

Movement Disorders
Acquired hepatocerebral degeneration
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Degenerative diseases of the central nervous system are a large and varied group of disorders that affect a range of neurologic function. Sleep disorders are commonly seen in patients with cerebral degenerative diseases. Much of this may be related to the underlying central nervous system damage to sleep regulatory centers of the brain. Sleep disorders may serve as a biomarker to predict development of a future neurodegenerative disorder. New research has suggested that disrupted sleep such as insomnia or sleep apnea may accelerate the degenerative process in conditions such as Alzheimer dementia and Parkinson disease. One potential mechanism is emerging evidence of the role of sleep in glymphatic clearance of metabolic waste products from the brain. Studies have demonstrated increased levels of beta-amyloid in cerebrospinal fluid of individuals with insomnia, sleep apnea, and disrupted sleep. Other studies have also shown that decreases in slow wave sleep (when glymphatic clearance seems highest) leads to a higher risk of dementia (68). Prompt attention to and treatment of sleep symptoms can result in significant improvement in quality of life, or possibly delay in progression of disease, and improvement in caregiver burden.
|
• Sleep disorders, such as chronic insomnia disorder, sleep apnea, restless legs syndrome, certain parasomnias, and circadian rhythm disorders, are disproportionally more common in patients with cerebral degenerative disorders than in the general population. | |
|
• Sleep disturbances in the setting of neurodegenerative disorders are sometimes secondary to localized damage to areas of the brain that control and regulate sleep and alertness. | |
|
• REM-sleep behavior disorder is a parasomnia frequently seen in patients with Parkinson disease and other alpha-synucleinopathies and can sometimes predate the motor and cognitive symptoms of the condition by several years or even decades. It is the first time that a sleep disorder can be used as a biomarker to predict a neurodegenerative disorder. | |
|
• Treatment of the underlying sleep disorder can not only help in improving quality of life, but may improve motor or cognitive symptoms of the underlying cerebral degenerative condition. | |
|
• There is emerging evidence that diagnosis and treatment of sleep disorders may delay onset or progression of neurodegenerative conditions such as dementia. |
The relationship between sleep disorders and neurodegenerative diseases has become increasingly more lucid as research into both areas has made significant progress. Indeed, a link between the two has been noted since the earliest descriptions of some neurodegenerative disorders. In the early 19th century, James Parkinson and his coworkers described clinical sleep abnormalities associated with extrapyramidal disorders (124). Subsequently, a variety of sleep disorders have been found in tandem with diseases such as Parkinson disease, multiple system atrophy, dementia with Lewy bodies (DLB), corticobasal degeneration, and others. However, the underlying sleep abnormalities were not extensively explored until relatively recently. In the latter half of the twentieth century, the advent of more sophisticated diagnostic techniques, such as polysomnography and improved EEG recordings, as well as the discovery of new treatments, allowed for major advances in the field (124). Emerging research is exploring how disrupted sleep may serve as a risk factor for developing neurodegenerative disorders or accelerating progression of the disease.
Sleep disorders are relatively common in neurodegenerative diseases, and the types and prevalence vary. The primary sleep disturbances in this class include insomnia, hypersomnia, parasomnias (including REM sleep behavior disorder), respiratory dysrhythmias, disturbed sleep-wake cycles, and excessive nocturnal motor activity (22; 94). For patients with neurodegenerative diseases, and dementia in particular, sleep disturbances may have a dramatic impact on function and quality of life. In this article, we describe some of the common presenting symptoms of these disorders and then discuss several of the neurodegenerative diseases in more detail. This review concentrates on Alzheimer disease, Parkinson disease, dementia with Lewy bodies, progressive supranuclear palsy, corticobasal degeneration, Pick disease, multiple system atrophy, olivopontocerebellar atrophy, and striatonigral degeneration.
The descriptions of sleep disorders will refer to the International Classification of Sleep Disorders, 3rd edition-Test Revision, published in 2023 (American Academy of Sleep Medicine 2014).
A number of symptomatic complaints are common in cerebral degenerative disorders. Patients with insomnia describe inadequate nighttime sleep, and the term insomnia itself refers to difficulty with initiating or maintaining sleep. This may be represented by difficulty falling asleep, frequent awakenings, early morning wakening, or feeling unrefreshed after sleeping. This will often result in feelings of daytime fatigue, irritability, mood changes, poor attention, trouble with motor skills, and may result in decreased ability to function at baseline during waking hours.
Hypersomnia, or excessive daytime sleepiness, is a complaint voiced by many patients with neurodegenerative disorders. Symptoms of hypersomnia include persistent sleepiness during waking hours, sleep attacks, trouble with concentration, irritability, anxiety, and impaired function ability during the daytime. Patients may find themselves falling asleep at inopportune times and places, which is often not relieved by sleeping at night, and can lead to frequent daytime naps, difficulty with memory, and even automatic behaviors for which the patient is largely amnestic. Hypersomnia can also lead to motor vehicle crashes or work-related accidents. Fatigue, distinct from sleepiness, is also a common complaint in patients with neurodegenerative disorders.
The parasomnias include a large group of disorders of arousal (NREM sleep parasomnias) or disorders associated with REM sleep. Patients with parasomnias may describe sleepwalking, sleep terrors, confusional arousals, complex behaviors, nightmares, and sleep paralysis. REM sleep behavior disorder is the most common parasomnia associated with neurodegenerative diseases and tends to present with dream enactment in the form of motor and verbal activity during sleep as a consequence of lack of the normal muscle atonia seen in REM sleep. The dream enactment activities can be mild or severe and may lead to injury to the patient and/or bed partner. REM sleep behavior disorder may predate other symptoms of Parkinson disease and other neurodegenerative diseases by up to several decades (138; 75; 43). In one study, the estimated 5-year risk of neurodegenerative disease was 17.7%, the 10-year risk was 40.6%, and the 12-year risk was 52.4% (132). Others have shown even higher rates, such as over 90% at 14 years (74). Furthermore, patients with Parkinson disease and REM sleep behavior disorder were found to be more likely to develop dementia as compared to patients who did not have this disorder at presentation (130) and may even predict future cognitive decline in memory and attention (37). The rates of phenoconversion from the onset of REM sleep behavior disorder diagnosis to expression of the alpha synucleinopathy is dose-dependent with time, that is the longer one waits from the onset of REM sleep behavior disorder diagnosis, the higher the risk of acquiring dementia. When researchers have looked closer at patients with “idiopathic” REM sleep behavior disorder, they have found prodromal or subtle motor abnormalities as well as nonmotor symptoms such as hyposmia, autonomic dysfunction, and cognitive deficits as compared to controls (19). Data from Olmsted County, Minnesota in patients with mild cognitive impairment and Parkinson disease indicated that progression to dementia and other neurodegenerative phenotypes occurred in most patients but those who develop mild cognitive impairment and subsequent dementia have clinical characteristics most suggestive of dementia with Lewy bodies (76).
