


General Neurology
Use of focused ultrasound in neurologic disorders
Jan. 13, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Bladder dysfunction is often a disabling manifestation of a variety of brain disorders, such as normal pressure hydrocephalus, dementia with Lewy bodies, vascular dementia, and frontotemporal dementia. Bladder dysfunction in brain disorders manifests with detrusor overactivity (urinary frequency, urgency, and urge incontinence). Spinal disorders, like trauma, infection, ischemia, hemorrhage, tumor, inflammation, and degeneration, produce capacity, hyperreflexic, and overactive bladder. Bladder dysfunction will also result from lesions of the conus medullaris, cauda equina, or peripheral nerves. Congenital Zika syndrome has been implicated in lower urinary tract dysfunction. A lower motor neuron type of urinary bladder manifests with an areflexic detrusor, a large hypotonic bladder, a tight and competent internal sphincter, and failure to empty. Acute cauda equina syndrome is often an emergency requiring urgent imaging and surgery. Clinical details, like a history of illness, physical examination, and pad count, along with urodynamic studies, help determine the optimum bladder treatment. Early treatment is essential to prevent renal damage and secondary bladder-wall changes, thus, improving long-term outcomes. Intradetrusor injections of onabotulinum toxin A have been found effective in improving bladder function and quality of life. Anti-Nogo-A antibodies augment neuronal sprouting, neuronal regeneration, and functional recovery. A review indicated that mirabegron, a β3-adrenoceptor agonist, is effective in neurogenic bladder unresponsive to antimuscarinic drugs. In a randomized trial, posterior tibial nerve stimulation improved all urodynamic parameters (bladder capacity and compliance, detrusor overactivity, maximum flow rate, and postvoid residual volume) in patients with multiple sclerosis compared to controls. Surgical treatment is indicated if all other forms of treatment, oral pharmacologic or intradetrusor injection, and intermittent catheterization fail. Bladder augmentation is the gold standard surgical procedure. The Artificial Urinary Sphincter, which is a prosthetic device, can restore bladder control and improve quality of life in patients with urinary incontinence caused by neurologic disorders. In this article, the author discusses various aspects of neurogenic bladder.
|
• Neurogenic bladder is a dysfunction of the lower urinary tract due to disease of the CNS or PNS involved in the control of micturition. | |
|
• A significant number of spinal cord injury patients have neurogenic bladder. | |
|
• Clinical manifestations of neurogenic bladder vary, depending on the level of neurologic involvement. | |
|
• Clinical details, along with urodynamic studies, help determine the possible causes of neurogenic bladder. | |
|
• Treatment is targeted to preserve renal function to keep patients continent, improve quality of life, and prevent urinary tract infection. | |
|
• Clean, intermittent self-catheterization is the best treatment for neurogenic bladder dysfunction. | |
|
• In addition, anticholinergics, antimuscarinic drugs, and botulinum toxin play an important role in the management. | |
|
• Surgical options are reserved for refractory neurogenic bladder. |
Neurogenic bladder is a dysfunction of the lower urinary tract due to diseases of the central nervous system or peripheral nervous system involved in the control of micturition. Hippocrates (c.460-370 BC) is credited with some of the first clinical descriptions of paralysis, bladder incontinence, and constipation related to spinal cord injury. In 1895, William Gowers (1845-1915) recognized three possible mechanisms of bladder dysfunction in acute myelopathy. First, he suggested that bladder dysfunction might result from spinal pathology. He observed the phenomenon of “retention of urine and subsequent overflow incontinence." Second, he noted that if lumbar enlargement was involved, the bladder was paralyzed, and urine flowed from the bladder as it entered. Finally, he explained that if the spinal cord is disconnected from higher centers, there is intermittent involuntary reflex bladder emptying (41).
During World War I, almost half of the patients with spinal cord injuries died from urinary tract infections or renal failure. In 1925, based on his experiments with cats, Frederick James Fitzmaurice Barrington (1884-1956) described Barrington nucleus or the pontine micturition center. This nucleus was thought to contain neurons that have an essential role in the control of bladder contraction (05). Bors and Comarr published a landmark textbook, Neurologic Urology, on the neurogenic bladder in 1971, which was then considered an authoritative work in the field (08).
Clean intermittent catheterization was first described in 1880 by William Frederick 60 (1834-1887) (60). In 1954 in England, Ludwig Guttmann (1899-1980) described a sterile non-touch technique of intermittent catheterization for the initial management of neurogenic bladder in spinal cord injury. Subsequently, Dr. Jack Lapides (1914-1995) at Michigan University, contributed extensively to the development of clean, intermittent catheterization. In 1927, DK Rose first introduced the cystometrograph. The term "urodynamics" was introduced by Dr. David M. Davis of Philadelphia, Pennsylvania in 1954.
Clinical manifestations of neurogenic bladder vary, depending on the site of neurologic involvement.
A lesion above the pontine micturition center leads to an uninhibited bladder due to loss of cortical control over the sacral reflex voiding centers. Impaired normal bladder inhibition results in detrusor overactivity during the filling phase. The common symptoms of detrusor overactivity include urinary frequency, urgency, and urge incontinence. The voiding phase is usually normal. Sphincters relax synergistically with detrusor contraction; thus, urinary bladder pressure remains normal.
