



Peripheral Neuropathies
Neuropathic pain: treatment
Jan. 19, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Lumbar disc disease is considered a very important cause of lower back pain. In lumbar disc disease, back pain occurs due to a complex of factors in association with disc narrowing. Sciatica is radiating pain along the path of the sciatic nerve and is usually caused by disc herniation, leading to inflammation of a displaced nerve root, but it may also occur in other conditions, such as metastasis. A herniated disc fragment is, in fact, a protrusion of the nucleus pulposus of the disc through the annulus fibrosus. A herniated disc, in severe cases, can produce dysfunction of the nerve. A meta-analysis indicated that genetic factors play a role in the pathogenesis of degenerative lumbar disc disease. A prior lumbar puncture is also associated with enhanced risk of degenerative disc disease. MR is the imaging method of choice for lumbar disc disease because of its multiplanar imaging capability, excellent resolution, and absence of hazardous radiation. CT remains an efficient and accurate method of evaluating the spine. MRI often reveals herniated discs in asymptomatic subjects as well. The prevalence of herniated discs increases with increasing age (peak is between 35 and 55 years). Medical management includes bed rest, analgesics, and muscle relaxants. Bed rest is a widely advocated measure in treating lumbar disc disease, but its effectiveness remains unconfirmed. Corticosteroids are used, either orally or injected into the epidural space or near a spinal nerve, to get relief from pain. A study found condoliase, a chemonucleolytic agent, safely and effectively treated lumbar disc herniation, reducing leg pain and disability with minimal side effects. Lumbar surgery is indicated when the patient either has cauda equina syndrome, progressive loss of motor strength, or severe intractable pain. One trial noted that potentially harmless stretch- and strength-based yoga exercises could provide significant relief in neuropathic pain due to lumbar disc herniation. Lumbar total disc replacement is an effective treatment option for symptomatic single-level lower lumbar discopathy. Minimally invasive discectomy is also increasingly being performed as the preferred surgical option for lumbar disc disease. Studies highlighting the role of artificial intelligence in improving the diagnosis and treatment of lumbar disk disease show promising results in accuracy and risk prediction. In this article, the author discusses these controversies and reviews the latest information on epidemiology, pathophysiology, diagnostic studies, and management.
|
• Lumbar disc disease is a frequent cause of lower back pain. | |
|
• Back pain occurs due to a complex of factors associated with disc narrowing. | |
|
• Sciatica is caused by disc herniation, leading to inflammation of a displaced nerve root, but may also occur in other conditions, such as metastasis. | |
|
• A herniated disc is a protrusion of the nucleus pulposus of the disc through the annulus fibrosus. | |
|
• MR is the imaging method of choice for lumbar disc disease. | |
|
• Medical management includes bed rest, analgesics, and muscle relaxants. | |
|
• Surgical treatment of symptomatic lumbar disc disease is controversial. | |
|
• Definite indications of surgery include cauda equina syndrome, progressive motor loss, and intractable pain. | |
|
• Treatment failures are common. |
Egyptian, Greek, Roman, and Arabic textbooks mention sciatica pain considered to be often originating from the hip joint. Descriptions of lumbago and sciatica are available in many ancient books like the Bible and the writings of Hippocrates (460-370 BC) (07). Laminectomy was performed for the first time in 1829, by Smith AG. Mixter and Barr published their original report of lumbar disc herniation in the New England Journal of Medicine as the cause of backache and leg pain (61). The introduction of MRI in the 1980s contributed tremendously in the understanding of lumbar disc disease.
Clinical terms in common usage are not uniformly defined, and they refer only to the radiologic or pathologic description and do not imply specific disease entities. A disc bulge indicates a nonfocal contour abnormality beyond the normal margins of the intervertebral space. A disc protrusion is a focal contour abnormality where disc material is contained behind an intact annulus. Disc extrusion refers to an extension of nuclear material through the annulus (disc rupture or herniation). The extent of disc extrusion may relate to the symptomatic potential of the disc: an intact annulus limits an associated inflammatory reaction, whereas an intact posterior longitudinal ligament limits the anatomic extent of herniation (38). Finally, a sequestered disc refers to disc material that is free in the epidural space, having lost contact with its parent disc.
Lumbar disc disease may represent either an important cause of pain and dysfunction or an entirely incidental neuroimaging finding without associated symptoms. Symptoms can range from low back pain to locally referred pain in the buttocks or hips, radicular pain in the legs (with or without leg weakness or numbness), or a cauda equina syndrome. The clinical onset is usually spontaneous, without any apparent precipitant. Onset can also be associated with heavy lifting, trauma, running, coughing, or sneezing.
A complaint of “sciatica” is nonspecific and must be analyzed carefully. We suggest the following working definition: electric-like or stabbing pain that radiates from the lower back or buttock into the posterolateral thigh or leg. Pain associated with nerve root pathology may possess stabbing, shooting, burning, or radiating features. When sciatica is related to nerve root impingement, position changes such as twisting or sitting in low chairs often exacerbate pain symptoms. Activities that cause a transient increase in the pressure gradient across the dura (coughing, straining at stool, or sneezing) may worsen pain. Leaning to one side or the other may lessen the pain. Uncommonly, symptomatic lumbar disc disease may be painless and only associated with numbness, tingling, or weakness. Gait may be limited due to pain or muscle weakness.
