be signs of a grim prognosis. Pathologically, using the SEND classification of severe hypoxic ischemic encephalopathy after cardiac arrest, 24 of 25 patients with either suppressed EEG or burst-suppression EEG had severe hypoxic ischemic encephalopathy (15).
Hyperthyroidism. Hyperthyroidism produces an increase of the frequency of the posterior dominant rhythm, but thyroid storm may cause diffuse slowing, which has been rarely reported to be bitemporal (58).
Hashimoto encephalopathy. Hashimoto encephalopathy, an autoimmune thyroiditis, has caused severe diffuse slowing as well as triphasic waves (59).
Pancreatitis. Pancreatitis can also cause EEG changes, such as bilateral theta activity and intermittent delta activity (06).
Posterior reversible encephalopathy syndrome (PRES). About 80% to 90% will have some sort of abnormal EEG, the most common abnormal pattern is generalized or background slowing (42). Those with focality do not always correspond to areas of MRI changes (30).
Renal encephalopathy. Renal encephalopathy presents on EEG much like hepatic encephalopathy except that epileptiform discharges may or may not be associated with clinical seizures (44).
Trauma. Trauma can cause both diffuse and focal abnormalities. The diffuse slowing seen is due to diffuse axonal injury whereas the focal slowing or epileptiform discharges result from injuries such as contusions or hemorrhages. Severe head injury may manifest as theta, alpha, or spindle coma, burst suppression, and an isoelectric EEG.
CNS infections. Infections of the CNS, such as meningitis, encephalitis, or meningoencephalitis, may also cause both diffuse and focal EEG abnormalities. The abnormalities may consist of diffuse or focal slowing, or focal or generalized epileptiform discharges, or both. Classically, herpes simplex encephalitis is associated with PLEDs, usually with a frequency of 1 to 2 Hz (65).
COVID-19. There were three metaanalyses of EEG abnormalities of generalized patients with COVID-19 infection (03; 51; 36). They found a high rate of diffuse slowing. One found that the slowing rarely affected the posterior dominant rhythm (51), and two metaanalyses found that about 10% were found without a posterior dominant rhythm (03; 51). The rate of status epilepticus was less than 6% in all three studies. This contrasts with a two of five patients with status epilepticus and another with status myoclonus, among five critically ill patients (11).
Alzheimer disease. Alzheimer disease has a nearly normal EEG in the early stages. As the disease progresses, more and more diffuse theta and then delta slowing is seen (12). Pathological slowing is not seen as part of the normal aging process. There may be some relative slowing of the background as age increases but not beyond the normal range for an adult (21). There is ongoing work looking at the use of EEG to help in the diagnosis and progression of Alzheimer disease, but a lack of agreement of the more than100 published articles on approaches and results limits their clinical use (09). One exciting development was revealed in a study that followed patients with prodromal dementia (66). They found that none of the patients who had FIRDA went on to develop Alzheimer disease. Given the many conflicting papers and the moderately high risk of bias of the paper, this result should be considered as only a possible correlation until replication.
Lewy body dementia. As noted in a class III paper by AAN’s risk of bias, 22% of patients with mild cognitive impairment who go on to develop Lewy body dementia or had an abnormal 123I-PF-SPECT scan will have FIRDA (66).
Vascular dementia. Vascular dementia may be of either the multi-infarct type or the Binswanger (microvascular) type. A combination of diffuse slowing and focal slowing are seen in multi-infarct dementia. Binswanger-type dementia is characterized by diffuse slowing.
Pick disease. EEG in Pick disease may appear normal to visual inspection, but computerized analysis may show subtle slowing (07).
Parkinson disease. EEG in Parkinson disease is normal in 48% to 64% of the patients (16; 70). The most common abnormality in the other patients consisted of mild diffuse slowing. This slowing may be correlated with cognitive impairment (41).
Huntington disease. Huntington disease produces a low-amplitude EEG (38). There may be differences in quantitative EEG between Huntington disease patients and normal controls (48), but the author of this article would recommend confirmation of these findings by a second study before implementing clinically.
Subacute sclerosing panencephalitis (SSPE). Subacute sclerosing panencephalitis is classically associated with periodic complexes that are very stereotyped and occur once every 5 to 7 seconds. The complexes consist of very high amplitude delta activity in which epileptiform discharges may be embedded (39).
Creutzfeldt-Jakob disease. Creutzfeldt-Jakob disease (CJD) manifests itself on the EEG with diffuse slowing, FIRDA, and periodic complexes. The periodic complexes are more frequent than those seen in SSPE, usually about once per second (25). The complexes contain stereotyped sharp and slow waves. These complexes may be unilateral initially and progress to be bilateral over weeks to months. The complexes do not seem to occur in variant Creutzfeldt-Jakob disease (69), although there are two cases that challenge this observation (05; 45). The series of 11 cases from Peru had seven patients with the 1 to 2 Hz periodic complexes (64), suggesting possibly that not all patients with Creutzfeldt-Jakob disease have periodic complexes.