A lesion between the pontine micturition center and sacral spinal cord (myelopathies of varying causes, including traumatic spinal cord injury) produces an upper motor neuron type of bladder. In upper motor neuron lesions, the urinary bladder is of small capacity, hyperreflexic, and overactive. The bladder fails to store. Voiding is obstructive due to detrusor-external sphincter dyssynergia. Prominent voiding symptoms include hesitancy, straining, slow and interrupted stream, or inability to void. Simultaneous detrusor and urinary sphincter contractions lead to an increased amount of residual urine and an increased risk of urinary infection and subsequent renal damage.
Bladder dysfunction will result from lesions of the conus medullaris, cauda equina, or peripheral nerves. Sacral cord or sacral nerve root injuries usually produce a lower motor neuron type of urinary bladder. A lower motor neuron type of urinary bladder manifests with an areflexic detrusor, a large hypotonic bladder, a tight and competent internal sphincter, and failure to empty (49).
Studies have indicated that people with spinal cord injuries are two to five times more likely to die than people without spinal cord injuries (66). One of the reasons for high mortality in these patients is that patients with a neurogenic bladder are at grave risk of developing serious renal complications. The most frequent medical and potentially serious complication in patients with neurogenic bladder dysfunction is urinary tract infection. Urinary tract infection may result in epididymo-orchitis, cystitis, and chronic pyelonephritis. Urinary tract infection may ultimately lead to renal failure.
Vesicoureteral reflux in patients with suprasacral spinal injuries is also responsible for transmitting urinary tract infections to the kidneys. Risk factors for urinary tract infection in patients with neurogenic bladder include bladder overdistention, high post-voiding residual urine, high-pressure voiding, bladder stones, and catheter use. Biofilm-causing microorganisms often responsible for urinary tract infection in these patients are Proteus, Pseudomonas, Klebsiella, Serratia, and Providencia species, along with enterococci and staphylococci (31).
Autonomic storm in spinal cord injuries (injury at levels above T-5-6) is a serious complication and a medical emergency that requires immediate attention. Noxious stimuli like urinary retention and bladder distension and constipation can activate an autonomic storm. It manifests with tachycardia, tachypnea, hyperpyrexia and severe hypertension, muscle overactivity, and profuse sweating. Patients with a neurogenic bladder are at risk for sexual dysfunction as well. Men with neurogenic bladder become infertile for several reasons, such as ejaculatory failure, impaired spermatogenesis, and poor semen quality (28).
Other kidney-damaging complications of neurogenic bladder include hydronephrosis and bladder stones. Compared to the general population, there is an exceptionally higher risk for patients with spinal cord injury developing bladder cancer. Complete destruction of the urethra is one of the long-term complications of continuous bladder catheterization in women with advanced neurogenic bladder. If left untreated or insufficiently treated, the high-pressure bladder may be destroyed by fibrotic changes in the musculature (28). Other long-term complications of neurogenic bladder are refractory urinary incontinence and urinary bladder malignancy (46).
Brain disorders. Bladder dysfunction is often a disabling manifestation of a variety of brain disorders. It tends to occur early in brain tumors, stroke, subdural hematoma, frontal lobe injury, and hydrocephalus. Lesions above the pontine micturition center usually produce voiding difficulties. Uninhibited sphincter relaxation in frontal lobe diseases may lead to urinary incontinence. Urinary incontinence is also associated with severe cognitive impairment in Alzheimer disease, Parkinson disease with dementia, dementia with Lewy bodies, vascular dementia, and frontotemporal dementia. Nocturia is the most common urinary complaint in more than 60% of patients with Parkinson disease. Urgency occurs in 33% to 54% of patients, and frequency is experienced by 16% to 36% of the patients. Detrusor overactivity is the commonest cystometric abnormality seen in patients with Parkinson disease. All patients with multiple system atrophy develop urinary disturbance. Both storage dysfunction manifestations (urgency, frequency, nocturia, incontinence) and voiding dysfunction manifestations (hesitancy, interrupted or poor stream, and double voiding) can be seen in these patients (65). The European MSA Study Group registry, which included consecutive patients with a clinical diagnosis of multiple system atrophy, revealed that symptomatic dysautonomia was present in almost all patients, and urinary dysfunction (83%) was more common than symptomatic orthostatic hypotension (75%) (40). Involvement of the pontine micturition center, sacral preganglionic nucleus, and Onuf nucleus is responsible for neurogenic bladder in patients with multiple system atrophy. Urinary dysfunctions in progressive supranuclear palsy patients are as extensive as those seen in multiple system atrophy (39). Stroke is another frequent cause of bladder dysfunction in neurologic practice. Approximately 70% of stroke patients have transient urinary incontinence after the acute stage is over (20). CSF shunt surgery in idiopathic normal pressure hydrocephalus helps improve lower urinary tract symptoms and storage dysfunction (04).
