
















Peripheral Neuropathies
Gold neurotoxicity
Dec. 30, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Other than hallucinogenic mushroom poisoning, at least five distinct neurologic or myologic presentations of mushroom poisoning have been reported for mushrooms of the phylum Basidiomycota: (1) acute encephalopathy, (2) cholinergic (muscarinic) syndrome, (3) erythromelalgia, (4) a disulfiram-like reaction, and (5) rhabdomyolysis. Some mushroom toxins produce their associated toxidromes by affecting neurotransmission. Except for the acute encephalopathy and myotoxic toxidromes, neurologic presentations of mushroom poisoning for mushrooms of the phylum Basidiomycota are rarely fatal. Fatalities have uncommonly occurred with other neurologic toxidromes (eg, cholinergic mushroom poisoning).
|
• Other than hallucinogenic mushroom poisoning, at least five distinct neurologic or myologic presentations of mushroom poisoning have been reported for mushrooms of the phylum Basidiomycota: (1) acute encephalopathy, (2) cholinergic (muscarinic) syndrome, (3) erythromelalgia, (4) a disulfiram-like reaction, and (5) rhabdomyolysis. | |
|
• Some, but not all, of the mushroom toxins of the phylum Basidiomycota produce their associated toxidromes by affecting neurotransmission. | |
|
• Fatalities may occur with some of these toxidromes, especially with rhabdomyolysis or cholinergic mushroom poisoning. |
Fungi of the phylum Basidiomycota are filamentous fungi composed of hyphae that reproduce sexually. Basidiomycota includes inter alia some fungi that might be grown or foraged for food (eg, mushrooms, puffballs, bracket fungi, other polypores, and chanterelles) and fungi that infest plants and might be secondarily ingested (eg, smuts, bunts, rusts).
Other than hallucinogenic mushroom poisoning, the toxidromes associated with fungi of the phylum Basidiomycota include cholinergic forms of mushroom poisoning (the muscarine toxidrome), mushroom-induced erythromelalgia (the acromelic acid toxidrome), mushroom-induced disulfiram-like reaction (the coprine toxidrome or "coprinus syndrome"), acute encephalopathy (the pleurocybellaziridine toxidrome), and myotoxic mushroom poisoning (typically with rhabdomyolysis in severe cases).
The neurologic presentations of hallucinogenic ("magic") mushroom intoxication and poisoning associated with fungi of the phylum Basidiomycota are considered in a separate article. The other toxidromes listed in the preceding paragraph are addressed here.
Among classifications of mushroom poisoning, this toxidrome corresponds to Group B of Barbato (03), Group 4 of Blackman (05), Group 2B of White (66), and Group 4 of the American Association of Poison Control Centers’ National Poison Data System (24).
Mushrooms of the Clitocybe and Inocybe genera contain muscarine concentrations up to 1.6%. Two small white Clitocybe species contain muscarine in such amounts that deaths have been recorded for eating those two Clitocybe species: the ivory funnel mushroom [Clitocybe dealbata (Sowerby) Gillet] and the false champignon mushroom [Clitocybe rivulosa (Pers.) P. Kumm.], which occur in the grasslands of Europe and North America. Both may be confused with several edible species (Marasmius oreades; Clitopilus prunulus). In addition, the red-staining Inocybe mushroom [Inosperma erubescens (A. Blytt) Matheny and Esteve-Rav.], which occurs in the beech woodlands of Europe, produces the same toxidrome. It may be confused with several others (Calocybe gambosa; Agaricus spp.; Cortinarius caperatus). Other mushrooms, including Amanita pseudosychnopyramis and species of Inosperma and Pseudosperma may contain muscarine (09; 17; 36; 68; 70).
Muscarine is a natural product found in certain mushrooms, particularly in Inocybe and Clitocybe species, such as the deadly C. dealbata. Muscarine is a nonselective agonist of the muscarinic acetylcholine receptors. It is, therefore, not surprising that there is a large amount of structural homology between muscarine and acetylcholine.
