


Stroke & Vascular Disorders
Neoplastic and infectious aneurysms
Dec. 29, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Nonsaccular intracranial aneurysms, including fusiform and dolichoectatic intracranial aneurysms, can occur in any of the intracranial arteries but are particularly prevalent in the vertebrobasilar and internal carotid arteries. They can be detected incidentally or present with neurologic complications, including ischemic stroke, intracranial hemorrhage, or compression of surrounding neural structures. Treatment of these life-threatening aneurysms is challenging and requires individualized approaches and careful judgement. Surgical approaches are sometimes feasible. Increasingly, novel endovascular techniques, including placement of flow-diverting stents and stent-assisted coiling, can successfully treat these aneurysms.
|
• Fusiform (nonsaccular) aneurysms are elongated dilations of intracranial arteries lacking a distinct neck. Dolichoectasia can be used as interchangeable term but can also describe a less severe spectrum of arterial dilation or tortuosity. Fusiform and dolichoectatic aneurysms can occur sporadically, or in association with atherosclerosis, arteritis, connective tissue disorders, and underlying hereditary conditions. | |
|
• The abnormal dilation of the blood vessel results from the fragmentation of the internal elastic lamina, atrophy of the smooth muscle layer, and connective tissue hyalinization. | |
|
• Fusiform and dolichoectatic aneurysms can present with ischemic strokes, intracranial hemorrhage, or symptoms related to compression of cranial nerves or brain structures, but they are also often asymptomatic and detected incidentally. | |
|
• Management of these aneurysms is challenging, but individualized surgical and endovascular approaches, selectively applied to symptomatic or larger aneurysms, can be effective in preventing growth or rupture. | |
|
• Application of advanced endovascular techniques, including flow-directing stents and stent-assisted coiling, has increasingly allowed successful treatment of complex nonsaccular aneurysms. |
The first description of abnormal elongated and dilated intracranial vessels is attributed to the Italian anatomist Giovanni Battista Morgagni in his text “De sedibus, et causis morborum per anatomen indagatis libri quinque” in 1761 (34). Before the introduction of cerebral angiography and modern imaging techniques, autopsy studies provided the main source of information about intracranial aneurysms (23). Moniz provided the first angiographic demonstration of a dolichoectatic aneurysm in 1934, but Dandy had previously described the clinical condition in 11 instances in the vertebrobasilar circulation and in six instances in the internal carotid artery circulation (33; 10).
An aneurysm is a pathologic, localized blood vessel dilatation, which is called “saccular” when the inflow and outflow points are in common and “nonsaccular” when arterial dilatation is greater than 1.5 times normal without a clearly defined neck (ie, the inflow and outflow points are longitudinally separate) (15). “Fusiform” (from Latin fusus, for spindle) aneurysm is a morphological term utilized for the nonsaccular type that denotes a circumferential ballooning of the vessel for a short segment, often with a spindle shape. “Dolichoectasia” comes from the Greek dolikhos meaning long and ektasis meaning distention of a tubular structure. Intracranial arterial dolichoectasia describes the presence of at least one ectatic or tortuous artery in the cerebral vasculature, usually with a uniform enlarged circumference (41). Conceptually, the terms fusiform aneurysm and dolichoectasia overlap, and some authors use them interchangeably, but important differences in their clinical features and morphology can be distinguished. A third subtype, “transitional,” has been proposed, which features focal circumferential dilatation, elongation, and displacement.
Classically, two forms of nonsaccular aneurysms are separated by their pathophysiology: (1) acute dissecting and (2) chronic fusiform or dolichoectatic aneurysms (35). Acute dissecting aneurysms will not be addressed in this article.
Additional names for nonsaccular intracranial aneurysm include basilar ectasia, S-shaped aneurysm, wandering basilar artery, tortuous basilar artery, cirsoid aneurysm, megadolichovascular malformation, megadolichobasilar artery, dolichomegavertebralis anomaly, and aneurysmal malformation (15). Aneurysms greater than 2.5 cm in diameter are referred to as "giant" (20). When a giant aneurysm partially thromboses, leaving tortuous vascular channels, it is called a “giant serpentine” aneurysm. In the past, the term “atherosclerotic aneurysm” was often applied to these vascular malformations; however, the cause-effect relationship between underlying atherosclerosis and dolichoectatic aneurysms remains to be elucidated, and the term should be applied with caution. Notably, the trend in study of dolichoectatic and fusiform aneurysms focuses on dilatation as the main pathologic feature, and consequently, the term “dilatative arteriopathy” has gained currency (27).
|
• Fusiform aneurysms commonly affect the vertebrobasilar and internal carotid arteries. | |
|
• Fusiform and dolichoectatic aneurysms can present with headache, cerebral ischemia, or hemorrhage but are often discovered incidentally. | |
|
• Large aneurysms can present with compression of cranial nerves or the brain. |
Intracranial nonsaccular aneurysms occur in both the vertebrobasilar and internal carotid artery circulations. Although generally thought to be more frequent in the former, the series of Anson and colleagues suggests that both circulations are affected approximately equally, fusiform aneurysms being more common in the internal carotid and middle cerebral artery distributions, and dolichoectatic aneurysms more common in the vertebrobasilar distribution (01). These aneurysms occur more commonly in elderly adults, with a markedly increased frequency in men in the vertebrobasilar circulation and a slight preponderance for women in the internal carotid artery circulation. Giant fusiform aneurysms occur less frequently in the anterior circulation (20%) than in the posterior circulation (80%) where the basilar trunk and posterior cerebral arteries are most frequently involved (13). Occasionally, multiple fusiform intracranial aneurysms or a combination of saccular and fusiform aneurysms occur in the same person (01).