Spinal cord disorders. The spine is affected by several common and uncommon disorders, such as trauma, infection, ischemia, hemorrhage, tumor, inflammation, and degeneration. All of these diseases can lead to the occurrence of myelopathic manifestations of varying severity. A majority of patients with spinal cord involvement have neurogenic bladder. Multiple sclerosis causes neurogenic bladder dysfunction in approximately 50% to 90% of patients. Transverse myelitis is an acute spinal cord disorder resulting in paraplegia or quadriplegia, a sensory level below the level of the lesion, and autonomic (bladder, bowel, and sexual) impairment. Etiologies for transverse myelitis can be parainfectious, paraneoplastic, drug- or toxin-induced, systemic autoimmune disorders, and acquired demyelinating diseases (27).
Urinary and fecal incontinence is common in young adults with spina bifida (63). Most studies estimate spina bifida incidence to be between 2 and 12 per 10,000 live births (66). Bladder dysfunction in children with spina bifida is associated with a more severe congenital anomaly, such as myelomeningocele, sacral agenesis, intraspinal lipoma, lipomeningocele, a diastematomyelia, or a fatty filum terminale with tethering of the cord. Patients with spina bifida often manifest with storage or emptying bladder abnormalities. Several cutaneous abnormalities point toward possible spinal dysraphisms. A skin lesion can be a subcutaneous mass, dermal vascular malformation, tuft of skin hair, midline dimple or sinus tract, or asymmetric gluteal cleft (02; 21).
Cauda equina syndrome (S2-S4 involvement), in addition to lower motor neuron type of bladder involvement, is characterized by “saddle-shaped” sensory loss and areflexic paraplegia. Spinal arachnoiditis frequently affects the lumbosacral region. The arachnoid matter becomes thickened, scarred, and adherent to the pia and dura, obliterating meningeal blood vessels. Spinal arachnoiditis strangulate many lumbosacral nerve roots. Low back pain and urinary disturbances are early symptoms, followed by asymmetric leg weakness and sensory loss that extends into the saddle area. The cytomegalovirus cauda equina syndrome is a dramatic and serious infectious disorder occurring in patients with HIV infection. Approximately 40% of patients with lumbar disc disease have abnormal urodynamic testing, and an even larger proportion complain of voiding symptoms. The most common urodynamic finding is detrusor areflexia, but underactive or overactive detrusor can also be observed (59).
Peripheral nerve disorders. Diabetes is the commonest cause of polyneuropathy globally, and it is also the commonest polyneuropathy leading to bowel, bladder, and erectile dysfunction. Several other polyneuropathies can manifest with bladder dysfunction, such as Guillain-Barré syndrome, human immunodeficiency virus-associated neuropathy, alcoholic neuropathy, porphyric neuropathy, and amyloid neuropathy. Pelvic plexus injury following abdominal perineal resection and hysterectomy involves both parasympathetic and sympathetic nerve fibers supplying to the bladder and rectum and leads to dysfunction of these structures (11).
Urinary bladder neural control mechanism. The urinary bladder and other lower urinary tract structures are meant to store urine and allow emptying at an appropriate time and place. The urinary bladder and lower urinary tract structures are controlled by the central nervous system (brain and spinal cord). Peripheral nerves from both the autonomic nervous system and somatic nervous system supply the urinary bladder (58).
Brain. The micturition control center of the brain is located in the frontal lobe. This frontal lobe micturition center is primarily inhibitory; it inhibits bladder activity until there is an appropriate time and place to void.
Brainstem. The mechanical process of urination is coordinated by the pons. The pontine micturition center is located in the rostral pons. This pontine center coordinates the urethral sphincter relaxation and detrusor contraction to facilitate voiding.
Spinal cord. The spinal cord contains neuronal tracts between the pons and the sacral spinal cord. When the sacral cord receives sensory information from the bladder, this signal travels up the spinal cord to the pons and then ultimately to the brain. The brain interprets this signal and sends a reply via the pons that travels down the spinal cord to the sacral cord and, subsequently, to the bladder. The sacral 2 to 4 spinal segments are responsible for bladder contractions. Somatic motor fibers that supply to the external urethral sphincter arise in Onuf nucleus (located in sacral 2 to 4 spinal segments) and reach the urinary bladder through the pudendal nerves.
Peripheral nerves. The peripheral nervous mechanisms for urinary voiding and storage involve efferent and afferent signaling in pelvic (parasympathetic), hypogastric (sympathetic), and pudendal (somatic) nerves.
Sympathetic postganglionic nerves. Sympathetic input is mediated via the hypogastric nerve and originates from T10 to L2 segments of the spinal cord.
Parasympathetic postganglionic nerves. Parasympathetic input originates from S2 to S4 spinal segments.
Somatic cholinergic motor nerves. Somatic nerve supply to the urethral sphincter originates from the anterior horn of S2 to S4 (nucleus of Onuf) and travels via the pudendal nerve.
Storage phase. The normal urinary bladder in adults accommodates approximately 300 to 600 mL of urine. The need to void generates when urinary volume reaches around 400 mL. Urination can be withheld by voluntary contraction of the external urethral sphincter. The sympathetic nervous system inhibits the detrusor muscle through b-adrenergic receptors and causes sphincteric contraction; micturition reflex is inhibited. These mechanisms, thus, ensure continence.
