Peripheral Neuropathies
Neuropathic pain: treatment
Jan. 19, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
SUNCT (short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing) is one of the rarest of all primary headache syndromes. It is one of the trigeminal autonomic cephalalgias, along with cluster headache and paroxysmal hemicrania. It is marked by frequent, short-lasting attacks of one-sided headache with associated cranial autonomic symptoms. SUNCT forms the majority subset of SUNA (short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms), in which the combination of conjunctival injection and tearing is not required for diagnosis. Reports and series have shown therapeutic benefits with medical treatments. Structural imaging studies report an association with aberrant vessels in contact with the trigeminal nerve in some patients, and functional imaging studies report hypothalamic activation. Microvascular decompression, occipital nerve stimulation, posterior hypothalamic region deep brain stimulation, and focal radiation therapy have all been reported to be effective in some medically intractable cases.
|
• SUNCT/SUNA are relatively rare but are very severe forms of primary headache syndromes belonging to the family of trigeminal autonomic cephalalgias. | |
|
• Functional neuroimaging studies in trigeminal autonomic cephalalgias, including SUNCT, report specific activation of the hypothalamus in association with the headaches. | |
|
• Structural imaging studies report that a significant proportion of patients have an aberrant vascular loop in contact with the ipsilateral trigeminal nerve, akin to the situation in trigeminal neuralgia. | |
|
• Transitional treatments include intravenous lidocaine, oral or intravenous corticosteroids, and greater occipital nerve blocks. | |
|
• Medical treatment options include lamotrigine, topiramate, gabapentin, pregabalin, duloxetine, and carbamazepine. | |
|
• In patients who are intractable to medical treatments, the surgical options include trigeminal microvascular decompression, occipital nerve stimulation, pulsed radiofrequency of the sphenopalatine ganglion, stereotactic radiosurgery, and posterior hypothalamic region deep brain stimulation. |
The syndrome of short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing, or SUNCT, was first described by Sjaastad and colleagues in 1978 (79). The syndrome was recognized in the revised International Classification of Headache Disorders (ICHD-II) in 2004 and modified in 2018 (35; 36).
|
3.3 Short-lasting unilateral neuralgiform headache attacks | |||
|
Description: Attacks of moderate or severe, strictly unilateral head pain lasting seconds to minutes, occurring at least once a day and usually associated with prominent lacrimation and redness of the ipsilateral eye. | |||
|
Diagnostic criteria: | |||
|
A. At least 20 attacks fulfilling criteria B to D | |||
|
B. Moderate or severe unilateral head pain, with orbital, supraorbital, temporal and/or other trigeminal distribution, lasting for 1 to 600 seconds and occurring as single stabs, series of stabs or in a sawtooth pattern | |||
|
C. At least one of the following cranial autonomic symptoms or signs, ipsilateral to the pain: | |||
|
1. conjunctival injection and/or lacrimation | |||
|
D. Attacks have a frequency of at least one a day for more than half of the time when the disorder is active | |||
|
E. Not better accounted for by another ICHD-3 diagnosis | |||
|
3.3.1 Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) | |||
|
Diagnostic criteria: | |||
|
A. Attacks fulfilling criteria for 3.3 short-lasting unilateral neuralgiform headache attacks | |||
|
B. Both of conjunctival injection and lacrimation (tearing). | |||
|
3.3.1.1 Episodic SUNCT | |||
|
Description: Attacks of SUNCT occurring in periods lasting from 7 days to 1 year, separated by pain-free periods lasting 1 month or more. | |||
|
Diagnostic criteria: | |||
|
A. Attacks fulfilling criteria for 3.3.1 short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing and occurring in bouts | |||
|
B. At least two bouts lasting from 7 days to 1 year and separated by pain-free remission periods of >1 month. | |||
|
3.3.1.2 Chronic SUNCT | |||
|
Description: Attacks of SUNCT occurring for more than 1 year without remission, or with remission periods lasting less than 1 month. | |||
|
Diagnostic criteria: | |||
|
