
Epilepsy & Seizures
Tonic status epilepticus
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Seizures are the most common neurologic emergency in the neonatal period. Depending on etiology and whether seizure burden is high, seizures are associated with increased mortality and neurodevelopmental sequelae. Although seizure duration is typically brief in neonates, seizure burden can be very high. If the summed seizure duration is more than 50% of a given time epoch, it is considered neonatal status epilepticus. However, no consensus on its definition exists. Status epilepticus has been redefined by the International League Against Epilepsy, but this definition does not take the specificities of neonatal status epilepticus into account. A new ILAE task force has been created to define this in neonates.
|
• Neonatal status epilepticus is poorly defined, but the most commonly used definition by the American Clinical Neurophysiology Society defines it as a condition in which the summed seizure duration is more than 50% of a given time epoch. | |
|
• The etiologies of neonatal status epilepticus are similar to those of neonatal seizures and are most often acute provoked rather than part of an existing epilepsy syndrome. | |
|
• Around 15% to 30% of neonates with seizures have a period or periods of status epilepticus, but overall, the incidence is higher in neonates with hypoxic-ischemic encephalopathy and inborn errors of metabolism. | |
|
• Status epilepticus is nearly always electrographic-only and, thus, requires diagnosis with EEG. | |
|
• There is no evidence base for the treatment of neonatal status epilepticus and, consequently, current recommendations are similar to those for neonatal seizures. |
In contrast to older children and adults, the definition of status epilepticus in neonates is not well defined. The following three concepts are currently in use.
Scher proposed neonatal status epilepticus as continuous seizure activity for at least 30 minutes or recurrent seizures for 50% or more of the recording time (42). Based on the Scher definition, with some modifications of the time epoch, the American Clinical Neurophysiology Society (ACNS) defined neonatal status epilepticus as being present when the summed duration of electrographic seizures comprises more than 50% of an arbitrarily defined 1-hour epoch (49).
Pisani based his definition of neonatal status epilepticus on the definition used for older children: continuous seizure activity for at least 30 minutes or recurrent seizures lasting a total of 30 or more minutes without definite return to baseline mental or neurologic condition (34). However, the majority of neonates with seizures have some degree of encephalopathy and sedation, making a clear return to baseline difficult, or even impossible, to evaluate.
The International League Against Epilepsy (ILAE) published a new definition of status epilepticus independent of age: status epilepticus is a condition resulting from failure of mechanisms responsible for seizure termination or from initiation of mechanisms leading to abnormally prolonged seizures (time point T1), which can have long-term consequences (time point T2), including neuronal death, neuronal injury, and alteration of neuronal networks, depending on type and duration (48). The classification system consists of four axes, which provide a framework for diagnosis and treatment. The four axes are (1) semiology, (2) etiology, (3) electroencephalography, and (4) age. Although the fourth axis includes the neonatal period, there is little consensus concerning the definition points T1 and T2 for this age group, which makes this definition difficult to use.
There is animal evidence that the immature hippocampus is more resistant to status-induced injury than the mature hippocampus (24). At the same time, clinical data indicate that outcome after neonatal seizures is related to seizure burden; specifically, the risk of poor outcome increases above a seizure burden of more than 12 to 13 min/h, even after adjusting for other important contributors to outcome such as seizure cause and illness severity (31; 19; 33; 10; 06; 03). Furthermore, it has been suggested that there is a higher risk of status epilepticus if treatment is commenced more than 2 hours after seizure onset (27).
Most neonatal seizures have a duration of less than 5 minutes, although overall seizure burden may be high (46; 08). Abend and colleagues suggested that in the absence of more rigorously defined parameters, it is probably useful in clinical practice to regard seizures that last longer than 5 minutes as extended or prolonged and to define status epilepticus as seizures that last longer than 30 minutes when researching the effect of seizure burden on outcome (01).
In summary, in the absence of a generally adopted definition for neonatal status epilepticus, the ACNS definition is most applicable to clinical practice. Additionally, the ILAE neonatal taskforce is working on a new definition for neonatal status epilepticus.
