

Peripheral Neuropathies
Polyneuropathy associated with anti-MAG IgM antibodies
Dec. 30, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
This article will highlight treatment strategies for the most common symptoms experienced by patients with multiple sclerosis. Neurologists often become the primary health care professionals for patients with multiple sclerosis. Therefore, it is incumbent on neurologists to not only be familiar with the management of disease-modifying therapies but also to be well versed at managing the symptoms that can accompany this diagnosis. Multiple sclerosis–related symptoms have a prominent role in daily functionality and quality of life; thus, knowledge about symptomatic management becomes critical. In this update, there is a focus on nonpharmacologic management of multiple symptoms, including cognition, sexual dysfunction, as well as gait disturbances, in those with higher disability scores.
References used in this review and in prior updates have been cited selectively.
|
• Patients with multiple sclerosis present with a wide variety of neurologic symptoms. | |
|
• The goal of individualized medicine is to treat each unique person in an individual way; this includes addressing symptoms in persons with multiple sclerosis that affect their quality of life. | |
|
• There are a wide variety of pharmacologic and non-pharmacologic therapies that may benefit individual patients. | |
|
• It is critical for neurologists to hone their skills in symptom management. |
The past couple of decades have led to increasingly rapid advances in disease-modifying therapies for multiple sclerosis. As such, there has been a plethora of information for neurologists to become familiar with to provide effective and safe long-term treatment options. However, the emphasis placed on our ability to modulate the immune system may sometimes distract attention from multiple sclerosis symptom management. Multiple sclerosis affects each patient in a unique manner, and symptoms of multiple sclerosis may range widely among different patients. These symptoms may have a significant impact on the quality of life in patients with such symptoms. As such, it is crucial that neurologists master not only making the diagnosis of multiple sclerosis and the disease-modifying therapy options but also the symptom management of the plethora of symptoms our patients’ faces. It is key to involve all stakeholders in potential solutions, working in a multidisciplinary way to ensure that patients with multiple sclerosis are part of the team in shared decision-making and disease management (81). Suboptimal symptom management may also be mistaken as progression of the disease, and knowledge about optimizing this management may help differentiate this diagnostic dilemma.
Neurologists are classically taught to localize lesions and to ascertain their etiology in pursuit of a diagnosis. Beyond this important step, patients need neurologists who can simultaneously treat their disease and day-to-day symptoms. This is why comprehensive care models, composed of neurologists as well as allied health professionals, are so crucial (16). However, it behooves neurologists to become adept at managing multiple sclerosis symptoms, even in the absence of a larger team; knowledge gained during residency training programs may be supplemented by journal articles in the Multiple Sclerosis Journal, Practical Neurology, International Journal of MS Care, and Multiple Sclerosis and Related Disorders.
|
• The goal of symptomatic therapy is to optimize the daily functioning of patients with neurologic dysfunction due to multiple sclerosis. | |
|
• Fatigue is quite common in multiple sclerosis but can also be multifactorial. It is important to help distinguish between these causes to help guide optimized treatment. | |
|
• Spasticity is a common symptom in multiple sclerosis and there are several pharmacologic, nonpharmacologic, and procedural options for treatment. | |
|
• Pain is another common and often challenging symptom to treat in multiple sclerosis. Pain can be classified into categories that aid in the selection of treatments: paroxysmal neuralgic pain, chronic neurogenic pain, and musculoskeletal pain. |
Fatigue. Fatigue has been defined as a reduction of effective output for the exerted input (19), “a subjective lack of physical and/or mental energy that is perceived by the individual or caregiver to interfere with usual and desired activities” (94), and as reversible motor and cognitive impairment, with reduced motivation and strong desire to rest (89). Fatigue may occur spontaneously or after provoking factors, such as physical or mental activity, as well as rises in body temperature. Fatigue may also be either acute or chronic in our patients with multiple sclerosis. It is usually worse in the afternoon and may be relieved by rest or sleep (89).
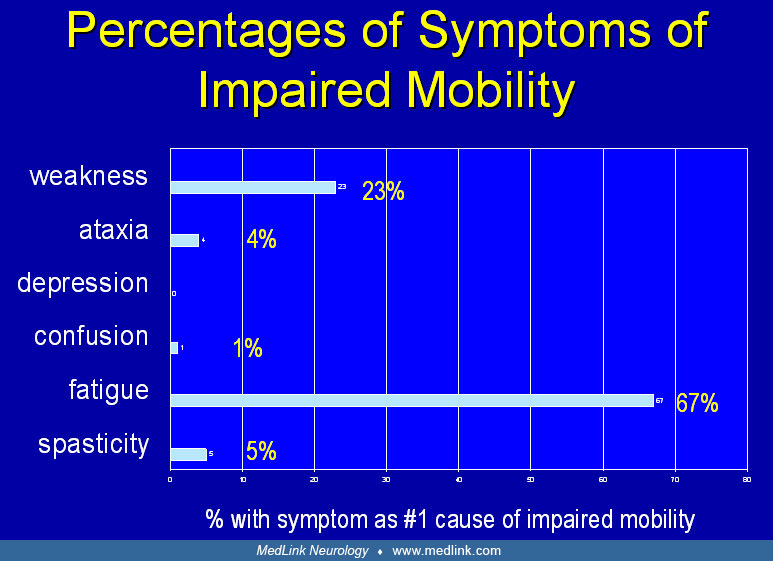
Fatigue is usually identified by patients as the most frequent and disabling symptom of multiple sclerosis, with 75% to 90% of patients with multiple sclerosis experiencing unusual fatigue as compared to about 30% of the general population. In fact, about two thirds of patients with multiple sclerosis list fatigue as one of their three most bothersome symptoms. Fatigue impedes mobility for 50% to 60% of patients (40). Social Security Disability may be awarded on the basis of fatigue, and fatigue is one of the two major reasons for unemployment among people with multiple sclerosis. Two monographs that are useful references for the management of fatigue have been published (94; 65).
Fatigue in multiple sclerosis can be from a variety of causes: mood disorders (such as depression), sleep pathology (such as sleep apnea, restless legs syndrome), medication side effect, or from multiple sclerosis itself. It is important for clinicians to help distinguish between these causes as it would impact treatments. New or worsening fatigue may also be a sign of a multiple sclerosis relapse. Unfortunately, no large, comprehensive study has been performed to define and differentiate the many theoretical causes of fatigue in this population. Still, it is important to distinguish fatigue as a consequence of modifiable conditions, such as sleep disorders.
Sleep pathology. Almost half of all patients with multiple sclerosis complain of sleep disturbances, with one in five diagnosed with an insomnia disorder (159). Sleep pathology includes periodic limb movements of sleep and restless legs, hypersomnia, insomnia or disrupted sleep, delayed sleep phase syndrome, and sleep apnea. In a small study, disrupted sleep has correlated with fatigue measured by the Fatigue Descriptive Scale (05).
Insomnia, the most common complaint, has many potential causes and it is critical for neurologists to take a good history to see if a potential etiology for insomnia can be elucidated. Conditions that are associated with insomnia include depression/anxiety, medication side effects, pain, nocturia, restless legs syndrome, muscle spasms, sleep-related leg cramps, inactivity, and possibly alterations of the wake-sleep cycle caused by central nervous system pathology. In a group of 60 patients in London, insomnia in the middle of the night was most often caused by nocturia and was associated with daytime fatigue (135).
Treatment of insomnia should begin with an attempt at arriving at a specific diagnosis and treatment. If none is found, then nonpharmacological options should be used initially, such as establishing good sleep hygiene. Good sleep hygiene includes establishment of regular sleep schedules with sufficient “wind-down” time prior to sleep onset and avoiding screen time before bed (such as computer, tablet, TV, or cell phone use). The use of screens that emit blue light, before bed, can decrease melatonin secretion and thereby cause difficulty with falling asleep. To help minimize exposure to blue light, dim the brightness on the device (night mode/dark mode or install a blue light-filtering app) and cut down screen time, starting 2 to 3 hours before bed. If needed, it is best to use a dim red lightbulb as a nightlight, as red is the color that least affects circadian rhythm. Stimulants and insomnia-producing drugs should be avoided if possible, and regular sleep schedules should be established with sufficient “wind-down” time prior to sleep onset. Patients should be encouraged to avoid pre-sleep computer use or watching television in the bedroom, which can cause activation and difficulty in falling asleep. Daily exercise may improve sleep quality. There have been small studies demonstrating a benefit for cognitive behavioral therapy for insomnia to help with improvement of sleep efficiency as well as actigraphy sleep outcomes (154). This can be pursued either via psychology assistance or, potentially, applications through smart phone markets. Nocturia should be eliminated if possible. Polysomnography is reserved for patients with suspected sleep apnea, periodic leg movements, or other conditions that require quantification.
Long-term treatment of insomnia using sleep-inducing pharmacological agents is generally discouraged. The melatonin receptor agonist, ramelteon, appears to decrease sleep latency without rebound in some patients with chronic insomnia. Benzodiazepines may be effective, and a 12-month open-label study using eszopiclone showed continued efficacy of treatment in primary insomnia (116). Clinicians should always be mindful of potential associated risks with these medications, including withdrawal if sudden cessation and risks of respiratory depression, particularly in older populations.
Sleep disturbance | Therapy |
Periodic leg movements | Diazepam (5 to 10 mg) |
Insomnia | Triazolam (0.125 to 0.25 mg) |
| |
Medication side effects. Fatigue can be a common side effect of prescription medications. Antispasticity agents, anxiolytics, antiepileptic drugs, and analgesics may cause sedation, which may be perceived as fatigue. Disease-modifying therapies such as interferon-beta may also be associated with relatively persistent fatigue. If fatigue-inducing medications are essential and irreplaceable, stimulant use may be considered in order to counteract this side effect. However, all medications should be reviewed to ensure there is a balance between side effects and benefits.
Affective disorders. Depression, anxiety, and perceived poor health are all associated with fatigue; at the same time, fatigue itself can induce social withdrawal and depression. Fatigue is worse for patients with tendencies for symptom somatization as well as for those who feel that they have little control over their environment (145).
Idiopathic lassitude. Lassitude is probably the most common and poorly understood form of multiple sclerosis fatigue. It may be the result of inefficient communication between areas of the brain that are supposed to interact whenever the patient is active. Diminished neuronal integrity, as demonstrated by diminished cerebral metabolism (112), lowered N-acetylaspartate-creatinine ratio (142), and greater brain atrophy (74), has been associated with high levels of subjective fatigue. Inflammation may also cause lassitude. Interleukin (IL)-1, released by inflammatory cells, can induce lassitude when injected into the ventricles of animals. A relapse of multiple sclerosis is often associated with severe fatigue, possibly due to this mechanism. It is thought that the severity of multiple sclerosis fatigue “does not correlate with the cumulative lesion load” or the presence of active brain lesions. Rather, it may correlate with localized lesions within the prefrontal, temporal, and thalamic regions (105). This type of fatigue may occur without preceding activity and may be helped by a brief nap.
Some multiple sclerosis–associated conditions may present with fatigue. Uhthoff phenomenon (the worsening of existing neurologic symptoms in the setting of increased body temperature), for example, may affect motor, cognitive, and other functions. It is precipitated by emotional stress, a rise in body temperature, and activity. Presumably, increased recruitment of neurons or using the same neurons for multiple tasks makes them refractory to excitation, whereas high body temperature shortens the duration of action potentials, leading to electrochemical transmission failure along demyelinated axons. Thus, any activity or condition that raises body temperature may result in fatigue and weakness. Furthermore, patients with multiple sclerosis have difficulty regulating body temperature, and this may be linked to fatigue severity. This may also explain why a trial with 650 mg of aspirin taken at morning and noon improved fatigue in patients with multiple sclerosis (155). There may also be some data for aspirin premedication reducing overall increases in body temperature in exercise and, thus, improving exercise performance (68). Turning the thermostat to a temperature of 65°F to 68°F may also help. The Multiple Sclerosis Association of America offers cooling vests free of charge to patients with heat sensitivity.
