






















Peripheral Neuropathies
Neuropathic pain: treatment
Jan. 19, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Tick paralysis is a potentially fatal disease that causes rapidly ascending weakness, particularly in children. The condition resolves on removal of the offending tick. Every physician should keep tick paralysis in mind when confronted with a patient with rapidly progressive paralytic symptoms or ataxia.
|
• Tick paralysis should be suspected in anyone with potential tick exposure who has an acute, flaccid paralysis or ataxia. | |
|
• Clinical diagnosis is only secured by identifying an attached tick, with removal yielding rapid improvement. | |
|
• Tick paralysis is a noninfectious, neurotoxic process that is seen more in children than adults. | |
|
• The primary diagnostic confusion is with Guillain-Barré syndrome. |
Tick paralysis, also sometimes referred to as tick toxicosis, was first described in Australia in 1824 and in North America in 1912 (40); additional cases were subsequently described in Africa, Australia, and Mediterranean countries. The clinical features of ascending paralysis and resolution after finding and removing a tick were recognized in the initial descriptions. Early reports included descriptions of paralysis in both humans and animals. Early attempts to understand the mechanism of muscle weakness used intentional infestation of various animals; these efforts demonstrated considerable variability in susceptibility between species, with sheep, cattle, and cats and dogs most vulnerable.
|
• Tick paralysis is characterized by a rapidly ascending paralysis that is clinically similar to other rapid paralytic conditions, such as Guillain-Barré syndrome and the Fisher variant. | |
|
• The typical presentation is with the development of an unsteady, ataxic-type gait followed by an acute symmetric ascending flaccid paralysis. | |
|
• Within 24 to 48 hours, weakness ascends to the trunk, causing difficulty in maintaining a seated posture, followed by involvement of the arms, after which bulbar function is affected with difficulties in speech and swallowing, often with accompanying unilateral or bilateral facial weakness and ptosis. |
Tick paralysis is characterized by a rapidly ascending paralysis that clinically resembles other rapid paralytic conditions, such as Guillain-Barré syndrome and the Fisher variant (29; 18; 16; 45; 36). The typical presentation is with development of an unsteady, ataxic-type gait followed by an acute symmetric ascending flaccid paralysis (30; 33). Within 24 to 48 hours, weakness ascends to the trunk, causing difficulty in maintaining a seated posture, followed by involvement of the arms. Soon afterward, bulbar function is affected with difficulties in speech and swallowing, often with accompanying unilateral or bilateral facial weakness and ptosis. Involvement of thoracic muscles and the diaphragm may result in respiratory failure. Sensory function and bowel and bladder control remain preserved. Examination reveals weakness whose severity and distribution vary with the duration of illness. In patients presenting early in the illness, gait may be ataxic, and tests of coordination may show dysmetria. Extraocular muscle weakness is common, with diplopia and ophthalmoparesis. Pupillary function can also be affected, with unilaterally or bilaterally fixed and dilated pupils. Dysarthria is common. Sensory testing is normal. Tendon reflexes are reduced or absent. The mortality rate can exceed 10% in cases allowed to progress without ventilator support.
Variations may occur in both disease onset and progression. Weakness may not always ascend in an orderly progression, and patients may present with both leg and bulbar weakness that worsens over hours to days (13). Weakness may also begin focally, and onset with monoplegia or unilateral facial paralysis has been reported (29; 01; 31). Unusual cases have been reported, including cases in which early symptoms are referential to a single trunk of the brachial plexus or severe autonomic dysfunction has occurred (15; 09).
In addition to skeletal muscle weakness, there may be pupillary dysfunction, vomiting, and changes in level of arousal. Children may present with irritability or lethargy (35) and occasionally have slowing on EEG recordings (18).
The clinical presentation and progression of weakness appear to be similar for ticks of North America (Dermacentor andersoni and Dermacentor variabilis) and Australia (Ixodes holocyclus) (18; 13; 16; 20; 25); however, there are differences in recovery after the tick is removed. Prompt improvement in strength (within 1 hour) is usual in cases associated with D andersoni and D variabilis. In contrast, weakness may progress for 24 to 48 hours after removal of the tick in cases associated with I holocyclus (29; 18; 11).