Muscarinic receptors function in both the peripheral and central nervous systems, mediating innervation to visceral organs. Muscarinic acetylcholine receptors in the peripheral nervous system are found primarily on autonomic effector cells innervated by postganglionic parasympathetic nerves. Muscarinic receptors mediate many functions of the parasympathetic nervous system. While the sympathetic nervous system readies the body for “fight or flight,” the parasympathetic nervous system functions as the unconscious restorative and energy-conserving system (subserving the so-called “rest and digest” functions). Muscarinic receptors are also present in ganglia and on some cells, such as endothelial cells of blood vessels. Within the central nervous system, the hippocampus, cortex, and thalamus have high densities of muscarinic receptors.
Muscarinic manifestations after wild-mushroom ingestion have been reported on several continents and may be fatal (58; 53; 10; 38; 23).
Several species of mushrooms can produce the classic muscarinic toxidrome, which is summarized by the mnemonic device DUMBELS: Diaphoresis/Diarrhea/Defecation [relaxation of the internal anal sphincter in setting of diarrhea], Urination [due to relaxation of the internal sphincter muscle of urethra and contraction of the detrusor muscles], Miosis, Bronchorrhea/Bronchospasm/Bradycardia, Emesis, Lacrimation, and Salivation/Sweating. The alternatives presented for some letters reflect the different explanations of the mnemonic in the literature, but all of the various options can be considered part of the muscarinic or parasympathetic toxidrome. An alternative mnemonic is SLUDGE: Salivation/Sweating, Lacrimation, Urination, Diaphoresis/Diarrhea/Defecation, Gastrointestinal distress or upset [from smooth muscle tone changes, cramping, and diarrhea], and Emesis. This muscarinic toxidrome specifically does not include nicotinic symptoms, which are summarized instead by the mnemonic MTWHFS (ie, the 1-letter abbreviations of the days of the week from Monday to Saturday, where Thursday is represented by an H because Tuesday already used the T): Mydriasis, Tachycardia, Weakness, Hypertension, Fasciculations, and Seizures.
Muscarinic effects usually begin within 30 minutes of ingestion. The duration of muscarinic effects is dose-dependent, though typically short-lived, especially when compared to other sources of cholinergic poisoning, such as pesticides (note, though, that pesticides impair acetylcholinesterase so also produce both muscarinic and nicotinic effects).
Management of cholinergic mushroom poisoning includes administration of anticholinergic medications until drying of respiratory secretions has occurred (eg, atropine intravenously, 0.02 mg/kg intravenously with a minimum single dose of 0.1 mg and a typical maximum single dose of 1 mg; or glycopyrrolate 10 mcg/kg intravenously with a typical maximum single dose of 0.2 mg). Bronchospasm can be treated with inhaled albuterol combined with ipratropium bromide. Poisoned individuals with signs of dehydration or shock should receive prompt fluid resuscitation. Persistent vomiting may require antiemetics (eg, ondansetron 0.1 mg/kg intravenously with a maximum typical single dose of 4 mg).
Liquid chromatography-mass spectrometry can be used to validate a clinical impression of muscarine poisoning from mushroom ingestion and can quantitate muscarine levels in blood, plasma, and urine (20).
Major causes of mortality are respiratory failure from the bronchorrhea.
Acromelic acid toxidrome corresponds to Group 6B of White's classification of mushroom poisoning (66) but is not covered by either Barbato (03), Blackman (05), or the American Association of Poison Control Centers’ National Poison Data System (24).
The consumption of two species of mushrooms is associated with mushroom-induced erythromelalgia: Clitocybe acromelalga [Paralepistopsis acromelalga] and Clitocybe amoenolens [Paralepistopsis amoenolens]. Clitocybe acromelalga [Paralepistopsis acromelalga] is found in Japan (27; 47; 46; 44), whereas Clitocybe amoenolens [Paralepistopsis amoenolens] is a rare and fairly well-localized species found only in southern France, northern and central Spain, central Italy, and Morocco (64).
Clitocybe acromelalga [Paralepistopsis acromelalga] has been known to cause mushroom-induced erythromelalgia for over a century in Japan, whereas Clitocybe amoenolens [Paralepistopsis amoenolens] has only been linked to this condition in the last 2 decades or so in France (21; 08; 45; 55; 56) and Italy (35; 39). In France, ingestion of the toxic mushrooms occurred because Clitocybe amoenolens was confused with edible common funnel cap mushrooms in the Lepista flaccida complex and with Infundibulicybe gibba (Pers.) Harmaja (21; 45).