No findings on physical examination have proven to be sensitive and specific (87). Nerve root tension signs like straight leg raise (also known as the Lasègue sign) and reverse straight leg raise tests are commonly thought to be the most helpful in diagnosis. To perform a straight leg raise test, extend the patient’s leg fully at the hip (with knee extended) while the patient is not contracting any leg muscles and is seated or supine. In this test, manual stretch of the sciatic nerve secondarily pulls on the irritated nerve roots. The maneuver is considered positive if patient experiences pain along the distribution of the lumbar roots. This sign may be more specific for L5-S1 root or sciatic nerve involvement, although this tenet has been disputed (23; 88). Some data have suggested that the most specific sign is when straight leg raising of the unaffected leg (crossed, straight leg raise) also reproduces symptoms in the affected leg, but this finding is not as sensitive (23). The reverse straight leg raise checks for L2-4 nerve root or femoral nerve involvement. The patient lies prone or stands by the examination table, and the examiner extends the leg posteriorly at the hip while the patient supports his or her weight on the opposite leg.
A positive straight leg raise or reverse straight leg raise does not exclude the possibility of hip or sacroiliac disease. Physical exam maneuvers that raise clinical suspicion for hip or sacroiliac disease are Patrick’s sign and heel percussion. In the former, hip or buttock pain is elicited by internal rotation of the hip with the knee in flexion. In the latter, hip or buttock pain is elicited by percussing the heel while the leg is fully extended.
When radiculopathy is present, the pattern of neurologic deficit aids in identifying the affected root. In the setting of pain, asymmetric reflexes are often the most objective findings. Despite common lore to the contrary, L5 root impingement can occasionally depress the ankle reflex. Isolated L5 involvement, however, should not abolish the ankle reflex. In chronic processes, muscle atrophy or fasciculations may develop. Weakness may increase the specificity of diagnosis but add little to sensitivity (87). A finger-floor distance, defined as the distance between the fingertips and the floor while bent at the hips in anterior flexion, of greater than 25 cm has been used by some authors to predict nerve root compression (88). Sensation is best tested in proximal and distal portions of dermatomal regions, but a normal sensory exam does not exclude nerve root pathology. Importantly, these neurologic findings are not specific to discogenic disease and may be present with any pathological condition affecting the same nerve roots (23). Lower lumbar pathology should not be associated with signs of sympathetic dysfunction nor myelopathy because the cord typically terminates the L1-2 vertebral level. The risk of foot drop is increased if a patient is a diabetic, if there is an acute episode, lateral recess, or foraminal type of herniation, or if there is disc calcification, canal occupancy greater than 50%, and 1.0 mm increase in anteroposterior diameter of the canal (57).
Infrequently, patients with lumbar disc can present with bilateral foot drop or cauda-equina syndrome. Cauda equina syndrome is a neurosurgical emergency. The cauda-equina syndrome is clinically characterized by lower motor neuron paraparesis, bowel or bladder incontinence, sexual dysfunction, and saddle-shaped sensory loss. Lumbar disease extends from L2/3 to L5/S1. The prognosis is good if patients are urgently treated (72; 18).
By contrast, neurogenic claudication secondary to lumbar canal stenosis is a chronic, slowly progressive condition that has an excellent surgical prognosis. Temporary nerve root ischemia is induced by positional changes that reduce the diameter of an already small lumbar canal. In normal individuals, standing and walking cause extension of the lumbar spine and result in a decrease of the lumbar canal diameter; sitting and bending forward cause flexion of the lumbar spine and increase canal diameter. Walking increases the energy demands placed on the lumbar nerve roots but does not result in nerve root ischemia. In the setting of an abnormally narrowed lumbar spinal canal, however, the combination of compressed nerve roots and increased energy demand during walking does result in lumbar nerve root ischemia. Thus, these patients typically present with ambulation-induced pain in the calves that resolves nearly immediately with sitting down or leaning forward. The most classic portrayal is the person whose symptoms improve with leaning forward on the grocery cart while shopping.
Panneerselvam and colleagues assessed the effects of lumbar disc herniation on male sexual activity and the impact of surgical intervention on sexual dysfunction (69). Lumbar disc herniation adversely affected sexual function in up to 77% of patients. Surgery helped to improve sexual function, and by 6 weeks, the majority had resumed sexual activity.
The majority of patients with acute low back pain, including those with uncomplicated discogenic disease, have a good prognosis. With conservative measures, most experience marked improvement of symptoms and return of function within days to weeks. MRI findings may also significantly improve with time in up to 88% of patients (80). Further morphologic changes may occur for over 2 years following symptom onset (60).
Lumbar disc disease and knee osteoarthritis are both age-related disorders and can exist together. Lumbar disc disease and knee osteoarthritis together are correlated with increased pain and dysfunction of the lower extremities. Patients with lumbar disc disease with knee osteoarthritis experience difficulty in daily activities due to knee pain even after lumbar spinal surgery. Hence, preoperative assessment for knee osteoarthritis is crucial while planning for lumbar spinal surgery (68).
An assessment of the readmission rate among 2635 surgically operated patients revealed that higher age, smokers, prolonged postoperative hospital stay, and renal failure independently predicted the possibility of readmission or a complication after lumbar decompression (11). Drop foot is a common disabling complication of lumbar disc disease. Even after decompressive surgery, foot drop does not recover most (82).