Respiratory dysrhythmias or dysfunction may present as nocturnal stridor, apneic events (central, obstructive, or mixed), as well as cluster breathing, Cheyne-Stokes respiration, and other abnormalities in the rate, rhythm, and amplitude of respiration (22; 94). Disturbances in the normal circadian sleep-wake cycle are also common in many of these disorders. Symptoms include insomnia, excessive daytime sleepiness, inability to sleep at the desired time, and resultant impairment in daily function. Although circadian rhythms may be affected by both external and intrinsic factors, in the case of the neurodegenerative disorders the primary problem is thought to be intrinsic. The “sundowning” phenomenon often seen in patients with dementia is related to this phenomenon.
Alzheimer disease and sleep. In patients with Alzheimer disease, sleep abnormalities may appear early in the disease process and may be a prominent feature. In dementia in general, reported abnormalities have included low sleep efficiency, high percentage of stage N1 sleep relative to other stages, decrease in slow wave sleep (stage N3 sleep), and increased frequency of arousals and awakenings (23). Moderate to severe Alzheimer disease patients were found to have less slow wave sleep, higher stage N1 sleep, and a lower number of spindles during NREM sleep as compared to age-matched controls with insomnia (154). Early in the disease course, circadian sleep-wake cycles are disturbed, and there is an increase in nighttime wakefulness, which worsens with disease progression. A number of distinct circadian rhythm abnormalities have been identified, and disturbances in the rest-rhythm activity have been identified (173; 107). In addition, a number of studies have shown that melatonin levels may be abnormal in patients with Alzheimer disease, suggesting a possible link with circadian rhythm and diurnal variation (162; 104). Later in the disease, REM sleep time is decreased, and there is increased REM sleep latency, which, along with abnormalities of the circadian rhythm, results in excessive daytime sleepiness. Further decreases in REM sleep have been noted in patients with Alzheimer disease who have sleep-disordered breathing (47). Sundowning and other disturbances of the sleep-wake cycle are common in Alzheimer disease, and may be influenced and exacerbated by a number of factors, including an unfamiliar environment, medications, and infection (71). Irregular sleep-wake rhythm disorder becomes more common as the degenerative disorder progresses. Irregular sleep-wake rhythm disorder is a circadian rhythm disorder where no major sleep period (typically less than 4 hours) is noted throughout a 24-hour period (per actigraphy or sleep logs), resulting in variable and disorganized sleep episodes (at least three sleep bouts) throughout the 24-hour cycle (07). One case series suggested higher rates of REM sleep without atonia in patients with Alzheimer disease, though not as high as in those with Parkinson disease or other synucleinopathies (60).
Obstructive sleep apnea has also been linked to Alzheimer disease, though the data for this are derived from smaller studies that are not typically specific to Alzheimer disease, and involve other types of dementia and cerebrovascular disease (11; 10). Some smaller studies have even suggested that there may not be a clear statistical difference between Alzheimer disease and controls in sleep disordered breathing (25). It should be noted that this is a disorder seen in a greater percentage of patients over 65 years than in the general population, though it is also influenced by risk factors similar to those seen in younger patients (12; 09). In a prospective study of 128 patients with mild to moderate Alzheimer disease who underwent overnight polysomnography, 90.6% of them had an apnea-hypopnea index over 5, with 39% having severe obstructive sleep apnea (59). There is also growing evidence that obstructive sleep apnea may lead to earlier onset of Alzheimer disease or accelerate accumulation of abnormal proteins in the brain due to decreased clearance and removal (57). Animal studies also suggest that intermittent hypoxia could also be playing a role in beta-amyloid overproduction and tau hyperphosphorylation (108).
Parkinson disease and sleep. Parkinson disease has been among the most studied of the neurodegenerative disorders with respect to sleep disorders. Sleep abnormalities in Parkinson disease have been reported since the initial descriptions of the disease itself. A variety of well-described sleep symptoms and disturbances affect Parkinson patients. Complaints of insomnia, parasomnias, daytime sleepiness, and sleep onset and maintenance difficulties are common (22). Fatigue is also a prominent complaint, though is subjective and in some studies does not appear to clearly correlate with depression, disease severity, or duration of disease in Parkinson disease patients (02). Fatigue and sleep disorders do seem to correlate with quality of life of Parkinson patients (148). Sleep studies in Parkinson patients have revealed several distinct abnormalities. These include deficiencies in slow wave sleep, total sleep time, sleep latency, efficiency, and overall architecture (158), as well as a decrease in REM sleep (177). Sleep fragmentation, altered dream phenomena, and hallucinations appear to be common in Parkinson disease patients according to some studies (120). A community-based study suggested a significantly increased prevalence of sleep disorders in the Parkinson disease population compared with controls, with the most common complaints being sleep fragmentation and early morning awakening (153). Airway obstruction (sleep apnea) or restrictive pulmonary function is also common in Parkinson patients (96), however, thus far it has not been clearly demonstrated whether the prevalence of obstructive sleep apnea in Parkinson disease is significantly increased over that of controls (66; 14; 96; 54; 51; 160). Parkinson disease patients may suffer from more obstructive sleep apnea due to limited mobility at night (not being able to turn over in bed), resulting in more sleep in the supine position, which is when obstructive sleep apnea is most prevalent (44). Obstructive sleep apnea may worsen nonmotor symptoms of Parkinson disease such as psychotic symptoms and apathy (101). Similarly, restless legs syndrome and periodic leg movements are also common in Parkinson disease. Some studies have suggested increased prevalence compared to the general population, but other studies have not shown clear evidence of significant differences, and no clear prospective trials have to date been completed (152; 117; 113). Evidence suggests that the prevalence of REM sleep behavior disorder is increased in Parkinson disease, as is REM sleep without atonia (169; 118). In one large cohort, the overall frequency of REM sleep behavior disorder was 46% in Parkinson disease patients, with rates increasing with age and disease duration (145). It is important to distinguish between REM sleep behavior disorder and nightmares as the treatment can differ significantly. In addition, symptoms themselves may be correlated to medication effect. A case series described rare occurrences of adult-onset sleepwalking in patients with Parkinson disease (129), though another study asserts that Parkinson patients have a higher prevalence of other parasomnias such as nightmares, sleep terrors, sleepwalking, and enuresis (176). Circadian rhythm disturbances have been described in patients with Parkinson disease (164), including disruption of circadian markers such as cortisol and melatonin levels (30; 166). A cross-sectional study of over 150 Parkinson patients demonstrated that with progression of Parkinson symptoms, a phase advance in the circadian rhythm also occurred (114).