A. Attacks fulfilling criteria for 3.3.1 short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing, and criterion B below | |||
|
B. Occurring without a remission period, or with remissions lasting <1 month, for at least 1 year. | |||
|
3.3.2 Short lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA) | |||
|
Diagnostic criteria: | |||
|
A. Attacks fulfilling criteria for 3.3 short-lasting unilateral neuralgiform headache attacks, and criterion B below | |||
|
B. Only one or neither of conjunctival injection and lacrimation (tearing). | |||
|
3.3.2.1 Episodic SUNA | |||
|
|
Description: Attacks of SUNA occurring in periods lasting from 7 days to 1 year, separated by pain-free periods lasting at least 1 month. | ||
|
|
Diagnostic criteria: | ||
|
A. Attacks fulfilling criteria for 3.3.2 short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms and occurring in bouts | |||
|
B. B. At least two bouts lasting from 7 days to 1 year and separated by pain-free remission periods of >1 month. | |||
|
3.3.2.2 Chronic SUNA | |||
|
Description: Attacks of SUNA occurring for more than 1 year without remission, or with remission periods lasting less than 1 month. | |||
|
Diagnostic criteria: | |||
|
A. Attacks fulfilling criteria for 3.3.2 short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms, and criterion B below | |||
|
B. Occurring without a remission period, or with remissions lasting <1 month, for at least 1 year. | |||
SUNCT, one of the trigeminal autonomic cephalalgias along with cluster headache and paroxysmal hemicrania, is comprised of brief attacks of moderate-to-severe pain lasting 5 to 240 seconds, with associated autonomic disturbances of conjunctival injection, lacrimation, rhinorrhea or nasal congestion, ptosis, or eyelid edema. In SUNCT, there must be both conjunctival injection and lacrimation present; in SUNA, autonomic symptoms may include either conjunctival injection, lacrimation, or neither, but not both. The International Headache Society describes the site of pain as unilateral orbital, supraorbital, or temporal pain, although it is clear from a large series that the pain may be experienced anywhere in the head (16). There is an ongoing debate regarding whether the separation into SUNCT and SUNA is useful. They could be simple variants of the same disease (47; 62). Lambru and colleagues reported the clinical phenotype of 63 patients with SUNA and 70 patients with SUNCT (47). The clinical and demographic characteristics of patients with SUNA were similar to those of patients with SUNCT. Ptosis and rhinorrhea were predictors of SUNCT. The presence of spontaneous-only attacks was a predictor for SUNA. In conclusion, Lambru and colleagues and Zhang and colleagues observed no major clinical differences between SUNCT and SUNA (47; 91). SUNCT is characterized by more prominent cranial autonomic features and can be triggered. The authors, therefore, propose that the two disorders should be placed together in a single diagnostic category.
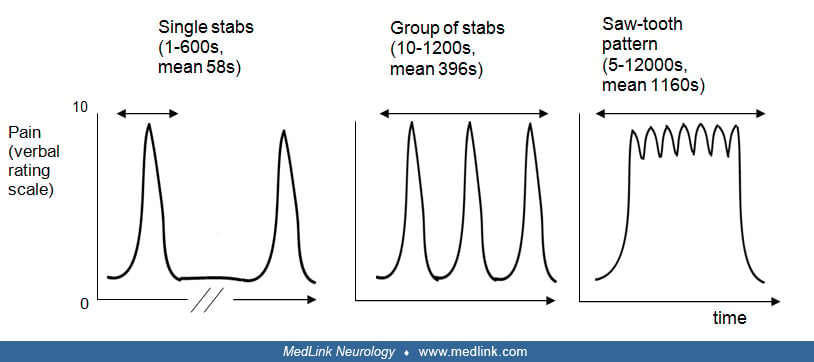
The pain is normally side-locked and remains unilateral throughout an entire attack. In rare instances, SUNCT pain can be bilateral or can affect alternate sides. Pain is described most often as a stabbing, burning, pricking, or electric shock-like sensation. Attacks may take on different characteristics: a single stab, which is usually short-lived with a mean duration of 60 seconds; a group of stabs; or a longer attack lasting many minutes to hours, comprised of many stabs between which the pain does not resolve to normal, thus, creating a “saw-tooth” effect (16; 10; 85).
There should be between 3 and 600 attacks per day, although these can occur as many single stabs within one group of stabs or one sawtooth attack. Furthermore, there is marked variation among patients in the frequency and duration of the attacks, thus, prompting the concept of “attack load,” measured in minutes of pain per day (16). The site of pain is predominantly in V1 in SUNCT and equally distributed between V1 and V2 in SUNA (45).
The differential diagnosis for these attacks includes paroxysmal hemicrania, cluster headache (especially in the long sawtooth attacks), and trigeminal neuralgia with cranial autonomic symptoms. Useful distinguishing aspects of the history include the short duration of attacks, triggerability from cutaneous stimuli, lack of refractory period between attacks, prominent autonomic symptoms, and agitation during attacks.
