

















General Neurology
Renal failure: neurologic complications
Jan. 28, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Estrogens, progestins, and androgens represent the three major classes of endogenous sex steroids. Prototypical hormones in each class are estradiol, progesterone, and testosterone, respectively. The prototypical hormones in each class include 17beta-estradiol, progesterone, and testosterone. Estetrol is a natural estrogen with important antioxidative activity.
It is very well-recognized that many neurologic conditions are triggered by hormonal imbalance changes associated with the menstrual cycle, pregnancy, menopause, and use of oral contraceptives. Besides their effects on reproduction, estrogens exert neuroprotective effects against development or progression of brain diseases. Thus, estrogens improve the negative aspects of aging and some age-associated diseases in affecting the nervous system, including hypertension. Advances in laboratory testing have increased the visibility of hormone-binding sites within the nervous system.
A more thorough understanding of the sex hormone-related neural function and dysfunction may permit rational hormonal and antihormonal therapies for many of the conditions.
|
• Plasma sex hormones are secreted from ovaries, testes, and adrenal glands but may also be derived from enzyme-mediated conversions of prohormones in extraglandular tissues. | |
|
• Sex hormones influence a broad spectrum of normal and abnormal neurologic functions. | |
|
• The immune, endocrine, and nervous systems communicate with each other through a myriad of various molecules, including cytokines, hormones, and neurotransmitters. | |
|
• Relationships between endogenous and exogenous sex hormones influence the development and progression of many neurologic conditions including migraine, stroke, and certain movement disorders like chorea, are well established. | |
|
• The effects of sex steroids on neurologic function in health and disease constitute a rapidly developing area of basic and clinical neuroscience. | |
|
• Fluctuating sex hormone levels also influence the expression of certain neuropsychiatric states and neuroendocrine disorders. |
A “steroid” is a biologically active four-ring organic compound with a specific chemical configuration. The steroid core structure is composed of 17 carbon atoms, bonded in four fused rings: three six-member cyclohexane rings (rings A-C) and one five-member cyclopentane ring (ring D).
Steroids vary by the functional groups attached to this 4-ring core and by the oxidation state of the rings. Steroids serve as important fluidity-altering components of cell membranes and as signaling molecules.
A “steroid hormone” is a steroid that acts as a hormone. Steroid hormones can be grouped into two classes: (1) corticosteroids (including mineralocorticoids), made in the adrenal cortex; and (2) sex steroids, primarily made in the gonads or placenta. So-called female sex hormones are progestogens and estrogens whereas male sex hormones are androgens. Despite the designations of “male” and “female” for classes of sex hormones, both sexes make some of each class, although the amounts differ across the sexes.
The biosynthesis of steroid hormones derives from cholesterol, a molecule with four linked rings and 27 carbons.
Cholesterol is first converted to a series of progestogens with 21 carbons (following the action of cholesterol side-chain cleavage enzyme). Progestogens can be converted by hydroxylation (at carbon 21) to mineralocorticoids or glucocorticoids (both with 21 carbons) or by an elimination reaction to androgens (with 19 carbons). Androgens can in turn be converted to estrogens (with 18 carbons) by the action of an aromatase enzyme that is located in estrogen-producing cells in the adrenal glands, ovaries, placenta, testicles, adipose (fat) tissue, and brain. The aromatase enzyme converts ring A to a monocyclic aromatic six-carbon ring.
Progestogen. “Progestogen” (also known as progestagen or gestagen) is a generic term for a class of steroid hormones that bind to and activate the progesterone receptor. Progestogens are named for their function in maintaining pregnancy (ie, progestational agents). All endogenous progestogens share a basic 21-carbon skeleton called a pregnane skeleton (C21) with ketone or hydroxyl groups at the C3 and C20 positions. Progesterone is the primary progestogen in the body, and it is produced primarily by the corpus luteum of the ovary and by the placenta. Progesterone levels in the blood vary significantly during the menstrual cycle.
“Progestins” are synthetic progestogens that are structural analogues of progesterone (253); examples include the 17α-hydroxyprogesterone derivative medroxyprogesterone acetate and the 19-nortestosterone derivative norethisterone. A progestogen is specifically added to estrogen regimens of postmenopausal hormone therapy when the uterus is still present because unopposed estrogen therapy promotes endometrial thickening and can increase the risk of uterine cancer whereas progestogen administration reduces this risk.
In women, progesterone helps regulate the menstrual cycle, maintain pregnancies, and prepare the mammary glands for lactation and breastfeeding following parturition.
The corpus luteum--a temporary endocrine gland that forms from the empty ovarian follicle after ovulation—becomes the main source of progesterone immediately after fertilization and implantation. After conception, the placenta forms and begins to secrete progesterone to supplement, and ultimately surpass, the progesterone already secreted by the corpus luteum. The high level of progesterone during pregnancy prevents other eggs from maturing and it also promotes changes in breast tissue to prepare for lactation. If fertilization does not occur, the corpus luteum breaks down, causing less progesterone to be produced; with progesterone levels dropping below those needed to maintain the uterine lining, it breaks away, resulting in menstrual bleeding.
Men also need progesterone to produce testosterone (progesterone is a metabolic intermediate in the biosynthesis of testosterone). In men progesterone also is necessary for spermiogenesis and sperm capacitation (ie, the physiological changes spermatozoa must undergo in order to have the ability to penetrate and fertilize an egg). In men, progesterone is produced by the adrenals and the testes.
Androgen. “Androgen” is a generic term for a class of natural or synthetic steroid hormones that regulate the development and maintenance of the male sexual phenotype by binding to androgen receptors. The androgen receptor (also known as NR3C4 or nuclear receptor subfamily 3, group C, member 4) binds to androgenic hormones in the cytoplasm and then translocates into the nucleus. The androgen receptor serves mainly as a DNA-binding transcription factor that regulates gene expression.
Androgens are present in both males and females, and they increase in boys and girls during puberty. The principal androgens are testosterone, dihydrotestosterone (DHT), and androstenedione.
Testosterone is the primary male sex hormone. Testosterone plays a key role in the development of male reproductive tissues (ie, testes and prostate) and secondary sexual characteristics (eg, increased muscle and bone mass and growth of body hair). Insufficient levels of testosterone in men may lead to frailty and bone loss.
Testosterone is an anabolic steroid, containing keto and hydroxyl groups at the 3 and 17 positions, respectively. In men the vast majority of testosterone (greater than 95%) is produced by the Leydig cells in the testes, with adrenal gland production accounting for most of the remainder; in women, testosterone is synthesized in far smaller total quantities by the adrenal glands, thecal cells of the ovaries, and, during pregnancy, by the placenta. Men have testosterone levels about seven to eight times greater than those in women. Testosterone is supplied to target tissues via the blood, where much of it is transported bound to a specific plasma protein, sex hormone-binding globulin. In target tissues, testosterone binds to and activates the androgen receptor. Testosterone is converted in the liver to inactive metabolites.
In males, androgens regulate the embryological development of the primary male sex organs and the pubertal development of male secondary sex characteristics. In particular, dihydrotestosterone causes differentiation of the penis, scrotum, and prostate in utero whereas in adulthood dihydrotestosterone contributes to balding, prostate growth, and sebaceous gland activity. In females, androgens are responsible for pubic and body hair growth and contribute to libido and sexual arousal.
Androgens are also used as medications, for example, in androgen replacement therapy (also known as testosterone replacement therapy) in cisgender men to counteract the effects of male hypogonadism, in hormone therapy in transgender men (female-to-male), and in anabolic-androgenic steroids (a category that includes both natural androgens as well as synthetic androgens) to stimulate muscle growth and appetite, induce male puberty, and treat chronic wasting conditions such as cancer and AIDS. Anabolic-androgenic steroids are also frequently used as performance-enhancing drugs in sports; such ergogenic use of anabolic-androgenic steroids (“doping”) is controversial because of the associated adverse health effects and the unfair advantage this provides in physical competitions. Consequently, use of anabolic-androgenic steroids is banned by most major sporting bodies.
Estrogen. “Estrogen” is a generic term for a class of steroid hormones that are important for sexual and reproductive development in women. The word “estrogen” (or “oestrogen”) was derived in the 1920s from the words "estros" (or "oestros," a periodic state of sexual activity in female mammals) and “genos” (ie, generating).
There are three primary estrogens in the human body, varying by the number of hydroxyl groups, from 1 to 4: estrone (E1), estradiol (E2), estriol (E3), and estetrol (E4).
Estradiol is the most potent of these and is also the most prevalent in non-pregnant females during their reproductive years.
In contrast, levels of estriol in nonpregnant women are almost undetectable, but during pregnancy estriol is synthesized in very high quantities by the placenta and is then the most produced estrogen in the body.
Estetrol is produced only during pregnancy by the human fetal liver; estetrol has important antioxidative activity and in animal models of neonatal hypoxic-ischemic encephalopathy was shown to enhance cell proliferation in primary hippocampal neuronal cell cultures in vitro and to decrease early gray matter loss and promote neuro- and angiogenesis in vivo (269).
In postmenopausal women estrone becomes the primary form of estrogen in the body.
Estradiol levels in the blood vary significantly during the menstrual cycle.
Circulating estrogens are bound to albumin or sex hormone-binding globulin. Like all steroid hormones, estrogens readily diffuse across the cell membrane; once inside the cell, they bind to and activate estrogen receptors in the cell nucleus of target tissues. The estrogen receptor is a dimeric nuclear protein. Like the androgen receptor, the estrogen receptor serves mainly as a DNA-binding transcription factor that regulates gene expression. The estrogen-receptor complex binds to specific DNA sequences called a “hormone response element” to activate the transcription of target genes. The estrogen receptor is expressed in specific tissues, including the ovary, uterus, and breast. Estrogens also bind to and activate rapid-signaling membrane estrogen receptors.
Estrogens are metabolized primarily in the liver via hydroxylation by cytochrome P450 enzymes and via conjugation by estrogen sulfotransferases (sulfation) and UDP-glucuronyltransferases (glucuronidation). In addition, estradiol (E2) is dehydrogenated by 17β-hydroxysteroid dehydrogenase into the much less potent estrogen estrone (E1). Estrogens are excreted primarily by the kidneys as conjugates via the urine.
Estrogens are frequently used as medications, for instance in postmenopausal hormone therapy and hormonal birth control.
In women, estrogens are responsible for the pubertal development of female secondary sexual characteristics including breast development, widening of the hips, and female fat distribution. In addition, estrogens are responsible for maturation and maintenance of the vagina and uterus and for maturation of ovarian follicles. In men, estrogens help regulate the maturation of sperm and may be necessary for a healthy libido.
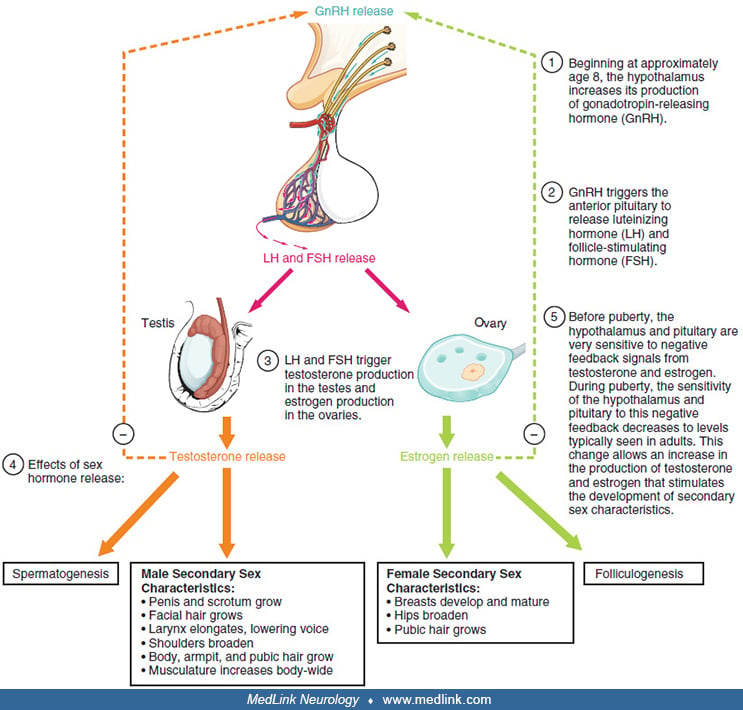
The hypothalamic-pituitary-gonadal axis. The hypothalamic-pituitary-gonadal axis refers to the hypothalamus, pituitary gland, and gonadal glands as if these individual endocrine glands were a single entity. This is a hierarchical system with multilevel negative feedback. Communication within the axis is accomplished by an array of hormones.
Gonadotropin-releasing hormone. Gonadotropin-releasing hormone (GnRH), as the name suggests, is a releasing hormone responsible for the release of gonadotropins (ie, glycoprotein polypeptide hormones). Gonadotropin-releasing hormone initiates activation of the reproductive axis by causing the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) from the anterior pituitary. In women, luteinizing hormone and follicle-stimulating hormone act on the ovaries to release estrogen and progesterone, whereas in men luteinizing hormone and follicle-stimulating hormone act on the testes to release testosterone.
