

Neuro-Ophthalmology & Neuro-Otology
Diplopia
Jan. 08, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Ischemic to the optic nerve is the most common cause of sudden visual loss in patients over 50 years of age. The conventional form of this condition is called nonarteritic anterior ischemic optic neuropathy (NAION) because it is limited to the optic disc. Occurring typically in just one eye in the context of “standard vasculopathic” risk factors, particularly diabetes, hypertension, and hyperlipidemia. Its precise pathogenesis is unresolved.
A much less common nonarteritic form is limited to the retrobulbar segment of the optic nerve and is therefore called nonarteritic posterior ischemic optic neuropathy. It occurs most often in the perioperative period after cardiac or spine surgery, but also in the setting of arteriosclerosis, herpes zoster infection, connective tissue disorders, surgical manipulation of the intracranial optic nerve, and radiation therapy in the region of the optic nerves and optic chiasm.
Another variant of ischemic optic neuropathy occurs after systemic hypotension (“hypotensive or shock-induced”). It has an anterior variant that affects only the optic disc segment, a posterior variant that is limited to the retrobulbar optic nerve segment, and a variant that affects both segments. Ischemic optic neuropathy has been linked to a variety of medications like amiodarone and phosphodiesterase inhibitors, but a causal relationship has not been firmly established. The visual loss in these nonarteritic variants extends from mild to severe and is largely irreversible. Treatment is not effective.
Finally, there is the uncommon but most perilous variant called arteritic ischemic optic neuropathy (AION). Occurring most often in giant cell arteritis. Arteritic ischemic optic neuropathy almost always affects the optic disc but may also affect the orbital optic nerve segment, as well as its dura and surrounding orbital soft tissues. Because the optic disc is affected in over 90% of patients, a posterior arteritic variant is hardly acknowledged. Limited to patients over age 50, it causes severe and irreversible visual loss, often in both eyes. High-dose corticosteroid treatment probably prevents second-eye involvement.
|
• Ischemic optic neuropathy is named according to cause (nonarteritic or arteritic) and location (anterior with optic disc swelling or posterior with an initially normal-appearing optic disc). | |
|
• Nonarteritic anterior ischemic optic neuropathy is a common cause of vision loss in individuals over 50 years of age and does not have a proven treatment. | |
|
• Nonarteritic anterior ischemic optic neuropathy is associated with vasculopathic risk factors, some medications, obstructive sleep apnea, and crowded optic nerve heads. | |
|
• Nonarteritic posterior ischemic optic neuropathy is rare. | |
|
• Arteritic anterior or posterior ischemic optic neuropathy is typically caused by giant cell arteritis, which requires emergent treatment to prevent other ischemic events. |
In 1966 Miller and Smith described a syndrome of acute, monocular, painless visual loss, afferent pupillary defect, and optic disc edema, terming it ischemic optic neuropathy (68). The term ischemic optic neuropathy identified the noninflammatory nature of the disorder, which previously had been variously named “vascular pseudopapillitis,” “arteriosclerotic papillitis,” and “ischemic papillitis.” Hayreh subsequently added the keyword “anterior” to denote those cases of ischemic optic neuropathy that included optic disc edema in the acute phase (nonarteritic anterior ischemic optic neuropathy), differentiating them from the rarer posterior ischemic optic neuropathy, in which the optic disc appearance is initially normal (37). The term arteritic ischemic optic neuropathy describes ischemic optic neuropathy that occurs in vascular inflammation, typically giant cell arteritis.
The typical clinical presentation of most forms of ischemic optic neuropathy (ION) is characterized by the sudden onset of vision loss in one eye in an older individual, with a reduction in visual acuity vision, peripheral visual field loss, or both. There will be a relative afferent pupillary defect except if both eyes are affected equally. In the acute stage of most variants, the ophthalmoscopic exam will show a segmentally or completely swollen optic disc. In the posterior ischemic optic neuropathy variants, the optic fundus will appear normal. In all variants, a pale optic disc develops months after the attack. Key features to delineate the conventional anterior nonarteritic anterior ischemic optic neuropathy from arteritic ischemic optic neuropathy are listed (in Table 1). Further details are provided in the subsections below.