SUNCT can occur at any time of the day, and unlike cluster headache, it does not show a striking circadian rhythm; only 7% of SUNCT sufferers and no SUNA patients have nocturnal episodes, although in 40% of SUNCT patients, the attacks can occur during sleep or wakefulness (16). SUNCT can present in episodic form with bouts and remissions, usually without circannual periodicity (16), although there may be seasonal variations (40).
A clinical series of 24 patients reported that the episodic form (58%) predominates over the chronic form (42%) (87). However, the duration of the symptoms of most of the patients in this series was relatively short, and the natural progression of these syndromes points to a tendency to become chronic. Indeed, in a larger series of 52 patients with a longer follow-up, 63% of SUNCT and 89% of SUNA patients had a chronic form (16). This is in contrast to cluster headache, which is episodic in most patients.
Most SUNCT patients will be pain-free between attacks, although in a cohort of 52 patients with SUNCT/SUNA, 22 had interparoxysmal pain (16). Most patients in that cohort who had background pain also had a personal or family history, or both, of migraine.
Nausea, vomiting, photophobia, and phonophobia are not normally associated with SUNCT, although they can be present, especially in patients with a previous or family history of migraine (16). The photophobia and phonophobia are usually ipsilateral in SUNCT, as compared to bilateral in migraine (39).
Triggers. Important clinical characteristics of SUNCT include triggerability of attacks from cutaneous stimuli such as touching the face, chewing, talking, or cold wind on the face or other stimuli such as bright lights or neck movements, although the latter have also been shown to be able to ease the pain (12). These triggers are more prevalent in SUNCT (74% to 80%) than SUNA (22% to 50%) (16; 87; 47). Other important features include a lack of refractory period between attacks, although in three patients with a phenotype otherwise suggestive of SUNCT, a refractory period lasting between 1 and 10 minutes after triggered attacks was consistently observed (69). Up to 58% of patients are agitated by the attacks, which is a feature of trigeminal autonomic cephalalgias (16).
General and neurologic examinations are normal in SUNCT patients during and between attacks, except for the documented autonomic signs, which quickly abate when the attack ends. In a cohort of 52 patients, 30% of SUNCT and 11% of SUNA patients had abnormal examinations; generally, these were sensory abnormalities at the site of attacks, either reduction of sensation or hyperesthesia to pinprick (16). Allodynia and hyperalgesia are also seen in all trigeminal autonomic cephalalgias, especially in those with migrainous comorbidity.
The natural history of SUNCT syndrome is not clear because of its rarity. However, patients with SUNCT and SUNA have been known to have their condition for up to 46 years (16). The first ever reported case of SUNCT was followed up for 28 years until the patient’s death (77).
Although primary headaches are lifetime conditions, the natural history for cluster headache and migraine is thought to remit with age (06). However, 23% of a cohort of SUNCT patients had secondary chronic SUNCT that had transformed from episodic SUNCT. All the SUNA patients had primary chronic SUNA (attacks for at least a year without more than a month’s break) (16).
The syndrome itself is not fatal and does not cause any long-term neurologic sequelae, as most individuals have normal examinations between attacks. The exception to this is the group of secondary SUNCT/SUNA, who may be subject to the morbidity and mortality of the underlying disease.
The social and economic burden of SUNCT is unknown. Prognosis at the present time is improving as more treatment strategies become available.
A 67-year-old man presented with an 11-year history of an episodic disorder marked by multiple daily attacks of short-lasting pain. Each attack lasted about 30 seconds, and he experienced between 10 and 20 attacks per day. Each headache was stereotyped; there was right-sided pain periorbital and forehead pain, with some radiation into the nose. The pain was a severe stabbing shooting pain, rated by the patient as a 10 on a scale of 1 to 10 in severity. There was ipsilateral conjunctival injection, lacrimation, nasal blockage, and rhinorrhea, and occasionally some agitation was associated with the attacks. Each attack lasted 10 seconds, and he could have single attacks or groups of attacks lasting up to a few minutes. The attacks could be precipitated by touching the right eyebrow, washing the face, and brushing the teeth. Most of his attacks were triggered and occurred during the day, although a few spontaneous attacks could wake him from sleep at night. There was no refractory period between attacks and no interictal pain. A period of increased frequency of attacks could be precipitated by disruptions in his sleep pattern, particularly jet lag after international travel. There was no previous history, although there was a family history of migraine. General and neurologic examination was normal. An MRI scan of the brain was normal.
