



Stroke & Vascular Disorders
Neoplastic and infectious aneurysms
Dec. 29, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The thalamus is involved in about one of every six nontraumatic intracerebral hemorrhages. Hemisensory loss, decreased level of consciousness, and hemiparesis are the usual manifestations of thalamic hemorrhage; nevertheless, depending on hematoma size and selective or global involvement of the different thalamic nuclei and neighboring structures, virtually any clinical neurologic finding may be seen in the setting of thalamic hemorrhages. In this article, the authors thoroughly address the broad clinical spectrum in terms of the intrathalamic location of both large and small bleedings. They also summarize the epidemiology, etiology, diagnostic workup, prognosis, and latest medical and surgical treatment options for thalamic hemorrhages.
|
• Thalamic hemorrhage is the second most common location of nontraumatic intracerebral hemorrhage, accounting for 10% to 15% of all hemorrhages. | |
|
• The clinical picture depends entirely on hematoma size, selective or global involvement of the different thalamic nuclei, and the involvement of neighboring structures. | |
|
• Arterial hypertension is the most common etiology, regardless of topographic location and hematoma size. | |
|
• Treatment is, for the most part, supportive medical care, including timely blood pressure control. |
During the early decades of the twentieth century, French neurologists (particularly Dejerine, Foix, and their colleagues) made important contributions concerning the vascular anatomy and pathology of the thalamus, including the description of clinical manifestations resulting from lesions at different vascular territories (21; 31). At the time, the so-called “thalamic vascular syndrome” was defined as a persistent contralateral hemianesthesia affecting both superficial and deep sensory modalities, a transient mild hemiparesis, and hemiataxia, with possible subsequent development of intolerable pain and choreoathetotic movements in the affected limbs (21). Some years after the initial description of the thalamic syndrome, Lhermitte and Baudouin provided some clinical findings that helped to discriminate between ischemic and hemorrhagic lesions of the thalamus (55).
Traditionally, thalamic hemorrhages, and those located in the caudate and putamen, were considered basal ganglionic hemorrhages. In 1959, however, CM Fisher pointed out pupillary and oculomotor function abnormalities observed in 13 patients with thalamic hemorrhages out of 102 patients with pathologically confirmed intracerebral hemorrhage. Fisher also found greater sensory deficit than motor dysfunction, as well as speech or behavioral manifestations resulting from the involvement of the left or right thalamus, respectively (29).
The introduction of the CT scan 40 years ago and, more recently, of brain MRI technology has made it possible to identify small hematomas, describe clinical subtypes of thalamic hemorrhages, and improve insight into the function of the different thalamic nuclear regions.
Thalamic hematoma characteristically occurs during activity; onset during sleep or rest is unusual (93; 49). Once the neurologic symptoms begin, they most often progress gradually over a period of minutes or, less often, hours (49). Though not common, transient clinical signs resembling transient ischemic attacks may occur in intracerebral hemorrhages. Thus, in a cohort of 17 patients with intraparenchymal hematomas and transient signs, two patients (both over 60 years of age) had small spontaneous thalamic hematomas (7.7 ml and 21 ml) with mild neurologic deficits (respective NIHSS scores 2 and 3) lasting 30 minutes and 5 hours, respectively (48).
Clinical manifestations of thalamic hemorrhages are broad. Their occurrence depends entirely on hematoma size, selective or global involvement of the different thalamic nuclei, and the involvement of neighboring structures. Hematomas have been classified based on topographical locations, size, and vascular territories (42; 46; 93; 16).
Posterolateral hematomas. Fifty percent of all thalamic hematomas are located in the posterolateral region (46; 49; 16). Sensory disturbances are commonly seen in large and small posterolateral hematomas due to the involvement of both the ventral posteromedial and the ventral posterolateral nuclei. Pure sensory stroke suggestive of, but not specific for, thalamic stroke has been observed occasionally in posterolateral thalamic hemorrhage (78). Spinothalamic, lemniscal, and discriminative modalities of sensation can be affected in different patterns. The distribution of sensory loss is variable, although hemibody hypesthesia is often found (42). In some very rare cases, acute isolated numbness restricted to the contralateral tip of the tongue and the lower lip may result from a small thalamic hematoma involving the medial part of the posterior ventromedial thalamic nucleus (88). Large and small hemorrhages may involve the adjacent posterior limb of the internal capsule, resulting in sensory loss associated with variable degrees of contralateral hemiparesis (49). Sensory ataxic hemiparesis may also occur but has been seen less often. The level of consciousness depends on hematoma size; stupor or coma occurs with large hematomas, whereas alertness is preserved with small hematomas (16).
An extensive spectrum of oculomotor disturbances is associated more frequently with large posterolateral hematomas. The most common abnormalities include horizontal-gaze deviation toward the lesion, upward gaze palsy, combined upgaze and downgaze palsy, and skew ocular deviation (42; 46). Contralateral gaze preference, ipsilateral Horner syndrome, horizontal gaze palsy, and convergence spasm (peering at the tip of the nose) may also occur, although less often (46; 49; 16). Interruption of corticofugal fibers mediating saccadic and smooth-pursuit eye movements at the level of posterior thalamus is thought to be responsible for hypometric saccades away from the hematoma, ipsilateral defective smooth-pursuit movements, and ipsilateral-reduced optokinetic nystagmus (42). Hemianopia and quadrantanopia are rare (42; 49). Aphasia (global, transcortical, or Broca type) or mutism in dominant hemisphere lesions, hemineglect, poor drawing, and poor copying in right-side thalamic bleeding are not frequent, although when present, they are mostly related with large hematomas (42; 46; 49; 16). Though a rather uncommon occurrence, agraphia may be the noticeable clinical finding in left-sided posterolateral hematomas, most likely due to the disruption of both thalamocortical and cortico-thalamocortical loops caused by reduced blood flow in the left cerebral cortex and thalamus as a result of the bleeding (77).
Involuntary movements, including myoclonus, asterixis, dystonia, chorea, and tremor, may be seen. These may occur in isolation or, more often, in a mixed pattern, anywhere from weeks to years after posterolateral hemorrhage (47). Damage of the ventroposterior lateral and ventroposterior medial nuclei and, to a lesser extent, of the posterior limb of the internal capsule is the anatomical basis of these involuntary movements (47).
Pusher syndrome (contraversive pushing away from nonparetic side, leading to a loss of postural balance) occurs in approximately one third of thalamic strokes and has often been associated with large posterior hematomas (44). The posterior thalamus seems to influence pathways for sensing gravity orientation.
Harlequin syndrome (intermittent and transient contralateral facial flushing with relative ipsilateral facial pallor) coexisting with Horner syndrome has been reported in a patient aged 53 years with a large posterolateral thalamic hematoma and intraventricular extension (68).
Dorsal hematomas. The frequency of dorsal hematomas is variable. A low frequency of 8% was found in a series of small hematomas (less than 2 cm in mean diameter), whereas series including both small and large dorsal hematomas have reported a frequency ranging between 15% and 28% (46; 49; 16). Consciousness is usually preserved. Ocular abnormalities are often absent, but when present, Horner syndrome and upward gaze palsy have frequently been noticed. Large left-side hematomas may produce aphasia (global or transcortical type), whereas corresponding right-side lesions have been associated with contralateral anosognosia (49). Mild or moderate contralateral hemiparesis may occur due to the extension of bleeding over the corona radiata. Sometimes, the only clinical finding is pure motor stroke or sensorimotor deficit. In either case, the disorder may be confused with a lacunar infarct. Inability to stand (thalamic astasia) despite normal motor power and alertness is found in only a few cases, with improvement occurring between 1 and 5 weeks after appearance (64).
