




Movement Disorders
Acquired hepatocerebral degeneration
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Progressive supranuclear palsy is a late-onset degenerative disease of the central nervous system characterized by balance difficulties, vertical gaze palsy, dysarthria, dysphagia, and axial dystonia. Pathologic findings include neurofibrillary degeneration of extrapyramidal neurons. It remains an intractable and underrecognized neurodegenerative illness with a median survival of only seven years. However, patients will benefit from accurate, early diagnosis that allows them to understand the prognosis, to avoid unnecessary tests and useless treatments, and to avail themselves of disease-specific support services. Advances in understanding the tau protein aggregation and mitochondrial dysfunction of progressive supranuclear palsy and the toxic and genetic insults underlying them are accruing swiftly. In this article, the author describes the subtypes of progressive supranuclear palsy as well as advances in pathology, imaging, and genetics of the disorder.
|
• Ophthalmoparesis, especially downgaze impairment, is a classic clinical feature of progressive supranuclear palsy that may appear later in the course of the disorder. | |
|
• Slowing of downward saccades appears earlier in the clinical course of progressive supranuclear palsy. | |
|
• Multiple subtypes of progressive supranuclear palsy have been identified, including the classic Richardson syndrome, progressive supranuclear palsy-parkinsonism (PSP-P), or pure-akinesia-with-gait-freezing (PAGF). |
The first complete clinicopathologic description of progressive supranuclear palsy was published in 1964 (146). However, there were 13 earlier clinical cases in the literature, six with autopsy (19). Some of these antedate the 1920s epidemic of postencephalitic parkinsonism, suggesting that progressive supranuclear palsy is not a variant of that condition despite their pathological similarity (20). The meticulously described motor disorder of a character in an 1857 Dickens novel is a convincing picture of progressive supranuclear palsy (88). Since the early 1960s when many astute movement disorder specialists were unable to recall having seen progressive supranuclear palsy, this disorder has become commonly recognized at movement disorder referral centers, comprising 4% to 5% of their cases of parkinsonism (46).
Monographs (93; 19) and a layperson's guide (44) are available. Lay organizations were founded in the United States in 1990 (The Society for Progressive Supranuclear Palsy) and in Europe in 1994 (The Progressive Supranuclear Palsy (PSP-Europe) Association).
Progressive supranuclear palsy is often initially misdiagnosed as Parkinson disease for at least the first 3 or 4 years after onset. Like Parkinson disease, it results in rigidity, bradykinesia, postural instability, dysarthria, dysphagia, and, in many cases, dementia. Unlike Parkinson disease, however, there rarely is tremor; postural instability is an early rather than later symptom; rigidity is worse at the neck than in the limbs; dysarthria is spastic, ataxic, and hypophonic rather than purely hypophonic (101; 77); dysphagia may be more symptomatic than in Parkinson disease because of its prominent oral component (143). Ling and colleagues showed micrographia without decrementing amplitude and lack of decrementing amplitude on finger taps progressive supranuclear palsy patients compared to Parkinson disease patients (92). Disease progression causes reduction of horizontal and vertical saccade amplitudes in progressive supranuclear palsy, but not Parkinson disease patients (148).
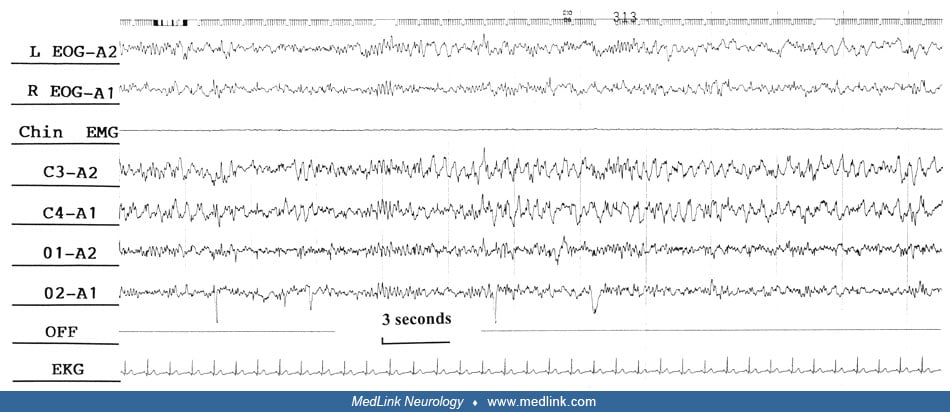
The most frequent initial symptom is postural instability, often taking the form of unheralded falls that prompt a workup for vestibulopathy, syncope, basilar ischemia, or epilepsy. This symptom usually remains the most disabling feature of progressive supranuclear palsy. The next most frequent presenting feature is mental disturbance in the form of personality change, emotional incontinence, or depression. Consequently, the first medical contact is sometimes a psychiatrist (46). The dementia is usually frontal in quality (49). One sign of frontal lobe dysfunction typically present in progressive supranuclear palsy is the “applause sign” (“signe de l’applaudissment”). This probably represents perseveration of automatic behavior (37). Patients with higher degrees of frontal lobe dysfunction exhibit the “jumping the gun” sign, which is defined as premature initiation of clapping before the start signal from the examiner (04). Purposeless groaning has also been reported in progressive supranuclear palsy (99). Sleep disturbances are disabling for some patients (05).
