








Neuro-Oncology
Choroid plexus tumors of childhood
Jan. 14, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author reviews the early and late manifestations of syringobulbia, the differential diagnosis of syringomyelia and hydromyelia, and the 90% chance of long-term stabilization or improvement with surgical treatment in Chiari-related syringomyelia. Crowding of the foramen magnum causing abnormal cerebrospinal fluid movement is thought to be the main contributor to Chiari symptoms and syringomyelia. After successful craniovertebral decompression, most patients with pressure dissociation headaches and blackouts improve. However, other large variety of other symptoms often present may not improve after surgery. Syringomyelia and associated conditions, such as arachnoiditis and the Chiari I anomaly, are now readily diagnosed by MRI. New MRI techniques allow for the identification of subtle arachnoid scarring or tethers in the subarachnoid space in idiopathic syringomyelia patients.
|
• MRI is the diagnostic modality of choice for syringomyelia and associated conditions, such as Chiari I anomaly or arachnoiditis, and for the differential diagnosis of syringomyelia and hydromyelia. | |
|
• Preventive measures for the development of syringomyelia include the careful use of epidural anesthesia and the avoidance of a traumatic or prolonged labor and maneuvers that may induce “craniospinal” dissociation, such as Valsalva maneuver. | |
|
• Advanced cases of disability in patients are seen less frequently nowadays due to the major impact that MRI has had in early diagnosis and improvement in surgical techniques. | |
|
• Chiari I patients may suffer from nonsuboccipital headaches, not triggered by the Valsalva maneuver. | |
|
• Some patients show progressive neurologic deterioration and disabling pain despite proper surgical drainage of the syrinx and correction of the associated craniovertebral anomaly. Pain is a frequent and disabling manifestation of syringomyelia and a persistent symptom. | |
|
• In children with Chiari I malformation and syringomyelia, the presence of comorbidities at birth has a negative impact on the result of surgical procedures. | |
|
• Idiopathic syringomyelia can be resolved by section of scars or tethers visualized in the subarachnoid space by new MRI techniques. |
Ollivier d’Angers first coined the name "syringomyelia" in 1824, but the condition was first recognized by Stephanus in 1545. Schultze first described its clinical picture; its relation to Chiari malformation was first outlined by John Cleland. Abbe performed the first reported surgical drainage of a syrinx in 1891, although claims were made that Horsley aspirated a syrinx in 1890. The “hydrodynamic” theory of syringomyelia was proposed by Gardner in 1965 and modified by Williams in 1978 with the “craniospinal pressure dissociation” theory.
Syringomyelia is a rare condition defined as the development of a fluid-filled cavity located inside the spinal cord; the fluid is similar to cerebrospinal fluid (14). The cavity lies outside the central canal and does not have ependymal lining; however, it may have a partial connection with the central canal. Hydromyelia, or “dilated central canal” or “slit-like syrinx,” is a thin cavity lined partially or completely by ependymal cells and located at the place of the central canal, which should have disappeared after birth. “Communicating” or foraminal syringomyelia refers to cavities with a direct communication with the fourth ventricle through the obex and is usually associated with hindbrain malformations. “Noncommunicating” or nonforaminal syringomyelia refers to cavities without communication with the fourth ventricle and is usually secondary to trauma and tumors of the spinal cord but is also associated to hindbrain malformations. The famous golfer Robert “Bobby” Jones suffered from syringomyelia and it has been speculated that the well-known cellist Jacqueline du Pret might have suffered from syringomyelia rather than multiple sclerosis.