Posterior-dorsal hematomas. Small hemorrhages may be confined to the far posterior area of the thalamus (posterior-dorsal hematomas), although they are rarely observed. As with dorsal hematomas, consciousness usually remains unaffected. Sensory and motor deficits are often transient and minimal or absent altogether. The pulvinar nucleus and the medial geniculate body are often affected. Therefore, transient constructional apraxia, topographic memory disturbance, and contralesional auditive extinction have been found in nondominant lesions, whereas left-side hematomas may be associated with fluent aphasia (46). A small hemorrhage involving the lateral geniculate body produced a transient horizontal nystagmus (spontaneous and evoked gaze) and a contralateral homonymous hemianopia (38).
Medial hematomas. Medial hematomas comprise one sixth of all thalamic hemorrhages (49; 16; 97). Early in the course, oculomotor abnormalities, such as paresis of the vertical gaze, Horner syndrome, and conjugate-gaze deviation opposite to the hematoma (the so-called “wrong way eyes”), are common in large hematomas but not in small ones (49; 16). Motor and sensory deficits are mild and often transient in small hematomas restricted to the medial thalamus. Disturbances of consciousness are often seen in medial hematomas and may fluctuate from confusion to stupor, depending on hematoma size. These hematomas nearly always involve the intralaminar nuclei (central lateral, paracentral, and centromedian), thus, hindering projections to the midbrain reticular formation. Moreover, large medial hematomas spread to the midbrain, also contributing to impairment of the awake state (16). In some instances, the onset of hematoma with headache, vomiting, nuchal rigidity, and impairment of consciousness due to ventricular drainage into the third ventricle may be confused with a subarachnoid hemorrhage. Later in the course, amnesic syndrome, personality changes, and abulia may be the notable complaints resulting from damage to the medial thalamus’ connections to the limbic system and prefrontal cortex (46).
Anterolateral hematomas. Rates of anterolateral hemorrhage vary between 5% and 20% (46; 49; 16). Ophthalmological examination is usually unremarkable in small hemorrhages, whereas large ones impair vertical gaze (49). Hemiparesis occurrence is related to involvement of the anterior portion of the posterior limb of the internal capsule. Sensory deficits are mild and transient. Confusion in the acute stage is often observed, and verbal-memory deficit, inattention, apathy, and abulia may be early and long-lasting prominent clinical findings (46; 16). These symptoms are due to the damage of nuclear structures projecting to the frontal lobe. In dominant-side lesions, mutism and aphasia (global or transcortical) are less often reported, as are neglect, anosognosia, and visual and tactile extinction in right-side hematomas (49).
Global or large hematomas. Finally, approximately 10% to 18% of all thalamic hematomas are of the global type (16; 97). Most commonly observed are nonspecific symptoms such as headache, vomiting, and a decreased level of consciousness at presentation, results of increased intracranial pressure and involvement of the brainstem reticular activating system. Ophthalmological examination may reveal a loss of upward gaze and, less frequently, combined upgaze and downgaze paresis, pure downgaze paresis, and skew deviation. Horizontal gaze preference toward the hematoma and, more rarely, “wrong-way eyes,” has also been noticed (71). Usually, both pupils are miotic and react poorly to light; this is due to involvement of the rostral sympathetic pathway and damage to the pupillary reflex arc running to the third nerve nuclei in the midbrain. At times, the ipsilateral miotic pupil is smaller than its counterpart. Selective miosis on the side of hematoma may occur, although rarely. Retractory nystagmus and convergence disorders may also be found when hematomas spill out to the thalamus, affecting the midbrain. Severe contralateral sensory and motor deficits are nearly always seen (16). Language disorders and hemineglect may also occur (93).
The literature shows that approximately 9% to 32% of patients with thalamic hematoma die (49; 16; 43; 87; 97). The highest mortality rates have occurred in patients with global (82%) and medial (61%) thalamic hemorrhages, whereas the lowest (6%) has been observed in patients with posterolateral hematomas (97).
In general, outcome is associated with hemorrhage size (49). This is true whether hemorrhage size is estimated by CT (67% mortality for hemorrhages greater than 10 cm3 in volume vs. 8% for those less than 10 cm3) or by clinical signs (50). In particular, the level of consciousness on admission predicts outcome: 60% of patients who are stuporous or comatose on admission die compared to only 7% of those who are alert or drowsy (93). Moreover, poor outcome 3 months after thalamic hemorrhage is related to stroke severity per the Canadian Neurological Scale (87). Early hematoma growth has been considered a marker of poor prognosis. In fact, significant hematoma expansion has been observed to occur in approximately 30% of patients with spontaneous intracerebral hematoma in the first 24 hours after onset. For each 10% hematoma enlargement, a consequent 5% increase in hazard of death and a 15% increase in poor functional outcome were noted in a pooled meta-analysis of 218 patients with spontaneous intracerebral hemorrhage (20).
In the ATACH-2 trial, 87% of 1000 patients had spontaneous deep hemorrhages; complete neuroimaging data were available for 336 and 444 patients with thalamic and basal ganglia hemorrhages, respectively (53). Intensive blood pressure reduction (target systolic blood pressure 110 to 139 mm Hg within 2 hours) was randomly assigned to 405 patients with deep hemorrhages mean aged 62 years, 83% of whom had had previous arterial hypertension, whereas standard treatment (target systolic blood pressure 140 to 179 mm Hg) was allocated to 375 patients with the same characteristics, 76.8% of whom had had previous arterial hypertension. Compared to standard treatment, intensive blood pressure reduction decreased hematoma expansion risk, specifically in basal ganglia, but not thalamic hemorrhages, regardless of the criterion used to define hematoma growth (either an increase greater than 33% in hematoma volume between baseline and 24-hour CT scans or an absolute increase of greater than 6 mL in hematoma volume) (53).
In an exploratory study, deep spontaneous intracerebral hemorrhage had a thalamic location in 54 out of 138 patients with no previous disability (75). The mean age of these patients was 64 years, 90% (49) patients had a previous history of arterial hypertension, the median hematoma volume was 13.8 cm3, and intraventricular hemorrhage occurred in nearly two thirds of cases. The optimal hematoma volume cut-point to predict less than or equal to 2 on the modified Rankin Scale at 3 months was 4.6 cm3 (sensitivity: 83.8%; specificity: 70.6%; area under the receiver operative characteristic curve: 0.88%). When a better outcome was defined as less than or equal to 3 on the modified Rankin Scale, the optimal hematoma volume cut-point was 5.5 cm3 (sensitivity: 93%; specificity: 77%; area under the receiver operative characteristic curve: 0.90). Unfortunately, the severity of intraventricular hemorrhage and the need for ventricular drainage were not included in the analysis, which may have biased the results (75).
The relation between the anatomical location of small primary intracerebral hemorrhages (less than 30 mL) and functional outcome at 30 and 180 days after stroke onset has been assessed in 466 patients enrolled in the CLEAR-IVH (Clot Lysis: Evaluating Accelerated Resolution of Intraventricular Hemorrhage) III trial (25). All patients included in this trial had a third or fourth ventricle obstruction. In this cohort with a mean age of 58 years, 332 patients (71%) had a thalamic hemorrhage; the mean Glasgow Coma Scale score at admission was 10 points; mean hematoma volume was 11.5 mL; and mean intraventricular hemorrhage volume was 24.1 mL. Thalamic hemorrhage was significantly associated with increased mortality and poor functional outcome at 30 and 180 days as measured by the NIHSS scale, modified Rankin Scale, and Barthel Index. Compared with patients with nonthalamic hemorrhage, patients with thalamic hemorrhage had a 4.8- and 2.8-fold higher death rate at 30 and 180 days after stroke onset, respectively (25).
In a retrospective series of 101 patients with thalamic hemorrhages, ventricular drainage occurred more often in global (94%) and medial (61%) bleedings and less frequently in anterolateral hematomas (97). Although controversial, the bulk of evidence suggests that intraventricular extension does seem to be associated with higher mortality (93; 49). The mechanism by which intraventricular extension exerts its negative effect is not clear. Although intraventricular hemorrhage is associated with increased size and with hydrocephalus, both of which are poor prognostic signs, intraventricular extension is an independent risk factor for death (99).