Fatigue similar to that seen with beta-adrenergic blockers has been linked to sympathetic vasomotor insufficiency (dysautonomia) in patients with multiple sclerosis (32). The amount of change in cardiac stroke volume and ejection fraction measured at rest when compared to hyperventilation is inversely correlated with fatigue, suggesting that abnormalities of vagal function may be a factor, resulting in fatigue (83).
Treatment: Some patients report improvement in fatigue after initiation of immunomodulators. The most commonly associated immunomodulatory agent noted with improvement in fatigue is natalizumab.
Chronic lassitude may be helped by caffeine, amantadine, and other stimulants (Table 2). The efficacy of amantadine is poorly supported at present (143). Although a well-controlled trial of modafinil showed no greater effect on fatigue in patients with multiple sclerosis than placebo (126), in the authors’ experience and in the experience of others (111), the vast majority of patients with multiple sclerosis report dramatic response to it. In a self-report survey, 84% of 119 respondents with “primary MS-related fatigue” who had used modafinil found it to be helpful for fatigue (136). A crossover pilot study showed armodafinil improves delayed verbal recall in patients with multiple sclerosis (15). Stimulants have also been used as adjuncts to treat depression and improve cognitive function after brain injury (18). Mixed amphetamine salts and methylphenidate are generic drugs that some patients find helpful. Although controlled release products are generally preferred, in some patients they interrupt sleep to a greater extent than immediate release products. Cases of sudden death have been tied to the use of stimulants in both adults and children, primarily among those with preexisting structural heart defects. These drugs may exacerbate some preexisting psychiatric disorders, including anxiety, depression, paranoia, major thought disorders, and bipolar disorder. Extended release and transdermal delivery systems for methylphenidate, extended release dexmethylphenidate, and the pro-drug isdexamfetamine dimesylate may offer advantages over the generics at a higher price.
Bupropion and some other antidepressants (Table 2) may be helpful in treating fatigue, although whether the effect is primary (25) or secondary due to amelioration of depression (122) is uncertain.
There are many studies supporting the effectiveness of regular exercise in lessening fatigue. A cross-sectional study found diminished fatigue in patients with multiple sclerosis who exercise, compared to those who are sedentary (138). Exercise three times weekly has been shown to improve fatigue and quality of life in patient-reported outcomes (80). Yoga has been shown to be as helpful as regular exercise in combating fatigue (102). There have also been several randomized controlled trials showing a benefit of mindfulness-based interventions as a means to improve fatigue (131). Acupuncture may also have some benefits with fatigue, although large, randomized control trials are needed (60).
Patients are often interested in low-dose naltrexone, which is highly touted on multiple internet sites as an effective therapy for virtually any multiple sclerosis symptom (and a host of other diagnoses). Naltrexone, an opioid antagonist at higher doses, appears to have a mixed agonist-antagonist effect at lower doses. A patient-funded study conducted by Bruce Cree examined the effect of low-dose naltrexone on quality of life in a double-crossover trial design (22). Patients with multiple sclerosis taking low-dose naltrexone reported improved quality of life, diminished pain, and improved self-reported cognitive function. No improvement in physical quality of life was found, and comprehensive standardized disability ratings (expanded disability status scale score) were not conducted as part of the trial. Low-dose naltrexone appears to be well tolerated, and further research may clarify whether it offers symptomatic treatment to patients with multiple sclerosis. Some have observed that patients with multiple sclerosis taking low-dose naltrexone tend to exhibit signs of euphoria, which may be perceived as improved energy level.
Class of drug | Drug | Comment |
Generalized stimulants | ||
• First line | Amantadine (100 to 400 mg) | Has few side effects; works in less than half of patients (98). |
Activates tubero-mammillary nucleus leading to an increase in extracelluar dopamine levels | Modafinil (100 to 200 mg, maximum 400 mg) | Does not produce much anxiety; 20% decrease in estradiol concentrations of contraceptive pills. |
Similar to modafinil, inhibits dopamine reuptake through activation of tubero-mammillary nucleus | Armodafinil (50 to 250 mg) | Does not produce much anxiety; 20% decrease in estradiol concentrations of contraceptive pills. |
• Second line | Methylphenidate (5 to 40 mg or extended release) | Formulations include extended release and transdermal patch; addictive, must rewrite prescriptions monthly. |
Dexmethylphenidate (10 to 20 mg) | ||
Mixed amphetamine salts (5 to 40 mg) | ||
Lisdexamfetamine dimesylate (30 to 70 mg) | In children, 39% decreased appetite, 19% insomnia. | |
“Energizing” antidepressants | Bupropion (100 to 300 mg) | May induce weight loss; contraindicated with history of seizures. |
Fluoxetine (5 to 40 mg) | ||
Venlafaxine (37.5 to 225 mg) | Extended-release formulations are more expensive but help with compliance. | |
Desvenlafaxine (50 to 100 mg) | ||
Temperature modulator | Aspirin (650 mg at morning and noon) | Single study suggests efficacy. |
Spasticity. Spasticity is a motor symptom associated with upper motor neuron dysfunction, and, as such, is commonly seen in multiple sclerosis. Spasticity may be manifested as an increase in tone at rest (rigidity), tone that increases with the speed of movement (spasticity), slow contraction of antagonistic muscles (dystonia), heightened tendon reflexes, and myoclonic jerks. These forms of spasticity may occur independently or together. Spasticity in multiple sclerosis is often related to spinal cord damage. The functional consequences of spasticity range from mild impairment of running to increases in adductor tone that compromise genitourinary hygiene. Spasticity can be profoundly disabling and may lead to permanent contractures. Despite the potentially disabling nature of spasticity, spasticity may be useful in severely weak and minimally ambulatory patients with multiple sclerosis in allowing them to stand, pivot, and transfer. Spasticity in multiple sclerosis can also worsen during pseudo-relapses, or when patients experience infections causing worsening of existing neurologic symptoms. Sub-primate systems have not proven useful in predicting the responses of humans to treatment of spasticity, so therapy largely has been empirically determined (156).
There are pharmacologic, nonpharmacologic, and procedural options for treatment of spasticity. Spasticity may improve with an exercise program (107). Passive and active muscle stretching may reduce the amount of medication required to treat spasticity and can prevent contractures. Reduction of pain reduces spasms.
First-line agents for spasticity include baclofen and tizanidine (Table 3); because they have different mechanisms of action and toxicities, they can be combined to improve outcomes (104). A phase 3 randomized, double-blind, placebo-controlled trial in 536 participants evaluated the safety and efficacy of arbaclofen, an extended-release active enantiomer of baclofen; this study was completed in 2019 and results are pending (NCT03290131).
In cases of severe sedation and other systemic side effects of baclofen or insufficient efficacy with oral baclofen, alternative modes of administration should be considered such as using intrathecal baclofen (ITB) pumps. ITB may especially benefit non-ambulatory patients when spasticity is painful, interferes with skin care or hygiene, or makes transfer and positioning difficult. It occasionally provides dramatic benefit for both nonambulatory and ambulatory patients. In particular, it may be helpful for ambulatory patients with good strength but significant gait abnormalities due to spasticity as well as some patients who would otherwise be non-ambulatory have been able to ambulate due to ITB pump placement. The systemic side effects of baclofen are minimal with this form of administration due to the differences from metabolism of oral administration. Patients generally undergo a test dose of ITB (via lumbar puncture with or without temporary catheter placement) to determine responsiveness prior to undergoing surgical implantation of the ITB pump. A guide to the step-by-step implementation of this treatment has been published (52).
Botulinum toxin injections can be used to relax single or small groups of spastic muscles (133). They are especially useful for patients with a painful, dystonic posture of a hand, foot, and occasionally the neck, and in patients with compromised personal hygiene due to adductor spasm. OnabotulinumtoxinA is FDA approved for upper extremity spasticity; other forms of botulinum toxin have also been used in clinical practice and in clinical trials for spasticity.
Although controversial, cannabinoid compounds have been investigated for multiple symptoms, including pain and spasticity in multiple sclerosis (101). A number of patients report that cannabinoids are beneficial in the management of their spasticity. In many studies, objective improvement has not been satisfactorily demonstrated to date (62), but there are a few studies showing some benefit. Trials to date are summarized in (157). Spasticity, as measured by the Ashworth scale (more recent trials of spasticity utilize the modified Ashworth scale), was not impacted by cannabinoids according to a large, randomized controlled trial (158). However, the study tracked secondary outcomes with self-reported measures. Self-reported pain, spasms, spasticity, and sleep quality improved in patients taking cannabinoids. Subsequent trials have confirmed self-reported improvement in pain and spasticity. Legal issues surrounding use of cannabis and its derivatives complicate clinical trial design in many locations, whereas cannabinoid compounds have received regulatory approval for use in other locations. Dronabinol is used off-label in the United States. Nabiximols has been approved to treat multiple sclerosis symptoms in Canada and in the United Kingdom (157). Ongoing trials in 2022 of cannabinoid compounds for spasticity in multiple sclerosis may help shed more light on efficacy information.
Class | Comment | |
First line drugs | ||
Baclofen (5 to 40 mg, every 3 to 6 hours) | Gamma-aminobutyric acid antagonist | May cause weakness, lethargy, confusion. |
Tizanidine (2 to 12 mg, every 3 to 4 hours) | Noradrenergic alpha-2 agonist | Sedation may help insomnia and painful nocturnal spasticity. |
Second line drugs | ||
Gabapentin (200 to 900 mg, three to four times daily) | Anticonvulsant | Useful for dystonic spasms. Renal metabolism. |
Carbamazepine (100 to 400 mg, three times daily) | Anticonvulsant | Useful for dystonic spasms. Can induce severe weakness. Risk of hyponatremia. |
Levetiracetam (250 to 1500 mg, twice daily) | Anticonvulsant | May avoid some of the cognitive problems induced by other AEDs. Renal metabolism. |
Diazepam (2 to 10 mg, two to three times daily) | Benzodiazepine | Some patients find diazepam better than first-line agents. |
Dantrolene (25 to 100 mg, three times daily) | Prevents Ca++ release from muscle stores | Causes weakness; must monitor liver enzymes. |
Speculative | ||
Clonidine | Alpha-adrenergic agonist | |
Cyproheptadine (max dose 16 mg) | Antihistamine and serotonin antagonist | Stimulates appetite. Ameliorates EAE. |
Some anticonvulsants and benzodiazepines have mild ameliorating effects on spasticity. Levetiracetam appears to modify phasic spasticity without inducing cognitive changes (45). It should be noted that ciprofloxacin use is inadvisable in patients taking tizanidine as it may increase tizanidine blood levels dramatically. Sativex is the only commercially available formulation containing cannabinoids and is used as add-on therapy for treatment of spasticity in adult patients with multiple sclerosis who are nonresponders to conventional antispastic therapies. Sativex has shown good safety profile and improvement in quality of life (34). It is not available in the United States.
Bladder dysfunction. Bladder dysfunction in multiple sclerosis can be variable from person to person; the varieties of bladder dysfunction include urinary urgency, urinary hesitancy and retention, urinary incontinence, and nocturia. Urgency, caused by detrusor hyperreflexia, is often associated with frequency due to reduced bladder capacity. Difficulty initiating flow is usually the result of inability to relax the external sphincter. A low flow rate may result from increased external sphincter tone or loss of tone in the detrusor. The latter, often referred to as areflexic bladder, is usually associated with marked leg spasticity or weakness. Detrusor-sphincter dyssynergia is used to describe the combination of a hyperreflexic bladder with inability to relax the external sphincter. Many patients with multiple sclerosis have this combination of symptoms resulting in urgency, hesitancy, and incomplete bladder emptying.
Outside of the impact that bladder symptoms have on daily quality of life for multiple sclerosis patients, it is also critical for neurologists to recognize these symptoms because untreated bladder dysfunction increases the risk of urinary tract infections. Three major risk factors for serious urinary tract complications are: an indwelling catheter, detrusor-sphincter dyssynergia in men, and detrusor pressures less than 40 cm of water. Aims of therapy should be to avoid these and to protect upper urinary tracts. Urosepsis, once a major cause of mortality among patients with multiple sclerosis, usually can be avoided (04).