Onset is usually insidious and rarely acute, occurring in young adults around the third or fourth decade; however, it is not rare in children for whom congenital anomalies are the classical etiologies (14). Initial manifestations include pain, numbness of the hands, stiffness of the legs, scoliosis, vertigo, oscillopsia, diplopia, dysphonia, dysphagia, laryngeal stridor, hiccups, paroxysmal cervicobrachial cough-induced pain, sweating abnormalities, torticollis, drop attacks, and neurogenic arthropathy. The dissociated sensory loss is commonly first observed along the ulnar border of the hand and forearm, extending to the arm, upper part of the chest and back in a cape or half-cape distribution, uni- or bilaterally, and in the face following an “onionskin” distribution. All types of sensation may be lost in a limb due to involvement of the root entry zone. In advanced cases, compression of the spinothalamic tracts or the posterior columns give rise to long tract signs in the legs. Wasting and weakness first appear in the hands and progress to the forearm, arm, and trunk.
Hypotonia, areflexia, and fasciculations are commonly observed. Upper limb jerks may be preserved or brisk, or the Hoffman sign may be present due to the Chiari anomaly. Involvement of corticospinal tracts in advanced cases leads to spastic paraparesis. In the presence of lumbar syringomyelia, upper and lower motor neuron signs are found in the legs. Horner syndrome is present in 5% to 23% of cases and is (often) the only sign of the disease. The incidence is probably higher because sympathetic denervation can be overlooked when the change in pupillary diameter is minimal. The diagnosis is best established by looking for subtle ptosis and miosis. Trophic changes in the hands include hyperkeratosis, scars from old burns, subcutaneous edema, or hematomas.
Neuropathic arthropathy may involve shoulder, elbow, and hand, separately or simultaneously. Rotatory or vertical nystagmus is the most common sign of syringobulbia. Others include an onionskin pattern of sensory loss in the face, palatal weakness, and tongue atrophy with fasciculations. The cavity may ascend to the pons or even the internal capsule.
Advanced cases may have gastrointestinal (nausea, vomiting, epigastric pain, constipation, fecal incontinence), respiratory (dyspnea, stridor, central and obstructive sleep apnea, respiratory arrest, and cardiovascular (orthostatic hypotension, postural tachycardia) manifestations. Involuntary movements include spinal myoclonus, postural tremor, and focal dystonia (19). In posttraumatic syringomyelia, onset of symptoms ranges from 3 months to 35 years after trauma and include an ascending sensory level, pain in the neck or arms, increased muscle weakness, and spasticity.
Pain is a major complaint in a significant proportion of syringomyelia patients and is probably due to disordered neuronal processing in the damaged dorsal horn.
Headache is a frequent presenting symptom when there is an associated Chiari I malformation. It is usually suboccipital, with neck pain worsened by the Valsalva maneuver, coughing, or sneezing.
Untreated syringomyelia tends to run a slowly progressive course, leading to severe disability. Advanced cases of disability in patients are seen less frequently nowadays due to the major impact that MRI has had in early diagnosis and improvement in surgical techniques. Nevertheless, it is known that, for some patients, syringomyelia improves or stabilizes without surgical treatment, and spontaneous resolution of syringomyelia has been observed more frequently using MRI (29).
Surgery has been reported as an effective and safe treatment for Chiari-related syringomyelia, with a 90% chance of long-term stabilization or improvement on average (01).
After successful craniovertebral decompression, most patients presenting with pressure dissociation headaches and blackouts improve. However, nonspecific symptoms, such as subjective dizziness and balance problems, may not improve (22). Although early decompression of Chiari I malformation with syringomyelia results in stabilization of scoliosis, surgery may be required to improve the spinal deformity (04). Even adequately operated patients may show subtle deterioration, most likely due to gliosis alongside the walls of the syringomyelic cavities, even though the syrinx is no longer distended. Bad prognosis is associated with symptoms of over two years duration, presence of ataxia, nystagmus, bulbar symptoms, muscle atrophy, dorsal column dysfunction, or a longer and deviated syrinx or narrowing of the subarachnoid space. Persistent dysesthetic pain can occur despite improvement or collapse of the syrinx on the postoperative MRI; it may remain the most disabling complaint for patients. Spontaneous drainage of the syrinx into the subarachnoid space may occur, usually in the context of an acute episode of local pain and neurologic deterioration (03).