In 2012, a new genus, Paralepistopsis, in the fungal order Agaricales (also known as gilled mushrooms for their distinctive gills or euagarics), was proposed for the two rare toxic species associated with mushroom-induced erythromelalgia: Clitocybe amoenolens from North Africa (Morocco) and southern and southwestern Europe and C. acromelalga from Asia (Japan and South Korea) (64).
An isolation method for acromelic acids A and B, and clitidine, which are venomous constituents of Paralepistopsis acromelalga, has been developed in Japan, utilizing liquid chromatography with tandem mass spectrometry (28).
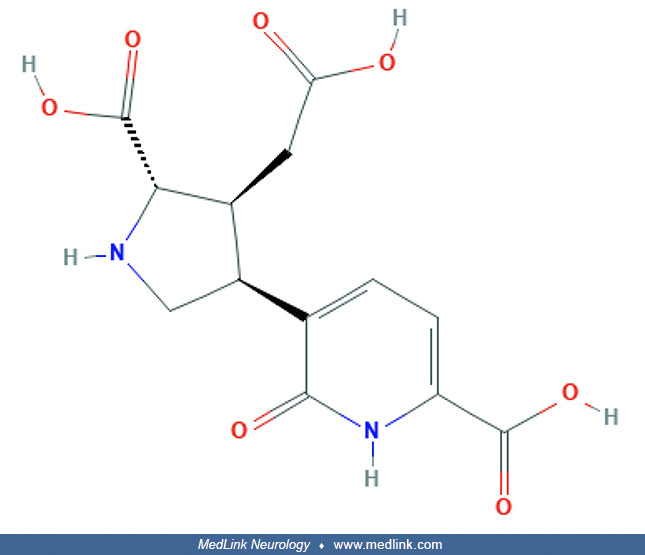
The causative toxin in Paralepistopsis acromelalga (and presumably also P. amoenolens) is acromelic acid, which comes in A and B forms.
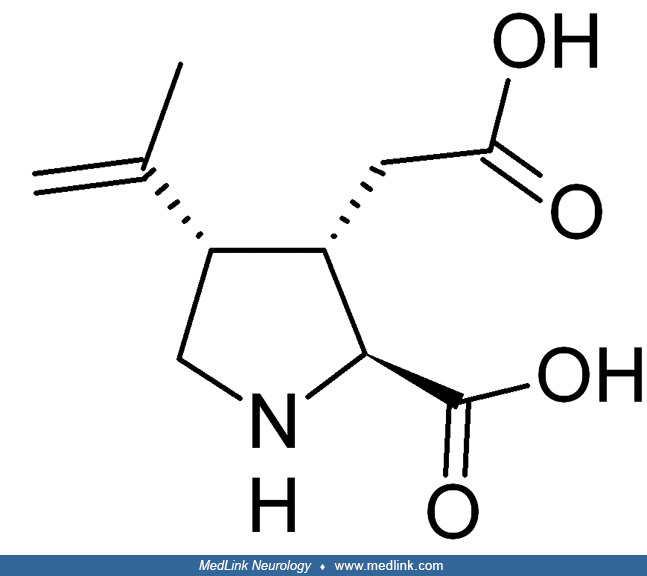
Both forms have a structural chemical formula resembling that of kainate acid or kainate (31; 43). Kainic acid, which occurs naturally in some seaweed, is a potent neuroexcitatory toxin that is an agonist for kainate receptors, a type of ionotropic glutamate receptor. Kainate receptors control a sodium channel that produces excitatory postsynaptic potentials when glutamate binds.
The syndrome of mushroom-induced erythromelalgia is characterized by varying intensities of paresthesias (tingling), followed by intense dysesthesias (burning pain) in the extremities, especially the feet (57).
In a French series, clinical features of erythromelalgia were observed in seven cases over a 3-year period. All patients had eaten the same mushroom species, Clitocybe amoenolens, gathered in the same French alpine valley (55). Mushroom-induced erythromelalgia generally lasted from 8 days to 5 months, although one person exhibited protracted symptoms for 3 years (18; 19).
Symptoms of erythromelalgia persist for about a month after ingesting the poisonous mushrooms (31).
