



Epilepsy & Seizures
Tonic status epilepticus
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Generalized onset tonic-clonic seizures are the most dramatic, severe, and common seizures of mainly syndromes of idiopathic generalized epilepsy. They manifest with violent generalized convulsions, loss of consciousness, and marked autonomic disturbances. They are usually spontaneous, but they may also be provoked by external, mainly photic, stimuli. They occur at any time, but mainly on awakening. They are often associated with severe complications that may also be fatal. They affect patients of all ages, except neonates. Additionally, patients may also suffer from other types of seizures, such as absences and myoclonic jerks. Syncope and psychogenic nonepileptic seizures are frequently misdiagnosed as generalized onset tonic-clonic seizures. Treatment is demanding because a significant number of currently available antiepileptic drugs may aggravate generalized seizures. In this updated article, the author details the clinical manifestations, pathophysiology, EEG, and neuroimaging of generalized onset tonic-clonic seizures and provides clues for correct diagnosis and optimal management of patients.
Historical aspects. The manifestations of GTCS are so dramatic that accurate descriptions can be found as early as 1050 BC in the twenty-fifth Babylonian cuneiform tablet devoted to miqtu (a disease in which the person loses consciousness and foams at the mouth) (05). A realistic depiction of GTCS, including marked cyanosis, can be seen in the painting The Miracles of St Ignatius of Loyola (1617) by Peter Paul Rubens (1577-1640) (79).
Gowers gives an excellent description of GTCS (38):
At the onset of the severe fit the spasm is tonic in character, – rigid, violent, muscular contraction, fixing the limbs in some strained position… When the cyanosis has become intense, the fixed tetanic contractions of the muscles can be felt to be vibratory, and the vibrations gradually increase until there are slight visible remissions. As these become deeper, the muscular contractions become more shock-like in character… Such attacks may commence with tonic spasm, or they may commence by, and sometimes consist only of clonic spasm… Precursory symptoms occasionally precede a fit, sudden jerks of the body or limbs. |
However, it was Henri Gastaut and his associates in Marseilles, France who provided us with superb descriptions of the clinical and EEG manifestations of GTCS, which have not been surpassed (33). Their description was based on a large number of combined clinical, EEG, and polygraphic investigations of GTCS in patients with epileptic disorders or induced by Metrazol or electroconvulsive treatment of psychotic patients. These were supplemented by cinematographic or videotaped filming and various other techniques. Contributions have been made with video-EEG analysis (57; 10).
ILAE classification and nomenclature. A fundamental distinction of all ILAE classifications is whether tonic-clonic seizures are of generalized or focal onset (25; 24; 04; 15; 29; 28).
According to the ILAE definitions, generalized seizures “originate at some point within, and rapidly engage, bilaterally distributed networks. Such bilateral networks can include cortical and subcortical structures, but do not necessarily include the entire cortex. Although individual seizure onsets can appear localized, the location and lateralization are not consistent from one seizure to another. Generalized seizures can be asymmetric.” Conversely, focal seizures “originate within networks limited to one hemisphere, which may be discretely localized or more widely distributed. Focal seizures may originate in subcortical structures” (04; 15; 29; 28).
The ILAE description of GTCS in the 1981 proposal is as follows (14):
The most frequently encountered of the seizures are GTCS, often known as grand mal. Some patients experience a vague ill-described warning, but the majority lose consciousness without any premonitory symptoms. There is a sudden, sharp tonic contraction of muscles, and when this involves the respiratory muscles, there is stridor, a cry or moan, and the patient falls to the ground in the tonic state, occasionally injuring him or herself. The patient lies rigid, and during this stage, tonic contraction inhibits respiration and cyanosis may occur. The tongue may be bitten and urine may be passed involuntarily. This tonic stage then gives way to clonic convulsive movements lasting for a variable period of time. During this stage, small gusts of grunting respiration may occur between the convulsive movements, but usually the patient remains cyanotic and saliva may froth from the mouth. At the end of this stage, deep respiration occurs and all the muscles relax, after which the patient remains unconscious for a variable period of time and often awakes feeling stiff and sore all over. He or she then frequently goes into a deep sleep and when awakened feels quite well apart from soreness and, frequently, headache. GTCS may occur in childhood and in adult life; they are not as frequent as absence seizures, but vary from daily to once every 3 months and occasionally to one every few years. Very short attacks without postictal drowsiness may occur on occasion. |
GTCS are defined as follows in the ILAE glossary (07):
Generalized tonic-clonic seizure (synonym: bilateral tonic-clonic seizure--formerly “grand mal” seizure, noun): bilateral symmetrical tonic contraction, then bilateral clonic contractions of somatic muscles usually associated with autonomic phenomena. |
Note that the terms “primarily” and “secondarily” GTCS should not be confused with the now obsolete terms of “primary” and “secondary epilepsy,” which have been rightly abandoned by the ILAE and by most physicians, though they are often used in formal reports of antiepileptic drug trials. Additionally, these terms are not used in the ILAE glossary (07). Furthermore, “primarily” and “secondarily” GTCS have been abolished in the ILAE definitions and “secondarily generalized tonic-clonic” has been replaced by “focal to bilateral tonic-clonic” (29; 28).
In the 2014 ILAE “Epilepsy diagnosis” manual, generalized onset tonic-clonic seizures are categorized amongst generalized convulsive seizures (15). Generalized seizures are convulsive, absence, tonic, atonic, and myoclonic.
“Generalized convulsive seizures are typically bilateral and symmetric although variants with asymmetry including head and eye deviation can be seen. A tonic clonic seizure is a seizure consisting of a tonic and a clonic phase, typically in this order, however variations such as clonic-tonic-clonic are also seen. A clonic seizure is a seizure involving bilaterally rhythmic jerking and may occur alone or in combination with tonic activity where there is bilaterally increased tone of the limbs typically lasting seconds to a minute. The jerking in a clonic seizure is more sustained and rhythmic than seen in a myoclonic seizure” (15). |
The most recent ILAE positional papers on the operational classification of seizure types retain the name “generalized onset tonic-clonic seizures” and classify them amongst “generalized onset motor seizures” (29; 28). Generalized onset seizures are motor (tonic-clonic, clonic, tonic, myoclonic, myoclonic-tonic-clonic, myoclonic-atonic, atonic, epileptic spasms) or nonmotor (absence) (typical, atypical, myoclonic, eyelid myoclonia). GTCS are defined as follows (29; 28):
“bilateral symmetric or sometimes asymmetric tonic contraction and then bilateral clonic contraction of somatic muscles, usually associated with autonomic phenomena and loss of awareness. These seizures engage networks in both hemispheres at the start of the seizure. Generalized myoclonic-tonic-clonic seizures begin with a few myoclonic jerks followed by tonic-clonic activity. These seizures are commonly seen in patients with juvenile myoclonic epilepsy and occasionally with other generalized epilepsies. It is arguable whether the initial jerks are myoclonic or clonic, but they are rarely sufficiently sustained to be considered clonic. Because there is a new seizure type (myoclonic-tonic-clonic) characterized by myoclonic movements preceding tonic (stiffening) and clonic (sustained rhythmic jerking) movements, it is important to document the early movements of a tonic-clonic seizure as being tonic. The clonic phase of a tonic-clonic seizure typically shows regularly decreasing frequency of jerks over the course of the event. During a tonic-clonic seizure, awareness is lost before or contemporaneously with the stiffening and jerking movements. Some tonic-clonic seizures may invoke a nonspecific feeling of an impending seizure or a brief period of head or limb version, neither of which invalidates a generalized onset, since biologic processes never exhibit perfect synchrony. The clinician has to judge whether a truly focal onset is present.” |
Generalized onset tonic-clonic seizures (GTCS) manifest with loss of consciousness from onset to the late phase of recovery, tonic-clonic convulsions, and significant autonomic disturbances. The main sequence of events can be described in the following illustrations (33).