Neonatal seizures in general and neonatal status epilepticus differ clinically from seizures in older children and adults due to immaturity of the brain. A classification of neonatal seizures has been published by the ILAE whereby seizures can be derived into electrographic-only (without clinical manifestations) and electroclinical (with clinical manifestations), and the latter into motor (automatisms, epileptic spams, clonic, myoclonic, sequential, tonic) and nonmotor (autonomic, behavioral arrest) (38). More than half of all neonatal seizures are electrographic-only. This is because the majority of neonates with seizures are critically ill and may be ventilated, sedated, and on muscle relaxation. In addition, treatment of seizures with phenobarbital or phenytoin will induce uncoupling, which means that electroclinical seizures become electrographic-only. Furthermore, neonatal seizures may be difficult to accurately diagnose because movements in sick babies can be misinterpreted and treated as seizures (22). For these reasons, EEG or aEEG is needed for the diagnosis of neonatal seizures and neonatal status epilepticus, as well as for the monitoring of treatment effect (08; 32; 38). A scoping review done by the ILAE neonatal task force found that there is substantial variation in the definition of neonatal status epilepticus throughout the literature without a unified definition (26).
The clinical presentation of neonatal status epilepticus has not been specifically evaluated, but it is likely that the initial presentation is similar to that of neonatal seizures (09; 34; 13). However, seizures tend to become electrographic-only with treatment, a phenomenon named uncoupling (09; 41). Uncoupling has been described after the use of phenobarbital and phenytoin, both of which are regularly used as first- and second-line antiseizure medications in neonates. Consequently, EEG is also required for the monitoring of treatment response in the management of neonatal status epilepticus. The review done by the ILAE did not find evidence to support that 30 minutes was more likely to be associated with pharmacoresistance or be associated with worse outcomes (26).
The occurrence of neonatal seizures is associated with a high risk of adverse neurologic sequelae, and in general, the prognosis of the seizures depends on the underlying etiology. Outcome tends to be worse after proven brain injury, such as hypoxic-ischemic encephalopathy or vascular brain insult, but also with cortical malformations or brain injury due to inborn errors of metabolism.
Regardless of the etiology, there is also evidence that high seizure burden, and status epilepticus in particular, is associated with poor prognosis (34; 30; 12; 19; 33; 10; 36; 13). A seizure burden of more than 12 to 13 per hour was associated with worse outcome compared to neonates with a lower seizure burden (31; 19). Neonates who experienced at least one episode of status epilepticus are at a higher risk of severe neurologic disability and post-neonatal epilepsy compared to neonates with isolated, recurrent seizures (34). A systemic review reported that the incidence of postneonatal epilepsy was 5% to 84%. It found that the incident of cerebral palsy was 9% to 78%, intellectual disability was 24% to 67%, developmental delay was 10% to 67%, and mortality was 1% to 62% (52). Another study found that neonates with seizure and a family history of epilepsy, abnormal neurologic examination at discharge, and at least two antiseizure medications at discharge should be monitored closely for epilepsy (04).
An infant was born at term via emergency cesarean section for prolonged stage 2 of labor and abnormal fetal heart tracing. Pregnancy was complicated by gestational diabetes. He required resuscitation, with APGAR scores of 4, 5, and 8 and cord pH of 7.1, but then stabilized. He did not meet criteria for cooling but was admitted to the NICU for observation. He required intravenous glucose for recurrent mild to moderate hypoglycemia. On day 2, he presented with an onset of clonic seizures of his right arm. An EEG confirmed that these events were focal seizures over the left central region.