Voiding phase. The cortical micturition center in the frontal lobe and cingulate gyri send inhibitory signals to the detrusor muscle to prevent the bladder from emptying until an appropriate occasion and place to empty the bladder is available. The conscious sensations associated with bladder activity are transmitted to the pons from the cerebral cortex. The pontine micturition center modulates the opposing activities of the parasympathetic and sympathetic nervous systems. The pontine micturition center sends excitatory signals to the sacral segments of the spinal cord that produce detrusor contraction while simultaneously sending inhibitory influence to the thoracolumbar cord that produces sphincter relaxation. Acetylcholine released by activation of parasympathetic neurons produces detrusor contraction and relaxation of the internal sphincter. Supraspinal voluntary signals have an excitatory effect on the somatic peripheral nerves and leads to opening of the external urethral sphincter. Simultaneous pelvic floor relaxation facilitates bladder emptying. During the bladder emptying phase, the cortical centers suppress the pontine micturition center, resulting in the reduction of sympathetic outflow with simultaneous enhancement of parasympathetic outflow to the lower urinary tract.
A significant number of patients with spinal cord injury have neurogenic bladder. According to the World Health Organization, every year around the world, between 250,000 and 500,000 people experience a spinal injury (67). A systematic review examined the incidence and prevalence of traumatic spinal cord injury in different countries worldwide. The global incidence of spinal cord injury varied from 8.0 to 246.0 cases per million inhabitants per year. The global prevalence varied from 236.0 to 1,298.0 per million population (22). In another epidemiological data analysis for 41 countries, the incidence of spinal cord injuries ranged from 3.6 to 195.4 patients per million globally (34). World Health Organization data suggest that the leading causes of nontraumatic spinal cord injury are neoplastic tumors and degenerative conditions of the spinal column, followed by vascular and autoimmune disorders. In many countries, like India, Peru, and Sweden, with a high incidence of tuberculosis and other infectious diseases, infective causes are dominantly responsible for nontraumatic spinal cord injury. The nontraumatic spinal cord injury incidence rate in Canada is estimated to be 68 per million. Australian data report an incidence of 26 per million (66). Medical and pharmacy claims were analyzed to characterize neurogenic bladder patients. There were 46,271 patients in the neurogenic bladder cohort and 9,315 and 4,168 patients in the multiple sclerosis and spinal cord injury cohorts, respectively. The mean age of neurogenic bladder patients was 62.5 years. A high frequency of lower urinary tract infections (29% to 36%), obstructive uropathies, and urinary retention were observed in these patients (43).
A meta-analysis, which included data from 189 articles (articles containing prevalence data), found the prevalence of neurogenic overactive bladder was 50.9% in patients with multiple sclerosis, 52.3% in those with spinal cord injury, 33.1% with Parkinson disease, and 23.6% with stroke (53).
Urinary urgency, frequency, and urgency incontinence are the most common symptoms, occurring in 37% to 99% of patients with multiple sclerosis. Voiding symptoms (hesitancy, feeling of incomplete bladder emptying, and urinary retention) are also common in this population, occurring in 34% to 79% of patients with multiple sclerosis (17). Parkinson disease studies report that storage symptoms are present in 57% to 83% of patients, whereas voiding symptoms are seen in 17% to 27% (65). In a large series, the incidence of urinary dysfunction in patients with multiple system atrophy was reported to be 83% (40). Approximately 15% of the patients with spinocerebellar ataxias can have lower urinary tract dysfunctions. Lower urinary tract dysfunctions can be seen in various types of spinocerebellar ataxias. Spinocerebellar ataxias should still be considered in patients with progressive cerebellar ataxia and urinary dysfunctions (32).
Congenital Zika syndrome is known to be associated with microcephaly and other central nervous system abnormalities. Congenital Zika syndrome has been implicated in lower urinary tract dysfunction. In a series, 22 congenital Zika syndrome patients were tested and found to have neurogenic bladder. Of the 22 patients, 21 had an overactive bladder. Increases in postvoid residual were noted in 40% of cases, whereas a urinary tract infection was noted in 23% of cases (14).
Up to 90% of spinal cord injuries are due to traumatic causes such as road traffic crashes, falls, and violence (67). Effective strategies should be strictly implemented to prevent spinal cord injuries. Prevention of nontraumatic spinal cord conditions (like spinal tuberculosis and vertebral malignancies) depends on the measures that are taken to improve public health and for effective control of disease. Folic acid supplementation has been shown to be an effective option that significantly reduces the risk of pregnancies affected by spina bifida or other neural tube defects (by around 50%) (66).
Patients often complain of straining in micturition, urinary incontinence, and a sensation of incomplete bladder emptying. Urinary retention and incomplete emptying can result from a number of non-neurologic causes. In a study of 122 patients who met the selection criteria for overactive bladder, detrusor overactivity was identified in 99 (79%) on urodynamics. The differential diagnoses that were identified in these patients were benign prostatic enlargement in 40 patients (32%), benign prostatic obstruction in 27 (22%), complications of prostate cancer treatment in 25 (20%), neurogenic bladder in 13 (11%), urethral stricture in seven (6%), idiopathic overactive bladder in six (5%), bladder stone in two (2%), bladder cancer in one (1%), and bladder diverticulum in one (1%) (07). The symptoms of benign prostatic hyperplasia are not just simple mechanical obstruction; the pathophysiology of this urologic disorder involves abnormalities of detrusor function, neuromuscular abnormalities of the prostatic urethra, and sensory abnormalities of the bladder wall (06).