The testosterone produced by the testes actually provides negative feedback to both the hypothalamus and pituitary gland, although some of the direct effect of testosterone at the pituitary level in men is mediated by estradiol (E2), presumably from conversion of testosterone (23).
Kisspeptin is a ligand for G protein-coupled receptor 54 (GPR54; aka Kiss1R) (186). Binding of kisspeptin to its cognate in gonadotropin-releasing hormone neurons within the arcuate nucleus of the hypothalamus stimulates release of the peptide hormone gonadotropin-releasing hormone (220). Kisspeptin-GPR54 signaling has an important role in initiating secretion of gonadotropin-releasing hormone at puberty (247). The activity of kisspeptin neurons is modulated by sex steroids and other regulatory factors (12).
Luteinizing hormone. Luteinizing hormone is a heterodimeric glycoprotein that is synthesized and secreted by gonadotropic cells in the anterior pituitary gland. In females, an acute rise of luteinizing hormone ("LH surge") triggers ovulation and development of the corpus luteum. In males, where luteinizing hormone had also been called interstitial cell-stimulating hormone, it stimulates Leydig cell production of testosterone. Luteinizing hormone levels in the blood vary significantly during the menstrual cycle.
Follicle-stimulating hormone. Like luteinizing hormone, follicle-stimulating hormone is a heterodimeric glycoprotein that is synthesized and secreted by the gonadotropic cells of the anterior pituitary gland. Follicle-stimulating hormone regulates pubertal maturation and the reproductive processes of the body. Follicle-stimulating hormone levels in the blood vary significantly during the menstrual cycle.
In both females and males, follicle-stimulating hormone stimulates the maturation of primordial germ cells.
In females, follicle-stimulating hormone initiates follicular growth, specifically affecting granulosa cells (or follicular cell), somatic cells that are closely associated with the developing oocyte in the ovary. With the concomitant rise in inhibin B, follicle-stimulating hormone levels then decline in the late follicular phase, allowing only the most advanced follicle to proceed to ovulation. At the end of the luteal phase, there is a slight rise in follicle-stimulating hormone that helps initiate the next ovulatory cycle. In contrast, in males, follicle-stimulating hormone activation of Sertoli cells sustains spermatogenesis and stimulates inhibin B secretion. Follicle-stimulating hormone induces Sertoli cells to secrete androgen-binding proteins, regulated by inhibin's negative feedback mechanism on the anterior pituitary.
The menstrual cycle. The menstrual cycle is a cyclic series of anatomical and physiological changes a woman's body goes through in preparation for a possible pregnancy. The first day of menstruation is considered day 1 and the preceding day is considered day −1; note that by convention there is no day 0. Cycle length varies from 24 to 38 days. Cycle length also changes between menarche (ie, when periods first start during puberty) and menopause (ie, when periods stop permanently).
The menstrual cycle can be considered as comprised of two linked cycles in different organs: one happening in the ovaries and the other in the uterus. Each cycle has several phases.
|
Cycle |
Preovulation |
Ovulation |
Postovulation | |
|
Ovarian |
Follicular phase |
Luteal phase | ||
|
Uterine |
Menstruation (a “period”) |
Proliferative phase |
Secretory phase |
The ovarian cycle begins with the development of a dominant follicle (under the influence of follicle-stimulating hormone), which produces estrogen as it grows. This follicular phase generally lasts from 10 to 22 days. Estrogen peaks just before ovulation, precipitating a spike in luteinizing hormone, which in turn triggers ovulation. At ovulation, the dominant follicle releases an oocyte from the ovary into the fallopian tube; this generally occurs about midway through the cycle, or about 13 to 15 days before the next period. In the ensuing luteal phase, the dominant follicle (now sans oocyte) transforms into a corpus luteum, a transitory endocrine organ that begins to produce progesterone and estrogen. If fertilization does not occur, the corpus luteum starts to degenerate between 9 and 11 days after ovulation, causing progesterone and estrogen levels to fall. Consequently, in the absence of fertilization, progesterone levels peak about halfway through this phase. The luteal phase typically lasts about 14 days but can range from 9 and 16 days.
The simultaneously occurring uterine cycle begins with menstruation with shedding of endometrium and blood through the cervix and vagina (typically 5 or 6 days but can be up to 8 days). Menstruation is triggered by the dropping progesterone and estrogen levels in the final phase of the ovarian cycle. Menstruation is followed by estrogen-induced proliferative phase with reproliferation of the uterine lining in preparation for possible pregnancy. After ovulation the uterus enters a secretory phase, when the endometrium begins secreting prostaglandins. Levels of prostaglandins F2α (PGF2α) and E2 (PGE2) rise during this phase. If pregnancy does not occur, progesterone and estrogen levels fall causing the endometrium to break down, while the prostaglandins cause uterine muscle to contract and uterine blood vessels to constrict, helping to induce menstruation. If pregnancy does occur, prostaglandin production is inhibited to allow fetal development to proceed, and the placenta begins producing hormones.
Pregnancy and puerperium. During the first stage of pregnancy, the trophoblast releases human chorionic gonadotropin, which enables the corpus luteum to continue producing estrogen and progesterone until the placenta develops. The placenta subsequently produces most of estrogen and progesterone necessary to sustain the pregnancy. Maternal serum levels of estradiol and progesterone begin to rise during the 6th to 8th week of pregnancy and gradually increase to their highest levels during the third trimester. By the third trimester, serum estradiol levels are 30 to 40 times higher and progesterone levels are 20 times higher than their peak levels during the menstrual cycle. Hormone levels drop sharply to the pre-pregnancy state during the puerperium (ie, from delivery to 6 weeks postpartum).
Menopause. Menopause marks the end of a woman’s reproductive years, when menstrual periods have stopped and when the ovaries no longer produce high levels of sex hormones. A corollary is that during menopause sex hormone levels no longer oscillate.
Estrogen-binding neurons are located in the preoptic area, medial basal hypothalamus, medial amygdala, and circumventricular organs. In addition, estrogen-binding neurons also reside, to a minimal extent, in the basal forebrain, the hippocampus, in several thalamic nuclei, sensory regions of the brainstem and spinal cord, and the neonatal neocortex (73; 65). The presence of estradiol receptors in hippocampus and hypothalamus suggests the possibility of direct effects of estradiol on brain cells. Successful neuroprotection produced by estradiol in hypertensive rats encourages treatment with non-feminizing estrogens and estrogen receptor modulators for age-associated diseases (68). Increase in sympathetic nerve activity is one of the crucial components involved in the development of hypertension in both men and women. Brain regions important for the regulation of sympathetic nerve activity have also been implicated in mechanisms underlying risk factors for hypertension such as obesity, stress, and inflammation. Further understandings of the mechanisms by which estrogen acts at these sites will be important areas to focus on for newer medications treating hypertension (111).
Sex hormones have both organizational and activational effects. Organizational effects refer to differentiation of neural circuitry from exposure to sex steroids during brain development in an irreversible fashion. Activational effects refer to reversible neurophysiological change by gonadal hormones on the mature nervous system.
During the neonatal and peripubertal periods, estrogens and aromatizable androgens induce trophic changes in the rodent hypothalamus, whereas in later life, estrogens accelerate aging-related changes in the endocrine hypothalamus that may contribute to the onset of reproductive senescence. These interactions are essential for regulation of the brain-pituitary-gonadal axis and for the establishment of normal patterns of sexual, cognitive, and autonomic behaviors at various phases (menstrual cycle, pregnancy, and menopause) (262; 94).
The neuroprotective and therapeutic effects of estetrol have been reviewed before and after hypoxic-ischemic encephalopathy (269). Estetrol has been shown to enhance cell proliferation in primary hippocampal neuronal cell cultures in vitro and promotes neuro- and angiogenesis in vivo.
|
• There is a well-established relationship between migraine and hormonal fluctuations in women. | |
|
• The peak prevalence of migraine occurs in women of reproductive age. | |
|
• Hormonal replacement with estrogen can exacerbate migraine and so can oral contraceptives. | |
|
• The frequency or severity of migraine attacks often diminishes with gestation, particularly in patients whose headaches are linked to the menstrual cycle. | |
|
• Migraine generally improves during pregnancy, particularly for women with migraine without aura. | |
|
• After childbirth, the recurrence rate of migraine attacks increases, especially during the first month, and some women may have a particularly intense migraine shortly after delivery because of the precipitous decrease in estradiol levels. | |
|
• Premenstrual migraines regularly occur during or after the time when the female hormones estrogen and progesterone drop to their lowest levels. | |
|
• Menstrual-related migraine should be suspected in females whose migraine occurs predominantly between 2 days before and 3 days after the start of menstruation in at least two of three consecutive menstrual cycles. | |
|
• Epilepsy may worsen around the time of ovulation or premenstrually (catamenial epilepsy) and during pregnancy. | |
|
• Catamenial epilepsy is the subset of epilepsy that includes women whose seizures are exacerbated by their menstrual cycle. In such women, seizures correlate positively with mean estrogen/progesterone ratios and negatively with plasma progesterone levels. | |
|
• The use of hormone replacement therapy after menopause produces an increase in seizure frequency and severity in women with a history of catamenial epilepsy. |
Sex hormones play an important role in a number of various neurologic disorders and diseases including headaches, cerebrovascular disease, seizures, movement disorders, brain malignancies, multiple sclerosis and other neuroimmunologic disorders, dementia, neuropsychiatric disorders, sleep disorders, catamenial sciatica, myotonic dystrophy, growth-hormone insufficiency, acromegaly, and porphyria.
Migraine. There is a well-established relationship between migraine and hormonal fluctuations in women.
The peak prevalence of migraine occurs in women of reproductive age (41). Not only are women much more likely to have migraine than men, but women have a higher burden of migraine-related symptoms and disability than men (41; 02) and the frequency and character of the headaches often change at periods of altered sex hormone levels, including menarche, menses, pregnancy, and menopause.
Hormonal replacement with estrogen can exacerbate migraine and so can oral contraceptives. Women often can precipitate new-onset migraine, exacerbate existing migraine, or exacerbation of, or change the character of migraine when taking oral contraceptives (241).
The frequency or severity of migraine attacks often diminishes with gestation, particularly in patients whose headaches are linked to the menstrual cycle (55). Migraine generally improves during pregnancy, particularly for women with migraine without aura (289; 180; 229; 183; 99; 120; 87; 09). The relative hormonal stability in pregnancy has been assumed to be the basis for the improvement in headache. Migraine may also first occur during pregnancy (211); migraine developing during pregnancy may indicate an underlying structural or functional disorder (289). After childbirth, the recurrence rate of migraine attacks increases, especially during the first month (230; 140; 120; 09), and some women may have a particularly intense migraine shortly after delivery because of the precipitous decrease in estradiol levels (227; 87). Compared to pregnancy, there is a postpartum increase in the mean intensity and duration of headaches, as well as in the mean number of analgesics used (229; 140). Some (229; 120; 09), but not all (140) studies report that breastfeeding exerts a protective effect against the reappearance of migraine.
Menstrual migraine (menstrually associated migraine, menstrually related migraine, menstruation-related migraine, catamenial migraine). Migraine often has a temporal relationship with menstruation. Premenstrual migraines regularly occur during or after the time when the female hormones estrogen and progesterone drop to their lowest levels.
In The International Classification of Headache Disorders 3rd edition (ICHD-3) of the International Headache Society includes criteria for “A1.1.1 Pure menstrual migraine,” “A1.1.2 Menstruation-related migraine,” “A1.2.0.1 Pure menstrual migraine with aura,” and “A1.2.0.2 Menstruation-related migraine with aura,” but in an appendix because of uncertainty over whether they should be regarded as separate entities (112). Note that for the purposes of ICHD-3, menstruation is endometrial bleeding resulting either from the normal menstrual cycle or from the withdrawal of exogenous progestogens, as in the use of combined oral contraceptives or cyclical hormone replacement therapy. Menstruation-related migraine without aura (A1.1.2) is characterized by attacks, in a menstruating woman, fulfilling criteria for migraine without aura and occurring on days −2 to +3 of menstruation in at least two of three menstrual cycles, and additionally at other times of the cycle. Pure menstrual migraine without aura (A1.1.1) is similar to menstruation-related migraine without aura (A1.1.2), but headaches occur only perimenstrually and at no other times of the cycle. A parallel arrangement applies for pure menstrual migraine with aura (A1.2.0.1) and menstruation-related migraine with aura (A1.2.0.2). There is no consensus on whether menstrual migraine attacks should be defined as starting instead of occurring on day 1 ± 2 of menstruation (277; 52).
Modifications of the ICHD-3 criteria have been proposed (52). For pure menstrual migraine, (1) attacks in menstruating women fulfil the ICHD-3 diagnostic criteria for 1.1 migraine without aura and/or 1.2 migraine with aura; (2) attacks occur exclusively during menstruation (during at least three menstruations) beginning on day 1 ± 2 (ie, days −1 to +3) of menstruation and at no other times of the cycle. If after a menstrual migraine attack, the patient is headache free for at least 24 hours, either spontaneously or as a result of treatment, and migraine reoccurs within the −1- to +3-day menstrual interval, the attacks are regarded as separate menstrual migraine attacks. For menstrually related migraine, (1) attacks in menstruating women fulfil the ICHD-3 diagnostic criteria for 1.1 migraine without aura and/or 1.2 migraine with aura; (2) at least half of all migraine attacks (during at least three menstruations) begin on day 1 ± 2 (ie, days −1 to +3) of menstruation. If after a menstrual migraine attack, the patient is headache free for at least 24 hours, either spontaneously or as a result of treatment, and migraine reoccurs within the −1- to +3-day menstrual interval, the attacks are regarded as separate menstrual attacks.