Syringobulbia usually complicates syringomyelia, possibly through the “slosh” concept (33). When intraspinal pressure is increased by straining or tightening of the abdominal muscles and cannot equalize intracranial pressure due to ectopia, this pressure is transmitted to the syrinx, and the fluid cyst travels upwards. Other long-term complications include neurogenic arthropathies, cervical spondylosis, central and obstructive sleep apnea, and sudden death (18). Complications after foramen magnum decompression include spinal cord damage by neck hyperextension or hyperflexion during intubation, spinal cord ischemia due to arterial hypotension, CSF leakage with formation of a symptomatic pseudomeningocele, posterior fossa bleeding, infection, hydrocephalus, cerebellar ptosis, and severe brainstem compression. Complications of shunting procedures are malfunction, local hematoma, infection, or a collapsed syrinx.
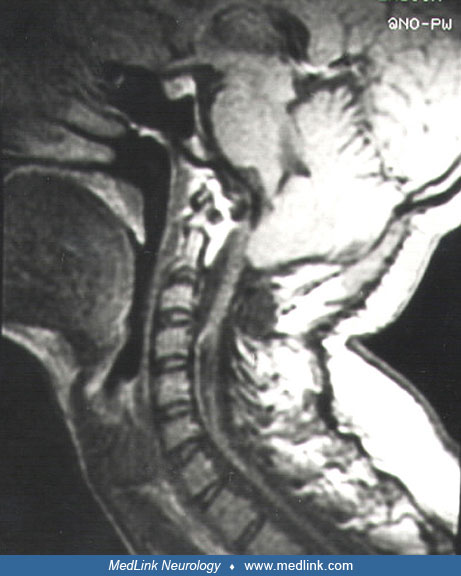
A 19-year-old female noticed mild progressive weakness and numbness distally in upper extremities for the last 12 months. Birth history was normal, and there was no history of head injury. On examination she had left Horner syndrome, bilateral weakness and wasting of intrinsic hand muscles, an area of suspended dissociated sensory loss from C3 to T8 bilaterally, areflexia in upper limbs, and brisk lower limb reflexes. Hairline was rather low, and there was a mild thoracic scoliosis. Nerve conduction studies showed reduced compound motor action potential amplitudes in both median and ulnar nerves as well as normal sensory nerve action potentials. An MRI showed a Chiari I anomaly and an extensive bilateral cervicothoracic syrinx.
The patient was treated with decompression of the foramen magnum and placement of two syringo-peritoneal shunts. She did well initially, but six months after surgery she developed progressively disabling headaches occurring specifically in the upright position or during periods of strenuous activity. An MRI showed further cerebellar descent, an abnormal angulation and indentation of the midportion of the medulla oblongata, and partial collapse of the syrinx. Symptoms disappeared after further duraplasty of the posterior fossa and extraction of the shunts. The condition has remained stable during a follow-up period of 10 years.
The explosion of knowledge provided by modern imaging has permitted new insight into the pathophysiological mechanism of syringomyelia. The current classification distinguishes 5 entities (Table 1) (14).