|
Arteritic Anterior ION |
Nonarteritic Anterior ION | |
|
Age at onset |
mean, 70 years |
mean, 60 years |
|
Gender |
women>men |
women=men |
|
Common associated systemic symptoms |
headache, jaw claudication |
none |
|
Mean visual acuity |
<20/200 |
20/30 |
|
Optic disc |
pale swelling >50% in affected eye; cup in unaffected eye is normal |
hyperemic swelling in affected eye; cup in unaffected eye is small |
|
Mean erythrocyte sedimentation rate |
70 mm/hour |
normal |
|
Fluorescein angiography |
optic disc and choroidal arterial filling delay |
optic disc arterial filling delay |
|
Natural history |
Vision rarely improves; fellow eye affected in 54% to 95% |
Vision improves slightly in up to 43%; fellow eye eventually affected in 15% |
|
Treatment |
systemic steroids |
none proven |
|
| ||
Arteritic ischemic optic neuropathy. Patients with arteritic ischemic optic neuropathy may present with acute vision loss in one or both eyes, sometimes with episodes of monocular transient vision loss in preceding days. Periocular pain is unusual. There will almost always be swollen, often pallid, optic disc in affected eyes. Other fundus manifestations include central and branch retinal artery occlusions, frequently accompanied by cotton wool spots and retinal hemorrhages. Patients may experience episodes of temporary vision loss prior to the onset of permanent ocular ischemia. Diplopia and eye pain can occur due to ischemia of the extraocular muscles and other orbital structures. Constitutional symptoms include headache, jaw claudication, scalp tenderness, weight loss, alopecia, fever, and depression. Multiple symptoms can occur simultaneously or stepwise due to the progressive involvement of other arteries. The progression can be rapid, and emergent treatment is necessary to reduce involvement of additional vascular beds.
Nonarteritic anterior ischemic optic neuropathy. The conventional form of nonarteritic anterior ischemic optic neuropathy usually presents as acute painless vision loss in one eye, often noted upon awakening. Visual acuity may be normal, but more often it is depressed to a mild or moderate degree. Any pattern of visual field loss may occur, the most common being altitudinal loss involving all or a portion of the superior or inferior hemifield. In some cases, vision can decline further over the initial few weeks. Vision loss can eventually involve both eyes, but simultaneous binocular involvement is rare.
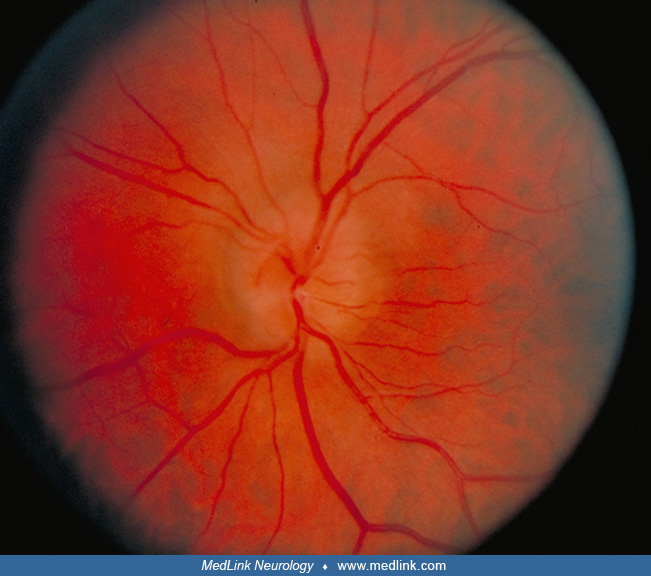
A hyperemic optic disc is observed on ophthalmoscopic examination, usually accompanied by nerve fiber layer hemorrhages. The optic disc may be completely swollen or partially swollen in one or more quadrants with preservation of optic disc structure in non-swollen regions of the disc.
There is frequently little correlation between the degree of optic disc swelling and the amount of visual acuity or visual field loss. Patients with NAION commonly have a type of optic disc structure called the “disc at risk,” which is a small diameter optic disc with or without a small (less than 0.3) or absent cup in the center of the disc (15). This feature is more easily identified in the unaffected eye.
Posterior ischemic optic neuropathy. Most cases of this variant occur spontaneously, after renal dialysis; spinal, cardiac, or organ transplant surgery; x-irradiation of the optic nerve; surgical manipulation of the retrobulbar optic nerve segments; herpes zoster infection; or connective tissue disease. Clinical manifestations will be similar to those of nonarteritic anterior ischemic optic neuropathy, except that the optic fundus will appear normal. Posterior ischemic optic neuropathy is a diagnosis of exclusion because more common causes of acute monocular visual loss with a relative afferent pupil defect and a normal-appearing optic disc are retrobulbar inflammation, infiltration by cancer, and compression by an orbital or intracranial mass lesion.
Hypotensive ischemic optic neuropathy. This variant occurs within hours to days of an episode of systemic hypotension of any cause. The optic disc may be swollen or appear normal.
Arteritic ischemic optic neuropathy. Visual recovery is rare. In the chronic phase, optic disc pallor is often accompanied by pathologic excavation of the disc, as axons and their supporting elements have been infarcted.
