Sleep Disorders
Sleeptalking
Jan. 18, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In today’s society, transmeridian air travel is a common mode of transportation. Individuals crossing several time zones can experience jet lag disorder, which is characterized by symptoms of difficulty falling asleep or excessive daytime sleepiness, general malaise, and somatic complaints. Jet lag disorder may be partially preventable or treatable by understanding the basics of circadian rhythm physiology and its intimate interactions with the sleep-wake cycle. The authors provide an update on the current understanding of jet lag disorder, including diagnostic criteria based on the ICSD-3-TR, pathophysiology, and therapeutic approaches to minimize symptoms, as well as when it is appropriate to accelerate alignment of the endogenous clock with the new time zone. Of note, there has been increased interest in this disorder in the context of optimizing performance for athletes who have to repeatedly cross multiple times zones as part of competition.
|
• Jet lag disorder is caused by a temporary mismatch between the timing of the sleep and wake rhythm generated by the endogenous circadian clock with that of the new time zone’s light-dark cycle and corresponding change in the timing of sleep and wake pattern and other behaviors, as well as the change in the light-dark cycle. | |
|
• Symptoms include difficulties in initiating and maintaining sleep, excessive daytime sleepiness, decrease in subjective alertness and performance, impairment of daytime functioning, and somatic complaints, with gastrointestinal symptoms being most common. | |
|
• Jet lag symptoms are more severe for most individuals when flying eastward. | |
|
• The best strategy for brief stays (2 to 3 days) in the new time zone is to keep the original sleep-wake schedule, if at all possible. | |
|
• For longer stays, timed melatonin with strategic exposure to light and avoidance of light at specific times are the best strategies to accelerate the alignment of endogenous circadian rhythms to the new time zone. |
Time-zone change syndrome (jet lag) did not exist prior to the invention of jet planes during World War II and became common when commercial transmeridian air travel by jet became commonplace in the 1960s. Hundreds of millions of travelers cross time zones by jet each year and, for the majority of travelers, jet lag is a minor and temporary nuisance. For a minority that travel frequently by jet, time-zone change syndrome is a major health problem. The current formal name used in the 3rd edition, text revision of the International Classification of Sleep Disorders is jet lag disorder. Alternate names include time zone change syndrome, jet lag syndrome, jet lag type, and flight dysrhythmia (01).
The diagnostic criteria established by the American Academy of Sleep Medicine in the International Classification of Sleep Disorders, 3rd edition, text revision state that criteria A through C must be met in order for a diagnosis of jet lag disorder to be made:
|
(A) There is a complaint of insomnia or excessive daytime sleepiness, accompanied by reduction of total sleep time, associated with transmeridian jet travel across at least two time zones. | |
|
(B) There is associated impairment of daytime function, general malaise, or somatic symptoms (eg, gastrointestinal disturbance) within 1 to 2 days after travel. | |
|
(C) The sleep disturbance is not better explained by another current sleep disorder, medical or neurologic disorder, mental disorder, medication use, or substance use disorder. |
Jet lag disorder involves a temporary mismatch between the timing of the endogenous circadian clock and timing required by the new time zone. Symptoms typically last 2 to 4 days but may persist for up to 7 to 10 days. Duration and severity of symptoms are typically proportionate to the direction of travel and the number of time zones crossed.
Individuals experience difficulties in initiating and maintaining sleep, excessive daytime sleepiness, fatigue, decrease in subjective alertness, and somatic complaints including frequent urination and gastrointestinal function disturbances (01).
Other common symptoms include difficulty concentrating, decrease in attention, irritability, and anxiety, which can lead to impaired daytime functioning. This alteration in executive function can result in errors in mental performance (26) and impaired decision-making ability. This can be particularly dangerous in airline pilots. Deployed military and elite athletes have been found to have deterioration in their athletic performance after rapid travel across time zones (19).
Following eastward travel, individuals may have difficulties with sleep initiation. These patients are attempting to sleep during a time when their internal circadian rhythm is promoting wakefulness. In the morning they often experience the opposite, with difficulty awakening and daytime fatigue as it is still their biological night, a time when the internal circadian clock is promoting sleep.