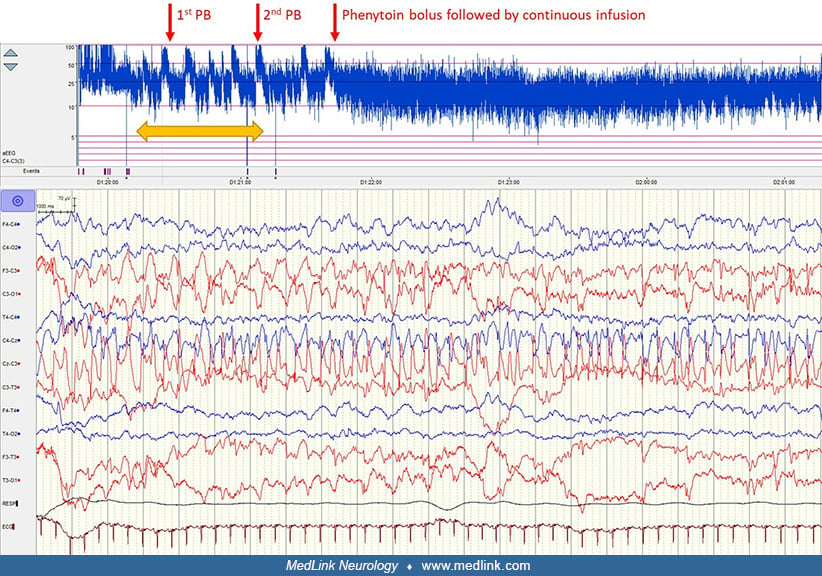
Onset of electroclinical seizures on day 2 with clonic seizures of the right arm. An EEG shows increasing seizure burden and period of status epilepticus (yellow arrow). Treatment (red arrows) with second dose of phenobarbital ...
After the first dose of phenobarbital, the seizures became electrographic-only (uncoupling). Over the next hour, there was an increase of electrographic seizure burden in keeping with status epilepticus. Treatment with a second dose of phenobarbital reduced seizure burden, but only the addition of phenytoin stopped the seizures. Maintenance treatment of both phenobarbital and phenytoin was continued for 3 days and then successfully tapered over a period of 3 days. An initial ultrasound of the head focal showed increased echogenicity in the left hemisphere. An MRI on day 7 confirmed an ischemic stroke of the left middle cerebral artery.
Neonatal seizures are of focal, lateralized, or multifocal onset because of immature neuronal networks. In some conditions, seizures may rapidly engage bilaterally distributed networks, such as spasms or myoclonic seizures (38). Consistent focal seizures indicate a focal brain injury, such as ischemic stroke or focal cortical malformation, whereas multifocal seizures are more likely due to a diffuse or global pathology, such as hypoxic-ischemic encephalopathy, meningitis, or a metabolic disorder. The onset of most neonatal seizures is from the central, temporal, or vertex regions (46; 17). However, the location of onset changes with gestational age. The central region onset predominated in neonates with a postmenstrual age (PMA) of at least 32 weeks, whereas occipital onset predominated in more premature infants; frontal onset is typically not seen before 28 to 30 weeks PMA (17).
The etiologies of neonatal status epilepticus are similar to those of neonatal seizures in general (Table 1) (34; 13) and are somewhat different in low- to middle-income countries compared to high-income countries (32; 51).
|
Acute provoked/Symptomatic | |
|
Etiology |
Specific conditions |
|
Acute neonatal encephalopathy |
Classic hypoxic-ischemic encephalopathy, antenatal and postnatal hypoxic events |
|
Vascular |
Arterial ischemic stroke, sinovenous thrombosis, subdural hemorrhage, subarachnoid hemorrhage, intraventricular hemorrhage, intraparenchymal hemorrhage, Vein of Galen malformation, giant arteriovenous malformation |
|
Infections |
Sepsis, meningitis, encephalitis, abscess |
|
Acute metabolic disorders |
Hypoglycemia, hyponatremia, hypernatremia, hypocalcemia, hypomagnesemia |
|
Head trauma |
Intrapartum, nonaccidental, accidental |
|
Toxic |
Intoxication, withdrawal seizures |
|
Other |
Extracorporeal membrane oxygenation, congenital heart disease, hypertensive encephalopathy |
|
Epilepsies with onset in the neonatal period | |
|
Etiology |
Specific conditions |
|
Cerebral dysgenesis |
Focal dysplasia, heterotopia, lissencephaly, hemimegalencephaly, polymicrogyria, schizencephaly |
|
Neurocutaneous syndromes |
Tuberous sclerosis, Sturge-Weber syndrome, linear sebaceous (epidermal nevus), incontinentia pigmenti, hypomelanosis of Ito |
|
Chronic infections |
TORCH** syndromes, congenital Zika virus syndrome |
|
Inborn error of metabolism |
Pyridoxine-dependent epilepsy, pyridoxal phosphate dependency, biotinidase deficiency, nonketotic hyperglycinemia, urea cycle defects, organic acidemias, molybdenum cofactor deficiency, maple syrup urine disease, glucose transporter 1 deficiency, and others |
|
Functional genetic epilepsies |
Channelopathies (eg, KCNQ2*, KCNQ3, SCN2A*, KCNT1), cell signaling disorders (CDKL5, BRAT1), synaptic transmission disorders (STXBP1) |
|
| |
In the majority of cases, the seizures are acute provoked (acute symptomatic) rather than an exacerbation of a defined electroclinical syndrome. Remote symptomatic status (known history if previous insult, such as posttraumatic) is unlikely in neonates due to the timeframe these usually occur. The most common etiology in term infants is hypoxic-ischemic encephalopathy followed by vascular causes (34; 13). In a case series of 91 neonates with seizures, only an abnormal neuro status and hypoglycemia were independent predictive factors for status epilepticus (13).