Nonarteritic anterior ischemic optic neuropathy. Optic disc edema resolves within 2 to 3 months. Visual function may decline for up to 3 weeks.
The Ischemic Optic Neuropathy Decompression Trial Research Group reported 42.7% overall spontaneous improvement of visual acuity of three lines or more (49). In a small study, optical coherence tomography (OCT) of the macula 2 weeks after presentation correlated with the ultimate visual outcome (25). Optic disc pallor develops without pathologic optic cup excavation, presumably because of a lower degree of infarction than in arteritic anterior ischemic optic neuropathy.
Fellow eye involvement in nonarteritic anterior ischemic optic neuropathy occurred in 15% in one study (49). Another analysis showed that it occurred in 30.6%, with a median latency of 1.2 years (82). Recurrent vision loss due to nonarteritic anterior ischemic optic neuropathy in a previously affected eye is very rare but has been documented in persistent nocturnal hypotension attributed to use of blood pressure medications in the evening (43).
Whether NAION is associated with a higher rate of subsequent cerebrovascular or cardiovascular events is unsettled. One study found an increased incidence of subsequent stroke (but not mortality) in patients with hypertension and diabetes (42). A study based on a national health insurance database reported a doubling of the hazard ratio for ischemic stroke in individuals with nonarteritic anterior ischemic optic neuropathy as compared to age-matched and gender-matched control subjects (60). This finding persisted after accounting for vascular comorbidities. A brain MRI study in 63 patients with nonarteritic anterior ischemic optic neuropathy revealed a significantly higher percentage of cerebral small vessel disease compared to control subjects matched for age, sex, and comorbidities (56). However, a review of the incidence of symptomatic stroke between 104 nonarteritic anterior ischemic optic neuropathy patients and age-matched control subjects found no significant difference (32).
A 62-year-old man with well-controlled hypertension and a 30-pack-year smoking history awoke with “darkened,” vision in the inferior visual field of the left eye 3 days prior to evaluation. He noted no headache, periocular pain with eye movement, scalp or temporal tenderness, jaw claudication, malaise, anorexia, or unusual joint or muscle pain. He had no neurologic symptoms.
Examination revealed a visual acuity of 20/20 in the right eye and 20/80 in the left eye. The temporal arteries were pulsatile and non-tender. There were no carotid bruits. A left afferent pupillary defect was present. The left optic disc demonstrated diffuse hyperemic edema, worse in the superior portion of the disc, with peripapillary flame hemorrhages and adjacent retinal arteriolar narrowing. No retinal arteriolar emboli were present. The remainder of the ophthalmologic examination was normal.
Visual field examination revealed an inferior altitudinal visual field defect in the left eye. The erythrocyte sedimentation rate was 18 mm/hour. He was instructed to stop smoking and to continue aspirin, but no additional therapy was recommended.
Over the next week, visual acuity worsened to 20/100, with an associated slight increase in optic disc edema, followed by vision stabilization. By 2 months following the onset of visual loss, the optic disc had become pale, especially in its superior half, with complete resolution of disc edema. By 6 months, visual acuity had improved to 20/60, but the visual field defect remained.
Arteritic ischemic optic neuropathy. This variant of ischemic optic neuropathy occurs almost exclusively in giant cell arteritis. Its etiology involves an environmental or infectious trigger in the context of systemic inflammation, primarily mediated by IL-6 (27). This process leads to the activation of dendritic cells, arterial invasion by monocytes and T cells, and cytokine and chemokine release, causing further immune cell recruitment, vascular injury, and intimal hyperplasia and fibrosis as well as neoangiogenesis (94). When the ophthalmic artery and its downstream branches are affected, flow to the optic nerve, retina, choroid, and other ocular structures is reduced.
Human autopsy studies have demonstrated ischemic necrosis of the prelaminar, laminar, and retrolaminar portions of the optic nerve, along with infiltration of the short posterior ciliary arteries by lymphocytes, macrophages, plasma cells, and multinucleated giant cells. Discontinuity of the internal elastic lamina is frequently seen in histological sections of the affected artery. Segments of the arteries have shown occlusion of the lumen by inflammatory thickening of the wall of the artery with or without thrombotic occlusion (66).