The following are important facts in regard to bladder function and can help clinicians distinguish between normal and abnormal:
(1) The normal bladder can accommodate 450 to 500 cc of urine before the urge to void. | |
(2) Normal volume of voided urine is 300 to 500 cc, three to eight times daily. | |
(3) Post-void residual urine volume is normally only a few milliliters. | |
(4) The detrusor muscle is muscarinic (parasympathetic) and contracts in response to acetylcholine to empty the bladder. | |
(5) Adrenergic stimulation increases the tone of the external sphincter and inhibits the parasympathetic innervation of the detrusor, increasing the capacity of the bladder to store urine. | |
(6) The usual progression of bladder symptoms in multiple sclerosis is hyperreflexia of the detrusor muscle, then detrusor-sphincter dyssynergia, and then areflexia. | |
(7) Most patients with multiple sclerosis with good leg strength will have a hyperreflexic bladder. Detrusor-sphincter dyssynergia and areflexia are usually not found in patients until leg weakness is present, but exceptions occur. |
Evaluation of bladder function includes gathering information about the number of times the patient voids, the degree of urgency and hesitancy, severity of nocturia, the amount of fluid intake, the force and constancy of stream, the amount of urine voided, and the amount of and circumstances leading to incontinence. With only a clinical history, however, nearly 50% of patients are misdiagnosed (59). A carefully recorded micturition diary describes urinary function more precisely than the history alone. Ultrasound urine volumes, ideally done at the time of first urge to void and after voiding (post-void residual), can be obtained noninvasively. Post-void residual urine volumes as measured by ultrasound do not correlate well with reported symptoms (64). Some patients may be managed initially with relative confidence based on history, micturition diary, and pre- and post-void residual urine. The goals of therapy are to maintain a residual urine volume of less than 100 cc, produce a ratio of residual volume to voided volume that is less than one third, and to prevent recurrent urinary tract infection.
A guide for the treatment of bladder dysfunction containing a number of algorithms is available (95). In the case of hyperreflexic bladder, behavioral management includes reduced intake of substances that may irritate or stimulate the bladder such as caffeine, acidic or high sugar content beverages, reduced fluid intake when a lavatory will be unavailable or before sleep, and timed voiding. Timed voiding requires the patient to anticipate when the next need to empty the bladder will occur and void before the urge to urinate is felt. Patients should not reduce fluid intake during the day when a bathroom is available because concentrated urine is more irritating to the bladder. Over-the-counter calcium glycerophosphate, 333 mg, one to two doses with meals can be useful in reducing urinary acidity and decreasing urgency. Pelvic muscle training and relaxation techniques may be of some benefit (149).
Anticholinergics with strong anti-muscarinic activity are the treatment of choice for a hyperreflexic bladder and for increasing bladder capacity. Oxybutynin, a commonly used and inexpensive agent, has potentially helpful weak muscle-relaxant and local anesthetic actions.
Anticholinergic therapies are often associated with the unpleasant side effect of dry mouth. This may cause patients to drink more fluids, aggravating their frequency. Glycerin swabs or candies can occasionally be helpful in combating this problem. Blurred vision in bright light and acute angle closure glaucoma can be precipitated by anticholinergics because they cause pupillary dilation. Another concerning side effect of anticholinergic medication is impaired cognition (93). In addition to traditional anticholinergics, many other drugs (antihistamines, cimetidine, prednisolone, theophylline, and digoxin) can have detectable anti-muscarinic effects, potentiating medication interactions in older and cognitively impaired patients. In such patients, physicians may wish to use darifenacin for its M3 selectivity or trospium chloride, tolterodine, or solifenacin, which have low lipid solubility limiting their entry into the brain. M3 receptors are found in gastrointestinal smooth muscle, salivary glands, iris sphincter, and bladder but not in CNS tissue. It also may be advisable to combine these medications with newer, and unfortunately more expensive, therapies to substitute for drugs with anticholinergic effects in order to reduce the “total cholinergic burden” in patients susceptible to confusion.
Class | Comment | |
Hyperreflexia | ||
Anti-muscarinic agents | Imipramine (10 to 50 mg, up to twice daily) | Anticholinergic, alpha-adrenergic agonist, and cortical effects. |
Oxybutynin (2.5 to 10 mg, up to three times daily or extended release daily) | Formulations include extended release and transdermal patch. | |
Tolterodine (2 to 8 mg, up to twice daily or extended release daily) | Extended-release compounds useful in minimizing side effects. | |
Trospium Cl (20 mg, once or twice daily) | Give on empty stomach; renally excreted. | |
Solifenacin (5 to 10 mg, once daily) | ||
Darifenacin (7.5 to 15 mg, once daily) | Relatively selective for M3 receptor. | |
Hyoscyamine (0.125 to 0.25 mg, three or four times daily or extended release 0.375 mg) | ||
Propantheline (15 to 30 mg, up to four times daily) | ||
Detrusor dyssynergia | ||
Alpha-adrenergic agonists | Clonidine (0.05 to 0.1 mg, twice daily) | May induce hypotension. Doxazosin should be gradually titrated in dose. Tamsulosin and alfuzosin should be given within half hour after a meal. |
Terazosin (1 to 5 mg, daily) | ||
Doxazosin (1 to 8 mg, daily) | ||
Tamsulosin (0.4 to 0.8 mg, daily) | ||
Alfuzosin HCl (10 mg, daily) | ||
Areflexia | Bethanechol (25 to 100 mg, three times daily) | Must rule out obstruction first. Do not use in asthma, CAD, PUD. |
Nocturia | Desmopressin (0.1 to 0.4 mg at bedtime) (48) | Independent of bladder function, follow for hyponatremia. |
Alpha-blockers are used to treat difficulty initiating a urinary stream (hesitancy) initially. Care must be exercised to avoid induction of hypotension when these agents are used. Saw palmetto, an herbal preparation available without prescription, has been used to alleviate symptoms of hesitancy in association with benign prostatic hypertrophy, but in a well-controlled and adequately powered study, one preparation performed no better than placebo (10). An areflexic bladder may respond to muscarinic agonists. Double-voiding, a Credé maneuver that applies pressure on the bladder, or a vibrator placed over the lower abdominal wall may improve emptying of an areflexic bladder.
Procedurally, Botox injections as well as permanent catheter placement can be considered in specific cases. In 2011, the FDA approved onabotulinumtoxinA, at a total dose of 300 units, for injection at multiple sites into the detrusor muscle (123) for the treatment of urinary incontinence due to detrusor overactivity associated with neurologic conditions, such as multiple sclerosis. A permanent intraurethral catheter is rarely appropriate and usually only used for patients with immobility and limited surgical options. Common problems associated with chronic catheter use include recurrent stones, urethral erosion, urinary leakage, and urinary tract infections. Suprapubic catheterization reduces the risk of infection and avoids the difficulties involved with intraurethral catheters (14). Urological surgery including suprapubic catheters, augmentation cystoplasty, continent urinary diversion, ileovesicostomy, external sphincter stent prosthesis and external sphincterotomy in men, and implantation of InterStim devices can be helpful, although the latter precludes future MRI examinations.
Referral to a urologist should be considered if a post-void residual volume is greater than 200 cc. Volumes in this range can be associated with chronically elevated pressures (greater than 30 cm of water) in the bladder that lead to reflux of urine into the ureters and, in the setting of bacteriuria, infection of the urinary tract. If urinary pressures are high, intermittent catheterization is needed to prevent recurrent urinary tract infections, albeit improper catheterization can also lead to recurrent infection. Women, as compared to men, have a short urethra that provides less resistance to the contraction of the detrusor muscle. Changes in the pelvic floor induced by surgery and childbirth and the thinning of the vaginal mucosa with menopause make women more likely to be incontinent, although these changes also lead to low bladder pressures.
Avoidance and prompt treatment of bladder infections is paramount to the care of multiple sclerosis patients. A urine analysis with urine culture should be obtained in the setting of new urgency or recurrence of older neurologic symptoms (recrudescence or pseudo-flare) to look for infection. Patients with altered bladder sensation, however, often do not have typical symptoms in the setting of a urinary tract infection (in particular, urinary urgency as many patients may already have this symptom at baseline). A urine analysis can screen patients using two of the most sensitive indicators of infection, (1) leukocyte esterase and (2) moderate bacteriuria by microscopy. Patients can be given a urine dipstick to test their urine at home if they have malaise or worsening symptoms in conjunction with low-grade fever. However, conventional urine analysis can overlook about 14% of infections (144). Therefore, patients with multiple sclerosis with a decline in neurologic status or a change in bladder function should obtain a urine culture, even if the dipstick test or urine analysis is normal. A 3-day course of trimethoprim-sulfamethoxazole as initial therapy is sufficient for uncomplicated urinary tract infections in patients with early multiple sclerosis and minimal bladder symptoms. If resistance to these drugs is high, antibiotic choice is based on susceptibility testing. Patients with high residual urine volumes and high bladder pressures or who are taking immunosuppressive therapy require longer periods of treatment (7 to 10 days) to eradicate infection (31). Patients taking immunosuppressive therapy should undergo a repeat urine analysis at 5 days after initiation of therapy to ensure an appropriate response and a culture 10 days after the completion of therapy to verify complete resolution of the infection.
Elevated white blood cell counts are not a definite indicator of infection when patients have urinary catheters. Patients with Foley catheters and more than 100,000 CFUs by urine culture should be treated only if symptomatic.
More than three urinary tract infections per year is another reason for referral to a urologist. Patients who self-catheterize may be more susceptible to infection and may benefit from suppression of bacteria with uroquid acid (methenamine/sodium biphosphate) or methenamine and vitamin C, four times daily. Suppression with antibiotics can be done by alternating treatments using 1 month of nitrofurantoin, 50 mg per day, followed by 1 month of trimethoprim-sulfamethoxazole or trimethoprim alone, 400 mg per day. More aggressive suppression can be accomplished by irrigation of the bladder with gentamicin 240 mg in 500 ml of normal saline with 1 ampoule of sodium bicarbonate daily for 7 to 10 days. Irrigation is performed after changing the bladder catheter. Initially, 60 ml of normal saline is used to irrigate the bladder via catheter. Then 30 ml of gentamicin solution is placed into the bladder, and the catheter is cross-clamped for 30 minutes. The gentamicin mixture is drained through the catheter.
Bowel dysfunction. Bowel-related pathology has been ranked the third most bothersome symptom in multiple sclerosis after fatigue and mobility concerns (110). Constipation historically has been defined as hard stools, straining, incomplete evacuation, use of manual maneuvers to pass stool, or a sense of difficulty passing at least one in four stools or fewer than three bowel movements per week. These symptoms should be ongoing for 12 weeks or more per year. Because patients tend to underestimate their stool frequency (73), a bowel diary may clarify the history. Any patient with blood in the stool, weight loss, or whose onset of symptoms occurs at an advanced age should be referred to a gastroenterologist for evaluation of an alternate etiology. Patients with multiple sclerosis are vulnerable to constipation resulting from medications (anticholinergics, nonsteroidal anti-inflammatory agents, calcium supplements, opiates, and amantadine), decreased mobility, and dehydration (114).
The treatment of constipation begins with behavioral therapies. Bowel entrainment can be fostered by timing elimination 30 to 60 minutes after the same daily meal. Regular exercise, dietary fiber and fruits, and good hydration all contribute to good bowel function. One half cup of a mixture of one-third prune juice, one-third apple sauce, and one-third bran cereal ingested once or twice daily is well tolerated and beneficial when symptoms are mild. Pineapple also seems to be particularly useful as a food that promotes regularity. Some patients have reported that the use of bifidobacteria-containing yogurt has been helpful for them.
Concentrated fiber preparations increase the bulk and water content of stool. Colonic bacteria metabolize natural fiber sources such as psyllium, oat bran, and fruits, which results in the release of gas. This phenomenon does not occur with synthetic or insoluble fibers such as methylcellulose and polycarbophil or wheat bran/dextrin. Stool softeners can be added to fiber. Softeners include docusate sodium and docusate calcium.
