

Neuro-Ophthalmology & Neuro-Otology
Diplopia
Jan. 08, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Idiopathic intracranial hypertension is a disorder of increased intracranial pressure that is most commonly seen in obese women of childbearing age. The pathophysiology remains under investigation. Symptoms include headache, transient visual obscurations, and pulsatile tinnitus. Papilledema is the hallmark sign of this disorder. Untreated, it can result in optic nerve injury, consequent visual field defects, and blindness. It continues to be a diagnostic and therapeutic challenge, and the incidence is rising as obesity becomes more prevalent. This update reviews the clinical features of idiopathic intracranial hypertension in adults and children, conditions with which it can be confused, diagnostic evaluation and criteria, and current therapeutic options.
|
• Headaches, transient visual obscurations, and pulsatile tinnitus are the most frequent early manifestations of idiopathic intracranial hypertension in adults. | |
|
• Obese women of childbearing age are most commonly affected by idiopathic intracranial hypertension, but the syndrome may occur in children, nonobese patients, and those over 45 years of age. | |
|
• Diagnosis of exclusion and careful history, examination, and work-up (neuroimaging, CSF examination) are required to rule out other etiologies. | |
|
• Visual acuity reduction or significant visual field loss at presentation is an ominous sign, requiring aggressive intervention. | |
|
• The Idiopathic Intracranial Hypertension Treatment Trial (IIHTT) provides evidence-based therapy for patients who have mild visual loss. | |
|
• A team approach to management is ideal, and a team leader (generally a neurologist or neuro-ophthalmologist) is critical. |
In 1897, Quincke first described a syndrome of elevated intracranial pressure and bilateral papilledema due to impaired cerebrospinal fluid circulation. Seven years later, Nonne recognized that this group of conditions mimicked an intracranial tumor and named them "pseudotumor cerebri." In 1937, Dandy suggested that pseudotumor cerebri resulted from increased cerebral blood volume. In 1955, Foley popularized the term "benign intracranial hypertension." Recognition of visual loss as a possible complication resulted in substitution of the descriptor "idiopathic" for "benign" in 1982 (24). The diagnostic criteria were updated in 2002 to reflect advances in neuroimaging techniques and to incorporate atypical presentations (44). Revised criteria in 2013 defined the diagnosis of pseudotumor cerebri syndrome in adults and children, including criteria for those in whom papilledema is absent (45). “Idiopathic intracranial hypertension” is the term applied when no secondary cause is found.
|
• Idiopathic intracranial hypertension most commonly affects obese women of childbearing age. | |
|
• Headache is the most frequent presenting symptom. Other common symptoms include pulsatile tinnitus and transient visual obscurations. | |
|
• Papilledema is the hallmark sign of the disorder. | |
|
• Vision loss is the most significant complication of idiopathic intracranial hypertension. |
According to the most current criteria (45), the following are required for the diagnosis of idiopathic intracranial hypertension:
|
(A) Papilledema. | |
|
(B) Normal neurologic examination, except for cranial nerve abnormalities. | |
|
(C) Neuroimaging. For obese women, normal brain parenchyma without evidence of hydrocephalus, mass, or structural lesion, and no abnormal meningeal enhancement on magnetic resonance imaging (MRI) with and without gadolinium; for other patients, MRI criteria listed for obese women, together with magnetic resonance venography (MRV) to rule out dural venous sinus thrombosis. If MRI is unavailable or contraindicated, contrast-enhanced CT may be substituted. | |
|
(D) Normal cerebrospinal fluid (CSF) composition. | |
|
(E) Elevated lumbar puncture opening pressure [>/=250 mm of CSF fluid in adults and >/=280 mm of CSF in children (250 mm of CSF if the child is not sedated and not obese)] in a properly performed lumbar puncture (lateral decubitus position). |
The diagnosis is considered “definite” if the patient fulfills criteria A through E.
Patients meeting criteria A through D whose CSF pressure is below the limit specified in criterion E have “probable” idiopathic intracranial hypertension.
If papilledema is not present, the diagnosis of idiopathic intracranial hypertension should not be made unless criteria B through E are satisfied and the patient has a unilateral or bilateral sixth cranial nerve palsy.
If papilledema and a sixth cranial nerve palsy are not present, idiopathic intracranial hypertension is “suggested” when criteria B through E are fulfilled and at least three of the following imaging findings are apparent:
|
(1) Empty sella. |
Most patients with idiopathic intracranial hypertension are obese women of childbearing age.
Idiopathic intracranial hypertension occurring in older adults (> 50 years) and in men is uncommon (09; 15). Patients with idiopathic intracranial hypertension and a normal body mass index (BMI) are more likely to have a secondary cause (eg, medication-induced) of intracranial hypertension (15).
Patients typically present with signs and symptoms of increased intracranial pressure. Headache is the most common presenting symptom and is reported in up to 90% of patients (87; 133). The Idiopathic Intracranial Hypertension Treatment Trial (involving a large prospective cohort of patients) found that the presence of headache and degree of associated disability was not associated with baseline CSF opening pressure (47). This trial and its findings are discussed in detail in the Management section of this article.
Transient visual obscurations, described as blurring or complete vision loss lasting for several seconds to minutes with rapid visual recovery, are reported in approximately 50% to 68% of patients with idiopathic intracranial hypertension (133; 122). Transient visual obscurations may occur following positional changes. Decreased visual acuity at presentation is less common and is often attributed to associated retinal changes or significant optic neuropathy (22; 98). Rapid and severe vision loss should raise the concern for possible fulminant idiopathic intracranial hypertension, which requires immediate diagnosis and treatment to help preserve vision (13).
Pulsatile tinnitus is present in approximately 50% to 60% of patients. In combination with other typical clinical features, it is highly suggestive of a diagnosis of idiopathic intracranial hypertension. Other symptoms include back pain, dizziness, photophobia, and diplopia (128; 133).
