
Neuro-Oncology
Visual pathway gliomas
Jan. 14, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Primary central nervous system lymphoma is an extranodal non-Hodgkin lymphoma that arises within and is confined to the nervous system, including the brain, spinal cord, leptomeninges, and eyes. In this article, the author discusses developments in managing primary central nervous system lymphoma.
|
• Primary central nervous system lymphoma is a non-Hodgkin (usually diffuse large B-cell) lymphoma that arises within, and generally remains confined to, the nervous system. | |
|
• Staging work-up differentiates primary CNS lymphoma from extra-CNS lymphoma with CNS involvement. | |
|
• In the immunocompromised setting, the disease is often associated with the Epstein-Barr virus. | |
|
• Treatment options include systemic chemotherapy, intra-CSF chemotherapy, radiotherapy, and targeted therapies. High-dose methotrexate forms the backbone of many treatment protocols. |
Primary central nervous system lymphoma was first described in 1929 by Bailey (06). Over the following 2 to 3 decades, cerebral lymphoma was recognized as a discrete entity but described under a variety of names, including reticulum cell sarcoma, histiocytic sarcoma, and microglioma, highlighting the debate regarding the malignant cell of origin; however, modern immunohistochemical studies definitively established the lymphocytic nature of this tumor.
Primary central nervous system lymphoma usually occurs in the brain as an intracranial mass (masses) but may also involve the spinal cord parenchyma, leptomeninges, and eyes. Most commonly, these other disease sites occur along with brain lesions, but occasionally they may be the only site of lymphoma or the presenting location of disease. The peak incidence occurs in the sixth and seventh decades of life in immunocompetent patients but is much younger for immunosuppressed individuals.
Because primary central nervous system lymphoma can be a rapidly growing neoplasm, most patients have symptoms for only a few weeks before coming to medical attention. Neurologic dysfunction can progress rapidly over a few days; however, some patients may have a more indolent course, with symptoms gradually evolving over months. This is particularly true of patients whose disease begins within the eye, and ocular symptoms may wax and wane for years before a definitive diagnosis is established. Rarely, patients have spontaneous remissions of symptoms and even mass lesions identified on imaging; more commonly, remission is precipitated by corticosteroid administration (04; 55; 44).
The overwhelming majority of patients present with symptoms and signs suggestive of a brain tumor. These can be categorized as either localizable or nonlocalizable. The localizable symptoms correlate with involved neuroanatomy. Approximately 50% to 70% of patients present with focal neurologic deficits (08). Because the frontal lobes are commonly affected, cognitive changes and an altered level of alertness occur in one half to two thirds of patients. As a presenting complaint, seizures are seen in only 10% of patients, compared to 25% to 75% of those with other primary or metastatic brain tumors (17). Nonlocalizable symptoms are typically due to increased intracranial pressure and include symptoms such as headaches, which are often worse when first awakening in the morning or may wake patients from sleep.
Ocular lymphoma involves the vitreous, uvea, or retina (65; 84). Symptoms are often subtle and consist of floaters or visual blurring. These symptoms are nonspecific, and patients are often initially diagnosed with uveitis or vitreitis of unknown etiology. The symptoms and inflammatory cells seen in the vitreous on slit-lamp examination may persist for years, eventually causing visual loss, although visual loss is rare in the early stages. The absence of a durable clinical response to the usual therapy, topical steroids, should suggest the diagnosis of ocular lymphoma. Most patients with ocular involvement also have nonocular CNS involvement (35). Ocular involvement of primary CNS lymphoma is estimated to occur in 15% of cases at initial diagnosis (40). Approximately 37% to 50% of patients with primary vitreoretinal lymphoma have concurrent CNS involvement (51). Furthermore, patients with primary vitreoretinal lymphoma are at risk of developing CNS disease during their disease, estimated at over 30% by 50 months, which necessitates close radiographic and oncologic surveillance (69).