Clinically, fusiform or dolichoectatic aneurysms may present with headache or other symptoms related to compression of adjacent brain structures, with infarction or transient ischemic attacks, or with rupture and hemorrhage. Often, however, they are discovered incidentally. Specific symptoms depend on aneurysm location.
Headache is a common symptom of large fusiform aneurysms. The pain is often severe, lateralized to the side of the aneurysm, occipital with basilar artery aneurysms, retro-orbital or frontal with internal carotid artery aneurysms, and may antedate other neurologic symptoms by days or months. Sometimes the headache is positional. The mechanism of the headache is generally attributed to traction on nearby pain-producing structures and can be relieved by surgically separating the aneurysm from these tissues. Nausea, vomiting, and neck stiffness strongly suggest subarachnoid hemorrhage.
Cerebral ischemia can occur due to abnormal antegrade laminar blood flow predisposing to thrombosis and embolism, or by occlusion of branch vessels due to stretching and obliteration of arteries arising from the vascular anomaly. The association between dilatative arteriopathy and imaging markers of global cerebral small vessel disease suggests that occlusion of small perforating vessels not limited to the affected artery is also an important cause of ischemic stroke in these patients (43; 12; 55). On the other hand, tandem atherosclerotic stenotic lesions sometimes coexist with fusiform aneurysms and can be responsible for symptoms. In a pooled analysis of patients with vertebrobasilar dolichoectasia, ischemic stroke was the most common presenting symptom, and the 5-year risk for developing ischemic complications was 18% for infarction and 10% for transient ischemic attacks (59). Large aneurysms frequently have intraluminal thrombus seen either on MRI or at surgery. Such a thrombus can propagate, occlude penetrating vessels (especially those originating from the basilar artery), and result in brainstem strokes (01). Rarely, the entire basilar artery may thrombose, leading to massive brainstem ischemia that can result in a locked-in syndrome or sudden death (51).
Hemorrhagic complications of fusiform and dolichoectatic aneurysms are not as uncommon as previously believed and carry a high mortality rate. Bleeding may occur in the subarachnoid space or the parenchyma. The prospective risk of rupture has been estimated to be 0.9% to 2.3% per year (15). Factors strongly associated with aneurysmal rupture include female gender, hypertension, aneurysmal enlargement, diameter greater than 10 mm and transitional type morphology (15; 39). The use of antiplatelets and anticoagulants require cautious consideration as hemorrhagic events are frequently preceded by symptoms secondary to thrombi formation and ischemia (52).
Compression of adjacent structures, particularly the cranial nerves or the brainstem, is the cause of symptoms in about one third of the symptomatic cases (01; 59). Single or combined cranial nerve deficits can result from a tortuous dolichoectatic basilar artery or frank aneurysmal dilatation (51; 41). The facial nerve is commonly affected and may manifest with hemifacial spasm, facial paralysis, or both. Compression of the trigeminal nerve producing trigeminal neuralgia is also often reported in the literature and can be effectively treated with microvascular decompression. Involvement of the oculomotor nerves (III, IV, or VI) will manifest with ophthalmoplegia, diplopia, or pupillary abnormalities. Infrequently, cranial nerves VIII, IX, X, XI, and XII are affected, either singly or in combination, together with long-tract findings.
Either aneurysmal dilation of the supraclinoid segment of the internal carotid artery, or an elongated basilar artery in which the bifurcation occurs above the suprasellar cistern, may affect the anterior visual pathway by mass effect. This can manifest as a progressive compressive optic, bitemporal hemianopsia due to chiasmal compression, homonymous hemianopsia due to injury of the optic tract, or even as a Foster-Kennedy syndrome. These compressive symptoms are usually both insidious and progressive. In rare instances, aneurysms of the cavernous carotid artery rupture into the sphenoid sinus and present as recurrent epistaxis.
An aneurysmal basilar artery can compress the brainstem, resulting in pontomedullary and cerebellar signs including downbeat nystagmus and internuclear ophthalmoplegia mimicking a posterior fossa mass lesion. Oculopalatal tremor has also been described due to compression of the medulla along the Guillain and Mollaret triangle (57). Motor weakness without sensory signs is frequent. Dysphagia, hiccups, and orthostatic hypotension occur infrequently. Rarely, obstructive hydrocephalus is present. The mechanism of hydrocephalus can be divided into “obstructive-visible” when the dolichoectatic aneurysm is compressing either the foramen of Monro, cerebral aqueduct, or the third ventricle, or “obstructive-invisible” when a “water hammer” effect is generated by the pulsatile blood flow of the dolichoectatic artery over the floor of the third ventricle, impairing normal flow of the CSF (14).
|
• Fusiform and dolichoectatic aneurysms carry substantial risks of ischemic stroke. | |
|
• Aneurysm growth can produce brainstem compression. | |
|
• Aneurysmal rupture can produce fatal hemorrhage. |
Fusiform and dolichoectatic aneurysms can be discovered incidentally and remain asymptomatic over time, or can become complicated by cerebral ischemia, compressive symptoms, hemorrhage, or death. The prognosis and rate of complications in patients with nonsaccular aneurysms and intracranial dolichoectasia varies according to the clinical presentation, morphological subtype, circulation affected, and size of the vascular anomaly.