The best-known feature of progressive supranuclear palsy, but one that may be late or not obvious, is impairment of ocular gaze, particularly in the downward direction.
A highly common early finding is slowing of downward saccades, which remain normal in amplitude until later in the course. Frequent associated ocular findings are horizontal square-wave jerks, slow and hypometric saccades, and paresis of upward gaze (122; 149). Impairment of downward opticokinetic nystagmus can help distinguish progressive supranuclear palsy from Parkinson disease (42). Lateral gaze paresis may occur late. Zwergal and colleagues show slower progression of horizontal gaze paresis compared to vertical and range of ocular motility in smooth pursuit decrease of 1.5 mm/year on upgaze, 1.6 mm/year on downgaze, and 1.4 mm/year on horizontal gaze (171).
"Apraxia" of lid movement and blepharospasm are common and the blink rate averages three to five per minute (normal 20 to 30 per minute) (45).
Approximately one third of patients with pathologically proven progressive supranuclear palsy present with relative asymmetry, tremor, and a useful, if transient, levodopa response that often prompts a diagnosis of Parkinson disease. Williams and colleagues named this variant “progressive supranuclear palsy-parkinsonism” (PSP-P) and the classic syndrome that comprises about half of all progressive supranuclear palsy patients, “Richardson syndrome” (PSP-RS) (163). The Richardson disease variant displays greater intensity of tau pathology than the progressive supranuclear palsy-parkinsonism (PSP-P) or pure-akinesia-with-gait-freezing (PAGF) variants (166). PAGF presents with early gait disturbance, micrographia, hypophonia, and eventual gait freezing (165). In studies of PAGF patients, severe atrophy has been found only in the globus pallidus, substantia nigra, and subthalamic nucleus (165). Progressive supranuclear palsy with corticobasal syndrome and progressive supranuclear palsy with speech apraxia have also been reported (89). PSP-pallido-nigro-luysian atrophy (PSP-PNLA) cases typically present younger and with earlier gait impairment, but later dysphagia than PSP-RS (03). A syndrome with falls, cerebellar ataxia, and supranuclear gaze palsy without dysautonomia has been proposed as progressive supranuclear palsy with predominant cerebellar ataxia (PSP-C) (72). Additional nonmotor symptoms are present in progressive supranuclear palsy. Sleep and mood issues, urinary frequency, nocturia, and constipation were reported in a study of 50 consecutive progressive supranuclear palsy patients (124). Cognitive dysfunction is also present and is associated with severity of progressive supranuclear palsy-related tau pathology (79). Apraxia of speech may be an early sign of progressive supranuclear palsy, but it can also be present in other disorders, such as corticobasal syndrome (121). Protracted coursed progressive supranuclear palsy (PC-PSP) has been described with an 11-year-old clinical course (40).
The diagnosis is typically first suspected by a physician noticing poor levodopa response and vertical gaze restriction in a parkinsonian patient. Clues that may aid earlier diagnosis are spastic or ataxic speech, contracted facies, slow downward saccades (albeit with normal amplitude at first), erect or hypererect posture, and a disorganized, ataxic-appearing gait with falls early in the disease course. In a study of 339 not demented progressive supranuclear palsy patients meeting the NINDS-SPSP, 221 of whom were considered “frequent fallers”, symptom duration, clinical measures of disease severity, and several motoric and oculomotor clinical parameters were associated with frequent falls (12).
Clinical presentation of corticobasal syndrome may be due to progressive supranuclear palsy pathology, and is termed PSP-CBS. More cortical tau burden in PSP-CBS corresponds with clinical findings of corticobasal syndrome such as apraxia (91). In addition, corticobasal degeneration pathology may present as a PSP clinical diagnosis (CBD-PSPS). Clinical progressive supranuclear palsy syndrome (PSPS) correlates with midbrain atrophy. Patients with progressive supranuclear palsy pathology but without PSPS did not have appreciable midbrain atrophy (160). Diffusion tensor imaging of nine CBS subjects (unknown pathology) compared to 18 probable or definite PSP cases, nine of whom were pathologically confirmed, showed more symmetric degeneration in PSP with more degeneration of the superior cerebellar peduncle and midbrain (162). The phenotypic spectrum of progressive supranuclear palsy is enlarging, with individual case reports of cerebellar ataxia and orthostatic hypotension in pathologically confirmed progressive supranuclear palsy.