Finally, a variety of other factors common in Parkinson disease may have significant impact on sleep, including depression, pain, motor difficulties, autonomic abnormalities, nocturia, nightmares, and medication. The motor symptoms themselves likely play a significant role in causing sleep symptoms because when these motor symptoms are targeted with therapy at night, such as long-acting dopamine or rotigotine patch, sleep is improved (163). Impaired ability to move in bed has been shown to affect sleep quality in Parkinson disease patients (175). Excessive daytime sleepiness is a commonly described problem in Parkinson disease, and can result in significant adverse effects on daily life, social interactions, and work performance. A number of studies have shown that medication side effects (particularly of dopamine agonists and L-dopa) can result in increased daytime sleepiness, though large population studies have also demonstrated increased daytime sleepiness in Parkinson disease patients irrespective of medications (158) or prior to treatment for Parkinson disease (157). Central hypersomnia has also been described in patients with Parkinson disease, including a narcolepsy phenotype due to neurologic disease, with low hypocretin levels measured in the cerebrospinal fluid (170). A cross-sectional observational study demonstrated that Parkinson patients that are DQB1*0602 positive, which is an HLA risk allele for narcolepsy, are three times more likely to experience excessive daytime sleepiness, further supporting the presence of a narcolepsy-like disorder in this population (03). Regardless of the exact etiology, these symptoms must be taken seriously if adverse effects such as motor vehicle accidents are to be avoided. Circadian rhythm disturbances have also been described in patients with Parkinson disease (164), including disruption of circadian markers such as cortisol and melatonin levels (30; 166).
Sleep in other cerebral degenerative conditions. Patients with progressive supranuclear palsy have a high prevalence of comorbid sleep disorders. Initially, the most common problem is insomnia. Some studies have found that as the disease progresses, sleep latency shortens and insomnia becomes more severe due to associated increased sleep fragmentation (05). Polysomnographic findings also include increased sleep fragmentation and increased stage N1 sleep along with reductions in sleep time, REM sleep, stage N3 sleep, sleep spindles, and K complexes (126; 28). Other problems associated with progressive supranuclear palsy, such as immobility and dysphagia, contribute to interrupted sleep patterns. Notably, it has been suggested that REM sleep behavior disorder and respiratory disturbances are not as pronounced in progressive supranuclear palsy when compared with Parkinson disease and other synucleinopathies. However, some research suggests that REM sleep without atonia and REM-sleep behavior disorder may in fact be as common in progressive supranuclear palsy as in Parkinson disease (15; 144).
Corticobasal degeneration is a less commonly diagnosed entity, and to date, extensive studies on sleep disturbances are limited. Case reports have described patients with REM sleep behavior disorder (79), periodic limb movement disorder, REM sleep without atonia (168), and insomnia (134).
When reviewing sleep complaints in patients with neurodegenerative disorders, it is also important to consider the changes in sleep architecture associated with normal aging. These include (but are not limited to) sleep fragmentation, reduced sleep efficiency, decreased sleep quality, and reduction on the amount and amplitude of slow wave sleep, along with other predictable changes (18). These changes often complement the more pronounced difficulties seen in patients with neurodegenerative disorders.
In general, the cerebral degenerative diseases described above are progressive disorders that tend to worsen with time. Sleep disorders in these patients are linked to the underlying disease process. Thus, as the disease itself worsens, the sleep disorders also tend to progress. There is growing evidence that poor sleep can alter abnormal protein production and clearance in the brain, contributing to acceleration and progression of the underlying neurodegenerative condition (35).
A 78-year-old man with diagnosed Parkinson disease presented to his physician’s office with his wife. He described that his motor symptoms were under good control, but for the last year he had been having increasing sleepiness during the day, forcing him to take naps regularly. He had initially thought that this might be a side effect of his medications, but after several trials of different medications and doses, he did not notice any relief. When his wife was asked about her husband’s sleep, she remarked that she noticed that he had been talking significantly more in his sleep, and more recently had begun to act out his dreams on a regular basis. On a few occasions he had even struck her while apparently trying to fight during his dream. She noticed that he had displayed some of these symptoms a few years before he was diagnosed with Parkinson disease. A baseline polysomnogram was performed and revealed abnormal augmentation of his limb and chin EMG tone during REM sleep, suggesting that the patient’s symptoms were most likely due to REM sleep behavior disorder, a problem commonly associated with Parkinson disease.
A trial of clonazepam therapy at 0.25 mg prior to bedtime was initiated and helped to control his symptoms, though he continued to describe daytime sleepiness. Notably, his polysomnogram had not shown evidence of obstructive sleep apnea, which can be worsened by benzodiazepine therapy. His neurologist suggested that if this continued to be a problem, melatonin could be tried as a possible alternative.