A report of 159 patients with vertebrobasilar nonsaccular intracranial aneurysms found an annual hemorrhage rate of 0.9%, increasing to 2.3% annually among the subset of nonsaccular aneurysms that were either fusiform or transitional subtypes. All patients with hemorrhage related to aneurysmal rupture died (15). In the same series, the 1- and 10-year risk of cerebral infarction was 2.7% and 15.9%, respectively, and the risk of recurrent cerebral infarction was 6.7% per patient year. Median survival was 7.8 years, with death most often due to cerebral ischemia (16). In another series of 156 patients with nonsaccular intracranial vertebrobasilar aneurysms of the dolichoectatic subtype (not including spindle-shaped fusiform or transitional subtypes) who were followed for an average of almost 12 years, 38% suffered an ischemic stroke and 13% an intracranial hemorrhage (40). Among this series of patients, there were three subarachnoid hemorrhages and 15 intracerebral hemorrhages during a mean follow-up of almost 10 years, for crude incidence rates of 2.2 per 1000 person-years for subarachnoid hemorrhage and 11 per 1000 person-years for intracranial hemorrhage (40).
A systematic review analyzed a total of 375 patients with vertebrobasilar dolichoectasia and determined a 5-year complication risk of 17.6% for ischemic stroke, 10.3% for brainstem compression, 10.1% for transient ischemic attacks, 4.7% for intraparenchymal hemorrhage, 3.3% for hydrocephalus, and 2.6% for subarachnoid hemorrhage. The overall estimated 5-year case fatality was 36.2%, with ischemic stroke being the most common cause of death (59). A meta-analysis of 15 studies comprising 827 patients with vertebrobasilar nonsaccular or dolichoectatic aneurysms, followed over 5093 patient-years, found estimated rates of growth of 6% per year, of rupture 3% per year, and of mortality 13% per year (36). Patients with fusiform aneurysms had higher growth rates (12% vs. 3%) and rupture rates (3% vs. 0%) compared to patients with dolichoectatic aneurysms, suggesting a poorer natural history for fusiform aneurysms.
Having clinical manifestations at the time of diagnosis is a strong predictor of subsequent complicated clinical course. Incidentally, discovered fusiform or dolichoectatic aneurysms have a relative low rate of complications compared to those presenting with ischemic stroke or brainstem compression (01; 59; 61). Recurrence rates of ischemic stroke can be elevated in patients with vertebrobasilar dolichoectasia, approaching 10% per year, and greater in those with more severe or widespread dolichoectasia (07). Persons with internal carotid artery circulation aneurysms fare better than those with vertebrobasilar system disease (01; 16), and patients with aneurysms of the posterior cerebral arteries fare better than patients with aneurysms of the proximal vertebrobasilar trunk (08). Size of the aneurysms is a predictor for fatal complications, and a diameter greater than 10 mm is associated with hemorrhage and brainstem compression (59; 41). Some authors have quoted mortality rates as high as 65% to 100% at two years for untreated giant aneurysms greater than 2.5 cm (20). Growth in aneurysm diameter is also correlated with an increasing number of symptoms, a tendency for increased subarachnoid hemorrhage risk, and a more than 10-fold higher 5-year mortality rate (56.5% vs. 3.7%) (31). Another series reported retrospective natural history data from 121 patients with unruptured intradural fusiform aneurysms (48). Importantly, in this series atherosclerotic aneurysms were separated by well-defined criteria from nonatherosclerotic aneurysms. When compared with patients with nonatherosclerotic aneurysms, case fatality and aneurysm progression rates were substantially higher in patients with associated atherosclerosis.
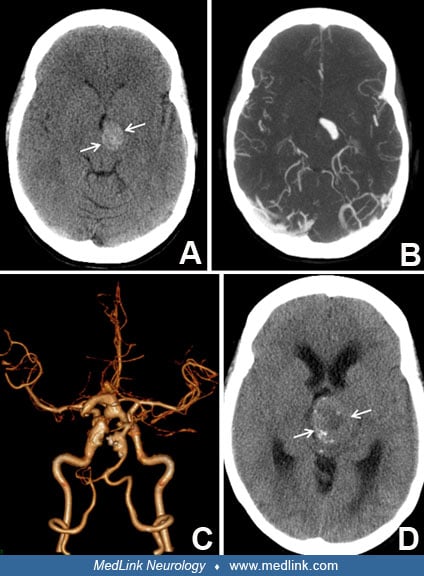
Case 1. A 59-year-old male with hypertension, diabetes, and dyslipidemia, with history of coronary disease treated with coronary bypass grafting, and with history of abdominal aortic aneurysm repair, presented with recurrent posterior circulation ischemic events, improving with intravenous tissue plasminogen activator on one occasion and intravenous heparin therapy on the second and third occasions. He was left with infarction in the territory of the left posterior cerebral artery, with right hemianopsia, and verbal memory deficits. CT scanning of brain revealed an ectatic basilar artery with mural calcifications (A). CT angiography demonstrated basilar artery dolichoectasia (B). He recovered and continued with stable deficits through 3 years of follow-up, on warfarin.
