

Epilepsy & Seizures
Tonic status epilepticus
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Although historically thought of as a childhood disorder, data demonstrate that tethered cord syndrome can present even in adults. Furthermore, the diagnosis and treatment are relatively straightforward in most patients, and permanent disability may result if tethered cord is not detected and corrected early. The authors describe the etiology, pathogenesis, presentation, diagnosis, and treatment of tethered cord syndrome in both adults and children.
• Although usually considered a childhood disorder, tethered cord syndrome can present in adulthood. | |
• Prior neurosurgical, urological, or orthopedic surgeries may increase the risk of tethering if around the spine, or have been performed due to symptoms that were not appreciated as due to tethered cord. | |
• Failure to timely diagnose and treat tethered cord syndrome results in worse long-term outcome. | |
• Neurologists are often the medical providers that make the diagnosis. | |
• Tethered cord syndrome describes a constellation of symptoms secondary to tethering of the spinal cord. | |
• Occult tethered cord syndrome is increasingly being recognized, presenting with either pain or urological symptoms in adults or children, respectively. | |
• Radiological diagnosis includes filum terminale thickness greater than 2 mm or conus medullaris position below L1-L2 on MRI. |
The first clinical description of the tethered cord syndrome appears to be in an 1857 report by A Johnson of a young child with worsening symptoms that improved after surgery; a lesion consistent with a lipoma was found, and the spinal cord was freed from its dural attachments. In 1875, Virchow introduced the term “spina bifida occulta.” Then, in 1891, a patient underwent untethering surgery by WL Jones for lower extremity weakness, atrophy, and deformities; division of a “dense adventitious fibrous band” was done, and the patient showed improvement 6 months after surgery. In 1916, the first description that symptoms could be worsened by activity was reported by WG Spiller (101). Recognition that early treatment might result in improved outcome was noted as early as 1918 by WM Brickner. Subsequent articles have reported tethered cord syndrome in many clinical situations, both in children as well as adults. The widespread recognition of the tethered cord syndrome is relatively recent, particularly as it relates to cases of myelomeningocele and lipo(myelo)meningoceles. The first recognition that multiple pathophysiological entities could give rise to this common clinical presentation was in the 1950s, and that was when terms such as “filum terminale syndrome” and “cord-traction syndrome” began to be used (28). The first major series was that of Hoffman, Hendrick, and Humphreys in 1976 (41), in which the term “tethered spinal cord” originated. Our current understanding of this syndrome has advanced to the point where it is now considered a lesion complex with heterogeneous causes (44; 02; 60; Yamada and Won, 2007; 120). Operative care of this lesion complex has advanced over the last few decades. Finally, our understanding of the pathophysiology of this condition was advanced by Yamada and colleagues who, using an experimental model of spinal cord tethering, found evidence of cellular ischemia (120; 25). An animal model was reported for tethered cord syndrome, based on chronic slow traction, which will hopefully yield new information on the pathogenesis of this syndrome, as well as help delineate when and if patients should undergo surgical intervention (43).
Tethered cord syndrome is most appropriately viewed as a clinical syndrome composed of a group of neurologic symptoms and signs, and caused by a collection of developmental anomalies of the caudal vertebrospinal axis or the consequences of their surgical repair. As noted by Humphreys, the term is descriptive at best because its clinical presentations are as variable as its causes (44; 02; 60; 119). It does not denote (1) causation; (2) whether the dysraphism is open or closed; (3) at what level the cord is tethered; or (4) whether the causative agent is intradural, extradural or both. There are 2 major groups of patients seen with this condition: (1) individuals with known spinal dysraphism who often have been previously operated on, and (2) individuals with a currently undiagnosed underlying spinal dysraphism. A neurologist is likely to encounter both types of patients. It is important to understand the clinical presentation of this condition, its proper evaluation, and when to consider referral to a neurosurgeon.