The following descriptions are mainly based on the classical work of Gastaut (33).
Symptoms preceding and heralding generalized onset tonic-clonic seizures (GTCS). Usually, their onset is abrupt and violent, with no prior warnings, auras, or other symptoms. However, a prodrome is often cited as a warning symptom of an impending GTCS. Prodrome is a nonepileptic, subjective or objective clinical alteration preceding the onset of an epileptic seizure by several hours. This can take the form of a headache, changes in mood or behavior, sleep disturbances, lightheadedness, anxiety, and difficulty concentrating before the attack. Prodrome should not be confused with aura, which is a brief focal seizure itself. Prodromes are most likely symptoms of systemic or metabolic disturbances that are the causative or precipitating factors of the following seizure (eg, hypoglycemia, premenstrual period) (60). Prodromes are attributed to a preictal increase in excitability of an epileptogenic focus or of the entire brain (33), but there is no proof for this. In this author’s experience, for almost all patients seen with a diagnosis of prodrome, this was either an epileptic seizure itself (brief or prolonged, focal or generalized) or a symptom of a metabolic or electrolyte disturbance that caused a GTCS (60).
Ictal events preceding the onset of GTCS may be clusters of absences or myoclonic jerks.
Clusters of myoclonic jerks typically precede GTCS in juvenile myoclonic epilepsy, a sequence called clonic-tonic-clonic seizure or myoclonic-tonic-clonic seizure.
Onset and sequence of GTCS proper (33; 57; 50; 10; 72). At the start of GTCS, eyes immediately open and remain open during the whole period of the attack. Asymmetrical lateral tonic deviation of the head and eyes at the start of a GTCS is of little practical diagnostic significance because it may occur in both generalized or focal onset TCS, and may be contralateral or ipsilateral to the epileptic focus in FBTCS. Brief symmetrical or asymmetrical clonic movements may also occur at the start of GTCS or SGTCS, and immediately before the tonic phase. Asymmetrical clonic jerks are more common in FBTCS and may last 3 to 21 seconds (30). However, lateralization of FBTCS is more likely, when head turning is forceful and prolonged, usually in a clonic motion with the chin pointing upwards, and eye version to the same side as the head version allows (55). The “sign 4” (extension of the elbow on the site contralateral to the epileptogenic focus and with elbow flexion of the ipsilateral elbow) may also be of lateralizing significance when it occurs at the onset of GTCS (50). The presence of any fisting, fanning, clawing, index finger pointing, or flaccid hand posturing can help distinguish focal or generalized onset tonic-clonic epileptic seizures from nonepileptic convulsions. Index finger pointing suggests focal onset tonic-clonic seizures, whereas fanning with evolution suggests GTCS (72).
Significant autonomic changes. Significant autonomic changes occur at the onset of GTCS, peak at the end of the tonic phase, and progressively improve with the onset of the clonic phase, but some continue in the immediate postictal period.
Tonic phase of GTCS. The tonic phase may be brief, for 1 to 3 seconds, or last longer, for 20 seconds. It consists of a sustained contraction of all skeletal muscles, producing a succession of characteristic body postures. Usually there is an initial brief phase of tonic flexion forwards (emprosthotonus), followed by a longer one of tonic extension backward (opisthotonus).
In tonic flexion, the arms are in elevation, abduction, and external rotation, with semiflexion of the elbows. The body is dorsiflexed, and the legs are less involved, but there may be flexion, abduction, and external rotation of the thighs and legs. This converts into tonic ventriflexion of the neck and trunk with extension of the limbs.
The tonic extension phase is heralded by forced closure of the previously wide-open mouth, which often causes tongue biting. The “epileptic cry,” a high, pinched, loud scream occurring at this stage, is caused by the tonic contraction of thoracic abdominal muscles, which forcibly emit air across the tightly closed vocal folds. The semiflexed arms slowly lower in adduction until the forearms are crossed in front of the chest. Their subsequent posture consists of extension and pronation at the elbow, with the fists clenched and wrists extended, or with the fingers extended and wrists flexed. The legs are in extension, adduction, and external rotation. Feet and big toes are also in extension (spontaneous Babinski sign). Tonic contraction of the diaphragm and chest wall muscles appears to be responsible for the cyanosis that results from inadequate alveolar ventilation.
Intermediate vibratory phase of GTCS. The tonic phase ends gradually with fine clonus (vibratory tremor), initially superimposing on dominant tonic rigidity. The clonus is of waxing amplitude and waning frequency, from 8 Hz down to 4 Hz. Distal muscles are affected before the proximal and facial masticatory muscles.
Clonic phase of GTCS. This is characterized by continuously repetitive, massive, symmetrical, and synchronous flexor clonic convulsions of the facial, trunk, and limb musculature. They last for 30 seconds to 1 to 2 minutes with progressively decreasing force, amplitude, and frequency (to 1 Hz). They may finally restrict only in the facial muscles or end with a massive clonic convulsion. The tongue is often bitten repeatedly during this clonic phase, and each convulsion may produce an epileptic cry. Towards the end of the clonic phase, the clonic convulsions may become asynchronous and asymmetrical, and side-to-side head and eye movements may also occur. Contraction of the bladder sphincter blocks urinary incontinence until the end of the clonic phase.
There is no difference between the duration (around 65 seconds) of the convulsive phases in generalized or focal onset TCS (20).
Recovery phase of GTCS.
Immediate postictal phase (comatose or stertorous phase) of GTCS. Recovery starts with the cessation of clonic convulsions though the patient remains comatose, unresponsive, and markedly hypotonic. Respiration is restored with a deep inspiration, which is usually followed by noisy, deep breathing associated with secretion of frothy and blood-stained saliva. Incontinence of urine occurs only at this stage. Fecal incontinence or ejaculation is rare. Skin resistance and blood pressure progressively return to pre-seizure levels. The patient becomes pale.
Five to 8 seconds later, there may be a new phase of tonic contraction that affects mainly the facial and masticatory muscles: teeth are tightly clenched, and the limbs and trunk (when involved) take a decerebrate-like posture. Autonomic abnormalities include mydriasis, tachycardia, sometimes with marked cardiac arrhythmia, and intense tachypnea. This state is associated with hypometabolism predominating in cortical structures. It is of variable duration, seconds to 3 to 4 minutes, or may not occur.