The patient had tried the following medications without success: oral indomethacin, sumatriptan, corticosteroids, verapamil, opiates, gabapentin, and carbamazepine. He had an intravenous infusion of lidocaine at 3 mg/kg/hour for 3 days, which rendered him pain-free but gave side effects of depression, so the infusion was stopped. He was started on lamotrigine 50 mg twice a day, which stopped the spontaneous attacks but not the triggered attacks. Topiramate 50 mg twice a day was added when his symptoms were more frequent due to travel, and this helped to reduce the frequency of the attacks.
Although SUNCT and SUNA are generally primary syndromes, they are proportionately more likely to be symptomatic to underlying pathology than the other trigeminal autonomic cephalalgias (52; 16; 25; 11). Secondary SUNCT and SUNA are typically seen with either posterior fossa or pituitary gland lesions (13), although local lesions can also cause these syndromes. In a cohort of 84 patients with pituitary tumors and headache problems, 10% had a trigeminal autonomic cephalalgia-like headache (52). Although these data need to be interpreted with caution, as this case series reported highly selected referrals to a tertiary referral neurosurgical service, it nonetheless highlights the possibility of an excess of pituitary disorders in SUNCT (14). Therefore, it is advised to perform an MRI of the brain in all patients with SUNCT or SUNA, given that the conditions are rare and life-long (77) and that the treatment of the pituitary pathology resolves the headache problem (59). Secondary SUNCT can also be caused by dorsolateral medullary infarction (42) and neurovascular compression (11).
Hypothalamic hypothesis. Given the prominence of cranial autonomic features in SUNCT and the PET findings of increased activity in the posterior hypothalamic region in cluster headache and paroxysmal hemicrania, activations in the same region in SUNCT in the first patient studied with fMRI seem broadly consistent (63). Five patients were studied with fMRI (four with left-sided attacks and one with bilateral attacks), and positive activation bilaterally in the region of the posterior hypothalamus was reported (19). Two patients with left-sided attacks had right-sided positive activation, and two patients with right-sided attacks had negative activation on the right side. In both patients with SUNA, there was negative activation bilaterally. There was no significant activation in this area in the patient with symptomatic SUNCT. The coexistence of SUNCT and hypnic headache also indicates a role for the hypothalamus (24). Clearly, the hypothalamic region plays a role in this condition, but much more work will be required to understand that role and how it may be exploited therapeutically.
Trigeminal neurovascular conflict. Because of the similarities between trigeminal neuralgia and SUNCT and the reported effectiveness of microvascular decompression in a few SUNCT patients with neurovascular conflict (29; 43; 81), some authors have studied these subjects, dedicating specific MRI views of the trigeminal nerves; they have found that 88% of subjects with SUNCT/SUNA have an aberrant arterial loop in contact or deforming the symptomatic trigeminal nerve (87). These findings raise the possibility of a key participation of peripheral mechanisms in the pathophysiology of SUNCT (41). An earlier series had reported that only 7% of patients had trigeminovascular loops, but patients were not investigated systematically with dedicated trigeminal scans in that series (16). A review identified neurovascular compression in 7% of patients (26). A case reported by Talavera and colleagues with SUNCT secondary to a cerebellopontine angle meningioma supports the hypothesis of trigeminal nerve involvement in the pathogenesis of SUNCT (82).
SUNCT and SUNA were thought to be extremely rare, with 50 cases of SUNCT published before 2003 (57). However, there have been additional case reports since then, as well as a large series of 43 patients with SUNCT and nine with SUNA published in 2006 (16), and a series of 17 patients with SUNCT and seven with SUNA published by an Australian group in 2008 (87). The Australian group estimated a prevalence of SUNCT/SUNA at 6.6 per 100,000 and a conservative annual incidence of 1.2 per 100,000 (87). An epidemiological study found two SUNCT-like syndromes in a population of 1838 (78). SUNCT affects men more than women with a male-to-female ratio of 2 to 1, although it seems that in SUNA, the male-to-female ratio is reversed (16). There is also one reported family with SUNCT (28).
The typical age of onset is between 40 and 70 years; the mean age of onset is 57 years (16). The youngest recorded patient had SUNCT at the age of 5 years (75), whereas the oldest is 88 years old (83). For SUNA, the youngest patient reported is age 11, and the oldest is age 58. Qaiser and colleagues reported 13 cases of SUNCT/SUNA in children and adolescents aged 3 to 18 years (73).
There are no identified risk factors and, thus, no known prevention for SUNCT syndrome.