The prognosis is uniformly good, with complete resolution of weakness. For North American tick paralysis, weakness may abate within an hour after tick removal, with full recovery in 1 to 2 days (30). In Australian tick paralysis, improvement may be slower, with continued progression for up to 48 hours after tick removal and substantial resolution within a week; full recovery may take several months (18; 11).
The primary complication is respiratory failure, which can cause death if not treated with ventilator support. If antitoxin is given, there may be anaphylactic reactions.
A 7-year-old girl presented to the emergency department after her parents noted her walking “funny.” On exam, she was mildly dysarthric and was drooling, which was new according to her parents. She had weakness in her feet, legs, and grip. Reflexes were absent. Her sensation was intact. Over the course of 3 hours, she became more dyspneic and required intubation for airway protection. While at her bed, stroking her hair, the girl’s mother felt a “knot” on her scalp. Careful inspection revealed an engorged tick, which was carefully removed with tweezers. Seven hours later, the patient was extubated successfully. She was discharged home the next day and was normal at a follow-up appointment 7 days later.
|
• Tick paralysis results from a neurotoxin elaborated by the female tick while feeding on blood from animal, or less commonly, human hosts. | |
|
• In North America, the vectors primarily implicated most commonly are the Rocky Mountain wood tick (D andersoni) and the American dog tick (D variabilis). |
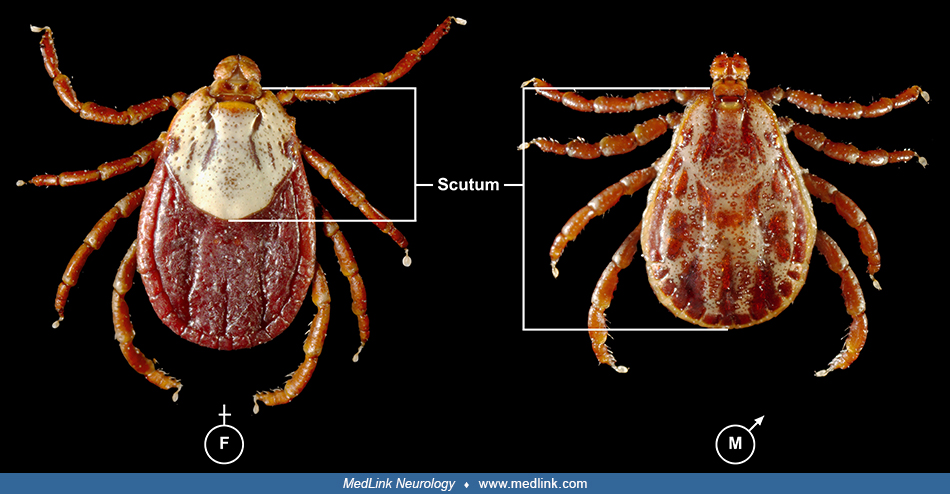
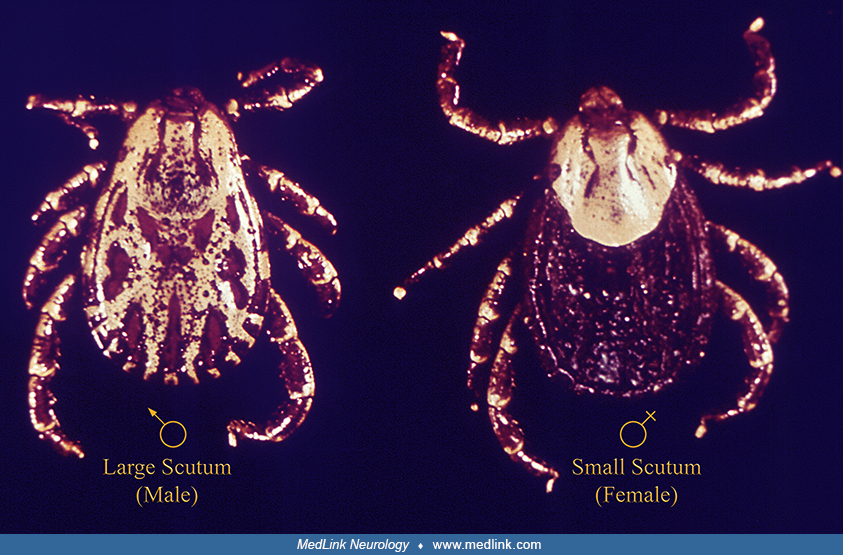
Tick paralysis results from a neurotoxin elaborated by the female tick while feeding on blood from animal, or less commonly, human hosts. Male ticks rarely cause tick paralysis (05). There are two classes of ticks: (1) hard-bodied (Ixodidae) and (2) soft-bodied (Argasidae), based on the presence or absence of a dorsal body shield. Many species of ticks are responsible for transmitting different infections, but only a few species can also produce neurotoxins in their salivary glands (39). Hard ticks engage in prolonged feeding on blood for up to 10 days; they secrete a variety of compounds from their salivary glands. These include anticoagulants and immune-modulating compounds, and in a few species, a toxin that can cause weakness (18). Although tick infestation in animals is part of the life cycle in the wild, paralysis is uncommon, though described most often in Australia (18). Few animal species are susceptible, and among domesticated animals, tick paralysis occurs in cattle, sheep, and household pets (ie, dogs and cats). Tick paralysis is relatively rare in humans.
The tick species that cause paralysis in humans vary geographically, with more than 40 such tick species implicated worldwide (17). Because of foreign travel, nonindigenous tick species may cause tick paralysis in a given locale (32).
The life cycle of ticks is complex, requiring 2 years and three hosts (18). The unfed female is more likely to attach to a human as the third host. Adult ticks are most abundant in the spring and early summer (the most common season for tick paralysis), but paralysis can also occur at other times of the year. The most common attachment site of paralysis-causing ticks is the scalp, behind the ear.