Leptomeningeal lymphoma presents with confusion, cranial neuropathies, radiculopathies that may be painful, symptoms of increased intracranial pressure (headache, nausea, and vomiting), or a combination of these symptoms. Tumor cells can gain access to the CSF by virtue of the periventricular location of lymphoma lesions, and leptomeningeal involvement can be documented in up to 40% of patients. Leptomeningeal lymphoma is more frequently a manifestation of CNS involvement in patients with extra-CNS lymphoma.
Spinal lymphoma often presents as a painless myelopathy with symptoms localizable to the cord level. Primary spinal cord lymphoma is exceedingly rare, accounting for only 1% of primary CNS lymphoma (85).
There are two widely used prognostication systems. The first is the International Extranodal Lymphoma Study Group (IELSG) prognostication system. In this system, points are allotted for age, performance status, serum LDH, CSF protein, and deep-seated lesions. These points can be utilized to calculate a prognostic score (27). The second system is the Memorial Sloan-Kettering Cancer Center (MSKCC) prognostic system. This system relies only on age and performance status to estimate survival (01). In both systems increasing age and worsening performance status are associated with shorter survival. The inferior outcomes with increasing age are also reflected in epidemiologic studies (64). On analysis of a contemporary population of primary CNS lymphoma patients, 2-year survival is approximately 50%, and 5-year survival is 38% with aggressive therapy (40).
In elderly patients, the presence of Epstein-Barr virus in tumor tissue suggests a worse prognosis with a shorter survival from primary CNS lymphoma (81). This may merely reflect a confluence of two potential negative prognostic factors, age and immunosuppression (which is often associated with Epstein-Barr virus positivity). Numerous other prognostic biomarkers have been investigated, at times with conflicting results.
A 54-year-old man with a history of depression gradually developed memory disturbances, poor concentration, apathy, and fatigue. His symptoms were initially attributed to depression, but then he noted that his left foot was dragging. An MRI with contrast demonstrated an irregularly enhancing lesion in the right frontal lobe with surrounding T2 hyperintensity and mild mass effect. HIV testing was negative. He was placed on steroids before undergoing brain biopsy. Unfortunately, the biopsy was nondiagnostic. His symptoms resolved on steroids, and he was subsequently tapered off. A few weeks later, he developed slurred speech, confusion, and gait instability. A repeat brain MRI with contrast demonstrated a new, enhancing right cerebellar lesion as well as faint enhancement within the right frontal lobe. Steroids were not restarted, and he underwent biopsy of the right cerebellar lesion. Pathology demonstrated a diffuse large B cell lymphoma. To complete lymphoma staging, he underwent ophthalmologic examination, including slit lamp examination and body PET scans. There was no evidence of systemic or ocular lymphoma. He was started on a high-dose methotrexate (HD-MTX) containing regimen and achieved a complete response before moving forward with consolidation therapy.
This clinical vignette demonstrates the importance of withholding steroids in suspected cases of CNS lymphoma. Corticosteroids work as a cytolytic agent against lymphomas and may result in a marked decrease or complete disappearance of brain lymphoma lesions (55; 44). When the residual lesions are biopsied, they are frequently necrotic, or nondiagnostic tissue is obtained, and no definitive diagnosis is made. In this case, pathologic confirmation of primary central nervous system lymphoma was delayed due to corticosteroid administration. Hyperosmotic agents such as mannitol of hypertonic saline, in place of steroids, can be considered a means to decrease cerebral edema if necessary.
The etiology of cerebral lymphoma in immunocompetent patients is incompletely understood.
Immunophenotyping studies suggest that the malignant B cells are derived from highly mutated late germinal center or postgerminal center B cells (59; 80).
In immunosuppressed patients, particularly those with AIDS or transplant recipients, the Epstein-Barr virus appears to have an important etiologic role (56; 20). Most adults have had acute Epstein-Barr virus infection in childhood, and a small population of B lymphocytes becomes immortalized by the virus. Proliferation of this latently infected population is controlled by circulating T-cells and rarely leads to malignancy; however, when the host immune system is no longer capable of suppressing this latently infected lymphocyte population, uncontrolled cell growth leads to tumor formation. These Epstein-Barr virus-driven lymphomas tend to develop in the nervous system because the brain is an immunologically privileged site offering further protection from immune surveillance (54).