Individuals traveling westward often experience sleepiness during the early evening hours as their internal circadian clock is promoting sleep. In addition, some experience difficulties maintaining sleep with early morning awakenings as their internal circadian clock is promoting wakefulness (01).
For most individuals, eastward travel results in more severe symptoms and is more difficult to adapt to than westbound travel. This is due to the fact that the endogenous circadian period in most humans is slightly longer than 24 hours. It is, therefore, much easier to adapt to the external cues in westbound travel where a delay shift is more easily achieved (09). However, there are individual differences related to age, gender, and ethnicity that also influence the ability to adjust to the direction of travel.
Acute complications of jet lag disorder. Acute jet lag symptoms are self-limited unless the patient travels frequently between time zones; in the latter case, chronic sleep disturbances with impaired performance and irritability may ensue. Some of the symptoms of jet lag may be associated with alterations in the microbiome (51).
Studies suggest that individuals with mood disorders are sensitive to circadian disruption and that transmeridian travel with subsequent jet lag may precipitate underlying mood disorders. Westward travel has shown increased rates of depressive episodes, whereas manic and hypomanic episodes are more likely triggered with eastward travel (18). In addition, more recent evidence demonstrates that mood may actually have a greater impact on the presence of jet lag symptoms than circadian misalignment (45). There are limited conclusive data on the relationship between mood and jet lag disorder, and further research is needed to identify strategies to limit the effects of transmeridian travel (18).
Female airline personnel have been found to have a higher incidence of menstrual disorders related to their frequent transmeridian travel and shift work (39).
Self-treatment with alcohol or nonprescription sedatives complicates the clinical picture in some cases. Sleep deprivation and alcohol exacerbate sleep apnea, and the combination of these, especially during night flights, will presumably act synergistically to worsen apnea even further.
Chronic complications of jet lag disorder. Over the past decade there has been significant interest in the long-term complications of jet lag disorder. Chronic circadian disruption by light at night and chronic jet lag were found to accelerate tumor growth in desynchronized animals (15). Studies involving mice found that chronic jet lag induced spontaneous hepatocellular carcinoma driven by jet lag induced genome wide gene deregulation and liver metabolic dysfunction (22). In addition, chronic jet lag alters the gut microbiome and promotes the development of fatty liver disease (59). Although chronic circadian disruption has been shown to be detrimental in animal studies, human data have not yet shown an increased cancer incidence in chronic jet lag (38; 28).
Long-term cognitive consequences of frequent jet lag are largely unknown, but a concern has been expressed about permanent structural and functional brain changes (14; 58). In rats, for example, repeated weekly jet lag reduced the circadian amplitude of gene expression in the SCN, and it also inhibited hippocampal neurogenesis. The degree of reduction in gene expression and in neurogenesis was dependent on the direction and duration of the circadian shifts; a greater decrease in neurogenesis was observed when the phase was advanced versus delayed (56; 25). Chronic jet lag has also been found to accelerate locomotor aging in Drosophila, and this effect was alleviated by environmental changes, which restored normal circadian rhythms (52).
A 49-year-old businesswoman complained of prolonged disturbed sleep after returning home from overseas flights. Two years previously she established an overseas enterprise that necessitated westward air travel over 10 time zones every 2 to 3 months, staying about a week and then returning home. Her sleep was normal until that time. When she visited her overseas subsidiary, she slept relatively well after the flight fatigue wore off. However, following her return home, she suffered from unbearable fatigue and sleepiness during the daytime hours, and her night sleep was fragmented and nonrestorative. The sleep disturbance would last for 2 to 3 weeks and gradually subside until her next flight. The disruption that the sleep disorder caused in her life was especially significant. When afflicted by the disorder, she was short-tempered and abusive toward family and employees, visited her physician for complaints of upset stomach and constipation, and felt depressed and helpless, being unable to get rid of sleepiness during the day. Her past medical history and examination were unremarkable. The patient was advised to start taking sustained-release melatonin 3 mg at the time corresponding to 20:00 hours in her home time zone, starting one day prior to departure from overseas and continue on the medication for 2 weeks following her arrival home. Additionally, during the first week at home, she was advised to use eszopiclone if unable to fall asleep for 1 hour after her habitual bedtime. Early evening physical exercise was also encouraged. The treatment allowed her to sleep much better at night after returning from her business travels, she was much less sleepy during the day, and felt her physical and mental well-being were much improved.