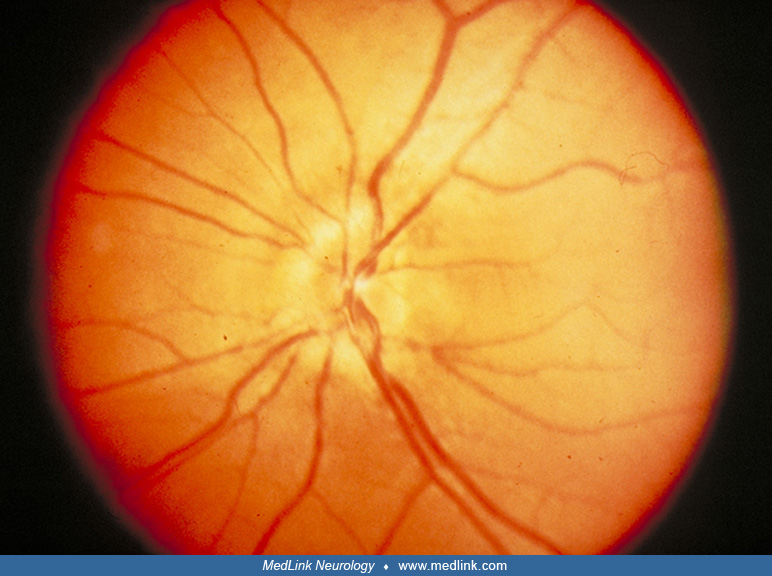
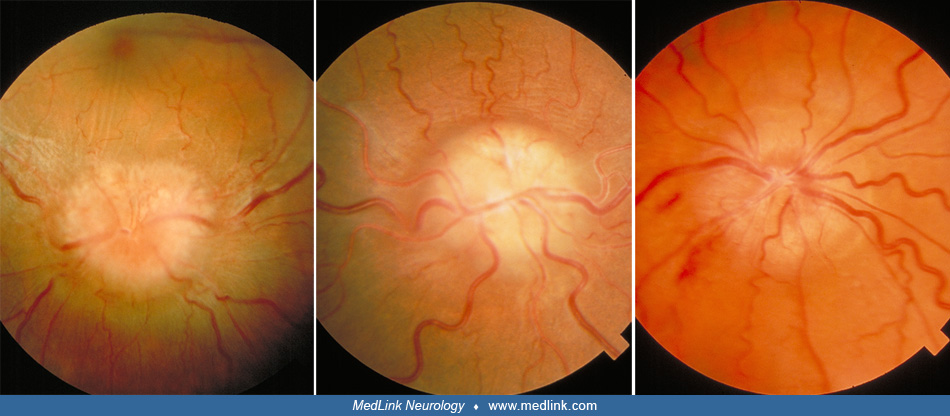
Papilledema is the hallmark of the disorder and is present in almost all patients with idiopathic intracranial hypertension.
Signs of optic disc swelling include elevation of the optic disc margins, a peripapillary halo, venous congestion and tortuosity, retinal exudates, nerve fiber layer hemorrhages, and retinal infarcts (also known as “cotton wool spots”). Extension of the disc swelling into the retina may produce choroidal folds and macular edema. High-grade papilledema is associated with higher baseline opening CSF pressure and is a risk factor for vision loss in this disorder (132).
Sixth nerve palsy (unilateral or bilateral) and comitant esotropia may also be present as nonlocalizing signs of increased intracranial pressure (133; 128).
Although papilledema at the time of diagnosis is typical of idiopathic intracranial hypertension, the disc edema may be asymmetric. The diagnosis of idiopathic intracranial hypertension without papilledema may be considered in patients with symptoms of raised intracranial pressure and elevated CSF opening pressure but no evidence of papilledema on clinical exam (134). Unless a sixth nerve palsy is present, neuroimaging evidence of increased intracranial pressure is also required to suggest this diagnosis (11; 45). Compartmentalization of the subarachnoid space of the optic nerves with impeding bidirectional CSF flow from the brain may explain this finding (71). Alternatively, the patient may have had mild papilledema months to years prior that subsequently resolved. Idiopathic intracranial hypertension without papilledema was estimated to have a prevalence of 2% in a prospective study of patients with refractory chronic daily headache (38) and 5% in a cross-sectional analysis of neuro-ophthalmology clinic patients (30). Compared to patients with papilledema, patients tend to be diagnosed later in their course, have higher rates of nonphysiologic visual loss, have lower opening pressure on lumbar puncture, and respond less favorably to medical therapy (30). Importantly, in patients without papilledema or evidence of resolved papilledema, vision loss should not be present (128).
Idiopathic intracranial hypertension in infants and young children can produce typical symptoms, as previously described. However, variable symptoms may also be present, such as vomiting and lethargy. Behavioral changes can also be seen and generally improve with treatment (104). Strabismus from sixth nerve palsy may be a presenting sign (75; 50). An open fontanelle in infants does not entirely preclude the development of papilledema. Younger patients may also be more likely to be asymptomatic, with papilledema discovered during routine eye examination. Additionally, young children may have difficulty recognizing and verbalizing their symptoms. In contrast to adults with idiopathic intracranial hypertension, the gender ratio in prepubescent children is nearly equal, and obesity is less likely to be present (106).
Causes of secondary intracranial hypertension include a variety of medications, cerebral venous sinus thrombosis, cerebral arteriovenous fistula, spinal cord tumors, gliomatosis cerebri, and other conditions. Because the treatment of secondary forms may be different, it is extremely important to investigate for secondary causes before concluding that intracranial hypertension is idiopathic (128).