Dysphagia is not uncommon in patients with acute thalamic hemorrhage. In 113 patients (mean age of 68) with acute thalamic hemorrhage, a bedside swallowing assessment (repetitive saliva swallowing test and modified water swallowing test) was carried out 2 days after hemorrhage onset. The hematoma was restricted to the thalamus in only 16% of these patients, whereas it also involved the adjacent internal capsule (70%) or the midbrain (14%) in the rest of the patients. At initial evaluation, 55% of the 113 patients had dysphagia; compared to patients without swallowing abnormalities, these patients were older, and they had a large median volume of hematoma, more intraventricular extension, a lower mean Canadian Neurological Scale score, more aphasia and neglect, a longer length of stay, and a lower rate of oral intake at hospital discharge (62).
Functional recovery in smaller hemorrhages depends on the site and size of hemorrhage (50). In recovery of activities of daily living, dorsal and anterolateral hemorrhages have the best prognosis, whereas more than one third of patients with posterolateral hemorrhages remain dependent (16). Medial hemorrhages also render a small percentage of patients dependent because of behavioral and cognitive deficits (46).
Hydrocephalus is not an infrequent complication of thalamic hemorrhage, occurring in about 30%. In most cases, it is probably due to the presence of subarachnoid blood impairing cerebrospinal fluid resorption.
Hypertensive thalamic hemorrhage has been thought to occur once in a lifetime. Repeated ipsilateral or contralateral hypertensive thalamic hemorrhage is uncommon; rebleeding may occur at an interval of months to years after the initial thalamic event. Primary hemorrhages that occur simultaneously in both thalami are uncommon. In a series of 105 patients (mostly from Asian background) with primary multiple simultaneous intracerebral hemorrhages identified in the literature from 1950 to 2013, 18% to 19% of patients with an average age of 64, of which 13 were male, had hemorrhages simultaneously in both thalami. The mortality rate in these patients was 31% (six patients), whereas 47% (nine patients) had a poor functional prognosis, and only 21% (four patients) had a favorable outcome (51).
The thalamic pain syndrome of troubling dysesthesias and spontaneous pain over the contralateral side occurs after a latency of days to weeks after the initial ictus and is often resistant to analgesics. It complicates thalamic hemorrhage less frequently (less than 20%) than infarction, suggesting that a specific, partial destruction of the posterior lateral region is required for its genesis (46).
Acquired complex multimodal perceptual (sound-color, grapheme-taste, and sound-tactile) synesthesias (the confusion of different sensory modalities) were reported in a 45-year-old hypertensive patient 9 months after a thalamic hematoma involving the pulvinar, lateral posterior, and ventral posterior lateral nuclei of the thalamus (32). Two hypotheses have been proposed to explain this exceedingly rare complication after a thalamic hematoma: an anomalous cortical connection or an aberrant activation of anomalous sensory regions in response to stimulation.
The “black hole” sign, an early imaging marker predicting hematoma expansion (see below) on noncontrast brain CT at admission, may also predict poor outcome. The black hole sign as outcome predictor in hemorrhagic stroke was assessed in a study involving 225 patients with intracerebral hemorrhage (mean age: 60 years; median admission hematoma volume: 13 mL; 25% of patients had thalamic hemorrhage), most of whom underwent medical management, whereas only 9% had surgical treatment (59). This sign was observed on noncontrast CT scan within 6 hours after the onset of symptoms in 32 patients (14%). Among patients with thalamic hemorrhage, the sign was found in 10% (6 of 57) patients. Patients with positive black hole sign had a significantly larger baseline volume hematoma, a significantly lower baseline Glasgow Coma Score, and significantly more midline shift at admission than patients with no black hole sign.
Regarding outcome, patients with black hole sign had significant differences in terms of in-hospital mortality (15% vs. 4%), mortality at 3 months (50% vs. 14%), and poor functional outcome defined as at least 4 on the modified Rankin scale (84% vs. 32%) from patients without this imaging finding. After adjusting for potential confounders, black hole sign increased the probability of poor outcome eight-fold. In patients with thalamic hemorrhage, the presence of this sign increased the probability of a worse outcome nearly 4-fold compared with patients without the sign (59).
Vignette 1. On awakening, a 51-year-old right-handed Hispanic man suddenly experienced severe headache and numbness on the left facial side, followed several minutes later by numbness in the left arm and left leg. Afterward, he was unable to walk without assistance. The patient’s medical history included untreated arterial hypertension 3 months before this admission and cigarette use (around 10 cigarettes per day) over 30 years. He denied alcohol or substance abuse. His bed partner complained of his loud nocturnal snoring, but no apneas or excessive daytime sleepiness had been previously observed.
On examination, the patient’s body mass index was 31.24 kg/m2, and his blood pressure was 180/100 mm Hg. No cardiac murmurs were audible, and he was drowsy. Both eyes showed downward deviation, with an additional inward deviation of the right eye.
An upward gaze palsy on voluntary saccadic and pursuit eye movements was observed. The pupils were equal in size (1.5 mm in diameter) and poorly reactive to light. Convergence was also impaired. There was no neglect and hemianopia by confrontation. A left sensory loss involving light touch, pain, temperature, position, and vibration was found. A left flaccid hemiparesis involving the arm and leg was also noticed. Kernig and Brudzinski signs were present.
Blood cell count, routine serum chemistries (including lipid profile), and electrolytes were normal. Prothrombin time (PT), activated partial thromboplastin time (APTT), and fibrinogen and platelet counts were also normal. An electrocardiogram and a transthoracic echocardiogram were normal. A nonenhanced CT of the patient’s brain showed a large right thalamic hemorrhage extending into the posterior limb of the internal capsule, putamen, and upper midbrain. Thalamic bleeding was associated with hydrocephalus, and the blood extended to the third ventricle and the lateral ventricles’ occipital horns.
The patient received only supportive care. An angiotensin-converting enzyme inhibitor was introduced on the fourth day after the onset of symptoms.
Vignette 2. While doing housework, a 30-year-old, right-handed Hispanic woman suddenly developed an acute throbbing pain in the frontal right side that radiated to the ipsilateral occipital region. Approximately 5 minutes later, she experienced paresthesias in the distal part of her left arm and then in the left leg. She had been healthy, although slightly overweight (BMI 26.56 kg/m2). She was free of any significant medical history and did not take any medication or use tobacco, alcohol, or illicit drugs. On arrival in the emergency room, her blood pressure was 110/60 mm Hg, and cardiac rhythm was regular; she was fully consciousness, and no speech disturbances were noted. A slight upward paresis and a right Horner syndrome were found. Visual fields and convergence were normal. Perception of pinprick, light touch, vibration, and position sense were decreased over the left hemibody, and hemiataxia involving mainly the left upper limb was also seen. No motor deficit was noted. On the third hospital day, she complained of symptoms suggestive of binge eating disorder, which eventually subsided 1 week later.
Blood cell count, routine serum chemistry, coagulation screening, and transthoracic echocardiography were all normal. No toxicology screen was done. An acute right anterior thalamic hemorrhage extending to the right upper midbrain was found on CT scan and brain MRI.
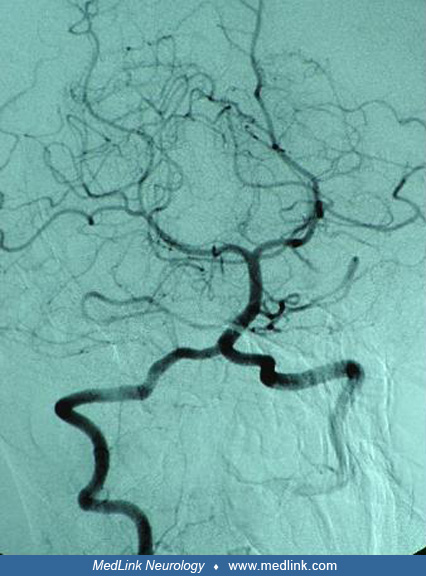
On the second hospital day, a digital subtraction angiography of the posterior circulation revealed no abnormality.