Jet lag disorder occurs due to a misalignment of an individual’s endogenous circadian timing with the external clock time (destination’s local time zone). After rapid travel, typically two or more time zones, the endogenous circadian system initially remains aligned to the environmental time cues of the home time zone and only slowly resets to the new environmental time schedule.
The severity and duration of these symptoms is dependent on many factors: the number of the time zones traveled, the direction of travel (east or west), departure and arrival times, the ability to sleep while traveling, exposure to local time cues, and individual differences in phase tolerance (01).
Flight-related stress and fatigue, in addition to sleep deprivation, contribute to the clinical picture in the first day or two on arrival to the new time zone.
Almost every cell in the organism has active molecular oscillators that regulate circadian gene expression in response to various time cues, mainly chemical changes induced by feeding and temperature changes (30). In the absence of a central clock to coordinate those rhythms, the myriad peripheral pacemakers would produce a cacophony of rhythms that would make a coordinated circadian behavior impossible.
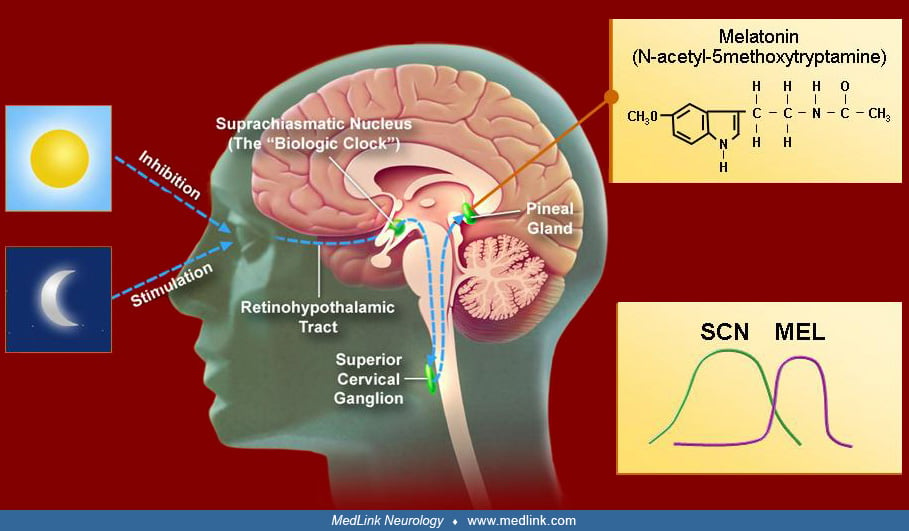
The paired suprachiasmatic nuclei (SCN) of the hypothalamus have been established as the site of the central mammalian circadian oscillator. This grouping of about 10,000 anterior ventromedial hypothalamic neurons manifests a high amplitude circadian pattern of firing both in intact, freely behaving animals and in vitro. The SCN is composed of multiple single cell circadian oscillators that, when synchronized, generate a coordinated circadian output that regulates peripheral “clocks” by transmission of circadian timing signals. This regulation is achieved by means of direct and indirect projections to other regulatory brain areas, modulating in turn their circadian outputs (44), and coordinating other overt rhythms (eg, arousal, hormonal secretion, temperature, feeding, etc.). Daily behavioral, vegetative, and circadian firing rhythms of other brain regions disappear if the SCN are lesioned, and some, but not all, rhythms are restored with fetal brain tissue transplants into the anterior third ventricle. Therefore, diffusible SCN output signals must also reach peripheral tissues, thus, adding to the orchestrating role of the SCN; these signals were identified as transforming growth factor-alpha and prokineticin 2.
The biological clocks of average humans of all ages have an endogenous circadian cycle of slightly more than 24 hours, generally about 24.2 hours (09; 55). If all temporal cues (zeitgeber, German for “time givers”) are removed, daily rhythms are progressively phase delayed relative to the external clock time. Keeping the basic 24-hour cycle involves daily synchronizing of the internal clocks with the shorter environmental cycle following external zeitgebers (a process known as entraining, a control of one oscillating process by another). This circadian correction is achieved by advancing the internal clocks by a fixed time period (about 0.2 hours) every day.