Tethered cord syndrome can present in childhood, and it most often does so in individuals with obvious spinal dysraphism, such as repaired myelomeningocele or lipo(myelo)meningocele. Clinical manifestations in children include progressive motor and sensory deterioration (particularly motor, with difficulties with gait or running); deterioration in urologic function; developmental or orthopedic deformities of the foot, leg, and spine; and, less commonly, back and leg pain (41; 55; 84; 35; 02; 15; 60; 119; Bowman et al 2008; 40). In adolescents, scoliosis, pain, and sphincter dysfunction predominate. Symptoms may be exacerbated by back flexion and extension. There may be a history of prior orthopedic or urological surgeries, especially if the possibility of tethered cord syndrome was not appreciated (02; 15; 60; 14). Although long thought to be a disorder of children, adult presentations, and the usefulness of surgical detethering has become increasingly appreciated (57; 121; 58; 29; 30).
Pang and colleagues were the first group to present a series of adults with tethered cord syndrome along with clinicopathologic correlation (77). Over half of the patients in their series were without neurologic problems during childhood. The other 44% had only minor nondisabling problems in childhood, such as fixed-foot deformities or mild sensorimotor findings. They suggested that although the underlying pathologies between the childhood and adult syndromes were similar, the clinical manifestations and outcomes were different. Since then, numerous case series have shown that adults are much less likely to present with scoliosis or foot deformities. Pain and sensorimotor changes are much more common in adults than in children. The pain is most frequently back or leg pain, nondermatomal, shocklike or burning in quality, often with referral to the anorectal region, and can occur in up to 80% of patients. The straight-leg raising test may be positive in patients with tethered cord syndrome, which is consistent with the observation that symptoms may be exacerbated by back flexion and extension, and low back pain may be seen. Bladder or bowel symptoms are frequently seen, although less frequently than in most childhood series. Cutaneous stigmata of spinal dysraphism, such as lumbosacral subcutaneous lipoma, midline hypertrichosis, and sacral nevi, are relatively common (20% to 50% of patients) but are not universal. On neurologic exam, weakness may be subtle or pronounced, with involvement of multiple myotomes. Both upper and lower motor signs may be seen. With sensory exam, skip lesions are common. Reflexes and tone are variable and may have both upper and lower motor signs in different areas (77; 58; 02; 60; 29; 54; 30). In 1 case presented by Jackson and colleagues, an adult patient with a history of laminectomy 35 years prior presented with tethered cord syndrome following a recent Chiari decompression, suggesting the ability for tethered cord syndrome to be acquired through iatrogenic causes (48).
Tethered spinal cord can present as congenital scoliosis (80; 02; 60; 68; 87). This is important to identify because the tethered cord should be repaired prior to or simultaneously with scoliosis surgery (15; 14; 11). Although there are reports of children presenting with tethered cord as isolated urinary incontinence with features of neurogenic bladder (93), larger studies have failed to show increased risk for tethered cord in patients presenting only with lower urinary tract dysfunction (71), and other studies have shown the correlation of urinary incontinence to be greater with sacral dysplasia rather than tethered cord itself (01). Intractable constipation has also been reported as a predictor for tethered cord (85), but a report failed to show any increased risk for tethered cord in children with chronic constipation (13). Some children with urinary symptoms alone and normal neuroimaging may represent occult tethered cord, and these patients represent a therapeutic challenge because many of them will spontaneously improve without treatment, and surgery may result in clinical deterioration in some (107). Given the high frequency of urinary incontinence and constipation in children, and the fact that most patients will improve either spontaneously or with medical treatment alone, it is difficult to advocate surgery for patients with bowel or bladder symptoms and no other evidence of tethered cord (112; 20; Liu et al 2007; Seldon 2007; 14). Additionally, although terminal syringomyelia can frequently be associated with tethered cord, it appears to make no difference in outcome whether or not the syrinx is treated (12). Arachnoid cysts can also be found in association with spinal dysraphism and may require treatment (82).