Neonates undergoing cardiac surgery have a higher incidence of status epilepticus compared to other etiologies, particularly those undergoing cardiopulmonary bypass surgery (11; 01; 25). Of the epilepsy syndromes with onset in the neonatal period, inborn errors of metabolism and some of the larger cortical malformations are more likely to present with status epilepticus. Although status epilepticus has been described in self-lining epilepsies, it is very rare, whereas seizure burden can be very high in the genetic early infantile developmental and epileptic encephalopathies.
Seizures occur more frequently in the neonatal period than at any other time in life due to age-specific, developmental factors that increase susceptibility to seizures and epilepsy as well as a high incidence of insults, such as hypoxia-ischemia or vascular events.
The immature brain has an increased neuronal excitability due to a number of factors (18):
|
• Glutamate signaling: increased receptor expression of excitatory glutamate receptors (AMPA, NMDA), with age-specific subunit composition | |
|
• GABA signaling: delayed development of efficient inhibitory mechanisms of the GABA system with overexpression of KCC2 (Na–K–Cl cotransporter), resulting in GABA-mediated depolarization in contrast to hyperpolarization in mature neurons. The maturation of the GABA signaling systems is site dependent (hippocampus before substantia nigra) and varies according to sex (earlier in female animals compared to male) (24). In fact, it is still unknown when these switches happen in humans. | |
|
• Channel expression: reduced GABA receptor expression with age-specific subunit composition |
Dendritic arborization, connections, and synaptic stabilizations are incomplete due to immaturity, and myelination is immature; this results in reduced spread of discharges and absence of generalization of seizures.
Seizures are the most common neurologic emergency in the neonatal period, with an incidence in term infants of 2 to 3 per 1000 live births (40). In preterm infants, the incidence is higher; up to 50 in 1000 live births may develop seizures (21). The incidence of status epilepticus in neonates is less clear and depends on the definition used (01). Using the most common definition (summed duration of electrographic seizure activity exceeding 50% of a given epoch), 15% to 43% of neonates experiencing seizures will experience a period of status epilepticus (23; 46; 29; 12).
The risk is higher with certain comorbidities, particularly neonates with congenital cardiac defects undergoing cardiac surgery and neonates requiring extracorporeal membrane oxygenation support (11; 01; 25; 20). Certain genetic etiologies (eg, KCNQ2 DEE) and inborn errors of metabolism often present with status epilepticus.
Status epilepticus is probably less common in preterm infants, which is in line with the finding that seizure duration is significantly shorter when compared to term infants (17), but there are no epidemiolocal studies.
Neonatal seizures must be differentiated from nonepileptic behaviors of the newborn (Table 2).