Acute urinary retention is common in elderly men. Aging produces adverse changes in detrusor function that may result in a decrease of detrusor contractility. Multiple causative factors may be responsible for retention in old age. Three main mechanisms may be responsible: obstructive, neurogenic, and detrusor underactivity in isolation or in combination (61).
The differential diagnosis of bladder dysfunction in women is stress incontinence, pelvic organ prolapse, bladder outlet obstruction, neurogenic bladder, prior pelvic surgery, bladder cancer, and urethral diverticulum. The primary disorder of sphincter relaxation or Fowler syndrome is an important differential diagnosis of urinary retention in females. It is characterized by painless urinary retention, polycystic ovaries, high urethral closure pressure, an increase in sphincter volume, and abnormalities of striated urethral sphincter electromyography. Other commonly encountered female non-neurogenic lower urinary tract dysfunction includes overactive bladder, interstitial cystitis, and painful bladder syndrome. A complete gynecologic, urologic, and neurologic examination is needed while evaluating women with urinary bladder dysfunction (48).
Clinical details, like a history of illness, physical examination, and “pad count,” along with urodynamic studies help determine the possible causes of urinary incontinence, urinary frequency, hesitancy and urgency, incomplete emptying, urinary retention, and other neuro-urologic symptoms. It is recommended that patients should maintain a 72-hour voiding diary. A urinalysis to rule out urinary tract infection and hematuria should always be performed. Other laboratory evaluations that can be performed are urine culture and sensitivity, serum creatinine, and creatinine clearance.
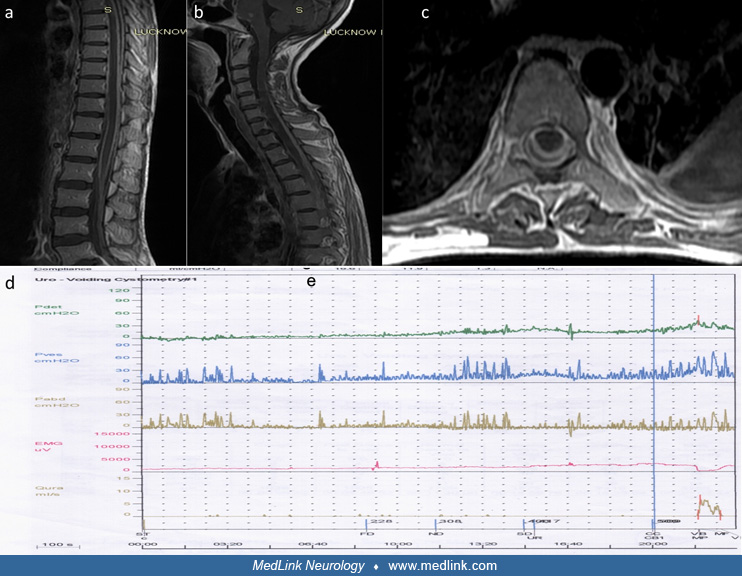
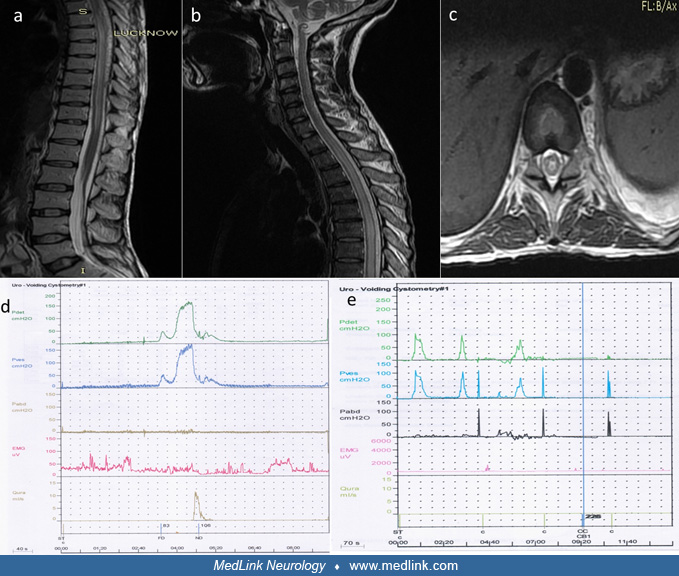
Urodynamics. Urodynamic studies evaluate the synchronicity of the bladder and urethral function for storing and voiding urine. Urodynamic assessment includes urinary flowmetry, postvoid residual urine volume, bladder cystometrogram, sphincter electromyography, Valsalva leak point pressure measurement, and urethral pressure profile (15).
Uroflowmetry. Uroflowmetry is a test to evaluate the voiding dysfunction. It assesses the volume of urine released, the speed at which it is released, and the length of the micturition. The patient is asked to void, and the volume of urine voided per unit time (ml/s) is noted. Low uroflow rate may reflect urethral obstruction, a weak detrusor, or a combination of both.