MDS-PSP diagnostic criteria published by Hoglinger and colleagues include four domains (oculomotor dysfunction, postural instability, akinesia, and cognitive dysfunction), with levels of certainty based on clinical findings in each domain, for example, vertical supranuclear gaze palsy being more certain than slowing of vertical saccade velocity (62).
The median interval from onset of the initial symptom, regardless of its nature, to onset of gait difficulty is 0.3 years; to the need for gait assistance, 3.1 years; dysarthria, 3.4 years; visual symptoms, 3.9 years; dysphagia 4.4 years; and death 7.3 years (46; 47). The problems that most frequently cause complications or death are falls and dysphagia with aspiration.
A 66-year-old woman began to experience diplopia and suffered one fall while running on uneven ground. Within the next few months, she acquired a staring expression, nonfluency of speech, a sustention tremor of both hands, and she suffered two more falls. One year after onset, she consulted a neurologist, who found square-wave jerks, slow and hypometric saccades with slowing worse in the downward direction, limitation of upgaze but not downgaze, mild rigidity at the wrists, wide-based gait, and a tendency to retropulse. MRI was normal. The diplopia responded modestly to prisms. Treatment with carbidopa and levodopa 25/100 four times daily gave no benefit, caused mouth dryness, and was subsequently reduced to three times daily. Amantadine 100 mg twice a day and sertraline at an unknown dosage gave no benefit or adverse effects.
Three years after onset, the patient was suffering from moderate social withdrawal, mild dysphagia for both fluids and solids (which had to be cut into small pieces), slowness in all manual activities, at least one fall per day if she walked unassisted, consistent urinary incontinence, and both primary and secondary insomnia. Examination revealed normal orientation and memory, mild bradyphrenia, a moderate degree of frontal behavioral disturbance, contracted facies, reduction of saccadic amplitudes (up, 5 degrees; down, 20 degrees; right, 35 degrees; left, 40 degrees) (normal is 50 degrees in each direction), frequent, large-amplitude square-wave jerks, inhibition of lid closing, mild spastic dysarthria, slowed swallowing of water with no aspiration, moderate neck rigidity, symmetric limb rigidity, slowing of distal rapid alternating movements, mild sustention tremor of the right hand, wide-based irregular gait requiring occasional reliance on walls or furniture, and an inability to recover from the pull test. The score on the PSP Rating Scale (0=normal, 100=worst possible) was 46.
Titration of carbidopa and levodopa to 1500 mg (of levodopa) per day gave no benefit and caused fatigue. Oxybutynin 5 mg twice daily helped the incontinence transiently. Amitriptyline titrated to 50 mg twice daily helped the balance and speech markedly for 4 or 5 weeks, when those symptoms returned to baseline. Confusion occurred two months later and the amitriptyline was tapered and discontinued with return of mentation to baseline and no worsening of gait.
Over the following year, the PSP Rating Scale score progressed gradually to 65, with progression of the frontal behavior, loss of all command eye movement, immobility of the neck to active and passive movement, and a need for major assistance in gait. There was only mild progression of dysphagia and no worsening of limb rigidity. Three months later, six years after symptom onset, the patient developed pneumonia and sepsis and died.
Brain autopsy showed neurofibrillary tangles 4+ in the subthalamic nucleus; 3+ in the striatum, globus pallidus, substantia nigra, locus ceruleus, and pontine base; 2+ in premotor and motor cortex, nucleus basalis, ventral thalamus, oculomotor nucleus, periaqueductal gray, medullary tegmentum, inferior olive, and cerebellar dentate; and 1+ in temporal cortex, red nucleus, and raphe nuclei. Neuronal loss was most marked in the subthalamic nucleus and in the ventral and lateral tier of the substantia nigra; it was moderate in the ventral and lateral thalamus. These changes are typical of progressive supranuclear palsy.
One case-control study failed to find any premorbid correlates of progressive supranuclear palsy among the many risk factors that have been associated with, or suspected of association with, other neurodegenerative disease (34), but another study found an association with lower educational attainment (48). The island of Guam in the Pacific and Guadeloupe in the Caribbean each harbors a cluster of patients with a different progressive supranuclear palsy-like disorder (24; 145). There have been no clear occupational or temporal clusters of progressive supranuclear palsy, but seven autopsy-proven familial clusters from five countries have been reported (128). Relatives of patients with progressive supranuclear palsy are more likely than controls to have parkinsonian signs or symptoms (34).
Further evidence for a genetic etiologic component is a well confirmed but weak association of the disease with the H1 haplotype of the gene for tau (30; 09; 57), a protein that forms abnormal intracellular aggregates in progressive supranuclear palsy.