Hyperosmolar agents, such as sorbitol, lactulose, and polyethylene glycol can be effective but may also cause bloating. The American College of Gastroenterology Chronic Constipation Task Force has made a grade A recommendation for both lactulose and polyethylene glycol for improving stool consistency and frequency (03). Pyridostigmine 30 to 60 mg or erythromycin 333 to 400 mg taken before meals may increase peristalsis.
A number of relatively inexpensive stimulants (bisacodyl, senna, cascara, and phenolphthalein) and saline laxatives are available for intermittent use. Some "natural remedies" contain significant amounts of senna and cascara. Decreased absorption of fats and fat-soluble products and induction of refractory constipation limit the use of all stimulants. Glycerin suppositories used every other day or bisacodyl suppositories every third day may also help.
Gastrointestinal propulsives include cisapride, domperidone, and metoclopramide. Cisapride and domperidone both have cardiac toxicity whereas metoclopramide can induce parkinsonism.
Lubiprostone is a chloride channel activator that increases intestinal fluid secretion. It has low systemic absorption but can cause nausea. Trials using 24 mcg twice per day appear to show benefit in chronic constipation. Another option may include linaclotide for chronic constipation.
Any individual with fecal incontinence should be assessed for constipation with overflow (National Guideline Clearinghouse 2004).
Sexual dysfunction. Sexual dysfunction generally affects patients with multiple sclerosis with spinal cord lesions or with insular or pontine lesions (130). In a healthy individual, during intercourse, multiple neural networks on both conscious and unconscious levels coordinate to reach a successful culmination. However, in multiple sclerosis, there are a variety of factors that may interfere with this. Decreased libido, numbness and dysesthesias, vaginal dryness, autonomic dysfunction, vascular insufficiency, emotional and cognitive impairment, spasticity, bladder dysfunction, and side effects of medications all can contribute to unsatisfactory intercourse. Specifically, of the medications commonly used to treat symptoms of multiple sclerosis, most antidepressants affect sexual function, although bupropion and mirtazapine generally spare the ability to achieve orgasm. Alpha-adrenoceptor antagonists, frequently used to treat urinary hesitancy, can lead to disorders of ejaculation. Oral baclofen can occasionally induce sexual dysfunction. Beta-blockers, antipsychotics, thiazide diuretics, and spironolactone may also induce sexual dysfunction. Marital discord can cause sexual dysfunction, but nearly 25% of patients believe that the lack of sexual fulfillment has contributed to marital problems. Surprisingly, corticosteroid treatment has been observed to sometimes improve sexual function (76).
Fifty percent to 75% of men with multiple sclerosis report erectile dysfunction. This has become much easier to treat with the development of oral phosphodiesterase inhibitors, such as sildenafil, vardenafil, and tadalafil. These medications should be used with caution or not at all when patients are taking other vasodilators. Medications that inhibit the P-450 system such as statins, protease inhibitors, and systemic triazole antifungals increase the plasma levels of the oral phosphodiesterase inhibitors and increase side effects. Vacuum devices and alprostadil urethral suppositories can be used alone or added to phosphodiesterase inhibitors. Intracavernous injections of prostaglandins E1, papaverine, and phentolamine in different concentrations can be effective as well. The cost of these preparations varies depending on the composition. As many as 25% of men with multiple sclerosis have premature ejaculation. This generally responds well to selective serotonin reuptake inhibitors taken an hour before intercourse.
Testosterone maintains sexual desire, and levels have been found to be slightly lower in men with multiple sclerosis. Other endocrine causes of erectile dysfunction include hyperthyroidism and prolactinomas. The vascular risk factors of inactivity, diabetes, hypertension, and dyslipidemia are associated with restricted pudendal artery flow and erectile dysfunction. Patients with Peyronie disease develop pain and penile curvature with erections that results in dysfunction. A more detailed review of erectile dysfunction is available (07).
The most common complaints of women with multiple sclerosis are inadequate lubrication, anorgasmia or hypo-orgasmia, reduced libido, diminished perineal sensation, as well as genito-pelvic pain/penetration disorder (84). An association of cerebellar disturbances and orgasmic dysfunction has been found (42). Vaginal creams and water-soluble lubricating jellies can be used to treat vaginal dryness. Petroleum-based jellies should be avoided because they can leave residues that promote bacterial vaginitis. Patients experiencing diminished sensitivity often respond to vibrators. Oral sildenafil may be an adjunct to sexual arousal, but small studies have shown only a limited effect on lubrication. This agent has also been compounded as a cream, sometimes combined with L-arginine, and applied to the clitoris with anecdotal success. Ten percent of women with multiple sclerosis have painful perineal dysesthesias that may be manageable with carbamazepine, gabapentin, or the local application of 2% Xylocaine gel. Women with incontinence should empty the bladder prior to intercourse, and those with high residual volumes should empty afterwards.
Intercourse for patients with urinary catheters and spasticity may be possible with proper positioning and treatment of spasticity. For diminished libido, treatment with bupropion may provide some benefit (125).
Cognitive behavioral therapy (CBT) is an effective approach for all female sexual dysfunction disorders through literature review, particularly with identifying factors contributing to sexual dysfunction and targeted management. However, there are limited clinical trials looking at this. Other potential nonpharmacologic interventions include acupuncture, yoga, psychoeducational interventions, and acceptance and commitment therapy (84). There are some data behind consideration of pelvic floor exercise in conjunction with mindfulness techniques or electromuscular stimulation with electromyograph biofeedback (35). However, more studies are required. Engaging the help of a certified pelvic floor physical therapist as well as referral to a sexual medicine clinic may also be of help.
In essence, bladder, bowel, and sexual problems remain common in patients with multiple sclerosis, and despite several treatment options available, overall satisfaction still remains low (151).
Pain. Pain is common in multiple sclerosis. Over half of the subjects in a cross-sectional study described acute or chronic pain syndromes during the course of the disease (92). Nearly a quarter of patients take analgesics daily as compared to less than 10% of a control population; 19.3% of patients with multiple sclerosis reported that pain interfered with daily life “all the time” versus 7.4% of controls (140). It is frequently challenging to differentiate between pain caused by tissue damage in multiple sclerosis and pain that is behaviorally associated. Although both can be difficult to treat, the latter may be characterized by confrontation between patient and caregivers. Other causes of pain should always be considered when a patient develops a new pain syndrome. Chronic neurogenic dysesthesias are commonly experienced in patients with secondary progressive multiple sclerosis (119).
Pain can be classified into categories that aid in the selection of treatments:
Paroxysmal neuralgic pain. Paroxysmal neuralgic pain is variably described as sharp, stinging, burning, shocking, or by an equivalent phrase. In a study, this was the most common type of pain experienced (41). These paroxysmal pains may be atypical in patients with multiple sclerosis when compared to "idiopathic" cases. Paroxysmal neuralgic pain includes trigeminal neuralgia, glossopharyngeal neuralgia, occipital neuralgia, pseudoradicular pain, and Lhermitte phenomenon.
Medication | Comment | |
First line | Gabapentin (300 to 900 mg, three to four times daily) | Renally metabolized, has few drug interactions. |
Pregabalin (100 to 300 mg, twice daily) | Calcium channel modulator similar to gabapentin. | |
Carbamazepine (200 to 400 mg, three times daily) | May induce severe weakness. Asians with HLA-B*1502 are subject to serious skin reactions. Monitor for hyponatremia. | |
Gabapentin (300 to 900 mg, three to four times daily) | ||
Phenytoin (200 to 600 mg, daily) | ||
Valproic acid, valproic acid ER (15 to 60 mg/Kg, daily in divided doses) | ||
Pregabalin (100 to 300 mg, twice daily) | Calcium channel modulator similar to gabapentin. | |
Second line | Oxcarbazepine (300 to 1200 mg, twice daily) | Fewer drug interactions and side effects than carbamazepine. |
Zonisamide (200 to 400 mg, daily) | May cause diminished sweating with increased body temperature. Is a sulfonamide. | |
Levetiracetam (500 to 2500 mg, daily) | Few drug interactions. | |
Of special use in trigeminal neuralgia | Topiramate (50 to 200 mg, twice daily) | May induce weight loss and a hyperchloremic metabolic acidosis. |
Misoprostol (200 µg, four times daily) | Prostaglandin E agonist. | |
Lamotrigine (100 to 400 mg, daily) | Dose must be carefully titrated, Stevens-Johnson syndrome. | |
Baclofen 40 to 120 mg daily in three to four divided doses | May cause weakness, lethargy, and confusion. | |
*AAN Summary of Evidence-based Guidelines advise that strong evidence exists only for the use of carbamazepine in the treatment of classical trigeminal neuralgia and that good evidence exists for only oxcarbazepine and topical ophthalmic anesthesia (01). | ||
Chronic neurogenic pain. Chronic neuropathic pain involves the feet and legs more commonly than the hands. Although chronic neuropathic pain is not associated with quantitative sensory threshold changes, mechanical or thermal hyperalgesia is common (139). If the pain is well localized, application of a 5% lidocaine patch is sometimes helpful. Up to three patches may be applied for up to 12 hours within a 24-hour period. Patches may be cut to fit the area involved. The long-lasting effects of short-term intravenous lidocaine treat chronic neurogenic pain as well as musculoskeletal pain (78). Capsaicin cream, 0.075% applied three to five times daily, may be an adjunct to other therapies. The cream should be initiated at the 0.025% dose and advanced slowly to the 0.075% concentration. Transdermal lidocaine patches (5% lidocaine) have been used effectively by some patients with chronic pain problems. Compounded topical creams are widely available to help ameliorate pain, and they may be useful in the treatment of pain related to multiple sclerosis.
Tricyclic antidepressants and anticonvulsants are the mainstay of treatment, but many therapies have been used when the pain is intense. To minimize side effects, one may start with gabapentin, and, if a partial response is obtained, consider adding an additional anticonvulsant or a muscle relaxant to assist at night, when pain may be most noticeable.
Medication | Comment | |
First line | ||
Antidepressants | Amitriptyline (50 to 150 mg) | Monitor for QTc prolongation at higher doses. |
Desipramine | ||
Duloxetine (20 to 60 mg extended-release daily) | ||
Anticonvulsants | Carbamazepine (200 to 400 mg, three times daily) | Monitor for hyponatremia. |
Gabapentin (300 to 900 mg, four times daily) | Renally metabolized, has few drug interactions. | |
Pregabalin (100 to 300 mg, twice daily) | ||
Second line | ||
Anticonvulsants | Zonisamide (200 to 400 mg, daily) | |
Lamotrigine (100 mg, twice daily) | Titrate slowly given risk of Stevens-Johnson syndrome. | |
Levetiracetam (500 to 2500 mg, daily) | ||
Pregabalin (up to 600 mg daily, in two or three divided doses) | ||
Oxcarbazepine (600 to 1200 mg, twice daily) | ||
Antispasticity | Baclofen (up to 200 mg, four times daily) | |
Tizanidine (up to 8 mg, four times daily) | ||
Opiates | See Table 7 | Doses are extremely variable; higher doses require contract and possible referral. |
Alpha-adrenergic agonist | Clonidine | |
Antidepressant | Duloxetine HCl (20 to 60 mg, twice daily) | |
Topical | Lidocaine 5% cream Capsaicin cream | |
Duloxetine HCl and venlafaxine, selective serotonin (5-HT) and norepinephrine (NE) reuptake inhibitors, are useful in diabetic neuropathy and in some forms of myofascial pain. A double-blinded randomized clinical trial demonstrated superiority of duloxetine over placebo in the treatment of the central neuropathic pain of multiple sclerosis.
If pain is severe only at night, a hypnotic may be helpful. Another consideration may be a neuropathic pain agent that has sleepiness as a component of its side effect profile, such as tricyclic antidepressants.
Treatment of nonmalignant pain with opiates should be done cautiously. Opiate abuse may vary demographically. A 2002 study reported that 21.5% of 242 inner-city drug users had taken sustained-release oxycodone, methadone, or hydrocodone within the prior 30 days (147). The use of a clinic with specialization in treating pain is recommended.