There are only rare adverse effects, although the adhesive used for longer-term recordings is a frequent cause of hair loss. Activation methods typically used like photic stimulation and hyperventilation can rarely precipitate generalized tonic-clonic seizures (photic stimulation 0.04%, hyperventilation 0.03%) (68; 31). In people with epilepsy, the risk of seizures depends on the series but ranges from 0.5% to 3% with hyperventilation (63).
No specific EEG finding is sufficient to independently determine the prognosis. The etiology is crucial in determining the prognosis. Causes that are reversible, such as drug intoxication or hypothermia, have a better prognosis than those that are irreversible, such as anoxic brain injury. Even the worst patterns such as burst suppression or an isoelectric EEG can be associated with a good prognosis if due to a reversible cause, such as general anesthesia. With an irreversible cause, spindle or alpha coma, low-and-slow activity, burst suppression, or an isoelectric EEG portend a poor outcome. Another factor with bearing on the prognosis is whether or not there are spontaneous changes in the background over time or following stimulation. Reactivity is a relatively good prognostic sign. The lack of reactivity, conversely, is a poor prognostic sign with a relative risk of 3.7 (95% confidence interval 2.0 to 6.9) of death for both nonhypoxic (61) and hypoxic patients. In one series, lack of reactivity yields 98% positive predictive value of unfavorable outcome in hypoxic encephalopathy. The presence of spindles (rather than spindle coma) also seem to be a relatively good prognostic sign (53), although a more modern examination only found K-complexes to be prognostic indication of higher chance of good outcome (60).
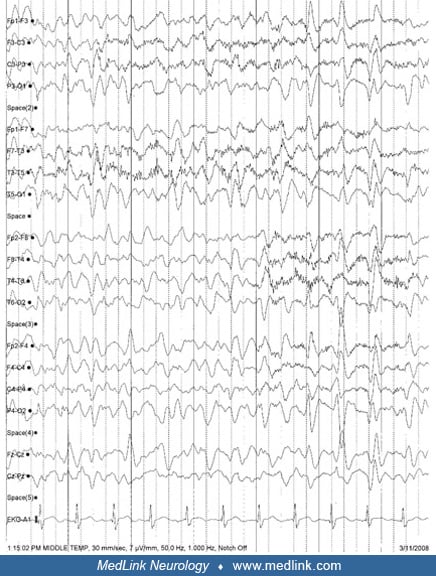
The patient was a 64-year-old man who had undergone chemotherapy with melphalan and then total-body radiation prior to autologous stem cell transfusion for multiple myeloma. He was noted to have an altered mental status about two weeks later. His Glasgow Coma Score was 2/2/4 = 8. Neurologic examination showed no abnormalities other than the altered mental status. The patient was febrile, but no source of infection was found despite pan-culturing that included cerebrospinal fluid. Liver enzymes, ammonia, sodium, calcium, and magnesium were normal. MRI of the brain was also normal. The EEG showed moderate (mixed theta and delta activity) slowing and triphasic waves.
The EEG was reactive to noxious stimulation. The EEG confirmed the encephalopathy and excluded depression or other non-neurologic cause for the mental status abnormality. The patient recovered. No follow-up EEG was performed.
The EEG records the electrical potential differences between different sites on the scalp, not the absolute voltage. As the electrical potentials change over time, the EEG records these changes as waves. The electrical potentials are the summation of the excitatory and inhibitory postsynaptic potentials in the underlying cortex. This activity reflects the ongoing cortical activity as it happens. Encephalopathy is associated with generalized slowing due to disruption of the normal thalamocortical circuits. This may be due either to dysfunction of the white matter connections to the cortex or dysfunction of the cortical neurons themselves.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
David Gloss MD
Dr. Gloss of The NeuroMedical Center in Baton Rouge has no relevant financial relationships to disclose.
See Profile
John M Stern MD
Dr. Stern, Director of the Epilepsy Clinical Program at the University of California in Los Angeles, received honorariums from Ceribell, Jazz, LivaNova, Neurelis, SK Life Sciences, Sunovian, and UCB Pharma as advisor and/or lecturer.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuromuscular Disorders
Dec. 09, 2024
General Neurology
Dec. 09, 2024
Neuro-Oncology
Dec. 05, 2024
Epilepsy & Seizures
Dec. 03, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 24, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Epilepsy & Seizures
Nov. 11, 2024