









General Neurology
Use of focused ultrasound in neurologic disorders
Jan. 13, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Organ transplantation is the last resort in patients having end-stage organ failure. Kidney transplantation is the most frequently performed transplantation. Liver, heart, and lung transplantation are also now routinely performed at many centers. Hematopoietic stem cell transplantation helps in restoring hematopoietic function in patients with severe hematological and immune disorders, and indications for transplantation are expanding to include other disorders such as multiple sclerosis. A variety of neurologic complications is encountered following all kinds of organ transplantation. Immunosuppressive drugs are also associated with various types of neurotoxicity.
A large number (30% to 60%) of transplant recipients experience neurologic complications of variable severity following solid-organ transplantation and hematopoietic stem cell transplantation. Seizures and encephalopathy are seen early in the posttransplant period. Organ transplant recipients are at risk of having opportunistic infections and other neurologic complications for several years after transplant. COVID-19 has a severe course in organ transplant recipients. Immunosuppressive neurotoxicity is responsible for additional complications. Posterior reversible leukoencephalopathy syndrome is seen following use of cyclosporine and tacrolimus (calcineurin inhibitors). Posterior reversible leukoencephalopathy syndrome presents with seizures and altered sensorium. Renal insufficiency and high blood tacrolimus levels significantly predict posterior reversible leukoencephalopathy syndrome among patients with lung transplantation. Prompt diagnosis of neurologic complications along with timely treatment is crucial to reduce the devastating morbidity and improve posttransplant survival. Metagenomic next-generation sequencing of cerebrospinal fluid has been found useful in organ transplant recipients who are likely to have a very wide variety of central nervous system infections.
|
• Approximately 30% to 60% of transplant recipients have some kind of neurologic complications. | |
|
• The risk of neurologic posttransplant complications can extend up to several years. | |
|
• The majority of posttransplant neurologic complications are either toxic, metabolic, or infective or are due to ongoing dysimmune regulation, resulting in either graft rejection or graft-versus-host disease. | |
|
• Seizures, stroke, encephalopathy, and opportunistic brain infections are frequent complications. | |
|
• Other complications include lymphoproliferative disorder, central pontine myelinosis, and central pontine myelinolysis (now more commonly known as osmotic demyelination syndrome). | |
|
• Immunosuppressants can cause neurotoxicity, ranging from mild tremors to posterior leukoencephalopathy syndrome. | |
|
• Liver transplants are more frequently associated with encephalopathy. | |
|
• Neurologic complications are associated with a high morbidity and mortality; therefore, prompt evaluation and treatment are imperative. |
Ancient Indian, Greek, Roman, and Chinese mythological accounts abound with many kinds of transplants, including those involving cadavers or animals (19). The first turning point for modern transplant practices was development of technique to perform vascular anastomoses. This Nobel Prize-winning technique was credited to a French doctor, Alexis Carrel. This surgical technique paved the way for solid-organ transplantation. Credit of first successful renal transplant, performed in 1954, is given to Dr Joseph Murray of the United States. Since then, kidneys have been the most frequently transplanted organ. Credit for the first liver transplant goes to Dr Thomas Starzl, who performed the transplant in 1963. Results were not encouraging initially, but now liver transplant is a successful treatment option for liver failure. Credit for the world's first heart transplant, done in 1967, is given to Dr Christiaan Barnard of South Africa. In the year 1963, a team of surgeons led by Dr. James D Hardy performed the first human lung transplant in the University of Mississippi Medical Center, United States. The discovery of cyclosporine, an immunosuppressant, brought a sea change in patient survival following organ transplantation. The development of organ transplantation roughly coincided with the concept of declaration of death by brain criteria.
Two common types of transplantation that are currently being practiced include-solid organ transplantation and hematopoietic cell transplantation. Solid-organ transplantation involves transplantation of kidney, liver, intestines, heart, lung, or pancreas. In stem cell transplants healthy stem cells are infused. Stem cells have capability to grow into any other cells. The prevalence of both hematopoietic cell and solid-organ transplantation is consistently increasing.
Both types of organ transplantation are associated with a variety of neurologic complications during the posttransplant period. A study observed that in 758 stem cell transplant recipients, 127 (16.8%) had some kind of infectious or noninfectious neurologic complication (64). In 971 consecutive patients with hematologic malignancies undergoing hematopoietic cell transplant, 149 (15.3%) patients reported neurologic complications during a median of 78 days after transplantation. Common central nervous system complications were encephalopathy, headache, stroke, seizures, posterior reversible encephalopathy syndrome, and myelopathy. Peripheral nervous system complications were neuropathies and myopathies and neuromuscular junction disorders, with 17% of the total peripheral nervous system complications being immune-related (09).