Nonarteritic anterior ischemic optic neuropathy. The mechanism of conventional nonarteritic anterior ischemic optic neuropathy is debated. The most common hypothesis proposes that a build-up of atherosclerotic plaque or structural changes in the wall of the posterior ciliary end-artery branches of the ophthalmic artery, exacerbated by structural "crowding" of the optic disc, eventually crosses a threshold beyond which inadequate perfusion produces irreversible axonal damage (05). Repetitive cycles of ischemia, axonal swelling, compression of blood vessels due to compartment syndrome, and further ischemia may lead to progressive nerve damage and eventual retinal ganglion cell death by apoptosis. Hayreh has proposed that nonarteritic anterior ischemic optic neuropathy sometimes occurs in the setting of nocturnal hypotension, which leads to inadequate arterial perfusion to the optic disc in the short posterior ciliary branch end-arteries and circle of Zinn-Haller surrounding the optic disc, making this a disease of the small-caliber arterioles and capillaries rather than the large-sized or medium-sized vessels affected by giant cell arteritis (38). Fluorescein angiography in nonarteritic anterior ischemic optic neuropathy has shown segmental filling delay of the optic disc and adjacent peripapillary choroid, suggesting impairment of flow at the level of the short posterior ciliary arteries (38). In contrast, the peripapillary choroidal filling was not consistently delayed compared to control subjects. One study showed that flow velocities in the ophthalmic arteries on the side of the eyes with nonarteritic anterior ischemic optic neuropathy were significantly decreased compared with those on the side of the unaffected eye (106). In that study, common and internal carotid intima-media thickness was significantly greater on the nonarteritic anterior ischemic optic neuropathy side than on the contralateral side.
Another theory is that there is the inadequate autoregulatory capacity of the arterial perfusion of the optic nerve in the setting of microvascular diseases, such as hypertension, diabetes, and atherosclerosis, or secondary to the effects of medications on autoregulation, such as erectile dysfunction drugs. Increased levels of endothelin-1 have been identified in patients with NAION (102; 101). One study suggested that sleep apnea may act as a permissive risk factor by affecting vascular endothelium in vasculopathic patients (03). A venous etiology for NAION has also been proposed (61). In this model, ischemia to the optic disc is preceded by venous congestion, leading to optic disc edema. Once optic disc edema occurs, cycles of ischemia and compression lead to further damage. In support of this theory is the observation that supports that many patients have asymptomatic optic disc elevation prior to the onset of vision loss from nonarteritic anterior ischemic optic neuropathy.
On rare occasions, nonarteritic anterior ischemic optic neuropathy can occur in several members of the same family, suggesting there may be a hereditary form of this disease. A familial form of nonarteritic anterior ischemic optic neuropathy has been identified in relatives that carry the mitochondrial mutation G4132A (30; 41).
A review of the histopathologic features in 193 eyes with NAION confirmed infarction in the prelaminar, laminar, and postlaminar regions of the optic disc (57). Cavernous degeneration of the optic nerve was noted in 36% of eyes, with mucopolysaccharide deposition in over half, frequently distorting the remaining intact nerve fibers. This finding supports the hypothesis of secondary damage of axons caused by swelling of adjacent axons. However, no consistent abnormalities were noted in the vessels within the optic disc, which belies the theory that structural damage to the arteries prior to the onset of vision loss is important.
Utilizing laser-activated rose bengal induction of microvascular thrombosis, rodent and primate models for nonarteritic anterior ischemic optic neuropathy have been developed (10; 22). These models have demonstrated that a cascade of molecular changes at the level of the optic nerve axons leads to optic nerve ischemia and apoptosis. Intravitreal anti-NOGO antibody has preserved axonal structure and optic nerve function measured by electrophysiologically (54). Prostaglandin J2 had similar effects and additionally decreased optic disc edema (69). Studies are needed to determine whether combining agents with different mechanisms could have a synergistic effect.
Posterior ischemic optic neuropathy. Posterior ischemic optic neuropathy is believed to result from impaired perfusion from the pial plexus to the retrobulbar portion of the optic nerve (39). The non-perioperative form of posterior ischemic optic neuropathy appears to be associated with underlying small vessel disease, such as diabetes, hypertension, and hypercholesterolemia. The perioperative form of posterior ischemic optic neuropathy is believed to result from a combination of blood loss and hypotension under general anesthesia. A large, multicenter, case-controlled study of perioperative ischemic optic neuropathy after spinal fusion surgery attributed the event to the following factors: obesity, male sex, Wilson frame use, longer anesthesia duration, high estimated blood loss, and a decreased use of colloid to maintain vascular volume (89). These results, along with medical claims-based studies demonstrating an association with obesity, need for blood transfusion, and carotid artery stenosis, suggest patient positioning and hemodynamic contributions to this condition (98; 97).