Among classifications of mushroom poisoning, coprine toxidrome corresponds to Group F of Barbato (03), Group 4 of Blackman (05), Group 4B of White (66), and Group 5 of the American Association of Poison Control Centers’ National Poison Data System (24).
The mushroom-induced disulfiram-like reaction is caused by species containing the fungal toxin coprine, such as the Coprinus atramentarius (“ink cap”) mushroom (41; 32) and Echinoderma asperum (also known as Lepiota aspera and as "freckled dapperling") (25).
The mushroom toxin coprine was first isolated in the mid- to late-1970s (26).
Metabolites of coprine inhibit aldehyde dehydrogenase (26; 61; 06; 62; 67); then, if alcohol is ingested hours to days later, the affected individual experiences a constellation of symptoms identical to that from drinking alcohol after taking disulfiram: headache, nausea, vomiting, flushing, tachycardia, and rarely hypotension. Co-ingestion of alcohol with the toxic mushrooms produces less intense effects because of the slower metabolism of coprine to its toxic metabolites.
Investigation of the mushroom-induced disulfiram-like reaction stimulated numerous research studies in hopes of developing a novel drug that would be useful in the treatment of alcoholism; unfortunately, the mutagenic and gonadotoxic properties of coprine made it unsuitable for therapeutic use (41). Disulfiram-like reactions are generally an uncommon form of mushroom poisoning (60).
After drinking alcohol, symptomatic patients with the coprine toxidrome develop headache, nausea, vomiting, flushing, tachycardia, and, rarely, hypotension (25).
In one report, five people experienced the same symptoms after consumption of self-collected Lepiota aspera mushrooms, which had been mistaken for edible mushrooms (eg, Amanita rubescens or Macrolepiota procera) (25). The mushrooms were sautéed and were initially well-tolerated; however, within a few minutes of drinking an alcoholic beverage, each of the affected individuals experienced facial flushing, throbbing headache, tachycardia, and shortness of breath. The unpleasant symptoms abated within a few hours without sequelae but could be precipitated again by further alcohol consumption for up to 48 hours.
Management is supportive.
No serious adverse outcomes have been reported after poisoning with coprine-containing mushrooms.
Pleurocybellaziridine toxidrome is included as Group 6D by White's classification of mushroom poisoning (66) but is not covered by either Barbato (03), Blackman (05), or the American Association of Poison Control Centers’ National Poison Data System (24).
Pleurocybella porrigens mushrooms, which are known in Japan as Sugihiratake and in North America as "Angel Wings," occur in various woodlands of North America, Europe, and Asia. They may be confused with the edible mushroom Pleurotus pulmonarius (commonly known as the Indian Oyster, Italian Oyster, Phoenix Mushroom, or the Lung Oyster). Ingesting these mushrooms can produce an acute encephalopathy toxidrome and death. Ingesting these mushrooms was the cause of two deadly outbreaks in Japan in 2004 and 2009 (59).
Although Japan’s Ministry of Health, Labor, and Welfare traced the source of the poisoning to the angel’s wing mushroom (Pleurocybella porrigen), the underlying toxin had initially evaded identification. Subsequent studies suggest that the toxin may be an unusual and unstable aziridine amino acid: 3,3-dimethylaziridine-2-carboxylic acid or what the Japanese investigators labeled "pleurocybellaziridine" or its metabolites, including various cytotoxic amino acids that share a common beta-hydroxyvaline backbone (52; 65; 59).
The fungal toxin "pleurocybellaziridine" (3,3-dimethylaziridine-2-carboxylic acid) is responsible for fatal outbreaks of mushroom poisoning in Japan after ingesting Pleurocybella porrigens mushrooms. These outbreaks pr...
Pleurocybellaziridine proved to be toxic to rat oligodendroglial cells in culture (65). There are no available pathological studies of fatal human cases or animal models.
These mushrooms have been associated with two deadly outbreaks in Japan in 2004 and 2009. In the Fall of 2004, 59 people in nine prefectures of Japan were sickened after eating Pleurocybella porrigens mushrooms. Seventeen (29%), with an average age of 70 and with histories of chronic kidney disease, developed an acute encephalopathy and died. In 2009, an additional fatality occurred involving a 55-year-old man who had been on hemodialysis for 3 months. Symptoms developed 13 to 18 days after eating the mushrooms and began with tremor and limb weakness and progressed to alterations of consciousness with intractable seizures and high fever. Three to 8 days after onset, brain imaging showed diffuse lesions in the cerebral cortex.