The patient remains unconscious throughout this postictal state. Pupillary and cutaneous reflexes are absent, deep tendon reflexes are often exaggerated, and Babinski sign is elicited in half of the patients. Unilateral pyramidal signs indicate focal onset TCS of contralateral cortical onset.
Late postictal phase of GTCS. This period of recovery is characterized by a gradual return to normality. Autonomic nervous system function normalizes, and pupillary, cutaneous, and tendon reflexes reappear, but muscle atonia persists. Reactivity to pain stimuli returns. Cognitive functions also return to normal, but confusion and automatisms may be initially marked (postictal epileptic automatisms). The patient is extremely tired and drowsy and goes into deep and lengthy sleep if left undisturbed. On awakening, the patient feels exhausted, usually complaining of severe throbbing headache, and has retrograde amnesia.
The usual duration of the late postictal phase (not including the sleep period) is 2 to 10 minutes.
On full recovery, the patients are totally amnesic of what happened during the GTCS and most of the postictal state. However, they are aware that something happened to them, mainly because of the memory gap, aching muscles, and traumas.
Autonomic changes of GTCS. Significant autonomic changes occur at the onset of GTCS, reach their peak at the end of the tonic phase, and progressively improve with the onset of the clonic phase. Some continue in the immediate postictal phase and return to baseline normal function in the late postictal phase.
Apnea is prolonged, starting immediately after the epileptic cry, and lasts throughout the entire tonic and clonic phases and, occasionally, into the initial postictal period. Heart rate and blood pressure increase markedly to double their pre-seizure values.
Bladder (intravesicular) pressure increases 6-fold, but urinary incontinence is prevented during the convulsions because of tonic contraction of the bladder sphincter muscles. Incontinence of urine occurs only in the immediate postictal phase because of relaxation of the urinary sphincter muscles. It does not occur earlier in the attack. It may be doubted whether the loss of urine and feces are due to epileptic spasms; they may occur after the fit and be due to loss of control (Jackson 1878).
The patient’s pupils dilate in the tonic phase and become unresponsive to light. Hippus (rhythmic pupillary contraction and dilatation) occurs in the clonic phase. Unvarying pupil dilatation occurs again in the immediate postictal phase.
Skin color changes are profound. Cyanosis caused by apnea-induced hypoxia is apparent in the convulsive stages, whereas pallor becomes apparent in the immediate postictal phase. Piloerection is common. Glandular hypersecretion produces marked sweating, hypersalivation, and tracheobronchial secretions.
Postictal metabolic and hormonal changes. Postictal metabolic and hormonal changes occurring immediately after GTCS last for approximately 1 to 2 hours. The most consistent changes are the elevation of serum lactate (56), prolactin (13), and serum creatine kinase. Rise of prolactin peaks 20 minutes postictally to 5 to 30 times the baseline levels and remains significantly elevated for 2 hours (21). Also, it has been reported that serum metalloproteinase 9 levels are significantly increased 1 to 3 and 24 hours after GTCS and decrease to control levels 72 hours after seizure (17).
Variants of GTCS. It should be emphasized that GTCS often vary in severity, duration of the tonic and clonic phases, and duration and symptoms of the recovery period. The clonic or tonic phase may predominate, recovery may be very slow or relatively fast, and postictal symptoms may be severe or relatively mild. The tonic phase may be brief, followed by lengthy clonic convulsions. In children, the tonic phase may be longer than the clonic phase. These variants of GTCS are sometimes difficult to differentiate from a genuine tonic or clonic seizure.
Another variant emphasized by Gastaut and Broughton manifests with significant asynchrony (up to several seconds) between the right and left sides of the body during the tonic and clonic convulsions (single GTCS with bilateral motor asynchrony? or two independent unilateral seizures?) (33).
Circadian distribution and precipitating factors of GTCS. GTCS may occur randomly at any time, day or night, and predominately in sleep or awakening. They are often precipitated by sleep deprivation, fatigue, excessive alcohol consumption, as well as external photic and other stimuli.
Generalized tonic-clonic status epilepticus. GTCS may fail to terminate spontaneously and may enter into a self-perpetuating, self-sustaining process of tonic-clonic status epilepticus (75).
See MedLink Neurology article: Generalized tonic-clonic status epilepticus.
GTCS in adults versus GTCS in children. Total seizure duration, tonic phase, postictal EEG suppression, and recovery phases were found to be significantly shorter in children than in adults (31). With cessation of medication, total seizure duration was significantly increased by a mean value of 8 seconds in children and 11 seconds in adults (31). However, the mean duration of GTCS (74.6 s) did not correlate with age, gender, location of MRI brain abnormalities, or duration of epilepsy (59). In contrast, the duration of seizures with onset age of younger than 2 years was significantly longer than those with onset age of older than 2 years.
One study focused on autonomic changes following generalized tonic-clonic seizures in adult and pediatric patients with epilepsy (68). It was found that the duration of post-ictal generalized EEG suppression strongly correlated with age and that age is a significant determinant of the sympathetic and parasympathetic response following a GTCS. Given the same post-ictal generalized EEG suppression duration, pediatric patients demonstrated stronger sympathetic activation and higher vagal suppression.
The prognosis of generalized onset tonic-clonic seizures in terms of long-term recurrence is syndrome- and cause-dependent. They may be:
|
• a one-off event or a one-off cluster of events in a short period of the patient’s life, such as in febrile GTCS or acute GTCS. | |
|
• infrequently recurrent in a lifetime, as seen in most cases of idiopathic generalized epilepsy. | |
|
• easily controlled with the appropriate prophylactic antiepileptic drugs or frequently recurrent and intractable. |
However, even one GTCS may be fatal. The complications of GTCS are either from a direct effect of the GTCS manifestations on the body or by accidents occurring as a result. Trauma of differing types and severity is the most likely complication. Skin changes, aspiration pneumonia, pulmonary edema, and death may occur.
Oral lacerations involving the tongue, lip, and cheek probably occur in 1 of 10 GTCS (50). These are more often unilateral than bilateral. Placing an object in the patient’s mouth to prevent tongue biting is erroneous and causes more harm than good. Mouth closure is so forceful that it can amputate a finger placed between the teeth or break the teeth if the object is metallic.
Skin abrasions and lacerations are caused by external trauma during GTCS. Skin petechial hemorrhages over the face, neck, and chest, as well as conjunctival hemorrhage, are due to capillary bleeding.
Craniocerebral trauma is caused by falls. Severe burns may occur while cooking or when falling into a fire.
Stress fractures as a direct consequence of GTCS without direct trauma occur in 0.3% of cases and are more common in elderly people (01; 77). They mainly affect the thoracic and lumbar vertebrae and are usually asymptomatic. More serious fractures are well reported in the literature. Vertebral compression and other fractures are the main complications during epilepsy monitoring when antiepileptic drugs are withdrawn.