This case demonstrates the risks of ischemic infarction that accompany the common form of basilar artery dolichoectasia in patients with typical atherosclerotic risk factors.
Case 2. A 36-year-old athletic female, without known vascular risk factors, presented during the third trimester of pregnancy with headache, slurred speech, and “twisted mouth.” Head CT scan showed an extra-axial mass compressing the left cerebral peduncle (A), recognized by CT angiography (B) as a partially thrombosed fusiform aneurysm of the left posterior cerebral artery. There was also tortuosity and ectasia of the basilar and left internal carotid arteries (C). Six years later, the vascular mass had expanded (D), producing severe midbrain compression and hydrocephalus, with spastic quadriparesis. She was treated with ventricular drainage and clipping of the left posterior cerebral artery proximal to the aneurysm.
Dilatative arteriopathy in cases like this, with severe progressive multifocal ectasia of cerebral arteries in the absence of a detectable generalized vasculopathy, can produce deficits due to cranial nerve and parenchymal brain compression as well as risks of ischemia or hemorrhage.
|
• Nonsaccular aneurysms form when there is disruption to the arterial wall causing vessel weakening. The pathogenesis is diverse and not fully understood. | |
|
• Atherosclerosis, dissection, trauma, genetic abnormalities in elastin and collagen metabolism, infection, and inflammation have all been implicated in the pathogenesis of nonsaccular aneurysms. | |
|
• Progression to nonsaccular aneurysms has been described as disruption of the internal elastic lamina with consequent intimal hyperplasia followed by neoangiogenesis within the hyperplastic intima. As the aneurysm progresses and neoangiogenesis continues, there is intramural hemorrhage with thrombus formation followed by ensuing hematoma recanalization. | |
|
• Adaptive remodeling contributes to aneurysm progression in atherosclerotic arteries. |
Nonsaccular aneurysms of fusiform, dolichoectatic, or transitional forms can arise from a wide variety of causes (Table 1). Abnormal arterial dilation is the final common pathway of any vessel wall disease that disrupts the tunica media and causes fragmentation of the internal elastic lamina (41). In the past it has been generally accepted that fusiform or dolichoectatic aneurysms commonly develop due to severe atherosclerotic weakening of the arterial wall (58). In particular, basilar artery dolichoectasia often appears in the setting of generalized atherosclerosis, as in vignette Case 1 (above). Scholarship has emphasized the association of dolichoectasia with small vessel disease and proposed a common etiopathogenesis between these two entities (22). Fusiform aneurysms can also likely result from focal intracranial dissections or other arteriopathies (65). It is helpful to recognize that dolichoectasia may be a final common pathway of any arterial wall disease that disrupts the structural integrity of the tunica media (41).
|
• Atherosclerosis |
Genetics. In some cases, a clear genetic basis for nonsaccular aneurysms can be identified. Fabry disease and late onset Pompe disease are hereditary lysosomal storage disorders in which the vacuolization of the vascular smooth muscle leads to the development of dolichoectasia (29; 30). In autosomal dominant polycystic kidney disease, dolichoectasia occurs in about 2% of cases (49). Rarely, in younger patients, fusiform aneurysms are due to congenital defects in the media connective tissue or smooth muscle cells, such as occurs in Marfan syndrome and Ehlers-Danlos syndrome type IV (24). Other genetic conditions associated with intracranial arterial dolichoectasia include pseudoxanthoma elasticum, fibromuscular dysplasia, neurofibromatosis type 1, sickle cell disease, alpha-1-antitrypsin deficiency, moyamoya disease, PHACE syndrome, and arterial tortuosity syndrome (27; 37).
Other causes of nonsaccular aneurysms. Dolichoectasia, particularly of the vertebrobasilar and carotid arteries, can be a relatively common manifestation in patients with atherosclerotic disease or cerebral small vessel disease. Fusiform aneurysms sometimes arise due to focal injury to the arterial wall due to spontaneous dissection, trauma, or inflammation. Rare cases occur due to bacterial or fungal infection in the arterial wall, termed “infective aneurysms.” Cases secondary to syphilitic arteritis have also been reported. Interestingly, there are case reports of fusiform intracranial aneurysms in children and adults with HIV infection or with varicella zoster infection. Inflammatory autoimmune conditions with CNS involvement, such as lupus erythematosus, can sometimes lead to fusiform aneurysm formation. Other rare involvement of the arterial wall with metastatic neoplasms can also sometimes result in focal mural weakening and fusiform aneurysm formation. Radiation-induced vasculopathy can occasionally induce the development of fusiform aneurysms. Finally, focal fusiform aneurysms or progressive transitional aneurysms can often be found without any identified risk factors or cause, suggesting the presence of an underlying idiopathic dilatative arteriopathy, as in the clinical vignette Case 2 (above).