Light is the main zeitgeber of endogenous clocks in humans, as it is in other animals and plants. The human circadian system is more sensitive to short-wave blue-green light than to long-wave red-spectrum light (54). The major afferent input to the SCN consists of a melanopsin-containing subset of intrinsically photosensitive retinal ganglion cells whose axons depart the optic chiasm to synapse on suprachiasmatic nuclei cells (04).
This retinohypothalamic tract transmits nonvisual, light-dark information to the SCN, which is mediated through glutamate. There is an additional light-dark information pathway from the intergeniculate leaflet (located within the lateral geniculate body of the thalamus), the geniculate-hypothalamic tract, where neuropeptide Y is the main neurotransmitter. The intergeniculate leaflet projects heavily to the SCN and other brain areas associated with circadian timekeeping. SCN are also densely innervated by serotonergic fibers from the brainstem raphe nuclei, and there is evidence that serotonin is involved in the behavioral and light modulation of the circadian rhythm.
Two features of the mammalian circadian system provide flexibility in circadian programming to exploit temporal regularities of social stimuli or food availability. One feature is the sensitivity of the SCN pacemaker to behavioral arousal stimulated during the usual sleep period, which can reset its phase and modulate its response to light-dark stimuli. Neural pathways from the brainstem and thalamus mediate these effects by releasing neurochemicals that inhibit retinal inputs to the SCN clock or that alter clock-gene expression in SCN clock cells. A second feature is the sensitivity of circadian oscillators outside of the SCN to stimuli associated with food intake, which enables animals to uncouple rhythms of behavior and physiology from light-dark cycles and align these with predictable daily mealtimes. The location of oscillators necessary for food-entrained behavioral rhythms is not yet certain. The role of these two features in resetting the circadian clock in humans is also uncertain (31).
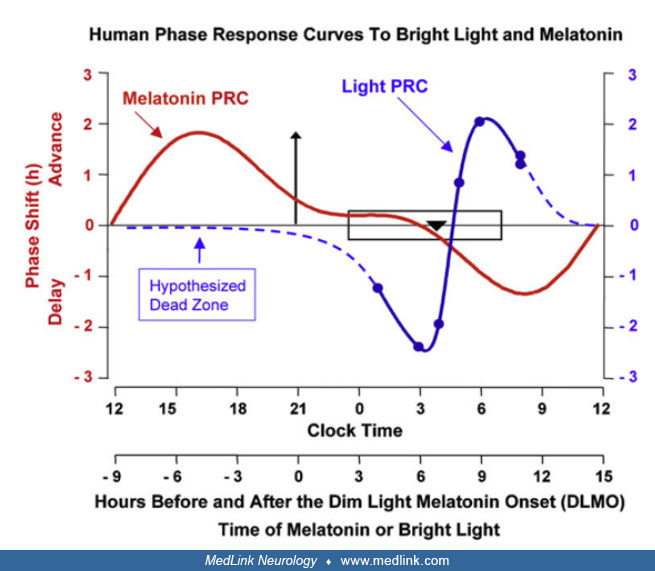
There are three fundamental characteristics to the resetting capacity of the human circadian clock by light. First, the maximal response only occurs at certain circadian times, generally a few hours before or after the nadir of core body temperature, which occurs a few hours before wake time (between 3:00 AM and 5:00 AM in most humans); thus, the “window of opportunity” for phase shift normally occurs during the dark period. Stimuli applied during most of the daylight period have little effect on circadian phase timing, although there is some evidence that the human circadian pacemaker may be sensitive to bright light throughout the day (20). Second, the direction of resetting (advance or delay) is dependent on the circadian time of exposure; light exposure early in the dark period delays the phase, whereas exposure late in the dark period advances it. Third, the amount of maximal daily resetting is limited to 1 to 3 hours (47). Plots of the magnitude and the direction of response (phase change) against the circadian time of light stimulus application (phase-response curve) reveal increasing amounts of delay from dusk to about halfway through the dark period (which roughly coincides with the nadir in core body temperature).