|
Nonepileptic “events” |
Manifestations |
Comorbidity |
|
Jitteriness and tremor |
Tremors, stimulus induced |
Often seen in mild hypoxic-ischemic encephalopathy and neonatal abstinence syndrome |
|
Bilateral tonic posturing |
Bilateral tonic extension of the arms and legs triggered by external stimulation; can usually be terminated by holding the limb |
Severe cortical brain damage, mostly perinatal |
|
Motor automatisms |
Repetitive stereotypic movements of limbs |
Often seen in mild hypoxic-ischemic encephalopathy and neonatal abstinence syndrome |
|
Apnea |
Oxygen desaturation |
May be seen in preterm infants, Undine syndrome, etc. |
|
Dystonic and tonic posturing |
Generalized or bilateral tonic or dystonic posturing of the limbs and trunk |
Neurologic disorders, gastroesophageal reflux (Sandifer syndrome) |
|
Benign neonatal sleep myoclonus |
Myoclonic jerks only during sleep in otherwise healthy infants |
None |
|
REM sleep behavior |
Smiling, grimacing, rhythmic eyelid twitching |
None |
|
Hyperekplexia |
Excessive reflexes, tonic spasms |
Genetic |
EEG is an essential tool in the diagnosis of neonatal seizures because nonseizure behaviors are often similar to ictal manifestations and cannot be reliably differentiated form other normal or abnormal behaviors. In addition, 50% to 70% of all seizures in the neonatal period are electrographic-only and can only be detected with EEG or aEEG monitoring (08).
Most neonatal seizures and neonatal status epilepticus are acute provoked or acute symptomatic. They are the response to an acute brain injury, most commonly hypoxic-ischemic encephalopathy (neonatal encephalopathy) and vascular insults (ischemic stroke, hemorrhage, etc.), but also to injuries due to cerebral infections and acute metabolic disturbances. Seizures as the first manifestation of an epilepsy syndrome are less common and represent only 10% to 20% of all neonatal cases with seizures (47). Overall, neonates with acute provoked seizures are at a higher risk of status epilepticus then neonates with early-onset epilepsy. According to the U.S. Neonatal Seizure Registry, 6 of 79 (8%) neonates with epilepsy presented with status epilepticus, in contrast to 85 of 532 (16%) neonates with acute provoked seizures (47).
The ILAE Task Force on Nosology and Definition proposed new terminology for epilepsy syndromes according to age of onset (56). Syndromes with onset in the neonatal and infantile period include the following (56):
|
• self-limited (familial) neonatal epilepsy | |
|
• self-limited (familial) neonatal-infantile epilepsy | |
|
• early infantile developmental and epileptic encephalopathies, which subsumes the former early myoclonic epilepsy and early infantile epileptic encephalopathy or Ohtahara syndrome | |
|
• epilepsy of infancy with migrating focal seizures |
In addition, a number of specific etiology syndromes are recognized (56):
|
• KCNQ2: developmental and epileptic encephalopathy | |
|
• early-onset vitamin-dependent (pyridoxine-dependent epilepsy and pyridoxamine 5’phosphate deficiency) | |
|
• CDKL5: developmental and epileptic encephalopathy |
As in all medical emergencies, the initial step in evaluating neonatal status epilepticus is to address the infant’s immediate medical needs (eg, airway, breathing, circulation). If the infant is stable, the initial diagnostic workup should concentrate on the common etiologies requiring prompt specific treatment. Family history, pre- and perinatal history, and a thorough physical examination with routine lab tests are standard clinical steps when evaluating suspected neonatal seizures.
Include lactate reading on blood gas; CRP: C-reactive protein; U&E: urea and electrolytes; LFTs: liver function tests; CSF: cerebrospinal fluid; PCR: polymerase chain reaction test; CT: computed tomography; MRI: magnetic re...
Seizures and, even more so, status epilepticus in neonates require confirmation with EEG or aEEG whenever possible because clinical diagnosis is unreliable, and a high proportion of seizures are electrographic-only (01; 08). The proportion of electrographic-only seizures increases after administration of antiseizure medication due to uncoupling (41). Conventional or full EEG is the gold standard for accurate neonatal seizure detection (45; 32; 38). The preferred setup is a polygraphic recording, including EEG, respiration, ECG, and one to two surface muscle channels. The American Clinical Neurophysiology Society recommends 24 hours of continuous EEG monitoring in all high-risk neonates (hypoxic-ischemic encephalopathy II to III; cerebral vascular insult, eg, perinatal arterial ischemic stroke, cerebral venous sinus thrombus, large intraventricular hemorrhage; cerebral infection; inborn error of metabolism; brain trauma; and congenital brain malformation). Using EEG as a screening tool in high-risk neonates rather than only for confirmation once clinical seizures are established is associated with worse treatment success (55).