|
Classification |
Pathogeny |
Etiologies |
|
Foraminal syringomyelia |
Hindbrain pathologies |
Chiari malformation (type I or II) |
|
Dandy Walker malformation | ||
|
Posterior fossa cysts | ||
|
Inherited or acquired bone malformations | ||
|
No clear hindbrain pathology |
Foraminal arachnoiditis | |
|
Nonforaminal syringomyelia |
Arachnoiditis |
Spine trauma |
|
Infections (eg, tuberculosis, listeria) | ||
|
Inflammation (subarachnoid bleeding) | ||
|
Herniated disc | ||
|
Focal arachnoid brindle | ||
|
Spinal arachnoid cyst | ||
|
Spinal dysraphism |
Tethered cord | |
|
Spina bifida and lipoma | ||
|
Diastematomyelia | ||
|
Tumoral syringomyelia |
Intramedullary tumors |
Ependymoma |
|
Hemangioblastoma | ||
|
Communicating syringomyelia |
Communication between 4th ventricule and central cord canal |
Hydrocephalus |
|
Hydromyelia or “slit-like” syrinx cavity |
Persistent dilated central canal |
Idiopathic |
Many familial cases of craniovertebral malformations, including syringomyelia, have been reported (12). It is likely that syringomyelia associated with Chiari I anomaly is genetically determined. Many patients with syringomyelia were born after a difficult labor. Syringomyelia may complicate basal or spinal arachnoiditis after bacterial meningitis, subarachnoid hemorrhage, tuberculosis, trauma, repetitive deceleration in skydivers (34), a CSF leak after brachial plexus avulsion (26), idiopathic intracranial hypotension (23), and reaction to radiopaque material, spinal anesthesia, or detergents. Exceptional cases of familial adhesive arachnoiditis associated with syringomyelia have been reported (21). Syringomyelia may be secondary to intra- or extramedullary spinal tumors and infratentorial tumors. Ependymomas and hemangioblastomas have a 50% incidence of associated syringomyelia.
In syringomyelia secondary to basal arachnoiditis as well as in a low percentage of syrinx associated to Chiari I anomaly, Gardner's “hydrodynamic theory” may be operative. CSF may be forced to enter through the obex into a patent central canal leading to communicating syringomyelia. In the majority of the Chiari I-associated cases, there is no demonstrable communication at the obex. The anatomical and physiological blocks to the CSF, which occur in response to brain expansion during cardiac systole, alter the flow from the cranial to the spinal subarachnoid space and force the cerebellar tonsils into the partially enclosed spinal subarachnoid space. Exaggerated spinal pulse pressures are generated, forcing movement of CSF from the subarachnoid space into the spinal cord through the Virchow-Robin spaces. Alternatively, these transmedullary pressure gradients may induce movement of the extracellular fluid normally produced within the spinal cord, particularly in narrow regions of the spinal CSF pathways. Abnormal accumulation of this interstitial fluid may constitute a “presyrinx” state, a potentially reversible alteration, seen in MRI as an enlarged spinal cord with parenchymal T1 and T2 prolongation before the appearance of syringomyelia, and which can manifest as an acute or chronic myelopathy (08).
The risk of developing a syrinx with Chiari malformation appears to be related to relative foramen magnum stenosis. Patients found to have a syrinx have a lower tonsillar position on imaging (09).
Subtle arachnoid scarring or tethers in the subarachnoid space can be detected and can provide a pathogenic explanation for an evolving idiopathic syringomyelia (14). Syringomyelia in the absence of a Chiari anomaly may also be due to an encroachment of neural structures in the posterior fossa, the so-called “tight cisterna magna.” Patients with this condition undergo craniocervical decompression with favorable results. It has been suggested that spinal cord cavities associated with tight cisterna magna should not be classified into an idiopathic group but rather into an organic group that is associated with foramen magnum lesions (07). Some idiopathic syringomyelia patients have abnormally narrow upper- and mid-cervical spinal canal diameters, which may cause longitudinal pressure dissociation and transmural pressure gradients, leading to cavity formation (28).
Extradural spondylotic compression of the spinal cord has been advocated as another etiology of syringomyelia (05). A purely extradural decompression could be sufficient to induce regression of the medullary cavitation.
In posttraumatic syringomyelia, necrosis and cysts resulting from fluid egress from damaged axons may develop at the site of spinal cord trauma. Alterations of aquaporin-4 expression or function may contribute to the fluid imbalance leading to syrinx formation or enlargement (10). A disturbance in the removal of K ions in tissue surrounding the syrinx cavity may contribute to water accumulation in the injured spinal cord, leading to syrinx formation or exacerbation of the underlying pathology (17).