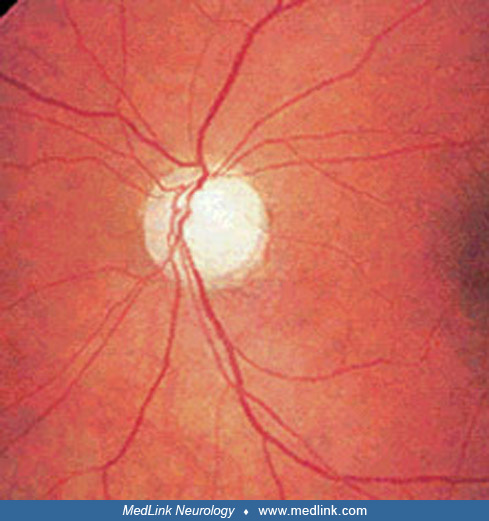
Visual prognosis is generally good. However, risk of permanent vision loss exists, usually secondary to optic neuropathy (22). The incidence of visual loss in idiopathic intracranial hypertension is difficult to estimate with certainty due to the lack of large, long-term prospective studies. In 1982, Corbett and colleagues published a long-term study of 57 patients with idiopathic intracranial hypertension and documented vision loss in 25% (24). Of nine patients who presented with vision loss, seven ultimately had severe vision or visual field loss, leading the authors to conclude that vision loss at presentation is a poor prognostic factor. Of note, this study was performed prior to the use of quantitative visual field testing and the introduction of modern criteria for idiopathic intracranial hypertension diagnosis and treatment algorithms. In a more recent retrospective study of 79 patients, visual field loss at diagnosis was a predictor of final visual field outcome, with 85% of patients presenting with marked visual field loss ending up with poor visual outcomes (94). However, many patients in this study were not followed long term. In the Idiopathic Intracranial Hypertension Treatment Trial, male patients and those with severe papilledema and vision loss at baseline were more likely to have poor visual outcomes (132). Other factors associated with poor visual outcomes include systemic hypertension and renal failure (28). Pubertal patients with idiopathic intracranial hypertension may be at higher risk of permanent visual loss than adults and young children (119). In a retrospective study of patients with consecutive idiopathic intracranial hypertension, black patients were more likely to have severe vision loss (16).
Even patients without optic disc pallor or clinical evidence of vision loss may have evidence of retinal ganglion cell loss after regression of papilledema when assessed using scanning laser polarimetry (81).
The prognosis of secondary intracranial hypertension can vary with the cause of the elevated intracranial pressure. Patients with papilledema in the setting of cerebral venous sinus thrombosis, for example, may have rapid vision loss and persistent visual field defects (86).
Even after resolution of papilledema and normal intracranial pressure, headache may persist in patients with idiopathic intracranial hypertension (48; 47). Some patients with resolution of symptoms and papilledema may continue to have elevated intracranial pressure on repeat lumbar puncture (24).
Psychogenic visual loss in patients with idiopathic intracranial hypertension is not uncommon and presents an additional management challenge, as practitioners aim to avoid unnecessary surgical intervention (97).
Approximately 2% to 3% of patients have a fulminant course of idiopathic intracranial hypertension characterized by rapid onset of symptoms and vision loss (126). Aggressive medical and surgical intervention is required to help preserve vision and avoid further vision loss. Admission to the hospital to help expedite diagnosis and treatment is often required, and close follow-up is mandatory to monitor for recurrence or treatment failure, including shunt malfunction (13).
There are minimal long-term data regarding the stability and recurrence of idiopathic intracranial hypertension. In a retrospective review of 410 patients with idiopathic intracranial hypertension and follow-up of 3 months of more, 8.3% of patients had a recurrence (123). The majority of patients experienced recurrence within 5 years of initial diagnosis, although 15% had a recurrence between 5 to 10 years of follow-up. Of note, many patients with recurrence were poorly adherent to treatment or intolerant to medication. In an analysis of 20 patients with more than 10 years of follow-up from this same cohort, six patients experienced worsening of disease between 28 and 135 months after presentation following a previously stable course (112). Weight gain may be a risk factor for recurrence (74). Retrospective reviews may be influenced by ascertainment and referral bias, as patients who are doing well are less apt to return for follow-up visits. However, given the risk of recurrence and delayed worsening and vision loss, patients with idiopathic intracranial hypertension should have long-term follow-up (112).
Most children with idiopathic intracranial hypertension have a favorable clinical outcome, the majority responding well to medical therapy (50). In a retrospective chart review of 60 patients, relapse was noted in 25% and was more common in patients who were 9 years of age or younger at diagnosis than in patients who were 12 years of age or older (129). The risk of relapse may be highest in the first 18 months after diagnosis (117).
A 12-year-old girl developed headaches that were intermittent and periocular. They were throbbing and pressure-like with accompanying dizziness, phonophobia, nausea, and vomiting. The pain worsened with routine activity, and she missed 6 days of school. She heard intracranial noises “like air rushing through my head” that were pulse-synchronous. One week later, she had double vision. A CT scan of the brain was normal, and she was treated with amoxicillin and decongestants for a presumed sinus infection. When she developed a noticeable esotropia, she came to the emergency department where a lumbar puncture revealed a high CSF pressure and normal CSF constituents. Examination found normal visual acuity, bilateral blind spot enlargement, an incomitant esotropia consistent with a sixth nerve palsy, and bilateral grade 3 optic disc edema. The patient had taken minocycline for acne for 6 months, which was discontinued. Acetazolamide was prescribed. The diplopia resolved shortly after the lumbar puncture, and she was asymptomatic with normal optic discs within 1 month.
This case illustrates several important aspects of diagnosis and management. The patient had secondary idiopathic intracranial hypertension, and her symptoms were identical to those of the idiopathic form. The patient was appropriately treated with acetazolamide in addition to discontinuing the minocycline.
• The exact pathophysiology of idiopathic intracranial hypertension is unknown. Several mechanisms have been proposed, including change in CSF dynamics and venous sinus abnormalities. Obesity and hormonal changes have also been implicated. | |
• Several disorders are associated with idiopathic intracranial hypertension, including obstructive sleep apnea and polycystic ovarian syndrome. | |
• Many medications have been associated with the development of increased intracranial pressure (ex, vitamin A, tetracyclines). |
The exact pathophysiology of idiopathic intracranial hypertension remains unknown, and several different mechanisms have been proposed. Pathological evidence of extracellular brain edema has been refuted (131). A dysfunction in CSF dynamics is possible, either through hyperproduction or increased resistance to absorption. Considerable attention has been focused on abnormalities in cerebrospinal fluid absorption at the level of the arachnoid villi, resulting from increased resistance to drainage across the arachnoid granulations (“arachnoid villi”). However, evidence suggests that the extracranial lymphatics, rather than the arachnoid villi, may be the primary site of CSF absorption (63). Any condition that decreases flow through the arachnoid villi or obstructs the venous pathway from the arachnoid granulations to the right heart may elevate intracranial pressure without producing ventriculomegaly.