There is increasing understanding of the biological basis of lymphoid malignancies, including primary CNS lymphoma. Mutations in MYD88 L265P are frequently seen in systemic diffuse large B-cell lymphomas as well as primary CNS lymphoma. The MYD88 gene codes for a B-cell signal adaptor protein with mutations leading to constitutive activation for the NF-kappaB pathway (66).
Most primary CNS lymphomas are classified as nongerminal cell B-cell-like (non-GCB) immunophenotypes according to the Hans classification system. In addition to MYD88, other mutations frequently seen are CD79B and CARD11, which are involved in the Toll-like and B-cell receptor signaling pathways (13). The primary CNS lymphoma mutational profile is most similar to the “MCD/C5” subtype for systemic lymphoma (15).
For decades, primary central nervous system lymphoma was an extremely rare tumor. In large autopsy series, it accounted for only 1% of all intracranial neoplasms; however, in both immunocompetent and immunocompromised patients, the incidence rose dramatically in the late 1970s and in the 1980s (24). Primary central nervous system lymphoma comprises approximately 2% of all primary CNS tumors in the United States (64). Across the overall population, this trend toward increased incidence appears to have stopped (32). However, the incidence in specific subgroups may be decreasing (HIV+), whereas in others it may be increasing (elderly).
In the apparently immunocompetent population, the primary central nervous system lymphoma incidence increased 3-fold during the 15 years from 1974 to 1988, and the incidence of primary ocular lymphoma increased 1.5-fold during the same interval (22). This increased incidence among the immunocompetent population has continued and is independent of improved diagnostic techniques or population bias (61); however, the incidence of systemic non-Hodgkin lymphoma has not risen significantly. The cause of this increase is unknown and cannot be attributed to improved methods of diagnosis, uniform nosology, or unrecognized AIDS-associated cases.
No method of prevention is known for primary central nervous system lymphoma. For immune-deficient patients, treatment of the underlying immunosuppression will reduce the risk of cerebral lymphoma.
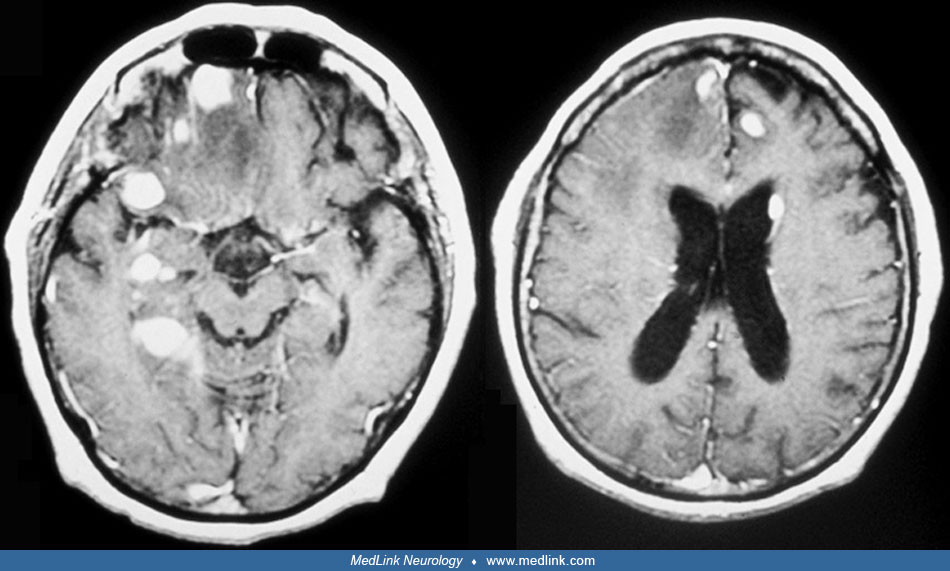
Patients with primary central nervous system lymphoma usually present with cerebral symptoms that prompt the physician to obtain CNS imaging. Although no absolute radiographic appearance exists that permits a definitive diagnosis, there are characteristic features that should strongly suggest the diagnosis and differentiate it from other space-occupying brain lesions such as demyelinating diseases, gliomas, meningiomas, metastasis, sarcoidosis, and toxoplasmosis. In immunocompetent patients, primary central nervous system lymphoma is usually isodense or hyperdense on CT scan before contrast administration and isointense or hyperintense on precontrast T1-weighted MR images.