Management is supportive.
Nearly a third of poisoned patients died in the 2004 Japanese outbreak. Death typically occurred about 10 days after seizures began.
Myotoxic mushroom poisoning is incorporated into Group 3 of White's classification of mushroom poisoning (66) but is not covered by Barbato (03), Blackman (05), or the American Association of Poison Control Centers’ National Poison Data System (24). White further dichotomizes myotoxic mushroom poisoning into Group 3A, or rapid-onset myotoxicity, and Group 3B, or delayed-onset myotoxicity (66).
Tricholoma equestre mushrooms. Tricholoma equestre (also known as T flavovirens and T auratum, and colloquially as "man on horseback" or "yellow knight") is a well-known mushroom species that occurs worldwide and had been widely considered a tasty and quite edible species. It should now be considered conditionally edible. T equestre can be confused with several other visually similar mushrooms, including T aestuans and T sulphureum.
Tricholoma equestre (also known as T. flavovirens and T. auratum and colloquially as "man on horseback" or "yellow knight") mushroom occurs worldwide and had been widely considered to be a tasty and q...
Tricholoma equestre toxicology. Experimental studies with a mouse model confirmed the involvement of T equestre in the etiology of rhabdomyolysis. The specific muscle toxin remains to be identified (29; 69; 16; 51).
Two toxins from a related species, T terreum, cause rhabdomyolysis in mice (29; 69), but these toxins have not been identified in T equestre (69; 16; 51). The toxins identified in T terreum were saponaceolide B and saponaceolide M. T equestra "has been banned from consum[ption] almost everywhere", whereas to date "no government authority has excluded T. terreum from human consum[ption]" (16). Various countries, including France, Spain, and Italy, condemned T equestre as poisonous and release public health warnings to prevent its consumption (30).
An experimental study in mice found that extracts of Tricholoma equestre mushrooms stored for 12 months at -20°C (-4°F) did not cause rhabdomyolysis (14).
In another experimental study in mice fed Tricholoma equestre (T. flavovirens) mushrooms, the plasma creatine kinase activity increased with consumption of these mushrooms, but the same was observed with the well-known and commercially important Boletus edulis (48). The authors concluded that the observed myotoxic effect "is probably not species-specific but represents an unspecific response and requires individual sensitivity and a great amount of ingested mushroom to manifest itself." A subsequent report by the same group found similar responses with several other mushroom species of diverse genera, reinforcing the conclusion that the response is nonspecific (in mice), which requires individual predisposition or sensitivity and a significant amount of ingested mushroom to manifest itself (49). An additional study found evidence in mice fed T. equestre of myo-, cardio- and hepatotoxic effects (50). These conclusions have subsequently been reiterated (51).
Other authors have since discounted the earlier human clinical results and the available experimental mouse studies for T. equestra and concluded that "T. equestre cannot be considered as a toxic species and does not appear to exhibit any greater health threat than other mushroom species currently considered as edible" (30). These authors advocated greater care when reporting cases of human poisoning to fully establish T. equestre as the causative agent with results of molecular phylogenetic analyses and to exclude interfering factors.
A survey of mushroom foragers in Poland, an analysis of Polish toxicology databases, and a small exposure trial among volunteers in Poland found no evidence of serious toxicity from T. equestre and found no evidence to indicate a significant risk of rhabdomyolysis. In a nationwide survey of Polish mushroom foragers, among 1545 foragers surveyed, 58% admitted to collecting and consuming T. equestre at least once per year, and 25%, admitted to consecutive consumption of T. equestre at least once in their lifetime for a median of 3 consecutive days (range 2 to 14 days) at a mean daily dose of 195 gm (maximum daily dose of 750 gm); no cases of rhabdomyolysis were identified, although seven individuals suffered from diarrhea and abdominal pain, and one individual was admitted to a toxicological unit and had a routine gastric lavage performed (30). The epidemiological database on mushroom poisonings in Poland was analyzed from the year 2008, and no cases of rhabdomyolysis were identified, despite estimates that at least several hundred thousand mushroom foragers in Poland consume T. equestre annually. The toxicological database indicated that mushrooms from the Tricholoma genus rarely caused poisonings, and no cases of rhabdomyolysis have been reported within the last decade. Hematological and biochemical parameters were also followed for a week in 10 volunteers consuming 300 g of molecularly identified T. equestre. The volunteers showed no hematological or biochemical alterations and experienced no adverse effects. The authors concluded that T. equestre is edible if consumed in rational amounts by healthy subjects.