The venous system may also play an important role through venous sinus stenosis and increased venous sinus pressure. The lack of ventriculomegaly may be attributed to cerebral venous hypertension (72). Several MRI studies have demonstrated venous sinus abnormalities in idiopathic intracranial hypertension patients. A retrospective case series of three patients found that in susceptible persons with venous sinus stenoses on venous imaging, prolonged and intense coughing can trigger idiopathic intracranial hypertension (21). Such aggressive and prolonged Valsalva maneuvers triggering clinical manifestations of idiopathic intracranial hypertension support a hydraulic model of pathogenesis where patients with high venous mural compliance may be more susceptible to resurgences of idiopathic intracranial hypertension. It remains unclear whether venous sinus stenosis is the result or the cause of increased intracranial pressure (92).
Obesity is strongly associated with idiopathic intracranial hypertension and has been implicated in its pathogenesis. Weight gain is associated with an increased risk of development of idiopathic intracranial hypertension as well as an increased risk of recurrence of the disorder. Adipose tissue also secretes numerous proinflammatory cytokines, chemokines, adipokines, and hormones that may be pathogenically linked to the development of idiopathic intracranial hypertension. Leptin is an adipokine that mediates hypothalamic regulation of satiety and weight control, and investigators have found elevated CSF leptin levels in idiopathic intracranial hypertension patients, even when controlled for body weight (08). Such findings raise the possibility of leptin resistance among idiopathic intracranial hypertension patients, as leptin levels are high, yet the affected patients remain obese. Leptin receptors are located within the choroid plexus, which is the principal site of CSF production, representing another possible connection to the development of idiopathic intracranial hypertension (57).
Obesity can also be viewed as a chronic inflammatory condition, which leads to a theory of pathogenic inflammation causing idiopathic intracranial hypertension. Cytokine antibody arrays and ELISA assessment showed significant elevations of CSF chemokine CCL2 in patients with idiopathic intracranial hypertension compared to controls (27). Significant elevations of IL-2 and IL-17 in the CSF of patients with idiopathic intracranial hypertension have also been documented (89; 57).
Hormonal factors may also play a role in the development of increased intracranial pressure. There are cases of development of raised intracranial pressure during corticosteroid treatment and with steroid withdrawal. Cortisol is regulated by the enzyme 11β-hydroxysteroid dehydrogenase type 1, which is abundant within adipose tissue. This enzyme has also been found within the choroid plexus, where it fuels cortisol, and possibly CSF, production. A novel 11β-hydroxysteroid dehydrogenase type 1 inhibitor is currently being investigated in a phase 2 study demonstrating in vivo evidence of effective inhibition of the enzyme (90; 88). Bariatric surgery in patients with idiopathic intracranial hypertension has been associated with reduced 11β-hydroxysteroid dehydrogenase activity (135).
The role of gut peptides in regulating intracranial pressure also remains at the forefront of idiopathic intracranial hypertension research. Glucagon-like peptide-1 (GLP-1) is a gut peptide secreted by the small intestine in response to food consumption. It stimulates glucose-dependent insulin secretion, inhibits glucagon release, and triggers satiety and weight loss. GLP-1 receptors have been localized to the choroid plexus; their role in modulating CSF production is speculative (57). Exendin-4, a GLP-1 mimetic currently utilized in the treatment of obesity and diabetes mellitus, was shown to reduce intracranial pressure in rats (12). The possible treatment application to humans with idiopathic intracranial hypertension requires further investigation.
The role of androgens has also been investigated. There are case reports of the development of idiopathic intracranial hypertension among transgender patients undergoing female to male transition with testosterone therapy and among hypogonadal males after androgen deprivation therapy for prostate cancer. There may be a “pathophysiological window” of testosterone levels in humans, with androgen excess in women and androgen deficiency in men that causes metabolic disturbances, such as increased visceral fat deposition and insulin resistance, thus, creating the possible neurometabolic syndrome of idiopathic intracranial hypertension (58).
There may be a genetic basis for idiopathic intracranial hypertension. Cases of familial idiopathic intracranial hypertension have been reported (23). In a review of 520 patients with idiopathic intracranial hypertension from Israel, 15 familial cases were identified (2.9% of the cohort) (73). The first genome-wide association study was conducted utilizing chromosomal DNA from 95 patients enrolled in the Idiopathic Intracranial Hypertension Treatment Trial, compared to controls. Of over 300,000 single nucleotide polymorphisms evaluated, three were identified as associated with idiopathic intracranial hypertension (rs2234671 on chromosome 2, rs79642714 on chromosome 6, and rs200288366 on chromosome 12), as well as three candidate regions with multiple associated single nucleotide polymorphisms on chromosomes 5, 13, and 14. Candidate genes LINC00359 and FOXN3 were identified for further studies (78).
Obstructive sleep apnea and idiopathic intracranial hypertension may coexist, and apneic episodes have been linked to a rise in intracranial pressure. A case-control study of men with idiopathic intracranial hypertension found that obstructive sleep apnea and symptoms associated with testosterone deficiency were more common in patients than in controls (40). A sub-study of the idiopathic intracranial hypertension weight randomized controlled trial (IIH:WT) found that sleep apnea was common in idiopathic intracranial hypertension, and improvements may be correlated with improvement in papilledema (137). Polycystic ovarian syndrome, autoimmune conditions, and renal failure have also been associated with intracranial hypertension (28; 54; 100).
Many medications have been reported in association with the development of raised intracranial pressure, including vitamin A and its derivatives (vitamin A supplementation, isotretinoin), antibiotics (particularly of the tetracycline class, sulfenazone, fluoroquinolones), growth hormone, lithium, corticosteroids, and cyclosporine (28; 41). Some case reports have associated hormonal contraceptive use with the development of increased intracranial pressure. This connection remains controversial. In a retrospective case control study, hormonal contraceptives were not significantly associated with idiopathic intracranial hypertension (69). The authors comment on several factors that may explain or refute the association between contraceptives and raised intracranial pressure, eg, young women of childbearing age are at highest risk for idiopathic intracranial hypertension and are the population most likely to be using contraceptives. Medication-induced intracranial hypertension can also be seen in children (75). A systematic review of drug-induced intracranial hypertension identified 259 reported cases (124). The authors suggest that drug-induced intracranial hypertension be diagnosed only if it develops within a reasonable time interval of drug administration and resolves on discontinuation of the drug.