The etiology of sleep disorders in cerebral degenerative disorders is thought to be secondary to the underlying disease processes. Abnormalities, particularly in the brainstem and hypothalamus, caused by cell death and protein deposition as well as other processes play a major role in disruption of normal sleep cycles. In idiopathic REM sleep behavior disorder, loss of dorsal lateral nigral hyperintensities typically only seen in patients with Parkinson disease are noted on MRI even though no motor symptoms have developed yet in these patients (50). It should also be noted that other factors can have a significant effect on sleep in these patients, including medication side effect, normal changes in sleep architecture with age, comorbid psychiatric abnormalities, social stressors, and even sleep disorders unrelated to the primary cerebral degenerative disorder.
Neurodegenerative diseases are often divided into two categories: the synucleinopathies and the tauopathies. These names derive from the abnormalities in underlying molecular mechanisms. In the tauopathies (including Alzheimer disease, progressive supranuclear palsy, Pick disease, and corticobasal degeneration) abnormal structure or phosphorylation of microtubule-associated proteins leads to both intra- and extracellular protein deposition. The synucleinopathies (Parkinson disease, diffuse Lewy body dementia, multiple system atrophy, striatonigral degeneration, and olivopontocerebellar atrophy) result from abnormalities of the protein alpha-synuclein, which accumulates abnormally in neurons and glia, as well as extracellularly. Abnormalities in related proteins ubiquitin and parkin are also important in the synucleinopathies.
In the cerebral degenerative disorders there can be direct effects on regions of the brain involved in sleep regulation, which contribute to the clinical symptoms and findings in workup. Effects of disease on the normal sleep-wake regulating centers of the brain are common. In particular, involvement of the brainstem and the hypothalamus has major effects. For example, animal studies have suggested a relationship between insomnia and the ventrolateral (hypothalamic) preoptic nucleus (90; 62). Damage to the lower brainstem hypnogenic neurons near the nucleus tractus solitarius can also result in difficulties in sleep initiation. Hypersomnolence can result from almost any lesion that affects the reticular activating system (including the pons, midbrain, thalamus, hypothalamus, and forebrain), with the dorsolateral hypothalamic nucleus playing a key role.
Additionally, other factors not directly related to underlying neurodegenerative disease may significantly influence sleep in this group of patients. These include such items as other medical conditions (pain, psychiatric disorders, etc.), medication side effects, physical discomfort related to the disease, the social environment, and sleep abnormalities related to aging. These must also be taken into account as contributing factors.
In Alzheimer disease, the main pathologic findings are diffuse neurofibrillary tangles and beta-peptide protein deposits. Disruption of the circadian sleep-wake cycle is a prominent feature, and some studies have suggested that the overall amplitude of melatonin and the rhythm itself may be decreased in Alzheimer disease, though exact mechanisms have not yet been elucidated (95). Also implicated has been the suprachiasmatic nucleus of the hypothalamus, which has been shown in postmortem studies to suffer cell loss compared to normal controls (24). In addition, decreased REM sleep in Alzheimer disease may be due to loss of cholinergic neurons, particularly in areas such as the nucleus basalis of Meynert or the pedunculopontine tegmental and laterodorsal tegmental nuclei. Emerging new research has highlighted an association between sleep disruption or deprivation and amyloid-beta levels in normal controls, suggesting sleep disruption as an accelerating factor in the progression to Alzheimer disease (146). Cerebrospinal fluid amyloid-beta levels were noted to be increased in insomnia patients as compared to controls (39) and in patients who were sleep deprived (91), suggesting that chronic sleep disruptions may have an effect on amyloid-beta metabolism in the brain. Early disruption in sleep may later forecast the longitudinal trajectory of cortical beta-amyloid deposition as measured with PET imaging in the human brain (172). A cross-sectional study further demonstrated that long and short sleep duration was associated with increased amyloid-beta burden as measured by PET (171). Another group found that self-reported poor sleep efficiency and sleep duration in cognitively unimpaired older adults were associated with faster accumulation of beta-amyloid in the brain as measured by PET (128). Sleep length, both short and long duration, has been found to be associated with early Alzheimer disease and mild cognitive impairment in one longitudinal study in 100 patients (93). This same type of hypothesis has been suggested for sleep disruption from sleep apnea and subsequent progression to Parkinson disease (40), as well as Alzheimer disease (52). One large cohort study demonstrated that patients with sleep-disordered breathing were 1.58 times more likely to develop Alzheimer disease after adjusting for the possible confounding variables (85). There is also evidence to suggest that the chronic intermittent hypoxia from obstructive sleep apnea may also be playing a role in cognitive deficits in dementia patients (86). Two meta-analyses and reviews demonstrated sleep disruption (subjective reports) as a risk factor for development of Alzheimer dementia (32; 140). One potential mechanism explaining the role of disrupted sleep in development of dementia includes evidence of abnormal sleep-dependent glymphatic clearance of metabolic waste products from the brain, possibly during slow wave sleep. A study in mild to moderate Alzheimer disease patients that were studied with polysomnography and cerebrospinal fluid samples demonstrated lack of deep sleep was associated with higher levels of NF-L, a marker of axonal damage in neurodegenerative conditions (155). Other researchers looked at a large prospective cohort and demonstrated that a loss of slow wave sleep percentage as measured on polysomnography was associated with a greater risk of incident dementia (68). A cross-sectional study looking at cognitively normal insomniacs demonstrated that insomnia symptoms were associated with higher cerebrospinal fluid beta-amyloid levels, further suggesting that sleep disruption may cause increased amyloid production (112). Interestingly, attempts to increase slow wave sleep with use of sodium oxybate did not result in decreasing cerebrospinal fluid amyloid levels more than in normal sleep (91). Another mechanism suggests that sleep and circadian disruption contribute to cognitive decline by activating neuroendocrine and neuroinflammatory signaling pathways that suppress hippocampal neurogenesis (78). Other emerging data suggest a different pathogenesis demonstrating an increase in cerebrospinal fluid orexin in patients with Alzheimer disease, resulting in sleep dysregulation along with deterioration and worsened cognition (87). However, a metaanalysis evaluating cerebrospinal fluid levels of orexin did not find a difference in Alzheimer disease patients versus controls; therefore, more research on the role of orexin in the pathophysiology of Alzheimer disease is necessary to better understand this possible mechanism (159). A randomized, placebo-controlled study had 38 cognitively impaired individuals take suvorexant (a dual orexin receptor antagonist) and demonstrated that suvorexant acutely decreased tau phosphorylation and amyloid-beta concentrations as measured by cerebrospinal fluid (92).