Post-void residual urine. The post-void residual urine assessment evaluates the volume of urine left in the bladder after urination is complete. If the post-void residual urine is high, the bladder may be acontractile, or the bladder outlet may be obstructed. Both of these conditions will cause urinary retention with overflow incontinence. Post-void residual urine volume involves transurethral catheterization to measure residual urine volume in the bladder immediately after voiding to determine the ability of the bladder to empty completely. Ultrasound is a noninvasive means of determining urine post-void residual volumes. Abnormal residual volumes are defined as volumes greater than 100 cc or greater than 20% of the voided volume. A residual urine volume over 100 cc carries a high risk of urinary infection.
Filling cystometrogram. A filling cystometrogram assesses the bladder capacity (the amount of fluid the bladder can hold), compliance (the pressure the bladder can withstand as it fills), and the presence of phasic detrusor contractions (causing patients to feel the urge to void). Bladder pressures are measured during filling and emptying by use of a transurethral catheter along with the measurement of intra-abdominal pressure.
Voiding cystometrogram. Voiding cystometrogram assesses bladder contractility and the extent of a bladder outlet obstruction. Pressure-flow studies simultaneously record the voiding detrusor pressure and the urinary flow rate.
Electromyography. Simultaneous electromyography is helps diagnose detrusor sphincter dyssynergia. Electromyography may provide information about denervation of the pelvic floor musculature or identify dyssynergia of the external urethral sphincter. Sphincter electromyography is performed using surface or needle electrodes.
Cystoscopy. Cystoscopy in patients with neurogenic bladder helps detect structural bladder lesions like bladder cancer and bladder stones. Cystoscopy should always be performed, particularly if the patient complains about hematuria.
Video-urodynamics. Video-urodynamic testing identifies anatomic and functional abnormalities of the urinary tract. Video-urodynamic testing combines the imaging findings of voiding cysto-urethrogram and multichannel urodynamics and effectively evaluates the lower urinary tract anatomy, such as vesicoureteral reflux and bladder diverticulum, as well as the functional pressure-flow relationship between the bladder and the urethra.
The principal objectives of treating neurogenic bladder are to preserve renal function, prevent damage of the upper urinary tract, keep the patient dry and continent, improve quality of life, and prevent lower urinary tract infections (25).
Drug treatment. Anticholinergic and antimuscarinic drugs (oxybutynin, tolterodine, darifenacin, fesoterodine, imidafenacin, propiverine, solifenacin, trospium chloride) are the most frequently used drugs for management of neurogenic bladder. These drugs bind to muscarinic receptors in the detrusor muscle, reduce the bladder storage pressure, and increase its capacity. Oxybutynin causes direct smooth muscle relaxation of the urinary bladder. Imipramine, a tricyclic antidepressive drug, also has a direct inhibitory and local anesthetic effect on the bladder smooth muscle. In addition, imipramine increases bladder outlet resistance at the level of the bladder neck. When these drugs are not tolerated or are ineffective, beta-agonists, phosphodiesterase inhibitors, and GABA-B agonist baclofen can be administered. For difficult emptying, alpha-adrenergic antagonists can be used. Selective and nonselective alpha-blockers have been partially successful in decreasing bladder outlet resistance, residual urine, and autonomic dysreflexia (33; 03; 35). Desmopressin, a synthetic analog of arginine vasopressin, is often used to reduce urine production and volume by the mechanism of enhancing water reabsorption at the distal and collecting tubules of the kidneys. It helps alleviate the discomfort of daytime frequency or nocturia, providing symptom-free periods of up to 6 hours (33; 03). Mirabegron is a beta3-adrenoceptor agonist that has been tried in the treatment of overactive bladder. A review indicated that mirabegron is also effective in treating neurogenic bladder unresponsive to antimuscarinic drugs (18). A systemic review and meta-analysis observed that the use of beta3-adrenergic receptor agonists improved urodynamics parameters and clinical outcomes, such as incontinence, in children as well (38).
A systematic review evaluated the benefits and safety of oral medications that relax the bladder muscle in treating bladder overactivity due to nerve issues. A thorough search conducted on September 1, 2022, led to the analysis of 23 trials involving 1697 patients (68). Compared to a placebo, these medications showed clinical benefits but also more side effects in treating this condition. Specifically, antimuscarinic drugs improved bladder function and reduced leakage and frequency, but they also increased dry mouth. Mirabegron, another medication, improved some bladder parameters with fewer side effects. The analysis found no clear superiority among these drugs.
Solifenacin is an antimuscarinic medication that relaxes the urinary bladder muscles to prevent frequent, urgent, or uncontrolled urination. Trospium chloride is a muscarinic antagonist that treats overactive bladder by blocking certain nerve impulses. It relaxes the bladder muscle, reducing urgency, frequency, and leakage. A randomized study looked at the effectiveness of two medications, solifenacin and trospium chloride, in treating urinary problems in people who have had a stroke. The study included 206 patients from two centers who were randomly assigned to receive one of the medications or a placebo. The results showed that both medications were effective in reducing urinary symptoms, such as urgency and frequency, compared to the placebo. The patients who received the medications also reported an improvement in their quality of life. However, the study found some differences in the effectiveness and safety of the two medications. Solifenacin was found to be more effective in reducing some urinary symptoms and had fewer side effects compared to trospium chloride. The study suggests that both medications can be effective in treating urinary problems in people who have had a stroke, but further studies are needed to confirm these findings (29).