Self-reported menstrual migraine diagnosis has poor accuracy (277). Two thirds of female migraineurs suffer from menstrual migraine (independent of self-reports), but pure menstrual migraine is rare (277). Prospective headache diaries are required for the diagnosis of menstrual migraine (277).
Menstrual-related migraine should be suspected in females whose migraine occurs predominantly between 2 days before and 3 days after the start of menstruation in at least two of three consecutive menstrual cycles. In women with both menstrual and nonmenstrual migraines, menstrual migraines are generally not associated with aura, are of longer duration, are more likely to be severe, are more likely to have nausea and vomiting, are associated with more functional disability, and are usually more resistant to treatment compared with attacks at other times of the month (244; 159; 39; 152; 87; 52). Compared to non-menstrual migraine, menstrual migraine is associated with a higher frequency of migraine-accompanying symptoms, more frequent and more severe migraine attacks, lower frequency of nonmigraine headache, an overall greater response to treatment with triptans, better improvement of migraine attacks during late pregnancy, and faster reappearance of migraine attacks postpartum (52).
Menstrually related migraine before pregnancy is associated with lack of headache improvement in the first and third trimesters of pregnancy whereas second-trimester hyperemesis and a pathological pregnancy course are associated with lack of headache improvement in the second trimester (229).
Headaches from pseudotumor cerebri can be secondary to estrogenic attenuation of the blood-brain barrier, and this might explain the female predilection for this disorder (303).
Cluster headache. In contrast to migraine, cluster headache mostly affects men (although a progressive decrease in the male-to-female ratio has occurred over time) (10). When considering the gender-specific features of cluster headache, women with cluster headache more often have clinical features (eg, nausea and osmophobia) that overlap with those of migraine (10). In addition, among women with cluster headache, the onset of disease often corresponded with changes in the levels of sexual hormones (menarche, postpartum, menopause) (10).
Cerebrovascular disease. Altered levels of sex hormones are associated with cerebral venous thrombosis, ischemic stroke, and subarachnoid hemorrhage (49; 42; 76; 239). Sex hormones can induce a hypercoagulable state, which may contribute to the development of cerebral venous thrombosis complicating pregnancy and the puerperium (85). Estrogen increases plasma levels of fibrinogen and clotting factors VII, VIII, IX, X, and XII. Ischemic stroke in users of oral contraceptives may occur in the carotid and vertebrobasilar distributions. Increased prevalence of mitral valve prolapse among users of oral contraceptives with ischemic stroke has been reported (81; 223).
Sex hormones have not been proven to play a role in mediating ischemic stroke among elderly men or women, though some of the data are conflicting. In a prospective study of incident cardiovascular disease among 552 community-dwelling elderly men (65 years and older), endogenous levels of testosterone, estradiol, and sex hormone-binding globulin were not associated with increased risk of coronary, cerebrovascular, or peripheral arterial events (59). In a nested case-control study of postmenopausal women from the Nurses' Health Study, among 419 postmenopausal women with confirmed incident ischemic stroke and 419 matched controls, testosterone and sex hormone-binding globulin levels were not associated with ischemic stroke among either current or never/past users of exogenous hormone therapy (121). In contrast, in a subset of 13,192 postmenopausal women free of prevalent stroke, as part of the Women's Health Initiative prospective cohort study conducted at 40 sites across the United States from 1993 to 1998, there was a statistically significant inverse association between serum sex hormone-binding globulin levels and ischemic stroke risk, with hazard ratios of 1.6 to 1.9 in different multivariate models (153); including potential mediators attenuated but did not eliminate these associations.
Several large randomized controlled studies indicate that hormone replacement therapy does not protect against stroke or coronary artery disease in women with established vascular disease and may actually worsen outcomes in this high-risk population (245; 33; 268).
Sex hormones alter the function and morphology of platelets and fibrin networks, and changes in platelet and fibrin network morphology offer one of the earliest confirmations of inflammation. Sex hormone levels, inflammatory processes, and thrombotic mechanisms are profoundly interconnected in predicting the outcome of cerebral ischemia (272).
Cigarette smoking and age greater than 35 years old significantly increase the risk of subarachnoid hemorrhage in users of oral contraceptives (198; 254). Female sex hormones may predispose to bleeding from both aneurysms and arteriovenous malformations, although the pathophysiological mechanisms underlying these phenomena remain controversial (74).
Epilepsy. Seizure disorders and antiepileptic therapy can significantly interfere with normal reproductive processes in women, and conversely changes in hormone levels associated with pregnancy can alter anticonvulsant levels and seizure control (209; 118; 280; 13).
Epilepsy may worsen around the time of ovulation or premenstrually (catamenial epilepsy) and during pregnancy (179; 108; 14; 13). The course of epilepsy and its management, therefore, is greatly influenced by specific phases of the reproductive cycle.
Pregnant epileptic women experience higher rates of maternal and fetal complications, including vaginal hemorrhage, prematurity, low birth weight, and perinatal mortality (274). Oral contraceptive failure and teratogenicity has been associated with the use of older enzyme-inducing anticonvulsants like phenytoin, phenobarbital, primidone, ethosuximide, and carbamazepine (304; 133; 279), but not with valproate or with newer antiepileptic medications such as lamotrigine, gabapentin, and vigabatrin (304; 40). Topiramate and felbamate may also affect contraceptive efficacy (225).
Catamenial epilepsy. Catamenial epilepsy is epilepsy with perimenstrual exacerbation, a phenomenon that occurs in about 40% of women with epilepsy. In such women, seizures correlate positively with mean estrogen/progesterone ratios and negatively with plasma progesterone levels (21).
Catamenial epilepsy is an epileptic condition in which there is clustering of seizures in relation to the menstrual cycle. Catamenial epilepsy is attributable to the neuroactive properties of steroid sex hormones combined with the cyclic variation in serum levels of these hormones (116). The frequency of catamenial epilepsy depends heavily on how the condition is defined (77; 116). In any case, patient claims about frequency of seizures in relation to menstruation are not always accurate (77).
Various classifications of catamenial epilepsy have been proposed (77), but the most widely used classification categorizes catamenial epilepsy into three patterns as either perimenstrual (C1), periovulatory (C2), or luteal (C3), based on the serum estradiol to progesterone ratio, and a 24- to 34-day menstrual cycle in which menses begins on day 1 and ovulation occurs 14 days prior to menstruation (116). For this classification, the menstrual cycle was divided into four phases with an adjustment for variable cycle length: menstrual phase (M) = -3 to +3, follicular phase (F) = 4 to 9, ovulatory phase (O) = 10 to -13, and luteal phase (L) = -12 to -4. Onset of menstruation was considered as day 1 and ovulation was considered to occur on day -14, with the negative number indicating 14 days before the onset of menstruation. The latter designation was used because ovulation generally occurs 14 days before onset of menstruation regardless of cycle interval. Using the system of Herzog and colleagues about one third of women with intractable partial epilepsy in their childbearing years have catamenial epilepsy (116).
The perimenstrual (catamenial pattern 1, C1) category of catamenial epilepsy is defined as a 2-fold or greater increase in average daily seizure occurrence during the menstrual (M) phase of the menstrual cycle (ie, occurring in normal cycles from 3 days before to 3 days after the onset of menstruation) compared with the follicular (F) and luteal (L) phases during normal ovulatory cycles (116). The designation of C1 as day -3 to 3 includes at least 3 days beyond the duration of progesterone withdrawal. Perimenstrual exacerbation of seizures has been attributed to withdrawal of the protective effects of progesterone (21) and more specifically to withdrawal of the progesterone-derived GABAergic neurosteroids due to the decline in progesterone level at the time of menstruation (213). Although the menstrual phase is characterized by marked decreases in both progesterone and estrogen levels, the estradiol to progesterone ratio is highest during the days before menstruation (C1) and ovulation (C2). Moreover, patients with the C1 pattern of catamenial epilepsy have lower progesterone levels than healthy controls during the menstruation phase of the menstrual cycle (82). Extrasynaptic δGABAA receptors, which are sensitive to neurosteroids and provide increased seizure protection, are upregulated during the perimenstrual period (213).
The periovulatory (catamenial pattern 2, C2) category of catamenial epilepsy is associated with a 2-fold or greater increase in average daily seizure occurrence during the ovulatory (O) phase (ie, occurring from days 10 to -13) compared with the follicular (F) and luteal (L) phases during normal ovulatory cycles (116). C2 extends beyond the preovulatory surge of estradiol and ovulatory onset of greater progesterone secretion. Periovulatory exacerbation of seizures has been attributed to the excitatory effects of estrogens. The ovulatory phase of the menstrual cycle is characterized by a surge of estrogen before ovulation, whereas an associated progesterone surge does not occur until ovulation actually occurs. This “estrogen effect,” without a corresponding progesterone surge of protection, intensifies seizure events.
The luteal (catamenial pattern 3, C3) category of catamenial epilepsy is associated with a 2-fold or greater increase in average daily seizure occurrence during the ovulatory (O), luteal (L), and menstrual (M) phases (ie, the entire second half of the cycle) than during the follicular (F) phase in inadequate luteal phase cycles (ie, abnormal or inadequate luteal phase cycles, days 10 to 3) (116). C3, like C1, involves the early days of menstruation, a period that extends beyond the withdrawal of progesterone premenstrually. Anovulatory females do not typically have a midcycle surge of progesterone, but still experience a surge in estrogen; these women have abnormally low progesterone levels during the ovulatory, luteal, and menstruation phases, regardless of whether ovulation occurs. Patients with C3 pattern of catamenial epilepsy have overall lower progesterone levels than healthy controls during the luteal phase of the menstrual cycle (82).
One caveat of this scheme is that neuroactive sex hormones may produce changes in the structure and biological activity of neuronal excitatory and inhibitory receptors that outlast the brief duration of the hormone-receptor interaction (116).
During menopause, there are marked changes in the production of gonadal hormones. Most of the sex hormones diminish initially around menopause, becoming irregular, and often showing wide and unpredictable fluctuations, and consequently variable effects on the frequency of seizures in those with a history of catamenial epilepsy (222). As menopause progresses, there is cessation of estrogen (estradiol) production by the ovaries and a marked decrease in risk of seizures during menopause if there was a catamenial relationship (222).
The use of hormone replacement therapy after menopause produces an increase in seizure frequency and severity in women with a history of catamenial epilepsy (109). Such women need closer anticonvulsant medication monitoring to maintain or reduce seizure occurrence (109). For menopausal women with a history of catamenial epilepsy and needing symptomatic relief (eg, when “hot flushes” are disruptive), estrogen-only preparations are relatively contraindicated but the combination of a single estrogenic compound (eg, 17-β-estradiol) and natural progesterone can be considered (109).
These anticonvulsants induce the hepatic cytochrome P450 microsomal enzyme system, which, in turn, accelerates catabolism of endogenous and exogenous sex hormones. Oral contraceptive failure does not occur with valproic acid, which may actually inhibit cytochrome P450 enzymes, causing elevations in plasma steroid concentrations. Valproic acid, however, may cause hyperandrogenism and polycystic ovaries (118; 204).
Of the newer antiepileptic medications, lamotrigine, gabapentin, and vigabatrin do not induce the hepatic P450 microsomal enzyme system, and oral contraceptive failure has not been reported with concomitant use of these drugs (304; 40). Topiramate and felbamate may affect contraceptive efficacy by affecting sex hormone pharmacokinetics (225). During pregnancy, serum levels of phenytoin, phenobarbital, and valproic acid may decrease by 30% to 40% of pregestational levels, with a lesser decline in carbamazepine. Primidone levels are reportedly stable during pregnancy, but the concentration of primidone-derived phenobarbital is reduced (146; 110).
Movement disorders. Both gestational chorea (chorea gravidarum) and oral contraceptive-related chorea are closely associated with prior rheumatic fever (74). Contraceptive-related chorea has also been reported in patients with a history of congenital cyanotic heart disease and Henoch-Schonlein purpura (218). In most cases, dyskinesias resolve completely by the end of pregnancy or after discontinuation of the contraceptive medication.
There are anecdotal reports in the early clinical literature of motor deterioration in idiopathic and neuroleptic-induced parkinsonism after exposure to exogenous estrogens. Although premenopausal women are reportedly more susceptible to drug-induced parkinsonism than men of similar age (31), postmenopausal estrogen therapy had no significant dopaminergic effect (259; 144).
Gonadal dysfunction, reduced androgen levels, and an abnormal hypothalamic-pituitary-gonadal axis have been reported in Huntington disease (237). In addition, a potential relationship between the gonadal dysfunction and abnormal hippocampal plasticity in Huntington disease may help explain the putative role of the HTT gene in the regulation of steroidogenesis in both the gonads and the brain (237).