Pathology and pathophysiology. The exact mechanism of formation of chronic nondissecting fusiform aneurysm and intracranial arterial dolichoectasia is unknown. One retrospective clinicopathologic series of 16 chronic fusiform aneurysms described a characteristic histological pattern (35). There was suggestion of a progression starting with (1) disruption of the internal elastic lamina with consequent intimal hyperplasia followed by (2) neoangiogenesis within the hyperplastic intima. As the aneurysm progresses and neoangiogenesis continues, there is (3) intramural hemorrhage with thrombus formation followed by (4) ensuing hematoma recanalization, usually in aneurysms that have grown larger than 20 mm. The initial injury to the tunica media can be driven by hemodynamic, anatomical, or biological factors. Regardless of the initial trigger, authors concluded that fragmentation of internal elastic lamina is the earliest event in vessel dilation, whereas the formation of intramural hematoma is the key step that leads to aneurysm progression and clinical manifestations.
Dolichoectasia of intracranial arteries, particularly involving the basilar artery, is common in stroke patients with atherosclerotic risk factors. During the process of chronic atherosclerosis, fibrous tissue may replace smooth muscle and elastic fibers of the internal elastic lamina, allowing vessels to stretch in length and width. When widening is extreme, the artery balloons into a fusiform aneurysm, whereas if both lengthening and widening occur, the aneurysm becomes dolichoectatic. Another mechanism potentially of relevance to dolichoectasia is the process of compensatory enlargement of atherosclerotic arteries known as “adaptive remodeling.” This has been described in various arterial beds, including the coronary arteries and cervical arteries (18). Adaptive remodeling produces enlargement of the external wall of the artery compensating for mural plaque, variably resulting in net preservation, constriction, or dilatation of the arterial lumen. Such a mechanism may also underlie some cases of arterial dolichoectasia in atherosclerosis.
Some authors, alternatively, have emphasized the preferential association of intracranial dolichoectasia with signs of lacunar stroke and imaging markers of small vessel disease (43; 11; 55). Patients with acute ischemic stroke and intracranial dolichoectasia have a larger number of lacunes, cerebral microbleeds, and white matter changes (54). Arterial dolichoectasia and cerebral small vessel disease might have an underlying common physiopathology that leads to an abnormal proteolytic activity, resulting in the pathological changes and clinical consequences characteristics of these conditions (27). Dysfunctional matrix metalloprotein activation and imbalance between protease and antiprotease activities in the extracellular matrix may lead to loss of elastic fibers, with disruption of the internal elastic lamina and consequent excessive dilatation (42; 22). In support of this concept, an animal model employing injection of elastase into the cisterna magna of mice successfully induced intracranial dolichoectasia (09). At the cellular level, elevation of matrix metalloproteinases has shown to be associated with white matter damage and perivascular inflammation around small penetrating vessels (45). Atherosclerotic plaque found in the affected basilar arteries has been considered by these authors a secondary effect of the arteriopathy and dilatation (42; 27). It is clear that the high degree of overlap between risk factors for atherosclerosis and those for microvascular disease leads to a frequent co-occurrence of these conditions, and it may be that typical intracranial dolichoectasia in vasculopathic patients arises from a mix of etiologies.
States of increased blood flow may also induce adaptive remodeling by increased wall shear stress and endothelial signaling factors, including nitric oxide production and cytokine production. Inflammatory cell infiltration of the tunica media of the arterial wall and release of inflammatory mediators may contribute to vessel weakening and growth of intracranial aneurysms (06). Breakdown of the internal elastic lamina can be documented experimentally due to high flow-induced arterial enlargement (32).
|
• Fusiform aneurysms are relatively uncommon in the general population but are found with increased prevalence in stroke patients. |
The prevalence of dolichoectasia varies according to the populations studied and the diagnostic criteria applied. Studies not confined to patients with clinical stroke found a prevalence of vertebrobasilar dolichoectasia between 0.8% to 6.5%, whereas series limited to patients with stroke report higher prevalences ranging from 3% up to 24% (12). Dolichoectasia is found in a number of patients with stroke of undetermined cause or small artery occlusion strokes, providing a possible etiology. Advanced age, male sex, and history of hypertension have been associated with dolichoectasia. A population-based study amongst community-dwelling adults living in rural Ecuador found that 3.2% had basilar artery ectasia (diameter greater than 4.5 mm), 11.6% had dolichosis, and 13.6% had dolichoectasia (ectasia, dolichosis, or both) (11). Similarly, a population-based study in a Chinese population reported basilar arterial dolichoectasia in 3.6% and intracranial arterial dilatation in 5.9% (64). These studies assessing the occurrence of abnormally dilated or tortuous intracranial arteries do not reflect the much lower prevalence of true fusiform aneurysms.
In a large autopsy series totaling over 16,000 cases, 15 (less than 0.1%) fusiform aneurysms were discovered (23). Among all aneurysms, fusiform aneurysms account for 5% to 9% (23). In Yu's large series of 50,000 angiograms, 31 fusiform aneurysms were discovered (0.06%), 14 of which were in the internal carotid artery circulation, eight in the vertebrobasilar circulation, and nine in both (63). Thus, true fusiform aneurysms are relatively uncommon.
No specific means of preventing the formation of fusiform and dolichoectatic aneurysms are known. Given the strong association between these aneurysms and vascular disease, strict control of traditional vascular risk factors, such as hypertension, hyperlipidemia, hyperglycemia, and cigarette smoking, might delay progression of these nonsaccular aneurysms.