Anti-Nogo-A antibodies. Myelin-associated neurite outgrowth inhibitor A (Nogo-A) is a protein present on the surface of cortical neurons. Nogo-A inhibits central nervous system angiogenesis and subsequent neuronal sprouting. Nogo-A inhibitors can potentially accelerate nerve fiber sprouting neuronal regeneration and subsequent functional recovery. In many experimental studies, anti-Nogo-A antibody has been evaluated in animals with spinal cord injury to facilitate neuronal regeneration with the objective to improve lower urinary tract dysfunction (56).
Botulinum toxin A. There is growing evidence that neurogenic detrusor overactivity can be effectively managed by injecting botulinum toxin type A in the detrusor muscle under cystoscopic guidance. This treatment has shown to be safe and effective on clinical and urodynamic parameters with significant improvement in quality of life. The vast majority of studies have been conducted with onabotulinumtoxin A. In patients with overactive bladder/idiopathic detrusor overactivity, onabotulinumtoxin A may be injected in 20 sites above the trigone. With all patients receiving onabotulinumtoxin, a clean intermittent self-catheterization should be encouraged because there is an increased risk of a high post-void residual volume, urinary retention, or both after the botulinum injection (57). In adult patients with multiple sclerosis or spinal cord injuries with urinary incontinence, intradetrusor onabotulinumtoxin A (200 units) produced significantly better improvement (in urinary incontinence episodes/week) at week 6 than placebo. Additionally, in patients with high spinal cord injuries, intradetrusor injections of onabotulinum toxin A effectively in decrease the episodes of autonomic dysreflexia and improve bladder function and quality of life (19). A randomized controlled trial further confirmed that abobotulinumtoxin A intradetrusor administration improved quality of life, symptoms, and bladder function in patients with spinal cord injury or multiple sclerosis with bladder muscle overactivity leading to incontinence (16). In this study, 485 patients (341 with spinal cord injury and 144 with multiple sclerosis) were randomized. A significant reduction was observed in mean neurogenic detrusor overactivity incontinence episodes per week at week 6 with both aboBoNT-A doses versus placebo. Significant improvements in quality of life and urodynamic parameters were also observed following abobotulinumtoxin A administration.
Autologous muscle-derived cells. Data from a prospective open-label physician-initiated study noted that intradetrusor injection of autologous muscle-derived cells improved bladder function in patients with underactive bladder. Autologous muscle-derived cells were collected from the quadriceps femoris muscle using an 8-gauge needle (24).
Indwelling catheterization. Indwelling catheterization should be performed in patients with uncontrollable incontinence or for urinary retention when the use of intermittent self-catheterization is not feasible.
Clean intermittent self-catheterization. Clean intermittent self-catheterization is the best treatment option for patients with neurogenic bladder dysfunction (12). When used for appropriate patients, it has been shown to promote continence, maintain safe bladder function, and improve quality of life. Clean intermittent self-catheterization should be started if the post-void residual urine exceeds one third of bladder capacity or is greater than 100mL (47). A 2023 article highlights the individualized approach required for clean intermittent self-catheterization (13). It emphasizes the need to consider each patient's specific symptoms and diagnostic results, promoting the concept of bladder voiding efficiency. Clean intermittent self-catheterization is particularly beneficial for patients with neurologic disorders like spinal injuries, multiple sclerosis, Parkinson disease, and cauda equina syndrome. Although some bladder issues are treated with anticholinergics or botulinum toxin, leading to the necessity of clean intermittent self-catheterization for bladder emptying, the article discourages the general use of indwelling or suprapubic catheters due to potential complications like infections, stones, and pain. It advocates for disposable catheters, tailored to individual needs, and urges hospitals to avoid a one-size-fits-all approach in bladder function management.
Suprapubic catheterization. Suprapubic catheterization minimizes the risk of urethral trauma. It is a safe and effective alternative to long-term urethral catheter use. The most common indication of a suprapubic catheter is in patients with spinal cord injuries and a malfunctioning urinary bladder.
Surgical treatment. Many surgical procedures, such as transurethral sphincterotomy, endourethral stents, urethral and bladder neck procedures, augmentation cystoplasty, and urinary diversion methods are used in refractory cases of neurogenic bladder. Surgery is an effective alternative in patients with persistent detrusor hyperactivity despite the use of clean intermittent self-catheterization and optimum anticholinergic drug therapy (55). Bladder augmentation is the gold standard surgical procedure used to increase bladder capacity and reduce storage pressures (52). Robotic-assisted bladder neck procedures are found effective, safe, and feasible, and they follow the same steps and principles as those of open surgery. Robotic-assisted bladder neck procedures are associated with less blood loss, improved cosmetics, and lower abdominal adhesions (23).
The Artificial Urinary Sphincter. The Artificial Urinary Sphincter is a device used to treat urinary incontinence caused by neurologic disorders. It is a prosthetic device that replaces the natural urinary sphincter, helping to restore bladder control and improve the quality of life. A narrative review of current literature highlights the device's efficacy and safety in both male and female patients. Although the device's functional durability may be lower in patients with neurogenic lower urinary tract dysfunction, it can still provide effective and safe continence outcomes. Long-term device survival rates range from several years to over a decade. Practical considerations, outcomes, and complications of the device are discussed, emphasizing the importance of individualized patient care and careful device selection (64).