Cutaneous stigmata are very common, seen in up to 60% of patients with tethered cord. These include hypertrichosis, cutaneous capillary hemangiomas, dermal sinus tracts, midline subcutaneous lipomas, lumbosacral skin appendages, and atretic meningocele “cigarette burn” lesions (02; 15; 60; 14; 17). However, a study showed that coccygeal pits are not associated with spinal dysraphism (115). It appears that a consensus has not yet been reached on what comprises the full spectrum of symptomatic tethered spinal cord. Even the definition of tethered cord is still being defined, given reports of a normal appearing filum terminale that can still exhibit histological abnormalities that lead to symptoms and respond to untethering (94; 95; 119). This is in part because accurate localization of the caudal tip of the spinal cord cannot be determined except surgically (neuroimaging is only an estimate), and filum thickness is less important than filum elasticity (119). Furthermore, some authors have speculated that some patients are genetically programmed to have a high conus and, thus, the position of the conus at a normal level is actually abnormal for that patient (102). Additionally, a normal filum but low conus medullaris (terminating below the midbody of L2) should always considered tethered cord (Kesler at al 2007; 119).
There is often a need for operative revision after index tethered cord release. Any patient with a history of tethered cord syndrome or other spinal cord anomalies, and who has had prior surgery and who then presents with new symptoms, may have retethering. This is unrelated to whether the original untethering procedure was for an asymptomatic or symptomatic condition (34). In fact, up to 25% of patients can experience retethering between 1 month and 20+ years after surgery (97). Surgery can arrest or even reverse these new symptoms, but careful monitoring is required to detect new symptoms (08; 05; 62; 97; 76).
A series study of 55 pediatric patients from a single medical center in Australia who underwent detethering surgery over a 5-year period reported the most common complications were wound infection and cerebrospinal fluid leak, with 6 children requiring reoperation for wound issues and 2 patients for cord retethering during the study period. There were no deaths or new neurologic deficits. Of children with preoperative deficits, 26.7% were documented to have improvement or resolution of their symptoms postoperatively. The highest rate of improvement occurred in children with motor or gait or sphincteric disturbance (106). Tethered cord release surgeries can also lead to development of spinal intramural arachnoid cysts. Although uncommon, these cysts must be considered in the case of new compressive symptoms after a procedure that penetrates the dura such as spinal cord untethering (32).
A review of surgical treatment of tethered cord syndrome in children in the United States demonstrated a steady trend of increasing operative treatment in more recent years. They demonstrated that older children tended to have more complications, longer lengths of stay, and higher hospital costs. They felt that the data supported surgical intervention at a younger age, in order to both improve outcome and reduce health care costs (99).
Data on adults suggest that surgery can be beneficial in improving symptoms, especially pain, but surgical intervention is advocated only in symptomatic patients (54; 30). Furthermore, surgical intervention in symptomatic adult patients has been reported to result in significant improvement and even reversal of neurologic deficits such as motor sensory dysfunction and bladder dysfunction (36; 27).
A 12-year-old girl presented to the spina bifida clinic. She previously underwent lumbar myelomeningocele repair in the neonatal period. She had a recent history of increased fatigue when walking more than a block. She also reported increased urinary leakage between her bladder catheterizations. There was no history of recent trauma.
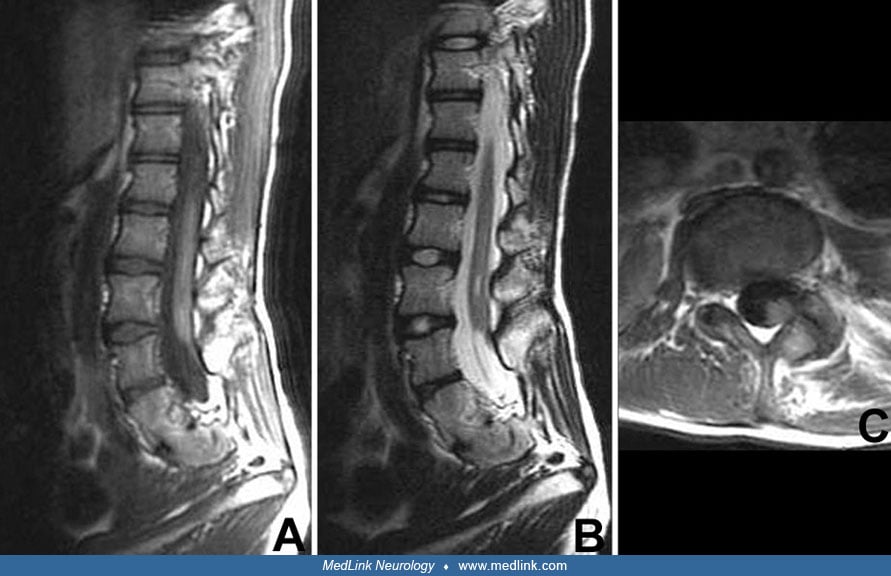
Her exam showed some increased weakness of both ankles with dorsiflexors. Her patellar deep tendon reflexes were hyperactive, and her ankle reflexes were absent (as they often were in myelomeningocele). The tone in her lower extremities was moderately increased. There was a sensory deficit below L5. Her gait was somewhat Trendelenburg and crouched. She had a vertical surgical scar in the lumbosacral region of her back. MRI of her lower spine showed a tethered spinal cord with the conus medullaris ending at L5.