Autopsy studies of patients with cardiac or cerebrovascular disease have shown that the pial vessels supplying the retrobulbar optic nerve may show arteriosclerotic changes. Some patients with these anatomic abnormalities show infarcts of the retrobulbar optic nerve (48). These findings support the hypothesis that posterior ischemic optic neuropathy is caused by arteriosclerosis in some cases. Histopathology of the optic nerve obtained from a patient with posterior ischemic optic neuropathy who had no underlying vascular disease and who suffered posterior ischemic optic neuropathy following profound hypotension and anemia showed infarction of the retrolaminar portion of the optic nerve (53). Pial vessels may be subject to compression due to local edema from hypoxia. Most patients with posterior ischemic optic neuropathy have no abnormalities on fluorescein angiography, indicating that the circulation to the eye is not involved.
Studies on a rat model of posterior ischemic optic neuropathy have shown that hemodilution and head-down tilt induce functional optic nerve changes and optic nerve swelling (121; 96).
Arteritic anterior ischemic optic neuropathy. The incidence of this ischemic variant has been reported at 0.36 per 100,000 population (52). It occurs exclusively in older individuals, with cases rarely seen under age 50. There is no gender predisposition, but the disease occurs more frequently in white people than in black or Hispanic individuals.
Nonarteritic ischemic optic neuropathy. Nonarteritic ischemic optic neuropathy is the most common form of acute optic neuropathy in patients older than 50 years of age, with an estimated annual incidence in the United States of 2.3 to 10.2 per 100,000, resulting in up to 6000 new cases each year (52).
The risk factors commonly associated with NAION are age, male gender, white race, and diabetes with end-organ involvement (19). A study demonstrated that the majority of patients are white, followed by Blacks and those of Asian origin. (07). Systemic hypertension has been documented in up to 49% of patients, with diabetes being present in up to 25% (42; 50). Carotid occlusive disease is not significantly associated with nonarteritic ischemic optic neuropathy (34).
Nonarteritic ischemic optic neuropathy has been identified occasionally as the cause of vision loss immediately following cataract or LASIK surgery. In one study, patients with a previous history of nonarteritic ischemic optic neuropathy had a 4-fold increased risk of developing nonarteritic ischemic optic neuropathy in the fellow eye after cataract surgery (58). Another study suggested no association (75).
The cause of nonarteritic ischemic optic neuropathy in younger patients or those without conventional arteriosclerotic risk factors has been a mystery. Studies of homocysteine levels and mutations of the methylene tetrahydrofolate reductase gene have shown conflicting results (13; 36; 35). Prothrombotic risk factors such as protein C, protein S, and antithrombin III deficiency have not been implicated (103). However, a patient with nonarteritic ischemic optic neuropathy had antiphospholipid antibody syndrome and the factor V Leiden mutation (112). A small retrospective study of factor V Leiden mutation in patients with nonarteritic ischemic optic neuropathy demonstrated a 25% occurrence (81).
Whether phosphodiesterase inhibitors used for erectile dysfunction or pulmonary hypertension cause nonarteritic ischemic optic neuropathy is unsettled. Nonarteritic ischemic optic neuropathy following their use has been documented (88; 87), but cup-to-disc ratios were small in all patients, and most patients also had typical risk factors for nonarteritic ischemic optic neuropathy, such as hypertension, diabetes, or hyperlipidemia. Notably, FDA-mandated prospective studies of individuals who used PDE-5 inhibitors in the month prior to NAION demonstrated increased odds of nonarteritic ischemic optic neuropathy among those who used PDE-5 inhibitors within five half-lives prior to the nonarteritic ischemic optic neuropathy event (17).
A causal relationship between nonarteritic ischemic optic neuropathy and amiodarone use has not been firmly established (79). In many cases, unilateral or bilateral optic disc edema may be present for weeks or months before vision loss occurs. Vision loss can be abrupt or insidious (84). Improvement in visual field loss or visual acuity has been documented with the discontinuation of amiodarone, raising the question of whether this form of optic neuropathy is truly nonarteritic ischemic optic neuropathy (40; 71; 70).
A meta-analysis suggested that obstructive sleep apnea could be a risk factor for nonarteritic ischemic optic neuropathy (122), but a causal relationship has not been documented (74; 09; 117).
A single-center retrospective case series of five patients linked nonarteritic ischemic optic neuropathy to high-altitude sickness. Patients exhibited a progressive course of vision loss and severe thinning of retinal nerve fiber layer (RNFL) (64).
Optic disc drusen, which are calcified deposits located in optic nerve head, have been proposed as an independent risk factor of nonarteritic ischemic optic neuropathy, based on a study that showed that nonarteritic ischemic optic neuropathy patients with optic disc drusen more often had no vascular risk factors as compared to nonarteritic ischemic optic neuropathy patients without optic disc drusen (99). In another study, the prevalence of optic disc drusen in young nonarteritic ischemic optic neuropathy occurring in patients aged 50 years or younger was significantly higher than in the general population (33).
Retinal vein occlusion and age-related macular degeneration have been associated with nonarteritic ischemic optic neuropathy (19).