Neuromodulation (including genital nerve stimulation). Surface electrical genital nerve stimulation is a technique that inhibits reflex bladder contractions and increases bladder capacity in patients with neurogenic detrusor overactivity. The stimulation amplitude needed for genital nerve stimulation is almost twice the amplitude that is required to produce the pudendal-anal reflex. Genital nerve stimulation is a tolerable technique, but efficacy is not proven (09; 10).
The Brindley procedure combines sacral anterior-root stimulation and a rhizotomy of posterior sacral roots. In selected spinal injury patients, the Brindley procedure helps in overcoming neurogenic detrusor overactivity (44).
A trial noted that administration of daily transcutaneous electrical nerve stimulation over the sacral region for 90 days significantly improved overactive bladder symptoms in patients with neurogenic overactive bladder compared to a control group that received anticholinergic drugs alone (42). Randomized trials have also shown that bilateral transcutaneous posterior tibial nerve stimulation significantly improves bladder function in patients with various lower urinary tract conditions, including spinal cord injury (26; 37). Another randomized trial further confirmed the efficacy of posterior tibial nerve stimulation in improving all urodynamic parameters (bladder capacity and compliance, detrusor overactivity, maximum flow rate, and postvoid residual volume) in multiple sclerosis in comparison to controls (45).
A clinical trial conducted in Switzerland investigated the effectiveness of the StimRouter® neuromodulation system for treating persistent lower urinary tract symptoms in patients with multiple sclerosis (54). The study involved these patients self-administering nerve stimulation through the skin near the tibial nerve over a period of 24 weeks. The results demonstrated significant improvements in bladder capacity and scores from the Overactive Bladder Questionnaire, suggesting reduced symptom severity and an enhanced quality of life. However, there was no significant change in scores from the Multiple Sclerosis Quality of Life-54 questionnaire. Patient satisfaction with the treatment was high, and no serious adverse events were reported. The study concluded that the StimRouter presents a safe, effective, and minimally invasive treatment option for patients with multiple sclerosis and stubborn lower urinary tract symptoms.
A study evaluated the effectiveness of repetitive transcranial magnetic stimulation in treating overactive bladder symptoms in stroke survivors (01). The study included 60 participants who were randomly assigned to receive either active or sham treatments. The active treatment group received low-frequency magnetic stimulation pulses to the pelvic floor muscle area, whereas the sham group received a reduced stimulation. The study found that the active treatment group showed significant improvements in their overactive bladder symptoms compared to the sham group. The treatment was also found to be cost-effective, improving the quality of life for the participants. The study's findings suggest that this treatment can be a useful option for alleviating overactive bladder symptoms in stroke survivors (01).
Pelvic floor muscle training. Pelvic floor muscle training is an effective conservative treatment modality in managing neurogenic bladder. It improves the problem of urine leakage and bladder symptoms. Moreover, it enhances the endurance and pelvic floor muscles among patients with multiple sclerosis (36; 62).
Knowledge about management and outcomes of pregnancy in patients with spinal cord injury and neurogenic bladder is limited. Panneck and Bertschy evaluated data from 13 studies about spinal cord injuries in pregnancy (50). Spinal cord injuries were cervical in 34.7%, thoracic in 61.2%, and lumbar in 4.1% of pregnant women. In all 34.7% of the women who used indwelling catheters, 25% performed intermittent catheterization, 11.5% used the Credé maneuver (extrinsic manual bladder compression), and 28.8% voided spontaneously. A total of 64% of the patients had at least one symptomatic urinary tract infection during pregnancy. Urinary tract infections were more common in women with indwelling catheters than in those using self-intermittent catheterization, using the Credé technique, or voiding spontaneously (50). During labor, the possibility of dangerous autonomic dysreflexia is likely. Epidural anesthesia should be administered early in labor to prevent autonomic dysreflexia. With proper management, most women with spinal cord injury will have successful vaginal deliveries (51).
The most important anesthetic complication in patients with spinal cord injuries and neurogenic bladder is autonomic dysreflexia. Autonomic dysreflexia manifests with headache, sweating, bradycardia, and severe hypertension. In patients with low and complete spinal cord lesions, surgeries (below the level of injury) may safely be performed without anesthesia, provided there is no history of autonomic dysreflexia or troublesome spasms. General anesthesia of sufficient depth is usually effective in controlling spasms and autonomic dysreflexia, but hypotension and respiratory dysfunction are grave risks. Spinal anesthesia is potentially safe, effective, and simple to perform in this vulnerable group of patients (30).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Ravindra Kumar Garg DM
Dr. Garg of King George's Medical University in Lucknow, India, has no relevant financial relationships to disclose.
See Profile
Federica Provini MD
Dr. Provini of the University of Bologna and IRCCS Institute of Neurological Sciences of Bologna received speakers' fees from Idorsia, Italfarmaco, and NeoPharmed Gentili Spa.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
General Neurology
Dec. 30, 2024
General Neurology
Dec. 13, 2024
Neuromuscular Disorders
Dec. 09, 2024
General Neurology
Dec. 09, 2024