Progressive supranuclear palsy is one of the tauopathies. The pathologic hallmarks are neuronal loss, gliosis, and flame-shaped and globose neurofibrillary tangles (NFT) composed of paired helical filaments and straight filaments of tau protein (68; 55). The tangles are similar to those in Alzheimer disease, but the tau protein consists almost solely of an isoform with four repeating copies of the microtubule-binding domain (4R-tau), rather than the 1:1 ratio of 3-repeat (3R-tau) and 4-repeat isoforms occurring in Alzheimer disease and in normals (25). Intronic variant rs564309 minor allele A in tripartite motif containing 11 (TRIM11) has been found to be associated with neurofibrillary tangles and is less common in PSP-RS than other phenotypic variants (151). In addition to NFT pathology, increased levels of phosphorylated and unphosphorylated tau oligomers have been demonstrated by Gerson and colleagues (43). Alternative splicing of the MAPT gene leads to expression of different tau isoforms. 4R-tau results from inclusion of exon 10 (100). Smith reports that microRNA-132 loss is associated with abnormal splicing of exon 10 (140). microRNA-132 appears to affect the neuronal splicing factor PTBP2 leading to imbalance in the 4R-tau to 3R-tau ratio. Six Japanese patients with early-onset progressive supranuclear palsy were found to have MAPT p.S285R mutations (115).
Progressive supranuclear palsy exhibits no amyloid deposition or apolipoprotein E allelic association (07). There is evidence that mitochondrial genetic defects (147), abnormal oxidation (29), and inappropriate transglutamination (75) contribute to the tau aggregation and cellular loss.
In a genome-wide association study, Jabbari and colleagues found a possible survival benefit with rs2242367, which affects levels of LRRK2 expression (65). Further research in model systems is needed to confirm the clinical relevance of this finding (28).
Phosphorylation is important for regulation of tau binding to microtubules and affects the association of tau with plasma membranes and nuclei. Glycogen synthase kinase-3 (GSK-3) mediated tau phosphorylation may play a role in pathogenesis of tauopathies. For example, axonal damage and motor impairment resulting from 4R tau overexpression in a mouse model is ameliorated with GSK-3beta expression (54).
The damage is greatest and most consistent in the substantia nigra, subthalamic nucleus, globus pallidus, superior colliculus, pretectal area, and substantia innominata (01). Cortical neuronal involvement has been documented (55), and thalamic relays to cortex have been found to be involved (56). Red nucleus, medulla, and dentate nucleus involvement has also been reported (165). In both PSP-P and Richardson syndrome, damage to subthalamic nucleus and substantia nigra are greatest. Less severe damage to parts of the midbrain other than substantia nigra in PSP-P may contribute to presence of tremor and moderate levodopa responsiveness in this variant (165). Temporal lobe structures with connections to the superior colliculus are involved with generation of the classic side-to-side movement seen with fixation termed “square wave jerks” (02). Kovacs and colleagues propose a sequential model of neuronal tau pathology spread in progressive supranuclear palsy (84). According to their model, neuronal tau pathology starts in the subthalamic nucleaus, substantia nigra, and globus pallidus and spreads to the midbrain and pons. The next step would be to the cerebellum and amygdala, followed by the frontal lobe, the parietal and temporal lobes, and, finally, the occipital lobe.
Dopaminergic, cholinergic, GABAergic, and adrenergic neurotransmitter systems are affected. The poor levodopa responsiveness may be the result of loss of cholinergic interneurons in the striatum, onto which synapse the dopaminergic terminals of the nigrostriatal tract, or of the internal segment of the globus pallidus, the major outflow from the basal ganglia. However, this explanatory model has been called into question (157). Mean cortical acetylcholinesterase activity was shown to be significantly reduced in progressive supranuclear palsy as compared to controls (59). Dementia Rating Scale impairment was seen in 57% of a group of 311 progressive supranuclear palsy patients, indicating a high level of cognitive dysfunction in this disorder (18). Mild deficits in autobiographical memory without temporal gradient were found in progressive supranuclear palsy patients, indicating a likely frontal retrieval deficit (169).
The first transgenic animal model of progressive supranuclear palsy has appeared (90). A toxin model using intravenous annonacin, a component of the tropical fruits associated with the progressive supranuclear palsy-like illness on Guadeloupe, has been reported (26).