The differential diagnosis of central nervous system complications depends on the post-treatment timeline. Within 1 month posttransplant, infection and metabolic derangements contribute to altered sensorium. The highest risk for opportunistic infections affecting the central nervous system occurs within 1 to 6 months. After 6 months, differential diagnosis of central nervous system manifestations includes opportunistic infections, de novo malignancies, and metabolic abnormalities because of graft dysfunction (86).
The majority of neurologic complications in the posttransplant period occur within 30 days. The neurologic complications include seizures, encephalopathy, stroke, opportunistic infections, lymphoproliferative disorder, central pontine myelinolysis, and neurotoxicity caused by immunosuppressants (08; 57). The most significant differences between hematopoietic cell transplantation and solid-organ transplantation occur in the first few weeks after transplant (Table-1).
|
Period after transplant |
Within 1 month |
1 month to 6 months |
After 6 months |
|
Types of complications |
Metabolic derangements leading to encephalopathy |
Opportunistic brain infections |
Disseminated infections |
|
Type of transplant |
Less than 1 month |
1 month to 6 months |
More than 6 months |
|
Solid-organ transplantation |
Metabolic encephalopathy Postoperative delirium Posterior leukoencephalopathy syndrome Seizures, stroke, neuropathy, immunosuppressant drug toxicity |
Fungi (Aspergillus, Cryptococcus), Toxoplasma gondii, viruses (like JC virus or varicella zoster virus), bacteria (like Nocardia) Listeria monocytogenes Posttransplant lymphoproliferative disorder Posterior leukoencephalopathy syndrome |
Organ failure Central nervous system infections like Progressive multifocal leukoencephalopathy, West Nile virus Varicella zoster Toxoplasmosis Aspergillosis Metabolic syndromes Posttransplant lymphoproliferative disorder Autoimmune encephalopathy, neuropathy and myopathy |
|
Allogeneic hematopoietic stem cell transplantation |
Stroke and seizures Posterior leukoencephalopathy syndrome Metabolic encephalopathy Pancytopenia leading to intracerebral hemorrhage and subdural hematoma cerebral venous thrombosis Nosocomial viral infection (HHV-6), such as viral, bacterial, and fungal infections, and toxoplasmosis Immune-mediated transverse myelopathy and cerebellar syndrome Peripheral neuropathy |
Fungal infections like aspergillosis and Candida Viral infections like HHV-6 encephalitis Immune mediated central and peripheral nervous system disorders Transplant-associated microangiopathy |
Chronic graft versus host disease Inflammatory autoimmune neuropathy and myopathy Inflammatory immune reconstitution syndrome Posttransplant lymphoproliferative disorder Neoplasms like lymphoma |
|
| |||
Seizures. Seizure disorder is a common neurologic complication in many posttransplant patients. Seizures are most common in liver and then heart recipients. Seizures in these patients are usually generalized. Immunosuppressant drug toxicity as well as metabolic abnormalities, such as hyponatremia, hypomagnesemia, hypoglycemia, and hyperammonemia, are often responsible for generalized seizures. In many patients, focal brain lesions (eg, hemorrhage, infarct, fungal abscess and de novo neoplasms) can cause focal seizures (44). Seizures are relatively uncommon in allogeneic hematopoietic stem cell transplantation.
Cerebrovascular complications. Ischemic stroke and intracerebral hemorrhage have been reported as complications of both solid-organ transplantation and hematopoietic stem cell transplantation. Strokes typically occur in the setting of hypertension, diabetes, cardiac arrhythmias, coagulation disturbances, bacterial endocarditis, and accelerated atherosclerosis, which may be pre-existing or may develop after transplantation. Heart transplanted patients are particularly vulnerable for cerebrovascular accidents (08; 57). Cerebrovascular complications are particularly common following hematopoietic stem cell transplantation. In a retrospective evaluation, 20 patients (4.4%) out of 459 adult patients who underwent allogeneic hematopoietic stem cell transplantation developed cerebrovascular complications. All cerebrovascular accidents occurred in the first 2 years after transplant. Intracranial hemorrhages were more frequent than cerebral infarction (45).