Giant nonsaccular aneurysms can mimic tumors by producing headache, seizures, hydrocephalus, and focal neurologic signs. Pressure on isolated cranial nerves can result in optic atrophy, trigeminal neuralgia, hemifacial spasm, or other cranial neuropathies for which the differential diagnosis is broad. Hypopituitarism and a bitemporal visual field defect can mimic a pituitary neoplasm. There can be increased intracranial pressure with papilledema. Neuroimaging usually easily confirms the diagnosis of aneurysm. Occasionally, a fusiform aneurysm may be misinterpreted as a tumor on noncontrast brain imaging. Unless contrast or vascular imaging is pursued before a biopsy, a disastrous procedure may result.
Transient ischemic attacks and stroke can be caused by large fusiform or dolichoectatic aneurysms. The results of a complete work up for other causes of stroke must be considered in reaching this conclusion. In such instances, investigation will frequently demonstrate intraluminal thrombus when the aneurysm is the cause for symptoms.
An abrupt onset of severe headache with or without focal neurologic symptoms suggests intracranial hemorrhage. Hemorrhage has sometimes been considered less likely with fusiform or dolichoectatic aneurysms than with saccular aneurysms. However, without question, hemorrhages can occur. In a long-term prospective study of 156 patients with vertebrobasilar dolichoectasia followed for an average of 9 years, six subarachnoid hemorrhages and 26 intraparenchymal hemorrhages occurred (39).
|
• Diagnostic workup depends on presentation; if subarachnoid hemorrhage is suspected, rapid nonenhanced brain CT followed by CTA should be done emergently. | |
|
• MRI brain with or without contrast is indicated in the evaluation of cranial neuropathies. | |
|
• Vessel imaging to better visualize the fusiform aneurysm can include CTA, MRA, or DSA. | |
|
• MRI/MRA are preferred imaging modalities for dolichoectasia/fusiform aneurysm characterization. | |
|
• CTA has similar advantages to MRA with good resolution for evaluating aneurysmal vascular lumen. | |
|
• High-resolution MRI vessel wall imaging detecting vessel wall enhancement can provide information on the stability of the aneurysm and early signs of aneurysm progression. |
Smoker and colleagues initially proposed basilar dolichoectasia diagnostic criteria based on computed tomography in 1986 (51). Ectasia of the basilar artery was defined as a diameter greater than 4.5 mm at the mid pons. In addition, a location lateral to the lateral margin of the clivus of dorsum sellae or a bifurcation above the suprasellar cistern defined elongation and tortuosity. Similar criteria have been extrapolated to the use of MRI and MRA with the additional advantage of providing a good anatomical association between the vascular anomaly and the surrounding neural structures.
The appropriate initial workup depends on the mode of presentation. Symptoms suggesting subarachnoid hemorrhage should be evaluated with rapid nonenhanced brain CT scan. In situations where subarachnoid hemorrhage is strongly suspected and radiologic tests are negative for blood, lumbar puncture should be performed, provided there is no evidence of mass effect in the posterior fossa. The initial CT scan is often immediately followed by CT angiography, which can detect dolichoectatic arteries and fusiform aneurysms as well as most saccular aneurysms larger than 2 mm in size. In contrast, presentation with cranial nerve palsy or signs of parenchymal compression should usually prompt brain MRI scanning (without and with intravenous contrast) and MR angiography (MRA).
MRI with MRA is also the test of choice to identify and characterize most incidentally discovered proximal fusiform and dolichoectatic aneurysms. It will demonstrate the dilated, tortuous vessel as a signal void region corresponding to the artery. Compared to catheter angiography, MRI/MRA has the advantage of more accurately determining the true size of aneurysm because catheter angiography can only outline the residual lumen without characterizing the vessel wall. Additionally, effects on adjacent structures and the presence of intraluminal thrombus will typically be better demonstrated on MRI. Contrast enhancement of the arterial wall and intramural hemorrhage can be detected by advanced MRI imaging and can provide early signs of aneurysmal progression (35). MRI may also assist in differentiating a primary fusiform aneurysm from one that is secondary to arterial dissection, where an intimal flap, wall hematoma, or double lumen may be demonstrated. High field strength MRI scanning is increasingly used to perform vessel wall imaging, with remarkable resolution.
CT angiography can provide many of the same advantages as MR angiography, with equal or better resolution for definition of the vascular lumen, and high sensitivity to mural changes, particularly mural calcifications. CT angiography is also becoming increasingly useful in assessing distal aneurysms.
In light of development of increasingly sophisticated endovascular interventions for dissections and nonsaccular intracranial aneurysms, diagnostic catheter angiography may be needed to help decide what therapeutic approach should be pursued.
Advanced imaging techniques may guide management in the future. Hemodynamic models based on axial MRA and CTA were able to distinguish between stable and unstable vertebrobasilar fusiform and dolichoectatic aneurysms. Unstable aneurysms had lower flow conditions, including lower shear rates, velocity, and vorticity, but higher oscillatory flow compared to stable aneurysms (04). High resolution MRI vessel-wall imaging has suggested that, as compared to saccular aneurysms, fusiform aneurysms exhibit more frequent and widespread wall enhancement, and that the degree of enhancement correlates with larger aneurysm size (26; 47).