In North America, the vectors primarily implicated are the Rocky Mountain wood tick (D andersoni) and the American dog tick (D variabilis) (13). In addition to being a cause of tick paralysis, the Rocky Mountain wood tick is also a vector of Rocky Mountain spotted fever (caused by the intracellular bacterium Rickettsia rickettsia), Colorado tick fever (caused by the Colorado Tick Fever virus), and tularemia (caused by the intracellular bacterium Francisella tularensis). The Rocky Mountain wood tick is found in the Rocky Mountain States and southwestern Canada from elevations of 4000 to 10,500 feet. The life cycle of this tick may require up to 2 to 3 years for completion. Larvae and nymphs feed on small rodents, whereas adult ticks feed primarily on large mammals. Adult ticks are primarily associated with pathogen transmission to humans.
The American dog tick (sometimes called a “wood tick”) is widely distributed east of the Rocky Mountains and in limited areas on the Pacific Coast. The highest risk of being bitten occurs during spring and summer. Adult females are most likely to bite humans. Like the Rocky Mountain wood tick, the American dog tick is a major vector of Rocky Mountain spotted fever (caused by the intracellular bacterium Rickettsia rickettsia).
In Australia, the I holocyclus tick is frequently a cause of tick paralysis and consequently is colloquially known as the Australian paralysis tick, or more simply as the paralysis tick (02). It is different from the so-called bush tick, but the two have been frequently confused. The tick is distributed along eastern coastal areas of Australia, particularly in Queensland in the northeast and New South Wales in the southeast (46).
In Africa, I rubicundus and Rhipcephalus evertsi have been implicated in causing tick paralysis.
Pathologic mechanisms of muscle weakness appear to vary between species of ticks. Detailed molecular studies of the toxins associated with tick paralysis are lacking, however, and data come from animal models, electrophysiologic studies, and similarities with other toxins (18). For D andersoni and D variabilis, there is apparently an interruption of sodium flux across the axonal membrane at nodes of Ranvier and at the neuromuscular presynaptic terminal, which would account for the diffuse slowing of motor and sensory conduction (distal latency and conduction velocity) noted clinically (41; 18). Altered flux at the presynaptic terminal could cause reduction in the release of acetylcholine, resulting in the low compound muscle action potential amplitude. For tick paralysis associated with I holocyclus, investigators demonstrated a reduction in acetylcholine release at presynaptic terminals, resulting in altered excitation-contraction coupling (18), but the underlying mechanism had remained obscure. It is now clear that the responsible family of neurotoxins, known as holocyclotoxins (HTs), induce muscle paralysis by inhibiting calcium-dependent transmitter release, a form of presynaptic inhibition (07).