Encephalopathy. Encephalopathy is generally an early complication and seen within the first month after transplantation. Posterior reversible encephalopathy syndrome is a rapidly developing condition that is characterized by headache, seizures, altered consciousness, and visual abnormalities. Neuroimaging characteristically shows dominantly white matter edema symmetrically involving the parieto-occipital regions of the brain. If promptly diagnosed and managed, the condition is completely reversible (47). Metabolic derangements, cerebrovascular accidents, central nervous system opportunistic infections, and neurotoxicity of immunosuppressant drugs are often held responsible.
|
• Seizures and status epilepticus |
Osmotic demyelination syndrome. Also known as central pontine myelinolysis, osmotic demyelination syndrome is a devastating neurologic deficit seen after rapid correction of hyponatremia. In a large retrospective series, among 997 posttransplant patients, central pontine and extrapontine myelinolysis were seen in 11 patients (1.1%) (21). The common clinical presentation of central pontine myelinolysis is altered sensorium, possibly progressing to locked-in syndrome. Central pontine myelinosis is more frequent in liver transplanted patients. Rapid correction of hyponatremia is considered responsible for this devastating complication (20).
Akinetic mutism. Akinetic mutism is a severe disabling condition characterized by inability to move (akinesia) and inability to communicate by speaking (mutism). Patients can communicate by ocular movements. Calcineurin inhibitor-induced neurotoxicity can occur after renal transplantation, despite normal serum levels (76; 51). Akinetic mutism is an exceptional manifestation of tacrolimus neurotoxicity.
Prompt recognition of the condition and timely withdrawal of tacrolimus can lead to reversal of the condition (69).
Opportunistic brain infections. Immunosuppression following organ transplantation increases the risk for opportunistic central nervous system infection and is associated with high mortality. Virus and fungal infections are the most frequent opportunistic brain infections in the organ-transplanted population. Bacterial and protozoal infections less frequently affect the central nervous system. Donor-derived infections, in many cases, result in central nervous system infection in organ recipients. Common pathogens thus transmitted are Balamuthia mandrillaris, Cryptococcus neoformans, lymphocytic choriomeningitis virus, and West Nile virus (38).
Virus infections. Transplant recipients have a higher risk of neurologic complications from West Nile virus infection. West Nile virus infection often presents as meningitis, encephalitis, or myelitis. In areas where West Nile virus is endemic, clinicians should have a high index of suspicion when treating patients presenting with febrile encephalopathy (85; 87; 33).
Progressive multifocal leukoencephalopathy is a fatal demyelinating disorder of the brain following immunosuppression after organ transplantation. Progressive multifocal leukoencephalopathy is caused by reactivation of the JC virus in an immunocompromised host. Progressive multifocal leukoencephalopathy clinically manifests with changes in personality, cognitive abnormalities, focal neurologic deficits, gait abnormalities, and cortical vision loss. MRI shows multiple subcortical white matter signal changes on T2-weighted and FLAIR imaging. There is, classically, no contrast enhancement or mass effect (90; 16). However, contrast enhancement can be seen when immunosuppression is reduced to combat the viral infection and if phenomenon of immune reconstitution inflammatory syndrome takes place.
In 2004, four recipients of organ transplants from a common organ donor died of unexplained encephalitis. Encephalitis developed within 30 days after transplantation. All four patients died within 2 weeks. Extensive testing demonstrated rabies virus both in donor and all the recipients (72).
The precise impact of COVID-19 on organ transplant recipients is not precisely known. The evidence on COVID-19 infections in kidney transplant recipients is limited to case reports and case series. A preliminary report suggests that SARS‐CoV‐2 infection has a severe course in solid organ transplant recipients (27). COVID-19 has been associated with acute hemorrhagic necrotizing and hypoxic encephalopathy in a heart transplant recipient (37). Westhoff and colleagues described meningoencephalitis and viral invasion of allograft in a patient who had received kidney and pancreas transplant 13 years ago (82). The patient presented with COVID-19 pneumonia along with impaired pancreas and kidney allograft function. Kidney biopsy showed tubular damage, and an interstitial mononuclear cell infiltrate and reverse transcriptase polymerase chain reaction test for SARS-CoV-2 in the biopsy specimen was positive. In addition, the patient had meningoencephalitis and SARS-COV-2 was demonstrated in CSF (82).
Infrequently, Epstein-Barr virus-related neurologic complications can pose diagnostic challenge. Ridha and colleagues described three patients with Epstein-Barr virus-related neurologic complications. One patient had myelitis, and another patient had Epstein-Barr virus encephalitis. Epstein-Barr virus-associated primary central nervous system posttransplant lymphoproliferative disorders can also have isolated neurologic involvement (10; 61).
Human herpesvirus 6 is an emerging viral infection responsible for a variety of central nervous system manifestations. Human herpesvirus 6 is frequently isolated from hematopoietic stem cell transplant recipients. This virus is less frequently noted in solid organ transplant recipients. Patients with human herpesvirus 6 typically present with encephalitis (88).