Other predisposing factors include increasing age, cervical and thoracic levels compared with lumbar, displaced fractures, and spinal instrumentation without decompression (30). When syringomyelia is secondary to spinal arachnoiditis or a spinal cord tumor, a vascular mechanism may be responsible. In tumor-associated syringomyelia, neoplastic growth may interfere with blood supply to the spinal cord and cause ischemia, necrosis, and cavity formation. Alternatively, it may affect tissue fluid drainage through perivascular spaces. Edema may play a major role in syrinx development and maintenance as well.
Determining the prevalence of Chiari malformation and an associated spinal syrinx is challenging. The estimated prevalence of syringomyelia is between 1.94 per 100,000 in Japan and 8.4 per 100,000 in Western countries (25). Imaging studies estimate Chiari malformation prevalence to be between 0.24% and 3.6%. Of those diagnosed on imaging, symptomatic cases vary greatly from 32% to 63% (11). Proportional rates from several series range from 0.4% to 1% of cases admitted to neurologic clinics. An autosomal dominant predisposition may be the primary factor in the appearance of familiar cases. Males and females are equally affected. Incidence of posttraumatic syringomyelia is 0.02% (06).
The avoidance of a traumatic and prolonged labor (including the use of forceps) may prevent the development of syringomyelia in predisposed newborns. Similarly, careful use of epidural anesthesia, avoiding entering into the subarachnoid space, may prevent the development of spinal arachnoiditis and syringomyelia. Finally, in the presence of a Chiari anomaly and disturbed CSF flow across the foramen magnum, avoidance of any maneuver that may induce “craniospinal” dissociation (such as excessive coughing, sneezing, or weight lifting) may prevent the enlargement of an established syrinx until appropriate decompression has been accomplished. Nevertheless, it is still controversial whether activity restriction is necessary in asymptomatic children with Chiari anomaly.
In hydromyelia, neurologic exam and electrophysiological testing are normal, and the central canal is less than 6 mm in diameter on MRI (24). To distinguish central canal dilatations from syringomyelia, cine MRI will demonstrate no flow signal inside the dilatation and no obstruction of CSF flow adjacent to it, unlike in syringomyelia (13). This distinction may require repeated scans and clinical examination. Filiform intramedullary cavities may be found incidentally in the dorsal spinal cord of normal young subjects; they are most likely due to persistence of the central canal of the spinal cord. Cervical spondylotic myelopathy can also present with lower motor neuron signs in upper limbs and upper motor neuron signs in lower limbs. Nevertheless, it is more common in the elderly, and there is no neurogenic arthropathy, trophic changes, or bulbar signs. On MRI there is narrowing of the spinal canal or cavitation. Motor neuron disease and progressive spinal muscular atrophy present with no sensory disturbances and a normal MRI. In multiple sclerosis, dissociated sensory loss, trophic changes, and neurogenic arthropathies are rare manifestations, CSF shows high IgG and myelin-associated protein, and visual evoked potentials are usually abnormal. Noncommunicating syringomyelia may occur in multiple sclerosis patients with spinal cord pathology. It can be a subtle finding without clinical correlates (32). Diabetes, leprosy, and hereditary sensory neuropathies may present trophic changes and dissociated sensory loss, but lower limbs are affected first, the distribution of the sensory abnormalities is in a glove and stocking pattern, and nerve conduction studies and nerve biopsy are abnormal. Spinal cord tumors may mimic syringomyelia, although pain is usually more severe, progression is more rapid, and there are no trophic changes or neurogenic arthropathies. An increased protein concentration in the CSF, an enlarged spinal cord, and enhancement of the lesion with gadolinium favors the diagnosis of an associated spinal cord tumor. Spinal syphilis is ruled out by the absence of dissociated sensory loss, increased CSF protein, and cell count with positive VDRL. Ulnar and median mononeuropathies and thoracic outlet syndrome rarely lead to trophic changes or neurogenic arthropathy. Sensory loss is localized to the distribution of the nerve affected. Nerve conduction studies confirm the entrapment, sensory nerve action potentials are abnormal, and MRI is normal.