Tick toxin does not appear to act immediately, and 2 to 6 days may elapse between infestation and onset of weakness (30). This may be explained either by delays in the elaboration of toxin in the salivary gland or time for enzymatic modifications of the toxin molecule (as occur, for example, with botulinum toxin).
|
• Young children aged 1 to 8 years old are the most common victims. | |
|
• In North America, most cases of tick paralysis occur from April to June, when adult Dermacentor ticks emerge from hibernation and actively seek hosts. |
Although adults with tick paralysis have been described, most series report children, perhaps because the toxin has more impact on a milligram-per-kilogram basis. Young children aged 1 to 8 years old are the most common victims, although cases in babies (22) and in the elderly have also been reported (13; 11; 24; 03). A cluster of cases in Colorado was remarkable for two afflicted individuals over 70 years of age, one of whom with no history of outdoor exposure (06). Young girls with long hair seem to be most vulnerable because the tick is more likely to escape initial detection.
In North America, most cases of tick paralysis occur from April to June, when adult Dermacentor ticks emerge from hibernation and actively seek hosts (13). Limited formal surveillance data exist for human tick paralysis. Between 1946 and 1996, Washington State required that all cases be reported (13). There were 33 cases, with two deaths occurring during the first 2 years of surveillance and none thereafter. In New South Wales, Australia, only two cases were discovered in the records of two large hospitals between 1983 and 1995 (18). However, tick paralysis is no longer a reportable disease and may be more common than suspected (16).
The geographic distribution of various ticks is shifting and will continue to shift with climate change (34; 43; 44).
|
• Protective clothing and repellants such as DEET may reduce the risk of acquiring a tick. | |
|
• Early removal of ticks is preventative for tick paralysis. | |
|
• Children playing in tick-infested areas should be carefully inspected for attached ticks during the spring and summer months, especially if the child exhibits muscle weakness or an unexplained change in behavior. |
The use of protective clothing and repellants such as DEET (N,N-Diethyl-meta-toluamide) may reduce the risk of acquiring a tick. Early removal of ticks is preventative. Children playing in tick-infested areas should be carefully inspected for attached ticks during the spring and summer months, especially if the child exhibits muscle weakness or an unexplained change in behavior. Long hair may hide ticks.
Ultrasonic pest-repellent devices are not effective (28).
The physical examination remains a crucial part of the workup for patients with acute and subacute weakness. Diagnosing tick paralysis depends on identifying the tick. The primary diagnostic issue in tick paralysis is including it in the differential diagnosis of acute ascending paralysis (16), and the possibility of tick paralysis should be considered in any individual, particularly a child, who presents with rapidly ascending paralysis after being in an area where ticks are prevalent. On clinical testing, the site of the lesion producing weakness localizes to peripheral motor nerves or the neuromuscular junction. This fact is based on intact cognition, relative symmetry of weakness, reduced or absent reflexes, flexor plantar responses, and intact sensation. Major differential diagnostic considerations include acute inflammatory demyelinating polyneuropathy (Guillain-Barré syndrome), the Fisher variant of Guillain-Barré syndrome, transverse myelitis in its early stages, botulism, and encephalitis or poliomyelitis, as may be seen in neuroinvasive West Nile virus infection (14; 10; 11; 30; 42; 36). Occasionally, there is confusion with suspected spinal cord compression, such as may occur from an epidural abscess (14). In some cases, sepsis was the initial diagnosis (33).
Tick paralysis is often misdiagnosed as Guillain-Barré syndrome (10; 11; 30; 38). A meta-analysis of 50 well-characterized cases of tick paralysis published between 1946 and 2006 highlights that misdiagnoses have been more common in recent years than in the past, with Guillain-Barré the most frequent erroneous initial conclusion (10). Patients received unnecessary therapies, such as intravenous immunoglobulin G and plasmapheresis. This suggests a strong need to educate neurologists and emergency room providers so that tick paralysis is considered early in the differential diagnosis of acute flaccid paralysis or ataxia. A subsequent comparative meta-analysis of tick paralysis in the United States and Australia showed that (1) the proportion of misdiagnoses of tick paralysis as Guillain-Barré syndrome was greater in the U.S. than in Australia, and (2) tick paralysis was increasingly misdiagnosed as Guillain-Barré syndrome during more recent reporting periods in the U.S. (11).