On CT or MRI scan, cerebral lymphoma typically has a dense and uniform enhancement pattern after contrast administration. Ring enhancement, which is usually seen with infections, brain metastases, and malignant gliomas, is distinctly uncommon in cerebral lymphoma. Lymphomatous lesions are frequently periventricular and have indistinct borders. Thirty-five percent of patients have more than one lesion. Intraparenchymal lesions may be located in the hemispheres (38%), thalamus/basal ganglia (16%), corpus callosum (14%), ventricular areas (12%), and cerebellum (9%) (49). Cerebral metastases, which can have a similar appearance to primary central nervous system lymphoma on MRI, are usually located at the cortical gray-white junction and watershed zones. The amount of edema associated with lymphoma masses may be highly variable. Some patients do have extensive peritumoral edema as seen with other brain tumors; however, many patients have little or no edema surrounding their lesions, a rare finding in other primary or metastatic brain tumors. On MRI, diffusion-weighted imaging often demonstrates restricted diffusion throughout the lesions (57). Calcifications frequently seen in oligodendrogliomas and low-grade astrocytomas are usually absent in primary central nervous system lymphoma.
These radiographic features, which are present in most patients, should lead to diagnostic consideration of primary central nervous system lymphoma, even before histologic confirmation is obtained. This consideration should affect the preoperative management of patients and help to avoid several pitfalls that complicate establishing the pathologic diagnosis.
When intracranial mass lesions are identified on CT or MR scan, the initial reaction is often to begin corticosteroid therapy to reduce perilesional swelling and improve the patient's neurologic status. Although this may be the proper approach for patients with metastases or malignant gliomas, it frequently destroys the opportunity to establish the diagnosis of cerebral lymphoma. Corticosteroids work as a chemotherapeutic agent against systemic and central nervous system lymphomas; they are cytotoxic and will produce cell lysis of malignant lymphocytes. At least 40% of patients have a marked decrease or complete disappearance of their brain lymphoma lesions, often within days of corticosteroid administration (39; 55; 44; 07). When the neurosurgeon biopsies residual lesions, frequently necrotic or nondiagnostic tissue, often demonstrating a T cell infiltrate, is obtained, and no definitive diagnosis is made, compromising subsequent treatment. Some consider resolution of an intracranial mass diagnostic of cerebral lymphoma; however, other lesions are known that contrast-enhance and resolve with steroid administration, such as multiple sclerosis and sarcoidosis, neither of which would require treatment with an HD-MTX regimen. Therefore, steroids should be withheld from patients whose cranial MRI or CT images suggest primary central nervous system lymphoma unless the patient is in imminent clinical danger of cerebral herniation, an extremely rare situation. Even in those circumstances, acute management plans can often utilize mannitol or hypertonic saline in place of steroids.
In HIV-positive patients, the radiographic appearance of primary central nervous system lymphoma is more variable and less distinctive. The lesions are hypodense (CT scan) or hypointense (MRI scan) before contrast and usually ring-enhancing, reflecting the high incidence of central necrosis seen in AIDS-related cerebral lymphoma (12; 43).
Diffuse enhancement is rarely seen in AIDS patients, and the lesions are more frequently cortical in location than in immunocompetent patients. No characteristic radiographic features of brain lymphoma exist in AIDS patients, and the lesions can be indistinguishable from toxoplasmosis or other infectious or neoplastic processes (54; 34). Positron emission tomographic scans or SPECT scans are reported to accurately differentiate cerebral lymphoma from infection in AIDS patients and may assist in early diagnosis. Particularly when combined with the detection of Epstein-Barr virus DNA in the CSF, these techniques can help facilitate a noninvasive diagnosis in many patients (05; 76). However, in most cases in the contemporary era, obtainment of a tissue diagnosis is necessary to move forward with confidence with the treatment via a high-dose chemotherapy regimen.