Nevertheless, carpal tunnel syndrome and ulnar entrapment at the elbow are more common in syringomyelia patients than in the normal population.
MRI is the diagnostic modality of choice. T1-weighted images best delineate cord and syrinx morphology, whereas T2-weighted sequences best evaluate for associated conditions such as myelomalacia, gliosis, or tumor. In the presence of a Chiari I anomaly, axial and sagittal T1-weighted images of the cervical spine should be performed to evaluate for a cervical syrinx.
If the syrinx cavity extends caudal to the field of view, a separate examination of the thoracic spine should be performed as well to define the full extent of the central syrinx cavity. Intracranial neuroimaging should be done to rule out hydrocephalus. Tonsillar descent is considered abnormal when it is more than 5 mm below the foramen magnum, and occasionally, it can only be revealed in the sitting position during surgery, the so-called “up-and-down Chiari malformation.”
New MRI sequences have been added to the basic morphological MRI. 3D constructive interference in steady state sequence and CSF flow void (cine-MRI) or phase-contrast MR of CSF flow dynamics are very useful in determining the site of obstruction of CSF pathways (35; 36; 31). Diffusion tensor imaging allows for the evaluation of the quality of the fiber bundles present around the lesion.
Caudal flow occurs normally during systole in the basal cisterns and in the spinal subarachnoid space. Following cardiac diastole, CSF motion reverses, flowing rostrally in the spinal canal. Flow dynamics assessed by cine phase contrast MRI could independently predict response to posterior fossa decompression. Following foramen magnum decompression, CSF should be identified anterior to the cervicomedullary junction and posterior to the tonsils on sagittal T1-weighted images. MR phase contrast imaging demonstrates pulsatile fluid motion in syrinx cavities in synchrony with the adjacent subarachnoid space, mainly in large cavities. Following decompression, syrinx flow decreases as the size of the cavity decreases. Slit-like syrinx cavities may be found in patients studied with MRI for radicular pain, paresthesia, numbness, or muscle spasm. They probably do not represent true syringomyelia but rather remnants of the central canal (hydromyelia) detected in a small percentage of adults. As hydromyelia does not represent a disease with an underlying pathology, no clinical or radiological progression has been seen.
Motor conduction velocity may be mildly reduced in upper limbs due to degeneration of the fastest conducting fibers. Normal sensory nerve action potentials indicate the preganglionic localization of the disorder. F-waves are prolonged in the presence of a cervical syrinx involving segments C8 and T1.
Somatosensory evoked potentials help to assess dorsal column function during shunt placement. Brainstem auditory evoked potentials (BAEP) are abnormal in a third of Chiari I malformation patients, but they do not add clinically relevant information in establishing which symptomatic patients with Chiari malformation should undergo surgical treatment. CSF composition is normal, but protein levels are raised in the presence of an associated tumor. Plain skull x-rays may show signs of arrested hydrocephalus, basilar impression, or platybasia. Cervical spinal x-rays may show a wide cervical spinal canal, occipitalization of the atlas, and fusion of cervical vertebrae.
The evidence that syringomyelia can spontaneously resolve makes the treatment strategy controversial. Because of the slow progression of symptoms and that surgery may lead to a neurologic deficit, some centers advocate waiting for signs of neurologic deterioration or change in MRI findings before operating. Others, however, argue that deterioration may be sudden and that surgical intervention is warranted in symptomatic Chiari malformation when the condition is diagnosed. Nevertheless, there is general agreement that early correction of abnormal CSF dynamics is the best alternative. Indications for surgery include symptoms from foramen magnum compression, advancing syringomyelia, suboccipital and lower central neck pain, particularly provoked by Valsalva maneuver, cape-like dissociated sensory loss, dysesthesias, gait difficulty, nystagmus, upper or lower extremity weakness, cranial nerve dysfunction, and blurred vision. Surgery is not recommended in the following situations: (1) contraindications to surgery, such as advanced disease with respiratory failure and severe deficits and kyphoscoliosis; (2) patients in stable condition who progressed fairly rapidly in the early stage and then became stable; (3) patients with spontaneous cure, which may be observed in 1% of cases (03); (4) asymptomatic patients; and (5) a spindle syrinx in a patient with pain. Children in whom scoliosis is the only manifestation may be treated conservatively because spontaneous shrinkage of the cavity may occur.