Tricholoma equestre myotoxic toxidrome. Individuals poisoned with Tricholoma equestre mushrooms typically present 1 to 3 days later with rhabdomyolysis. From available reports, most individuals consumed the mushrooms repeatedly over several days prior to becoming ill. Manifestations include a marked elevation in the plasma level of creatine kinase as well as a red to brown color of the urine with pigmented granular casts.
Concern was first raised in southwestern France. Between 1993 and 1998, 12 cases of rhabdomyolysis with three deaths occurred in French adult men and women after three to six consecutive meals of T. equestre mushrooms (04; 57). One to 3 days after the last meal, patients presented with painful muscle weakness, mainly in the upper part of the legs, which worsened over a period of 3 to 4 days. This was accompanied by the development of leg stiffness and dark urine. Eight patients also developed facial erythema, mild nausea without vomiting, and profuse diaphoresis; five had hyperpnea. Laboratory studies showed marked serum elevations of creatine kinase, with a mean level of 226,067 units per liter in the women and 34,786 units per liter in the men, with corresponding increases in aminotransferases (consistent with the well-characterized muscle release of AST and ALT). Electromyography and nerve conduction studies showed evidence of muscle injury without nerve damage; complex and generally myotonic activity was present, without fibrillation, in the proximal thigh muscles. Histologic analysis of quadriceps muscle biopsy specimens in six patients showed signs of a direct muscle injury with well-preserved fascicular architecture but a “nibbled” appearance of the myofibrils and, in some cases, edema in the absence of vacuoles or the accumulation of glycogen or lipid. In the three patients who died, samples of the psoas muscles, arm muscles, myocardium, and diaphragm also showed evidence of acute myopathy.
In all but the three patients who died, most symptoms resolved with the gradual normalization of serum enzyme values over 15 days, although muscular weakness persisted for several weeks. The three patients who died experienced increasing dyspnea at rest, followed by increasing rales at both lung bases; hyperthermia (a temperature of up to 42°C or 107.6°F); signs of acute myocarditis, including cardiac arrhythmia, cardiovascular collapse, and widening of the QRS complex without severe acidosis; and laboratory evidence of renal dysfunction accompanied by hyperkalemia (potassium, 6.0 to 7.2 mmol per liter) and hypocalcemia (calcium, 5.6 to 8.3 mg per deciliter). The three patients had creatine kinase values of 632,000, 138,900, and 295,700 U per liter, with isoenzyme MB making up 0.5% to 0.7% of the total.
Four cases of acute Tricholoma equestre mushroom poisoning were reported from Poland in 2009, involving three adults and one child (01). The patients had eaten from 100 to 400 grams of the mushroom within a few consecutive meals. After consuming about 1000 grams of T. equestre for 3 to 4 days, the subjects developed myalgia, fatigue, muscle weakness, and, in two cases, acute respiratory failure. Maximal serum CK was 48,136 U/L in the adults and 306 U/L in the child. Maximal serum levels of AST and ALT were 802 U/L and 446 U/L in adults and 39 U/L and 56 U/L in the child. One patient (age 72 years) developed acute respiratory failure and died on the second day of hospitalization. In the other patients, the clinical signs and biochemical abnormalities resolved from 2 to 3 weeks after admission. A subsequent report from this group reiterated these observations (02).
Four cases of T. equestre mushroom poisoning were reported from Lithuania between 2004 and 2013 (33), among which one person died. In the fatal case, a 44-year-old man had eaten standard portions of T. equestre on 3 consecutive days and on the subsequent day developed nausea without vomiting as well as fatigue, myalgia, muscle weakness, profuse diaphoresis without fever, and respiratory insufficiency. Laboratory tests on admission showed elevations of creatine kinase (CK 16590 IU/L), aspartate aminotransferase (AST 1524 IU/L), and alanine aminotransferase (ALT 579 IU/L). Although clinical findings and laboratory tests were consistent with rhabdomyolysis, no renal insufficiency was observed. The patient’s health condition worsened during the first few hours, with body temperature reaching 42°C (107.6°F). His CK value reached 34,600 IU/L. The patient died from a heart attack on the sixth day after consumption of T. equestre.