Patients with single lesions are most often confused with patients harboring other malignant primary brain tumors such as gliomas. The extent of tumor resection may favorably influence survival of patients with gliomas, and complete radiographic resection is often the surgical goal. In primary central nervous system lymphoma, there is longstanding evidence to support worse outcomes with surgical resection. However, this is being debated by some (83; 86; 68).
Patients with chronic immunosuppression, such as those after organ transplant, are at higher risk of developing post-transplant lymphoproliferative disease. A minority of these cases, up to 15%, can present only the CNS (25).
Brain MRI scan with gadolinium is the single most important imaging study for the evaluation of a patient with primary central nervous system lymphoma. It will define the areas of tumor and may demonstrate leptomeningeal involvement in an occasional patient. CT scan can be used when MR scanning is not available, but it is inferior. Stereotactic biopsy is indicated for pathologic confirmation. At this time there is no definitive serum or CSF diagnostic biomarker that can be utilized in all patients in place of biopsy.
Once the diagnosis of primary central nervous system lymphoma is established, all patients should undergo an ophthalmologic examination, including slit-lamp, to exclude ocular involvement. Patients with spinal symptoms should have a spinal MRI with contrast. This is not typically indicated for patients without symptoms localizable to the spine. Lumbar puncture to look for leptomeningeal spread of tumor with CSF cytology, CSF protein, flow cytometry, and IgH gene rearrangement PCR studies may be performed. It is unclear whether it adds any diagnostic value. In patients with positive CSF, the CSF should be followed to assess treatment response. Molecular biomarkers are not widely used for diagnosis of primary CNS lymphoma; however, there is increasing evidence that MYD88 L265P mutations and elevated levels of interleukin-10 (IL-10) may be reliable CSF biomarkers but require additional validation (28).
Systemic staging of 128 patients with cerebral lymphoma revealed that only five (3.9%) had evidence of occult systemic disease (63). All HIV-positive patients should undergo systemic staging because they have a high incidence of extranodal lymphomas with secondary central nervous system involvement. In both immunocompetent and immunocompromised scenarios, many contemporary clinicians and investigators would favor PET scan of the body to evaluate for occult extra-CNS disease. Bone marrow biopsy may be included as a component of the extra-CNS staging. It is unclear how much this adds to the staging yield. Testicular ultrasound may be considered as well in men to exclude an occult testicular lymphoma metastatic to brain, although it is unclear if this adds additional sensitivity to the staging (63). Furthermore, all patients should have an HIV-1 serology because HIV positivity may influence management.
Contemporary primary central nervous system lymphoma treatment is often divided into induction chemotherapy (when the goal is to achieve a complete radiographic response) and consolidation chemotherapy (when additional therapy is administered to treat any microscopic disease that remains). Conventional therapy for primary central nervous system lymphoma in the past had been whole-brain radiotherapy, which almost always causes tumor regression; however, tumors recur and lead to death within 12 to 18 months for most patients. Gross total resection or surgical debulking offers little or no survival benefit compared to biopsy. However, this view has been challenged by the subset analysis of a large phase III study (83) and subsequent additional investigations (86; 68). The addition of chemotherapy to cranial radiotherapy or the use of chemotherapy alone prolongs life and disease-free survival. The chemotherapy regimens are built around a high-dose methotrexate (HD-MTX) backbone (18; 02; 19; 29; 09; 71).
Survival is enhanced only when the chemotherapeutic drugs employed or the drug delivery method is capable of penetrating the blood-brain barrier. HD-MTX is the single most active agent against cerebral lymphoma. Its optimal dosing is still unclear, with doses up to 8 gm/m2 being utilized routinely. The combination of HD-MTX and whole-brain radiation is associated with an overall 2-year survival of 43% to 73% (26). When combined with chemotherapy, cranial irradiation initially treated the whole brain to a total dose of approximately 4500 centigray; however, more recent studies demonstrate potential benefit from lower doses (33) or from omitting it completely (48). Higher total doses or boosts to areas with bulky disease do not improve local control but does increase toxicity. Focused radiotherapy or stereotactic radiosurgery is associated with high rates of in-field and out-of-field recurrence (75); in turn, it is not often utilized. The neurotoxicity from brain radiation is more pronounced in elderly patients (over the age of 60). Therefore, it is reasonable to defer radiotherapy in this age group, particularly if a complete response is achieved with chemotherapy alone (79). The trend in newer clinical trials and contemporary off-trial management to use more aggressive, multiagent chemotherapy regimens that permit dose reductions or elimination of radiotherapy as initial treatment.