In progressive supranuclear palsy brainstem lesions are the major contributing factor. There have been suggestions that locus ceruleus or pontomesencephalic nuclei may be involved. In addition, degeneration of nigrostriatal neurons may result in deafferentation of frontal lobes from the striatum (71).
Corticobasal degeneration is characterized clinically by corticospinal tract and extrapyramidal features, tremors, apraxia, myoclonus, dystonia, cognitive dysfunction, and prominent cortical and basal ganglia atrophy. It is one of the lesser studied of the neurodegenerative disorders with respect to sleep, however, REM sleep behavior disorder has been described in several reports (168). Midbrain and pontine structures have been shown to be affected in this disease, and it is postulated that such involvement may account for the sleep disorders (79). Gliosis seen in corticobasal degeneration, particularly in frontal and parietal areas and subcortical regions, may have effects similar to those noted in progressive supranuclear palsy (22).
In Parkinson disease, involvement of the pedunculopontine nucleus, locus ceruleus, pontine ceruleus alpha nucleus, and raphe nuclei are implicated in disorders of REM sleep and slow wave sleep, and have been directly localized in some animal studies (151). The pedunculotegmental nucleus involved pathways mediating both locomotion and REM sleep, and loss of cholinergic neurons, may be the underlying etiology of disorder in this area (158). Fatigue, a common symptom in Parkinson disease patients, may be due to reduced serotonergic function in the basal ganglia and limbic structures as observed in PET studies of patients with Parkinson disease (125). Decreases in melatonin production and hypothalamic neuron loss have been noted in patients with Parkinson disease, likely contributing to circadian rhythm dysfunction (29). Similarly, diffuse Lewy Body disease, characterized by dementia, extrapyramidal symptoms, and psychosis (visual hallucinations are classic) shows the effects of Lewy body deposition and neuronal degeneration in the substantia nigra, locus ceruleus, and raphe nuclei (22).
The prevalence of sleep disorders among patients with cerebral degenerative disorders varies based on disease but is likely underreported in general. Overall estimates have put prevalence at 40% to 80%. The numbers vary from disease to disease. For instance, sleep disorders are seen in 74% to 98% of idiopathic Parkinson disease patients, and sleep apnea is estimated in 33% to 53% of patients with probable Alzheimer disease (22). A systematic review of the literature found that patients with Lewy Body dementia had higher sleep disturbance symptoms as compared to Alzheimer disease (49% of patients as compared to 24%, respectively) (80). There is also research suggesting that poor sleep caused by sleep apnea may play a more significant role in worsening cognitive function and decline in black patients as compared to white patients. The fact that numerous studies have demonstrated that sleep disorders go more undiagnosed and recognized in black populations suggests this may be playing a role in magnifying health disparities in this population when it comes to dementia and sleep (41).
As curative treatments for most of the underlying cerebral degenerative disorders have yet to be discovered, primary prevention of the associated sleep disorders is difficult due to the intrinsic pathology. However, treatment of sleep disorders themselves is extremely important with respect to prevention of other comorbidities and possibly for slowing down progression or onset. For example, treatment of sleep apnea is essential as it has been associated with increased risk of cardiovascular disease, hypoxia during sleep, cerebral vascular disease, and impaired glucose tolerance. Ensuring that patients are getting adequate amounts of sleep for their age may also help with prevention or reducing the risk of future neurodegenerative conditions.
The differential diagnosis is broad for patients presenting with sleep complaints such as insomnia or excessive daytime sleepiness. Apart from primary disease as a direct causative mechanism, other primary sleep disorders must be considered. In the elderly, a number of sleep disorders are possible, including sleep apnea, restless legs syndrome, periodic limb movement disorder of sleep, insomnia (due to a variety of mechanisms), circadian rhythm abnormalities, and parasomnias, among others (18). In addition, other factors may contribute to sleep disturbances, including comorbid medical conditions, medication effects, psychiatric disorders, and other primary neurologic disorders.
|
• A detailed history and physical examination, including receiving a history from family or a close contact, is an important step in identifying possible etiologies of the patients’ sleep complaints. |
Perhaps most important in the initial evaluation of sleep disorders in patients with neurocognitive deficits is a detailed history and physical exam. Often it is necessary to interview several family members or others who have close contact with the patient as he or she may not be able to provide adequate history. One study demonstrated a discrepancy between subjective and objective sleep reports in patients with early to moderate stage Alzheimer disease, suggesting usefulness of actigraphy in addition to sleep logs in this patient population (106). Close attention should be paid to sleep history as well as to neurologic and medical problems that could affect sleep (including pain), and a careful psychiatric evaluation is essential as this is often comorbid in neurocognitive disorders. A thorough inspection of medications and timing of doses is important.