The FDA Anesthetic and Life Support Drug Advisory Committee has concluded that physicians need to meet seven documentation requirements when making opiates part of pain management for nonmalignant pain. These requirements are: (1) appropriate history and examination, (2) a “recognized medical indication,” (3) a written treatment plan, (4) a pain management treatment plan signed by the patient, (5) reasonable follow-up where progress is reviewed, (6) maintenance of accurate records, and (7) close monitoring of patients with a history of substance abuse. The doses of opiates necessary to control pain vary greatly, although the goal should always be keeping the dose of these addictive medications low. Combinations of deterrent agents and opiates are being developed to reduce the addictive potential of opiates when used to treat pain.
Drug | Dose |
Morphine | 15 or more mg, every 4 hours |
Extended-release morphine | 15 to 60 mg, every 12 hours |
Oxycodone | 5 to 10 mg, every 4 hours |
Extended-release oxycodone (increasingly abused) | 30 mg, every 12 hours |
Fentanyl transdermal patches 25 to 100 mcg/hr can be used in patients who are tolerant to oral opioids. The 25 mcg/hr dose of fentanyl is equivalent to approximately 100 mg/day oral morphine, 50 mg/day oral oxycodone, 12 mg/day oral hydromorphone, or 30 mg/day oral methadone.
Clonidine or tizanidine can be used as an adjunct to opiate use. Intrathecal morphine (800 to 10,000 µg per day) and clonidine (400 to 750 µg per day) can be used if a continuous infusion pump is implanted (63).
Cannabis-based medications are being tested in chronic pain states with modest effects on pain and few side effects (113).
Headache or back pain. Headache or back pain can be a sign of a relapse. In some situations, such as retrobulbar optic neuritis, pain may be well localized. There are conflicting epidemiological data on whether migraine headaches are more common in patients with multiple sclerosis than in the general population (55), and headaches in patients with multiple sclerosis may be caused by the multiple sclerosis itself or as a side effect of the disease-modifying agents or symptomatic therapies. Treatment of chronic headaches in patients with multiple sclerosis is no different from idiopathic headaches. The side effect profile of each oral agent must be considered when determining what to use for patients with multiple sclerosis with headaches; for example, topiramate should be used cautiously in patients with cognitive concerns. Botox injections and CGRP inhibitors can also be considered.
Musculoskeletal pain. Musculoskeletal pain can be caused by ligamentous and bursal inflammation from inactivity, overuse of muscle groups, improper mechanics of joint movement, muscle spasms, pressure sores, and other syndromes of undefined etiology. Most neurologists will utilize orthopedic and rheumatologic consultants to manage these diverse problems. A high incidence of hypovitaminosis D has been found in American patients with nonspecific musculoskeletal pain. However, treatment with vitamin D did not improve chronic pain in randomized, controlled clinical trials (152; 137).
Due to the association of corticosteroid use and avascular necrosis of the femoral head and other bones, neurologists should be familiar with its symptoms and differential diagnoses. The absence of pain with flexion and extension of the hip and external rotation (Patrick-Fabere test) is useful in differentiating trochanteric bursitis from intra-articular hip disease (127).
The basis of treatment for most musculoskeletal pain is the application of heat, stretching and strengthening exercises, bracing, and nonsteroidal anti-inflammatory drugs. Therapies that are useful in chronic pain syndromes may be of use in this setting (see above). Patients with multiple sclerosis are commonly affected by common painful conditions such as migraine and fibromyalgia (chronic, widespread, axial pain). All three conditions are more common in women. Pregabalin, duloxetine, and milnacipran are now approved for the pain of fibromyalgia.
Neuropathic pain significantly reduces the quality of life of multiple sclerosis patients. Current treatment strategies include antidepressants, anticonvulsants, and some other pain medications including cannabinoid drugs. Not only does the efficacy of these drugs vary between patients, they sometimes provide insufficient relief of pain with superimposed unwanted side effects (97).
Paroxysmal (nonpainful) disorders. Recurrent, brief, painless neurologic symptoms occur infrequently yet are treatable symptoms of multiple sclerosis. If the physician is unaware of these manifestations of multiple sclerosis, they can be misconstrued as functional. Symptoms often begin suddenly or subacutely and continue for weeks to months. Paroxysms usually last seconds but may occur several times a week to several times an hour. These disorders include tonic (dystonic) muscle spasms, diplopia, and convergence spasm; dysarthria, ataxia, and paresthesias; akinesia and motor impersistence; itching and paresthesias; and nausea and diarrhea (103; 86). Anticonvulsants are the mainstay for the treatment of entrenched paroxysmal symptoms (Table 5).
Pruritus. Intense itching can be problematic. Anecdotally, anticonvulsants, antidepressants (particularly mirtazapine), and antihistamines may benefit this condition.
Cognitive disorders. Between 40% and 65% of patients with multiple sclerosis have measurable cognitive disorders by neuropsychological testing. Cognitive impairment appears early in the course of multiple sclerosis, affecting over half (57%) of patients with clinically isolated syndromes (30). Interestingly, cognitive abnormalities were found in patients with spinal cord and optic nerve localizations for their symptoms. Finally, a small series of patients with “subclinical” multiple sclerosis shows cognitive impairments either at discovery or after a brief follow-up (43). Although cognitive impairment is common, it appears to change slowly, at least in treated patients (124). Only 5% to 7% of multiple sclerosis patients will display severe dementia (13).
It is critical that alternative and reversible causes of memory dysfunction be evaluated in all patients with multiple sclerosis. This includes both mood disorders and sleep pathology, as discussed in other sections of this article, particularly given the high prevalence of these confounders in patients with multiple sclerosis. Additionally, thyroid function tests and vitamin B12 should be examined.
Formal neuropsychological testing suggests that measures of information-processing speed (49), word list generation, and verbal memory (02) are the earliest markers of impairment. Correlation with gait impairment is poor, and cognitively impaired patients may appear otherwise relatively well. Although cognitive dysfunction is not usually severe, even mild impairments can greatly disturb people with high baseline ability.
Underemployment, social isolation, and greater need for assistance at home and in the community are experienced by cognitively impaired people. Few studies have characterized the types of cognitive deficits that patients with multiple sclerosis experience. Although it is commonly believed that most of the intellectual decline is subcortical, cortical demyelination can be severe. Subpial lesions found in the infoldings and sulci of the brain may be the cause of cognitive defects, particularly in patients with progressive multiple sclerosis (67). Numerous studies have now shown that cognitive impairment correlates with atrophy of deep and cortical gray matter and with axonal loss.
A number of batteries are available to diagnose cognitive decline. A practical 15-question survey, the MS Neuropsychological Screening Questionnaire, provides reasonable sensitivity for the detection of cognitive impairment when completed by a non-patient informant (09; 08).
A multicenter, randomized, double-blind clinical trial has not shown any benefit on memory for patients with multiple sclerosis treated with donepezil compared to placebo (66). Unfortunately, a study investigating whether memantine could benefit those with cognitive impairment was stopped early due to worsening of neurologic symptoms in those taking memantine at higher-than-recommended doses (146). Methylphenidate improves tests of attention in patients with multiple sclerosis with impaired attention (44), as it does in people with these deficits who do not have multiple sclerosis. A small double-blind, placebo-controlled, crossover study testing the efficacy of armodafinil in reducing cognitive problems in patients with multiple sclerosis revealed an improvement in delayed memory (15). The care partner/caregiver may be the most reliable observer when measuring response to therapy.
Pseudobulbar affect. Pseudobulbar affect is defined as an inappropriate emotion response, such as laughing or crying, to a particular situation. A large-scale, cross-sectional, point prevalence epidemiological study (PRISM or Pseudobulbar Affect Registry Series) revealed that pseudobulbar affect (as measured by the Center for Neurologic Studies Lability Scale or CNS-LS) occurs in approximately 40% of patients with multiple sclerosis (23; 29; 28; 58; 56; 57). Inappropriate or involuntary emotional responses such as laughing or crying can cause significant emotional distress, social isolation, and embarrassment. A fixed-dose combination of dextromethorphan and quinidine (20 mg/10 mg) reduced episodes of pseudobulbar affect by 49% over 12 weeks in a randomized, controlled, clinical trial (108) and was approved by the FDA in November 2010. This can occasionally be cost prohibitive to patients and, if this is the case, the prescription can be sent to a compounding pharmacy. Another medication that may provide benefit is fluvoxamine. In a small trial, emotional outbursts dropped considerably when patients took 100 mg fluvoxamine each evening (51). Pseudobulbar affect is underrecognized and underreported, so patients should be screened during office visits as it appears to be undertreated (108), especially considering the availability of an FDA-approved treatment.
Movement disorders and ataxia. There are numerous etiologies for movement disorders in multiple sclerosis. Some are iatrogenic, such as carbamazepine-induced dystonia and athetosis in patients with advanced multiple sclerosis, whereas others, such as restless legs syndrome, may be more prevalent in patients with multiple sclerosis than in the rest of the population. Even when they resemble treatable idiopathic conditions, movement disorders associated with multiple sclerosis generally respond poorly to treatment. Given that tremors are common within the multiple sclerosis population, it is important for neurologists to be able to determine the difference between essential tremor, resting tremor, and cerebellar tremor.
Treatment of essential tremor has more success, with gratifying outcomes using propranolol and other beta-adrenergic blockers, primidone, benzodiazepines, gabapentin, high-dose topiramate, and levetiracetam. Initial treatment may consist of either propranolol 40 mg twice daily or primidone 50 to 250 mg at night. Deep brain stimulation is effective in the treatment of essential tremors but is reserved for medical failures. Some drugs, including caffeine, beta-adrenergic agonists, selective serotonin reuptake inhibitors, excess thyroxin, clozapine, and lithium may induce an essential tremor that disappears when the drug is withdrawn or the dose is lowered.
There are case reports of success with deep brain stimulation in treating tremor in multiple sclerosis, and the FDA is currently considering the results of a National Institutes of Health (NIH)-funded trial of dual lead deep brain stimulation for Holmes tremor in multiple sclerosis. A resting tremor may be amenable to deep brain stimulation and a rubral or cerebellar tremor, is typically less responsive.
Cerebellar tremor (particularly of the head) due to multiple sclerosis may respond to vagal nerve stimulation (75). Tremors that are particularly prominent in a single plane can be ameliorated by botulinum toxin injections. Antihistamines and benzodiazepines are commonly used to treat unsteadiness but are rarely beneficial.
Other forms of tremor and dysmetria respond suboptimally to medications that are generally selected empirically. Acetazolamide, isoniazid, buspirone, carbamazepine, glutethimide, ondansetron, and levetiracetam have been reported to be useful in some, but not all, studies. Providers should be aware of the potential for a placebo effect with any medication and should not continue them without intermittent reassessment.
Transient ataxia may result from sudden discontinuation of selective serotonin uptake inhibitors and can be mistaken for an exacerbation. A systematic review of therapy for ataxia has failed to find any pharmacotherapy to be of benefit (88). Occupational and physical therapists can evaluate the need for adaptive equipment to help deal with ataxia and tremor.