Some combination chemotherapy regimens used for systemic lymphomas are not efficacious in the treatment of primary CNS lymphoma because the most active agents (eg, cyclophosphamide, doxorubicin) cannot penetrate an intact blood-brain barrier (73; 58). High-dose cytarabine, procarbazine, thiotepa, and temozolomide are examples of active agents that can penetrate the blood-brain barrier. It is less clear whether other agents, such as the monoclonal antibody rituximab, provide adequate blood-brain barrier penetration (74; 50; 31; 42; 71).
High-dose chemotherapy with autologous stem cell transplant, a successful regimen used in systemic lymphomas, has also been attempted in primary CNS lymphoma, both in the newly diagnosed (03; 46; 47; 21) and recurrent setting (78; 77). Kasenda and colleagues reported a 5-year overall survival of 82% (median survival 104 months) in 34 patients with newly diagnosed primary CNS lymphoma (age < 67 yrs) who were able to undergo ASCT with tolerable toxicity. In the study reported by Alimohamed and colleagues, all treatment-related mortality occurred in patients over the age of 60 with poor performance status (03). The randomized phase 2 cooperative group study, Alliance 51101, is evaluating the role of ASCT as a consolidation regimen. It has completed accrual, and its final results are eagerly awaited. Preliminary results demonstrate that a substantial proportion of patients could not move forward with consolidation (11). Subsequent results demonstrated that myeloablative consolidation with ASCT was associated with superior 2-year progression-free survival but not 2-year overall survival. Data suggest that stem cell transplantation is feasible even in an elderly population who were previously considered not good candidates for aggressive therapy (72).
The necessity of intrathecal chemotherapy is unknown; the use of high-dose methotrexate achieves therapeutic CSF levels and produces similar results as the combination of systemic and intrathecal therapy. There has been a strong trend away from including intrathecal therapy to treat newly diagnosed primary central nervous system lymphoma at many centers (45).
The optimal treatment for ocular lymphoma is also unknown but should eradicate disease and prevent relapses in the central nervous system. Options include systemic chemotherapy, intravitreal chemotherapy, and/or radiotherapy. Ocular lymphoma may be treated with ocular radiotherapy to a total of 3600 to 4000 cGy; however, this form of local therapy does not prevent or treat primary central nervous system lymphoma. High-dose cytarabine and high-dose methotrexate can reach the vitreous humor and may be useful in treating ocular lymphoma (82; 10). Intraocular injection of methotrexate has also been effective for ocular lymphoma.
Diagnosis of primary brain lymphoma in HIV-positive patients is usually more expeditious now and does not require failure of empiric antitoxoplasmosis therapy that can take weeks, leaving the patient neurologically compromised. The treatment choice is usually determined by the patient’s overall condition and CD4 count. Cranial radiotherapy is used in debilitated patients with very low CD4 counts to achieve rapid palliation. High-dose methotrexate is employed in patients with a good performance status, and it is usually well tolerated (30; 41). Immune reconstitution with antiretroviral therapies plays an important role in the treatment of cerebral lymphoma in HIV-positive patients (71). Regardless of specific therapy, patients may not have the predicted clinical improvement because cerebral infectious processes may coexist with brain lymphoma.
The management of elderly patients with primary central nervous system lymphoma is often made on a case-by-case basis and is influenced, at least in part, by medical comorbidities and their perceived influence on the tolerability of specific treatment regimens. In the sole phase 3 clinical trial (G-PCNSL-SG-1), elderly patients (over 70) appeared to experience decreased benefit and increased toxicity from aggressive chemotherapy (70). These age-related findings have not been seen across all therapeutic trials (71). Although the degree of benefit varies between populations, chemotherapy should be considered the preferred initial treatment for all patients with cerebral lymphoma and should be given before radiation therapy for those patients perceived to be able to tolerate the chemotherapy regimens.