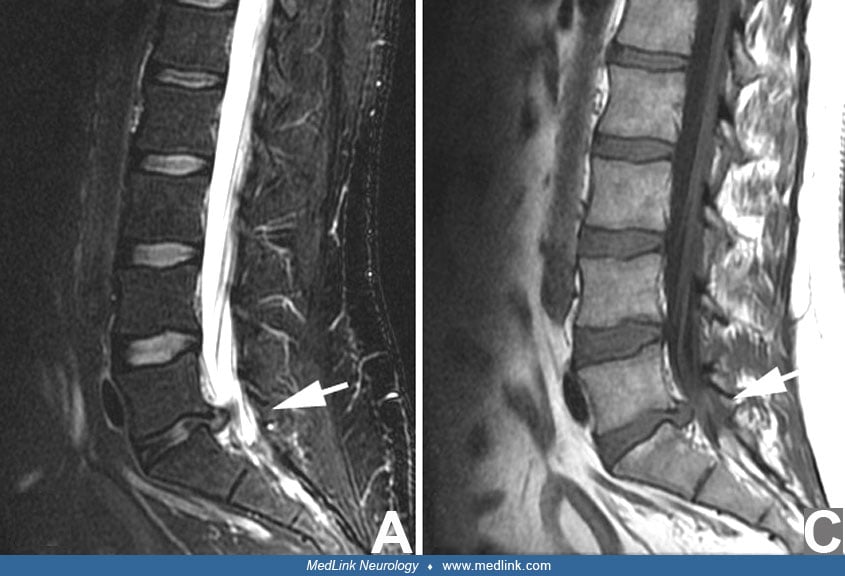
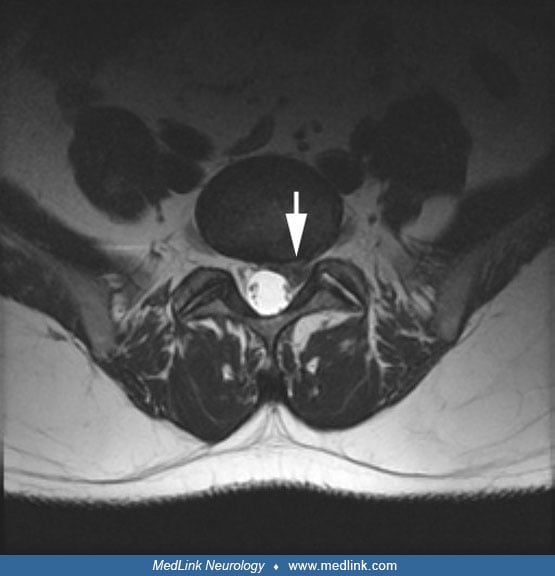
A 32-year-old female physician had a sudden onset of lancinating left leg pain. She had no recent trauma, although she had been frequently lifting her 1-year-old twins. The pain began in the buttock and traveled down to the left lateral thigh and calf. The pain was exacerbated by coughing and improved by lying supine. There was no weakness, numbness, saddle anesthesia, or incontinence. The pain progressed over the the next days to weeks. On exam, she had breakaway weakness of her left leg, a depressed left ankle jerk, and mild numbness of the lateral left calf extending to the dorsum of her foot. A lumbar MRI showed a left-sided, large L4/5 disc protrusion compressing the left L5 root in the lateral recess. Given her symptoms, neurologic examination, and imaging, she was offered surgical L5 decompression. However, she elected to pursue conservative management with nonsteroidal anti-inflammatory drugs. Over the next several months, her pain gradually subsided. A repeat lumbar MRI 6 months later showed a decreased size of the L4/5 disc protrusion.
The effects of mechanical stress and load bearing accelerate age-related degenerative change in the disc. Frank herniation of the disc may ultimately be associated with involvement of the nerve roots.
The intervertebral discs are thickest in the lumbar region, reflecting their dual purpose of supporting the upper body and providing flexibility. Lumbar movements are mainly flexion and extension, with a lesser degree of rotation and lateral flexion. The anatomic elements of these large-scale actions are both active (paraspinal muscles) and passive (vertebrae, ligaments, and intervertebral facet joints). Motion segments (ie, functional units) are made up of two adjacent vertebrae, paired facet joints, and an intervening disc. Layers of hyaline cartilage separate the disc from direct contact with the bony vertebral bodies. This entire structure can be thought of as an individual intervertebral joint or symphysis.
Each disc has two distinct parts: the outer annulus fibrosus and the inner nucleus pulposus. The gel-like inner nucleus is rich in proteoglycans and functions as a resilient shock absorber. The nucleus pulposus is contained and anchored by the outer, tough, and collagenous annulus. Alternating oblique layers of fibrous tissue give the annulus its tensile strength. The annulus is bonded to the vertebral epiphyses and is also supported by the anterior and posterior longitudinal ligaments. Two facts may contribute to the frequency of posterolateral disc herniation: (1) the layers of the annulus are incomplete posteriorly, and (2) the posterior longitudinal ligament does not extend completely to the posterolateral aspects of the disc.
Disc physiology is unique. There is only nerve and blood supply to the outer annulus. The inner annulus and the nucleus pulposus receive nutrients and metabolic products via diffusion from nearby blood vessels. As a result, two opposing processes passively determine the disc’s state of hydration. The mechanical compression of the disc generates hydrostatic pressure, forcing water outward. The macromolecules within the nucleus generate colloidal pressure, encouraging water to move into the disc.