There is a lack of prospective trials on the management of fusiform aneurysms and intracranial arterial dolichoectasia. The objectives of therapy focus on protection from bleeding, ischemic stroke, and mass effect. The natural course of untreated fusiform and dolichoectatic aneurysms carries a significant high risk of complications and death (16). On the other hand, these aneurysmal dilatations are particularly difficult to treat due to lack of an identifiable neck and risk of compromising distal flow. Different surgical and endovascular techniques have been used to treat these vascular malformations; however, the utility and timing for intervention remains unclear. Patient selection remains a very important determinant to avoid complications and reach good outcomes.
When the aneurysm is responsible for severe headache, cranial nerve compression, brain compression, or hydrocephalus, surgical decompression followed by direct treatment of the aneurysm can be considered. Similarly, in the setting of hemorrhage, efforts to secure the aneurysm should generally be undertaken if feasible. Additionally, aneurysm enlargement over serial imaging studies has been shown to predict rupture and death (31) and usually signals the need to consider intervention. It is widely accepted that surgical and endovascular treatment of fusiform and dolichoectatic aneurysms is difficult technically and must be individualized, depending on location, size, symptoms, and flow characteristics.
Medical treatment. In patients presenting with acute cerebral ischemia the use of intravenous thrombolytics has been shown to be safe and effective (19); hence, patients should be treated according to the current guidelines for management of acute stroke. Secondary stroke prevention is more controversial. Initial reports advocated anticoagulation to prevent ischemic complications; however, the risk of serious hemorrhagic complications might outweigh any benefits. There have been no randomized trials comparing these two different approaches, and thus, treatment decisions must be based on clinical judgment, weighing individual patient characteristics. Conservative management should include antiplatelet agents and vascular risk-reduction measures such as blood pressure control and cholesterol-lowering therapy. In patients with luminal thrombus formation, surgical or endovascular aneurysmal isolation or endovascular thrombectomy may avert further embolic events but risks the occlusion of branching vessels, distal flow compromise, thromboembolism, or dissection.
Surgical treatment. Surgical treatments of nonsaccular aneurysms include (1) reinforcement of the aneurysm dome by wrapping, (2) direct clipping, (3) resection and re-anastomosis, (4) trapping and distal bypass, (5) proximal occlusion, (6) transposition, and (7) thrombectomy, endarterectomy, and aneurysmorrhaphy. Arterial reconstructions by wrapping or clipping are procedures reserved for aneurysms that cannot be eliminated from the circulation. Wrapping is the least successful technique because rebleeding and symptom progression rates are high when the aneurysm itself is not eliminated. Clipping is difficult because these aneurysms do not have a neck; external refashioning with clips can sometimes provide satisfactory results. Resection and re-anastomosis require that just a short segment of the artery be involved. Historically, aneurysmal isolation with resultant obliterative thrombosis and involution has been the most popular surgical strategy and can be achieved either by proximal occlusion or trapping (13). In the case of vertebrobasilar lesions, flow reduction by sacrifice of a single vertebral artery is preferred when there is good collateral flow. When collaterals are adequate, flow reversal can be achieved by bilateral vertebral artery or proximal basilar artery occlusion. For lesions presenting with acute mass effect, aneurysmal trapping with hematoma decompression should be considered. A surgical bypass is required when the collateral flow for the territory supplied by the parent artery is insufficient. Finally, if tortuous vessels cause brainstem or cranial nerve compression in the absence of intraluminal thrombus, symptoms can sometimes be relieved by vessel transposition or microvascular decompression (44).
Endovascular treatment. With the development of sophisticated catheters, detachable balloons, coils, and stents, endovascular approaches to fusiform and dolichoectatic aneurysms have become increasingly viable as alternatives to open surgical management (65). Endovascular approaches can be grouped as deconstructive or reconstructive (20). Deconstructive techniques include parent artery occlusion and trapping. Endovascular proximal arterial occlusion and trapping of the aneurysm can be performed with detachable balloons or coils. It carries the advantage of allowing prior evaluation of tolerance to the procedure by balloon occlusion test assisted by clinical and angiographical evaluation as well as other monitoring methods such as electroencephalography and evoked potentials. When the patient is not able to tolerate the balloon occlusion test, microsurgical creation of a bypass in combination with endovascular treatment can performed. In contrast to deconstructive approaches, reconstructive endovascular techniques aim to perform aneurysm embolization with preservation of the parent artery. The advent of balloon-assisted coiling, stent-assisted coiling, balloon-in-stent-assisted coiling, and even stent-in-stent remodeling has advanced the ability of the interventionalist to treat aneurysms with circumferential dilatation or wide necks (08; 28). In particular, stent-assisted coiling, excluding the coil mass from the arterial lumen with a stent, has become a frequent solution to this problem. Sometimes multiple overlapping stents are required for complex aneurysms (60). Procedure-related complication rates can be high (19% in this series).