Kisspeptin is an important regulator of reproduction, and the neurons are localized in the arcuate nucleus. The activity of kisspeptin neurons is modulated by sex steroids and other regulatory factors (12).
Wilson disease can produce chorea, seizures, and psychosis from the toxic effects of excessive copper deposition in neural tissues (184). An increase in serum ceruloplasmin levels can occur during pregnancy and after treatment with exogenous estrogens. In normal individuals, serum ceruloplasmin and copper levels increase during pregnancy and after administration of estrogen or estrogen-progestogen contraceptives (300). Although ceruloplasmin levels are characteristically low in Wilson disease, exposure to hormonal contraceptives may elevate falsely normal ceruloplasmin levels into the normal range, leading to a delay in diagnosing Wilson disease (234).
Intracranial malignancies. Meningiomas are more common in obese women and in patients with hormone-dependent breast carcinoma (236; 126). They occur more frequently in women than in men and rarely prior to pubertal period (235; 200; 126). Meningiomas undergo a relatively rapid expansion during pregnancy, followed by spontaneous regression during the postpartum period (234; 107). Similarly, there are anecdotal reports of the enlargement of astrocytomas during pregnancy, followed by spontaneous regression in the puerperium (187). In addition, acoustic neuromas (20) and pituitary adenomas (80) may show responsiveness to sex hormones.
Neuroimmunologic disorders. Multiple sclerosis is more prevalent among women than men. Among women with multiple sclerosis, cognitive functions and physical performance deteriorate during the premenstrual period (105). In addition, the relapse rate of multiple sclerosis declines by almost 70% in the third trimester of pregnancy, an effect more robust than that from treatment with interferon-beta, glatiramer acetate, or intravenous immunoglobulin (122; 56). In contrast, multiple sclerosis exacerbations are more common during the first 3 postpartum months (286).
In a systematic review, there was no difference in the rates of relapse before and after menopause and evidence of a potential causal effect of estrogen depletion on disability was deemed inconclusive (131). The effect of hormone replacement therapy on the natural course of the disease remains to be defined.
Dementia. In a meta-analysis of 12 observational studies, Massoud and colleagues revealed that postmenopausal estrogen replacement therapy appears to be associated with a significantly decreased risk of developing Alzheimer disease (177). In addition, it has also been shown that postmenopausal estrogen replacement therapy protects against the development of dementia in women with Parkinson disease (219).
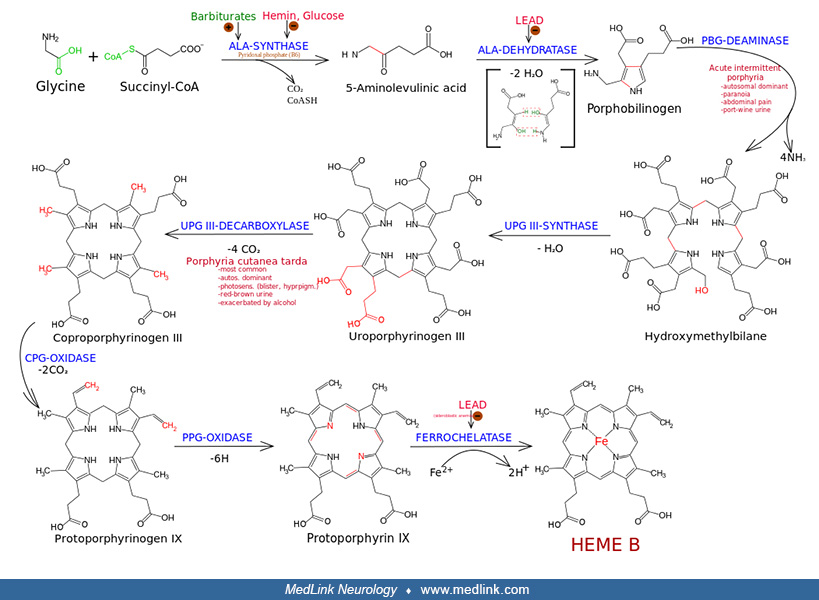
Neurologic manifestations in porphyria, when present, include seizures, behavioral symptoms, and sensorimotor and autonomic neuropathies. Estradiol and other steroids with a 5beta configuration induce the enzyme δ-aminolevulinic acid synthase and may precipitate porphyric crises. Oral contraceptives increase urinary excretion of this enzyme in normal individuals, and, therefore, asymptomatic relatives of patients with porphyria need to be made aware of the potential consequences (234).
Neuropsychiatric disorders. Neuropsychiatric symptoms of premenstrual syndrome include headache, fatigue, depression, irritability, or changes in dietary habits. Symptoms typically begin toward the end of the luteal phase of the menstrual cycle and usually, but not invariably, resolve with the onset of menses.
Depression and other major affective disorders may also develop in association with the menstrual cycle, the puerperium, and menopause (216). Sex hormones have been shown to produce stress effects, which ultimately impact emotional learning and memory (185).
Psychotic disorders characterized by extreme agitation, hallucinations, paranoid delusions, incoherent speech, and mood lability may arise during the postpartum period or may recur consistently during the late luteal phase of the menstrual cycle (284).
Sex hormones produce stress effects that ultimately impact emotional learning and memory (185).
Sleep disorders. Changes in the balance of estrogen and progestin may also impact sleep-related issues as evidenced by their replacement. For example, female sex hormones may help improve sleep in hypogonadal women by shortening mean sleep latencies, prolonging the duration of rapid eye movement sleep periods, and reducing nocturnal movement arousals (238; 201; 128).
Progestins have also been shown to improve hypoventilation in a patient with central sleep apnea (188). Removal of a benign testosterone-producing ovarian tumor resolved obstructive sleep apnea in one case (71) whereas progestin administration improved hypoventilation in a patient with central sleep apnea (188). In addition, testosterone administration has been shown to increase the hypocapnic apnea threshold in premenopausal women (299; 58).
Choi and colleagues demonstrated that testosterone can decrease and cortisol can increase pain induced by electrical stimulation, suggesting that acute clinical pain may be relieved by controlling stress and managing consequent stress-related testosterone and cortisol (57). In their review, Bale and Epperson discussed potential underlying mechanisms driving sex differences across the lifespan in stress responses and their relevance to disease (25).
Neuromuscular disorders. Catamenial sciatica, a radiculopathy related to endometriosis, causes pain in the nerve or nerve root distribution, which usually begins 2 to 3 days before the onset of menses (228). Pain may continue for a variable duration after cessation of flow. In addition to pain, patients may have numbness, weakness, and loss of ankle reflexes. Endometriotic sciatica is less likely to respond to bed rest, and the imaging findings are usually unimpressive (54).
Sex differences in pain sensitivity have been well recognized; however, pathophysiology is incompletely understood. A study by Veldhuijzen and colleagues evaluated how pain-related neural processing varies across the menstrual cycle with fluctuating sex hormone levels (275). It revealed no significant cycle phase differences for pain intensity stimuli applied during functional magnetic resonance imaging scans.
Estrogens may influence the natural history of Bell palsy, recurrent brachial plexopathy, and carpal tunnel syndrome (287). Myotonic dystrophy patients may have dysfunction of testicular peritubular myoid cells and corpus cavernosum smooth muscle, contributing to hypergonadotropic hypogonadism and impotence in men (178).
Kennedy disease, or spinal and bulbar muscular atrophy, is an X-linked neuromuscular disease caused by an abnormal CAG trinucleotide repeat expansion in the androgen receptor gene. Although cases continue to be misdiagnosed as amyotrophic lateral sclerosis, several features distinguished this disorder from other motor neuron disorders: (1) clinical onset in middle life; (2) X-linked recessive inheritance; (3) proximal spinal and bulbar muscular weakness and atrophy; (4) generalized fasciculations, especially prominent about the lips and chin; (5) absence of pyramidal tract (upper motor neuron), cerebellar, or sensory involvement; (6) a slowly progressive course with an apparently normal life span; and (7) gynecomastia.
Estrogens may also influence the natural history of Bell palsy, recurrent brachial plexopathy, and carpal tunnel syndrome (287).
Disorders of growth hormone. A reduction in desire and arousability, both in men and women, together with an impairment of erectile function in men, have been described both in patients with growth hormone deficiency and acromegaly. However, it remains unclear whether they are directly dependent on the hormone defect or excess, or whether they are consequence of the hypogonadism or any other clinical complications affecting sexual function (92).
Porphyria. Women with acute intermittent porphyria frequently have cyclic symptoms, particularly during the luteal phase of their menstrual cycles (01). Similarly, most females affected by catamenial attacks have premenstrual attacks (ie, in the luteal phase of the menstrual cycle) (16). Some patients experience disabling attacks with almost every menstrual cycle (16). Furthermore, estradiol, some other steroids, and controlled ovarian hyperstimulation for in vitro fertilization may precipitate porphyric crises (191).
A 24-year-old woman presented with a recurring history of left buttock pain with radiation to the posterior thigh, calf, and sole of the foot. Symptoms were present during her menstrual cycle and for at least 3 to 4 days afterwards. The patient had no symptoms during the rest of her cycle. Neurologic examination during the symptoms revealed no weakness; muscle stretch reflexes were reduced at the left ankle, and sensory examination was essentially unremarkable. Laboratory testing revealed EMG findings were consistent with an S1 radiculopathy, and MRI showed ectopic endometrium surrounding the S1 vertebral body encroaching on the S1 nerve root. Laparoscopic surgery removed the foci of endometriosis. The patient was symptom-free in the 3-month follow-up period after her surgery.
|
• During the neonatal and peripubertal periods, estrogens and aromatizable androgens induce trophic changes in the hypothalamus, whereas in later life, estrogens accelerate aging-related changes in the endocrine hypothalamus that may contribute to the onset of reproductive senescence; these interactions are essential for regulation of the brain-pituitary-gonadal axis and for the establishment of normal patterns of sexual, cognitive, and autonomic behaviors at various phases (eg, menstrual cycle, pregnancy, and menopause). | |
|
• The pathogenesis of menstrual migraine is not fully understood, but investigators have suspected that it may be related to estrogen or prostaglandin withdrawal. | |
|
• Estrogen priming lowers the seizure threshold in the hippocampus in animal models, and, similarly, it was recognized that administration of estrogen-based hormonal therapies can increase seizure frequency in some women with epilepsy. | |
|
• Progesterone has a neuroprotective effect on hippocampal neurons in seizure models induced by kainic acid; progesterone’s anticonvulsant and neuroprotective effects are apparently due to the steroid's actions on GABAA-benzodiazepine receptor complexes rather than intracellular progesterone receptors. |
Estrogen-binding neurons are located in the preoptic area, medial basal hypothalamus, medial amygdala, and circumventricular organs. Estrogen-binding neurons also reside, to a minimal extent, in the basal forebrain, the hippocampus, several thalamic nuclei, sensory regions of the brainstem and spinal cord, and the neonatal neocortex (73; 65). Estradiol receptors in hippocampus and hypothalamus imply that estradiol directly affects brain cells.
During the neonatal and peripubertal periods, estrogens and aromatizable androgens induce trophic changes in the hypothalamus, whereas in later life, estrogens accelerate aging-related changes in the endocrine hypothalamus that may contribute to the onset of reproductive senescence. These interactions are essential for regulation of the brain-pituitary-gonadal axis and for the establishment of normal patterns of sexual, cognitive, and autonomic behaviors at various phases (menstrual cycle, pregnancy, and menopause) (262; 94).
Sex hormones have both organizational and activational effects. Organizational effects refer to differentiation of neural circuitry from exposure to sex steroids during brain development in an irreversible fashion. Activational effects refer to reversible neurophysiological change by gonadal hormones on the mature nervous system.
Sex steroid regulation of the balance of neuroexcitatory and neuroinhibitory activities may have a role in modulating clinical susceptibility to different neurologic conditions such as migraine, catamenial epilepsy, premenstrual dysphoric disorder, and premenstrual syndrome (89).
Progesterone acts on neurons directly by activating progesterone receptors (through enhanced expression of alpha-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid receptors) and through metabolic conversion to neurosteroids (130).
Menstrual migraine. Associations have been reported between estrogen “withdrawal” in the late luteal/peri-menstrual period (ie, shortly before and during menses) and attacks of migraine without aura, and between high estrogen states and attacks of migraine with aura (172; 240; 159; 156; 155). Other potential contributing factors include: (1) release of prostaglandins (ie, from shedding endometrium) that sensitize peripheral nociceptors; (2) decline in serum magnesium levels; (3) decreases in inhibitory neurotransmitters (eg, serotonin, GABA) that modulate neuronal firing rates within second-order neurons of the trigeminal system (175); (4) modulation calcitonin gene-related peptide in the trigeminovascular system; and (5) modulation of cortical spreading depression susceptibility.
The pathogenesis of menstrual migraine is not fully understood, but investigators have suspected that it may be related to estrogen or prostaglandin withdrawal (174; 162; 205; 273). However, existing studies are limited by methodologic inconsistencies, small sample sizes, and variable case definitions (205).