SUNCT can coexist with migraine, with 50% of SUNCT patients having migrainous biology, which is higher than the 11% to 15% migraine prevalence in the general population (16). Among migraine subtypes, SUNCT and SUNA have been reported to coexist with hemiplegic migraine in a series of 10 patients (46). SUNCT has also been known to coexist with migraine and cluster headache (16) and also with trigeminal neuralgia. In some patients, the background interictal pain in SUNCT may be attributable to migrainous biology and an analgesic overuse syndrome. There is also a report of a family association of SUNCT (28).
As the attacks of SUNCT can vary in length from a few seconds for the single stab to many minutes or even hours for the groups of stabs or saw-tooth attacks, the differential diagnosis includes the other trigeminal autonomic cephalalgias, namely cluster headache and paroxysmal hemicrania. It is important to differentiate SUNCT from the other trigeminal autonomic cephalalgias, because they each have different treatment approaches. In cluster headache, attacks last 15 to 180 minutes, with a frequency of one every other day, up to eight per day. In paroxysmal hemicrania, the attacks are shorter (2 to 30 minutes) and more frequent (1 to 40 per day) (35). There is an interictal pain in 47% of SUNCT and 22% of SUNA patients, and in these cases, hemicrania continua, with its constant unilateral pain, enters the differential diagnosis as well. It is often useful to ask the patient to draw a diagram of their attack; a long attack may be mistaken for cluster headache or paroxysmal hemicrania until the “saw-tooth” element is recognized as SUNCT.
Therapeutic trials can also be useful in the diagnosis of SUNCT/SUNA. In contrast to paroxysmal hemicrania or hemicrania continua, there is no reproducible indomethacin effect in SUNCT/SUNA, and in contrast to cluster headache, there is no important effect of oxygen, sumatriptan, or verapamil (17).
SUNCT is often misdiagnosed as trigeminal neuralgia, especially first-division trigeminal neuralgia (05). Symptoms pointing to SUNCT/SUNA as opposed to trigeminal neuralgia include the prominent distribution of pain in the ophthalmic division of the trigeminal nerve, triggering of attacks from cutaneous stimuli, and a lack of a refractory period to these triggers (16).
Because SUNCT/SUNA can be secondary or symptomatic of underlying structural pathology, including pituitary, posterior fossa, or local lesions, it is mandatory that a brain MRI with pituitary views and blood tests for pituitary function be a minimal work-up for SUNCT/SUNA. The general and neurologic examination in SUNCT/SUNA is usually normal, but the increased incidence of trigeminal autonomic cephalalgia-like headaches in patients with pituitary tumors (52) and the growing case reports of symptomatic SUNCT/SUNA suggest that brain imaging should be performed, even if the attacks are typical and the examination is normal. Data report that a high percentage of subjects with these syndromes have neurovascular conflict with the trigeminal nerve (87). In view of the emerging evidence of long-lasting benefits after surgical decompression of the trigeminal nerve (Williams and Broadley 2010), the diagnostic work-up of SUNCT and SUNA should include dedicated MRI cuts of the trigeminal nerves.
In terms of therapeutic trials, SUNCT may be differentiated from cluster headache by the lack of response to oxygen and from paroxysmal hemicrania by the lack of response to indomethacin. Two studies showed a striking response of SUNCT and SUNA patients to intravenous lidocaine (18; 87).
Because the attacks are so short, attack therapy is not a useful concept in SUNCT/SUNA. One can use short-term prevention in the hospital with lidocaine, which arrests the problem, and long-term prevention to minimize disability out of the hospital.
Lidocaine. A trial of intravenous lidocaine in 11 patients reported some relief to total abolition of their symptoms, the longest pain-free period being 3 weeks in a patient with chronic SUNCT, 12 weeks pain-free in chronic SUNA, and 6 months pain-free in a patient with episodic SUNCT (15). Another clinical study reported excellent results with subcutaneous administration of lignocaine (87). The pain was abolished completely in 79% of patients without significant adverse events, except for a case of a provoked epileptic seizure in a subject with a history of epilepsy. A trial of intravenous or subcutaneous lidocaine is, thus, warranted for both diagnostic and therapeutic purposes. ECG monitoring is advised during the infusion. The following therapies for short-term prevention were not effective: sumatriptan 6 mg sc, oxygen, indomethacin 100 mg, DHE intravenous, and corticosteroids (85).