Acute mushroom poisoning with Tricholoma equestre was reported in a 5-year-old Polish boy who ate 300 to 400 grams daily for 4 consecutive days (13). Signs included acute respiratory failure, muscle weakness (involving especially the pelvic girdle), and urinary retention. The boy could not sit or stand without assistance, and his bladder had to be catheterized. Laboratory tests showed only minor muscle injury with maximal creatine kinase 306 U/L, aspartate aminotransferase 39 U/L, and alanine aminotransferase 56 U/L. Clinical signs and biochemical abnormalities resolved within 12 days of admission. The authors suggested that the clinical picture of T. equestre poisoning may be different in children and adults.
Patients with this syndrome have now been identified in France, Poland, and Lithuania (12; 22; 33).
Management. The primary treatment goals are similar to rhabdomyolysis from other causes; these include (1) prevention and treatment of acute renal failure from heme pigment-induced acute kidney injury and (2) correction of significant electrolyte abnormalities. Early detection, close monitoring (especially serum electrolytes, creatinine, CPK, urine output, and cardiac effects), and good supportive care are the main treatment modalities. A normal saline infusion is used to replete fluid losses. Urine output should be closely monitored, maintaining a minimum urine flow of approximately 4 mL/kg per hour (ie, 200 mL per hour in adults). Poisoned individuals should be monitored for significant electrolyte abnormalities, particularly hyperkalemia, hyperphosphatemia, and hypocalcemia. Management of hyperkalemia is of particular importance because it may be life-threatening if untreated. Because hypocalcemia is usually transient and asymptomatic, calcium administration should be avoided unless severe symptoms (eg, tetany) are present.
Adverse outcomes. Tricholoma equestre myotoxic mushroom poisoning has a high case fatality rate, at least among those who develop overt rhabdomyolysis, with about a quarter of affected patients dying, usually of cardiovascular complications (04; 34; 57; 11; 07).
Russula subnigricans mushrooms. The Russula subnigricans Hongo mushroom occurs in Asia and North America. The species was named by Japanese mycologist Tsuguo Hongo (1923 to 2007) in 1955. It may be confused with the edible mushroom Russula nigricans. Reports from at least three Asan countries have now linked this mushroom with myotoxic mushroom poisoning.
Cycloprop-2-ene carboxylic acid toxicology. Maatsuura and colleagues isolated the small, highly strained toxin cycloprop-2-ene carboxylic acid from Asian R. subnigricans and demonstrated that this compound was associated with fatal rhabdomyolysis in mice (40). This carboxylic acid is also presumably responsible for rhabdomyolysis in humans.
Cycloprop-2-ene carboxylic acid toxidrome. In an outbreak of R. subnigricans poisoning in Taiwan, two patients progressed to rhabdomyolysis, whereas seven patients recovered in 1 day with supportive care at home (34). The most severely ill patient presented with rhabdomyolysis associated with severe electrolyte disturbances (hyperkalemia, hypocalcemia), pulmonary edema, respiratory failure, acute renal failure, ventricular tachycardia, and circulatory shock.
In a report from China, seven people from a single family each ate 10 to 100 gm of cooked wild mushrooms that were later identified as R. subnigricans Hongo (37). All of the family members were hospitalized the following day with nausea, vomiting, diarrhea, dizziness, fatigue, and muscle weakness, and five also had myalgias, mainly in the upper legs. The median initial level of creatine kinase was 2063 U/L (range 126 to 66,950 U/L), with corresponding elevations in aminotransferase enzymes (AST and ALT), and in some cases with associated hypokalemia and hypocalcemia. In four of the six patients who survived, weakness progressed and was accompanied by further elevations of CK values and the production of dark urine. These four patients were subsequently treated with hemodialysis to prevent acute kidney injury. From the third day, muscle strength and serum CK levels gradually normalized. The patient who died declined despite hemodialysis: his serum CK level increased to 228,750 U/L, and he developed hyperthermia (40°C or 104°F), signs of severe dehydration, and acute myocarditis, including cardiac arrhythmia, cardiovascular collapse, and widening of the QRS complex.