Aspiration pneumonia is an uncommon (around 4 in 1600 patients) (19) but potentially life-threatening complication caused by the aspiration of saliva, tracheobronchial secretions, or vomiting. It occurs in the postictal rather than the ictal phase of GTCS, when oral secretions are not usually increased and there is cessation of respiratory movements. The risk of aspiration pneumonia is higher in institutionalized patients and in those with swallowing difficulties, increased oral secretions (19), lowered resistance to infection, or depressed airway reflexes from drug or alcohol abuse. Positioning the patient in a lateral decubitus position in the immediate postictal phase significantly decreases the risk of aspiration.
Pulmonary edema is rare and potentially life-threatening if untreated. It is usually misdiagnosed as aspiration pneumonia. Its exact pathophysiology is unknown. Pulmonary edema usually resolves rapidly with oxygen, independent of diuretic use. It is associated with high mortality, mainly in older patients.
Accidental (falls, drowning) and non-accidental deaths (aspiration, pulmonary edema, cardiac arrhythmias, cardiac asystole) may occur during or immediately after GTCS. Furthermore, the risk of sudden unexplained death in epilepsy is significantly higher in patients with GTCS than in patients with other types of seizures (31; 69). Adults have a tenfold higher incidence of sudden unexplained death in epilepsy than children. Identifiable electroclinical differences between adult and pediatric GTCS may be relevant in explaining lower sudden unexplained death in epilepsy risk in children. Postictal generalized EEG suppression and postictal tonic electromyography activity are possible biomarkers of sudden unexplained death in epilepsy risk (31; 62).
In a multivariate-adjusted logistic regression model, left atrial diameter in echocardiography and QTc in ECG were significantly and independently associated with GTCS patients in comparison with healthy subjects (63).
Troponins are very sensitive biomarkers of myocardial injury and can be elevated after a GTCS (27). Patients at risk are the elderly and those with cardiovascular risk factors. Elevation of troponin levels after a GTCS reflects a minor ischemic cardiac injury related to the demand ischemia during the sympathetic overactivity that accompanies a GTCS (27). A multicenter observational, cross-sectional study assessed accidental injuries in patients with generalized tonic-clonic seizures of any type (67). The following are the numbers of generalized tonic-clonic seizures in the last 12 months: one (41.9%), two to five (42.4%), and greater than five (15.8%). In total, 59.6% of the patients had experienced at least one accidental injury associated with tonic-clonic seizures in the last 12 months, the most common being head injuries (35.5%), dental injuries (4.9%), burns (4.9%), and fractures (3.9%). A total of 25.1% had suffered at least one serious injury. Risk factors associated with suffering an injury were etiology (symptomatic or with unknown etiology focal and idiopathic generalized epilepsy), number of seizures in the last year (more than one), and psychiatric comorbidities (67).
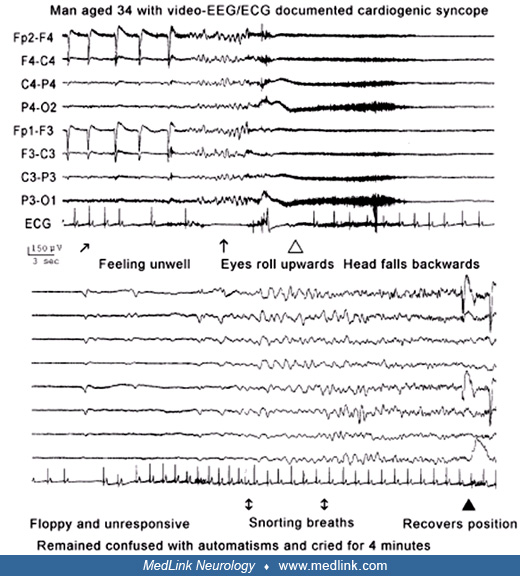
A 34-year-old man was referred for routine EEG because of two episodes misdiagnosed as GTCS in the last 2 months. The first occurred on his way home after college. He did not recall events until waking in the ambulance with the paramedics telling him that he had had a seizure. He had no memory of the preceding 30 minutes. He had bitten his tongue, but there was no incontinence. This was considered a GTCS, and treatment with valproate was initiated.
During routine video-EEG, this patient developed sinus bradycardia and then ventricular standstill for 9 seconds, with one escape ectopic beat as documented with ECG.
After this video-EEG, a cardiac pacemaker was implanted, and the patient remained well in the next 6 months of follow-up.
According to the ILAE definitions, generalized seizures originate at some point within and rapidly engage bilaterally distributed networks. Such bilateral networks can include cortical and subcortical structures but do not necessarily include the entire cortex. Although individual seizure onsets can appear localized, the location and lateralization are not consistent from one seizure to another. Generalized seizures can be asymmetric (04; 15; 29; 28).
Generalized onset tonic-clonic seizures are most common in idiopathic generalized epilepsies in otherwise normal people.
The pathophysiology of generalized tonic-clonic seizures (GTCS) is not precisely known, as indicated by the ILAE Core Group report (24):
|
GTCS involve brain stem, possibly prefrontal, and basal ganglia mechanisms. Ictal initiation of primarily bilateral events are predominantly disinhibitory, but other mechanisms are responsible for ictal evolution to the clonic phase, involving gradual periodic introduction of seizure-suppressing mechanisms. Several discrete types might be identified – future investigation is needed to determine which of these types represent unique phenomena: | ||
|
• reactive GTCS (acutely provoked seizures) | ||
|
Some experimental evidence suggests that the mechanisms of ictal initiation could be different for some or even all of these subtypes of GTCS, and that there may even be more than one mechanism of initiation within each of the subtypes. | ||
The centrencephalic, corticoreticular, and cortical theories that have been proposed explain the synchronous and bilateral nature of the generalized discharges associated with absence seizures, GTCS, and loss of consciousness.
The analysis of these theories by their main protagonists can be found in the classic book The Physiopathogenesis of the Epilepsies (34) and in reviews (12; 22; 26). Gastaut attributed “the entire GTCS to be a diffuse subcortical reticular discharge, which leads to activation of inhibitory systems and, at the end of the seizure, to a transient postictal state of cortical depression” (33).
Animal and human data suggest that the various types of generalized epileptic seizures involve selective networks (while sparing others) that engage in abnormally synchronous and high-frequency neuronal oscillation. The pathophysiology of absence seizures is better understood than that of any other type of generalized seizure (see MedLink clinical summary “Typical absences”). The pathophysiology of GTCS is different than that of absence seizures, but there may be a similar interplay of oscillations in networks intensely involving not the whole brain homogeneously but, rather, the focal bilateral regions most intensely, especially the frontal and parietal association cortex, thalamus, basal ganglia, and brain stem (09; 08; 06). Other cortical regions appear to be relatively spared, or at least less intensely involved (37). The cerebellum may also play a role in GTCS termination and postictal suppression.