Genetics. The H1 haplotype of the tau gene on chromosome 17q21 (93.7% vs. 78.4%) and the H1/H1 genotype (87.5% vs. 62.8%) are overrepresented to a modest but statistically significant degree in patients with progressive supranuclear palsy compared to controls (09). Both H1 and H1/H1 are also overrepresented in corticobasal degeneration (63) and, to a slightly lesser degree, in Parkinson disease. Patients with progressive supranuclear palsy who are H1/H2 heterozygotes may display a lesser tau burden at autopsy than H1/H1 homozygotes (164). However, the Richardson disease and progressive supranuclear palsy-parkinsonism phenotypes do not differ with regard to H1 haplotype frequency (166). The H1c haplotype, which is more specifically associated with progressive supranuclear palsy than other H1 subhaplotypes, increases expression of tau, especially of the 4-repeat variant, which includes the product of exon 10, the location of one of the microtubule-binding repeat domains (23; 108). Patients homozygous for the H1 haplotype may have earlier onset age, according to one study, but apolipoprotein E status has no effect on the disease course despite its effect on Alzheimer disease (08).
Although the tau mutations in frontotemporal dementia and parkinsonism linked to chromosome 17 (FTDP-17) affect microtubule binding domains of the C-terminus of the tau protein, the progressive supranuclear palsy variants affect domains that interact with the neural plasma membrane. FTDP-17 is a primary tauopathy with overlap of pathological features with progressive supranuclear palsy, Alzheimer disease, corticobasal degeneration, and Pick disease (165). Clinically typical progressive supranuclear palsy is most likely associated with the tau progressive supranuclear palsy susceptibility genotype (H1/H1) and doublet tau protein pattern (64 and 69kDa) (107). The pathogenic effect of the H1 haplotype may be a simple overexpression of tau protein via a variant in the tau promoter that is part of the haplotype (87). Or the pathogenic locus may exist at a distance from the tau gene itself, as the H1 haplotype includes multiple flanking genes in 5’ and 3’ directions (117). One promising lead is that a single base substitution in a regulatory region of the tau gene has been found to be the statistically most critical variant in the H1 haplotype (123). Although progressive supranuclear palsy is almost always sporadic, rare families with the phenotype have been reported, a few of which have point mutations in the tau gene, similar to families with frontotemporal dementia linked to chromosome 17. Zhao and colleagues propose that apoptosin-mediated caspase cleavage of tau plays a role in the pathogenesis of progressive supranuclear palsy (170). Imaging studies with 18F-AV-1451 radioligand for tau do not reflect the tau pathology of progressive supranuclear palsy in cortex and white matter, perhaps due to decreased tau burden relative to Alzheimer disease and less binding to 4R filaments. There is increased basal ganglia binding of this radioligand, but it is unclear if this is true tau pathology or off target binding (120; 142). In later studies, 18F-AV-1451 (also named 18F-T807 or 18F-Flortaucipir) was able to differentiate between progressive supranuclear palsy and Alzheimer disease pathology (141).
A genome-wide association study found increased risk of progressive supranuclear palsy associated with eukaryotic translation initiation factor 2-alpha kinase 3 (EIF2AK3), myelin-associated oligodendrocyte basic protein (MOBP), and syntaxin-6 (STX6) as well as variants of the gene coding for tau protein (61). A genome-wide association study by Chen and colleagues confirmed association with chromosome 17 at or near the MAPT gene (27). A metaanalysis by the same authors confirmed association of rs1768208 polymorphism of the MOBP gene with progressive supranuclear palsy (27). This polymorphism was associated with white matter variance in the midbrain and superior longitudinal fasciculus in sporadic frontotemporal lobar degeneration cases (106). In another genome-wide association study involving 152 corticobasal degeneration cases and 3311 controls, and 67 corticobasal degeneration cases and 439 controls in a replication stage, an association was found with MAPT at 17q21 (which codes for tau protein) and with MOBP at 3p22 (which codes for MOBP) (82). The authors concluded that corticobasal degeneration and progressive supranuclear palsy share a genetic risk factor at these two loci.
Linkage to 1q31.1 has been demonstrated in one large Spanish family (129). Another locus, at chromosome 11p11-p12, has been incriminated by pooled genome-wide analysis. The two leading candidate genes in that interval participate in DNA repair and in lysosomal function (103). Increased risk of progressive supranuclear palsy and corticobasal degeneration has been reported with VEGF mutations (14).
STX6, EIF2AK3, and MOBP genes on chromosomes 1, 2, and 3, respectively, have been implicated by genome wide association studies, but direct coding changes in these genes could not be identified (39). Sanchez-Contreras and colleagues confirmed these GWAS associations and included SLCO1A2 (rs11568563) and DUSP10 (rs6687758) (131).
An unusual case of familial PSP-P phenotype was identified with sequence variants in the FBXO7 and VPS35 genes and neuropathology consistent with Braak stage VI Parkinson disease as opposed to the classic tau pathology (105). The patient had poor response to levodopa. However, the authors also describe that the patient had hallucinations requiring quetiapine, which is not classic for PSP (10). Given that hallucinations were found by a different group in a VPS35 carrier (139), clinically and pathologically this case may perhaps be viewed as PARK17 parkinsonism with hallucinations as opposed to PSP-P.