Secondary intracranial hypertension in adults may result from impairment of cranial venous outflow and subsequent venous hypertension. Chronic ear disease, head injury, intracranial arteriovenous fistulas, meningeal tumors, surgical ligation of extracranial veins, cardiac failure, chronic respiratory disease, and jugular paragangliomas can all contribute to cranial venous outflow obstruction (62). Transverse sinus stenosis has been widely implicated, although whether it is the cause or the result of elevated intracranial pressure remains debatable (will be discussed further in the Management section). Venous sinus stenosis can resolve when the intracranial pressure is lowered by lumbar puncture or shunting procedure.
Case control studies have not been performed in the pediatric population to identify those conditions associated with secondary intracranial hypertension. Case reports suggest a link to parameningeal infections, endocrinopathies, Lyme disease, vitamin A usage, human growth hormone, Down syndrome, venous sinus thrombosis from mastoiditis, otitis media, obesity in adolescents (but not in preadolescents), endocrine disorders (such as hypoparathyroidism), medications, and malnutrition (28; 75; 14). Nonetheless, even when a potential inciting exposure is identified, obesity may be considered in children with idiopathic intracranial hypertension. A study of children with secondary pseudotumor cerebri found no difference in body mass index compared to children with primary (idiopathic) pseudotumor cerebri, with 79% being overweight or obese (102).
|
• The incidence of idiopathic intracranial hypertension is highest in obese women of childbearing age. | |
|
• The incidence in the United States may be increasing commensurate with the rising incidence of obesity. |
A 1988 United States survey disclosed an incidence of idiopathic intracranial hypertension of 0.9 per 100,000 people, increasing to 13 per 100,000 in women 20 to 44 years of age and 10% over ideal body weight and 19.3 per 100,000 in women 20 to 44 years of age and 20% over ideal body weight (33). The female to male ratio was 8 to 1, and the average age at diagnosis was approximately 27. A similar incidence has also been reported in Israel (67).
An analysis from Minnesota found that the incidence of idiopathic intracranial hypertension doubled from 1.0 per 100,000 to 2.0 per 100,00 between 1990 and 2014, in parallel with an increase in the incidence of obesity (70). Similar findings were reported in an analysis of a large administrative healthcare dataset in the United States from 1997 to 2016 (52). However, routine screening of morbidly obese individuals for symptoms and signs of idiopathic intracranial hypertension has a low yield (77).
At present, there is no known method to prevent idiopathic intracranial hypertension, although maintaining a normal weight is likely useful.
Brain tumors. Although the diagnosis of idiopathic intracranial hypertension may seem apparent, particularly when it affects an obese female of childbearing age, it is a diagnosis of exclusion. Most importantly, a mass lesion causing intracranial hypertension must be ruled out. The initial manifestations of space-occupying lesions may include headaches, other focal neurologic deficits, behavioral changes, cognitive decline, seizures, fatigue, and visual manifestations. Such signs and symptoms of brain tumors overlap with those of idiopathic intracranial hypertension. A study of children with brain tumors who were first evaluated by an ophthalmologist found that the most common visual findings were decreased vision with optic disc pallor or papilledema (05).
Headaches due to other causes. Clinicians should be aware of the striking similarities between the headache phenotypes of brain tumors, migraine, and idiopathic intracranial hypertension. Tension headache, migraine headache, medication overuse headache, and depression may coexist in patients with idiopathic intracranial hypertension (48). Therefore, it is essential to perform a careful ophthalmoscopic examination in patients with long-standing headache, particularly in those who are young, female, and overweight. Infrequently, increased intracranial pressure can be seen in patients without papilledema, as discussed previously (idiopathic intracranial hypertension without papilledema) (30).
Secondary intracranial hypertension. Secondary intracranial hypertension in adults may result from impairment of cranial venous outflow and subsequent venous hypertension. Chronic ear disease, head injury, intracranial arteriovenous fistulas, meningeal tumors, surgical ligation of extracranial veins, cardiac failure, chronic respiratory disease, and jugular paragangliomas can all contribute to cranial venous outflow obstruction (62).
Other disorders that may be mistaken for idiopathic intracranial hypertension include cerebral venous sinus thrombosis, intracranial infection, and intracranial malignancy. Cerebral venous sinus thrombosis was eventually detected in approximately 9% of patients with intracranial hypertension initially diagnosed as idiopathic (85). Most of the patients were “atypical,” and an underlying cause for the venous sinus thrombosis was identified in all but two patients. Headache may precede the onset of focal deficits and seizures in patients with cerebral venous sinus thrombosis and is frequently refractory to common pain medications (60). Transverse sinus stenosis has been widely implicated. The presence of ophthalmoparesis, other than sixth nerve palsy, should prompt the search for venous sinus thrombosis or a hypercoagulable state (42). Magnetic resonance venography of the head is often obtained with magnetic resonance imaging of the head to exclude a cerebral venous sinus thrombosis.
The Biological basis section (etiology and pathogenesis) discusses associated and underlying disorders in detail. The most relevant conditions, including both those associated with idiopathic intracranial hypertension and those responsible for secondary intracranial hypertension, can be viewed from the Associated Disorders link in the article menu.