Children rarely have discogenic disease unrelated to trauma. From the second decade onward, disc degeneration becomes increasingly common. In the aging process, the lumbar disc nucleus desiccates and hardens. The degree and pattern of disc degeneration varies between individuals, and asymptomatic or subclinical disease is common.
At birth, the disc is small in proportion to the vertebral bodies, and the nucleus pulposus occupies half the total disc volume. Beginning in the second decade, disc growth exceeds the vascular supply; the latter ultimately supplies only the outer annular layers. The nucleus loses notochordal cells, fibrocartilaginous tissue invades from the annulus, water content decreases, and there is loss of proteoglycan aggregation. In middle age, the annulus undergoes myxomatous degeneration and develops fissures. In the elderly, the disc is a thinned plate of fibrocartilage. These ongoing structural changes stem from a combination of the declining blood supply to the disc and the decreasing diffusion capacity of the matrix, resulting in an unfavorable environment for cell growth. A pathophysiologic model that attributed the reduced blood supply associated with aging to atherosclerosis of the local lumbosacral arteries has sparked an ongoing series of pathological and clinical studies (44; 43; 54).
Although the processes responsible for disc degeneration are clear, the precise source of disc-related pain is often enigmatic. Historically, it was understood that there was no direct nerve supply to the disc and no anatomical basis for local disc pain. It is now clear that nerve twigs found in the outer third of the annulus could act as pain generators (09). The sinuvertebral nerves originate from the sympathetic chain or mixed spinal nerves and enter the spinal canal through the intervertebral foramina. These sensory nerves innervate many spinal canal structures that are pain-sensitive, including the ventral dural sac, the posterior longitudinal ligament, and the posterior annulus fibrosus. The sinuvertebral nerves at each segmental level vary in number (2 to 6) and derivation. Considerable vertical overlap and variability exists in the area supplied by individual sinuvertebral nerves. A nerve at one segmental level does not provide exclusive supply to the disc at that level and may even supply contralateral intraspinal structures. This complexity helps explain why the location and extent of back pain may be an imprecise indicator of the level of disc pathology.
Most lumbar disc pathology involves the L4-L5 and L5-S1 interspaces. Disc abnormalities at L1-L2, L2-L3, and L3-L4 account for less than 5% of the total. Lumbar disc protrusions are most often posterolateral and affect either descending or exiting nerve roots. At a given lumbar disc level, a posterolateral disc protrusion passes underneath the root exiting at the same interspace and abuts the root exiting the segment immediately below as it travels to its foramen. Thus, an L4-L5 posterolateral disc protrusion typically compromises the L5 root and leaves the L4 root unaffected. Similarly, an L5-S1 posterolateral disc protrusion usually impinges on the S1 root. However, a nerve root can be compromised anatomically at any point along its intraspinal course (approximately 6 inches for the S1 root), even though locations other than that described above are less common. For example, a far lateral disc protrusion may actually compress the exiting nerve root at that level.
The clinically observed discrepancy between anatomical displacement of disc material and the resulting neurologic symptoms suggests that the underlying mechanism is not simply one of physical nerve root compression. The mobility of nerve roots – as demonstrated on MRI where they readily gravitate to the posterior aspect of the spinal canal – and gelatinous substance of the herniated nucleus make pure compression an unsatisfying or incomplete explanation. As demonstrated in animal models, sudden exposure of the nucleus pulposus to the immune system via herniation results in an inflammatory response that secondarily involves the nerve roots over the course of several days. One novel study even found that exposure of the dorsal root ganglion to nucleus pulposus material induced cell apoptosis within 24 hours of exposure (64). Such an inflammatory component of disc herniation may partially explain why a course of steroids is sometimes helpful in treating pain associated with acute disc herniation.
Genetic factor. A meta-analysis indicated that genetic factors play a role in the pathogenesis of degenerative lumbar disc disease. Castillo-Avila and colleagues noted FokI polymorphism is significantly associated with lumbar disc disease and disc herniation (14).
Prior lumbar puncture. A prior lumbar puncture is also associated with enhanced risk of degenerative disc disease. In a population-based study, Moinuddin and colleagues analyzed 950 cases who underwent lumbar puncture and 1876 subjects who did not undergo a lumbar puncture (62). The risk of developing degenerative disc disease from the time of lumbar puncture was 13.8% versus 9.4% among controls at 5 years.
The epidemiology of lumbar disc disease is poorly defined. Approximately 70% to 80% of the adult population will have a functionally significant episode of low back pain over a lifetime. Analysis of United States national survey data showed that one fourth of adults report low back pain in the past 3 months and that the annual proportion of all physician visits attributable to low back pain was 2.3% for the year of the survey (22). Prospective cohort data revealed an 18.6% annual incidence of low back pain; the overwhelming majority (92%) of these cases were of mild severity (13).
In Finland, a total of 65,912 lumbar discectomy operations were performed between 1997 and 2018 (71). In 1997, the annual discectomy rate was 83 per 100,000 person-years, and in 2018, it came down to 58 per 100,000 person-years. However, the incidence of microdiscectomy increased during this period from 41 per 100,000 person-years in 1997 to 47 per 100,000 person-years in 2018. The incidence of open discectomy decreased 71%, from 41 per 100,000 person-years in 1997 to 12 per 100,000 person-years in 2018 (71).