A number of drugs have shown efficacy in the prevention of SUNCT and SUNA. Due to the small number of patients, only one small placebo-controlled trial exists for topiramate versus placebo (85). Treatment is based on a trial-and-error approach (03). The largest open-label study thus far evaluated the treatment response in 161 patients with SUNCT and SUNA (50). Most patients responded to lamotrigine (56%), followed by oxcarbazepine (46%), duloxetine (30%), carbamazepine (26%), topiramate (25%), pregabalin, and gabapentin (10%). Mexiletine and lacosamide were effective in some patients but poorly tolerated. Intravenous lidocaine given for 7 to 10 days led to improvement in 90% of patients. Only 27% of patients responded to a greater occipital nerve block. No statistically significant differences in responders were observed between SUNCT and SUNA. The therapeutic similarities between SUNCT and SUNA support the hypothesis that these conditions are variants of the same disorder.
Lamotrigine. Lamotrigine given in an open-label manner at doses up to 300 mg daily was reported as highly efficacious (20; 33; 54; 10; 85). Lamotrigine had a moderate-to-good effect in 68% of SUNCT patients and 25% of SUNA patients in an open-label study (15). In an Australian series, the response to lamotrigine depended on the subtype of SUNCT. Lamotrigine was found to give an excellent response in episodic SUNCT but a poor response in those with chronic SUNCT (87). Lamotrigine has also been found to be effective in a case of SUNA (68). The range of doses found to be effective is 25 to 600 mg (17). Problems with lamotrigine include a skin reaction that may progress to Stevens-Johnson syndrome.
Topiramate. Topiramate has been reported to be effective at doses of up to 300 mg daily (56; 74; 58; 30; 85). Fifty-two percent of SUNCT patients had a good response to topiramate in an open-label study, although the response in SUNA was less clear (15). A placebo-controlled, double-blind crossover trial of topiramate 50 mg twice daily in five patients with SUNCT showed a good response in two patients, response to placebo in one patient, and no response at all from the other two patients (17). In another study, topiramate was moderately effective in one subject but ineffective in five others, although no information has been given about the dose used in the trial (87). Although small in numbers, the attack frequency, placebo-control, and reality of studies in rare conditions combine to suggest that topiramate can be described as an effective treatment of the disorder.
Patients with a previous history of renal stones, glaucoma, or depression and those who are underweight should not be offered topiramate as a first-choice agent to prevent development of known side effects.
Gabapentin. SUNCT has been shown to respond to gabapentin, with complete suppression of attacks in three of nine patients treated with 800 to 2700 mg daily (31; 37; 72), and was minimally effective in one patient with SUNA at an unknown dose (84). Interestingly, it was effective in 60% of SUNA patients but only 45% of SUNCT patients in an open-label trial (15). It is, therefore, suggested for use in SUNA, and as a second-line agent in SUNCT.
Carbamazepine and oxcarbazepine. Carbamazepine has been a mainstay of treatment in trigeminal neuralgia and has also been reported as having a good or partial effect in SUNCT at doses up to 900 mg per day (57), although not in all patients (15). There is a case of SUNCT responding to oxcarbazepine (21). One patient was reported who responded to a combination of oxcarbazepine (600 mg) and gabapentin (400 mg) (55).
Zonisamide. Zonisamide is an anticonvulsant drug reported to be beneficial in the prophylaxis of migraine and neuropathic pain (02; 66). Its mechanisms of action are very similar to that of topiramate (07). In common with the various other drugs reported to be effective in SUNCT, its mechanism of action includes blockade of voltage-dependent sodium channels. For this reason, it was tried in a SUNCT patient who did not tolerate carbamazepine with excellent results on a long-term follow-up (38).
Dihydroergotamine. Intravenous dihydroergotamine, which is frequently used in refractory migraine, is not effective in SUNCT or SUNA (16/24 patients) and can lead to dramatic worsening of the SUNCT/SUNA (48).
Galcanezumab. One case of SUNCT in a 67-year-old man refractory to treatment was reported who responded to the monoclonal antibody against calcitonin gene-related peptide, specifically galcanezumab (09).
Botulinum toxin A. A botulinum toxin A injected around the orbit was reported to be effective in a SUNCT patient refractory to oral treatments (89). Zhang and colleagues reported a case of a 12-year-old boy refractory to nine different medical treatments (92). The symptoms of SUNCT disappeared after the injection of 2.5 to 5 units of botulinum toxin A in the ipsilateral gum, temporal area, orbit, and cheek.
Combination of drugs. In keeping with our experience, significant benefits may be provided using a combination of drugs, as reported in a case of SUNCT treated with a combination of oxcarbazepine and gabapentin (55). One advantage of combination therapy may be a reduction of drug-related side effects because lower drug dosages are used.