Polysomnography with video monitoring is generally the most informative test to consider when pursuing a diagnosis of a sleep disorder. This can help to delineate abnormalities of sleep architecture and severity of pathology, including parasomnias, respiratory disturbances (including obstructive sleep apnea), and abnormal motor activity. Polysomnography can help distinguish obstructive from central sleep apnea. It can also be used when evaluating for nocturnal stridor, which can be seen in patients with multiple system atrophy. Multiple system atrophy patients with stridor not only have a higher apnea-hypopnea index (AHI) as compared to patients without stridor, but they have also been found to have more “sighs” noted during polysomnography in both wake and sleep (122; 136). One study of 35 patients with dementia with Lewy bodies who underwent polysomnography found occipital slowing on awake electroencephalography in 34% of patients, absence of sleep spindles and K complexes in 12.9%, slow frequency sleep spindles in 12.9%, and delta activity in REM sleep in 19.2% (58). Increased EMG tone in the chin and limbs during REM sleep can be helpful in the diagnosis of REM sleep behavior disorder in patients who have a history of dream enactment behavior. Increased tonic chin EMG activity during REM sleep was found to predict future development of Parkinson disease in patients with idiopathic REM sleep behavior disorder as compared to patients who had solely increased phasic chin EMG activity during REM sleep (131). Multiple sleep latency testing can provide useful information about daytime sleepiness, hypersomnolence, and narcolepsy. Actigraphy is another useful means of gathering information by measuring limb movements while both asleep and awake, though it provides less detail into sleep architecture than does polysomnography or multiple sleep latency testing and is not as well studied (147). One study suggests that using a combination of questionnaires along with actigraphy can be helpful in diagnosing REM sleep behavior disorder with good specificity, but not sensitivity (88). One other study validated the use of the Mayo Sleep Questionnaire as having adequate sensitivity and specificity in the diagnosis of REM sleep behavior disorder among the elderly (26). One study reported that patients with multiple system atrophy not only had high muscle tone during REM sleep but had diffuse muscle overactivity in the axial and limb muscles during NREM sleep as compared to patients with Parkinson disease (143). The use of home sleep apnea testing in cerebral degenerative disorders is limited and there are concerns that patients with cognitive or motor symptoms may not be able to properly place sensors for testing. In addition, home sleep apnea testing does not evaluate for REM sleep without atonia, parasomnias, and other motor activities commonly seen in this population. Home sleep apnea testing in one small study of Parkinson disease patients led to high failure rate and other difficulties such as underestimation of the degree of sleep-disordered breathing (63).
Further testing options should be based on the clinical scenario. Pulmonary function testing, along with arterial blood gas, may be useful for assessing baseline respiratory disease and abnormalities in acid-base balance, which can contribute to sleep disorders or be a manifestation of them. Polysomnography with transcutaneous carbon dioxide monitoring can uncover underlying sleep-related hypoventilation, which may be present in patients with multiple system atrophy (149; 109). Polysomnography includes partial EEG monitoring, but if nocturnal seizures are suspected, then formal EEG monitoring can be helpful. EMG testing can identify neuromuscular disorders often associated with cerebral degenerative disorders.
Many of the cerebral degenerative disorders do not yet have definitive cures or treatments, but when available, treatment of the underlying disease and symptoms can have a beneficial effect on sleep symptoms and quality of sleep. One study demonstrated that identifying and treating sleep disorders in the population may also be a priority to improve caregiver burden, as poor sleep predicted caregiver well-being more than motor symptoms of Parkinson disease (20). Treatments commonly used to reduce motor symptoms of Parkinson disease seem to also assist in consolidating sleep and improving alertness. This has been noted with Parkinson disease medications such as pramipexole (174), rotigotine (127), rasagiline (119), levodopa/carbidopa/entacapone (121), as well as with deep brain stimulation (21). In addition, attention to and management of other factors that can contribute to sleep disturbances is necessary. For example, maintaining regular sleep-wake schedules and avoiding prescription and over-the-counter medications that may affect sleep are important (08). Exercise (high-intensity) has been show to improve sleep efficiency (based upon polysomnography) and sleep quality in Parkinson patients (06). Specific treatment of sleep disorders should be tailored to the sleep disorder diagnosis. Keep in mind also that many sleep disorders are multifactorial in nature, and many are associated with older age in general. For all patients with dementia, adherence to proper sleep hygiene, such as maintaining a regular sleep wake schedule, are recommended.
Disorders involving excessive motor activity during sleep, including restless legs syndrome and periodic limb movements of sleep, can be treated with commonly available medications. Alpha-2 delta ligands, such as gabapentin or pregabalin, are common first-line medications for restless legs syndrome or periodic limb movement disorder (142). Dopaminergic medications, including levodopa, pramipexole, pergolide, and ropinirole are alternate treatment options but have lost favor for being first-line options due to risks of augmentation. Evaluating iron status and supplementing iron may also improve restless legs syndrome.
Insomnia is a manifestation best approached by addressing the possible underlying triggers. Various measures to improve sleep hygiene may be attempted, including avoidance of stimulants such as caffeine and nicotine, exposure to light during the day and synchronization of circadian rhythms, avoiding heavy meals and fluids prior to bedtime, exercising regularly, avoiding temperature extremes, and using the bedroom only for sleeping purposes (17; 111). Pharmacologic therapy, particularly sedative hypnotics, may be used judiciously as they may have significant adverse side effects in the elderly and particularly in patients with significant cerebral degenerative disorders. These include such medications as zolpidem, zaleplon, eszopiclone, ramelteon, and triazolam, among others. The main concerning side effects common to these hypnotics include cognitive dysfunction and increased risk of falls. Few hypnotics have been specifically tested in this population. Prolonged-release melatonin (2 mg) was shown to improve sleep quality in a randomized, double-blind, placebo-controlled, multi-center trial of Parkinson patients (04). Prolonged release melatonin helped improve sleep maintenance and cognitive functioning in mild to moderate Alzheimer disease patients in one randomized, placebo-controlled, multicenter study (167). A systematic review and metaanalysis also asserted effectiveness and safety of melatonin administration in Alzheimer patients with insomnia (150). Evidence-based review guidelines by the American Academy of Sleep Medicine suggest clinicians not use melatonin as treatment for insomnia, based upon doses of 2 mg of melatonin (137). One randomized, placebo-controlled trial studied eszopiclone in 30 patients with Parkinson disease and insomnia. Eszopiclone did not significantly increase sleep time but did subjectively improve quality of sleep and was reasonably tolerated as compared to placebo (103). One randomized, triple-blinded control study used eszopiclone and zolpidem in patients with Alzheimer disease and demonstrated that they can be effective in clinically improving sleep in the short term, but it raised concerns about safety and tolerance in their subjects (89). Eszopiclone in a recent randomized control trial in Alzheimer patients demonstrated improvements in quality of sleep and cognitive function as compared to the control group (73). Doxepin has also been shown to be effective in improving insomnia symptoms in one small, randomized trial in Parkinson disease patients (133). Trazodone, melatonin, and clonazepam were studied in Parkinson patients in a double-blind, randomized trial, demonstrating that all three improved sleep quality with minimal adverse events (64). A Cochrane database review suggested lack of evidence to help guide treatment for sleep problems in dementia, particularly with benzodiazepines and nonbenzodiazepine hypnotics. There was some evidence to support the use of trazodone (low dose of 50 mg) and no evidence that melatonin (up to 10 mg) helped sleep (99). Low dose (50 mg) of trazodone improved sleep in one randomized, placebo-controlled study of 30 dementia patients (33). A randomized, double-blind, placebo-controlled 4-week trial in mild to moderate Alzheimer disease patients demonstrated an improvement in total sleep time with use of suvorexant, a dual orexin receptor antagonist (67). There are further trials looking into dual orexin receptor antagonists as a class of drugs for use in this population. There was also a phase 2 trial looking at the safety and efficacy of lemborexant in Alzheimer disease patients with irregular sleep-wake phase disorder (a circadian rhythm disorder), showing improvements in sleep continuity with no serious adverse events (105). There is growing interest in the use of this class of medications, the dual orexin receptor antagonists, due to improved safety as compared to other hypnotics as well as data suggesting that the orexin system may be playing a role in the underlying neurodegenerative process in dementia (93).