Amplitude-integrated EEG (aEEG) may be used if no EEG is available. It is a bedside quantitative EEG technique that has the advantage of being more widely available and timesaving, and it requires no extensive expert training. In the majority of cases, aEEG will identify whether a neonate has seizures or not but is less sensitive for individual seizure detection and evaluation of seizure burden (39). Seizures that are short, of low amplitude, or are outside the centrotemporal region are often missed. Use of two aEEG channels, a combination with EEG raw channels, or other quantitative EEG trends will improve detection rate.
Neuroimaging is part of the routine investigation of seizures to detect structural etiologies, such as hemorrhage, infarction, and cortical malformations, but also to evaluate the extent of brain damage after hypoxic-ischemic encephalopathy and other insults. A brain ultrasound should be done within the first 1 to 2 days in all neonates with seizures. MRI (or CT if MRI is not available) is ideally done after 7 days, or later if the infant is not stable.
The aims of treatment are as follows:
|
• Treatment of the underlying cause to stop seizures promptly and effectively. This is typically only effective in acute metabolic causes, such as hypoglycemia or acute electrolyte disturbances. | |
|
• Acute pharmacological treatment of ongoing status epilepticus. Status epilepticus, even if electrographic only, should always be considered a medical emergency, and treatment needs to be initiated as soon as possible. | |
|
• Prevention of recurrence of seizures or status epilepticus. As most seizures in the neonatal period are acute provoked seizures, maintenance treatment should only be for a few days, and antiseizure medication should be tapered before discharge. Treatment beyond the neonatal period does not reduce the risk of later epilepsy nor improve neurodevelopmental outcome. Prolonged antiseizure treatment is indicated if seizures continue despite treatment or if seizures reappear after withdrawal. |
Guidelines for the management of neonatal seizures lack evidence base due to the lack of randomized controlled trials (07; 54; 37). There is even less evidence for the treatment of status epilepticus in neonates (02). Phenobarbitone is used worldwide as a first-line medication, and a high-quality randomized controlled trial with EEG has shown that it is effective in up to 70% of neonates (43). In addition, a systematic review of levetiracetam indicated that it is effective in only 45% of neonates (15); therefore, it is not recommended as a first-line medication. The choice of second-line medication is controversial and includes phenytoin, levetiracetam, midazolam, or lidocaine for most etiologies of seizure (37). If a channelopathy is suspected based on the clinical history or EEG, then a sodium channel blocker should be used. In a neonate with known or suspected cardiac disorder, than levetiracetam may be preferred (37). Levetiracetam has a more favorable pharmacokinetic and safety profile, but it has been suggested that it is less effective in neonates with hypoxic-ischemic encephalopathy or vascular insults (15). Consequently, many centers prefer phenytoin or benzodiazepines, although there are no randomized studies with sufficient numbers comparing second-line medications. The timing of treatment is important. There is evidence for a significantly lower seizure burden and fewer seizures in the infants treated with antiseizure medication within 1 hour of seizure onset (27).
Table 3 summarizes antiseizure medications currently being used for seizures and status epilepticus in neonates derived from the available literature and personal experience of the authors.