Greater occipital nerve injections. Two patients with SUNCT and six patients with paroxysmal hemicrania have undergone lidocaine blockades of the greater occipital nerve with no benefit (70; 01). One study demonstrated a moderate-to-good effect of greater occipital nerve injection of steroid and lidocaine in 63% of SUNCT patients (17). This has the advantage of rendering the patient pain-free and, therefore, free of systemic drugs for up to a few weeks, which may allow the titration of preventive medications. The largest series with the longest observation time was reported by Miller and colleagues (65). At a mean follow-up of 44.9 months (range 13 to 89), there was a 69% improvement in attack frequency with a response rate (defined as at least a 50% improvement in daily attack frequency) of 77%. Attack severity was reduced by 4.7 points on the verbal rating scale and attack duration by a mean of 64%. Improvements were seen in headache-related disability and depression. Adverse event rates were favorable, with no electrode migration or erosion reported.
Peripheral nerve block. Yalin and colleagues reported that infra- and supraorbital nerve blocks were effective in a pregnant woman with SUNCT (88).
Trigeminal microvascular decompression. Significant benefits with trigeminal microvascular decompression were reported in patients with refractory SUNCT and abnormal vascular loop in contact with the symptomatic trigeminal nerve at the root entry zone (51; 29; 81; 43; 32; 41; 34). An Australian group, in view of the significantly high percentage of patients with the association of abnormal vascular loop and SUNCT/SUNA syndromes, treated nine patients who had intractable pain with microvascular decompression. There was complete pain relief after the procedure in 67% of patients and minimal complications at a follow-up of 9 to 32 months (mean 22.2 months) (86). The largest study so far was an uncontrolled open-label prospective single-center study conducted between 2012 and 2020, evaluating the efficacy and safety of trigeminal microvascular decompression in refractory chronic SUNCT or SUNA in patients with magnetic resonance imaging evidence of trigeminal neurovascular conflict ipsilateral to the pain side (44). The study group consisted of 47 patients, of whom 31 had SUNCT and 16 had SUNA. The mean post-surgery follow-up was 57 months. Postoperatively, 78.7% of patients obtained either an excellent or a good response. Although more data are required with long-term follow-up, trigeminal microvascular decompression may be considered in patients with treatment-refractory SUNCT or SUNA and aberrant loops impinging on the ipsilateral trigeminal nerve shown on brain MRI.
Occipital nerve stimulation. Because occipital nerve stimulation has been reported to be effective in other primary headache syndromes, including chronic migraine and cluster headache, this therapeutic modality was tried in six patients (five SUNCT, one SUNA) (76). At a median follow-up of 14 months (range 4 to 19 months), four patients reported a substantial improvement (90% to 100%), one reported moderate benefit (50%), and one patient reported a temporary marked benefit (75%) for 6 months followed by recurrence of headache at the pre-occipital nerve stimulation baseline for the subsequent 11 months. The procedure was well-tolerated, though one patient developed hemicrania continua 1 month after implantation and was successfully treated with indomethacin. Another case series in nine medically intractable cases of SUNCT and SUNA reported a positive response to occipital nerve stimulation in all but one patient after a median follow-up of 38 months (49). The largest case series was reported by Miller and colleagues (65). They presented data on 31 patients with medically intractable short-lasting unilateral neuralgiform headache attacks. At a mean follow-up of 44.9 months (range 13 to 89), there was a 69% improvement in attack frequency with a response rate (defined as at least a 50% improvement in daily attack frequency) of 77%. Attack severity was reduced by 4.7 points on the verbal rating scale and attack duration by a mean of 64%. Improvements were seen in headache-related disability and depression. Adverse event rates were favorable, with no electrode migration or erosion reported. Occipital nerve stimulation appears to offer a relatively safe treatment option, without significant morbidity, for medically intractable SUNCT/SUNA. Smit and colleagues summarized the results from three studies with occipital nerve stimulation (ONS) in 41 patients (80). After a mean follow-up of 42.5 months, patients reported a 62% improvement in pain severity and 69% change in frequency of attacks. Major adverse events included local infection, lead migration, and local pain.
Hypothalamic region/midbrain tegmentum deep brain stimulation. In view of the functional imaging evidence of activation of the posterior hypothalamus region being linked to attacks of SUNCT, 3 patients with intractable SUNCT have been reported to have had a good response to deep brain stimulation in the region of the posterior hypothalamus, being pain-free or almost pain-free at 18 months (08), 12 months (53), and 15 months follow-up (04), respectively. In a second series, 11 patients with SUNCT refractory to medical treatment and occipital nerve stimulation were treated with deep brain stimulation of the ventral tegmental area of the posterior hypothalamus (64). After a median follow-up time of 29 months the improvement of daily attacks was 78%, and 82% of the patients had a reduction of attack frequency greater than 50%. Though the deep brain stimulation target has been described as the posterior hypothalamus, careful anatomical localization of the target reveals that it is at the midbrain tegmentum rather than the posterior hypothalamus (60).