Nonpharmacologic interventions, including stimulus control therapy, sleep restriction therapy, psychotherapy, and cognitive behavioral therapy for insomnia, should be considered first-line and have been shown to be effective in improving sleep efficiency and decreasing awakenings at night (72). Given barriers such as access and expense, pilot studies have shown improvement in insomnia in Parkinson disease patients using computerized cognitive behavioral therapy (123).
Table 1 provides additional suggestions for the treatment of insomnia in patients with dementia.
|
• Cognitive-behavioral therapy for insomnia may be somewhat more limited in those with cognitive impairment and might increase caregiver burden. | ||
|
• Circadian cues (34; 83) | ||
|
- Light: bright-light therapy used in the delay portion (ie, the evening, 7:00 PM to 9:00 PM) may help normalize circadian rhythms in patients with advanced sleep phase syndrome* | ||
|
- Physical activity: 3 to 6 hours before bedtime | ||
|
• Hypnotics (84) | ||
|
- Short-acting nonbenzodiazepine agents: eszopiclone, zaleplon, zolpidem | ||
|
- Suvorexant (67) | ||
|
- Trazadone 50 mg | ||
|
• Melatonin agonists | ||
|
- Ramelteon | ||
|
| ||
Treatment of excessive daytime sleepiness likewise centers on treatment of the factors causing disruption of nocturnal sleep or poor overall quality of sleep. A variety of factors may be implicated, including sleep disordered breathing, pain, and medication effect, among others. As mentioned previously, dopamine agonists in Parkinson disease can be problematic in this respect. Comorbidities such as other medical and psychiatric issues should also be explored and treated. Sleep disordered breathing, including obstructive sleep apnea, is one of the most commonly encountered problems. Treatment for obstructive sleep apnea includes nasal continuous positive airway pressure (primary), bi-level positive airway pressure, weight loss, and avoidance of exacerbating factors such as medications and alcohol. Mandibular advancing oral appliances can also be used for obstructive sleep apnea, though use in patients with neurodegenerative conditions is limited. One small study found that oral appliances can be effective and tolerated in Parkinson disease patients with sleep apnea (36). Continuous positive airway pressure has been shown in some small studies to reduce subjective daytime sleepiness in Alzheimer disease (42). One randomized placebo-controlled trial demonstrated decreased arousals and more stage 3 sleep with use of CPAP as compared to placebo CPAP (45). Another randomized, placebo-controlled crossover study of Parkinson patients showed improvements in sleep architecture and objective measures in sleepiness when treated with CPAP (110). Trials with CPAP have shown benefits of slowing cognitive decline (46; 161) and improving cognition (13) in patients with Alzheimer disease who suffer from sleep apnea. A retrospective review of multiple system atrophy patients demonstrated that the use of CPAP for sleep apnea improved quality of life of both patients and their caregivers (38). It should be noted that in patients with severe neurodegenerative disorders, particularly dementia, compliance with continuous positive airway pressure may be more difficult. However, there are data published indicating that compliance rate may not be much different in patients with mild cognitive impairment than the general population (31). In patients with multiple system atrophy, one retrospective study demonstrated that over 66% discontinued CPAP after a year (141), with over 75% of Parkinson disease patients dropping out in another study due to issues with CPAP tolerance (156). In patients with more severe respiratory compromise, particularly in those patients with neuromuscular weakness, nocturnal ventilatory support and tracheostomy may be required. One study demonstrated improvements in both sleep apnea and hypoventilation with adaptive servoventilation in patients with multiple system atrophy (65). In those patients with persistent sleepiness, a trial of stimulant medications may be considered with modafinil, armodafinil, or methylphenidate. A published clinical practice guideline from the American Academy of Sleep Medicine on the treatment of central disorders of hypersomnolence gave a conditional recommendation for use of armodafinil for the treatment of hypersomnia secondary to dementia with Lewy bodies, and a conditional recommendation for the use of modafinil or sodium oxybate for the treatment of hypersomnia secondary to Parkinson disease (97).
In those patients exhibiting parasomnias, an important initial part of management is ensuring safety for the patient and any bed partners. The most commonly encountered parasomnia in patients with cerebral degenerative disorders is REM sleep behavior disorder, which is treated primarily with clonazepam. Although no large randomized trials have been performed yet to evaluate medical therapy, clonazepam has been shown to have beneficial effect in several smaller studies (139; 116) and is generally accepted as first line treatment (70). The initial starting dose is generally 0.5 mg per night and may be increased up to 2 mg, or as tolerated. It should be noted that clonazepam can have other adverse side effects, including possibly contributing to a worsening of obstructive sleep apnea or worsening balance in patients already with ataxia. The most recent AASM Clinical Practice guideline gives a conditional recommendation for use of clonazepam, immediate release melatonin, and transdermal rivastigmine for REM sleep behavior disorder secondary to a neurodegenerative condition (70). Melatonin has been used as a possible therapeutic option in studies using doses of 3 to 12 mg and has more support in the literature than other substances with the exception of clonazepam (81; 82; 27). Data suggest that melatonin may have an advantage over clonazepam given that the latter is a respiratory depressant and has a long half-life, placing patients at increased risk of falls (100). Melatonin was less likely to lead to sedation and had less frequent adverse effects than clonazepam. According to a review, most patients responded positively to melatonin 6 mg with restoration of abnormal behavior, but treatment with a combination of melatonin and clonazepam may be needed for refractory patients (98).