The direction of phase change then rapidly switches to maximal phase advances when the stimulus is applied near the beginning of the second half of the dark period, after which the advance response declines as the light stimulus moves closer to subjective dawn (53). The daily phase-advance in humans that keeps pace with the 24-hour day is a process that occurs immediately following arising in the morning and exposing the eyes to sufficient light.
The role of melatonin in the human circadian cycle is modulatory. The SCN express dense melatonin receptors, probably establishing a feedback mechanism. It is not clear whether endogenous melatonin entrains other circadian rhythms. Exogenous melatonin, however, can shift circadian phase, exhibiting a phase-response curve that is roughly a mirror image of the phase-response curve of light (07). The direction and the magnitude of the shift depend on the circadian time at which the melatonin is applied. With exogenous melatonin, peak phase advance occurs prior to the time of dim light melatonin secretion onset (2 to 3 hours before sleep onset), and peak phase delay occurs about 12 hours later. It also affects other endogenous rhythms, like temperature, cortisol secretion, and the sleep-wake cycle. Appropriately timed light exposure and melatonin may reinforce a desired effect (41); indeed, it is possible that the physiological role of the night melatonin secretion is to reinforce the daily resetting of the endogenous clock by the morning light and to provide additional fine-tuning (02; 27). Mutually reinforcing timed application of light and exogenous melatonin is used in treating circadian rhythm sleep disorders (41; 36).
The sleep-wake cycle is a major overt manifestation of the circadian rhythm, possibly through SCN direct and indirect projections to wake- and sleep-promoting brain regions. However, compared to other endogenous rhythms like core body temperature or melatonin, it is more loosely associated with the circadian pacemaker and is also influenced by noncircadian homeostatic factors (eg, prior sleep deprivation). Sleep propensity is governed at any time by the interaction of two processes: (1) an oscillating circadian process coupled to other circadian rhythms (eg, melatonin secretion and core body temperature rhythms) that promote sleepiness at night and contribute to the afternoon “siesta” period; and (2) a monotonously increasing homeostatic process reflecting prior sleep deprivation that discharges during sleep (10). The detailed description of the interaction of these processes is beyond the scope of this review; suffice is to say that the classic 2-process interaction model is an abstraction, and the net result of sleep alertness is much more than the algebraic sum of the two processes.
A significant, partially genetically determined, interindividual variability exists, which determines, among other factors, the person’s being an evening or morning type (24).
In transmeridian travelers, the homeostatic process remains essentially unchanged (although it may be influenced by in-transit sleep deprivation), whereas the circadian process is initially aligned with the external time of origin and undergoes gradual realignment with zeitgebers of the place of destination. This change of the relationships between the homeostatic and the circadian sleep processes adds to the temporary disruption of sleep periodicity.
The adjustment process of the circadian timing system to a new external time schedule is slow and asymmetrical, being faster for westbound flights (32). The directional asymmetry of the amounts of daily adjustment may be due to the longer than 24-hour intrinsic circadian period of most individuals, which favors phase delay (equivalent to westward travel) over advance (eastward travel). However, after crossing eight or more time zones in the eastward direction, re-entrainment is frequently achieved by antidromic phase response (ie, further phase delay, rather than advance) (50; 40). This is metaphorically similar to the need to drive around the block in order to reach the beginning of a one-way street. After these long flights, sunlight at dusk may be misinterpreted as dawn and vice versa, thus, confusing the circadian system and causing it to re-entrain in the opposite direction.
The re-entrainment issue becomes even more complicated if the traveler is jet-lagged to begin with (eg, she travels a multi-legged trans-meridian journey), if she begins her travel while being a shift-worker, or if she is an extreme evening person.
The exact biological origin of the malaise in jet lag disorder is unknown. Intuitively, malaise may result from the dissociation among the broad array of internally timed functions other than sleep-wake cycle due to the apparent slower adjustment of some individuals. For example, the apparent cortisol rhythm phase adjusts more slowly than other rhythms after time-zone shifts and will, therefore, be dissociated in timing for a few days relative to rhythms that have synchronized faster (35). In addition, the timing of some entrainment signal may also heighten some of the jet lag symptoms. Recent data have shown that meal timing in airline personnel may have a relationship to symptoms of anxiety and depression (57). However, it is possible that the apparent difference in the rate of entrainment is due to different masking influences of external variables on uniformly entraining internal rhythms.