The peak prevalence of low back pain is between ages 35 and 55, and women and men are equally affected. Risk factors for an episode of low back pain include occupational lifting, exposure to industrial sources of vibration, cigarette smoking, osteoporosis, arthritis, and possibly genetic predisposition. Studies demonstrate the importance of psychosocial risk factors such as job stress, work satisfaction, and depression (17). Controversy exists over which patient-related factors increase the risk of transformation to chronic low back pain, but data concluded that intense pain persisting beyond 8 weeks was more highly correlated than psychosocial factors (37). Interestingly, the severity of low back pain and the attributed level of disability are often discrepant (81).
Only a subset of patients with low back pain will have discogenic disease, and the lifetime prevalence of a clinical herniated lumbar disc syndrome is estimated to be from 1% to 3%. Epidemiological data are complicated by the lack of direct correspondence between radiological or surgical findings and the nonspecific symptomatology.
There is a high prevalence of long-term bowel, bladder, and sexual dysfunction post-cauda equina syndrome, with functional and psychosocial consequences. Our results demonstrate the need for preoperative information and subsequent screening, and long-term multidisciplinary support for these complications (51).
There are few prospective data on the prevention of lumbar disc disease. However, mechanical stress can give rise to low back symptoms and may contribute to disc degeneration. Employees and the general public should be made aware of preventive measures. Simple advice may include flexing at the knees rather than stooping to lift or ensuring regular postural change when sitting at a keyboard or assembly line. There is inconclusive evidence for the efficacy of structured educational programs (back school), lumbar support devices, and exercise in preventing lumbar disc disease (86; 84; 39).
The features of low backache, referred pain to the legs or buttocks, and radicular-type pain seen in lumbar disc disease are not specific. Rather, they are common to many other conditions (31). The large differential diagnosis encompasses diverse pathologies involving the nerve roots, meninges, spine, paraspinal muscles, and viscera.
|
Degenerative |
• Discogenic disease |
|
Neoplastic |
• Primary |
|
Inflammatory |
• Arachnoiditis |
|
Metabolic |
• Osteoporosis |
|
Traumatic |
• Vertebral fractures |
|
Congenital |
• Spondylolysis |
|
Referred pain |
• Viscera (intra-abdominal or intra-pelvic) |
|
Psychogenic |
A primary objective of the diagnostic workup is to identify sinister causes of low back pain. The clinician should be alerted by historical and examination risk factors for serious disease (Table 2), and further investigation should be directed by the clinical scenario. The investigations of most use in the specific setting of lumbar disc disease are radiographic imaging and electromyography.
|
On history: | |
|
• Fever, chills, or weight loss | |
|
On examination: | |
|
• Unexplained fever | |
In general, radiological investigation is overused in the clinical setting of acute low back pain. Neuroimaging usually is needed only when there is no relief from the pain within 4 to 6 weeks of medical treatment, and the patient is considered a potential candidate for lumbar epidural steroid injections or surgery (21).
Spine imaging can identify the level of a diseased disc and define its relation to the lumbosacral roots. Plain radiographs of the lumbar spine are not of direct use in diagnosing disc disease but are indicated for suspected fracture, vertebral column instability, neoplasm, or spine infection among patients at risk. CT imaging of the spine to evaluate patients with low back pain may be helpful for patients who cannot undergo an MRI. The resolution is less optimal than MRI but can identify degenerative disc and facet disease. CT myelography and MRI produce highly detailed and comparably accurate images of the lumbar spine and are the anatomic investigations of choice for diagnosing of disc disease (40; 41). MRI can image surrounding soft tissues and is not subject to bony artifact.
MRI may demonstrate a reduced signal intensity of degenerating discs, annular fissures and tears, integrity of the posterior longitudinal ligament, and enhancement of compromised (and presumably pain-generating) roots. Routine MR myelography has been shown to be of limited diagnostic value (66). Positional MR imaging has yet to convincingly show additive diagnostic power; importantly, the definition of normal parameters is lacking (91). The role of conventional myelography is limited, but it may add important information in lateral recess nerve root impingement (04). The utility of discography and other invasive testing is controversial (74; 73).
MRI often reveals herniated discs in asymptomatic subjects. The prevalence of herniated discs increases with advancing age (21). MRI of asymptomatic young adults will show a significantly abnormal disc in approximately one of four cases (08). A Danish cross-sectional cohort of 40-year-olds with and without low back pain found a point-prevalence of disc bulges in 28% and, more significantly, abnormal disc contour in 25% (46). Another study of 148 asymptomatic patients at a Veteran’s Affairs Medical Center found that baseline MRIs had abnormal disc findings of protrusion in 33%, bulge in 44%, extrusion in 6%, and annular tear in 38% (42). Further, an exact match between clinical exam localization and MRI findings in patients with lumbosacral radicular syndromes was shown in less than one third of subjects (85). Similarly, a prospective study of 200 subjects free of low back pain at baseline that compared baseline MRIs with those obtained at the time of clinical events of acute low back pain found that 84% of subjects had improved-to-unchanged imaging findings (12). A congenital laminae defect of L5 may be a potential risk factor leading to lower lumbar disc herniation in the young (83).