The patient underwent a spinal cord untethering. Postoperatively, she had improved endurance and ankle dorsiflexion strength. Since the untethering, her clinical improvement has remained stable, with no new symptoms or signs of a tethered spinal cord.
During fetal life, the spinal cord extends to the sacral (coccygeal) area. There is a progressive ascent of the conus medullaris between 12 and 33 weeks’ gestation such that the conus is at or above the L3 vertebra by 33 weeks’ gestation, at or above L2-L3 disc space by 40 weeks’ gestation, and at or above the L1-L2 disc space by 2 months after birth (10). In fact, MRI and ultrasound data suggest that the conus may be at the L1-L2 space as early as 40 weeks’ gestation (15). The shortening of the cord is secondary to retrogressive differentiation that results in the filum terminale, cauda equina, and ascension of the conus relative to the vertebral bodies; continued growth of the vertebral column causes further ascension of the conus, stretching of the filum, and growth of the cauda equina. A study showed that the conus medullaris most commonly terminates at the L1-L2 disc space and, in the absence of tethering, virtually never extends past the midbody of L2 (50).
Tethered cord may be congenital (primary) or acquired (secondary). Primary causes of tethered cord are associated with congenital anomalies (114; 111; Argawalla et al 2007; 15; 60; 70; Clark et al 2016; 39), including meningocele, split cord, caudal agenesis, meningocele manqué (spontaneously healed meningocele), fatty filum terminale, imperforate anus, dermal sinus, lipoma, pseudotails, and others. Furthermore, there are multiple developmental syndromes associated with tethered cord such as neurofibromatosis-1, Klippel-Feil syndrome, FG syndrome (short stature, large head, congenital hypotonia, developmental delay, and other anomalies), Klippel-Trenaunay-Weber syndrome, Dandy-Walker anomaly, the Ehlers-Danlos syndromes, Haberland syndrome, Chiari malformation (type 1 or 2), OEIS (omphalocele, exstrophy of the cloaca, imperforate anus, and spinal malformations with tethered cord), and VATER (vertebral malformations, imperforate anus, tracheoesophageal fistula, and renal-radial anomalies) or VACTERL syndrome (VATER with cardiac and limb defects). A report demonstrated tethered cord in 39% of children with VACTERL, 7.9% with anal atresia, and 2.4% with tracheoesophageal fistula (75). Secondary causes of tethered cord syndrome include infection, trauma, tumor, and fibrosis, which can disrupt the normal anatomy of the caudal spinal cord. In fact, anything that alters the normal relationship between the filum and conus may result in tethered cord (Argawalla et al 2007; 60; 25). A study showed that adipose tissue on neuroimaging correlated with a low lying conus and fatty filum, whereas nerve twigs on filum pathology correlated with abnormal urodynamics (105).