Several case reports have described nonarteritic ischemic optic neuropathy during COVID-19 infection or after COVID-19 vaccination. Although the pathogenesis is not well understood, it is speculated that the immune-mediated response or direct ischemic events secondary to virus-associated endotheliopathy contributed to the impaired microvascular network of the optic nerve head (76; 80; 118).
A prospective comparative study showed that three or more injections of intravitreal anti-VEGF were risk factors for developing nonarteritic ischemic optic neuropathy in patients with diabetes (21).
Posterior ischemic optic neuropathy. Posterior ischemic optic neuropathy has an incidence of only 0.087% (14). Patients with posterior ischemic optic neuropathy associated with surgery are younger than those whose posterior ischemic optic neuropathy is attributed to underlying vasculopathy (100). Posterior ischemic optic neuropathy following spine surgery decreased between 1998 and 2013 (98; 97).
In medical claims-based studies, ischemic optic neuropathy following cardiac surgery was associated with carotid artery stenosis and degenerative eye conditions (97). Ischemic optic neuropathy following spinal fusion surgery was associated with older age, male gender, obesity, and transfusion (98).
Nonarteritic anterior ischemic optic neuropathy. There are no data regarding whether improved control of vascular risk factors or correction of hypotension in overly treated systemic hypertension might decrease the risk or severity of nonarteritic ischemic optic neuropathy in the fellow eye.
Data regarding the role of aspirin in decreasing the severity of nonarteritic ischemic optic neuropathy and reducing its incidence of fellow eye involvement after the initial episode do not demonstrate a clear-cut beneficial effect (08). One study suggested that larger doses of aspirin (325 mg daily) might be more effective than lower doses (100 mg daily) in preventing second eye involvement (104), but the numbers of patients in each group were small. Although a cause-and-effect relationship between use of PDE-5 inhibitors and prompt development of nonarteritic ischemic optic neuropathy in one has not been firmly established, most practitioners counsel patients who have suffered single-eye NAION that there may be increased risk of nonarteritic ischemic optic neuropathy in the fellow eye (86). A prospective study demonstrated that non-adherence to sleep apnea treatment in patients with prior nonarteritic ischemic optic neuropathy was associated with an increased risk of second eye nonarteritic ischemic optic neuropathy (02). Further studies are required to determine the role of the institution of continuous positive airway pressure or other treatment.
Perioperative ischemic optic neuropathy. In ischemic optic neuropathy associated with surgical procedures, particularly spinal surgery, prophylaxis is directed at avoiding large intraoperative hypotension, significant blood loss, perioperative anemia, prolonged surgery, and pressure on the orbit and globe, particularly if the patient is in the prone position. A preoperative risk factor scoring system for perioperative ischemic optic neuropathy in spinal fusion surgery proposed that the highest relative risk was for a man, aged 40 to 64 years with obstructive sleep apnea (108). Another study identified hypertension, chronic anemia, and carotid artery stenosis as risk factors, acknowledging that perioperative ischemic optic neuropathy occurs even without these risk factors (77).
Nonarteritic and arteritic ischemic optic neuropathy. These forms must be differentiated from nonischemic optic neuropathies that manifest with optic disc swelling, including optic neuritis, syphilitic or sarcoid-related optic nerve inflammation, cancerous infiltration of the optic nerve, optic nerve compression, asymmetric (apparently uniocular) papilledema due to elevated intracranial pressure, and other forms of optic disc edema, including diabetic papillopathy, papillophlebitis, sinusitis, vasculitis, orbital inflammation, IgG4-related disease, and meningoencephalitis. Optic neuritis has a similar speed of onset and causes a similar pattern of visual field loss. However, older age at onset, lack of periocular pain with eye movement, segmental or pallid optic disc edema, and optic disc hemorrhages favor nonarteritic ischemic optic neuropathy.
In atypical cases, brain and orbit MRI can be helpful in differential diagnosis. Fluorescein angiography may show delayed optic disc filling in nonarteritic ischemic optic neuropathy, whereas the timing of filling is normal in optic neuritis (06). MRI is typically normal in nonarteritic ischemic optic neuropathy, whereas enhancement is usually seen in optic neuritis (93). Another study found that diffusion-weighted imaging and postcontrast enhancement of the intraorbital optic nerve are more likely to occur in optic neuritis, whereas postcontrast enhancement of the optic disc is more likely in nonarteritic ischemic optic neuropathy (01). One MRI study showed that retrobulbar optic nerve enhancement and the distribution of cerebral white matter lesions are helpful in differentiating optic neuritis from nonarteritic ischemic optic neuropathy (85).