A second brain MRI performed 4 months after the acute thalamic hemorrhage disclosed a cavernous malformation in the right midbrain peduncle extending to the ipsilateral thalamus.
The most common underlying etiology, regardless of topographic location and hematoma size, is longstanding arterial hypertension, as may be seen in more than 80% of patients (93; 49; 16). Although rare, acute rises in blood pressure have also been documented in certain instances of thalamic hemorrhage, such as in autonomic dysreflexia (uncontrolled sympathetic output in patients with a chronic spinal cord injury above the T6 spinal level) (24).
Arteriovenous malformations involving the thalamus account for 11% of all arteriovenous malformations and approximately half of the deep arteriovenous malformations (92). These deep lesions with central drainage into either the basal vein of Rosenthal or the internal cerebral vein are more prone to bleeding (85). Thus, thalamic hemorrhage may occur as the initial clinical presentation of arteriovenous malformations or rebleeding (85). Intraparenchymal hemorrhage is the second most common clinical presentation of cavernous malformations. Thalamic cavernous angiomas are not common and are seldom found as etiology.
Intracranial hemorrhage is a well-established major complication of anticoagulant and fibrinolytic agents. However, direct oral anticoagulants and warfarin-associated thalamic hemorrhage are not commonly found as etiology (34). Bleeding during warfarin therapy may occur either with high levels of anticoagulation or when the international normalized ratio is within the therapeutic range (93). Large, deep hemispheric hematomas also involving the thalamus have been found in cases of intraarterial thrombolysis (45). A type 1 heterozygous protein C deficiency was complicated with a left thalamic hematoma without associated cerebral venous thrombosis or venous hemorrhagic infarction (65).
Hematoma in the thalamus subsequent to rupture of an aneurysm arising from P1 segment of the posterior cerebral artery has been reported. A CT scan taken 48 hours after bleeding showed a thalamic hematoma and a rapid disappearance of blood in the subarachnoid space. Brain MRI demonstrated a close relationship between the thalamic hematoma and the dome of the aneurysm (18). Another case of thalamic hemorrhage, involving the pulvinar and initially thought to be due to chronic arterial hypertension, was found on further imaging a month later to be the result of a lateral posterior choroidal aneurysm, which was successfully treated by surgical resection (33).
Thalamic hemorrhage is an uncommon complication after internal carotid endarterectomy or stenting (14). In rare cases, thalamic hemorrhage may be a complication of stereotactic removal of intraventricular tumors (73) or the initial presentation of a previously unknown anaplastic astrocytoma (56). Stereotactic thalamotomy for movement disorders can be followed by perioperative small thalamic hematomas (95); more rarely, delayed thalamic hemorrhage has been reported after deep-brain stimulation (100).
Other less common etiologies include polyarteritis nodosa (23), pseudoxanthoma elasticum as a first manifestation (10), Sturge-Weber syndrome (76), chronic alcoholism (16), drug abuse (including cocaine, amphetamines and sympathomimetics) (13), preeclampsia (89), multiple honeybee stings (82), Plasmodium vivax malaria in the absence of thrombocytopenia and disseminated intravascular coagulation (84), and cerebral autosomal-dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) (54). Although uncommon, single or recurrent thalamic hematomas may also occur (with or without concomitant intraventricular hemorrhages) in the setting of moyamoya disease, particularly among young Asian and non-Caucasian adults (83).
A patient with a history of untreated mild arterial hypertension was reported to have developed a thalamic hematoma 1 hour after taking a single dose of 50 mg of sildenafil for the first time in his life. In this report, it was suggested that sildenafil might have caused cerebral vasodilation, leading to an increase in blood flow in the brain and raising the risk of intracranial bleeding (01). Despite laboratory and neuroimaging investigations, an etiology cannot be identified in 10% to 30% of patients with thalamic hemorrhage (16). High-serum alpha-tocopherol levels were found within the first few hours of thalamic hemorrhage in two older patients, both of whom experienced mild blood pressure elevation during hospitalization and had a history of high daily vitamin E supplementation (52). Neither patient used antithrombotic medications, and hemorrhage etiology could not be determined despite investigations. It has been hypothesized that vitamin E may interfere with blood coagulation by hindering factor IX activity or acting as a vitamin K antagonist. Moreover, vitamin E may decrease platelet aggregation via a protein kinase C-dependent mechanism.
Coronavirus disease (COVID-19), the severe acute respiratory syndrome caused by coronavirus type 2 (SARS-CoV-2), has rapidly spread worldwide since December 2019. Ischemic or hemorrhagic stroke is increasingly recognized in association with COVID-19. Intracerebral hemorrhage in the setting of confirmed COVID-19 infection has been reported in healthy young individuals and in patients having preexisting arterial hypertension or while on anticoagulation. Two patients with thalamic hemorrhage (a previously healthy young individual and an older patient with vascular risk factors) had COVID-19 infection confirmed by reverse transcription-polymerase chain reaction (RT-PCR) assay (35; 72). SARS-CoV-2 has neurotrophic properties, but the underlying mechanism in COVID-19-induced intracerebral hemorrhage is still unknown. Virus-induced endothelial injury, angiotensin-converting enzyme receptor dysfunction, hyperfibrinolysis, and disseminated intravascular coagulation in the setting of COVID-19 infection have been proposed as possible intracerebral hemorrhage mechanisms (72; 63). The role of preexisting arterial hypertension, cerebral amyloid angiopathy, and anticoagulation in cerebral hemorrhage associated with COVID-19 must be clearly defined.
Each thalamus is a 4 cm oval-shaped structure that lies adjacent to the third ventricle. It is comprised mainly of gray matter and serves as a relay station for most central neural systems, each compartmentalized into a nerve nucleus. There are four important sources of blood supply for the thalamus: the thalamoperforants, which arise from the basilar artery bifurcation and supply the medial aspect of the thalamus; the thalamogeniculates, which supply the posterolateral aspect; the posterior choroidal artery, which supplies the dorsal portion; and the tuberothalamic artery, which arises from the posterior communicating artery and supplies the anterior portion. The compartmentalization of neurons into nuclei gives rise to different clinical syndromes when different regions of the thalamus, supplied by different arterial systems, are affected.
Surges in arterial pressure, weakened vessel wall structure, and impaired hemostasis contribute to arterial or venous rupture and subsequent hemorrhage. Of these, vascular structural pathology appears to be most important. Hypertensive vasculopathy, the most frequent cause of thalamic hemorrhage, is a degenerative change in the wall of small arteries characterized by loss of muscular components, hyaline and fibrinoid change, and microaneurysm formation (30). As the thalamus is supplied almost exclusively by these small arteries, it is especially vulnerable to the pathologic consequences of hypertensive vasculopathy, including hemorrhage. Other causes of weakened arterial wall structure include arteriovenous malformations in which high venous pressure and congenitally abnormal vessel wall structure lead to an increased risk of cerebral hemorrhage. Sympathomimetic drugs, amphetamines, cannabis, and cocaine can produce intracerebral bleeding by inducing vasculitis-like abnormalities or the rupture of previously occult arteriovenous malformation, or it can be associated with hypertensive crisis (13). Abnormal vessel wall structure in the neovascularity of cerebral neoplasms leads to their propensity to hemorrhage (41).
Active bleeding is usually completed within 20 hours after onset. Blood infiltrates along white matter tracts and compresses the gray matter, producing an area of hypoperfusion surrounding the hematoma, which may represent either a true perihemorrhagic ischemia or a zone of reactive oligemia due to reduced metabolic demand (86). Because of its close proximity to the third ventricle, intraventricular extension is common in thalamic hemorrhage, occurring in 30% to 60% of patients (93; 49). Brain edema after intracerebral hemorrhage first appears in 7 to 8 hours and progresses over the next 1 to 5 days. Interaction between thrombin and vascular endothelial growth factor, which results in altered vascular permeability, is thought to be the key step in brain edema development. Resorption of blood takes place over weeks to months, leaving a cavity lined by hemosiderin-laden macrophages and surrounded by ischemic necrotic tissue.