In mammals, there are two sets of convulsive seizure circuitry: the forebrain and the brain stem seizure circuitry. In humans, focal seizures correspond with those of the forebrain circuitry, GTCS with those of the brain stem circuitry, and focal onset TCS with forebrain seizures that secondarily evoke brain stem seizures (46). The clinical and electrophysiological manifestations of GTCS (including initiation, continuation, and termination) in humans closely resemble generalized brain stem seizures in genetically epilepsy-prone rats (GEPR) and Papio papio (46).
Advanced functional neuroimaging techniques have been used in the study of spontaneous GTCS in patients with epilepsy (09; 40; 44) or GTCS induced by electrotherapy in psychiatric patients (09). On the basis of their findings, Blumenfeld and associates proposed a model in which GTCS involve the cortical regions of seizure onset and selective bilateral regions of seizure propagation (09). Corresponding subcortical networks are also involved, whereas other cortical regions may be relatively spared or even inhibited during seizures. The behavioral manifestations of GTCS can be explained by selective abnormal regional cortical excitation and inhibition, together with the involvement of brain stem networks (09).
Certain cortical regions, especially the insular, cingulate, and orbitofrontal cortices, are key structures that integrate sensory input and influence diencephalic and brainstem regions regulating blood pressure, cardiac rhythm, and respiration. Cortical thickening and thinning was documented in cardiovascular and somatosensory areas of patients with generalized tonic-clonic seizures (58). These may contribute to dysfunctional cardiorespiratory patterns during seizures, as well as longer-term sudden unexplained death in epilepsy risk (58).
See underlying disorders and Table 4.
Avoidance of precipitating factors and appropriate prophylactic antiepileptic drug treatment are important.
The differential diagnosis should distinguish generalized onset tonic-clonic seizures from nonepileptic paroxysmal events and focal onset tonic-clonic seizures (60; 49). Subsequently, syndromic diagnosis includes differentiation from mainly other idiopathic generalized epilepsies.
The diagnosis is almost always based solely on the clinical history, which should be obtained in a skilled way, often requiring lengthy interrogation(s) of the patient and witnesses. Children also (if verbal) have surprising insight into their illnesses. In taking the medical history, every piece of information should be patiently gathered in order to synthesize the whole pattern of transient events, from the time they started to their end and up to normality. This should include:
|
• Details of the paroxysmal events (and not just of the most dramatic ones) |
Differentiation from non-epileptic paroxysmal events. Considering their dramatic and stereotypical features, generalized tonic-clonic seizures should not be difficult to diagnose. So, why are non-epileptic paroxysmal events so frequently misdiagnosed as GTCS and, less often, vice versa? The main reasons for misdiagnosis are as follows:
|
• The patient is amnesic of the ictal events, although other symptoms preceding GTCS are often of diagnostic value. | |
|
• The events have not been adequately witnessed, although the physical and mental consequences of GTCS are often of diagnostic value. | |
|
• The events, even when adequately witnessed and identified, are abbreviated in diagnostic terms (tonic-clonic seizures or grand mal or syncope or pseudoseizure) rather than describing in detail what happened. |
Of the numerous imitators of epileptic seizures, syncope, and convulsive nonepileptic paroxysmal events are more likely to be misdiagnosed as GTCS.
Syncope. Syncope (neurally mediated or cardiogenic) is commonly misdiagnosed as GTCS.
The setting and stimulus are the most important factors in allowing the presumptive diagnosis of syncope. In differentiating syncope from GTCS, textbooks usually emphasize the characteristics of syncope listed in Table 1. However, there are also a good number of important points to consider, and these are listed in Table 2.
• Precipitating factors or triggers such as upright position, bathroom, crowded and humid places, lack of food, unpleasant circumstances, and venipuncture | ||
• Prodromal symptoms of cerebral ischemia, such as dizziness, greying of vision, and tinnitus | ||
• Gradual onset over seconds to a minute | ||
• Pallor and sweating | ||
• Lack or rare occurrence of convulsions (other than myoclonic jerks), incontinence of urine, or tongue biting | ||
• Brief duration (1 to 30 seconds) | ||
• Rapid recovery with no postictal confusion | ||
| ||
• Convulsions occur in 70% to 90% of syncopes, and symptoms include myoclonus, tonic flexion or extension, more complex movements, and automatisms such as lip licking, chewing, or fumbling. | ||
• Visual hallucinations (a perception of grey haze, colored patches, glaring lights, or more complex scenes involving landscapes, familiar situations, or people) and, less often, auditory hallucinations (rushing and roaring sounds, traffic and machine noises, and talking and screaming human voices, but never intelligible speech) are frequent (60%) in both convulsive and non-convulsive syncope (53). | ||
• Syncope usually happens in an upright position but may also occur in the supine position. | ||
• Sudden onset, urinary incontinence, and trauma are not uncommon. | ||
• Abdominal pain that may be confused with epigastric aura may occur at onset. Auras comprising epigastric, vertiginous, visual, or somatosensory experiences occur both in neurally mediated and cardiogenic syncope. | ||
• Pallor and sweating are not invariable symptoms at onset and may be symptoms of autonomic epileptic seizures with or without focal onset tonic-clonic seizures. | ||
• Complete recovery may not be rapid and postictal confusion may occur, although neither of them reaches even close to the severity of that after GTCS. | ||
• Eyes are always open during syncope, as in GTCS, and the most consistent oculomotor sign is an upward turning of the eyes early in its course, which may be followed by lateral eye deviation (54). | ||
| ||
Of the various cardiogenic syncopes, the long QT syndrome is of particular significance because it may be associated with convulsive syncopes that closely imitate GTCS. The mechanism of the syncope is a ventricular tachyarrhythmia, normally Torsades de pointes, triggered by fear or fright, particularly during exercise, especially when that exercise is emotionally charged, and during sleep.
Psychogenic nonepileptic seizures. Psychogenic non-epileptic seizures are among the commoner recurrent paroxysmal events imitating and misdiagnosed as GTCS (35; 65). Convulsive psychogenic status epilepticus (commonly referred to as convulsive pseudostatus epilepticus) is common in patients with psychogenic non-epileptic seizures, and it is often misdiagnosed as genuine and life-threatening convulsive status epilepticus (43; 66; 23; 42). These patients commonly have multiple episodes of “status” and receive intensive care unit management. They usually have a history of other unexplained illness and deliberate self-poisoning. Episodes of anticonvulsant-induced respiratory arrest may occur.
The key differences between psychogenic non-epileptic seizures and GTCS are detailed in Table 3.