Acute inflammatory demyelinating polyneuropathy is the most common form of acute ascending paralysis. Although acute inflammatory demyelinating polyneuropathy resembles tick paralysis in its pattern of weakness and tendon reflex abnormalities, tick paralysis differs from acute inflammatory demyelinating polyradiculoneuropathy in that it usually progresses more rapidly, has normal cerebrospinal fluid, and has no electrodiagnostic evidence for primary demyelination. The Fisher variant with ophthalmoplegia, ataxia, and areflexia also has features in common with tick paralysis but differs in that tick paralysis includes muscle weakness, whereas the Fisher variant does not. Transverse myelitis may be considered early in the course of tick paralysis when weakness is confined to the legs; however, later progression of tick paralysis to include weakness of cranial nerve-innervated muscles would exclude a myelopathy. Furthermore, sensory loss along with bladder and bowel incontinence would be expected with transverse myelitis. Botulism should also be considered. Most cases of gastrointestinal-derived botulism occur in infants, whereas tick paralysis occurs when children are older and are active outside. Additionally, weakness in botulism follows a descending pattern of progression. A poliomyelitis-like illness has been reported due to West Nile virus and may occur without signs of encephalitis (26). However, systemic symptoms of fever, chills, and stiff neck are not seen in tick paralysis, and cerebrospinal fluid in West Nile virus infections reveals inflammation.
|
• A high index of suspicion should be maintained because tick paralysis may occur in nonendemic areas or among individuals without known outdoor exposure, is readily treatable if identified, and may be fatal if overlooked. | |
|
• A thorough skin examination should be performed on admission in any patient with new-onset ataxia and ascending paralysis. | |
|
• The most striking electrophysiologic finding in tick paralysis is reduced compound muscle action potential amplitude that begins within days of symptom onset. |
Clinical suspicion of tick paralysis is typically low because of the rarity of the condition. Regardless of the rarity of the condition, though, a high index of suspicion should be maintained because tick paralysis may occur in nonendemic areas or among individuals without known outdoor exposure, is readily treatable if identified, and may be fatal if overlooked (06; 01; 32; 42; 19). A thorough skin examination should be performed on admission in any patient with new-onset ataxia and ascending paralysis (19).
Delays in finding a tick or considering the possibility of tick paralysis lead to unnecessary diagnostic studies, treatments, and medical costs (33). Further, this delays recovery or results in unnecessary morbidity and potentially even death. In one retrospective series of cases presenting to an emergency room in southern Louisiana, four of nine cases involved a delay in accurate diagnosis.
Routine laboratory studies, including serum electrolytes and cerebrospinal fluid, are normal. Occasionally, serum creatine kinase levels are mildly elevated (18).
Electrodiagnostic studies are important in confirming the location of the lesion to peripheral nerves and, thus, narrowing the differential diagnosis (08; 41; 18; 16; 45). The most striking electrophysiologic finding in tick paralysis is reduced compound muscle action potential amplitude that begins within days of symptom onset. Following removal of the tick, compound muscle action potential amplitude increases within days but may not reach normal values for weeks or months. A comparison of compound muscle action potential amplitudes reveals a 50% to 75% reduction in amplitude in all nerves tested. Distal latencies and conduction velocities of motor nerves are mildly prolonged, at the limits of normal, but return to values well within the normal range over weeks or months. Sensory nerve action potential amplitudes remain within the normal range but may increase over weeks or months. Repetitive nerve stimulation tests at low frequencies (2 Hz) and high frequencies (20 to 50 Hz) are normal, and there is no facilitation after exercise. During the phase of acute weakness, needle electromyographic studies may be essentially normal, except for evidence of muscle membrane irritability (41).