Thalamic hemorrhages make up 10% to 15% of all intracerebral hemorrhages. However, clinical series of thalamic hemorrhages based on Turkish and Japanese populations have showed higher figures (49; 43). Thalamic hemorrhages occur more frequently in people 60 years of age and older (42; 46; 93; 16; 87). Most CT-based series of thalamic hemorrhages are small, which has hindered establishing clear gender predominance. However, females prevailed in two clinical series of thalamic hemorrhages (49; 16). Restricted thalamic hemorrhages occurred more frequently than thalamic infarcts in nonwhites (93).
Age, male sex, and arterial hypertension are well-established risk factors for intracerebral hemorrhage (05). Available evidence suggests that blood pressure-lowering strategies reduce the risk of a first stroke by 25% to 30% (19). Intracerebral hemorrhage has an annual recurrent bleeding rate of approximately 2% (40). Besides benefits in primary prevention, reduction in blood pressure reduces the risk of further intracerebral bleeding by 50% in patients with prior hemorrhage (79). In case-control studies, high alcohol intake (greater than 56 g/d) has been found to lead to a 3-fold increase in the risk of intracerebral hemorrhage by impairing coagulation and directly affecting the integrity of cerebral vessels (05). Thus, there is no doubt that an efficient reduction in blood pressure and an ending of alcohol abuse are important measures for the primary and secondary prevention of hemorrhage in the thalamus. The American Heart Association’s latest guidelines for spontaneous intracerebral hemorrhage management recommend a blood-pressure goal of 130/80 mm Hg after the acute period to prevent hemorrhage recurrence (36). The association between smoking and intracerebral hemorrhage is still controversial; however, it is altogether advisable that current smokers quit smoking (05).
Although coagulopathy may also be a risk factor for thalamic hemorrhage, it is difficult to translate this into a strategy for primary prevention of thalamic hemorrhage.
Other underlying conditions (such as arteriovenous malformations) leading to or increasing the risk of thalamic hemorrhage are often unknown before the intracerebral hemorrhage. This makes preventative strategies difficult in these patients as well. After hemorrhage has occurred, obliteration of arteriovenous malformations by a single or combined treatment modality (microsurgery, endovascular embolization, or stereotactic radiosurgery) may be undertaken to prevent subsequent hemorrhages, primarily when the treatment modality warrants both low complication and higher obliteration rates. In a case of 53 patients with small arteriovenous malformations in the thalamus who were treated by stereotactic radiosurgery, thalamic location accounted for 3.4% of 1557 cerebral malformations treated by radiosurgery (27). The mean patient age was 35.8 years; 89% experienced bleeding as the first clinical manifestation of arteriovenous malformation, and Spetzler-Martin scores of III and IV were recorded in 42% and 28%, respectively. The mean treatment volume was 1.43 cm3. Complete obliteration occurred after one or two procedures in 67% of patients. Hemorrhagic risk after radiosurgery was 3.9% and 1.9% in the first and second year, respectively, and the mortality rate was 3.9%.
It has long been debated whether lipid-lowering therapy, particularly with statins, increases the risk of hemorrhage. A systematic review and meta-analysis of statin and non-statin low-density lipoprotein cholesterol-lowering (LDL-C-lowering) therapies assessed the risk of hemorrhagic stroke (09). This meta-analysis comprised 37 large randomized clinical trials of mostly statin LDL-C-lowering therapies with at least 2 years of follow-up. Statin therapy slightly increased the risk ratio of hemorrhagic stroke by 32% and 14% in trials of secondary and primary prevention, respectively. Statin therapy intensity was not associated with the baseline and the magnitude of LDL-C reduction. Neither ezetimibe nor proprotein convertase subtilisin/kexin type 9 (PCSK-9) inhibitor nor triglyceride-lowering therapies increased the hemorrhagic stroke risk (09).
A patient presenting with acute neurologic deficit related to thalamic function may have a cerebral infarction or hemorrhage. There are no reliable clinical means of distinguishing the two, necessitating a diagnostic imaging study.
Evaluation of a patient with thalamic hemorrhage should include a detailed history and physical examination to identify possible risk factors or etiologies such as previous diagnoses of arterial hypertension or arteriovenous malformation, use of anticoagulants, illicit drug abuse, or abuse of alcohol.
Baseline laboratory studies should include complete blood and platelet counts, liver functions, renal panel, serum glucose, inflammatory markers (erythrocyte sedimentation rate, or C-protein reactive), cardiac troponin, and electrocardiogram. A coagulation profile (prothrombin time, partial thromboplastin time) and specific tests for direct oral anticoagulants may be particularly helpful when anticoagulant-related intracerebral hemorrhages and underlying malignancy or hematological disorders are suspected. A urine toxicology screening is advisable in adolescent or young patients without intracerebral hemorrhage risk factors (36).
Due to its high sensitivity, specificity, rapid acquisition time, and availability in emergency departments, noncontrast CT scan is still the preferred imaging procedure to exclude the presence of intracerebral hemorrhage (36). It also allows definition of size, location of the bleeding within the thalamus, and spreading into neighboring structures (internal capsule, lentiform nucleus, subthalamus, midbrain and subcortical white matter). In addition, the presence of ventricular blood, the occurrence of hydrocephalus, and surrounding edema may be recognized with CT scan. Hematoma evolution may be also monitored by noncontrast brain CT.
Conventional MR images with T1- and T2-weighted sequences are not sensitive to blood in the hyperacute stage, whereas gradient echo-MRI sequences or susceptibility-weighted sequences can also detect intracerebral hemorrhage during this period with high accuracy (61; 36). In a multicenter study of 62 patients with acute intracerebral hemorrhage, gradient echo-MRI was found to be useful for diagnosis with a sensitivity of 100% within the first 6 hours after symptom onset (28). Nevertheless, its use may be limited due to a lack of tolerability or the presence of a cardiac pacemaker, or it may be altogether unavailable.
Determination of the cause of thalamic hemorrhage relies on patient age and prior history. When thalamic hemorrhage occurs in a patient with known arterial hypertension, often no other cause is sought, whereas in normotensive patients and, particularly, those younger than 45 years of age with thalamic hemorrhage, a digital subtraction angiography is still the currently preferred practice, according to results reported by nearly 700 physicians involved in the care of patients with intracerebral hemorrhage in three European countries (17). If hemorrhage suggests an underlying structural lesion, further investigations may include MRI, MR angiography/venography, CT angiography/venography, or conventional angiography (61; 36). MRI has been found to be superior to CT in providing useful data to rule out the presence of underlying arteriovenous malformations or tumors, although small arteriovenous malformations may be missed with this technique, or the underlying structural lesion may be obscured by the acute hematoma (61). MR-echo gradient sequences identify cavernous malformations better than MRI. MR angiography or CT angiography may also reveal structural lesions. CT angiography may provide better vascularization detail than MR angiography.