|
• Idiopathic intracranial hypertension is a diagnosis of exclusion, and work-up is necessary to exclude other causes of increased intracranial pressure. | |
|
• Typical diagnostic studies include neuroimaging (MRI, MRV brain) followed by lumbar puncture with measurement of opening pressure (lateral decubitus position) and collection of CSF studies. | |
|
• A full ophthalmic examination is essential, including assessment of papilledema and formal visual field testing. | |
|
• A thorough review of medication use should be obtained to identify any medications associated with increased intracranial pressure (such as vitamin A, minocycline). |
Neuroimaging studies and a lumbar puncture are essential in the work-up of idiopathic intracranial hypertension to exclude other causes of increased intracranial pressure (45). Imaging studies are usually the first part of the diagnostic evaluation to exclude structural causes, typically magnetic resonance imaging (MRI) of the brain with contrast. Magnetic resonance venography (MRV) is also usually obtained to rule out a venous sinus thrombosis, particularly in cases with atypical or fulminant presentation. Computed tomography of the head (CT) and CT cerebral venography (CTV) are less sensitive than MRI and MRV at detecting some causes of raised intracranial pressure (eg, meningeal disorders, tumors) as well as subtle imaging findings associated with idiopathic intracranial hypertension (109; 128). Common imaging findings in idiopathic intracranial hypertension include empty sella, flattening of the posterior sclera, distention of the perioptic dura, protrusion of the optic nerve head into the vitreous cavity (papilledema), and tortuosity of the optic nerve. The empty sella results from bony enlargement of the sella from chronically raised intracranial pressure (80). CTV and MRV often reveal smooth-walled transverse sinus stenosis or sinus flow gaps, which can be mistakenly interpreted as thromboses (25). Imaging findings attributed to idiopathic intracranial hypertension can be seen in patients without raised intracranial pressure. In a retrospective imaging study, flattening of the posterior aspect of the globe was most specific for the diagnosis of idiopathic intracranial pressure (02). Imaging findings are not predictive of visual outcomes (110).
A lumbar puncture is also obtained to confirm increased intracranial pressure and exclude secondary etiologies (eg, infection). To obtain an accurate opening pressure, the lumbar puncture should be performed with the patient in the lateral decubitus position. In adults, opening pressure greater than 25 cm water is considered high. Pressures between 20 and 25 cm water are borderline in adults. The upper limit of normal in children is 28 cm water (07). The CSF contents, including cell count and protein, should be normal (128).
A full ophthalmologic examination is necessary for the diagnosis of idiopathic intracranial hypertension and monitoring response to treatment. Examination should include formal assessment of visual acuity, extraocular motility and alignment, and ophthalmoscopic examination (papilledema). Formal visual field testing is mandatory. Common visual field defects include enlargement of the physiologic blind spot, nasal step defects, arcuate defects, and generalized peripheral constriction (65). Echography (A scan and B scan) and optical coherence tomography (OCT) may be helpful in differentiating papilledema from congenitally elevated optic discs (pseudopapilledema), including those with optic disc drusen (84; 114).
|
• Goals of treatment are to preserve visual function and relieve symptoms. Management is dictated by vision loss, severity of symptoms and papilledema, and response and tolerance to medical therapy. | |
|
• Treatment options include weight loss, medication (primarily acetazolamide), and surgery (optic nerve sheath fenestration, shunting, venous sinus stenting). | |
|
• The Idiopathic Intracranial Hypertension Treatment Trial (IIHTT) was a randomized controlled clinical trial of acetazolamide and placebo in addition to a weight reduction diet. This study provides evidence-based guidance for patients presenting with mild vision loss. |
Medication and weight loss. Medical therapy includes weight loss and medications (primarily carbonic anhydrase inhibitors) (49; 61; 79; 115).
Discontinuation of a causative agent is mandatory but may not be sufficient. Patients with intracranial hypertension from a secondary cause often need additional treatment to prevent visual loss (43). Treatment strategies are similar in adults and children.
Obesity is associated with the development of idiopathic intracranial hypertension. Weight loss is often recommended. In a prospective study of 20 women with a BMI over 25, a low-calorie diet for 3 months resulted in substantial weight loss (15.7 kg/34.6 lbs on average), with an associated decrease in intracranial pressure and improvement in headache, papilledema, and visual fields (115).
Medication options include acetazolamide and, less commonly, topiramate and diuretics (furosemide). Use of acetazolamide, furosemide, methazolamide, and topiramate for the treatment of idiopathic intracranial hypertension is off label.
The Idiopathic Intracranial Hypertension Treatment Trial, sponsored by the National Eye Institute, studied the effect of acetazolamide and a supervised diet (aimed at losing at least 6% of body weight within 6 months) compared to placebo and a supervised diet in patients with mild visual loss (46). Perimetric mean deviation as measured by the Humphrey Visual Field Analyzer ranged from -2 to -7 dB at study entry, and the primary outcome measure was change in the perimetric mean deviation at 6 months. The starting dose of study medication was 500 mg twice daily and was gradually increased to 2 grams twice daily, or the maximum tolerated dose (133). At 6 months, participants randomized to acetazolamide therapy had improved perimetric mean deviation, papilledema grade, vision-related quality of life, and a greater reduction in weight than patients randomized to placebo and weight loss. The overall treatment effect was an improvement of 0.71 dB, with a more robust effect (2.27 dB) in participants with more severe papilledema at baseline (Frisén papilledema grade of 3 to 5). Acetazolamide was not superior to placebo for reducing headache disability. Based on the study results, treatment with acetazolamide up to 4 grams daily combined with a weight loss regimen is recommended for patients with mild visual loss. There are no evidence-based guidelines for treating patients with severe visual field loss at presentation (101), but treatment may involve high-dose medical therapy and surgical intervention.
Other carbonic anhydrase inhibitors have been used in idiopathic intracranial hypertension, including methazolamide and topiramate, and may be considered when patients are intolerant to acetazolamide (128). In an open-label study of topiramate versus acetazolamide, the dose of topiramate was started at 50 mg per day and titrated as needed. Of note, acute angle closure glaucoma can develop after starting topiramate (20). Furosemide, a loop diuretic, can also be used but requires electrolyte monitoring. Corticosteroids have many side effects, and steroid withdrawal can precipitate a rebound rise in intracranial pressure.
Lumbar puncture. Therapeutic lumbar punctures may be useful as a temporizing measure in cases of fulminant idiopathic intracranial hypertension, but repeated lumbar punctures as a long-term therapeutic option poses risks of infection and post-procedure overdrainage, with resultant low-tension headache (65).
Surgery. Surgical options for idiopathic intracranial hypertension are generally reserved for patients with moderate-to-severe visual loss when medical therapy alone is inadequate or in fulminant presentations. Surgical options include optic nerve sheath fenestration, cerebrospinal fluid diverting procedures (lumboperitoneal shunting, ventriculoperitoneal shunting), temporizing cerebrospinal fluid diversion [lumbar or ventricular drain], and cerebral venous sinus stenting. The choice of procedure often depends on available resources at various institutions, and more than one type of procedure may be necessary (130).