A single case of simultaneous presentation of progressive supranuclear palsy and behavior variant of frontotemporal dementia was reported due to a sporadic mutation in the progranulin (GRN) gene (c.1498G> A, p.V500I) (35).
Two separate surveys in the United Kingdom found the age-adjusted prevalence of progressive supranuclear palsy to be approximately 5 per 100,000 population, about 3% to 5% of the prevalence of Parkinson disease (136; 109). Men appear to be slightly more frequently affected than women. Approximately half of the patients with progressive supranuclear palsy experience the initial symptoms during their 60s, with one fourth each in their 50s and 70s (101; 46). However, the age-specific incidence is highest in the oldest measurable decades (15).
Parkinson disease is the condition most frequently confused with progressive supranuclear palsy. Its variant, dementia with Lewy bodies, can resemble progressive supranuclear palsy, but with more dementia. The combination of frequent square-wave jerks and low blink rate may provide a clinically convenient distinction of progressive supranuclear palsy from Parkinson disease (06). Multiple system atrophy, parkinsonian type (formerly known as “striatonigral degeneration”), usually has less vertical gaze palsy and more dysautonomia than progressive supranuclear palsy (76), but a case report of pathologically confirmed progressive supranuclear palsy with dysautonomia has been presented (104). A multi-infarct state (167) would feature vascular abnormalities on MRI and usually pyramidal signs or focal cortical deficits. Corticobasal degeneration is far more asymmetric than progressive supranuclear palsy and exhibits more apraxia and cortical sensory loss. Patients with progressive supranuclear palsy pathology at autopsy have been described to have clinically manifest corticobasal syndrome (PSP-CBS) (91).
Less important considerations that can mimic progressive supranuclear palsy, particularly by virtue of producing vertical gaze palsy, are multiple system atrophy, the parkinsonism-dementia-amyotrophic complex of Guam, Whipple disease, neuroacanthocytosis, progressive external ophthalmoplegia, and hydrocephalus. For patients with only bulbar signs, myasthenia gravis or motor neuron disease should be considered. Dorsal midbrain mass lesion from cysticercosis may approximate some features of progressive supranuclear palsy including gaze palsy and falls (138). A progressive supranuclear palsy-like phenotype has also been reported with hypoxia (74). In addition to the choreic phenotype, Niemann Pick disease type C may have a phenotype consisting of ataxia and supranuclear gaze palsy, which may be confused with progressive supranuclear palsy (85).
One progressive supranuclear palsy–like phenotype that is increasingly recognized is anti-IgLON5 disease (41; 50). This autoimmune disorder associated with anti-IgLON5 antibodies is characterized by a complex sleep disorder, rapid periodic leg movements during wakefulness that may briefly continue following sleep onset, cognitive decline, severe gait instability, chorea predominantly affecting the limbs (also orofacial dyskinesia), and oculomotor dysfunction similar to that observed in patients with progressive supranuclear palsy. At autopsy these patients may have characteristic aggregates of tau protein in the tegmentum and brainstem. Patients with this disorder respond poorly to immunosuppressive therapy and may die of sudden death during sleep or wakefulness. It appears that the IgLON5 autoantibodies are directed predominantly against brainstem and hypothalamic neurons.
Clinical diagnostic criteria have been formulated using a large autopsy series (94). Beyond a careful physical examination, MR imaging is the only workup required for most people suspected to have progressive supranuclear palsy. MRI’s principal goal is to rule out a multi-infarct state or hydrocephalus. Midbrain atrophy disproportionate to that of the pons or cerebellum is a specific but not a highly sensitive sign of supranuclear palsy (134; 132; 31). According to Massey and colleagues, sagittal midbrain measurement of <9.35 mm and midbrain to pontine base ratio of 0.52 provided 100% specificity for progressive supranuclear palsy, as opposed to multiple system atrophy, Parkinson disease, or normal controls (102). A study of 23 PSP-RS patients and 42 Parkinson disease patients found 99% diagnostic accuracy when differentiating these disorders via midbrain area (168). The marked midbrain atrophy when viewed on sagittal MRI suggests the image of a “penguin” or of a “hummingbird” (114; 97; 161). Clinical decline is correlated with frontal lobe and midbrain atrophy (71). Primary progressive apraxia of speech was noted to have midbrain atrophy, but milder than in progressive supranuclear palsy, suggesting a possible relationship between the disorders (159).