• Often precipitated by stressful circumstances (stress is also a precipitating factor in epilepsies) | ||
• Can be induced in response to suggestion (useful in diagnostic provocative activating techniques; also called “inductions”) | ||
• Occur in wakefulness and in the presence of witnesses (not unusual in epilepsies) | ||
• Lack stereotypical characteristics | ||
• “Convulsions” consist of asynchronous, asymmetrical, waxing and waning, accelerating and decelerating, convulsive-like movements, often with pelvic thrusts, flailing, and tremors. These may be interrupted or resistant to restraint, and imitate seizures from the supplementary somatosensory area and not GTCS. | ||
• Eyes are commonly closed (probably the most important symptom to differentiate from GTCS and syncope, in which the eyes are invariably open). | ||
• Attempts to open the eyes passively often result in tightening of the eyelids (this may also occur in postictal confusion after GTCS). | ||
• “Give-way weakness” on examination is common. | ||
• Consciousness may be retained throughout or shows marked fluctuations. | ||
• There is no actual postictal confusion. The patient may become emotional and cry after the end of the non-epileptic seizure (this symptom is not unusual in patients with epileptic seizures). | ||
• Postictal breathing is more rapid, normalized more rapidly, and is unlikely to be stertorous respirations. | ||
• Postictal behavior of responding to questions in a whispered voice or responding to commands with focal motor responses is common and may be helpful in the diagnosis of psychogenic non-epileptic seizures (11). | ||
• Intractable to antiepileptic medication (also occurring in epilepsies) | ||
• Diagnostic traps: at least one of the usual signs associated with GTCS (tongue biting, falling, or incontinence) is reported by more than half (66%) of the patients with nonepileptic seizures (18). | ||
• At least one of the usual signs associated with GTCS (tongue biting, falling, or incontinence) is reported by more than half (66%) the patients with non-epileptic seizures (18). | ||
| ||
Differentiation from focal onset tonic-clonic seizures. Differentiation of generalized onset from focal onset tonic-clonic seizures may be easy when patients also have other types of seizures:
• Absences and myoclonic jerks in GTCS |
EEG frequently shows:
• Generalized discharges of spike/polyspike wave in GTCS |
Brain MRI may document structural abnormalities in FBTCS.
According to one report, asymmetry of limb movements in the clonic phase, side-to-side axial movements, and asymmetric seizure termination occur more frequently (p < 0.05) in focal compared to generalized onset tonic-clonic seizures (30).
Generalized onset tonic-clonic seizures occur in syndromes of idiopathic generalized epilepsy (Table 4). Patients with the syndromes of epilepsy with GTCS alone and epilepsy with phantom absences and GTCS always manifest with generalized onset TCS (61). Whether GTCS of epileptic encephalopathies are of generalized or focal onset is debated.
IGE syndrome | Prevalence | Patients with GTCS |
IGE with GTCS alone | Uncertain; 1% to 5% of patients with GTCS only | 100% |
Juvenile myoclonic epilepsy | 2.7% to 10.2% of patients over 14 years old with epilepsy | Over 90% |
Juvenile absence epilepsy (JAE) | Unknown; probably 8% of patients with IGE | 80% |
Childhood absence epilepsy (CAE)* | 10% of children less than 15 years old with epilepsy* | 10% may develop solitary of infrequent GTCS in adolescence or adult life* |
Epilepsy with myoclonic absences | Rare; less than 0.5% of patients with IGE | 50% to 75% prior or concurrently with the absences |
Epilepsy with myoclonic-atonic seizures (Doose syndrome) | 1% to 2% of childhood epilepsies? | 75% febrile and afebrile GTCS usually preceding the onset of myoclonic-atonic seizures |
IGE with phantom absences | 10% of IGE and 3% of patients older than 16 years with epilepsy | 100%, though some patients (possibly less than 10%) are not identified if they do not develop GTCS |
Perioral myoclonia with absences | Rare; less than 1% of children with typical absences seizures | 100% |
Eyelid myoclonia with absences (Jeavons syndrome) | 13% of patients with IGE and absences and 3% of adult patients with epilepsy | Probably unavoidable in all untreated patients |
Autosomal dominant cortical tremor, myoclonus and epilepsy | Unknown; mainly prevalent among Japanese and Italian populations | 80% |
| ||
Patients with generalized onset tonic-clonic seizures of idiopathic generalized epilepsy may need only EEG and ECG. Brain imaging is obtained in order to exclude the possibility of focal onset generalized tonic-clonic seizures (SGTCS).
Interictal EEG. Interictal EEG of patients with generalized tonic-clonic seizures varies considerably, from entirely normal to severely abnormal, depending on the underlying epileptic syndrome, frequency of seizures, and treatment. Idiopathic generalized epilepsy–related interictal EEG abnormalities usually consist of generalized discharges of spike/polyspike waves appearing on a normal background. Focal EEG abnormalities are frequent in idiopathic generalized epilepsy and should not be interpreted as evidence of focal epilepsy. An awake EEG may be normal, but significant abnormalities may occur in sleep EEG or on awakening. Hyperventilation, photic stimulation, and other modes of activation are useful in revealing precipitating factors.
Ictal EEG. In routine EEG, the electrical signature of GTCS is usually masked by muscle artifacts in all derivations except those from the vertex. Accurate EEG description has mainly been derived from patients who were pharmacologically paralyzed at the time of GTCS (33). The ictal EEG discharges are diffuse and generalized, with approximately synchronous and symmetrical amplitude on the corresponding areas of both sides.
The onset of the tonic phase is marked by a brief (1-3 s) period of flattening or with low-voltage fast rhythmic activity at about 20 Hz or fast spiking. This gradually becomes more synchronized, increases in amplitude, and slows in frequency to a sustained 10 Hz rhythm (“epileptic recruiting rhythm” is the preferred term of Gastaut). In the intermediate phase and clonic phase, slow waves of increasing amplitude and decreasing frequency superimpose and gradually rhythmically interrupt the 10 Hz fast rhythms of the tonic phase. Finally, the EEG assumes a pattern of repetitive, high-amplitude polyspike–slow-wave complexes that increase in amplitude and slow down to 1 Hz. The clonic convulsions correspond to the polyspikes, whereas the periodic muscle atonia corresponds to the slow waves.
The postictal period is characterized by diffuse background suppression (flat or isoelectric EEG) or a burst suppression or triphasic wave pattern of several seconds to 2 or 3 minutes (longer in children). This is followed by diffuse slow waves that gradually increase in frequency and amplitude. The periods of coma and confusion and the return to normality correlate fairly well with dominant delta activity, theta activity, and the return of a normal alpha rhythm after several minutes.\
Variants of tonic-clonic seizures have expected EEG patterns based on clinical grounds. Those with relatively prolonged tonic or clonic phases have correspondingly longer periods of recruiting rhythm or polyspike-wave discharges.
Surface electromyography (EMG). Surface electromyography shows sustained and continuous muscle contraction at around 50 Hz, which corresponds to the tonic phase of GTCS and is concurrent with the EEG recruiting rhythms (33; 16). This is followed by repetitive EMG bursts—EMG paucity at the frequency of the slow waves of the intermediate phase and spike-wave complexes of the clonic phase. The EMG bursts correspond to the clonic convulsions. Each slow wave is associated with a decrease and then abolition of muscle tone.
Accelerometry-based wearable sensors allow long-term reliable seizure monitoring in the free-living environment and, thus, contribute to ascertaining seizure frequency and, thereby, better seizure management (47).