Unfortunately, studies have identified no clear hormonal difference in reproductive-age women with menstrually related migraine versus those with nonmenstrually related migraine (84). Attempts at preventing menstrually related migraine with oral estrogen supplements or estradiol implants did not result in overall clinical improvement and in fact some women experienced more headaches than before the treatment (251; 252). Furthermore, administration of progesterone against a background of prolonged exposure to high estrogen levels did not provoke migraine, nor did its subsequent withdrawal result in migraine (252). More recently, investigators have concluded that “estrogen and progesterone can be preventative or provocative for migraine headache under different circumstances, depending on their absolute serum levels, constancy of exposure, and types of estrogen/progesterone derivatives” (175), but this vague statement seems to reflect continued uncertainty over the specific hormonal relationship that is producing the cyclic pattern of menstrually related migraine.
One study reported that women with menstrual and menstrually related migraine headaches have a significantly higher number of migraine attacks during the late luteal/early follicular phase of falling estrogen (ie, perimenstrually) and lower number of attacks during rising phases of estrogen (162). Although the authors concluded that the findings “confirm a relationship between migraine and changing levels of estrogen, supporting the hypothesis of perimenstrual but not postovulatory estrogen ‘withdrawal’ migraine,” the finding is suspect because the women were in fact selected for having the specific pattern of headaches that they were then found to have.
Improvement of migraine without aura after menopause is generally attributed to the absence of variations in sex hormone levels, not necessarily the lower levels of circulating sex hormones (157).
Cerebrovascular disease. Several different mechanisms may be involved in the interaction or association of sex hormones with cerebrovascular disease incidence. Sex hormone levels, inflammatory processes, and thrombotic mechanisms are profoundly interconnected in predicting the outcome of cerebral ischemia (272).
Sex hormones can induce a hypercoagulable state, which may contribute to the development of cerebral venous thrombosis complicating pregnancy and the puerperium (85). Estrogen increases plasma levels of fibrinogen and clotting factors VII, VIII, IX, X, and XII.
Estrogens can alter cerebrovascular tone either by acting directly on vascular smooth muscle or by altering central prostaglandin, serotonin, opioid, or prolactin metabolism (234; 34). Many of the detrimental effects of aging on ischemic stroke outcome in females can be replicated by ovariectomy, suggesting that hormones such as estrogen play a neuroprotective role (171). Animal models have also demonstrated evidence of estradiol-mediated protection in hypertensive encephalopathy (68).
Premenopausal women are less likely to develop hypertension than age-matched men, but after age 60 the incidence of hypertension increases in women and surpasses that seen in older men (111). A decline in estrogen levels with age may be involved in the increase in hypertension in older women (111). Brain regions important for the regulation of sympathetic nerve activity (eg, the subfornical organ, the paraventricular nucleus, and the rostral ventral lateral medulla) also express specific subtypes of estrogen receptors (111).
Polymorphisms in the estrogen receptor β gene (ESR2) are associated with an increased risk of first-ever stroke in Chinese women, and among Chinese women with a specific polymorphism the use of combined oral contraceptives significantly increased the risk of hemorrhagic stroke—a multiplicative gene-environment interaction (295).
The prevalence of mitral valve prolapse is increased among users of oral contraceptives with ischemic stroke (81; 223).
Female sex hormones may predispose to bleeding from both aneurysms and arteriovenous malformations, although the pathophysiological mechanisms underlying these phenomena remain controversial (74).
In oral contraceptive users, cigarette smoking and age greater than 35 years significantly increase the risk of subarachnoid hemorrhage (198; 254).
Catamenial epilepsy. It has been known for 50 years that estrogen priming lowers the seizure threshold in the hippocampus in animal models (265), and similarly it was soon recognized that administration of estrogen-based hormonal therapies can increase seizure frequency in some women with epilepsy. It is now recognized that estrogens have epileptogenic properties whereas progestins have anticonvulsant properties (189; 62; 280). Estrogen both augments glutamatergic neurotransmission and suppresses GABAergic neurotransmission, favoring epileptogenesis, whereas progesterone has the opposite effect (189; 62). Cyclical changes in the circulating levels of estrogens and progesterone play a central role in the development of catamenial epilepsy (280; 215).
Synaptic functioning and neuronal excitability in the hippocampus are subject to both long-term and short-term excitatory modulation by sex steroids (292; 293). In particular, intracellular estrogen receptors are present in the hippocampus allowing estrogen to have long-term genomic effects with influence synaptic transmission (293). Estrogen and progesterone also have rapid nongenomic effects on CA1 neurons relevant to synaptic transmission over periods of seconds to minutes (293). A progesterone metabolite (ie, 3α-hydroxy-5α-dihydroprogesterone) binds to the GABAA receptor to potentiate the GABA-activated chloride current in CA1 neurons (168) and estradiol directly increases NMDA-mediated receptors of glutamate activity at the neuronal membrane, facilitating excitation and inducing repetitive firing of hippocampal pyramidal neurons in CA1 (267; 249; 248; 293). Dendritic spine density on CA1 hippocampal pyramidal cells also fluctuates during the menstrual cycle as a function of estradiol levels, using a mechanism that requires activation of NMDA receptors (294; 115). In addition, estriol also inhibits GABA and promotes kindling and epileptiform discharges (03); although estriol is only produced in significant quantities during pregnancy (via placental aromatization of fetal androgen), it can be synthesized in smaller quantities in nonpregnant individuals (in the liver by hydroxylation of estrone).
Progesterone has a neuroprotective effect on hippocampal neurons in seizure models induced by kainic acid (91); progesterone’s anticonvulsant and neuroprotective effects are apparently due to the steroid's actions on GABAA-benzodiazepine receptor complexes rather than intracellular progesterone receptors (91).
Seizures during pregnancy. Increased seizure activity during pregnancy may result from two different effects: a dominant estrogenic effect early in pregnancy that directly affects the central nervous system to lower the seizure threshold, and a decrease of at least 50% in plasma levels of anticonvulsant drugs late in pregnancy (209). In general, plasma anticonvulsant levels fall during pregnancy and rise during the puerperium (136). During pregnancy, serum levels of phenytoin, phenobarbital, and valproic acid may decrease by 30% to 40% of pregestational levels, with a lesser decline in carbamazepine. Primidone levels are reportedly stable during pregnancy, but the concentration of primidone-derived phenobarbital is reduced (146; 110). Several factors contribute to the fall in plasma anticonvulsant levels fall during pregnancy, including reduced absorption, increased volume of distribution, reduced protein binding, increased clearance, and noncompliance (136).
Movement disorders. Oral contraceptives may unmask latent chorea by augmenting dopaminergic neurotransmission in basal ganglia previously damaged by rheumatic or hypoxic encephalopathy (234).
Intracranial malignancies. Sex steroid receptors have also been reported in malignant lymphomas, metastatic breast cancers, hemangioblastomas, and anaplastic ependymomas, suggesting that the natural history of these neoplasms may be influenced by sex hormones and their antagonists (143; 202; 138; 246).
The greater prevalence of meningioma in obese individuals may be related to higher circulating estrogen levels derived from the aromatization of androstenedione to estrone in adipocytes (139). Although estrogens promote the growth of meningiomas, the presence of progestin receptors may well indicate a more favorable prognosis because progesterone receptor-negative meningiomas have been associated with a greater tendency for brain invasiveness, higher mitotic indices, and necrosis (266).
Astroglial tumors predominantly express estrogen receptor beta, and expression levels reportedly decline with increasing histological grade of malignancy (29; 36).
Oligodendrogliomas have also been reported to contain sex steroid receptors and could theoretically be subject to hormonal manipulations (281; 203).
Neuroimmunologic disorders. Over 50% of patients with multiple sclerosis experience cognitive deficits, and hippocampal-dependent memory impairment has been reported in more than 30% of these patients. Although postmortem pathology studies and in vivo magnetic resonance imaging demonstrate that the hippocampus is targeted in multiple sclerosis, the neuropathology underlying hippocampal dysfunction remains unknown (301). Prolactin does not fall in the sex hormone group. However, given its extraordinary neuroprotective and remyelinating properties, it is now being considered as a disease-promoting factor in multiple sclerosis (60). Reduction in the exacerbation of multiple sclerosis during pregnancy has been thought to be from gestational immunosuppression of estradiol, progesterone, human chorionic gonadotropin, human placental lactogen, cortisol, alpha-fetoprotein, and interleukin-10 (122; 56).
In animal studies, pregnancy significantly delays the onset of experimental allergic encephalomyelitis (a model for multiple sclerosis) after inoculation with spinal cord homogenate or myelin basic protein (134; 86; 26).
Dementia. Two thirds of patients with Alzheimer disease are women. Gonadal steroids are thought to contribute to the gender disparity in Alzheimer disease. The “estrogen hypothesis” posits that sex hormones (especially 17β-estradiol) exert a neuroprotective effect by shielding females’ brains from disease development whereas postmenopausal estrogen dysfunction may exacerbate or precipitate the pathophysiological changes underlying Alzheimer disease in women (207). Indeed, the onset of menopause is associated with the emergence of Alzheimer disease-related brain changes in women in contrast to men of the same age (207). In particular, estrogens reduce the deposition of fibrillar beta-amyloid and modulate apolipoprotein E expression, thus, ultimately suppressing neuritic plaque formation (231; 114).
Neuropsychiatric symptoms. Estrogen may facilitate drug abuse in women by interacting with reward- and stress-related systems (19). Females are more vulnerable than males to key phases of the addiction process including initiation, drug bingeing, and relapse (19). In addition, phases of the menstrual cycle when estrogen levels are high are associated with enhanced positive subjective measures following cocaine and amphetamine administration. Similarly, in animal studies, the administration of estrogen increases drug taking and facilitates the acquisition, escalation, and reinstatement of cocaine-seeking behavior.
Over 90% of menstruating women report some premenstrual symptoms such as headaches and moodiness. Proposed causes include an increased luteal phase estrogen-to-/progesterone ratio, hypothyroidism, hyperprolactinemia, and disordered renin-angiotensin-aldosterone axis (217; 216). Estradiol augments N-methyl-D-aspartate-mediated glutamate receptor activity whereas progesterone enhances gamma-aminobutyric acid-mediated chloride conductance, but it is unclear whether premenstrual dysphoric disorder can be explained by these mechanisms.
Sleep disorders. Estrogen and progestin may help improve sleep in hypogonadal women by shortening mean sleep latencies, prolonging the duration of rapid eye movement sleep periods and reducing nocturnal movement arousals (238; 201; 128). Progestins have also been shown to improve hypoventilation in a patient with central sleep apnea (188).
Neuromuscular disorders. Catamenial sciatica or low back pain is seen, with ectopic endometrial tissue destroying lumbar vertebrae or even invasion of the lumbosacral plexus in the retroperitoneal space and implantation within the sciatic nerve sheath.
Patients with myotonic dystrophy may have dysfunction of testicular peritubular myoid cells and corpus cavernosum smooth muscle, contributing to hypergonadotropic hypogonadism and impotence in men (178).
Abnormally high estrone levels have been reported in male patients with motor neuron disorders like amyotrophic lateral sclerosis, bulbospinal muscular atrophy (Kennedy disease), Kugelberg-Welander disease, and Duchenne muscular dystrophy (271). Testosterone, luteinizing hormone, and follicle-stimulating hormone levels were all essentially normal, except for low follicle-stimulating hormone levels in Duchenne muscular dystrophy patients. Because these patients were not overweight and did not have liver or glandular abnormalities, the elevated serum estrone levels presumably resulted from increased peripheral androgen-to-estrogen conversion.
Kennedy disease, or spinal and bulbar muscular atrophy, is an X-linked neuromuscular disease caused by an abnormal CAG trinucleotide repeat expansion in the androgen receptor gene. During protein synthesis, the CAG repeats are translated into a series of uninterrupted glutamine residues, forming what is known as a polyglutamine tract ("polyQ"). Such polyglutamine tracts are subject to increased aggregation and deposition of misfolded proteins. Therefore, spinal and bulbar muscular atrophy belongs to a family of “polyQ diseases,” a group of fatal neurodegenerative disorders caused by protein-mediated, toxic, gain-of-function mechanisms that include dentato-rubro-pallido-luysian atrophy (DRPLA), Huntington disease, and various inherited spinocerebellar ataxias (ie, types 1- 3, 6, 7, and 17).
Disorders of growth hormone. Reductions in sexual desire and arousability are reported in male and female patients with disorders of growth hormone (either growth hormone deficiency or acromegaly), together with an impairment of erectile function in men with these disorders, and it remains unclear whether these problems are directly dependent on the growth hormone defect or excess or whether they are consequence of the hypogonadism or any other clinical complications affecting sexual function (92).
Porphyria. The principal acute porphyrias include acute intermittent porphyria, hereditary coproporphyria, and variegate porphyria. Each of these is due to a separate genetic defect in the pathway of heme synthesis.
In hepatocytes, a critically low level of intracellular heme triggers overproduction of the precursor molecules, δ-aminolevulinic acid and porphobilinogen. Raised concentrations of δ-aminolevulinic and porphobilinogen are associated with inherited deficiency of hydroxmeythyl bilane synthase in acute intermittent porphyria and with allosteric inhibition of hydroxmeythyl bilane synthase by accumulating coproporphyrinogen and or protoporphyrinogen in variegate porphyria and hereditary coproporphyria (182).