A meta-analysis revealed that MRI evidence of disc bulge, degeneration, extrusion, protrusion, Modic 1 changes, and spondylolysis were more frequent in adults 50 years of age or younger with back pain compared with asymptomatic persons (10). Modic changes are characterized by changes in vertebral bone marrow signal intensity on MRI.
Electromyography, nerve conduction studies, and F waves are of limited value in diagnosing lumbar disc disease. An H reflex is a better method for diagnosing an S1 radiculopathy, although this is not specific lumbar disc herniation (48). A prospective study evaluated the clinical and electrophysiological findings in patients with lumbosacral radiculopathy due to herniated disc. One hundred and eight patients with L4, L5, or S1 radiculopathy were enrolled. Sensory loss in the painful dermatome was the most frequent finding at physical examination (56% of cases). EMG was abnormal in at least one muscle supplied by femoral and sciatic nerves in 45 cases (42%). The most frequent motor nerve conduction abnormalities were a delay of F-wave minimum latency and decreased compound muscle action potential amplitude from extensor digitorum brevis and abductor hallucis in L5 and S1 radiculopathies, respectively. Sensory nerve conduction findings were usually normal, the amplitude of sensory nerve action potential was infrequently reduced (63). Absolute correlation between neuroimaging and electromyographic evaluation for localization is seen in approximately three fourths of patients (26). Fifteen percent to 18% of patients with normal physical exams will demonstrate relevant and subclinical electrophysiological abnormalities (52).
In the context of possible radiculopathy, electrophysiological studies can help decide the following issues:
|
(1) Is an imaging abnormality functionally relevant to focal motor or sensory symptoms and signs? | |
|
(2) Is the source of pathology actually a lumbosacral radiculopathy, or is it instead due to anterior horn cell, plexus, or distal peripheral nerve involvement? | |
|
(3) How severe is the motor deficit? EMG allows quantitative grading of the current deficit, and progression can be accurately charted over time. | |
|
(4) Are the motor findings on examination attributable to breakaway weakness associated with pain during movement, a central nervous system cause of weakness, or limited motor effort? | |
|
(5) In a patient with negative imaging, is there objective and functional evidence for true, underlying radicular pathology? |
Importantly, root lesions are proximal to the dorsal root ganglion, leaving the sensory nerve intact between the dorsal root ganglion and the nerve’s target. Thus, sensory nerve action potentials are nearly always normal in pure root lesions – even in the setting of complete dermatomal sensory loss, whereas pathology distal to the dorsal root ganglion will reduce the sensory nerve action potentials. Nerve root compression may also result in findings of axonal loss or focal demyelination. Motor nerve conduction studies are often normal in the absence of severe or multisegmental motor root involvement.
The classic finding of a myotomal pattern of axonal denervation or reinnervation on needle EMG remains the most sensitive electrophysiological sign of radiculopathy (02). However, a myotome is commonly affected incompletely. As a result, several muscles sharing the same root but supplied by different peripheral nerves should be evaluated for evidence of partial reinnervation. Abnormal spontaneous EMG activity (ie, fibrillations and positive sharp waves) does not develop in an acutely denervated distal muscle until approximately 3 to 5 weeks following axonal injury. Reinnervation begins after approximately 12 to 16 weeks; it is marked by the development of long-duration motor unit potentials and a decrease in abnormal spontaneous activity. Evaluation of paraspinal muscles can be important in distinguishing radiculopathy from plexopathy and in diagnosing very recent nerve root injury. These very proximal muscles are the first to reveal evidence of acute denervation (approximately 7 to 10 days following an injury) and are the first to normalize.
For patients who present with acute low back pain (duration less than 12 weeks), the emphasis of the initial assessment is on the exclusion of sinister etiologies. Neoplastic, infective, and traumatic etiologies are particularly important to identify. The remaining group of patients (including most cases of lumbar disc disease) has a favorable prognosis. Conservative measures, without further investigation, represent the most appropriate initial management. If there is no improvement and the pain becomes chronic, additional investigation is indicated.
Chronic low back pain (duration greater than 12 weeks) represents a distinct clinical entity separate from acute low back pain. The causes of chronic low back pain are heterogeneous, making it difficult to formulate global management algorithms. A comprehensive attempt to formulate protocols for the management of acute low back pain was published by the Agency for Health Care Policy and Research in 1994. Abbreviated versions of these algorithms are available from several sources (27).
Most acute lumbar disc herniations tend to improve over time with or even without treatment. In 1986, Deyo and colleagues failed to demonstrate a benefit from bed rest longer than 2 days (19) for acute back pain. A systematic review of bed rest and acute low back pain also suggested no beneficial effect and possibly some harmful effects (36). Another systematic review showed that simple advice to stay active effectively promoted the recovery of patients with acute low back pain (55). Several nonpharmaceutical, noninvasive treatments are used to enhance recovery. Physical therapy will often assist patients in the functional adaptation to a neurologic deficit or pain, but an objective benefit to final outcome is difficult to demonstrate. Traction has not been shown to be effective. Back school has been shown to be of moderate benefit in treating nonspecific low back pain (39).