Disproportionate atrophy of the superior cerebellar peduncle on MRI can also help distinguish progressive supranuclear palsy from its close mimics, including multiple system atrophy (118). In addition, there are differences in superior cerebellar peduncle imaging between PSP-RS and PSP-PD. An automated system to analyze the superior cerebellar peduncle has been proposed (110). An “eye-of-the-tiger” sign, high T2 signal in a V formed by the lateral and medial putamen with normal signal between them, occurs in a minority of patients (132). Diffusion tensor imaging (DTI) evaluation of progressive supranuclear palsy versus controls reveals sensitive (0.92) and specific (1.0) differences in radial diffusivity in the superior cerebellar peduncle (78). This is in contrast to middle cerebellar peduncle and pontine crossing tract DTI changes in moderate to advanced MSA (113). Interestingly, the apparent diffusion coefficient MRI sequence has been reported to show increased signal in the middle cerebellar peduncle of progressive supranuclear palsy that is absent in MSA of the parkinsonian type and in other progressive supranuclear palsy mimics (119). However, another study shows that Richardson syndrome has been found to have statistically significant differences in average apparent diffusion coefficient (ADCave) values in the superior cerebellar peduncle on magnetic resonance imaging as compared to Parkinson disease and healthy volunteers (126). Whitwell and colleagues demonstrated disruption of thalamic connectivity with superior cerebellar peduncle degeneration in progressive supranuclear palsy, likely due to dentatorubrothalamic tract degeneration (158). Mean diffusivity in the vermis is higher in patients with PSP-RS, as opposed to patients with Parkinson disease or healthy subjects. Evaluation of mean diffusivity in the entire cerebellar hemisphere via median values allows for differentiation between multiple system atrophy and PSP-RS (111).
Both SPECT (51) and PET using deoxyglucose (17) show prefrontal hypoactivity in progressive supranuclear palsy. PET imaging of dopaminergic terminals shows severe involvement of the caudate and putamen in progressive supranuclear palsy, but relative sparing the caudate in Parkinson disease (22). Tau-PET tracers (F-FDG and F-THK5351) have been used on a research basis (98). Magnetic resonance spectroscopy of the lentiform nuclei can distinguish progressive supranuclear palsy from normal and from Parkinson disease (33). Transcranial 2-D ultrasound has been reported to discriminate progressive supranuclear palsy, which displays hyperechogenicity of globus pallidus but not substantia nigra, from Parkinson disease, where the opposite pattern occurs (156; 155). However, it has not been established that any of these tests can more accurately distinguish early or equivocal progressive supranuclear palsy from its mimics than can a good history and neurologic examination. Early (first 10 minutes) perfusion dominant imaging with F-FP-CIT PET (pCIT) may provide discrimination between Parkinson disease and progressive supranuclear palsy additional to classic dopamine transporter imaging (69). The PET ligand [18F]-AV-1451 has shown abnormal binding in bilateral pallidum and rostral interstitial nucleus of the medial longitudinal fasciculus in a case report of a single patient with clinical diagnosis of Richardson syndrome (53). 11C-pyridinyl-butadienyl-benzothiazole 3 (C-PBB3) positron emission tomography may help in differentiating between progressive supranuclear palsy and corticobasal syndrome as well as Alzheimer disease (135).
The pontine nuclei, dentate nucleus, and cerebellum are less affected in PAGF as compared to Richardson syndrome. Functional scans reveal normal frontal lobe metabolism in PAGF (165). Diffusion tensor imaging (DTI) shows diffuse involvement of the thalamus in progressive supranuclear palsy, most prevalent in the anterior aspect, including the anterior and medial nuclei. In corticobasal degeneration, there is asymmetric involvement of the motor thalamus (38). DTI also shows inferior fronto-occipital fasciculus changes in progressive supranuclear palsy patients, especially those with severe frontal cognitive symptoms versus controls (86).
A clinical syndrome of corticobasal degeneration may be due to progressive supranuclear palsy pathology (PSP-CBS) (70). Corticobasal degeneration pathology, in turn, may cause a Richardson syndrome phenotype (83). Postural instability occurs later than in Richardson syndrome (154). Progressive non-fluent aphasia may also be due to progressive supranuclear palsy pathology (70).
The Progressive Supranuclear Palsy Rating Scale (PSPRS) can monitor the clinical state and provide prognostic information (47). A copy is available at the following website: http://www.psp.org. A neural network model of PSPRS and Unified Parkinson Disease Rating Scale (UPDRS) data found individual scale items that were associated with frequent fallers and may be amenable to rehabilitation or other interventions. These include PSPRS arising from chair, gait, and sitting down parameters (11).
A clinical scale measuring quality-of-life is also now available (137).
Biomarker research shows lower CSF N-terminal and C-terminal tau protein concentrations in progressive supranuclear palsy compared to normal controls and Alzheimer disease (153). Decreased p-tau levels and CSF neurofilament light chain are being investigated as biomarkers for progressive supranuclear palsy (64). Skin biopsy and evaluation with antibodies for phosphorylated tau are also being investigated (127). Volumetric MRI changes correlate with disease progression (150).