In a case report from Korea of R. subnigricans poisoning, a 51-year-old man cooked with wild mushrooms that he gathered 1 day earlier (11). He shared the meal with his wife and son who ingested a single piece of mushroom, experienced nausea, and ate no more. The man nevertheless ate the mushrooms without immediate symptoms, but 6 hours later complained of vomiting, diarrhea, and myalgia. He was hospitalized with hypotension (systolic blood pressure 60 mm Hg), requiring intravenous dopamine support. He complained of generalized myalgia, chest discomfort, palpitations, and dyspnea. Despite intensive care management, he suffered from rhabdomyolysis, acute kidney injury, severe hypocalcemia, respiratory failure, ventricular tachycardia, and cardiogenic shock, and ultimately died.
In another report from Korea of R. subnigricans poisoning, four family members (two men and two women) ate wild mushrooms that had been picked from a forest (42). The index case was a 64-year-old man who presented with a12-hour history of substernal chest discomfort, nausea, vomiting, and myalgia. Laboratory tests revealed elevated serum troponin I. He was diagnosed with non-ST segment elevation myocardial infarction. Subsequently, two family members who ate mushrooms together with the index case developed rhabdomyolysis requiring intensive care unit management. With conservative management, including primary fluid resuscitation, these three patients were discharged without complications. R subnigricans poisoning was revealed after investigation. The remaining family member developed nausea, vomiting, and diarrhea immediately after mushroom ingestion and was treated and released from a hospital emergency department.
In three cases of myotoxic mushroom poisoning in Thailand, the mushrooms were also identified as Russula species by an experienced mycologist (63).
Management. The primary treatment goals are similar to rhabdomyolysis from other causes; these include (1) prevention and treatment of acute renal failure from heme pigment-induced acute kidney injury; and (2) correction of significant electrolyte abnormalities. Early detection, close monitoring (especially serum electrolytes, creatinine, CPK, urine output, and cardiac effects), and good supportive care are the main treatment modalities. A normal saline infusion is used to replete fluid losses. Urine output should be closely monitored, maintaining a minimum urine flow of approximately 4 mL/kg per hour (ie, 200 mL per hour in adults). Poisoned individuals should be monitored for significant electrolyte abnormalities, particularly hyperkalemia, hyperphosphatemia, and hypocalcemia. Management of hyperkalemia is particularly important because it may be life-threatening if untreated. Because hypocalcemia is usually transient and asymptomatic, calcium administration should be avoided unless severe symptoms (eg, tetany) are present.
Adverse outcomes. Among 17 cases of clinical poisoning, at least seven developed rhabdomyolysis (41%), and two died (12%) (34; 37; 11).
Several other reports of myotoxic mushroom poisoning have been published, though in most cases with a less-clear association with a specific mushroom species and without identification of a potential toxin (15; 71; 63).
In a retrospective study from Thailand during a 5-year period (2012 to 2016), 38 individuals developed myotoxic mushroom poisoning without clear association with known myotoxic species (three others in this series ate mushrooms identified as Russula species) (63). Common presenting symptoms were gastrointestinal symptoms and myalgia. The median onset of gastrointestinal symptoms was 2 hours after mushroom ingestion, with a range from 10 minutes to 24 hours. Symptoms suggesting rhabdomyolysis developed after a median of 24 to 48 hours, with a range of 2 hours to 5 days. For patients with rhabdomyolysis, acute kidney injury occurred in half of the cases, and hyperkalemia occurred in one third of cases. Median initial and maximum creatine phosphokinase (CPK) levels in patients with rhabdomyolysis were 31,145 and 47,861 U/L, respectively. The mortality rate was 27%. Treatments included intravenous fluid, urine alkalinization, hemodialysis, and peritoneal dialysis.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Dec. 30, 2024
General Neurology
Nov. 09, 2024
General Neurology
Nov. 05, 2024
Headache & Pain
Nov. 04, 2024
Peripheral Neuropathies
Oct. 25, 2024
Peripheral Neuropathies
Jul. 17, 2024
Neurotoxicology
Jul. 15, 2024
Neurotoxicology
Jul. 01, 2024