Gait (walking) impairment. Gait dysfunction occurs in multiple sclerosis for a variety of reasons, including weakness, spasticity, and balance difficulties due to ataxia and sensory loss. Management of difficulty walking includes appropriate exercise to improve strength and assistance with mechanical devices as needed. Ankle-foot orthoses allow greater mobility, with decreased risk of falling and injury. For patients with significant imbalance, walkers may help with safety. Reducing fatigue and spasticity may also improve gait, although reduction of spasticity with pharmacotherapy may cause the clinical appearance of increased weakness. A few anecdotes and suggestions may be helpful to patients and providers:
(1) A supervised exercise regimen, especially if pushed to the individual’s limit, may improve exercise capacity, fatigue, and measurements of quality of life (80). Regular exercise may affect inflammation, appearing to raise resting concentrations of both TNF-alpha and IFN-gamma in patients with multiple sclerosis (17). This is usually best accomplished and sustained by small, incremental changes in one’s regular exercise habits. | |
(2) Weight loss to ideal body weight is desirable. Obesity in patients with multiple sclerosis is associated with higher relapse risk and disability progression (117). | |
(3) Stretching prior to activity and maximizing treatment of spasticity in appropriate patients may prevent falls. | |
(4) Balance therapy and gait training can improve coordination in some individuals. | |
(5) If the patient walks more comfortably behind a grocery cart, he or she is often a good candidate for a rolling walker. | |
(6) If hyperextension of the knee with walking cannot otherwise be treated, a long-leg brace should be considered. | |
(7) An ankle-foot orthosis is helpful in stabilizing patients with foot drop. Electrical devices that stimulate the peroneal nerve distal to the knee have been well-received by patients but are generally not reimbursed by third-party payers (some nonprofit organizations assist patients with funding). Functional electrical stimulation “produces a muscle contraction that lifts the foot during the swing phase of gait by electrically stimulating the common peroneal nerve via either surface or implanted electrodes” (87). | |
(8) One-story housing, appropriate seating, and placing safety bars in bathrooms will conserve energy and improve safety. |
A phase 3, placebo-controlled randomized clinical trial demonstrated improvement in walking speed and subjective walking assessments in 35% of patients with multiple sclerosis treated with dalfampridine ER, compared with 8% in placebo-treated patients (38). Because of some increased risk of seizures, subjects with abnormal EEG were excluded from the study. A second phase 3 trial demonstrated similar results, with 43% responders in those treated with dalfampridine ER versus 9% in those treated with placebo (37). In 2010, dalfampridine ER 10 mg every 12 hours was approved by the FDA as a treatment to improve walking in patients with multiple sclerosis. In 2012, a post-marketing trial failed to demonstrate the efficacy of lower dose dalfampridine ER (5 mg every 12 hours). In a subset of study participants, there was a statistically significant improvement in the distance walked for 6 minutes in those on standard dalfampridine ER 10 mg every 12 hours versus placebo (increase of 129 feet vs. increase in 42 feet, p = 0.014). There is some improvement in EDSS scores in patients with relapsing-remitting multiple sclerosis treated with this drug (150).
In addition, gait-specific symptomatic therapy is now available commercially and can also be obtained from a compounding pharmacy. It should be noted that compounded 4-aminopyridine (4-AP) has been used in multiple sclerosis practice for decades; however, compounding is not FDA-regulated and may be associated with risk of dosing errors. Furthermore, compounded 4-AP has a relatively short therapeutic duration of effect. Based on this experience, extended-release dalfampridine (dalfampridine ER), a twice-a-day, sustained-release form of 4-aminopyridine, was studied in patients with multiple sclerosis with walking impairments.
A pilot randomized controlled trial with 20 patients found an improvement in both walking and balance ability with a 12-week combined training intervention involving a resistance and aerobic regimen (39). This was also reflected in an improved quality of life with reduced depression and fatigue. This brings into mind the importance of neurologists considering both a pharmacologic and nonpharmacologic approach to the symptoms of multiple sclerosis.
A small study (n=14) using lower extremity resistance exercises over 8 weeks, combined with blood flow restriction to trigger ischemic repair mechanisms in the legs, saw an improvement in strength in individuals with advanced disability (EDSS 6–7) (71).
Comorbid psychiatric disease.
Depression and anxiety. Emotional distress occurs commonly in multiple sclerosis. A Canadian population-based study found major depression to be about 2.3 times more prevalent in persons with, than without, multiple sclerosis, affecting approximately 26% of patients between 18 and 45 years of age (106). The lifetime prevalence of major depression in multiple sclerosis appears to be about 50%, with higher rates for presence of some depressive symptoms. Those with left anterior temporal or parietal lesions by MRI scan may be at a slightly increased risk (129). Among male veterans with multiple sclerosis, risk factors for depression included high risk of falling, bowel impairment, absence of a marital partner, unemployment, and poverty (153). Depressed veterans were likely to utilize health care providers more frequently than non-depressed individuals. Although it has been difficult to establish, many experienced clinicians feel that interferon-beta therapy may bring out depressive symptoms in multiple sclerosis patients. Patients with multiple sclerosis have a higher incidence of bipolar disorder than the general population (121). There is evidence that interferon-gamma production by peripheral blood mononuclear cells falls with the treatment of depression (90), suggesting these drugs, or the depressed state, affect immunity. Newer studies suggest that multiple sclerosis–related psychiatric phenomenology is related to a disconnection syndrome, secondary to neurodegenerative damage plus diffuse inflammation (82).
A quick, simple screen developed for use in primary care has been validated in multiple sclerosis (91). It identifies 99% of patients meeting the criteria for a major depressive disorder. The test is not specific for major depression because 27% of those identified had a less severe form of depression. The screen consisted of two questions: (1) “During the past 2 weeks, have you often been bothered by feeling down, depressed, or hopeless?” (2) “During the past 2 weeks, have you often been bothered by little interest or pleasure in doing things?”
Antidepressants may even be used to address multiple symptomatic complaints by taking advantage of their side effects. Discontinuation of antidepressants depends on the severity of the depression and the residual symptoms. In general, planned treatment discontinuation may begin as early as 6 months, but longer periods of therapy are associated with a lower recurrence rate (72).
Antidepressant treatment may prevent loss of hippocampal cells in patients with recurrent depression (128), and their stimulation of neurogenesis may be crucial to the treatment of depression (120). These observations suggest that the use of antidepressants may be warranted for extended periods in patients with recurrent depression.
Drugs blocking the reuptake of both 5-HT and NE (SNRIs) produce a high rate of treatment response for depression and anxiety, generally showing a slight superiority to drugs that block only 5-HT (SSRIs) uptake for patients with moderate to severe depression. However, they also have more side effects including nausea, constipation, fatigue, insomnia, sexual dysfunction, night sweats, dry mouth, erectile dysfunction, and activation of hepatic metabolism systems. Unlike SSRIs, SNRIs are helpful in relieving pain (Table 8). 5-HT and NE reuptake inhibitors do so with the following relative potencies – the higher the number, the higher affinity for the transporter (5-HT:NE): milnacipran (2:1), duloxetine (9:1), venlafaxine (30:1) (134). Of these, only venlafaxine, due to its affinity for the dopamine transporter, can cause hypertension. Patients using antidepressants that inhibit the reuptake of serotonin concomitantly with nonsteroidal anti-inflammatory drugs can increase upper gastrointestinal bleeding by 12-fold (69).
Energizing antidepressants | Comment |
Fluoxetine (10 to 40 mg) | May benefit the course of multiple sclerosis. |
Venlafaxine (37.5 to 225 mg) | May aggravate hypertension. |
Desvenlafaxine (50 to 100 mg) | R-enantiomer of venlafaxine. |
Bupropion (100 to 400 mg) | May aggravate seizures; spares sexual function. Sometimes combined with SSRI. |
Analgesic antidepressants | |
Amitriptyline (50 to 150 mg for pain; up to 300 mg for depression) | Moderate anticholinergic effects. Weight gain problematic. |
Desipramine (100 to 200 mg) | Tricyclic with mild anticholinergic properties. |
Duloxetine (20 to 60 mg, once or twice daily) | |
Sedating antidepressants | |
Trazodone (50 to 300 mg) | |
Antidepressants used in special circumstances | |
Mirtazapine (7.5 to 30 mg) | Possibly useful in tremor and nausea; spares libido. Has mixed, unique MOA. |
Imipramine (25 to 75 mg, at bedtime) | Useful for headache and nocturia. |
Anxiolytic antidepressants | |
Sertraline (25 to 100 mg, daily) | |
Paroxetine (20 to 60 mg, daily) | May be more sedating. |
Citalopram (20 to 60 mg, daily) | Does not induce liver enzymes. May be more sedating. |
Escitalopram (10 to 20 mg, daily) | S-enantiomer of citalopram. |
Patients with resistant depression should be followed by a psychiatrist. Some people with refractory depression will respond to antipsychotics, mood stabilizers, thyroid hormone, or vagal nerve stimulation; the latter was approved by the FDA in 2005. People with bipolar disorders often require a mood stabilizer such as lithium, lamotrigine, or divalproex in addition to an antidepressant.
In patients willing and motivated to change behaviors, insight-oriented psychological counseling can treat depression. Psychotherapy and pharmacotherapy appear to be synergistic, producing more rapid and long-term results. Exercise is beneficial in improving depression in multiple sclerosis (107), while also helping patients become stronger and slimmer, improving cardiovascular fitness, reducing fatigue, increasing positive social interactions, and contributing to better bowel function.
The prevalence of anxiety in patients with multiple sclerosis is estimated to be up to almost 32%, with the prevalence of anxiety symptoms ranging up to 63%. The lifetime prevalence is estimated to be three times greater in patients with multiple sclerosis compared to the general population (130). As such, it is critical for neurologists to recognize this entity. As there have not been any controlled trials particularly looking at anxiety in multiple sclerosis patients, we can presume the pharmacologic management of anxiety in this population should mirror that of the general population. Typically, selective serotonin reuptake inhibitors and cognitive behavioral therapies are first-line agents. Serotonin-norepinephrine reuptake inhibitors can also be considered.
Combative or psychotic behavior. Psychotic symptoms are not common in multiple sclerosis, but those most commonly described in the multiple sclerosis population include hallucinations, delusions, agitation, blunted affect, and sleep disturbance. Psychosis is more commonly seen with an increased lesion burden in the medial temporal lobe (130).
Similar to patients with Alzheimer disease, these patients’ behavior can be modified with low doses of antipsychotic medication (24). The typical and atypical neuroleptics relieve symptoms to a similar degree, with the exception of clozapine, which appears uniquely efficacious. Atypical neuroleptics have significantly fewer side effects, especially in regard to movement disorders (53); however, they may induce obesity and arrhythmias. These drugs may be especially useful when patients develop steroid psychosis and occasionally in refractory anxiety and pain syndromes.
Aripiprazole | |
Extrapyramidal: 0 | |
Clozapine | |
Extrapyramidal: 0 | |
Olanzapine | |
Extrapyramidal: ± to + | |
Quetiapine | |
Extrapyramidal: ± | |
Risperidone | |
Extrapyramidal: ± to + | |
Ziprasidone | |
Extrapyramidal: ± to + | |
| |
Vitamin D deficiency. Research into the role of vitamin D in heart disease, chronic pain, multiple sclerosis progression, cognitive function, and depression highlights scientific interest in this vitamin. Although adequate vitamin D and calcium have long been thought necessary to bone health (see Osteoporosis section), they appear to be important in many aspects of health. Epidemiological studies suggest that a low intake of vitamin D may be a risk factor for multiple sclerosis (96). A serum 25-hydroxyvitamin D level below 20 ng/ml is considered a deficiency by many experts, but levels below 30 ng/ml may be inadequate for optimal health (50). There is no medical consensus on optimal levels for patients with multiple sclerosis. The Institute of Medicine suggested an upper limit of 4000 IU daily for most individuals (115). So far, there is little evidence to support the idea that vitamin D supplements reduce relapses in multiple sclerosis.
Osteoporosis. Osteoporosis may be defined clinically by a fracture from a low-impact trauma (due to a fall from a standing height or less) or fragility (no obvious trauma), or by a low bone mineral density. Clinicians should expect patients with multiple sclerosis to have osteoporosis, which seems to be linked to inflammation found in a number of chronic disease states and other factors mentioned below. Dual-energy x-ray absorptiometry (DEXA) is the current standard for assessing bone density. T scores are used in people over 50 and compare density to normal gender-matched young adults. Z scores are used for those under 50 (especially in premenopausal women) and are age- and sex-matched. A score less than or equal to -2.0 is of concern, although some experts would be concerned at a Z score below 1.0 (77). DEXA scans can be useful in following the efficacy of therapy for patients with bone loss. Because of the variability in measurements, the recommended interval is generally between 2 and 5 years, although this can be done more frequently in patients at high risk for fracture while on aggressive therapy. Patients with multiple sclerosis lose bone mass more rapidly and experience more fractures than age- and gender-matched controls. They also may have low levels of vitamin D, possibly due to low dietary intake and avoidance of the sun (21). Immobility causes loss of bone, and bed rest for 1-year results in loss of more than 10% of bone density. The use of glucocorticosteroids demineralizes bone. Continuous use of the older antiepileptic drugs phenytoin, phenobarbital, carbamazepine, or primidone has also been associated with diminished bone mineral density and is estimated to increase the risk of hip fracture by 29% over 5 years in women over the age of 65 years (26). Thyroid hormone excess is another cause of osteoporosis and is frequently iatrogenically induced and a thyroid-stimulating hormone test should be measured in all patients taking thyroid replacement.