The connection between the filum and conus is important because it allows the cord to stretch during flexion and extension movements. However, although the filum stretches linearly with applied tension, the spinal cord elongates in a nonlinear fashion, and the caudal portion of the cord stretches the most when tension is applied (41). With increased linear stress, blood flow to the caudal cord is impaired, resulting in hypoxia and impaired oxidative metabolism (120; 40; 103). Because the degree of traction correlates with the amount of dysfunction, the damage goes from being initially reversible to irreversible with increased stretch or prolonged traction. This explains how adults can present with tethered cord syndrome: the tethering has always been present, but extrinsic factors outside the cord, such as increasing fibrosis of the filum; growth spurt during the late-teen and early-adult period; increased physical activity, especially with flexion and extension of the spine; or osteoarthritic spinal stenosis, which restricts movement of the cord and filum, can all result in increased stress to the caudal spinal cord (120; 40; 103). Patients with spinal dysraphism that limits cord movement are predisposed to developing tethered cord (91). Further, adults can present after a precipitating event (ie, disc herniation), suggesting that the adult tethered cord may be under just enough tension as to not cause symptoms, and any increased stretch or tension that reduces blood flow could lead to hypoxia and tethered cord syndrome (22). Even normal daily movements of the neck and back may cumulatively result in increased tension, causing symptoms to develop over years. Also, lesions such as a dermal sinus, lipoma, tumor, scar tissue, or fibrous tissue can progress, resulting in later-onset symptoms (120; 40; 103).
Heterozygous missense mutations at VANGL1 and FUZZY have been indicated as risk factors for tethered spinal cord syndrome as well as altered methylation of MGMT and maternal folic acid deficiency. Copy number variants have been found in genome of affected patients which include the COX8C gene. COX8C is associated with metabolic disorders of the nervous system (124).
As previously mentioned, tethered cord is associated with numerous congenital spinal cord and anorectal malformations, as well as numerous malformation syndromes. Further, several studies have showed linkage to various chromosomal regions. However, because tethered cord can result from many different etiologies, it likely represents a multifactorial process due to a combination of genetic and environmental factors. The incidence of neural tube defects is 0.17 to 6.39 per 1000 live births worldwide, with a decline over the past 20 years due to folic acid supplementation and termination of pregnancy with prenatal diagnosis. Folic acid supplementation has had the greatest impact on reducing the incidence of myelomeningocele, which is clearly associated with tethered cord (98). The incidence and prevalence of occult spinal dysraphism is unknown (15; 97). However, due to inadequate folic acid supplementation, neural tube defects continue to occur (66).
As discussed above, trauma, via either direct blows to the back or falls on the buttocks, to an already tethered cord can precipitate neurologic deterioration. Trauma should, therefore, be avoided, and the at-risk patient should be properly educated. Also, repeated or forceful stretching of an already stressed tethered cord could cause cord dysfunction. Such activities as straight-leg raising, forced forward bending, and prolonged sitting should be avoided or done carefully (Yamada et al 1995; 120; 40; 103). Because all patients with myelomeningocele by definition have tethered cord, folic acid supplementation could at least reduce the incidence of these patients. To reduce the risk of neural tube defects, the U.S. Center for Disease Control and most countries recommend a healthy diet and folic acid supplementation of 400 ug per day periconceptionally (33). Other neural tube defect risks include mothers very young or very old in age, toxic medications, obesity, and zinc deficiency (46). In the case of known disorders such as lipomas of the conus medullaris, preventative surgery before the first year of life is recommended to prevent future neurologic deterioration from subsequent spinal cord tethering (17).
With any case of neurologic deterioration in a patient with known spinal dysraphism, one must be suspicious of potential lesions throughout the entire neuroaxis and, thus, MRI of the entire spine should be performed (51). Deterioration in a patient who has previously undergone spinal surgery should be assumed to be due to tethered cord syndrome because scar tissue can cause (or worsen preexisting) tethered cord. Chiari malformation, syringohydromyelia, and shunt malfunction are possible reversible causes of symptoms that mimic tethered cord syndrome (15). In older age groups, both lumbar spinal stenosis and lumbosacral disc disease can cause symptoms suggesting tethered cord syndrome (18). Patients that do not meet imaging criteria for tethered cord syndrome (filum thickness greater than 2 mm or conus lower than L1-L2) may still have tethered cord due to other lesions (eg, filum lipoma) and may benefit from surgery (113). However, patients with normal imaging, referred to as minimal tethered cord syndrome, represent a controversial population; certainly other causes for symptoms should be explored before performing detethering on these patients (15; 21; 95; 102; 107).