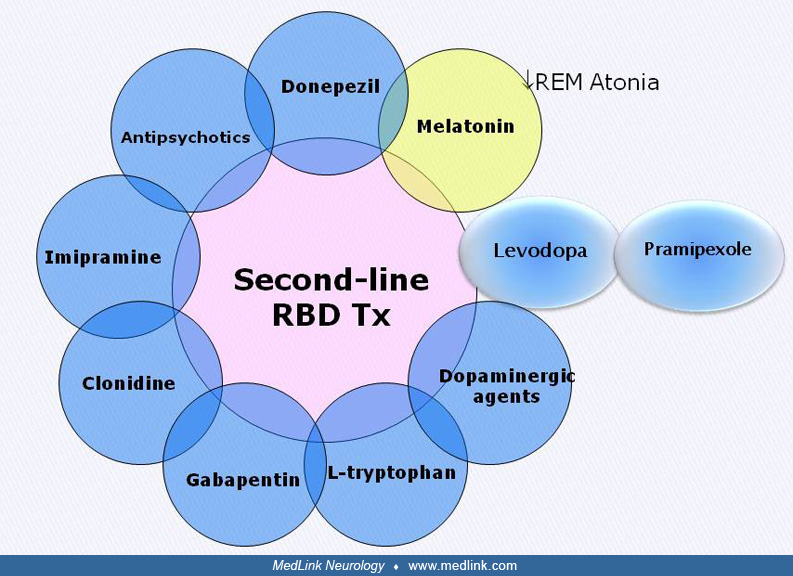
Ramelteon has also been studied in an open-label trial for REM sleep behavior disorder with positive results (77). Pramipexole and acetylcholinesterase inhibitors can be considered according to the guidelines, including a study on rivastigmine in refractory REM sleep behavior disorder (53). Only very limited data (case series) have shown effectiveness of desipramine, clozapine, and carbamazepine (16). In one small double-blind, placebo-controlled crossover study, 18 patients with Parkinson disease and REM sleep behavior disorder were given 5-hydroxytriphtophan (5-HTP), which is the intermediate metabolite of L-tryptophan in the production of melatonin and serotonin (102). This study demonstrated decreased self-report of dream enactment frequency along with improvement in motor symptoms during the day as rated by the Unified Parkinson Disease Rating Scale (UPDRS) part II (102). Use of cannabidiol (CBD) in a double-blind, placebo-controlled trial in 33 patients did not show reductions in REM sleep behavior disorder symptoms in Parkinson patients as compared to placebo (48). A customized bed alarm has been shown to have utility as an effective method to prevent sleep-related injury in REM sleep behavior disorder. This intervention is most suitable in cases of pharmacologically refractory REM sleep behavior disorder and for those patients who are unable to tolerate drug therapy (69).
Principal therapy for REM sleep behavior disorder is shown in Table 2, and the following diagram depicts second-line therapy.
|
• Formal neurologic exam (01; 56; 61) | |
|
• Level A: Safety intervention: removal of sharp objects from the bedroom, sleeping in a sleeping bag until the condition is managed, covering the windows, etc. (27) | |
|
• Avoid aggravating drugs: caffeine, selective serotonin reuptake inhibitors, monoamine oxidase inhibitors, tricyclic antidepressant | |
|
• Level B: Clonazepam nightly (approximately 90% effective) (27) | |
|
• Level B: Melatonin (doses between 3 and 12 mg nightly) (82; 27) | |
|
• Levodopa, dopamine agonists | |
|
• Anticonvulsants | |
|
• Pressurized bed alarm (69) |
Patients with circadian rhythm disorders may benefit from the use of light treatment or exogenous melatonin in an attempt to reset the intrinsic circadian clock. The combination of 5 mg of melatonin at bedtime and one hour of morning light exposure, but not each on its own, was found to improve daytime wakefulness and improve sleep disruption in a randomized controlled trial in patients with Alzheimer disease (55). A systematic review found improvement in agitation, sundowning, sleep quality, or daytime functioning in dementia patients with use of melatonin at night (49). Timed light therapy for one hour intervals twice daily for two weeks in Parkinson disease patients improved sleepiness as well as sleep quality in one randomized trial (165).
A variety of new treatments are becoming available that can significantly improve sleep symptoms or treat an underlying sleep disorder. This is important because in this patient population (just as in others), sleep disorders can have a severe and detrimental effect on daily function, including alertness, memory, and mentation. Treatment of sleep problems themselves is often possible and can result in a significant improvement in quality of life. Newer hypnotic agents targeting orexin (possibly only a single orexin receptor and not dual blocking) are being researched for better effectiveness and safety in this population. Other new options for treatment of sleep apnea have included hypoglossal nerve stimulation and even medical treatment options for obstructive sleep apnea such as a combination of aroxybutynin and atomoxetine, which is still awaiting approval from the FDA and is in trials phase (135).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Raman K Malhotra MD
Dr. Malhotra of Washington University School of Medicine in St. Louis has no relevant financial relationships to disclose.
See Profile
Alon Avidan MD MPH
Dr. Avidan of the University of California, Los Angeles, received consulting fees and honorariums from Harmony Bioscience for speaking engagements and review panel service, from Eisai for speaking engagements, and from Merck, Takeda Pharmaceuticals, and Idorsia as a consultant.
See Profile
Antonio Culebras MD FAAN FAHA FAASM
Dr. Culebras of SUNY Upstate Medical University at Syracuse has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Movement Disorders
Jan. 20, 2025
Sleep Disorders
Jan. 18, 2025
Movement Disorders
Dec. 29, 2024
Neurogenetic Disorders
Dec. 26, 2024
Neurogenetic Disorders
Dec. 23, 2024
Neurogenetic Disorders
Dec. 23, 2024
Neurogenetic Disorders
Dec. 13, 2024
Sleep Disorders
Dec. 03, 2024