Bone loss can be minimized by weight bearing exercise, cessation of smoking, avoidance of high alcohol intake, ingestion of 1500 mg of calcium (in three divided doses) and 600 to 800 IU of vitamin D daily for both men and women. Calcium carbonate is less expensive than calcium citrate but requires stomach acid for absorption. Patients taking gastric acid-inhibiting drugs should take calcium citrate. The absorption of some medications, such as levothyroxine, fluoroquinolones, or angiotensin-converting enzyme inhibitors, is inhibited by calcium and should be taken only when a 90-minute interval occurs between their combined use. Vitamin D supplementation may also improve muscle strength, and a meta-analysis has suggested it reduces falls in those at risk (12).
Common correctable causes of osteoporosis may be sought through relatively simple testing such as serum calcium and phosphorous; 24-hour urine calcium and, if elevated, parathyroid hormone level; liver function panel; creatinine; serum protein electrophoresis to exclude multiple myeloma; thyroid panel; and hormone levels (in men with multiple sclerosis this includes testosterone levels as they have an increased risk of hypogonadism) (47). Postmenopausal women not receiving hormone replacement are at increased risk for osteoporosis. In menopausal and postmenopausal women with multiple sclerosis, hormone replacement therapy may be indicated to prevent or reduce osteoporosis. There is no good evidence that estrogen adversely affects the disease process in multiple sclerosis (47).
Patients with T or Z scores below -2.0 or with scores below 1.5 and additional risk factors or previous vertebral or hip fracture should be treated with pharmacological intervention. When any of these conditions are encountered, bisphosphonate therapy can be undertaken using alendronate, risedronate, or ibandronate. Bisphosphonates inhibit bone resorption by reducing osteoclast activity. The first two come in sustained release formulations that can be given once weekly. Ibandronate can be taken once monthly. Patients must take these medications 30 to 60 minutes before the first morning meal with a full glass of water and remain erect for 30 minutes after taking them. They should not lie down until they have eaten breakfast. Bisphosphonates should not be used, or should be used cautiously, in patients with hypocalcemia, renal insufficiency, esophageal irritation, or trouble swallowing. Other treatments include raloxifene, nasal calcitonin, and teriparatide. The selective estrogen modulator raloxifene avoids some of the cardiac and breast cancer risks of estrogen. It is contraindicated in patients with a history of venous thromboembolic events. Nasal calcitonin is administered as one dose in alternating nostrils daily. It does not appear to be as potent as the other therapies and is generally considered second-line therapy. Teriparatide is a recombinant human parathyroid hormone analogue. It is the first anabolic drug approved for the treatment of severe osteoporosis. Although it is a potent drug, it must be given subcutaneously at a dose of 20 micrograms once daily and has significantly more side effects than the other compounds. It also is currently five to eight times more expensive than the other drugs.
The monoclonal antibody, denosumab, an inhibitor of the receptor activator of nuclear factor-κB ligand, improves low bone mass in postmenopausal women, offering another approach to treat osteoporosis (79).
Sialorrhea and dry mouth (xerostomia). Sialorrhea is rather rare in multiple sclerosis. It can be treated with a mouth rinse made of four drops of atropine ophthalmic solution in 30 ccs of water. The patient should rinse with but not swallow this solution. Botulinum, 80 units of toxin A or 1000 units of toxin B, can be injected into the submandibular and parotid glands on each side.
Dry mouth induced by medications is a more common problem and more difficult to treat. For mild symptoms, glycerin candies may be helpful. For more severe cases, artificial saliva such as Biotene or BioXtra may be helpful.
Visual problems. Many states have services for people with low vision, including large print books and tape recording of important materials at no cost. Several computer programs improve the contrast and size of print displays on monitor screens. All patients with chronic visual complaints should be referred to an ophthalmologist and possibly a low vision specialist.
Acquired primary gaze pendular nystagmus can be severely disabling due to the illusion of constant motion of the environment. Gabapentin will occasionally reduce nystagmus and improve visual acuity (06). Anecdotally, nystagmus responds to cannabinoids, baclofen, and memantine. Severe disabling nystagmus can be treated with retrobulbar injections of botulinum toxin, but induction of ptosis is a risk.
We just discussed the most frequent symptoms of multiple sclerosis and adequate symptomatic treatment, which may improve multiple sclerosis patients’ quality of life. Some severe and fortunately less common symptoms also deserve to be mentioned. The symptoms we discuss below usually occur in gravely disabled multiple sclerosis and may lead to their death. By knowing the causes of death of patients with multiple sclerosis, clinicians can take measures to prevent and treat them. In a series spanning 1972 to 1988, it was observed that despite normal longevity in the majority, 47% of patients with multiple sclerosis died of the direct complications of their disease, not counting suicide (118).
(1) Patients who are no longer ambulatory almost always have respiratory compromise (132). These patients may die as a result of restrictive lung disease resulting in hypercarbia and suppressed respiratory drive. They often become slowly more confused and somnolent as they retain carbon dioxide, which sometimes can be treated with nocturnal assisted breathing devices (BiPAP).
(2) The urinary tract, lungs, and decubitus ulcers all can be the source of infections that lead to death. Infection must always be considered as the cause of a sudden change in neurologic status in a patient with multiple sclerosis.
(3) Some patients die of pulmonary emboli secondary to deep vein thrombosis. Although the use of warfarin is problematic in this population, compression stockings, aspirin, and elevation of the legs may be helpful in preventing this complication of the disease.
(4) Falls resulting in hip fractures and subsequent surgery are especially pernicious for patients with advanced multiple sclerosis. Osteoporosis is a common, treatable problem in multiple sclerosis. To prevent falls, strength and balance training and the use of vitamin D (greater than 800 IU) and calcium (greater than 500 mg) supplements appear helpful (54).
(5) Suicide may account for up to 15% of all deaths of patients with multiple sclerosis (118). The relative risk of suicide is highest within the first 5 years of the diagnosis of multiple sclerosis, with about 50% of all suicides happening in that timeframe (130).
(6) Hypothermia (temperature less than 35 degrees Celsius) appears to be an ominous development in people with advanced multiple sclerosis. Such patients may have other signs of dysautonomia, particularly postural hypotension that precedes temperature regulation problems.
The goal of this report is to provide a convenient, practical, and timely reference to use in initiating therapies for the common symptoms of multiple sclerosis patients. These recommendations are not exhaustive.
As important as familiarity with pharmacotherapy is, it is worth little unless a therapeutic alliance exists between provider and patient. Concerned, careful, and nonjudgmental listening will increase the likelihood that most of the patient’s problems are addressed. This can only be done by setting aside adequate time to spend with patients, which is challenging in the current reimbursement environment. Physicians are not doing a good enough job in addressing the concerns of patients: it was found that for the six most common problems of patients with multiple sclerosis (ie, bladder dysfunction, fatigue, spasticity, pain, depression, and sexual dysfunction), only spasticity was treated in more than 40% of patients (36). To be a skilled listener, the physician must let the patient tell his or her story. However, being a skilled listener is not synonymous with being a passive listener. Many patients with multiple sclerosis have cognitive impairments that may make a concise history difficult to elicit. Careful listening also helps to establish a sense of trust that allows the patient to introduce critical, personal issues.
One attempts to use therapies with minimal safety concerns, good tolerability (fewer side effects), high efficacy, and minimal costs. Unfortunately, this ideal combination of features rarely exists, and new medications often deliver lower side effect profiles at a premium price. Many otherwise well-informed professionals have little knowledge of the costs of treatment. Costs are often concealed from healthcare providers by insurance drug plans that categorically separate drugs into generic and non-generic (brand) and because preferred therapy may differ among insurers based on factors such as rebates awarded by suppliers to payers that are unrelated to retail price.
The ultimate goal of the medical care of patients with multiple sclerosis should be to enhance quality of life, both by slowing the disease process (through disease-modifying therapies) and by managing or eliminating symptoms and thereby improving functionality. Multiple sclerosis management has transitioned from a model of reducing long-term complications and disguising symptoms to a model of enhancing functioning. As newer therapies emerge, it is important for the neurologist to help patients adapt to their limitations and to attempt to intervene strategically to minimize and control individual symptoms. Although a comprehensive review of systems is universally used to compile a problem list for each patient, targeted clinical history taking and questionnaires are increasingly being used to help focus the care of individual patients. Patient-reported outcomes (PROs) are considered reliable predictors of outcomes and prognosis, and, therefore, are being recorded as part of large international clinical trials.
Physicians must consult pharmacologic texts and package inserts for the various therapies. The large range of symptoms experienced by people with multiple sclerosis frequently results in the simultaneous use of numerous pharmacological therapies (polytherapy, polypharmacy). Understanding the pharmacologic effects of some medications, for example, of induction of liver enzymes plus the interdependent distribution and metabolism of combinations of therapies may be daunting. As the number of novel agents increases, it will become even more difficult to fully predict multiple interactions and to ascertain their clinical significance. Despite the emphasis placed on electronic prescribing, safeguards built into electronic medical records are not ideal and may be burdensome. Clinical pharmacists and case management programs through pharmaceutical distributors and third-party payers are crucial in easing this burden. Patients and their physicians often overlook the potential interactions poised by the significant use of complementary and herbal medications; this is why a full and complete medication list should be regularly reviewed. Although medications may be extremely useful in enhancing patients’ quality of life, ideally the fewest number of distinct medications should be used. The physician’s role is to help guide the patient in weighing the benefit versus risk of each symptom and its potential management. The goal of this report is not to encourage off-label use of FDA-approved medications, but rather to outline common prescribing practices that may have profound benefits to patients.
A strategic and comprehensive approach to managing multiple sclerosis symptoms is paramount to improving and enhancing the quality of life of multiple sclerosis patients. This often becomes the most time-intensive component of clinical encounters. In a survey done by Cofield and colleagues on the usage of marijuana in multiple sclerosis patients, most would favor legalization but are hesitant to discuss with health care providers (20).
The physician needs to become acquainted with the adverse effects and drug interactions of all of the drugs that are used in the patients he or she follows. It is also important to understand that symptomatic therapies for multiple sclerosis could impact the course of the disease.