Optic nerve sheath fenestration. The mechanism by which optic nerve sheath fenestration resolves papilledema and preserves visual function is not entirely elucidated. It is believed to serve as an additional pathway for CSF egress or to cause subarachnoid scarring around the optic nerve, serving as a mechanical blockade to shift pressures away from the retrolaminar optic nerve. Success of optic nerve sheath fenestrations may also be related to a cyst-like structure that develops contiguous to the fenestration site, diverting CSF away from the confines of the optic nerve sheath, or by improving blood perfusion to the optic nerve head (53). Fenestrations can be completed via a medial or lateral orbitotomy or superomedial lid crease incision (65). A systematic review found 23 studies of optic nerve sheath fenestration, all case series or case reports (818 total patients) (64). This procedure appears to have similar efficacy in both children and adults (127). Unfortunately, it may fail at any time after surgery (39), and patients may require a supplementary surgical intervention (16.9% in a systematic review) (64). If the papilledema is chronic, this modality may be less successful.
Lumboperitoneal and ventriculoperitoneal shunting. Shunting offers the benefit of treating the underlying problem of elevated intracranial pressure. CSF shunting procedures have demonstrated effectiveness in improving visual acuity, visual field, and papilledema (116; 59; 108). However, shunting procedures have high failure rates, requiring one or more shunt revisions in most cases (130; 116). Long-term survival of the shunt may not be necessary in idiopathic intracranial hypertension as high intracranial pressure is often self-limited (17). A programmable shunt valve may help diminish the complications of ventriculoperitoneal shunting (138), particularly when used in conjunction with a ventricular access device. This device is inserted stereotactically into the frontal horn of the lateral ventricle, providing an access point for measuring CSF pressure in the setting of suspected shunt failure (96). Stereoscopic surgical navigation is helpful to achieve cannulation of normal-sized ventricles when standard maneuvers are unsuccessful (51). Stereotactic frameless procedures have been employed with good initial results but with a 50% failure rate at 1 year (136). Direct comparison studies of the various surgical procedures have not been performed, although ventriculoperitoneal shunts may require revision less frequently than lumboperitoneal shunts (93; 17).
Of note, a multicenter, prospective study comparing the efficacy of optic nerve sheath fenestration and ventriculoperitoneal shunting for the treatment of idiopathic intracranial hypertension in patients with moderate to severe vision loss was recently terminated due to low enrollment (Surgical Idiopathic Intracranial Hypertension Treatment Trial – SIGHT – Clinical Trials Identifier: NCT03501966).
Venous sinus stenting. Venous sinus stenting has emerged as a possible minimally invasive treatment option for medically refractory idiopathic intracranial hypertension. Improved MR venographic technology has identified dural venous sinus stenoses. Whether this venous narrowing is pathogenic or the result of elevated intracranial pressure remains unresolved. Case reports and case series document normalization of CSF opening pressures after endovascular stenting of transverse sinus stenoses (32; 139), whereas others have detailed resolution of venous sinus narrowing after CSF drainage by cervical/lumbar drainage or CSF diversion procedures (72; 10; 26; 120; 56).
Evidence for the benefit of venous sinus stenting comes from numerous case series (both prospective and retrospective). There are no randomized controlled trials for this intervention to date (125; 34; 03; 31; 111; 19; 76). A systematic review and meta-analysis analyzed 20 articles and 474 total patients (99). More than 90% of patients had improvement in papilledema, and approximately 80% had improvement or resolution in headache. Average reduction in CSF opening pressure was 16.8 cm water in a single cohort of patients with idiopathic intracranial hypertension after venous sinus stenting, independent of acetazolamide use or weight loss (105). A retrospective chart review documented that the duration of acetazolamide treatment among patients who underwent venous sinus stenting decreased from 571+/-544 days in medically treated patients to 188+/-209 days among stented patients (113).
The criteria for patient selection for stenting remain unclear. Noninvasive neuroimaging alone (magnetic resonance or CT venography) is unsatisfactory when identifying possible venous sinus stenoses amenable to stenting; rather, pressure gradients are generally measured across stenotic areas utilizing cerebral catheter angiography/venography and manometry. Pressure gradients of at least 8 mmHg are commonly considered necessary to prompt stenting. Patients most often undergo unilateral transverse sinus stenting, even if bilateral stenoses are present, generally along the dominant or higher-pressure gradient side (65). Currently, stenting is largely considered for patients who are unable to tolerate conventional medical treatments. Some recommendations for the selection and treatment of patients with idiopathic intracranial hypertension with venous sinus stenting include (37):
|
• Noninvasive venous imaging utilized as a screening tool to determine candidacy for cerebral venography/catheter angiography. | |
|
• Diagnostic catheter angiography on patients failing medical therapy (persistent symptoms). | |
|
• BMI not used as criterion for candidacy for diagnostic catheter angiography. | |
|
• Venous sinus manometry to be completed prior to stenting, with pressure gradient of greater than or equal to 8 mmHg. | |
|
• Diagnostic catheter angiography and manometry should be performed while patients are awake, as studies indicate that general anesthesia may underestimate pressure gradients. | |
|
• No consensus regarding the superiority of one specific stent device. | |
|
• No data to support bilateral transverse sinus stenting over unilateral stenting, or the use of multiple stents to reduce the risk of stent failure. | |
|
• Antiplatelet agents should be administered prior to, and for at least 3 to 6 months after, stenting. |
Markedly elevated lumbar puncture opening pressures (> 50 cm CSF) prior to stenting and persistent papilledema after stenting were associated with a refractory course, requiring later shunting (55). Highest degrees of improvement in maximum mean intracranial venous pressure and pressure gradient after stenting have been documented among more obese patients (107). Patients with higher mean pressure gradients and higher changes in pressure gradients after stenting may achieve more favorable outcomes (91). A meta-analysis of optic nerve sheath fenestration, shunting, and stenting evaluating 30 studies containing class 3 evidence (82) found that visual acuity improved with all three modalities, and headache improved modestly with shunting and venous sinus stenting. The authors concluded that there is insufficient evidence to recommend or reject any of the treatment modalities. Future prospective, randomized trials including venous sinus stenting are needed to provide a more vigorous assessment of the efficacy of this newer treatment modality.