|
Medication |
Loading Dose |
Maintenance |
Common Adverse Effects |
Comments |
|
Phenobarbitone |
20 mg/kg IV Repeated with 10 to 20 mg/kg, as needed |
3-6 mg/kg/day IV or oral |
Respiratory depression, depressed consciousness, hypotension, hepatotoxicity (rare) |
Efficacy in 50% to 70% |
|
Phenytoin/Fosphenytoin |
20 mg/kg PE over 20 minutes |
4 to 8 mg/kg/day in two divided doses over 10 minutes |
Infusion site irritation (less with fosphenytoin), sedation Cardiac toxicity, particularly arrhythmias, hypotension, arrhythmia |
Efficacy in approximately 50% Target level 10 to 20 mcg/ml |
|
Levetiracetam |
40 mg/kg/day IV Second loading dose 20 mg/kg IV, if required |
40 to 60 mg/kg/day in three divided doses |
Mild sedation, irritability, adverse effect on behavior in older children, hepatotoxicity (rare) |
Efficacy in 20% to 45% Optimal dosing and target level not known |
|
Lidocaine |
2 mg/kg IV over 10 minutes |
7 mg/kg/hr for 4 hours, reduce to 3.5 mg/kg/hr for 12 hours, reduce to 1.75 mg/kg/hr for 12 hours, then stop |
Cardiac toxicity, particularly arrhythmias; sedation; hypotension; proconvulsive in high doses |
No randomized controlled trials, but retrospective studies show relatively good efficacy as second- and third-line drugs Adapt dose for postmenstrual age and therapeutic hypothermia |
|
Midazolam |
0.05 to 0.15 mg/kg |
60 mcg/kg/hour, titrated upward in steps to effect (maximal 300 mcg/kg/hour) |
Respiratory depression, depressed consciousness, hypotension, myoclonus in preterms |
No randomized controlled trials, but retrospective studies show relatively good efficacy as second- and third-line drugs |
|
Topiramate |
Do not load |
No dose-finding studies in neonates; studies used 5 to 10 mg/kg |
Necrotizing enterocolitis in neonates, irritability, feeding problems and weight loss, metabolic acidosis, neurotoxic (? dose dependent) |
Not recommended in the neonatal period No randomized controlled trials Doses of 50 mg/kg may be neurotoxic |
|
Bumetanide |
Unknown |
Recommended dosing as diuretic agents is 0.005 to 0.1 mg/kg/day Unclear as antiseizure agent; studies used 0.05 to 0.2 mg/kg |
Dehydration, hypotension, electrolyte disturbances, hearing loss |
Not recommended in the neonatal period No approved dosing for neonates |
Regardless of the choice of drug, there is evidence that early diagnosis and standardized treatment of seizures are associated with less progression to status epilepticus and shorten the time of hospital stay (14). Other studies have shown that implementation of a neurocritical care program with EEG monitoring leads to early treatment and improved seizure control, with overall decreased administration of seizure medication (53; 05; 55). Despite the medications listed in the table, there are few data on ketamine administration in neonates. A study by Jacobwitz and colleagues demonstrated that ketamine was associated with few adverse events, and seizures often improved after administration in neonatal status epilepticus (16).
Neonatal seizures in general, particularly neonatal status epilepticus, are associated with increased mortality and morbidity. Risk factors for adverse outcome include low birth weight (below 2.5 kg), low Apgar scores, abnormal neurologic examination at seizure onset, cerebral ultrasound abnormalities, failure to respond to antiseizure medication, and presence of neonatal status epilepticus. Adverse neurologic sequelae are seen in up to 80% of children with a history of neonatal seizures and are typically characterized by a variable combination of cerebral palsy, global developmental delay, and epilepsy (35). In a systematic review, postnatal epilepsy was found in 18% of neonates with seizure (35), whereas a multicenter study in neonates with acute provoked seizures described epilepsy at 2 years of age in 13% of children (44).
Status epilepticus is associated with a higher risk of mortality and a worse outcome compared to isolated or recurrent seizures (28; 13). This was even more marked in preterm infants.
Causes for adverse outcome are multifactorial, and there is no doubt that etiology and comorbidity of seizures plays a major role. However, there is now evidence that seizure burden also independently influences outcome. A high seizure burden of over 12 to 13 minutes per hour has been reported to be a significant risk factor for mortality and adverse short-term and long-term neurodevelopmental outcome (33).
Thus, identification of high seizure burden, and particularly status epilepticus, in neonates is important as it has implications for treatment and for prognosis (50).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Elissa G Yozawitz MD
Dr. Yozawitz of the Albert Einstein College of Medicine received consulting fees from IQVIA and advisory board honoraria from Sermo.
See ProfileRonit Pressler MD
Dr. Pressler of University College London, GOS Institute of Child Health received honorarium from Kephala and UCB as a consultant, from Autifony Therapeutics Limited and Longard for service on an advisory board, and from Natus for teaching.
See Profile
Solomon L Moshé MD
Dr. Moshé of Albert Einstein College of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jan. 20, 2025
Epilepsy & Seizures
Jan. 09, 2025
Epilepsy & Seizures
Jan. 09, 2025
Epilepsy & Seizures
Dec. 23, 2024
Epilepsy & Seizures
Dec. 19, 2024
Neurogenetic Disorders
Dec. 15, 2024
General Neurology
Dec. 14, 2024
General Child Neurology
Dec. 10, 2024