The ILAE Neurophysiology Task Force has published a comprehensive 2-part review on the role of EEG in the diagnosis and classification of epilepsy syndromes: a tool for clinical practice (51; 52).
Serum levels of lactate and prolactin are raised in generalized tonic clonic seizures and focal onset tonic clonic seizures, which are useful in their differentiation from syncope and nonepileptic attacks (13; 21). Early postictal serum lactate concentrations are superior to serum creatine kinase concentrations in distinguishing generalized tonic-clonic seizures from syncopes (56). Serum prolactin levels are normal in generalized tonic-clonic status epilepticus.
Lifestyle and avoidance of seizure precipitants. Advice about circadian distribution, lifestyle, and seizure precipitants may be as important as drug treatment (49). Avoidance of precipitating factors and adherence to long-term medication are essential to avoid seizures. Some patients experience GTCS only after encountering precipitating factors. Patients may have myoclonic jerks despite treatment only after excessively violating these factors, and others may have seizures exclusively after awakening, which may not affect their daily duties. Advice on the risk of sleep deprivation and alcohol is mandatory; avoidance of alcohol indulgence and compensation for sleep deprivation are essential.
Prophylactic antiseizure drug therapy. GTCS occur in patients with syndromes of idiopathic generalized epilepsy. Therefore, antiseizure drug choice and length of treatment are syndrome-related. Treatment of idiopathic generalized epilepsy with old and new antiseizure drugs is demanding (Table 5). There are two main reasons for this. First, some antiseizure drugs of benefit in focal epilepsies may be deleterious in idiopathic generalized epilepsy. Second, the efficacy of antiseizure drugs differs even within seizures of idiopathic generalized epilepsy. This is because the generation of absences, for example, is a result of a predominance of inhibitory activity, in contrast to generalized convulsive seizures, in which an excess of excitatory activity is present (08).
|
Antiseizure drugs licensed for GTCS (sole or adjunctive) |
Other types of seizures |
|
Carbamazepine |
Exaggerates absences and myoclonic jerks |
|
Clonazepam |
Also licensed for absences and myoclonic jerks and may exaggerate GTCS in JME |
|
Lamotrigine |
Also licensed for absences but exaggerates myoclonic jerks |
|
Levetiracetam |
Also licensed for myoclonic jerks |
|
Perampanel |
Adjunctive treatment |
|
Phenobarbital |
Also licensed for myoclonic jerks but exaggerates absences |
|
Phenytoin |
Exaggerates absences and myoclonic jerks of JME |
|
Primidone |
Also licensed for myoclonic jerks but exaggerates absences |
|
Topiramate |
Not licensed for absences or myoclonic jerks |
|
Valproate |
Also licensed for absences and myoclonic jerks |
|
| |
Most seizures and syndromes of idiopathic generalized epilepsy respond well to the appropriate antiseizure drug, but treatment is often life-long.
Children and women with idiopathic generalized epilepsy merit special concern and management. The fact that almost 50% of patients with idiopathic generalized epilepsy are taking “ill-advised antiseizure drug” medication (03; 74) is a grave problem that needs to be addressed.
Misdiagnosis and inappropriate antiseizure drug treatment are confounding factors that account for avoidable major intractability, morbidity, and sometimes mortality in idiopathic generalized epilepsy.
See Medlink Neurology articles: Pharmacological treatment of epilepsy in adolescents and adults and Anticonvulsants.
Prophylactic antiseizure drug therapy of patients with newly identified GTCS of idiopathic generalized epilepsy. Before starting prophylactic antiepileptic medication in a patient with newly diagnosed PGTCS, a physician should be confident of the following:
|
(1) The patient unequivocally has GTCS. This requires definite exclusion of non-epileptic paroxysmal seizures and FBGTCS. | |
|
(2) The patient needs prophylactic antiseizure drug treatment. This requires precise diagnosis of etiology, epileptic syndrome, frequency, and severity of GTCS; the likelihood of relapse or remission; precipitating factors and patient/family concerns; and understanding of the risks versus the benefits of the antiseizure drug. Hard-and-fast rules are not always applicable. | |
|
(3) The most appropriate antiseizure drug is selected for this particular patient with this particular type of epileptic syndrome. The appropriate antiseizure drug is that which is the most likely to be truly prophylactic as monotherapy for the seizures of the patient without causing undue adverse reactions. | |
|
(4) The starting dose and titration of the selected drug should be in accordance with the appropriate recommendations, the age, and, primarily, the particular needs of the treated patient. All these should be thoroughly explained to the patient/guardian and ensured that they are well understood. |
In the ILAE report of evidence-based guidelines on initial monotherapy efficacy and effectiveness, the major conclusions for GTCS are as follows (36):
|
• Absence of class I and class II randomized control trials | |
|
• No antiseizure drugs reach the highest levels of evidence (levels A and B) for efficacy/effectiveness for adults with GTCS. | |
|
• No adequate comparator exists for this category. | |
|
• Class IV evidence suggests that carbamazepine, oxcarbazepine, and phenytoin may precipitate or aggravate PGTCS and, more commonly, other generalized seizure types in these patients; therefore, these drugs should be used with caution in these patients. |
In deciding the first monotherapy option for patients with PGTCS, it should be remembered that antiseizure drug prophylactic therapy is often lifelong in most idiopathic generalized epilepsies, and, therefore, adverse effects from chronic use should be considered.
Prophylactic antiseizure drug therapy of patients with intractable GTCS of idiopathic generalized epilepsy. In general, GTCS and idiopathic generalized epilepsy have a better prognosis with, and a more favorable response to, appropriate antiseizure drugs than structural/metabolic and focal epilepsies. Most patients with idiopathic generalized epilepsy are easily controlled with appropriate medication; refractory patients are rare (32). Prevalence of intractable idiopathic generalized epilepsy may be in the order of 10% to 30%, and this is mostly due to delayed or inappropriate treatment (73).
Management of patients with intractable GTCS of idiopathic generalized epilepsy, provided that they truly suffer from epileptic seizures, should include the following steps:
|
(1) Based on clinical and EEG evidence, establish whether patients also have seizures other than GTCS (absences, myoclonic jerks), and make sure that these are generalized and not focal onset TCS. Previous EEGs, particularly in untreated stages, are invaluable. | |
|
(2) Establish precipitating factors and circadian distribution, as well as their effect with regard to intractability. | |
|
(3) List, in chronological order, all antiseizure drugs previously used and in what doses and combinations. Establish which antiseizure drugs were beneficial and which made the situation worse. | |
|
(4) Thoroughly consider the current situation regarding the seizures that are more predominant and more disturbing and antiseizure drugs that are definitely or possibly effective, ineffective, or contraindicated with respect to seizures and side effects. | |
|
(5) Thoroughly consider all of the above, including compliance, in making a definite plan of which antiseizure drugs should be withdrawn and which of the indicated antiseizure drugs should be increased in dosage or added to the scheme. | |
|
(6) Of the newer antiseizure drugs, those that are likely to be effective as monotherapy are also the most likely to be suitable in polytherapy. The order of priority may be levetiracetam, lamotrigine, topiramate, and zonisamide. |
Older antiseizure drugs in the treatment of GTCS (in the order of efficacy). Valproate has superior efficacy over all other antiseizure drugs in all seizures and syndromes of idiopathic generalized epilepsy. Valproate monotherapy controls GTCS in 70%, myoclonic jerks in 75%, and absence seizures in 75% of patients with idiopathic generalized epilepsy. The major problem is that valproate is undesirable in women because of its teratogenic effects and its tendency to cause weight gain and polycystic ovary syndrome.