Drug treatment of progressive supranuclear palsy remains unsatisfactory (81). There is no disease-modifying therapy, but one longitudinal study suggested a potential protective role of lifetime estrogen exposure (116). Levodopa ameliorates the bradykinesia and rigidity in about one third of cases but the benefit rarely persists beyond 1 or 2 years (66; 67; 112). Patients with progressive supranuclear palsy are relatively resistant to dopaminergic motor and psychiatric side effects, so large dosages (up to 2000 mg per day, with decarboxylase inhibitor) are usually well tolerated and are worth a trial. Levodopa improved dysphagia in a series of three patients (152).
Amitriptyline and amantadine can ameliorate certain deficits in progressive supranuclear palsy, but anticholinergic side effects often limit their use and adequate controlled trials are lacking (112). Centrally acting cholinergic medication, despite the profound cholinergic deficit in progressive supranuclear palsy, has been disappointing or deleterious (96; 95). Behavioral issues such as apathy and impulsivity can exist in up to two thirds of patients (80). Behavioral symptoms and impaired activities of daily living were the main drivers of caregiver burden in progressive supranuclear palsy (73).
A speech pathologist can help manage the dysphagia and perhaps institute a communication method for dysarthric patients. Feeding gastrostomy should be considered after the first confirmed episode of frank aspiration or of aspiration pneumonitis, if the patient requires more time to finish a meal than the household can practically provide, if there is significant weight loss because of reduced intake, or if a minor degree of aspiration occurs with every mouthful.
Rehabilitation strategies for progressive supranuclear palsy have been proposed, but no outcome data are available on more than one or two patients in any protocol, and no crossover or parallel control data are available. It is important to modify the home environment to reduce the potential injury from falls. Electroconvulsive therapy, adrenal striatal implantation, and pallidotomy are of no benefit. Blepharospasm responds well to botulinum toxin injection, and dry eyes from infrequent blink can be treated with topical lubricants. Botulinum toxin injections into neck flexor muscles for torticollis dystonia are inadvisable because of the risk of exacerbating the dysphagia, but injection into the extensor muscles for disabling retrocollis is often successful. Deep brain stimulation surgery of the pedunculopontine nucleus has been tried with some success in small, open-label case series (36), but unilateral surgery did not improve balance or falls in a prospective trial with patients randomly assigned to 1-week blocks of stimulation ON or OFF settings in a double-blind fashion (133).
Clinical trials of disease-modifying therapy included the glycogen synthase kinase 3 beta (GSK3b) inhibitor and tideglusib (NP-12) (13). Tideglusib failed to meet the Tauros clinical trial primary end point of improvement in overall clinical status, but there is reduction of global brain atrophy on this treatment (60). Lithium was not tolerated, but sodium valproate continues to be investigated in progressive supranuclear palsy for its GSK-3 inhibition. Unfortunately, trials of riluzole and rasagiline were unsuccessful (125). Tau aggregation inhibitor davunetide, an 8 amino acid peptide, failed to show neuroprotection in progressive supranuclear palsy. There was no improvement in progressive supranuclear palsy rating scale or Schwab and England Activities of Daily Living (SEADL) scale over placebo in the davunetide study (16). A subgroup analysis of patients in the davunetide study looking at amantadine showed a potential benefit on SEADL, which became statistically nonsignificant after correcting for age, baseline PSPRS, and coenzyme Q10 use (58). The authors suggested a study to specifically analyze amantadine in progressive supranuclear palsy. Pyruvate, creatine, and niacinamide are being studied to address mitochondrial dysfunction (144). Research therapies aimed at tau have not been successful (32).
Open label cerebellar transcranial magnetic stimulation with intermittent theta burst improved cerebellar functional connectivity as measured by resting state fMRI (21). A standardized progressive supranuclear palsy rating scale (PSPRS) has been developed to increase consistency in clinical studies (52).
No cases of progressive supranuclear palsy during pregnancy have been reported.
Patients with any form of parkinsonism should avoid neuroleptic tranquilizers. The dysphagia of progressive supranuclear palsy dictates special precautions against aspiration. The retrocollis of progressive supranuclear palsy may narrow the airway, requiring tracheostomy for intubation (130).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Robert Fekete MD
Dr. Fekete of New York Medical College received consultation fees from Acadia Pharmaceutical, Acorda, Adamas/Supernus Pharmaceuticals, Amneal/Impax, Kyowa Kirin, Lundbeck Inc., Neurocrine Inc., and Teva Pharmaceutical, Inc.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Movement Disorders
Jan. 20, 2025
Movement Disorders
Dec. 29, 2024
Neurogenetic Disorders
Dec. 26, 2024
Neurogenetic Disorders
Dec. 13, 2024
General Child Neurology
Dec. 01, 2024
Neurobehavioral & Cognitive Disorders
Nov. 28, 2024
General Neurology
Nov. 25, 2024
Neurobehavioral & Cognitive Disorders
Nov. 15, 2024