Although the pathogenesis of attacks is not completely understood, δ-aminolevulinic acid may be the toxic agent that acts on nerves because other disorders associated with excess production of δ-aminolevulinic acid but not porphobilinogen (eg, lead poisoning and hereditary tyrosinemia) have similar clinical presentations to acute intermittent porphyria (35; 256). This is not the full explanation, though, because plasma and urinary δ-aminolevulinic acid levels correlate poorly with porphyria symptoms (256).
Most attacks of acute intermittent porphyria are precipitated by hormonal factors (256), and cyclic symptoms and catamenial porphyric crises have been reported in patients with acute intermittent porphyria due to a triggering effect of menstrual cycle hormones (302; 16; 103; 17; 01; 127). Women with acute intermittent porphyria frequently have cyclic symptoms (132; 01), particularly during the luteal phase of their menstrual cycles (01). Similarly, most females affected by catamenial attacks have premenstrual attacks (ie, in the luteal phase of the menstrual cycle) (16). In a population-based study in Finland, nearly one third of the women had symptoms of porphyria associated with the menstrual cycle but these seldom proceeded to an acute attack (132). Nevertheless, some patients experience disabling attacks with almost every menstrual cycle (16).
Administration of oral contraceptives, progestins, or androgens can interrupt ovulation and have been beneficial in preventing perimenstrual attacks in some patients (197; 103) but they also precipitated attacks of porphyria in others, including some with previously latent disease (145; 290; 302; 196; 142; 17; 37). In a population-based study in northern Sweden, more than half of the women with acute intermittent porphyria had used oral hormonal contraceptives and about 25% of oral contraceptive users with manifest acute intermittent porphyria reported attacks associated with such drugs (17). In addition, danazol, a synthetic steroid with weak androgenic properties, was used in an attempt to prevent cyclical attacks but instead exacerbated the disease (142). Withdrawal of oral contraceptives has also been anecdotally reported to trigger attacks (95).
Some preliminary studies demonstrated an increase in porphobilinogen but not coproporphyrin or uroporphyrin with oral contraceptive agents (δ-aminolevulinic was not measured) (129), whereas later studies with low-dose oral contraceptives found that they did not affect measured porphyrin precursors (including δ-aminolevulinic) or urinary porphyrin excretion (103).
The frequent exacerbations in women with porphyria treated with oral contraceptives, progestins, or androgens prompted consideration of novel alternatives such as agonistic analogues of gonadotropin-releasing hormone (Gn-RH; eg, “D-His“). Gonadotropin-releasing hormone analogues can suppress ovulation and cyclical increases in ovarian steroids without inducing δ-aminolevulinic acid synthase 1; this inhibits porphyrin precursor excretion (though not to normal levels) enough to suppress cyclic attacks in acute intermittent porphyria and hereditary coproporphyria (16; 296; 123). The optimal duration of gonadotropin-releasing hormone analogue administration is unknown.
In the dominantly transmitted acute porphyrias, a functional gene is inherited from the unaffected parent, so residual enzyme activity is typically 50% or normal, which is generally sufficient for heme homeostasis (22). Nevertheless, upregulation of δ-aminolevulinic acid synthase may cause accumulation and release of porphyrins and their precursors from the liver (256); this can occur cyclically due to normal hormonal oscillations in the menstrual cycle or with administration of various medications such as oral contraceptives and testosterone.
Benign intracranial hypertension. Benign intracranial hypertension (pseudotumor cerebri) can be secondary to estrogen-mediated effects on the blood-brain barrier, which may explain the female predilection for this disorder (303).
Traumatic brain injury. Sex steroid regulation of the balance of neuroexcitatory and neuroinhibitory activities may have a role in modulating clinical susceptibility to different neurologic conditions such as migraine, catamenial epilepsy, premenstrual dysphoric disorder, and premenstrual syndrome (89).
Estrogens can alter cerebrovascular tone by either acting directly on vascular smooth muscle or by altering central prostaglandin, serotonin, opioid, or prolactin metabolism (234; 34). Many of the detrimental effects of aging on ischemic stroke outcome in females can be replicated by ovariectomy, suggesting that hormones such as estrogen play a neuroprotective role (171). The late luteal phase decline in plasma estradiol appears to play an important role in the precipitation of catamenial migraine (172; 283). Many of the detrimental effects of aging on ischemic stroke outcome in females can be replicated by ovariectomy, suggesting that hormones such as estrogen play a neuroprotective role (171).
Estrogens and progestins have been shown to have epileptogenic and anticonvulsant properties, respectively (189; 62; 280). Estrogen augments glutamatergic and suppresses GABAergic neurotransmission, favoring epileptogenesis, whereas progesterone has the opposite effects (189; 62). Some investigations have demonstrated the existence of at least three patterns of catamenial seizure exacerbation: perimenstrual and periovulatory in ovulatory cycle, and entire luteal phase in anovulatory cycle. Cyclical changes in the circulating levels of estrogens and progesterone play a central role in the development of catamenial epilepsy (280). It has been recognized that oral contraceptives may unmask latent chorea by augmenting dopaminergic neurotransmission in basal ganglia previously damaged by rheumatic or hypoxic encephalopathy (234).
Over 50% of patients with multiple sclerosis experience cognitive deficits, and hippocampal-dependent memory impairment has been reported in more than 30% of these patients. Although postmortem pathology studies and in vivo magnetic resonance imaging demonstrate that the hippocampus is targeted in multiple sclerosis, the neuropathology underlying hippocampal dysfunction remains unknown (301). Prolactin does not fall in the sex hormone group. However, given its extraordinary neuroprotective and remyelinating properties, it is now being considered as a disease-promoting factor in multiple sclerosis (60).
Sex steroid receptors have also been reported in malignant lymphomas, metastatic breast cancers, hemangioblastomas, and anaplastic ependymomas, suggesting that the natural history of these neoplasms may be influenced by sex hormones and their antagonists (143; 202; 138; 246). Astroglial tumors predominantly express estrogen receptor beta, and expression levels reportedly decline with increasing histological grade of malignancy (29; 36). Oligodendrogliomas have also been reported to contain sex steroid receptors and could theoretically be subject to hormonal manipulations (281; 203). Although estrogens have been shown to enhance cerebral endothelial cell permeability and posttraumatic brain edema, progesterone suppresses posttraumatic cerebral edema and intracranial hypertension through the inhibition of cerebrospinal fluid production by the choroid plexus and reduction in blood-brain barrier permeability (149; 303; 221; 83; 97).
Sex hormone-induced disorders involve both white and gray matter. Reduction in the exacerbation of multiple sclerosis during pregnancy has been thought to be from gestational immunosuppression of estradiol, progesterone, human chorionic gonadotropin, human placental lactogen, cortisol, alpha-fetoprotein, and interleukin-10 (122; 56). Estrogens have been shown to reduce the deposition of fibrillar beta-amyloid and to modulate apolipoprotein E expression, thus, ultimately suppressing neuritic plaque formation (231; 114).
Progesterone is a potent neurosteroid that can protect damaged cells in the central and peripheral nervous systems and has rapid actions that go well beyond its effects on the classical intranuclear progesterone receptor. Progesterone holds promise as a treatment for traumatic brain injury. Its multiple neuroprotective mechanisms of action may work synergistically to prevent the death of neurons and glia, leading to reduced morbidity and mortality following traumatic brain injury (27; 255).
Pain. Pain-related neural processing varies across the menstrual cycle with fluctuating sex hormone levels (275). In addition, testosterone can decrease pain induced by electrical stimulation whereas cortisol can increase pain (57).
Stress response. Sex differences in stress responses can be found at all stages of life and are largely driven by gonadal hormone changes that occur over dynamic periods of development and maturation (25).
|
• No gender difference in migraine prevalence is apparent before puberty, but during the reproductive years, migraine is three times more common in women than men. | |
|
• In women, migraine attack frequency and severity vary with reproductive status. | |
|
• Among women migraineurs, both in the general population and presenting to specialist clinics, at least half identify menstruation as a trigger for attacks, and between one fifth and one third of the subgroup of women with migraine without aura experience migraine attacks associated with menstruation. | |
|
• Compared with all other phases of the menstrual cycle, incidence of migraine without aura is greatest during a 5-day perimenstrual period (ie, occurring on days -2 to +3 of menstruation). | |
|
• Compared with migraine at other times of the cycle, menstrual attacks last longer (some more than 72 hours) and are more severe, more likely to relapse, less responsive to pharmacologic treatment, and associated with greater menstrual distress and work-related disability. |
Premenstrual syndrome. Premenstrual syndrome occurs in approximately 30% of women during their reproductive years.
Migraine. There are significant gender-related differences in the epidemiology and natural history of migraines such that they need to be separately analyzed for men and women (90). No gender difference in migraine prevalence is apparent before puberty, but during the reproductive years, migraine is three times more common in women than men (240; 39; 34). In women migraine attack frequency and severity vary with reproductive status (159; 156; 39).
Migraines are three times as common in adult women as in men; however, no gender difference in the prevalence of migraine is apparent before puberty (240; 34). Almost two thirds of women with migraine experience perimenstrual exacerbations of their headaches (catamenial migraine). Headaches attenuated by pregnancy may relapse at the time of parturition due to a sudden fall in sex hormone levels (230).
Menstrual migraine (catamenial migraine). Among women migraineurs, both in the general population and presenting to specialist clinics, at least half identify menstruation as a trigger for attacks (84; 66; 161; 102; 78; 61; 06; 159; 39; 155), and between one fifth and one third of the subgroup of women with migraine without aura experience migraine attacks associated with menstruation (224). The peak incidence of migraine during the menstrual cycle occurs on the days directly before and after the first day of menstruation, whereas the lowest risk for headache is around the expected time of ovulation (125; 258; 78; 159; 155). For most women with menstrual migraine, migraine also occurs at other times of the month (ie, “menstrually related” migraine); fewer than 10% to 20% of women report migraine exclusively with menstruation and at no other time of the month (ie, “pure” menstrual migraine) (161; 102; 63; 78; 159; 155; 282; 226).
Compared with all other phases of the menstrual cycle, incidence of migraine without aura is greatest during a 5-day perimenstrual period (ie, occurring on days −2 to +3 of menstruation) (125; 258; 78; 159; 226).
In a longitudinal E-diary study among 526 premenopausal women with migraine, prevalence of menstrual migraine did not differ significantly between women with migraine without aura and migraine with aura (59% versus 53%, respectively) (278). The increased risk of migraine attacks without aura during the perimenstrual window did not differ significantly for women with migraine without aura and those with migraine with aura. The perimenstrual window was not associated with an increased risk of attacks with migraine aura. Women with migraine with aura more often reported increased migraine frequency during pregnancy and breastfeeding compared to women with migraine without aura.
Compared with migraine at other times of the cycle, menstrual attacks last longer (some more than 72 hours), are more severe, more likely to relapse, less responsive to pharmacologic treatment, and associated with greater menstrual distress and work-related disability (30; 258; 61; 06; 100; 159; 159; 159; 75; 135; 155; 167; 199; 226). Among women with menstrually-related migraine, menstrual headaches are associated with a higher pain score than other attacks (159; 155; 226). In a study using diary data from 155 women, migraine was most likely to occur perimenstrually and was more likely to be severe at this time: indeed, compared with all other times of the cycle, migraine was 1.7 times more likely to occur during the two days before menstruation and 2.1 times more likely to be severe and 2.5 times more likely to occur during the first three days of menstruation and 3.4 times more likely to be severe (159).
Catamenial epilepsy. The occurrence and distribution of patterns of catamenial epilepsy were studied in a prospective, observational study of a heterogenous cohort of women with epilepsy on no hormonal therapies (285). The authors measured progesterone concentrations for one to three cycles in women who recorded one or more menstrual cycles with one or more seizures. Catamenial patterns were defined as 2-fold or greater than average daily seizure frequency around menstruation (C1), ovulation (C2), and for anovulatory cycles, from midcycle through menstruation (C3). Twelve of 23 (52%) eligible women met criteria for catamenial epilepsy: of those with catamenial epilepsy, five demonstrated only a C1 pattern, two only a C2 pattern, and five a combined C1/C2 pattern.
Cerebrovascular disease. Hypertension, migraine, and age greater than 35 years old were associated, but independent, risk factors for cerebral infarction in patients taking oral contraceptives (48; 113). Although less often implicated than estrogens, progestins may contribute to the danger of cerebral infarction by promoting hypertension, hypercoagulability, and adverse serum lipoprotein levels (260; 270).
There are significant gender-related differences in the epidemiology and natural history of migraines such that they need to be separately analyzed for men and women (90). Epilepsy may worsen around the time of ovulation or premenstrually (catamenial epilepsy) and during pregnancy (179; 108). The course of epilepsy and its management, therefore, is greatly influenced by specific phases of the reproductive cycle.
Movement disorders. Epidemiological studies have suggested that early menopause may be a risk factor for the development of Parkinson disease (32; 206; 147; 233).
Patients with chorea gravidarum are at increased risk of later developing oral contraceptive-related dyskinesias (93; 208). There is recurrence of chorea in almost one of five women with subsequent pregnancies (96).
The greater prevalence of meningioma in obese individuals may be related to higher circulating estrogen levels derived from the aromatization of androstenedione to estrone in adipocytes (139). Although estrogens promote the growth, the presence of progestin receptors may well indicate a more favorable prognosis because progesterone receptor-negative meningiomas have been associated with a greater tendency for brain invasiveness, higher mitotic indices, and necrosis (266).