Unusual presentations of tick paralysis have also been studied with electrophysiological methods. In one case, nerve conduction studies and electromyography indicated a conduction block involving the lower trunk of the left brachial plexus, and subsequent nerve excitability studies distal to the site of the tick bite demonstrated an abrupt increase in refractoriness (considered to be a marker of recovery from inactivation of Na+ channels), suggesting a defect of distal neural transmission (23). One case report was remarkable for prominent denervation, with a slow recovery, which could reflect a different form of tick paralysis (12).
Electrodiagnostic studies serve an important role in excluding other causes of ascending paralysis. The abnormalities seen in tick paralysis do not fulfill nerve conduction criteria for primary demyelination, thus, excluding acute inflammatory demyelinating polyradiculopathy (Guillain-Barré syndrome). Normal repetitive stimulation testing excludes myasthenia gravis and botulism, although some examples of botulism may not show a decrement or facilitation.
Ticks can be missed on CT or MRI, but in more than one case, a retrospective review of the cranial CT and MRI studies revealed superficial nodules on the scalp that correlated to the location of the attached tick (04; 21; 37).
|
• Weakness will progress to respiratory failure if the tick remains attached. | |
|
• Ticks responsible for tick paralysis are most commonly found embedded in hair or near the hairline and less commonly in the gluteal folds. |
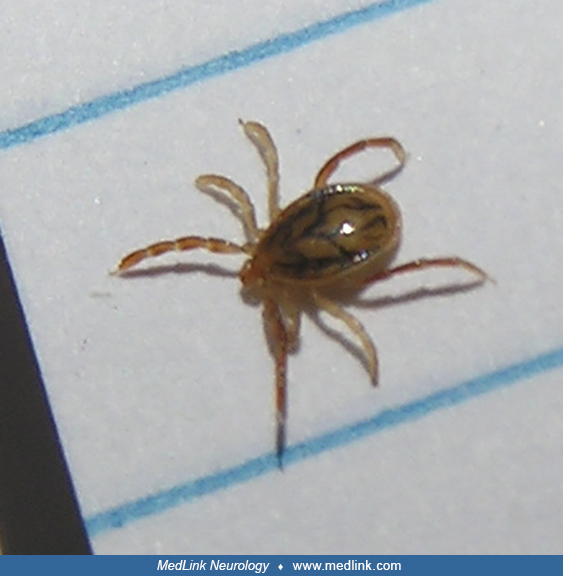
The key to the diagnosis and treatment is the discovery of the tick. Weakness will progress to respiratory failure if the tick remains attached (40; 30; 38). Indeed, the diagnosis has been made at autopsy (35). The engorged tick has a diameter of approximately 10 to 15 mm. It is most commonly found embedded in hair or near the hairline and is easily missed, but other overlooked sites include the gluteal folds (42; 24). Discovery may be largely accidental, and suspicion of the diagnosis requires searching the scalp with a fine-toothed comb (24; 16). If a tick is found, it is prudent to look for the possibility of additional ticks. Removal of the tick should include all parts; occasionally, portions of the mouth of the tick may remain and require excision. The best method of removal is to grasp the tick close to the skin with forceps and slowly pull the tick out (27).
Commercial antitoxin is available in Australia for I holocyclus-related tick paralysis and has been used when clinical symptoms are severe (18). Derived from hyperimmune canine serum, the dose is diluted 1 in 10 in Harman solution or normal saline and given intravenously. Patients must be watched for anaphylactic reactions and serum sickness. Treatment with adrenaline or antihistamines may be required. No antitoxin is available in the United States for D andersoni and D variabilis because symptoms resolve promptly after removal of the tick.
Tick paralysis is rare in women of reproductive age and, thus, little information is available.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Douglas J Lanska MD MS MSPH
Dr. Lanska of the University of Wisconsin School of Medicine and Public Health and the Medical College of Wisconsin has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Peripheral Neuropathies
Jan. 19, 2025
Peripheral Neuropathies
Jan. 19, 2025
Peripheral Neuropathies
Dec. 30, 2024
Peripheral Neuropathies
Dec. 30, 2024
Peripheral Neuropathies
Dec. 30, 2024
Peripheral Neuropathies
Dec. 30, 2024
General Neurology
Dec. 30, 2024
Infectious Disorders
Dec. 27, 2024