Optic nerve inflammation associated with syphilis or sarcoidosis is often associated with other intraocular inflammatory signs, such as uveitis. Proptosis, lid abnormalities, and eye movement abnormalities favor a diagnosis of an orbital process, including inflammation or tumor. Atypical features of nonarteritic ischemic optic neuropathy include age of onset of less that 40 years, periocular pain, lack of vasculopathic risk factors, bilateral simultaneous onset, recurrent attacks, macular star figure, and lack of regression of disc edema after 4 weeks (11).
Posterior ischemic optic neuropathy. Posterior ischemic optic neuropathy must be differentiated from other retrobulbar optic neuropathies, such as infectious and noninfectious optic neuritis, traumatic, compressive, hereditary, and toxic optic neuropathies.
Presumed perioperative ischemic optic neuropathy should be differentiated from other causes of postoperative vision loss such as central retinal artery occlusion, which should show a cherry red spot on ophthalmoscopic examination within 24 hours of onset and retinal nerve fiber layer thickening on optical coherence tomography even earlier.
Nonarteritic ischemic optic neuropathy. Anatomical risk factors for nonarteritic ischemic optic neuropathy include a crowded optic disc (“disc at risk”), vitreopapillary traction, and optic disc drusen (99; 33; 59). An increase in intraocular pressure may induce impaired blood flow autoregulation (18). COVID-19, its vaccination, syphilis, and herpesvirus infection may be implicated (105). The systemic disorders include septic and cardiogenic shock, hypovolemic crisis, nocturnal systemic arterial hypotension, metabolic syndrome, cardiovascular and cerebrovascular diseases, chronic renal failure and dialysis, obstructive sleep apnea, and hypercoagulable states.
Posterior ischemic optic neuropathy. Posterior ischemic optic neuropathy occurs in the setting of chest, spine, and middle fossa brain surgery, and in arteriosclerosis, herpes zoster infection, connective tissue disorders, and radiation to the anterior visual pathway. Provocative medications include phosphodiesterase type-5 inhibitors, amiodarone, interferon-alpha, oral contraceptives, sumatriptan, and antihypertensive therapy taken before sleep.
Arteritic ischemic optic neuropathy. In patients over age 50, arteritic ischemic optic neuropathy must be suspected. Accordingly, laboratory testing includes erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and platelet count. Most cases will show marked elevation of erythrocyte sedimentation rate (mean 70 mm/hour, often more than 100 mm/hour) and CRP. Acute phase reactant elevation is, however, merely an indication of inflammation or cancer. On the other hand, ESR may be normal in up to 16% of patients with arteritic ischemic optic neuropathy.
Arteritic ischemic optic neuropathy may demonstrate perineural enhancement in retrobulbar optic nerve on MRI (63). Restricted diffusion of the optic disc or nerve was seen on MRI in anterior ischemic optic neuropathy (12; 78). A study using 3-tesla high-resolution vessel wall MRI showed that enhancement of ophthalmic artery, optic nerve sheath complex, posterior ciliary, or extracranial arteries could be used to distinguish between arteritic and nonarteritic anterior ischemic optic neuropathy (73).
Doppler ultrasound of the temporal and axillary arteries is used as a noninvasive adjunct to biopsy. In one large study, the presence of the halo sign in the temporal artery was as sensitive and nearly as specific as temporal artery biopsy (65). However, a metaanalysis found that sensitivity and specificity of temporal artery ultrasound were only 68% and 81%, respectively, using biopsy as the gold standard (92). In a further meta-analysis, high-resolution MRI of the superficial temporal artery had a sensitivity of 91% and a specificity of 78% compared to biopsy, with significantly higher specificity when using 3D high-resolution MRI rather than 2D (123). Imaging of the aorta using MRI or PET can confirm the initial diagnosis and assist in monitoring for relapsing disease (119).
A positive temporal artery biopsy confirms the diagnosis of giant cell arteritis. This procedure is recommended in any case of ischemic optic neuropathy in which arteritis is suspected. A biopsy length of at least 1 cm is recommended to avoid missing skip lesions (24; 67). A positive biopsy provides support for the long-term use of systemic corticosteroid therapy, with its attendant systemic complications.
Nonarteritic anterior ischemic optic neuropathy. This variant is a clinical diagnosis. Retrobulbar imaging, rarely performed, is apart from enhancement of the optic disc. In the rare cases when it is caused by hypotension or cavernous sinus venous thrombosis, MRI may demonstrate restricted diffusion (120; 23). A meta-analysis demonstrated that peripapillary capillary density, nerve fiber layer thickness, and macular ganglion cell complex thickness measured by optical coherence tomography angiography are reduced in nonarteritic anterior ischemic optic neuropathy (62).