Jet lag disorder can affect individuals of any age, sex, and racial group. Virtually all individuals will experience jet lag symptoms after crossing three or more time zones. Some individuals are more susceptible to developing symptoms than others. The individual differences in the ability to adjust to rapid shifts in time zones may be related to endogenous circadian period whereby individuals with longer circadian periods (who tend to be late chronotypes) adapt better to westward travel, and those with shorter circadian periods (who tend to be early chronotypes) adapt better to eastward travel (12).
It may be possible to preadjust for destination schedule by changing the origin sleep time in the proper direction a few days prior to travel. This change may reduce the adaptation period at the destination (06; 13); however, this may not always be practical.
In-transit sleep may be beneficial if it coincides with the home schedule, provided circadian readjustment is not needed. If circadian adjustment is required, sleep should be avoided unless it coincides with the destination schedule. For short stays (2 to 3 days) in the new time zone, retaining the home sleep-wake schedule may be beneficial in preventing jet lag symptoms during the layover, if practical (29). During the first few days in the new time zone, peak alertness periods of the domestic and the new zones may overlap; thus, it may be possible to schedule an important event at a time that coincides with this alertness window. If attempting to adjust to the new time zone, long naps should be avoided at the destination for they might anchor the circadian rhythms to the home time. Brief naps in anticipation of an important event at an inconvenient circadian time may improve alertness and performance.
For patients who present with symptoms consistent with jet lag disorder in the context of recent transmeridian travel who have no prior history of sleep disturbances, jet lag is the most likely diagnosis. Travel fatigue secondary to poor sleep, dehydration, and dietary modifications secondary to the travel experience should also be considered. Nonetheless, a thorough history and physical examination should be performed to exclude other underlying medical conditions or sleep disorders. It is important to be suspicious of an independent sleep disorder if symptoms persist beyond 2 weeks while the patient remains in the same time zone.
Jet lag disorder is a clinical diagnosis. Objective laboratory testing such as actigraphy, polysomnography, or measurement of circadian phase markers are not routinely indicated (01).
There are several questionnaires available for evaluation of jet lag disorder and its symptoms, including the Stanford Sleepiness Scale (17), Columbia Jet Lag Scale (48), the Liverpool Jet Lag Questionnaire, and the Charite Jet Lag Scale (03). The Columbia Jet Lag Scale is currently the only questionnaire that has been validated to assess the presence and severity of jet lag (46). These questionnaires are not often used or required in the clinical setting. However, they play a crucial role in research studies to help establish a more uniformed interview method for the diagnosis of jet lag and symptom monitoring.
Jet lag disorder symptoms are generally self-limited. However, as any traveler can testify, travel time is valuable; therefore, treatment, if both safe and effective, is justified.
When the expected length of stay at a destination is brief (2 days or less), management is aimed at alleviating jet lag symptoms rather than phase shifting circadian rhythms. American Academy of Sleep Medicine practice parameters recommend maintaining home-based sleep hours for brief travel rather than adopting the destination sleep schedule whenever practical (33).
Treatment strategies aimed at alleviating symptoms of jet lag include agents that promote sleep, medications that promote wakefulness, and circadian phase shifting techniques. Currently, there are no U.S. Food and Drug Administration approved pharmacologic agents specifically for the treatment of jet lag disorder.
With all of these treatment strategies, there is evidence from field and lab-based studies that beginning phase shifting efforts (advancing or delaying) prior to travel can hasten adjustment to the new time zone; however, practically, this is not always possible (11; 13).
Medications that promote sleep. Zolpidem taken before bedtime on the first few nights after travel may be helpful by improving sleep quality and duration (49) but not other components of jet lag disorder (16). American Academy of Sleep Medicine practice parameters recommend the use of a benzodiazepine receptor agonist for the short-term treatment of jet lag-induced insomnia; however, the potential adverse effects, such as complex behaviors, headache, dizziness, and morning drowsiness, and the possibility of rebound insomnia after discontinuation of hypnotics should be considered (33).