Phenobarbital was historically the preferred drug in the treatment of GTCS and juvenile myoclonic epilepsy. It worsens absences. It is rarely used in developed countries because of side effects.
Phenytoin is effective in GTCS. It deteriorates absences and possibly myoclonic jerks; however, it is rarely used in developed countries because of side effects.
Carbamazepine is considered effective in GTCS, but it may be avoided in idiopathic generalized epilepsy because it aggravates absences and myoclonic jerks (74).
Clonazepam, even in small doses of 0.5 to 1 mg, is probably the most potent anti-myoclonic drug, with some anti-absence effect. It may deteriorate GTCS or, by suppressing myoclonic jerks, deprive patients of the warning symptoms of an impending GTCS.
Acetazolamide has been used for treating GTCS in cases resistant to conventional treatment, although its use may induce nephrolithiasis.
Newer antiseizure drugs in the treatment of GTCS (in the order of efficacy). Because of levetiracetam’s efficacy in all types of seizures (generalized and focal), including PGTCS, and its safer adverse effects profile, it appears to be the most promising substitute for valproate.
Lamotrigine is effective in GTCS and absence seizures but aggravates myoclonic jerks. It has important pharmacodynamic interactions with valproate.
Topiramate is also effective in many types of seizure, including GTCS, but its adverse effect profile is of concern.
Perampanel and lacosamide are the newest antiseizure drugs used for the treatment of GTCS (78).
Zonisamide may be an additional therapeutic option, although randomized controlled trials in adults with PGTCS are lacking.
Rufinamide and clobazam have been approved for Lennox-Gastaut syndrome and may be effective for GTCS. Cannabidiol is approved for seizures associated with Lennox-Gastaut syndrome, Dravet syndrome, and tuberous sclerosis complex.
Cenobamate and brivaracetam have been approved for focal seizures, and although they have not specifically been tested for GTCS, they may be effective.
An expert evaluation of regulatory data and five criteria for antiepileptic drug selection for the treatment of generalized tonic-clonic seizures has been published (71). Eight antiepileptic drugs (carbamazepine, clobazam, lamotrigine, levetiracetam, perampanel, phenytoin, topiramate, and valproate) approved in Europe and in the United States for the treatment of both focal and generalized onset of tonic-clonic seizures were evaluated using five criteria: (1) efficacy, by seizure type; (2) adverse effects; (3) interactions; (4) adherence and dosing; and (5) mechanism of action. The authors found the following results: (1a) there is class 1 evidence of the efficacy of only four antiepileptic drugs in controlling generalized onset tonic clonic seizures (lamotrigine, levetiracetam, perampanel, and topiramate); (1b) there is no class 1 evidence of the efficacy of any antiepileptic drug in focal onset tonic clonic seizures, although some evidence from pooled/subgroup analyses or meta-analyses supports the use of the four antiepileptic drugs (levetiracetam, perampanel, topiramate, and with less robust data, lamotrigine); (2) antiepileptic drugs are associated with different, but to some extent overlapping, common adverse effect profiles but have differing idiosyncratic adverse effects; (3) pharmacokinetic interactions are seen with most, but not all, antiepileptic drugs and are most common with carbamazepine and phenytoin; (4) good adherence is important for seizure control and is influenced by frequency of dosing, among other factors; (5) mechanism of action is also a consideration in rationalizing antiepileptic drug selection when switching or combining them (71).
Intranasal midazolam during presurgical epilepsy monitoring is well tolerated, delays seizure recurrence, and protects from generalized tonic-clonic seizures (48).
Drug withdrawal. Most syndromes of idiopathic generalized epilepsy with GTCS are life-long. Relapses are probably unavoidable after the withdrawal of medication. However, if seizures are mild and infrequent or increasing with age and treatment duration (41), drug withdrawal could be attempted. This should be in small decrements, probably over years, warning the patient that the reappearance of even minor seizures, such as absences or myoclonic jerks, mandate continuation of treatment. EEG confirmation of the seizure-free state is needed during the withdrawal period. However, a normal EEG does not mean that the patient does not have active epilepsy and that antiseizure drug withdrawal is safe. Conversely, ictal EEG abnormalities with seizure manifestations (eg, jerks or absences) are a definite indicator of continuing with proper antiseizure drug treatment.
Non-EEG devices for home monitoring. Non-EEG devices are commercially available for long-term home monitoring of convulsive epileptic seizures but with little scientifically valid information and no consensus on which system works for which seizure type or patient (76; 39). However, accelerometry-based wearable sensors allow long-term reliable seizure monitoring in the free-living environment (47).
In pregnancy, GTCS impose an increased risk of damage to the mother and her unborn baby (64). Of 3806 pregnancies of 3451 women with epilepsy taking part in the European and International Registry of Antiepileptic Drugs and Pregnancy (EURAP), 66.6% remained seizure-free throughout pregnancy (02). GTCS occurred in 15.2% of the pregnancies. Women with idiopathic generalized epilepsies were more likely to remain seizure-free (73.6%) than women with localization-related epilepsy (59.5%; p < 0.0001). Compared with other monotherapies, pregnancies exposed to lamotrigine were less likely to be seizure-free, 58.2% (p < 0.0001); had more GTCS, 21.1% (p < 0.0001); had a greater likelihood of deterioration in seizure control from first to second or third trimesters, 19.9% (p < 0.01); and were more likely to require an increase in drug load, 47.7% (p < 0.0001). Although the majority of women remain seizure-free throughout pregnancy, a more proactive approach to adjusting the dose of all antiseizure drugs in pregnancy should be considered, in particular for those pregnancies with seizures occurring in the first trimester and those exposed to lamotrigine, in order to reduce the risk of deterioration in seizure control (02).
Valproate and topiramate are highly teratogenic (see MedLink Neurology article: Pregnancy and epilepsy).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Henry Hasson MD
Dr. Hasson of Albert Einstein College of Medicine has no relevant financial relationships to disclose.
See Profile
Solomon L Moshé MD
Dr. Moshé of Albert Einstein College of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jan. 20, 2025
Epilepsy & Seizures
Jan. 09, 2025
Epilepsy & Seizures
Jan. 09, 2025
Epilepsy & Seizures
Dec. 23, 2024
Epilepsy & Seizures
Dec. 19, 2024
Epilepsy & Seizures
Dec. 03, 2024
Epilepsy & Seizures
Dec. 03, 2024
Epilepsy & Seizures
Dec. 02, 2024