Promising new agents are being investigated in treating primary central nervous system lymphoma. The targeted therapy ibrutinib (a Bruton tyrosine kinase inhibitor), which has proven successful in extra-central nervous system lymphomas, has appeared tolerable in primary central nervous system lymphoma. Early results are promising, and further study results are eagerly awaited (23; 52; 53; 16).
Increasing understanding of the molecular basis of primary CNS lymphoma, especially dysregulation of Toll-like receptor and B-cell receptor signaling, which induce constitutive NFκB activation, has led to the evaluation of multiple signaling pathways that can be exploited therapeutically. Inhibitors of Bruton tyrosine kinase, such as ibrutinib, and mucosa-associated lymphoid tissue lymphoma translocation protein 1 (MALT1), such as lenalidomide or pomalidomide, have been studied and have shown evidence of activity in recurrent primary CNS lymphoma (36; 37; 67).
Immunocompetent patients treated with cranial irradiation alone have a median survival of 12 to 18 months and a 5-year survival of only 3% to 4%. When high-dose methotrexate-based chemotherapy is combined with radiation, the median survival increases to 40 to 60 months (18; 02; 19) with a 5-year survival of 23%. Of note, many therapeutic trials have not reported outcomes out to the 5-year landmark.
Even though immune recovery induced by highly active antiretroviral therapy leads to improved survival of patients with AIDS-associated cerebral lymphoma, overall prognosis remains poor (60; 38). This may, however, change in the contemporary era (45). Treatment of HIV-related primary central nervous system lymphoma leads to a median survival of only 2 to 5 months after cranial irradiation, although a few patients have prolonged survival when chemotherapy is added to radiotherapy (12; 30). Treatment with radiation therapy, completion of radiation therapy, receipt of a total dose of 30 Gray, ongoing therapy with two or more antiretroviral drugs, less than 1e AIDS-defining illnesses, and the absence of nonfocal CNS symptoms (such as confusion, cognitive decline, and memory loss) are associated with prolonged survival (60).
Complications may arise from treatment of primary nervous system tumors. Cranial irradiation combined with chemotherapy is associated with delayed leukoencephalopathy, leading to progressive dementia, ataxia, and urinary incontinence. Symptoms typically occur a median of 1 year after diagnosis and primarily affect patients 60 and older. Leukoencephalopathy can be diagnosed only in the absence of a tumor. Chemotherapy alone has a much-reduced risk of delayed neurotoxicity and is the recommended treatment for patients older than 60. Young age and a good performance status are important prognostic factors for response and survival, regardless of treatment. HD-MTX can crystalize in the renal tubules, leading to renal failure and, in turn, slowing excretion of MTX. The risk of this is decreased with the administration of alkalinized intravenous fluids and oral bicarbonate.
Limited information is available regarding primary central nervous system lymphoma in pregnancy. Pregnancy is not a contraindication to diagnostic biopsy in a patient with an intracranial mass; however, chemotherapy and cranial irradiation should not be administered to pregnant patients because of the risk of fetal damage. A delay in treatment may not adversely affect maternal prognosis, but early delivery to initiate therapy should be considered in patients with significant neurologic deficits (62). Single-agent rituximab has been used as a bridge to definitive therapy in a patient diagnosed during pregnancy (14).
Patients with cerebral lymphoma safely tolerate general anesthesia for craniotomy or stereotactic biopsy procedures.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Karan S Dixit MD
Dr. Dixit of Northwestern University Feinberg School of Medicine has no relevant financial relationships to disclose.
See Profile
Rimas V Lukas MD
Dr. Lukas of Northwestern University Feinberg School of Medicine received honorariums from Novartis and Novocure for speaking engagements, honorariums from Cardinal Health, Novocure, and Merck for advisory board membership, and research support from BMS as principal investigator.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Stroke & Vascular Disorders
Dec. 29, 2024
Neuro-Oncology
Dec. 13, 2024
Neuro-Oncology
Dec. 05, 2024