Agents that promote wakefulness. Armodafinil is a central nervous system stimulant used to improve wakefulness in patients with excessive daytime sleepiness in obstructive sleep apnea, shift-work sleep disorder, and narcolepsy. It is the longer-acting R-enantiomer of modafinil. In a double-blind, randomized, placebo-controlled study, armodafinil at 150 mg was found to improve subjective alertness and other jet lag symptoms (43). Of note, armodafinil is not currently FDA approved for use in jet lag disorder.
Caffeine is a common agent used to counteract sleepiness. In a systematic review of 13 randomized trials evaluating patients with jet lag or shift-work sleep disorder, caffeine was found to improve attention, memory, orientation, and perception compared with placebo (21). However, the dose and timing of caffeine must be controlled in order to avoid disrupting nocturnal sleep.
Amphetamines are not currently recommended due to their well-known side effects, including hypertension, arrhythmias, and addiction potential.
Circadian phase resetting. Some symptoms of jet lag disorder can last for several days after a flight due to the slow adjustment process of the circadian system. Times average from 60 minutes of phase adjustment per day after a phase advancing shift (eastward travel) and 90 minutes per day after a phase delaying shift (westward travel) (05). A combination of timed melatonin and light therapy can be useful in mitigating the effects of jet lag disorder (34). The objective is to improve sleep quality and daytime alertness by realigning the endogenous circadian rhythm with the required sleep and wake times of the destination’s time zone.
Melatonin. Melatonin can be beneficial for the treatment of jet lag disorder both due to its phase shifting and soporific effects. For that reason, melatonin has been more frequently studied in eastward travel, where it can be taken near bedtime in the new time zone in order to facilitate a circadian phase advance and provide a mild hypnotic effect. Based on available data, current dose recommendations are 0.5 to 5 mg (33). The use of the prescription melatonin agonist tasimelteon during simulated eastward travel resulted in improved total sleep time and daytime sleepiness; however, tasimelteon is not currently FDA approved for use in jet lag disorder (37).
Timed light exposure. The solar light-dark cycle is the primary environmental time cue for synchronizing the circadian rhythm. Bright light exposure results in suppression of melatonin secretion by the pineal gland as well as phase shifting effects. Natural light exposure is the ideal mechanism for counteracting jet lag symptoms. Strategic light exposure and avoidance has been found effective in minimizing jet lag symptoms. Optimal timing and avoidance of light is dependent on the direction of travel and the number of time zones crossed (23).
Bright light exposure has phase shifting effects with phase delay or advance following early morning or late evening exposure, respectively, according to the phase-response curve (08). Individuals flying eastward, for example, are advised to avoid bright light in the early morning while exposing themselves to bright light in the early afternoon. This strategy is aimed at advancing the circadian rhythm. In contrast, when flying westbound, individuals are advised to maximize their light exposure in the afternoon and early evening to delay circadian timing.
If natural sunlight is not available, artificial bright light that simulates sunlight is an option. Various modalities include lamps, light boxes, and light visors.
Meal timing. There are a handful of studies looking at the role of dietary modification in adapting to jet lag. The Argonne Anti Jet Lag diet focuses on an alternating schedule of feast and fast days prior to travel, with carefully timed protein and carbohydrate intake (42). Although the 95 subjects who participated in the study reported subjective improvement, the study was not blinded and can be complicated to follow. As such, general recommendations at this stage are to focus on adjusting the eating schedule to the new time zone on arrival to help speed the entrainment of peripheral clocks.
Successful treatment results in more rapid adjustment of the sleep-wake schedule and other rhythms to the new time zone.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Phyllis C Zee MD PhD
Dr. Zee of Northwestern University Feinberg School of Medicine received consulting fees from Eisai and Jazz and a research grant from Vanda.
See ProfileSabra M Abbott MD PhD
Dr. Abbott of Northwestern University Medical School has no relevant financial relationships to disclose.
See Profile
Bradley V Vaughn MD
Dr. Vaughn of UNC Hospital Chapel Hill and University of North Carolina School of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Sleep Disorders
Jan. 18, 2025
Sleep Disorders
Dec. 03, 2024
Sleep Disorders
Dec. 01, 2024
General Neurology
Nov. 09, 2024
Sleep Disorders
Nov. 04, 2024
Sleep Disorders
Oct. 27, 2024
Sleep Disorders
Oct. 14, 2024
Sleep Disorders
Oct. 14, 2024