Recent years have also seen increasing use of a flow-diverting stents with closed-cell mesh designs that direct blood flow away from the aneurysm while preserving flow in the parent vessel and adjacent branches. When flow diversion is successful, angiographic stasis occurs in the aneurysm, preventing rupture and causing the aneurysm to decrease in size over time. These flow-diverting stents have been approved for use in European countries for some years and more recently were approved in the United States, and their use for both saccular and fusiform aneurysm embolization is increasing. In particular, the Pipeline embolization device has become a common tool for endovascular treatment of fusiform aneurysms. Flow diverting stents can be used in both anterior and posterior circulation fusiform aneurysms, and both elective aneurysm treatment and treatment of ruptured aneurysms can be accomplished with flow-diversion techniques (02). Even aneurysms in small distal vessels, such as the distal anterior cerebral artery, can sometimes be successfully treated with flow-diverting stents (38). A systematic review found reports of a total of 1704 aneurysms (81% saccular and 18% fusiform) treated with flow-diverter devices, with more than an 80% rate of final complete occlusion, and with a neurologic morbidity rate of 3.5% and a mortality rate of 3.4% (03). However, retrospective review suggests that fusiform embolization with the pipeline device is more often associated with incomplete occlusion or major complications in fusiform aneurysms than in treatment of dissecting or saccular aneurysms (21). A series focused on Pipeline embolization treatment of 109 fusiform intracranial aneurysms in 104 patients found a complete occlusion rate of 68%, with a 17% complication rate and a 3% mortality rate (56). Another series suggested that complete occlusion was achieved more often in the aneurysms of the posterior circulation than in the anterior circulation (62). Comparison of outcomes between 233 fusiform aneurysm patients treated with endovascular approaches to 79 patients treated with microsurgery using propensity score adjustment suggested no significant differences in clinical outcomes. Of note, patients who undergo stenting are then committed to at least a short period of dual antiplatelet therapy likely followed by monotherapy.
(A) Pre-procedural anterior and lateral angiographic views of a large (7 x 23 mmm) fusiform basilar artery aneurysm with two daughter sacs, presenting with third cranial nerve compression. (B) Angiographic reconstructed image a...
Prevention of aneurysm progression. Finally, the better understanding of the pathophysiological events that lead to the formation and growth of fusiform and dolichoectatic aneurysm has suggested as a future goal the targeting of specific molecular pathways in the progression of these vascular malformations. Similarities in the biological characteristics between aortic aneurysms and nonsaccular intracranial aneurysms suggest consideration of medical therapies proposed for prevention of aortic aneurysm growth, such as doxycycline or roxithromycin (46). Several trials have examined the effectiveness of losartan in restricting aortic aneurysm growth in Marfan syndrome with inconclusive results (17). Antiangiogenic drugs such as bevacizumab, rapamycin, or thalidomide, targeting neo-angiogenesis and bleeding within the thickened intima, may prove to have a role in slowing the progression of fusiform aneurysms (50).
There has also been a growing interest in targeting inflammatory pathways to slow progression of fusiform aneurysms. One target of interest is the tumor necrosis factor-alpha (TNF-alpha) inflammatory cascade. A small preliminary study using the TNF-alpha inhibitor infliximab suggested a decreased aneurysmal growth rate and stabilization in two treated patients (05). Other studies have taken a renewed interest in statins and their effect on potentially decreasing vessel wall inflammation and slowing the rate of aneurysm growth.
Surgical and endovascular treatment of fusiform aneurysms is generally reserved for larger, more often symptomatic or progressing aneurysms; therefore, outcomes cannot be directly compared to results observed in aneurysms treated expectantly. Reported case series reflect the complexity and difficulty of surgical treatment of these cases. One surgical case series reported a 30% complication rate, with no operative mortality in 38 surgically treated patients followed over a mean period of 2.8 years; 58% made good recoveries (Glasgow Outcome Scale score 1), 20% had moderate disabilities (Glasgow Outcome Scale score 2), 8% had severe disabilities (Glasgow Outcome Scale score 3), and 15% died (01). Steinberg and colleagues reported a series of 201 patients with nonclippable posterior circulation aneurysms treated with different degrees of proximal vessel occlusions (53). Patients who underwent flow reduction had an excellent/good outcome in 63% of cases. Patients undergoing flow reversal by complete proximal flow arrest had a 74% chance of excellent/good outcome, whereas patients who underwent trapping of the aneurysm with thrombectomy achieved good outcomes in 71% of patients. A series of 56 patients treated with flow-diverting stents followed for a mean of 325 months showed 15% mortality (02). Good recovery (mRS ≤2) was achieved in 87% of patients that were initially asymptomatic but only in 55% of symptomatic cases. Lin and colleagues, reporting early United States experience with use of the “pipeline” flow diversion stent in the treatment of 26 patients with ruptured aneurysms, including six fusiform aneurysms, described a periprocedural complication rate of 19% and a complete occlusion rate of 78% in follow-up angiograms (25). These studies demonstrate both the considerable morbidity and the encouraging success that can be achieved in the treatment of these challenging aneurysms.
No clear influence of pregnancy on aneurysm appearance or progression has been described.
Anesthesia techniques similar to those used for other difficult aneurysm surgeries should be used. Electroencephalographic and evoked potential monitoring and barbiturates titrated to burst suppression must be considered. When prolonged interruption of blood flow is likely, hypothermic circulatory arrest may be necessary.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

James R Brorson MD
Dr. Brorson of the University of Chicago has no relevant financial relationships to disclose.
See ProfileLina Chervak MD
Dr. Chervak of University of Chicago Medicine has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
Dec. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Sleep Disorders
Oct. 14, 2024
Developmental Malformations
Sep. 22, 2024