Case reports of patients presenting with tethered cord syndrome resembling plantar fasciitis and peripheral neuropathy (07), resembling Charcot-Marie-Tooth disease (100), or due to arteriovenous fistula (90; 64), have been reported in adults. Furthermore, pseudo tethered cord has been reported after lumbar puncture (74).
Cases with known dysraphic states. Any neurologic deterioration in a person with any type of known dysraphic state should be considered secondary to an underlying reversible condition. Each case should be aggressively evaluated with an eye towards identifying any potentially surgically correctable lesions such as tethered cord, syringohydromyelia, or hydrocephalus. It is not always clear whether once a lesion is found that surgical correction will reverse the symptoms. Implied in this approach is the need for a detailed assessment of the individual's baseline neurologic status and anatomy on which future potential changes can be looked for. Unfortunately, this is not always possible, and a "clinically educated" decision is the best that can be offered. A history of recent, rather than past or longstanding neurologic deficits, increases the likelihood of reversibility (15; Hainjovic and Trnka 2007; 14; 29). This is consistent with the model that reversible symptoms progress to irreversible with prolonged time between symptom onset and surgical correction. However, even patients with multiple prior surgical revisions or longstanding symptoms may still show neurologic improvement or reduction in pain with surgery (05; 36).
The conditions that are frequently associated with neurologic deterioration caused by cord tethering are myelomeningoceles and meningoceles; lipomyelomeningoceles and spinal or filum lipomas; split cord malformations; short, thickened filum terminale (greater than 2 mm in diameter); and fibrous bands that sometimes continue through the dura to bone and result in the dimpling of overlying skin. Other conditions include adhesions of the filum, conus, and nerve roots to the posterior or lateral dura; congenital dermoid cysts and sinuses; neuroenteric cysts; and sacral dysplasia, which can result in cord tethering, sometimes additionally with lumbosacral stenosis. Furthermore, if the patient undergoes spinal surgery for repair of a myelomeningocele or congenital scoliosis for example, later neurologic deterioration may be due to scarring from the surgery resulting in adhesion and tethering of cord (15; 14). All patients with myelomeningocele have tethered cord by definition, but detethering surgery is typically done only when patients begin to have symptoms of tethered cord syndrome (86; 89); therefore, these patients require frequent follow-up, usually with a multidisciplinary clinic. Some authors, however, argue that prophylactic detethering should be done at the time of the original surgical repair (92).
Baseline neurologic status is assessed with a complete neurologic history and physical exam. Particular attention should be paid to thorough strength (manual motor testing) and sensory examination and assessment of perineal function (bladder and bowel function, including cremasteric reflex and anal wink). It is often helpful to assess urologic status with urodynamic studies. Many authors recommend preoperative and postoperative urodynamic testing because it offers objective evidence of improvement after surgery and also provides a means for early detection of recurrent symptoms (125; Argrwalla et al 2007; 60; 71; 26; 122). Even patients with very mild symptoms can have abnormal urodynamics (42; 62; 26). Detrusor overactivity is considered the most common finding when evaluating urologic status in tethered cord syndrome (109). This is particularly important because tethered cord syndrome remains a clinical and anatomic diagnosis.
With the widespread availability of MRI, the evaluation of lumbosacral anatomy has become noninvasive and detailed (68; 87). MRI easily demonstrates the filum thickness and whether or not the conus ends at the proper place, or if it is caudally displaced. Placement of the conus below the L1-L2 interspace or filum thickness greater than 2 mm is consistent with tethered cord (Argrwalla et al 2007; 60). Some patients with tethered spinal cord have been demonstrated to have a normally positioned conus; however, they often have other associated abnormalities such as lipomas or fibrosis that were identifiable on MRI (113; 108; 95). As the quality of MRI improves, the sensitivity for identifying filum abnormalities will continue to improve (24).
We are left with the following conclusion: MRI imaging can easily tell us whether a spinal cord is anatomically tethered, and the gold standard for surgical decisions regarding the diagnosis of tethered cord is clinical history and exam, preferably obtained on a serial basis.