Neuroimmunology. The higher prevalence of multiple sclerosis in females, along with the observed modulation of disease activity during pregnancy and the postpartum period, has suggested a hormonal influence in multiple sclerosis (60). In animals, pregnancy significantly delays the onset of experimental allergic encephalomyelitis (a model for multiple sclerosis) after inoculation with spinal cord homogenate or myelin basic protein (134; 86; 26).
Similar to studies published in the past, no significant differences on gender and traumatic brain injury were seen in a study by Niemeier and colleagues (193). The premenstrual syndrome occurs in approximately 30% of women during their reproductive years.
Psychotic disorders characterized by extreme agitation, hallucinations, paranoid delusions, incoherent speech, and mood lability may arise during the postpartum period or may recur consistently during the late luteal phase of the cycle (284).
Data indicate that estrogen may facilitate drug abuse in women. For example, phases of the menstrual cycle when estrogen levels are high are associated with enhanced positive subjective measures following cocaine and amphetamine administration in women (19).
Neuromuscular. Peripheral nervous system involvement is relatively less common compared to the central nervous system disorders.
Porphyria. In a population-based study in northern Sweden, more than half of the women with acute intermittent porphyria had used oral hormonal contraceptives and about 25% of oral contraceptive users with manifest acute intermittent porphyria reported attacks associated with such drugs (17).
In animals, pregnancy significantly delays the onset of experimental allergic encephalomyelitis (a model for multiple sclerosis) after inoculation with spinal cord homogenate or myelin basic protein (134; 86; 26).
Epidemiological studies have suggested that early menopause may be a risk factor for the development of Parkinson disease (32; 206; 147; 233). Patients with chorea gravidarum are at increased risk of later developing oral contraceptive-related dyskinesias (93; 208). There is recurrence of chorea in almost one of five women with subsequent pregnancies (96).
The greater prevalence of meningioma in obese individuals may be related to higher circulating estrogen levels derived from the aromatization of androstenedione to estrone in adipocytes (139). Although estrogens promote the growth, the presence of progestin receptors may well indicate a more favorable prognosis because progesterone receptor-negative meningiomas have been associated with a greater tendency for brain invasiveness, higher mitotic indices, and necrosis (266).
Similar to studies published in the past, no significant differences on gender and traumatic brain injury were seen in a study by Niemeier and colleagues (193). The premenstrual syndrome occurs in approximately 30% of women during their reproductive years. Psychotic disorders characterized by extreme agitation, hallucinations, paranoid delusions, incoherent speech, and mood lability may arise during the postpartum period or may recur consistently during the late luteal phase of the cycle (284). Data indicate that estrogen may facilitate drug abuse in women. For example, phases of the menstrual cycle when estrogen levels are high are associated with enhanced positive subjective measures following cocaine and amphetamine administration in women (19).
Peripheral nervous system involvement is relatively less common compared to the central nervous system disorders. Catamenial sciatica or low back pain is seen, with ectopic endometrial tissue destroying lumbar vertebrae or even invasion of the lumbosacral plexus in the retroperitoneal space and implantation within the sciatic nerve sheath. On occasions where evidence of endometriosis is minimally seen, surgical exploration of the sciatic nerve may be required for diagnosis (24; 54). Abnormally high estrogen levels have been reported in male patients with motor neuron disorders like amyotrophic lateral sclerosis and bulbospinal muscular atrophy (Kennedy syndrome), Kugelberg-Welander disease, Duchenne muscular dystrophy, and Crow-Fukase syndrome (POEMS syndrome) (271).
Prevention relies on control of the underlying sex hormonal dysfunction.
The prognosis of any neurologic event occurring in the setting of sex hormonal dysfunction depends on the specific clinical situation and etiology of the process in question.
|
• Combined hormonal contraceptives have been considered contraindicated for women who have migraine with aura, particularly because the high estrogen-dose formulations of these drugs used in the 1960s and 1970s clearly increased the risk of ischemic stroke in this group of women. | |
|
• Systematic reviews have found an additive increase in stroke risk with combined hormonal contraceptive use in women with migraine with aura, with some studies suggesting a 2- to 4-fold increased risk of stroke among women with migraine who use combined hormonal contraceptives compared with nonuse. | |
|
• Combined hormonal contraceptives should not be routinely employed in females who have migraine with aura. | |
|
• Combined oral contraceptives can initiate or aggravate migraine without aura in some women, though the headaches generally improve after several months of combined oral contraceptives use. | |
|
• With persistent migraine without aura while on sustained use of combined oral contraceptives, attacks are more likely to occur during the pill-free week, a condition referred to as oral contraceptive-induced menstrual migraine. | |
|
• Combined oral contraceptives are useful for women with menstrual migraine who require contraception, although attacks tend to occur during the pill-free interval; if these are contraindicated (as is at least relatively the case in migraine with aura), depot progestogen is an alternative as it also inhibits ovulation and can improve migraine, provided amenorrhea is achieved. | |
|
• Oral contraceptive failure is associated with the use of older enzyme-inducing anticonvulsants but not with newer nonenzyme-inducing antiepileptic medications. | |
|
• Several different approaches have been proposed for treatment of catamenial epilepsy, including: (1) premenstrual or periovulatory supplementation of anticonvulsant doses; (2) addition of an adjunctive antiepileptic drug; (3) cyclic administration of acetazolamide, a mild diuretic with weak antiepileptic activity; and (4) progesterone supplementation. |
Menopausal hormone therapy. As reported initially in 2013, ischemic stroke risk was increased during menopausal hormone replacement therapy in the Women's Health Initiative but there was no significant effect after the cessation of therapy (170) and no difference in mortality at long-term follow-up (169).
In 2016, an observational cohort study of combined oral contraceptive therapy in 5 million French women found that for the same type of progestogen, an estrogen (ethinylestradiol) dose of 20 μg versus 30 to 40 μg was associated with lower risks of ischemic stroke, myocardial infarction, and pulmonary embolism (288).
In 2017, a pooled analysis of data from population-based cohort studies found that menopausal hormone therapy is not associated with increased risks of incident ischemic or hemorrhagic stroke when initiated early in relation to menopause onset, regardless of the route of administration, type of hormone therapy, active ingredient, or duration of use (49). Instead, initiation of menopausal hormone therapy within five years following menopause onset, as compared to never use, is associated with a decreased risk of ischemic and hemorrhagic stroke (49). However, late initiation of single hormone therapy with conjugated equine estrogen is associated with elevated risks of ischemic and hemorrhagic stroke, and late initiation of combined hormone therapy is associated with an elevated risk of hemorrhagic stroke (49).
Another large cohort of Danish women suggested that the specific route of administration was important, finding that although oral estrogen increased risk of stroke, absorption through the skin had no impact and vaginal estrogen actually had a decreased risk (150). When given by nonoral routes, there was no association between hormone replacement therapy and stroke and instead hormone replacement therapy may have been preventative (150).
In several large randomized controlled studies, menopausal hormone therapy did not protect against either stroke or coronary artery disease among women with established vascular disease and instead it may have worsened outcomes in this high-risk population (245; 33; 268).
For hormone replacement therapy in menopausal women with migraine, nonoral routes of estrogen delivery provide stable levels and are more likely to improve migraine than oral estrogens, which produce variable day-to-day levels (190; 154; 155). Optimal doses of continuous estrogens can control both migraine and menopausal symptoms but too high a dose of estrogen, particularly if coupled with surges of endogenous estrogen, can trigger migraine auras (154). Using only the lowest doses of transdermal estrogen necessary to control vasomotor symptoms will minimize the risk of unwanted side effects (154; 158). Note that in contrast to contraceptive doses of ethinylestradiol, the presence of migraine aura does not contraindicate use of physiological doses of natural estrogen (158). Additional progestogen, necessary for women without a prior hysterectomy to minimize risks of endometrial cancer, can exacerbate migraine (154).
Combined hormonal contraceptives. Combined hormonal contraceptives have been considered contraindicated for women who have migraine with aura, particularly because the high-estrogen-dose formulations of these drugs used in the 1960s and 1970s clearly increased the risk of ischemic stroke in this group of women (45). Systematic reviews have found an additive increase in stroke risk with combined hormonal contraceptive use in women with migraine with aura, with some studies suggesting a 2- to 4-fold increased risk of stroke among women with migraine who use combined hormonal contraceptives compared with nonuse (264; 239).
Combined hormonal contraceptives should not be routinely employed in females who have migraine with aura (291; 50; 64; 239). If migraine with aura develops in a woman on combined oral contraceptives, these should generally be discontinued, and other methods of contraception should be used instead. This issue, though, is controversial. Some have considered migraine with aura to be an “absolute contraindication” to the use of combined oral contraceptives, and guidelines from the U.S. Centers for Disease Control and Prevention still consider combined oral contraceptives to have “unacceptable health risks (method not to be used)” (64) whereas other authorities advocate a risk/benefit assessment that does not preclude their use in this situation (45) or indicate only that “oral contraceptives should be used with caution as this may add to the risk of stroke in this population” (243). Based on the lower estrogen doses used in modern formulations, one group concluded that the risk of stroke among women taking low-dose oral combined hormonal contraceptives is “tenuous at best and perhaps nonexistent” (53). A systematic review noted a lack of good quality studies assessing risk of stroke associated with low dose estrogen use in women with migraine; the authors recommended that, “Since the absolute risk of stroke is low even in the presence of these risk factors, use of [combined hormonal contraceptives] in women who have migraine with aura should be based on an individualized assessment of harms and benefits” (239).
Some literature reviews and syntheses have concluded that stroke risk is not significantly increased in women who have migraine with aura with current hormonal contraceptive preparations that contain less than 30 μg of ethinyl estradiol; moreover, ultra-low-dose formulations containing less than 20 μg of ethinyl estradiol may help prevent menstrual migraine and reduce the frequency of aura (45). Other reviews have concluded that: (1) women using combined oral contraceptives have a higher risk of stroke, even with a lower estrogen dosage and different types of progestogen, regardless of the duration of use; and (2) use of combined oral contraceptives associated with migraine, smoking, hypertension, hypercholesterolemia, obesity, and a sedentary lifestyle further increases the risk of stroke (148). These disparities will only be resolved with better quality studies assessing risk of stroke associated with low-dose estrogen use in women with migraine. Progestogen-only contraceptives are considered safe (148).
Combined oral contraceptives can initiate or aggravate migraine without aura in some women, though the headaches generally improve after several months of combined oral contraceptives use (07; 08). With persistent migraine without aura while on sustained use of combined oral contraceptives, attacks are more likely to occur during the pill-free week, a condition referred to as oral contraceptive-induced menstrual migraine (07; 08).
In females taking combined oral contraceptive pills, if migraine without aura occurs during the pill-free interval in a cycle, options include: (1) using alternative contraception methods; (2) changing to a more estrogen-dominant pill; (3) adding low-dose estrogen supplementation after 21 days of combined oral contraceptives during the 7-day pill-free interval (43; 07; 08); (4) using extended-cycle combined oral contraceptive regimens (ie, greater than 28 days of active combined hormones) (261; 07; 44; 79; 08; 87); and (5) using a progestogen-only pill (07; 08). One extended-cycle combined oral contraceptive regimen requires taking the pill continuously for 9 weeks rather than 3 (ie, so-called "tricycling"), followed by the usual 7-day pill-free interval, producing five rather than 13 withdrawal bleeds per year (07; 08). Even longer extended regimens have been tried: compared to the standard 21/7-day oral contraception regimen, a 168-day extended regimen of combined oral contraceptive containing 3 mg of drosperinone and 30 mcg of ethinyl estradiol led to a decrease in headache severity along with improvement in work productivity and involvement in activities (261). A progestogen-only pill is a safe option even for women suffering from migraine with aura (in whom combined oral contraceptives are contraindicated) and its use can reduce the frequency of migraine attacks and the duration of aura symptoms (07; 08).
Combined oral contraceptives are useful for women with menstrual migraine who require contraception, although attacks tend to occur during the pill-free interval (154). If these are contraindicated (as is at least relatively the case in migraine with aura), depot progestogen is an alternative as it also inhibits ovulation and can improve migraine, provided amenorrhea is achieved (154). Oral progestogen-only contraception is not used in the management of menstrual migraine because it does not inhibit ovulation and is often associated with a disrupted menstrual cycle (154).
Oral contraceptive failure is associated with the use of older enzyme-inducing anticonvulsants, but not with newer nonenzyme-inducing antiepileptic medications (304; 40). Older enzyme-inducing anticonvulsants, like phenytoin, phenobarbital, primidone, ethosuximide, and carbamazepine induce the hepatic cytochrome P450 microsomal enzyme system, which, in turn, accelerates catabolism of endogenous and exogenous sex hormones (304; 133; 279). Oral contraceptive failure does not occur with valproic acid, which may instead inhibit cytochrome P450 enzymes, causing elevations in plasma steroid concentrations; valproic acid, however, may cause hyperandrogenism and polycystic ovaries (118; 204). Of the newer antiepileptic medications, lamotrigine, gabapentin, and vigabatrin do not induce the hepatic P450 microsomal enzyme system, and oral contraceptive failure has not been reported with these drugs (304; 257; 40). Topiramate and felbamate may affect contraceptive efficacy by affecting sex hormone pharmacokinetics (225).