Approximately one third of patients with intracerebral hemorrhage showed the “spot sign” –defined as at least one focus of enhancement within the hematoma margin and without external vascular communication—on CT angiography performed early after symptom onset. There is currently no consensus about the minimum Hounsfield unit density, size, and morphological patterns of this radiological sign (96; 22; 26; 37). This bright spot is found somewhat less frequently when the bleeding involves either the basal ganglia or the thalamus (26). Moreover, contrast extravasation (seen as a pooling of contrast in the hematoma area after postcontrast CT in the location of the CTA spot sign) was observed in approximately half of the patients with a spot sign on CT angiography within the first 6 hours after intracerebral hemorrhage (26; 37). Early hematoma expansion on subsequent imaging has been associated with spot positivity and contrast extravasation (37), whereas the presence of the spot sign increases the risk of in-hospital mortality and poor functional outcome at 3 months (22). Contrast extravasation was observed on CT angiography in 20% of 139 patients with primary intracerebral hemorrhages mostly located in the deep gray matter. This radiological finding was associated with an increased rate of early hematoma expansion and was found to be an independent predictor of poor outcome and mortality at 3 months (57). A 9-point prediction score for identifying patients with intracerebral hemorrhage at risk of hematoma expansion has been developed and independently validated (12). In the development cohort of this prediction score, the hemorrhage was located in the basal ganglia and thalamus in nearly half of the cohort’s 817 patients; 40% of the hemorrhages were lobar, whereas the remainder were found in the brainstem and cerebellum. The prediction score included clinical and radiological parameters available on initial evaluation. A high risk of hematoma growth was associated with a shorter time to initial brain CT (less than 6 hours), a large baseline hematoma volume (> 60 mL), the presence of the CTA spot sign, and warfarin use (12). A high score (4 to 9 points) was associated with a 4.5-fold increased risk of hematoma expansion compared to a low score (0-3 points). In a secondary analysis that excluded patients with previous warfarin treatment, the prediction score was associated with a 3.2-fold greater likelihood of hematoma growth (12). A prediction score that reliably identifies patients at the highest risk of hematoma expansion would be useful for selecting those requiring more intensive care or tailored treatment to prevent hematoma growth. Additionally, it would be valuable for appropriately selecting patients for clinical trials designed to evaluate different treatment methods to prevent expansion and, consequently, improve outcomes.
The “black hole” sign, another imaging marker that may be useful to predict early hematoma expansion, was found in 14.6% of 206 patients on nonenhanced CT scan within 6 hours after onset of spontaneous intracerebral hemorrhage, mostly located in the basal ganglia and thalamus (60). The black hole sign was defined as a hypoattenuated area (black hole) encapsulated within a hyperattenuating hematoma with a clearly defined border, which may suggest bleeding of different age within the hematoma. In this cohort of patients, hematoma growth on nonenhanced CT scan performed within 30 hours of baseline imaging was found to occur five times more frequently in patients with black hole sign than in those with no black hole sign, 32% versus 6%, respectively (60). In a meta-analysis of 1495 patients with intracerebral hemorrhage analyzed in five studies (four with a retrospective design; two with fewer than 200 patients), the black hole sign as an imaging marker to predict hematoma expansion showed a low sensitivity (0.30) and a high specificity (0.91), whereas the positive and negative likelihood ratios were 3.5 and 0.77, respectively (101).
The “blend sign”—a peculiar pattern of hematoma heterogeneity—is another imaging marker of hematoma expansion. A blend sign was observed in 20% of 182 patients with spontaneous intracerebral hemorrhage on noncontrast-enhanced brain CT performed within 6 hours after stroke onset (90). These 182 patients had a mean age of 68 years and a median hematoma volume of 22 mL. Nearly half of all hemorrhages in this cohort were located in the basal ganglia. The blend sign was a reliable predictor of neurologic deterioration in the first 48 hours and showed a somewhat higher specificity and positive and negative predictive value than the spot sign for predicting neurologic deterioration in basal ganglia hemorrhages (90).
Another imaging marker, called “the island sign” based on an extreme hematoma shape irregularity observed on noncontrast brain CT, may predict early hematoma expansion and further neurologic deterioration. The island sign as a predictor of hematoma growth was assessed in a prospective study of 225 patients with spontaneous intracerebral hemorrhage (58). The mean age of these patients was 60 years, and their median baseline hematoma volume was 13 mL; 61% of the hematomas were located in the basal ganglia, and 20% were found in the thalamus. The island sign was defined as any of the following two radiological findings on noncontrast brain CT: the first, at least three small, scattered hematomas (round or oval) all separate from the main hematoma (separate islands); the second, more than four small hematomas (bubble-like or sprout-like, but not lobulated), some or all of which may connect with the main hematoma (connected islands). On baseline CT scan, the island sign was observed in 16% (41 of 225) of patients. Hematoma expansion on a follow-up CT scan occurred in one third of patients (85 out 252); the island sign was significantly more common in patients with hematoma expansion (38/85, or 44%) than in those without expansion (3/167, or 1.8%) (58).
The updated American Heart Association’s guidelines for managing spontaneous intracerebral hemorrhage recommend CT angiography be performed within the first few hours after intracerebral hemorrhage to identify patients at risk of subsequent hematoma expansion (36).
The treatment of patients with thalamic hemorrhage is, for the most part, supportive medical care. Due to medical and neurologic instability during the acute phase of intracerebral hemorrhage, management should take place either in an intensive care unit or a stroke unit (36). Basic measures include continuous cardiopulmonary monitoring, airway protection in patients with suppressed levels of consciousness, screening for dysphagia, strict glucose control, prophylaxis against deep venous thrombosis, early mobilization, and rehabilitation. Moreover, intracranial and cerebral perfusion pressure, hemodynamic function, and neurologic function should be continuously monitored (36).
Treatment of sustained, severely elevated blood pressure is advisable to avoid recurrent or continued hemorrhage. The current guidelines of the American Heart Association recommend acute lowering systolic blood pressure to 140 mm Hg in patients with systolic blood pressure between 150 and 220 mm Hg and no contraindications to acute blood pressure treatment. This recommendation is safe and may improve the functional outcome (36).
Two prospective trials reported the effect of intensive blood pressure lowering within the first 6 hours after onset of supratentorial hemorrhage (03; 04). In both trials, intensive blood pressure lowering was found to be associated with a reduction in hematoma growth at 24 hours that was not associated with a poor clinical outcome. Thus, a first attempt to explore a blood-pressure target in 346 patients (most of Chinese origin) with acute intracerebral hemorrhage found that achieved on-treatment systolic blood pressure of between 130 and 140 mm Hg (median of 135 mm Hg) throughout the first 24 hours was associated with the greatest reduction of hematoma growth (06).
In an international multicenter prospective study (INTERACT-2) of 2829 patients with intracerebral hemorrhage and a mean age of 63.5 years, the safety and effectiveness of early intensive blood pressure lowering was compared with standard antihypertensive treatment based on currently recommended guidelines. The study randomly assigned 1399 patients (median NIHSS score of 10 points, 84% with a deep intracerebral hematoma) to early intensive treatment to lower their blood pressure (target systolic level of < 140 mm Hg within 1 hour), whereas the remaining 1430 patients (median NIHSS score of 11 points, 83% with a deep intracerebral hemorrhage) were assigned to guideline-recommended treatment (target systolic level of < 180 mm Hg) (02). In both groups, the choice of intravenous antihypertensive agent (mostly alpha-adrenergic antagonist) was left up to the treating physician, and the median time from onset of hemorrhagic stroke to initiation of intravenous treatment was shorter in the intensive-treatment group than in the standard therapy group (4.0 hours vs. 4.5 hours). A significant difference in mean systolic blood pressure was observed among both groups at 1 hour (150 mm Hg in the intensive treatment group vs. 164 mm Hg in the standard treatment group). The mean hematoma volumes at baseline for the patients undergoing intensive blood pressure lowering and those assigned to guideline-recommended treatment were 15.7 ml and 15.1 ml, respectively, and an absolute difference of 1.4 ml between both groups was observed at 24 hours (18.2 ml in the intensive-treatment control group and 20.6 ml in the standard-treatment group). At 90 days, a nonsignificantly higher rate of poor outcomes (death or major disability) was observed in the standard treatment group (56%) as compared to the intensive-treatment group (52%), although an ordinal analysis of scores on the modified Rankin scale suggested that intensive blood pressure treatment did, in fact, improve functional outcomes (02). No difference was observed in the death rate from any cause in either group.