Cases that present without a known underlying dysraphic state. Unlike the patient with a known dysraphic state, who is likely to present to a multidisciplinary spina bifida clinic, some patients present with symptomatic tethered cord with no known underlying (or occult) dysraphic state. These patients can present in many settings, not least of which could be a neurologist's office. Usually, these patients develop symptoms during childhood, but they can become symptomatic at an earlier age or during adolescence or adult life. Neurologic dysfunction is often slowly progressive. Symptoms and signs can appear stable over serial exams, sometimes for years. However, even within this seemingly stable setting, minor neurologic deficits may progress significantly and suddenly following minor traumatic events (77; Iskandar et al 1998; 36). Neurologic dysfunction manifests itself by lower extremity paresis and deformity, spinal deformity, sensory loss (including trophic ulceration), and changes in bladder and bowel function (23; 35; 58; 02; 60). Dysfunctional bladder may be the only presenting manifestation in adults (55), although this is not universally accepted (112; 21; 95). Although urinary incontinence in children has not been shown to be predictive of occult spinal dysraphism (71), children with occult tethered cord tend to present more often with urinary symptoms, in contrast to adults who present more often with pain complaints (107). Orthopedic deformities include progressive scoliosis and pes cavus, varus, or valgus deformities of the foot, or leg-length discrepancies (02; 15; 60; 40; 31). Most often, these deformities are unilateral, and progressive atrophy of the lower extremities can be seen. Also, patients with anorectal and urogenital malformations have a higher incidence of tethered cord syndrome (114; 15; 40; 75). Unless a clear spinal dysraphism is identified, however, these children should be treated medically rather than surgically (19).
Workup of these individuals may include the following (02; 15; 60; 40):
State of the art management of tethered cord syndrome includes early identification (particularly in high risk individuals with spinal dysraphism), appropriate decisions on who to operate on, and good postoperative follow-up. Although the decision to operate is easy in symptomatic patients with spinal dysraphism, it is not always clear when to operate in asymptomatic patients. In a review Yaltirik and colleagues proposed that asymptomatic patients with non-spina bifida associated tethered cord syndrome and concomitant scoliosis may benefit from fusion with osteotomies without untethering and should be followed conservatively as scoliosis patients (118).
In terms of the surgical procedure, primary attention is paid to releasing the stretched spinal cord. However, clinicopathologic correlations have shown that not all of the actual etiology for tethering can be noted preoperatively (83; 119; 117). The point to emphasize is the importance of having a neurosurgeon with operative experience with tethered cord syndrome involved in managing the case. Most authors or neurosurgeons now believe that infants with lipomeningocele and a tethered cord should be operated on in the first few months of life before they become symptomatic. Certainly, symptomatic children should be operated on, preferably when symptoms are absent or mild (Argawalla et al 2007; 15; 60; 14; 106). Although surgery in adults may involve greater risk of neurologic injury than in children (especially in the elderly), and benefit may be reduced, especially if the symptoms have been longstanding, it is a low-risk procedure with significant benefit in the right patients (29; 73). Because neurologic deficits are generally irreversible, early surgery is recommended (47; Huttman et al 2001; 58; 37; 29). Minimally invasive approaches have been used, and outcome data appear similar to the traditional open approach (78). Spinal column shortening has been proposed as a safer alternative to direct spinal cord untethering with favorable outcomes and fewer complications but further research is required to establish efficacy (04). Intraoperative monitoring is also frequently used to help reduce the incidence of neurologic injury, and it will likely become the standard of care (Lew et al 2006; Argawalla et al 2007; 60; 79; 88).
For postoperative care, bed rest in the prone position post untethering is recommended for a duration of 10 days. Prophylactic acetazolamide is often administered to reduce CSF production and prevent leakage in untethering surgeries, but has been shown to be unnecessary and possibly harmful due to the side effects (96).