A wide variety of symptomatic medications are used for low back pain. Simple analgesics and nonsteroidal anti-inflammatory agents constitute first-line treatment. Muscle relaxants can be useful in patients with associated paraspinal muscle spasm, particularly at night in patients kept awake by spasm. Chronic pain associated with psychological morbidity may respond to tricyclic antidepressants. Benzodiazepines should be avoided because of their potential for dependence. Unremitting, severe pain may be relieved by circumscribed courses of opiate analgesics; however, the efficacy of opiates in the treatment of chronic back pain has not been established, and substance use disorders are common (59). Injections of anesthetic agents or steroids may be useful for temporary relief or diagnostic purposes in selected patients with focal symptomatology related to a single segmental level, particularly in terms of short-term pain relief (03). Intradiscal administration of autologous platelet-rich plasma in patients with chronic lumbar discogenic pain has been shown to alleviate pain (56; 53).
Local inflammation has a role in the pathogenesis of disc disease and associated symptoms. Corticosteroids are used, either orally or injected into the epidural space or near a spinal nerve, to get relief from pain. In a randomized-controlled study, Goldberg and colleagues noted that a short course of oral steroids resulted in modestly improved function but no improvement in pain among patients with acute radiculopathy due to a herniated lumbar disc (33). There were no differences in surgery rates at 52-week follow-up. The efficacy of a single glucocorticoid intradiscal injection (during discography) was assessed in a randomized-controlled trial in patients with chronic low back pain with active discopathy. At one month, the percentage of responders was higher in the glucocorticoid intradiscal injection group (36 of 65) than the control group (21 of 63). The effect did not last long as the groups did not differ in chronic low back pain intensity at 12 months (65). In another study, the efficacy of interlaminar epidural steroid administration in patients with multilevel lumbar disc pathology was assessed. The visual analog scale and Oswestry Disability Index scoring posttreatment were higher in the group that received 10 mL 0.25% bupivacaine, compared with the group that received 10 mL 0.25% bupivacaine plus 40 mg methylprednisolone at L4 to L5 intervertebral space (67). Fang and colleagues demonstrated that the addition of corticosteroids to epidural injection of an anesthetic agent was associated with a better Oswestry Disability Index compared with local anesthetic alone (28). In lumbar disc disease, more studies are needed to prove the efficacy of corticosteroids.
Condoliase, also known as SI-6603, is a chemonucleolytic agent. It is an enzyme that breaks down glycosaminoglycans, which are a type of molecule found in the nucleus pulposus of intervertebral discs. A study suggested that condoliase may have provided a safe and effective treatment option for patients with lumbar disc herniation. The study found that participants who received a single injection of condoliase experienced significantly greater improvement in their worst leg pain at 13 weeks compared to those who received a sham injection. The average reduction in worst leg pain was 41.7 points in the condoliase group, compared to 34.2 points in the sham group. Although the difference in pain reduction between the two groups was not statistically significant at 52 weeks, the results still favored the condoliase group. Additionally, the condoliase group showed greater improvements in herniation volume and disability scores at all time points. The treatment was generally well-tolerated, with the most common side effects being spinal abnormalities and back pain (45).
Surgical intervention is mandatory and urgent in acute cauda equina syndrome. Decompressive surgery within 48 hours of the onset of symptoms results in a lower frequency of persistent bladder dysfunction (49). Surgery is also indicated when a chronic, objective motor deficit is worsening despite conservative management. Much debate exists regarding the efficacy of surgery for patients outside these circumscribed categories, and little prospective data help predict which patients are likely to be successfully treated. Carefully crafted prospective operative versus nonoperative studies continue to be hampered by design limitations such as patient crossover between the treatment groups and vague specification of nonoperative management (89; 90). Incapacitating pain alone in the setting of disc disease is controversial as an indication for surgery. Clearly, the number of lumbar fusion surgeries performed in the United States has disproportionately increased compared to other types of major surgery, and in the absence of definitive evidence for a change in efficacy (20). Lumbar total disc replacement is an effective treatment for symptomatic single-level lower lumbar discopathy (34; 30). Minimally invasive discectomy, like microendoscopic discectomy and percutaneous endoscopic discectomy, are now increasingly being performed as a preferred surgical option for lumbar disc disease. Minimally invasive discectomy minimizes muscle and soft tissue damage (01; 77).
A systematic review and meta-analysis were conducted to compare robot-assisted and freehand techniques in transforaminal lumbar interbody fusion surgery. The analysis included 21 studies with 539 participants. The results showed that robot-assisted surgery had higher accuracy in pedicle screw placement and reduced proximal facet joint violations compared to freehand surgery. Additionally, robot-assisted surgery was associated with reduced blood loss and radiation exposure. However, the duration of surgery was comparable between the two groups. The review suggests that robot-assisted technology can enhance precision in this type of surgery, but its integration into clinical practice may be limited by factors such as longer preoperative preparation time and the need for specialized training. Overall, the study provides evidence for the potential benefits of robot-assisted surgery in transforaminal lumbar interbody fusion (35).
Inversion therapy and acupuncture as alternative therapies are quite popular because of extensive advertisement by the media. A trial noted that potentially harmless stretch- and strength-based yoga exercises could provide significant relief in neuropathic pain due to lumbar disc herniation (95). Inversion therapy involves hanging upside down. It is supposed that a head-down position takes gravitational pressure off the nerve roots and discs in the spine and leads to the opening up of intervertebral foramen, straightening of the spinal curves, and stretching of the spinal musculature. No high-quality studies are available to substantiate the benefit of inversion therapy in lumbar disc disease. Acupuncture is becoming increasingly popular in the United States and other parts of world. Acupuncture is frequently used for pain relief caused by lumbar disc disease. A systematic review noted limited evidence for the effectiveness of acupuncture treatment for acute postoperative pain after back surgery (16). Ozone therapy, in many countries, is promoted as an alternative or additional treatment option for lumbar disc disease. In addition to a reduction in herniated disc volume and disc shrinkage, ozone therapy is considered to have anti-inflammatory and analgesic properties. A systematic review noted that ozone therapy appears to yield positive results when applied percutaneously for the treatment of chronic low back pain (58).