Gamma knife stereotactic surgery. Gamma knife surgery is a well-known treatment for trigeminal neuralgia (23), whereas its effectiveness in treatment for trigeminal autonomic cephalalgias is yet to be established. Given the clinical similarities between trigeminal neuralgia and SUNCT, two patients with medically refractory SUNCT have been treated with gamma knife stereotactic surgery targeting both the trigeminal nerve and the sphenopalatine ganglion (22; 61). Both patients obtained a significant improvement. However, the follow-up was long enough in one case (39 months) but too short in the second case (4 months) to draw any meaningful consideration. No side effects were reported after the procedures. Another case series included five patients with chronic SUNCT who underwent gamma knife radiosurgery of the trigeminal nerve and sphenopalatine ganglion. All patients reported a reduction in pain attacks (27). A systematic literature search revealed six patients with SUNCT treated with radiosurgery (90). Four patients had a benefit from gamma knife radiosurgery. Smit and colleagues summarized data from nine patients in six publications (80). Seventy-eight percent of patients reported a change in attack frequency after a mean follow-up of 20.8 months.
Sphenopalatine ganglion pulsed radiofrequency. Ornello and colleagues treated nine consecutive patients with chronic SUNCT/SUNA refractory to medical treatments with sphenopalatine ganglion pulsed radiofrequency (67). After a follow-up of 30 months, seven patients were considered responders to the treatment defined as a reduction of headache episodes greater than 30%. Three patients experienced a worsening of head pain for 2 to 4 weeks immediately after the procedure.
A review summarized the results of interventional therapies for treating SUNCT and SUNA (80). Included were SUNCT and SUNA studies reporting outcomes following occipital nerve stimulation, pulsed radiofrequency of sphenopalatine ganglion, stereotactic radiosurgery, deep brain stimulation, or microvascular decompression of the trigeminal nerve. A successful response was defined as a greater than 50% reduction in severity of attacks or a greater than 50% reduction in the number of attacks. The rate of successful responses for the various treatments were occipital nerve stimulation 33 of 41 (80.5%), pulsed radiofrequency of the sphenopalatine ganglion 5 of 9 (55.6%), deep brain stimulation of the ventral tegmental area 14 of 16 (86.7%), stereotactic radiosurgery to the sphenopalatine ganglion or trigeminal nerve 7 of 9 (77.8%) ,and microvascular decompression 56 of 73 (76.7%).
Treatment should be initiated with drug treatment. In patients who fail medical therapy or cannot tolerate it, and trigeminovascular compression on MRA, trigeminal microvascular decompression is recommended. In patients who fail this approach or do not show trigeminovascular compression, bilateral occipital nerve stimulation is recommended. In patients who fail occipital nerve stimulation, deep brain stimulation of the tegmentum of the posterior hypothalamus should be considered.
Treatment of secondary/symptomatic SUNCT/SUNA. Treatment of the underlying structural pathology, such as medical or surgical removal of a pituitary tumor, can relieve the symptoms, although there are cases where the dopamine agonist bromocriptine has exacerbated the syndrome (52). Nevertheless, a series showed that both primary and secondary forms of the disease will respond to symptomatic management as outlined above (17).
There is little information on how pregnancy affects SUNCT. One documented patient stated that pregnancy worsened her symptoms (71). In terms of treating pregnant patients with SUNCT or SUNA, the greater occipital nerve injection should be considered, as it does not carry the teratogenic risk of systemic medications.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Hans-Christoph Diener MD PhD
Dr. Diener of the University of Duisburg-Essen received honorariums from Lundbeck and Novartis as an advisory board member.
See Profile
Shuu-Jiun Wang MD
Dr. Wang of National Yang-Ming University and Taipei Veterans General Hospital has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Jan. 19, 2025
General Neurology
Dec. 30, 2024
Headache & Pain
Dec. 19, 2024
General Neurology
Dec. 02, 2024
Headache & Pain
Nov. 30, 2024
Headache & Pain
Nov. 22, 2024
Headache & Pain
Nov. 18, 2024
Headache & Pain
Nov. 04, 2024