Bariatric surgery. Bariatric surgery may be helpful in the long-term management of idiopathic intracranial hypertension in morbidly obese individuals. Bariatric surgery is not useful in the setting of acute visual loss. A clinical trial randomized 66 patients with idiopathic intracranial hypertension to bariatric surgery or community weight management (Weight Watchers) (95). The bariatric surgery group had greater reduction in intracranial pressure and improved quality of life.
Treatment strategies are similar in adults and children. The Idiopathic Intracranial Hypertension Treatment Trial did not include children, and there are no equivalent clinical trials for the pediatric population (50). If medical management is pursued, an acetazolamide dosage of 10 to 25 mg/kg/day divided BID or TID is commonly used. Surgical options may also be explored in patients with vision loss.
Medication-associated intracranial hypertension. A thorough review of medications associated with idiopathic intracranial hypertension should be performed at baseline (124). Discontinuation of a causative agent is mandatory but may not be sufficient, and patients may require further treatment with medication or surgery.
Treatments on the horizon. Based on the posited metabolic pathogenesis of idiopathic intracranial hypertension, an 11β-hydroxysteroid dehydrogenase type 1 inhibitor was investigated in a phase 2, double-blind, randomized, placebo-controlled trial (88). The drug was well tolerated, and in vivo evidence of 11β-hydroxysteroid dehydrogenase type 1 inhibition was demonstrated. The primary clinical outcome was change in intracranial pressure. At 12 weeks, pressures were not statistically different between the drug and placebo groups, although an exploratory within group analysis demonstrated a statistically significant reduction in intracranial pressure in the drug group.
Complication rates of optic nerve sheath fenestration. Complications have been reported in 15.6% to 40% of patients (65). Such complications include diplopia (3.4%-26%), anisocoria (tonic pupil; 9.7%-13.4%), corneal dellen (0.8%-2.2%), cranial nerve palsies (7.2%), orbital hematoma (7.2%), perilimbal conjunctival filtering blebs (less than 0.4%), conjunctival abscess (less than 0.4%), orbital apex syndrome (less than 0.4%), and traumatic optic neuropathy (less than 0.4%) (53).
Complications of cerebrospinal fluid shunting. The main complication of cerebrospinal fluid shunting is shunt failure, often defined as the need for shunt revision, replacement, or removal. Failure rates of ventriculoperitoneal shunts among patients with idiopathic intracranial hypertension were 20% at 1 year, 35% at 2 years, and 52% at 3 years in a retrospective cohort; 1 out of 19 patients required removal of the ventriculoperitoneal shunt due to meningitis and gangrenous small bowel (59; 17).
Other complications of ventriculoperitoneal shunting include intracranial hemorrhage and difficulty with shunt placement within small ventricles of idiopathic intracranial hypertension patients, resulting in catheter malposition.
A 27% rate of shunt obstruction is reported among lumboperitoneal shunts, the most common cause being migration of the peritoneal catheter (35). Shunt overdrainage also occurs more readily among lumboperitoneal shunts, with a published rate of 13%, contributing to low-pressure headaches (35). Karabatsou and colleagues published a 1% infection rate per lumboperitoneal shunting procedure (66). Further complications of lumboperitoneal shunting include subdural hematoma formation and cerebellar tonsillar descent/acquired Chiari malformation (up to 70% incidence in a pediatric population; 14% among idiopathic intracranial hypertension adults) (51).
More unusual complications of both types of shunts include intraabdominal pain, retroperitoneal hematoma, and cerebrospinal fluid leak (118; 53).
Due to the complications listed above, shunt revision rates can be quite high, upwards of 60% for lumboperitoneal shunts and 30% for ventriculoperitoneal shunts (01).
Complications of dural venous sinus stenting. These include re-stenosis proximal to the stent or along a contralateral nonstented stenosis, which may occur in up to 20% of procedures (06), subdural in-stent thrombosis, stent migration, epidural/subdural/subarachnoid hemorrhage, uncontrolled intracranial hypertension, development of an intracranial dural arteriovenous fistula, femoral pseudoaneurysm, and retroperitoneal hematoma. Two deaths have been reported, one from a severe cerebellar hemorrhage (04; 121; 18; 83). Stent survival was 87.8% at 120 days (06). Re-stenting was necessary in 9.8% to 12% of cases (125; 06).
There are no clear guidelines for pregnancy and idiopathic intracranial hypertension, and the literature to date is composed primarily of case series and expert opinions. Idiopathic intracranial hypertension may develop or worsen in pregnancy. Of note, gadolinium contrast with MRI is not recommended during pregnancy. Venous sinus thrombosis must be considered when idiopathic intracranial hypertension develops in the puerperium after a miscarriage or an ectopic pregnancy (36). Many patients without vision loss can be managed conservatively, and treatment options are similar to those for nonpregnant patients. Acetazolamide is Food and Drug Administration (FDA) pregnancy category C (animal studies demonstrating adverse effect, but no adequate studies in humans). If this medication is used, it should be done in consultation with obstetrics and weighing the risk of progressive vision loss. Surgical interventions can be considered in medically refractory cases with vision loss and include serial lumbar puncture, optic nerve sheath fenestration, and shunting. Increased intracranial pressure during labor and delivery is transient. Vaginal delivery in patients with idiopathic intracranial hypertension has not been associated with worse visual outcomes (68). A multidisciplinary approach is essential for the care of pregnant patients with idiopathic intracranial hypertension (103).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Tatiana Deveney MD
Dr. Deveney of University of Michigan has no relevant financial relationships to disclose.
See Profile
Jonathan D Trobe MD
Dr. Trobe of the University of Michigan has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
Neuro-Oncology
Dec. 13, 2024
Neuro-Ophthalmology & Neuro-Otology
Dec. 02, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 24, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuromuscular Disorders
Oct. 29, 2024