Certainly, improvement in urodynamics are important in deciding which patients should undergo surgery, and there have been efforts in predicting which patients are more likely to improve (26), as well as attempts to understand the threshold for surgery in patients with occult tethered cord and urinary symptoms (122; 06). This is especially important, given reports of spontaneous improvement in urodynamics in children with congenital spinal lipomas, a known cause of tethered cord (09). This also correlated with data that filum terminale lipomas may actually spontaneously disappear, and if found in asymptomatic patients should be considered incidental findings according to the authors (16).
For those patients with recurrent tethered cord, pain management is of concern when further untetherings pose unlikely improvement and increased risk. Neuromodulation has been suggested as an alternative therapeutic option to achieve pain relief. Implantation of a dorsal spinal cord stimulator can give relief from neuropathic pain secondary to recurrent tethered spinal cord (110; 72).
Neurologic outcome after cord untethering can be good. Adults may not improve as much as children (77), although the more important factor may be length of symptoms. Surgery during the asymptomatic period or when symptoms are mild may result in better outcomes (58; Argawalla et al 2007; Haijnovic and Trnka 2007; 60; 14; 40). However, even late release can result in improvement for some patients (36). In adults, pain symptoms improve the most following surgery, although the majority of patients also have improvement or stabilization in motor strength and bladder function (77; 45; 58; 29). In children, pain is a less common symptom, but most patients have stabilization or improvement in strength and bladder function (Argawalla et al 2007; 15; Lew and Kothbauer et al 2007; 14; 63). Grading systems to assess the degree of intraoperative untethering have been published (53), along with scales to rate clinical symptoms pre-and post-untethering (46) and attempts to better classify various subtypes of tethering (83). Outcome depends on the pathology and severity of symptoms. A retrospective study has shown those with diastematomyelia and thickened filum presenting with tethered spinal cord have a better outcome than those with myelomeningocele or meningocele (46). Several studies have addressed the frequent need for operative revision after index tethered-cord release (08; 112; 58; 05; 62; 97; 76).
A study demonstrated features on MRI following tethered cord release that may be useful in monitoring for change and detecting early recurrence of retethering (52). Another study reported improvement in intraoperative transcranial electrical motor-evoked potentials, although there was no correlation with long-term outcomes (81).
An overview of tethered cord surgeries in the United States demonstrated mortality rate, complication rate, and length of stay as 0.0005%, 9.48%, and 5.6 days, respectively (56). Complications from surgery can include hemorrhage/hematoma; infections, including meningitis; deep venous thrombosis or pulmonary embolism; neurologic decline/injury; retethering; and CSF leak (Argawalla et al 2007; 60).
The most common complication of tethered cord syndrome in pregnancy is urinary tract infection. In 10% of pregnancies hydronephrosis, intestinal obstruction, and renal complication occur due to the presence of the fetus. Caesarean section is often conducted due to pelvic bony abnormalities, but vaginal birth may be performed as well. There is an increased risk for newborns to have neural tube deficits (4% to 7%) and 4.0 mg of folate is recommended every day to prevent neural tube deficits (67).
Symptoms of tethered cord syndrome can become worse after childbirth in the lithotomy position (77). Therefore, care needs to be taken with a patient with known spinal dysraphism.
Unless surgery is indicated shortly after birth, MRI should be delayed until at least 3 months of age so that sedation may be utilized for optimal imaging in infants when evaluating patients with occult spinal dysraphism (109).
A case report exists documenting the occurrence of a spinal hematoma following spinal anesthesia in a patient with spina bifida occulta (116).
In adults with tethered spinal cord the conus medullaris ends at a lower level, even extending to L5-S1. Spinal anesthesia administered through a dural puncture should be avoided due to the possibility for serious injury to the spinal cord. Secondary hematoma can lead to a compression injury and possibly irreversible damage (61).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Justine Ker BA
Justine Ker of Tulane University School of Medicine has no relevant financial relationships to disclose.
See ProfileStephen L Nelson Jr MD PhD
Dr. Nelson of Tulane University School of Medicine received honorariums from BioMarin and LivaNova for speaking engagements.
See Profile
Michael V Johnston MD†
Dr. Johnston of Johns Hopkins University School of Medicine had no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jan. 20, 2025
Sleep Disorders
Jan. 18, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuromuscular Disorders
Dec. 29, 2024