The Antihypertensive Treatment of Acute Cerebral Hemorrhage (ATACH-2) trial—the latest phase III multicenter randomized controlled clinical trial designed to study the efficacy of early intensive reduction of systolic blood pressure in primary supratentorial intracerebral hemorrhage—was prematurely terminated due to futility after a prespecified interim analysis (80). In that study, 1000 patients (mean age: 62 years; NIHSS: 11 points; Asian ethnicity: 56%) were allocated to intensive or conservative blood pressure lowering therapy. Both patient groups received intravenous nicardipine within 4.5 hours of stroke onset and for the following 24 hours. Acute blood pressure reduction to a target systolic blood pressure of 110 to 139 mm Hg in the intensive group did not yield a significantly lower death rate or functional dependency compared with a conservative treatment target of 140 to 179 mm Hg (80).
A pooled analysis of individual patient data acquired in the main phase of INTERACT-2 and ATACH-2 trials from 3809 adults with spontaneous intracerebral hemorrhage and elevated systolic blood pressure revealed a favorable functional outcome at 90 days in patients with mild and moderate hemorrhage severity who achieved stable systolic blood pressure as low as 120 to 130 mm Hg within the first 24 hours of antihypertensive treatment (74). Patients were mean aged 63.1 years, 82% of patients had basal ganglia or deep hemorrhages, median NIHSS score was 11 points, and median time from stroke symptom onset to randomization to either of the intensity-lowering blood pressure treatments was 3.6 hours. The pooled analysis found a linear trend for magnitude of systolic blood pressure reduction and functional independence; thus, every 10 mm Hg reduction in systolic blood pressure was associated with a 10% increase in the odds for a good functional outcome (modified Rankin score 0 to 3) at 90 days. Early systolic blood pressure reduction to achieve values as low as 120 to 130 mm Hg was safe and not associated with more harmful renal effects (74).
The results of a meta-analysis assessing the efficacy and safety of intensive blood pressure lowering in acute intracerebral hemorrhage as opposed to standard management have become available (11). This meta-analysis involved five randomized controlled trials comprising 4360 patients with acute intracerebral hemorrhage who had been assigned to either intensive or standard blood pressure treatment. A systolic blood pressure lower than 140 mm Hg was the target in most patients in the intensive group, except in one small trial where the target was defined as lower than 110 mm Hg. A systolic blood pressure lower than 180 mm Hg was the target in most patients in the standard group, except in one trial where it was defined as ranging from 110 to 130 mm Hg. In both groups, the time from stroke onset to randomization was from 3 to 8.5 hours, and the NHISS score range was 9 to 12 points. Deep location of intracerebral hemorrhage occurred in 73% to 90% of patients included in this meta-analysis. No difference in stroke mortality at 3 months was observed between the groups. The patients in the intensive treatment group had a non-significantly lower death trend and functional dependency at 90 days and a lower hematoma expansion rate than those in the standard treatment group. Intensive blood pressure lowering was not associated with serious adverse events (11).
Intensive blood pressure reduction in the hyperacute (1 to 24 hours) and acute (2 to 7 days) phases of intracerebral hemorrhage showed a trend toward a favorable outcome, which was estimated by an ordinal analysis of the modified Rankin scores. This open, randomized controlled trial at its end included 2794 patients (68% enrolled in China) with spontaneous intracerebral hemorrhage (median volume of 10.2 ml; thalamic or basal ganglia location in 77% of patients) who were randomized into two blood pressure treatment groups. The first group had a target systolic blood pressure level of less than 140 mm Hg to be reached within 1 hour after randomization and maintained for the next 7 days. In the second group, treatment was started when systolic blood pressure was over 180 mm Hg. In both groups, the main intravenous antihypertensive agents were urapidil (an intravenous alpha-adrenergic antagonist), followed by nicardipine or nimodipine (calcium channel blockers). At 90 days, an overall relative risk reduction of 13% in poor functional outcomes favored intensive systolic blood pressure treatment. The lowest risk of functional disability was observed when systolic blood pressure ranged between 130 and 139 mm Hg in the acute phase of intracerebral hemorrhage (07).
Consequently, the real benefit of early blood pressure management (including the choice of blood pressure lowering agent) in patients with acute intracerebral hemorrhage requires an answer based on conclusive data, which are still lacking.
Elevated intracranial pressure may develop in patients with large thalamic hemorrhages. Head elevation and avoidance of hyposmolar intravenous fluids are basic measures in all patients with large hemorrhages. Hyperventilation to a PCO2 of 25 mm Hg decreases intracranial pressure by lowering cerebral blood flow. Hyperosmolar diuretics such as mannitol and hypertonic saline solution can also be useful to decrease elevated intracranial pressure.
Obstructive hydrocephalus may complicate thalamic hemorrhage when there is intraventricular extension. Although ventriculostomy is generally recommended for this complication, it has not been shown to improve prognosis (99; 16).
In general, thalamic hemorrhages have not been considered for surgical therapy because of their deep location in the brain and the fear that surgery might cause additional neurologic deficits. In the STICH multicenter trial, 1033 patients with spontaneous supratentorial intracerebral hemorrhage were randomized to the best conservative treatment or early surgical removal of hematoma (less than 72 hours after stroke onset). Open craniotomy was chosen as the surgical procedure by most neurosurgeons. In this trial, 284 and 300 patients with basal ganglia or thalamic hemorrhages were allocated to early surgery or conservative treatment, respectively. In these deep-hemorrhage patients, no differences in favorable outcomes at 6 months were noted between the two treatments (69). There is no convincing evidence of the benefit of surgical treatment of thalamic hematomas (69; 36). Minimally invasive operative procedures are preferred over conventional craniotomy when surgical treatment is deemed necessary in patients with spontaneous supratentorial intracerebral hemorrhages (36).
The SWITCH trial compared 6-month outcomes in patients with severe, deep, spontaneous intracerebral hemorrhage who underwent either decompressive craniectomy and best medical treatment (BMT) or BMT alone (08). This trial comprised 201 adult patients under 75 years of age with either a basal ganglia or thalamic spontaneous intracerebral hemorrhage and a Glasgow Coma Scale (GCS) score between 8 and 13 points, NIHSS score between 10 and 30 points, and intracerebral hemorrhage volume between 100 and 300 ml who were randomized to one of two arm groups within 66 hours after stroke onset. Decompressive craniectomy without hematoma evacuation was performed within 6 hours after randomization. The median age was 61 years, and the median hematoma volume was 57 mL. The median time from stroke onset to craniectomy was 26 hours, and the median diameter of the decompressive craniectomy was 13 cm. At 6 months, patients in the craniectomy group showed an absolute risk reduction of 13% in the primary endpoint (modified Rankin Scale 5 to 6) compared to the BMT group. Nevertheless, survival was associated with severe disability in both arms.
One hundred and five patients with a first thalamic hematoma (10 to 35 ml of volume) were non-randomly divided into two groups: the first group (45 patients) was treated by aspiration (within 4 to 48 hours after the onset of bleeding; 10.4-hour mean time to operation) and subsequent thrombolysis with urokinase, and the second group (60 patients) received conservative treatment (15). A significant difference in cumulative mortality rate (28% in the conservative group versus 11% in the aspiration group) was observed at 30 days after hemorrhage. The NIHSS score at 30 days after stroke onset was significantly lower in the aspiration group (14.2) than in the medically treated group (16.5). Half of the patients in the aspiration group had a favorable outcome (Glasgow Outcome Scale greater than 3) at 90 days after stroke onset versus one-third of patients in the conservative group, which is a significant difference. There was no difference between the groups with regard to the rate of complications (rebleeding, intracranial infection, and pneumonia) (15).