Posterior ischemic optic neuropathy. Neuroimaging of the optic nerves/orbit and brain should be performed in suspected posterior ischemic optic neuropathy to rule out an alternative cause of optic nerve injury. Enhancement and restricted diffusion in the orbital segment of the optic nerves has been demonstrated (29; 16).
Arteritic ischemic optic neuropathy. If giant cell arteritis is suspected, early corticosteroid therapy is critical to avoid irreversible vision loss in the unaffected eye. It should be instituted immediately. Confirmation by temporal artery biopsy should be done as soon as possible and ideally within 2 weeks of treatment initiation, as corticosteroid treatment that persists beyond that period will attenuate the pathologic signs. High dose intravenous methylprednisolone at 500 mg to 1 g per day for the first 3 to 5 days is most often recommended, particularly when the patient is seen in the acute phase. This delivery mode produces higher blood medication levels more rapidly than does oral therapy and may provide better visual outcomes (20; 45). After that, oral prednisone at doses up to 100 mg daily is administered in follow-up and tapered slowly.
Tocilizumab, an anti-IL6 receptor antibody, was shown by the GiACTA trial to reduce cumulative corticosteroid doses in patients with giant cell arteritis, to increase the likelihood of sustained remission, and to lengthen the time to first relapse (116; 114; 115). The American College of Rheumatology/Vasculitis Foundation recommends adding tocilizumab to oral corticosteroid treatment. If clinical remission is not achieved, abatacept (CTLA4-Ig) or methotrexate may be added (67). The European League Against Rheumatism limits its recommendation for using tocilizumab as adjunctive therapy to patients with refractory or relapsing disease or to those who have an increased risk of corticosteroid-associated complications (46).
Frequent monitoring of systemic and ophthalmic manifestations, fundus examination, and laboratory indicators of inflammation, such as the ESR and CRP, should be performed after the diagnosis of giant cell arteritis has been established. Partnership with a rheumatologist is valuable.
Nonarteritic anterior ischemic optic neuropathy. No treatment has been demonstrated to improve visual outcomes in nonarteritic anterior ischemic optic neuropathy. Optic nerve sheath decompression (49; 51), optic neurotomy (109; 110), vitrectomy (72), intravitreal injection (55; 90; 95), aspirin, anticoagulants, antiplatelet agents, vasodilators, vasopressors, prostaglandin E1 (113), intraocular pressure-lowering agents, steroids, diphenylhydantoin, erythropoietin (83), and levodopa (31; 47) have failed to provide benefit. A Cochrane review confirmed that optic nerve decompression surgery is ineffective in nonarteritic anterior ischemic optic neuropathy (26).
The controversy over the utility of corticosteroid treatment of nonarteritic anterior ischemic optic neuropathy is far from settled. In favor of their use is the postulate that optic disc swelling may constitute a compartment syndrome. Hayreh and colleagues reported improvement of visual acuity in patients with visual acuity of 20/70 or worse who received treatment with oral prednisone within 2 weeks of onset (44). Unfortunately, the nonrandomized methodology limits the generalizability of the finding because some number of patients with nonarteritic anterior ischemic optic neuropathy sustain spontaneous improvement. A randomized controlled trial examining the effectiveness of oral corticosteroids in nondiabetic nonarteritic anterior ischemic optic neuropathy patients did not demonstrate improvement in visual outcome (107). However, oral corticosteroid treatment was associated with faster resolution of optic disc edema and improved electrophysiologic measures. A retrospective study of intravitreal triamcinolone found that injection within 15 days of symptom onset led to improvement of visual acuity and visual field at 6 months (28).
Intravitreal small interfering ribonucleic acid (siRNA) is an emerging neuroprotective treatment for Nonarteritic anterior ischemic optic neuropathy. By inhibiting caspase-2, siRNA prevents the apoptosis cascade of neurons (111). In a phase 1 trial, 53.6% participants had gained three or more lines of visual acuity at 3 months of follow-up (91). None of the subjects had worsening of visual acuity by three or more lines. A phase 2/3 randomized, controlled trial was terminated in 2020 when their interim analysis did not warrant continue enrollment. The current management strategy involves identification and alteration of possible risk factors with an emphasis on prevention.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Yan Yan MD PhD
Dr. Yan of Ren Ji Hospital and Shanghai Jiao Tong University School of Medicine has no relevant financial relationships to disclose.
See Profile
Jonathan D Trobe MD
Dr. Trobe of the University of Michigan has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
Neuro-Oncology
Dec. 13, 2024
Neuro-Ophthalmology & Neuro-Otology
Dec. 02, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 24, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuro-Ophthalmology & Neuro-Otology
Nov. 22, 2024
Neuromuscular Disorders
Oct. 29, 2024