Preliminary studies have shown that local administration of autologous adipose-derived mesenchymal stem cells has shown promise in the treatment of lumbar disc disease. Autologous mesenchymal stem cells help regenerate intravertebral discs by restoring the extracellular matrix and restoring cellular function. Mesenchymal stem cells and their exosomes prevent further disc degeneration progression (92; 94).
Total disc replacement. Total disc replacement has emerged as an alternative in treating lumbar disk pain, addressing the limitations of traditional fusion or discectomy. Total disc replacement offers a potential solution by preserving spinal mobility and reducing reoperation rates (29).
Artificial intelligence in lumbar disk disease. Studies in lumbar disk disease management have utilized AI models to enhance diagnosis, treatment, and postoperative care. For example, Soin and colleagues utilized decision-tree algorithms to diagnose spinal pain and found an accuracy of 72% against practitioners' diagnoses (78). Bharadwaj and colleagues showed the promise of deep learning in classifying spinal conditions from MRI scans, with high accuracy in both segmentation and classification tasks (06). Kocaman and associates employed the XGBoost algorithm to predict lumbar disc herniation with high accuracy by analyzing MRI scans, highlighting the potential for AI to aid in early diagnosis (47). Shan and colleagues identified significant risk factors for reoperation in lumbar disc herniation patients, with XGBoost outperforming traditional logistic regression in predicting reoperation risk (76). Stroop and associates assessed ChatGPT's ability to provide medical information on lumbar disc herniation, finding it effective but not exhaustive, indicating a need for careful integration of large language models in clinical communication (79). Collectively, these studies underscore the evolving role of AI in improving the accuracy of diagnosis and the efficacy of treatments for lumbar disk disease, with an emphasis on the need for ongoing evaluation and refinement of these advanced technologies in clinical settings.
Deep learning models have demonstrated exceptional proficiency in analyzing MRI scans of the lumbar spine. These models have exhibited high precision in segmenting lumbar spine features, grading disc degeneration, and localizing abnormalities, thereby augmenting the diagnostic accuracy and reliability of clinical assessments. Furthermore, the automation of anatomical feature segmentation and reconstruction has significantly reduced the time and potential human error associated with manual methods, thereby streamlining the diagnostic process. In addition to their diagnostic applications, AI-based models have also been employed in clinical decision support systems, facilitating tasks such as predicting surgical outcomes, assessing disability, and detecting complications (05; 25; 75; 93).
Spontaneous regression of herniated disc tissue has frequently been noted. Herniated disc tissue can completely resolve following conservative treatment. In a systemic review, follow-up imaging found spontaneous regression in 96% of cases for disc sequestration, 70% for disc extrusion, 41% for disc protrusion, and 13% for disc bulging. The complete resolution rate of disc herniation was 43% for sequestrated discs and 15% for extruded discs (15).
Overall outcomes are similar for patients who are either treated with early surgery or conservative treatment (with eventual surgery if needed). Pain relief is faster for those who are subjected to early surgery (70). However, many patients experience little to no benefit from surgery. A nationwide, web-based, prospective, longitudinal 1-year outcomes registry in the United States enrolled 7951 patients with disc herniation, canal stenosis, lumbar spondylolisthesis, recurrent-disc herniation, and adjacent vertebral segment disease. Patients were followed up to 12 months after spine surgery. Only 65% of patients reported that outcomes met expectations, and 12% reported they would not undergo surgery again. Many patients experience little to no benefit from surgery. Smoking, depression, back dominant symptoms, a prior spine surgery, and symptom duration of more than 3 months were associated with unsatisfactory results when assessed 12 months after lumbar spine surgery (32).
Risk factors significantly related to recurrent lumbar disc herniation were smoking, disc protrusion, and diabetes.
Although low back pain is a common symptom in pregnancy, lumbar disc disease does not occur with greater frequency than in age-matched nonpregnant controls (50). MRI is preferable to CT as an imaging modality as there is no fetal exposure to ionizing radiation. The initial management of pregnant women affected by lumbar disc disease is conservative, and its primary aim is to manage the pain. In unresponsive patients with severe radicular pain and progressive neurologic symptoms, surgery should be considered. Laminectomy and microdiscectomy are most commonly used techniques that can be safely performed during pregnancy. Endoscopic discectomy may be an alternative (24). A coexisting disc is not regarded as a necessary indication for caesarian section.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Peter J Koehler MD PhD
Dr. Koehler of Maastricht University has no relevant financial relationships to disclose.
See Profile
Federica Provini MD
Dr. Provini of the University of Bologna and IRCCS Institute of Neurological Sciences of Bologna received speakers' fees from Idorsia, Italfarmaco, and NeoPharmed Gentili Spa.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Jan. 19, 2025
Peripheral Neuropathies
Jan. 19, 2025
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
Peripheral Neuropathies
Dec. 30, 2024
Peripheral Neuropathies
Dec. 30, 2024