In a meta-analysis that included 11 studies (totaling 1717 patients with primary supratentorial hemorrhage, an average age between 56 and 67 years, and a mean hematoma volume from 33 to 59 ml), all the patients received conservative medical treatment for intracerebral hemorrhage. The study aimed to compare the efficacy of minimally invasive surgery (stereotactic or neuroendoscopic hemorrhage evacuation) against either open surgery or medical management alone (81). Patients who underwent minimally invasive surgery showed a significant 36% reduction in the relative mortality risk, a nonsignificant 5% reduction in death or dependent survival, and a nonsignificant 24% increase in independent survival (81). Thus, this meta-analysis suggests that minimally invasive surgery (stereotactic, neuroendoscopic, or burr hole evacuation) may be an effective step in the treatment of primary supratentorial hemorrhage, although important issues remain to be clarified, such as which patients will benefit most from this kind of intervention and what risks are involved.
A randomized, controlled, open-label, blinded-endpoint phase 3 explanatory trial evaluated functional outcomes in patients who underwent minimally invasive surgery versus standard medical care (39). Patients with nontraumatic supratentorial intracerebral hemorrhage larger than 30 mL as measured by the ABC/2 method were randomized to minimally invasive surgery (stereotactic catheter placement in the hematoma followed by clot aspiration and thrombolytic irrigation thereof in 255 patients) or standard medical care (in 201 patients). The primary efficacy endpoint was a good outcome, defined as a modified Rankin score of 0 to 3 and assessed 365 days after presentation. All patients included in the trial were over 18 years of age, with a Glasgow Coma Scale score of 14 or less or an NIHSS score of 6 or higher and no disability before stroke; their hematomas showed no expansion (up to 5 mL of growth was allowed) within 6 hours after diagnostic head CT, and their intracerebral hemorrhages were all due to small-vessel disease. Deep hemorrhage was most frequent in both patient groups (65% in the minimally invasive surgery group and 58% in the standard medical care group). The initial NIHSS score was 19 in both groups, whereas hematoma volume before randomization was slightly larger in the minimally invasive group (45.8 mL) than in the standard medical care group (45.3 mL). At the end of the intervention, hematoma volume measured by CT was 12.5 mL in the minimally invasive surgery group and 43.7 mL in the routine medical care group. Rates of symptomatic bleeding and brain bacterial infections were similar in both groups. At 365 days, the groups showed no significant differences in functional outcome: 44% of patients in the minimally invasive group had a good functional outcome compared to 42% in the standard medical care group. Nevertheless, mortality at 365 days was lower in patients with minimally invasive surgery (15%) than in the standard medical care group (23%) (39).
Functional outcome in patients with supratentorial hypertensive hemorrhage was compared between those treated with minimally invasive surgery (endoscopic surgery or stereotactic aspiration) and those treated with small bone flap craniotomy (2 cm in diameter) (98). This multicenter trial randomly assigned 721 patients with hypertensive supratentorial hemorrhage (mean age 56 years with a median GCS score of 9 and a mean hematoma volume of 49 ml) to one of the above treatments within the first 24 hours after hemorrhage onset. Basal ganglia (71%) and lobar hematomas (20%) were the main locations, and 8.6% of hematomas were in the thalamus. At 6 months, favorable outcomes (modified Rankin scale 0 to 2) were found to be significantly higher in patients who had deep hemorrhages (basal ganglia or thalamus) treated with endoscopic surgery or stereotactic aspiration compared to those who underwent craniotomy. Around one third of endoscopic surgery and stereotactic aspiration patients had favorable outcomes, whereas outcomes were favorable in only 14% of craniotomy patients. Mortality at 1 month after treatment was similar in the two groups (98).
The value of ultra-early hemostatic therapy (recombinant-activated factor VII) remains in doubt because no benefit on mortality or functional outcome was demonstrated in 840 patients with noncoagulopathic intracerebral hemorrhages included in the largest phase III trial, despite the hemostatic effect observed (66). Nevertheless, in a posthoc analysis of this phase III trial, a better outcome was observed among patients aged less than 70 years, with a baseline hematoma volume of less than 60 mL, a baseline intraventricular hemorrhage volume of less than 5 mL, and a time from onset to treatment of fewer than 150 minutes (67). The effect of the hemostatic agent tranexamic acid on hematoma growth is currently being investigated in a multicenter, randomized, placebo-controlled (two arm 1; 1), double-blind phase 2 trial (The Spot Sign and Tranexamic Acid on Preventing ICH Growth – AUStralasia Trial) (STOP-AUST) based on positive results observed in trauma patients and in an observational study of ethnic Asian patients with acute intracerebral hemorrhage. One hundred patients with acute intracerebral hemorrhage and “spot sign” evaluated on CTA (considered an imaging marker of ongoing bleed) will be randomized to receive tranexamic acid (active treatment arm) or a placebo within 4.5 hours of intracerebral hemorrhage onset (70). The primary outcome will be intracerebral hemorrhage growth at 24 hours, and the secondary outcome measures will include an absolute increase in hematoma volume, major thromboembolic events, and a modified Rankin scale score at 90 days (70).
The hemostatic effect of tranexamic acid in reducing hematoma growth and improving the outcome of adult patients with spontaneous intracerebral hemorrhage was assessed in the TICH-2 randomized placebo-controlled phase 3 trial (91). This trial comprised 2325 participants with a mean age of 68.9 years and a mean hematoma volume of 24 mL; 59% and 32% of participants had a deep or lobar hematoma, respectively, and 56 (22%) out of 249 patients who had a CTA showed a positive spot sign. After randomization, 1161 patients received tranexamic acid (1 g in intravenous bolus followed by an infusion of another 1 g over 8 hours) or a placebo within 8 hours of stroke onset. At 3 months, the modified Rankin Scale showed no significant differences in functional status between the patient groups. At 24 hours, tranexamic acid yielded a small reduction in hematoma volume (1.37 ml) compared with the placebo group. Patients who received tranexamic acid had significantly fewer serious adverse events at days 2, 7, and 90 compared with the patients in the placebo group. The most common safety outcome was seizure, occurring in 7% of patients in both groups. Tranexamic acid did not increase either the frequency of venous thromboembolism or arterial occlusions (91).
A retrospective analysis of functional outcome at 6 months in 533 patients with intracerebral hemorrhage showed that a thalamic hematoma volume greater than 22 ml has a 2.6-fold higher poor outcome risk (modified Rankin scale 4 to 6) (94). In this study, 12.5% (67) of the 533 patients had a thalamic hemorrhage, 50% had a modified Rankin score between 3 and 5, 10% had a good functional outcome (modified Rankin score lower than 2) at 6 months, and 10% died (94).
Pregnancy may be a risk factor for thalamic hemorrhage for several reasons. First, hemodynamic changes in pregnancy, including increased cardiac output, heart rate, and blood volume, are believed to increase the risk of intracranial hemorrhage from arteriovenous malformations and intracranial aneurysms (89). Certain pregnancy-related conditions may increase the risk of intracerebral hemorrhage, including bleeding diatheses such as idiopathic thrombocytopenic purpura and disseminated intravascular coagulation. Finally, pregnancy-induced hypertension may lead to hypertensive vasculopathy and intracerebral hemorrhage (89).
Effects of anesthetic agents on cerebral blood flow, cerebral metabolism rate, and intracranial pressure should be considered in the acute or subacute phase of intracerebral hemorrhage to avoid worsening of neurologic status either by increase in intracranial hypertension or critical reduction of perihematoma cerebral blood flow. Inhalational anesthetic agents produce direct cerebral vasodilatation and an increase in cerebral blood volume, whereas hypnotic agents, benzodiazepine derivatives, and opioids reduce cerebral metabolic rate and cerebral blood flow.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Julien Bogousslavsky MD
Dr. Bogousslavsky of the Swiss Medical Network has no relevant financial relationships to disclose.
See ProfileJorge Moncayo-Gaete MD
Dr. Moncayo-Gaete of Universidad Internacional del Ecuador has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
Dec. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Stroke & Vascular Disorders
Oct. 29, 2024
Sleep Disorders
Oct. 14, 2024
Developmental Malformations
Sep. 22, 2024