Specific neurologic disorders. Several specific neurologic disorders may be amenable to hormonal therapies or require modifications in management during periods of significant changes in sex hormone levels.
Migraine. There are different ways of approaching a patient with migraine at various phases of life. The initial approach to the management of gestational or nongestational migraine should be nonpharmacological. This approach is critical during the first trimester when risks of teratogenicity and embryotoxicity are at the peak. Among the nonpharmacological migraine prophylaxis, only relaxation techniques, biofeedback in particular, and acupuncture have accumulated sufficient evidence in support of their efficacy and safety (04).
Pharmacotherapy for migraines can be abortive or prophylactic (55). The prophylactic properties of magnesium, riboflavin, and coenzyme Q10 are probably low, but their lack of severe adverse effects compared to other used medications makes them good treatment options. Some vitamins and dietary supplements have also been proposed (04). Serotonin 5-HT1D receptor agonists are effective for both noncatamenial and menstrual migraine (38). Lasmiditan, a high affinity and selective 5-HT1F receptor agonist, was effective in the treatment of perimenstrual migraine attacks in a randomized, double-blind, placebo-controlled clinical trial (165); lasmiditan treatment was associated with freedom from migraine-related head pain at two hours, early onset of efficacy, and sustained efficacy. Bromocriptine therapy (2.5 mg three times daily) has also been shown to reduce menstrual migraine in most patients (116; 173). Anti-CGRP (calcitonin gene-related peptide) monoclonal antibodies or CGRP receptor antagonists have good efficacy and safety in the treatment of menstrual migraine (124). Refractory cases of severe catamenial migraine may benefit from late luteal phase therapy with prostaglandin inhibitors (eg, naproxen, 250 to 500 mg orally twice daily) and mild diuretics (72). Danazol (200 mg twice daily for 25 days) has been utilized for premenstrual migraine associated with endometriosis (47). The triptans are currently rated by the United States Food and Drug Administration (FDA) as Category C agents. Soldin and colleagues have looked into the effects of the seven types of triptans currently available on the U.S. market (almotriptan, eletriptan, frovatriptan, naratriptan, rizatriptan, sumatriptan, and zolmitriptan) on pregnancy (250). Information on the use of sumatriptan during pregnancy is relatively more abundant, given that it has been on the market longer than the other triptans. There are no data to suggest teratogenicity for any of the triptans, although preterm birth rates appear to be elevated.
There are limited data that support the use of hormone contraceptive use in menstrually related migraines (51).
During pregnancy, the choices are complicated by safety concerns for the developing fetus (see Table 2).
|
Medication |
Safety |
Effectiveness |
|
Propranolol |
+++ |
+++ |
|
Memantine |
+++ |
++ |
|
Coenzyme Q10 |
+++ |
+ |
|
Magnesium |
+++ |
+ |
|
Onabotulinum toxin A |
++ |
+++ |
|
Amitriptyline/nortriptyline |
++ |
+++ |
|
Venlafaxine |
++ |
++ |
|
Gabapentin |
++ |
+ |
|
Riboflavin |
++ |
+ |
|
Verapamil |
++ |
+ |
|
Calcitonin gene-related peptide targeting agents |
+ |
+++ |
|
Topiramate |
+ |
+++ |
|
Candesartan |
+ |
++ |
|
Lisinopril |
+ |
++ |
|
Feverfew (Tanacetum parthenium) |
+ |
+ |
|
Valproic acid |
- |
+++ |
|
| ||
Menstrual migraine (catamenial migraine). The low frequency and constricted time period of attacks in most patients with menstrual migraine supports an initial symptomatic approach with specific drugs.
Acute treatment. For acute treatments, rizatriptan has the best overall evidence (152), but sumatriptan, rizatriptan, NSAIDs (eg, naproxen, mefenamic acid), and ergot derivatives are among other options (101; 38; 263). A network meta-analysis to compare the relative efficacy of treatments for menstrual migraine found that sumatriptan 100 mg is the most effective for acute treatment (298).
Preventative therapies. Preventative therapies may be considered in those who either have failed abortive medications or have attacks lasting longer than 2 days (174), but this should only be pursued once the association between migraine and menstruation has been confirmed with prospective records kept for a minimum of three cycles (154). They can be administered during only the perimenstrual time period or continuously throughout the menstrual cycle. Short-term prophylactic therapies are generally preferred because menstrual migraines generally last for only 1 to 4 days, but continuous prophylactic therapies may be considered in those with attacks that are refractory to short-term therapies. Prophylaxis for menstrual migraine should be tried for a minimum of three cycles before it is considered ineffective.
Short-term intermittent prophylactic (also called “mini-prophylaxis” or “mini-prevention”) options include perimenstrual prophylaxis with triptans, NSAIDs (eg, naproxen or mefenamic acid), magnesium, estrogen (percutaneous or transdermal), or dihydroergotamine (101; 06; 104; 263; 152). For females with predictable menstrual-related migraine that does not respond adequately to standard acute treatment, preventive treatment can be considered with triptans on the days migraine is expected (192; 50; 243; 152); frovatriptan (2.5 QD or BID), naratriptan (1 mg BID), and zolmiptriptan (2.5 mgs BID and 2.5 mgs TID) are effective preventative agents when administered for 4 to 5 days during the perimenstrual time period, though frovatriptan appears to be the triptan of choice based on overall efficacy in this patient group (243; 298). Naproxen sodium (eg, 550 mgs BID given 6 days before to 7 days after menses) is also effective for prevention of menstrual migraine (72).
Monoclonal antibodies (eg, galcanezumab, erenumab, or fremanezumab) designed to attach to and block calcitonin gene-related peptide (CGRP) are also effective for migraine prevention in women with menstrually related migraine (276; 166). For erenumab and fremanezumab, the reduction in migraine days under treatment was similar during the menstrual window and the remainder of the menstrual cycle (276).
Hormonal preventive therapies. Various options are available for hormonal treatment of menstrual migraine. Each of these has potential advantages and disadvantages (273), although evidence of prevention using hormonal treatments is poor (51; 28; 67).
Some recommend estrogen supplements for menstrual migraine prevention (eg, 1.5 mg of transdermal estradiol gel applied for 7 days, beginning 10 days after ovulation and continued through the second day of menstrual bleeding; or transdermal estradiol patches, 0.1 mg, started three days before the onset of menses and continued for 7 days) even though evidence from controlled trials is limited and inconsistent with some small trials reporting benefit (66; 70; 163), whereas others did not (11). Although perimenstrual percutaneous estradiol showed benefit during treatment in some trials, this was offset by deferred estrogen withdrawal, often triggering postdosing migraine shortly after the gel was stopped (66; 163). To minimize the issues of estrogen withdrawal, estrogen can be “added back” during the hormone-free interval: so, if withdrawal bleeding is scheduled, adequate estrogen supplementation (ie, estrogen add-back therapy) can be given with estradiol-17b during the pill-free week to limit the decrease to an equivalent of 10 mg of ethinyl estradiol or less, a level that can prevent estrogen-withdrawal headaches or menstrually related migraine (87). If the patient is menstruating regularly, additional progestogen for endometrial protection is not required. Other options include extended-cycle dosing of an ultralow-dose contraceptive ring and gonadotropic-releasing hormone antagonists (87).
A continuous preventative therapy is generally utilized for patients with irregular menses and those who have not had success with short-term-prevention approaches. One long-duration oral-contraceptive approach involves taking combined oral contraceptives containing both ethinyl estrogen and progestin continuously for 9 weeks rather than 3 (ie, so-called "tricycling"), followed by the usual 7-day pill-free interval, producing five rather than 13 withdrawal bleeds per year (141). Alternative nonhormonal therapies include standard prophylactic agents such beta-blockers, calcium channel blockers, tricyclic antidepressants, and anticonvulsants.
Note that many antiepileptic medications used in migraine prevention can affect the efficacy of oral contraceptives and hormonal treatments, so caution is warranted (152). Many antiepileptic medications can cause enzyme induction affecting oral contraceptives and other hormonal treatments. Topiramate at doses below 200 mg/day has the least effect on oral contraceptives.
Catamenial epilepsy. Several different approaches have been proposed for treatment of catamenial epilepsy including: (1) premenstrual or periovulatory supplementation of anticonvulsant doses; (2) addition of an adjunctive antiepileptic drug; (3) cyclic administration of acetazolamide, a mild diuretic with weak antiepileptic activity; and (4) progesterone supplementation (117; 297; 280). The current consensus in catamenial epilepsy focuses on progesterone supplementation during the luteal phase, with limited estrogen manipulations due to concerns that estrogen manipulation may cause seizure provocation (28). Although data from uncontrolled studies suggest that hormone therapy with progesterone may be useful in the treatment of catamenial epilepsy, the efficacy of progesterone for this indication has not been demonstrated in controlled trials (194). Variations in concentrations of antiepileptic drugs across the menstrual cycle may contribute to increased seizure susceptibility.
Movement disorders. Chorea gravidarum carries a good prognosis. The condition is usually self-limited, and premature delivery is rarely required. Women with a history of oral contraceptive-induced or gestational chorea should probably minimize further exposure to any estrogen-containing medications. In severe cases, use of neuroleptics may afford symptomatic relief (93; 208). In patients with Wilson disease, normalization of serum ceruloplasmin levels by estrogen administration is of no significant benefit and may produce deterioration in some patients (300).
In patients with Wilson disease, normalization of serum ceruloplasmin levels by estrogen administration is of no significant benefit and may produce deterioration in some patients (300).
Neuroimmunologic disorders. Although not FDA approved, intravenous steroids have been used as standard of care for multiple sclerosis attacks in pregnancy. Prophylactic therapy (eg, interferon-beta) should be discontinued three months before planned conception and should not be used during pregnancy or when breastfeeding (122; 195). In a study, intravenous immune globulin immediately postpartum seemed to have a beneficial effect on multiple sclerosis relapse rate in the first six months after delivery (106). Ziehn and colleagues demonstrated for the first time that testosterone is a viable therapeutic treatment option that can restore both hippocampal function and disease-associated pathology that occur during autoimmune disease (301).
Testosterone is a therapeutic treatment option that can potentially restore both hippocampal function and disease-associated pathology that occur during autoimmune demyelinating disease (301).
Dementia. The third Canadian Consensus Conference for the Diagnosis and Treatment of Dementia (2006) recommended against the use of estrogen-progestin replacement therapy for reducing the risk of dementia in postmenopausal women. It also concluded that there is insufficient evidence for or against the prescription of androgen replacement for cognitive dysfunction in elderly men.
In a cohort of postmenopausal women at risk for dementia, high and low insulin resistance groups revealed a significant metabolic decline of the medial prefrontal gyrus, irrespective of the randomized hormone therapy group (210).
Neuropsychiatric disorders. Psychotic disorders may be refractory to conventional therapies (neuroleptics, lithium, electroconvulsive therapy) but respond well to particular hormonal interventions, including the use of oral contraceptives and danazol (88; 69; 18).
Numerous hormonal and nonhormonal therapies, including oral contraceptives, bromocriptine, gonadotropin-releasing hormone agonists, diuretics, prostaglandin inhibitors, vitamin B6, and lithium, are prescribed for the management of premenstrual syndrome and premenstrual dysphoric disorder (216).
Although oral contraceptives may precipitate depression in susceptible individuals, estrogen replacement may help with postmenopausal depression (98; 181).
Neuropsychiatric disorders. Psychotic disorders that are refractory to conventional therapies (neuroleptics, lithium, electroconvulsive therapy) may respond well to specific hormonal interventions including the use of oral contraceptives and danazol (88; 69; 18).
Although oral contraceptives may precipitate depression in susceptible individuals, estrogen replacement may help with postmenopausal depression (98; 181).
Neuromuscular disorders. Symptoms of catamenial sciatica may show dramatic improvement with standard therapy for endometriosis, including danazol, progestins, and in refractory cases, bilateral oophorectomy (24; 151; 232).
In an anecdotal report, high-dose testosterone therapy yielded considerable symptomatic improvement in a patient with bulbospinal muscular atrophy (137).
Catamenial sciatica (endometriosis). Symptoms of catamenial sciatica may show dramatic improvement with standard therapy for endometriosis, including danazol, progestins, and in refractory cases, bilateral oophorectomy (24; 151; 232). In an anecdotal report, high-dose testosterone therapy yielded considerable symptomatic improvement in a patient with bulbospinal muscular atrophy (137).
Sleep disorders. One case reported that removal of a benign testosterone-producing ovarian tumor resolved obstructive sleep apnea (71). In addition, testosterone administration has been shown to increase hypocapnic apnea threshold in premenopausal women (299; 58).
Porphyria. In addition to standard treatment involving removal of precipitating factors and intravenous administration of hemin for acute attacks (15), gonadotropin-releasing hormone analogues have been utilized in the management of catamenial acute intermittent porphyria and hereditary coproporphyria (if cyclic attacks are frequent) (296; 05).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
General Neurology
Jan. 28, 2025
General Neurology
Jan. 23, 2025
General Neurology
Jan. 20, 2025
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025