|
Class of agent |
Agent |
Known effect |
Effect on MS |
MS Trial |
|
Alpha-2 adrenoreceptor agonist |
Clonidine |
Unclear | ||
|
Alpha-2 adrenoreceptor antagonist |
Yohimbine (pre), mirtazapine |
Inhibits the production of TNF |
Unclear | |
|
Alpha antagonist (postsynaptic) |
Prazosin |
Ameliorates EAE |
Possibly beneficial | |
|
Beta adrenoreceptor antagonist |
Propranolol |
Enhances the production of TNF |
Unclear | |
|
Beta-1 adrenoreceptor agonist |
Isoproterenol |
Inhibits the production of TNF |
Unclear | |
|
Beta-2 adrenoreceptor agonist |
Albuterol, salmeterol terbutaline |
Enhances IL-10 production. Terbutaline ameliorates EAE |
Possibly beneficial |
Report (61) |
|
Serotonin agonist |
Fluoxetine |
Inhibits LPS-induced TNF |
Unclear | |
|
Serotonin antagonist |
Cypro-heptadine |
Blocks effect of serotonin on LPS-induced TNF, but decreases EAE |
Unclear | |
|
Dopamine agonists |
Pramipexole |
Inhibits prolactin, ameliorates EAE |
Unclear | |
|
Prostaglandins inhibitors |
NSAIDs |
Ameliorates EAE |
Possibly beneficial | |
|
PGE-1 agonists |
Misoprostol, alprostadil |
Misoprostol ameliorates EAE |
Possibly beneficial | |
|
NO synthetase inhibitors/HMG-CoA reductase inhibitors |
Simvastatin, atorvastatin |
Ameliorates EAE; possibly reduces the MRI changes of MS |
Possibly beneficial, however, may inhibit benefits of interferon-beta |
+ Report (148) |
|
ACE inhibitors |
Captopril |
Decreases macrophage function, but increases PGE and decreases EAE |
Unclear | |
|
MMP inhibitors |
Minocycline |
Ameliorates EAE |
Beneficial |
+ Report in MinoCIS trial (85) |
|
Antiviral antibiotics |
Valacyclovir, acyclovir |
Unclear |
+ Report (70); however, not statistically significant in a randomized trial (33) | |
|
Glutamate antagonists NMDA |
Amantadine, anticonvulsants |
Unclear |
+ Report (109), consensus guidelines state that amantadine produces moderate improvement in subjective fatigue, concentration, memory, and problem solving when compared with placebo in multiple sclerosis (46) | |
|
Glutamine antagonists AMPA/kainate |
Ameliorates EAE |
Possibly beneficial | ||
|
PPAR-gamma ligand (anti-diabetic agent) |
Pioglitazone |
Ameliorates EAE |
Possibly beneficial |
Under study, + Report (100) |
|
PPAR-alpha ligand |
Gemfibrozil |
Possibly beneficial | ||
|
Sodium channel blockers |
Phenytoin gabapentin, topiramate, zonisamide |
Could increase intracellular calcium; but most have multiple actions |
Unclear |
Phenytoin under study as a neuro-protective agent |
|
Statins |
Anti-inflammatory |
Block IFN signaling—hi does danger with IFN Rx | ||
|
25-OH Vitamin D3 |
Vitamin D |
Interacts with dendritic cells |
Epidemiological evidence suggests reduced susceptibility to MS |
Meta-analysis showed no evidence of using vitamin D to prevent multiple sclerosis (27) but included one poorly done negative study |
|
Vitamin A/anti-acne |
Isotretinoin |
Interacts with dendritic cells. May down regulate TH17 cells and induce Treg cells. |
MS patients deficient in retinoid receptors, may enhance interferon-beta activity |
The prognosis of the symptoms described is not discussed. Failure to address some symptoms, however, can lead to marked increases in mortality, morbidity, and dramatic changes in quality of life.
Many of the non-pharmacological behavioral therapies cited can be continued throughout pregnancy. In almost all cases, pharmacological treatment of symptoms should be discontinued for at least one full menstrual cycle prior to attempting pregnancy. It is important to know the means of the various pregnancy categories, which appear in all package inserts:
|
A |
Well controlled human studies show no risk |
|
B |
Animal studies show no risk, but no human studies available or Animal studies show a risk, but well-controlled human studies fail to demonstrate a risk |
|
C |
Animal studies show a risk, but no human studies available or No animal or human studies available |
|
D |
Well controlled human studies show a risk, but the benefits of treatment may outweigh risk |
|
X |
Well controlled human studies show a risk and the benefits do not justify the risk |
Visit 1. A 40-year-old woman is being seen in neurology clinic. She was diagnosed with relapsing-remitting multiple sclerosis at the age of 32 and secondary progressive disease with superimposed relapses at the age of 38. She had taken an immunomodulator for 6 years beginning at the age of 34 years. At presentation, she complained primarily of imbalance, chronic headaches, and fatigue. Less problematic were insomnia, constipation, diminished sexual interest, and urinary urgency. Her past medical history was remarkable for depression and hypertension. Neurologic examination showed moderate weakness and spasticity of the right leg, mild sensory loss that involved both legs, and an unsteady gait producing an Expanded Disability Status Scale of 4.0.
When asked how the imbalance, headaches, and fatigue interfered with her life, the patient reported that she was too exhausted to both work and be a mother. As this was explored further by repeating her key complaints, the patient volunteered that she did not feel that she was a "worthwhile" person. She did not feel that she was firm enough with her 16-year-old daughter.
The most urgent and treatable problems were identified by the physician. Fatigue was the patient's most pressing problem, preventing effective social interactions. Her feeling of worthlessness was an important clue to a possible cause of her fatigue: depression. Because fatigue is often multifactorial, other types of lassitude were explored. The patient stated that she became tired and confused when she had multiple tasks to address, and she thought more slowly than she had a few years ago. She did not exercise. She did not have excessive daytime sleepiness, although she slept poorly, often worrying about maintaining her health long enough to provide for her children. Nocturia contributed to her insomnia because she got up twice a night. It appeared that the patient's fatigue had at least three components: (1) idiopathic lassitude, (2) depression, and (3) insomnia.
Urgency was a minor problem. A history documenting her urinary complaints was taken as follows:
Question: How often do you urinate during the day?
Answer: Nine to ten times
Question: What volume do you urinate?
Answer: The same as always, about a cup
Question: Does anything cause leakage of urine?
Answer: Sneezing causes wetting of underwear
Question: Do you feel you empty incompletely?
Answer: Yes
Question: Do you have difficulty starting or experience interrupted flow?
Answer: No
Question: Do you have bladder infections?
Answer: Fewer than one per year
Question: Were your children delivered vaginally?
Answer: Yes
Question: Other pelvic surgeries?
Answer: No
Question: Do you have symptoms of menopause?
Answer: No
The patient appeared to have a spastic bladder, but there was concern about the integrity of the pelvic floor related to the deliveries of her children.
Treatment. A parsimonious use of medications was initiated by grouping problems into syndromes. Fatigue, headache, insomnia, cognitive dysfunction, and unhappiness may have been aggravated by depression. Many treatment choices were possible, but bupropion SR 150 mg twice daily was chosen because it can be energizing and does not increase appetite or diminish libido. Behavioral therapies such as anticipatory resting and energy conservation were reviewed with the patient. She was asked to see a physical therapist to increase her exercise to help her strength and fatigue and prevent constipation, and the therapist was asked to assess her gait to see if bracing was indicated for her right ankle.
Oxybutynin 2.5 mg two to three times daily was begun, and the patient was asked to avoid caffeinated beverages. Urgency was also treated by adding the acid-neutralizing supplement calcium glycerophosphate and by timed voiding. Although acidifying the urine with vitamin C and cranberry juice may suppress bacterial growth, it may also make urgency worse.
To improve compliance, the patient was educated about expectations for treatment as well as potential side effects. Bupropion might aggravate insomnia and induce anxiety, and oxybutynin might aggravate constipation. As a precaution, she was told to increase her intake of fruits, cereals, and vegetables. She was advised to ask her primary care physician, who was monitoring her blood pressure, if switching her antihypertensive treatment, containing a thiazide diuretic and spironolactone, to another class of agent, might help her sexual dysfunction. Finally, she was asked to see a counselor, who advised her to ask her employer for reasonable accommodations at work.
Visit 2. The patient brought with her the medications she’d been taking. She understood the goals for her therapy. She felt less depressed but had concerns about her ability to relate to her daughter. Her energy continued to be less than she would have liked. Her headaches were unchanged. Bladder control was much better during the day, but she still experienced nocturia once or twice a night. The physical therapist did not feel that either an ankle foot orthosis or a peroneal functional stimulation device would benefit her gait but did suggest an exercise regime. Her supervisor at a large company was familiar with the American Disabilities Act. He allowed her to take two short breaks in the afternoon and to leave early 1 day per week.
The patient’s neurologic examination was unchanged. During this visit, spasticity, bladder management, headache, insomnia, and the possibility of counseling for her relationship with her daughter were reviewed. A detailed history of the patient’s spasticity was taken:
Question: Has spasticity gotten worse since your last visit?
Answer: No
Question: Are there tonic spasms or spontaneous contractions?
Answer: No
Question: What are the situations that make it worse?
Answer: Prolonged walking
Question: Does it interfere with hygiene or sex?
Answer: No
The patient's spasticity was relatively uncomplicated and may respond to medication alone. Baclofen was begun with a dose of 5 mg twice daily that was slowly increased to 10 mg three times daily. Fatigue was discussed as a side effect to baclofen.
Due to the possibility of an anatomic problem with the angle of the urethra, the patient was referred to a neuro-urologist. Because she had continued headache, imipramine 10 mg was started at bedtime with instructions to gradually increase the dose to 50 mg. This might also help her nocturia. As an additional treatment for nocturia, she was asked to reduce her fluid intake after 9 PM and empty her bladder at bedtime. She was told that she could stop the morning dose of oxybutynin because imipramine would have a persisting anticholinergic action in the morning.
Finally, because she described herself as spiritual, she was referred to a counselor at her church to help improve her relationship with her daughter.
Visit 3. The patient reported some successes at this visit but was irritated because most interventions were unsuccessful. The neuro-urologist assigned her Kegel exercises, found that she had an estrogen deficiency, and prescribed estrogen cream. All of these were helpful for bladder control. Her nocturia was much better as well.
However, baclofen made the patient groggy and weak, so she called the physician’s office, and tizanidine was prescribed. Tizanidine made her even sleepier. Spasticity was addressed with physical therapy to assist in stretching exercises and mild daily exercise. She took baclofen nightly to reduce spasticity when the side effect of fatigue and sleepiness was welcomed.
Although imipramine had helped her headache and nocturia, she was unhappy because she had gained 4 pounds in the previous 2 months.
Her daughter would not cooperate with the church-based counselor and responded with hostility to this approach.
Despite the difficulty of managing all of the patient’s symptoms, she understood that she could continue to work with her physician to maximize her symptom control. She felt that her feelings and concerns were validated, even when specific therapy was unsuccessful. She and her physician reviewed possible lifestyle modifications to assist her symptoms, such as stress management for headache, careful energy expenditure for fatigue with realistic expectations, and mild exercise to help develop stamina.
Treatment. The physician suggested the following:
Spasticity. For the present, no pharmacological therapy was given. Should the spasticity worsen, small doses of botulinum-A in appropriate leg muscles might help. The treatment to be prescribed for headache, topiramate, might also help with spasticity.
Fatigue. Methylphenidate 20 mg ER, up to 5 days out of 7 as needed, was prescribed. Arrangements were made to check the patient’s blood pressure in 2 weeks.
Weight gain and headache. Imipramine was discontinued. If nocturia recurred, she was told to call and hyoscyamine 0.375 mg could be instituted at night. She was treated with topiramate starting at 25 mg and increasing to 100 mg at night. First, it was established that she was not allergic to sulfa and had no history of kidney stones. Next, she was told that topiramate might produce some nausea and cognitive difficulties.
Neuropsychiatric. The patient was referred to a social worker or psychologist for counseling and possibly cognitive testing. Job- and family-related issues and degree of depression were to be addressed.
Much of the symptomatic care delivered by neurologists to patients with multiple sclerosis was anecdotally derived or suggested by relatively small open-label case reports or clinical trials that do not meet the rigor of level 1 evidence. However, two symptomatic medications, extended-release dalfampridine and fixed-dose dextromethorphan plus quinidine, which address different multiple sclerosis symptoms, were studied in patients with multiple sclerosis with specific symptoms (gait dysfunction and pseudobulbar affect, respectively). Where little evidence-based documentation exists, therapies discussed here reflect the authors’ biases and the biases found in expert opinion summaries such as this one. Data for this review were obtained using MEDLINE and Google Scholar searches using keywords multiple sclerosis, fatigue, spasticity, cognition, pain, and depression. Neurologic journals accessible to the authors were reviewed, and information from articles of interest was incorporated. Only articles written in English were utilized.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Anna Shah MD
Dr. Shah of The University of Colorado School of Medicine received consulting fees from Amgen, TG Therapeutics, and Merck/EMD Serono as an advisory board member.
See Profile
Anthony T Reder MD
Dr. Reder of the University of Chicago received honorariums from Biogen Idec, Genentech, Genzyme, and TG Therapeutics for service on advisory boards and as a consultant as well as stock options from NKMax America for advisory work and an unrestricted lab research grant from BMS.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Dec. 30, 2024
General Neurology
Dec. 28, 2024
Neuroimmunology
Dec. 20, 2024
Neuroimmunology
Dec. 20, 2024
Neuroimmunology
Dec. 12, 2024
Neuroimmunology
Dec. 07, 2024
Neuroimmunology
Nov. 27, 2024
Neuroimmunology
Oct. 23, 2024