Because shunting of the syrinx carries the risk of spinal injury, there is a strong tendency that surgical treatment of syringomyelia associated with the Chiari malformation should be directed at reconstructing normal CSF pathways. Most authors currently recommend bony decompression with opening and patching of the dura as the initial treatment. Plugging of the obex and exploration of the fourth ventricular outlet are becoming less common because there is rarely a functional communication between the fourth ventricle and the syrinx. Furthermore, this procedure may produce bradycardia, postoperative respiratory distress, or damage to the hypoglossal and vagal nuclei. In the uncommon case of a patient with a Chiari I malformation and extensive subarachnoid scarring, simple bone and dural decompression will not eliminate the obstruction of the free flow of CSF within the subarachnoid spaces and may not induce resolution of syringomyelia. If hydrocephalus is present, it has to be treated first. Endoscopic third ventriculostomy provides a durable method of treatment for hydrocephalus associated with Chiari malformation. Section of the filum terminale is another useful strategy in cases with terminal syringomyelia and a tethered spinal cord and without a Chiari anomaly.
When foramen magnum decompression is unsuccessful, shunting of the syrinx is appropriate, although the best type of shunting procedure to use remains unclear. Syringoperitoneal and syringopleural shunting place the distal catheter into a seemingly low-pressure extrathecal site. Some authors consider the preferred treatment to be syringosubarachnoid shunt through a dorsal root entry-zone myelotomy at the level of the largest part of the syrinx, in order to prevent cord damage and in order to obtain some relief of pain.
Shunting is also the method of choice in idiopathic syringomyelia, but in these cases, the section of abnormal arachnoid scarring or tethers in the subarachnoid space visualized by any of the new dynamic MRI techniques may lead to resolution of the syrinx (27).
When syringomyelia is secondary to trauma or adhesive arachnoiditis, results are less promising; postoperative recurrence of adhesions is the rule. The treatment focuses mainly on alleviating pain, improving quality of life, and managing symptoms. The role of surgical treatment remains unclear, but when used, surgical treatments usually include releasing a tethered cord and restoring CSF flow. Techniques include decompressive laminectomy-adhesiolysis and augmentation duraplasty in arachnoiditis cases, ventriculoperitoneal shunt for hydrocephalus, cyst extirpation in pseudomeningeal cyst, and both anterior and posterior decompression-fusion in the case of postlaminectomy kyphosis (15).
Acute surgical complications include infection, hemorrhage, and CSF leakage. Long-term complications may be technical-related such as pseudomeningocele, a bony opening too large or too small, inadequate restoration of CSF flow, and instability (02).
Untreated syringomyelia tends to run a slowly progressive course.
Epidural anesthesia may promote the formation of subarachnoid or intramedullary cysts in previously healthy pregnant women (20).
General anesthesia is preferred to epidural or spinal anesthesia. Nitrous oxide and isoflurane have been used safely (16).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Martín A Nogués MD
Dr. Nogués of the FLENI Foundation has no relevant financial relationships to disclose.
See Profile
Matthew Lorincz MD PhD
Dr. Lorincz of the University of Michigan has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
Jan. 14, 2025
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
General Neurology
Dec. 30, 2024
Neuromuscular Disorders
Dec. 29, 2024
Developmental Malformations
Dec. 26, 2024