Bacteria. Nocardiosis is an opportunistic infection caused by Nocardia, a gram-positive Actinomycetes, that is likely to affect transplant recipients. The common sites of infection are lung, brain, and skin. Nocardial infection often manifests as single or multiple brain abscesses. Nocardia farcinica is most frequent Nocardia species to cause brain lesions. Many patients have asymptomatic nocardial brain lesions. Nocardiosis, in hematopoietic cell transplanted host, is primarily a lung infection with frequent dissemination. Many patients have asymptomatic nocardial brain lesions. It is recommended that neuroimaging should always be performed in hematopoietic cell transplanted host with nocardiosis regardless of neurologic symptoms (07). In multivariable analysis, high calcineurin inhibitor levels, tacrolimus, and high-dose corticosteroids, higher patient age, and a longer stay in the intensive care unit are associated with development of nocardiosis (18; 17).
Listeria monocytogenes is an uncommon cause for brain involvement in organ transplanted patients. Listerial meningoencephalitis, rhombencephalitis, and listerial brain abscesses are rare and are found mostly in patients with solid-organ transplants. Listerial brain abscesses manifest as single or multiple brain abscesses (73; 77).
Tuberculosis is a major opportunistic infection seen in solid-organ transplanted patients. Extra pulmonary, miliary, and disseminated forms of tuberculosis are frequently reported in these patients (52; 04). Given the similarity of the clinical presentation of CNS tuberculosis to other neurologic opportunistic infections, especially cryptococcal meningitis and cerebral toxoplasmosis, a high index of suspicion should be maintained for other opportunistic infections.
Fungus. Solid-organ transplant recipients are at enhanced risk of life-threatening invasive fungal disease. The posttransplant population is at a significantly increased risk for a variety of fungal infections of brain (75).
Cryptococcal meningitis (caused by Cryptococcus neoformans) is particularly common in Kidney transplanted patients (29). In a retrospective series of 500 kidney transplantations in Portugal, six patients developed infections with Cryptococcal neoformans, with an incidence of 1.2% (three disseminated, two meningeal, and one cutaneous) (46). Cryptococcal meningitis clinically manifests with headache, fever, confusion, behavioral abnormalities, and focal neurologic deficits. For a prompt diagnosis, lumbar puncture with measurement of CSF opening pressure and cryptococcal antigen assay is required. India ink staining remains a more frequently used diagnostic method for diagnosing cryptococcal meningitis.
Aspergillosis is caused by the fungus Aspergillus fumigatus. Invasive aspergillosis in organ transplanted patients with severe immunosuppression is associated with exceptionally high mortality. Aspergillus is the most frequent fungus causing brain abscesses in organ transplanted patients (53). Intracranial aspergillosis presents either as meningitis, mycotic aneurysms, infarctions, or mass lesions. Aspergillus fungus is highly angioinvasive, resulting in large hemorrhagic infarctions and single or multiple brain abscesses (63). Simultaneous lung involvement is seen in a majority of patients with intracranial aspergillosis. Intracranial aspergillosis clinically presents with rapidly evolving altered sensorium, seizures, and focal neurologic deficits. Diagnosis is confirmed on demonstration of fungus in biopsied brain tissue.
Mucormycosis is an invasive fungal infection, caused by the “Mucormycetes” group of fungi. Mucormycetes are ubiquitous organism and are present in soil. A large number of patients of mucormycosis have been reported in association with Covid-19. Mucormycosis generally affects the nasal sinuses and eyes. Mucormycosis frequently affects the brain and dominantly affects the cavernous sinus region. If cerebral mucormycosis it not promptly recognized and treated, disease is universally fatal. Many reports of mucormycosis have also been described in organ transplant recipients who were treated for Covid-19 (05; 39).
Protozoa. Toxoplasmosis, caused by Toxoplasma gondii, is the most common protozoal brain infection in organ transplanted patients. The liver is a frequent site of cyst carriage, confirming that transplantation of an organ from a seropositive donor to seronegative recipient brings high risk for acquired toxoplasmosis (06). A total of 87 toxoplasmosis cases were recorded (58 hematopoietic stem cell transplant, 29 solid-organ transplants); the 6-month survival rate was lower among Toxoplasma-seropositive recipients and among hematopoietic stem cell and liver recipients (62). Toxoplasmosis is clinically characterized with fever, headache, seizures, altered sensorium, and focal neurologic deficits. Infrequently, the disease is disseminated and presents as encephalitis. The diagnosis of toxoplasmosis is confirmed with the demonstration of Toxoplasma gondii organisms in blood, body fluids, or tissue. Neuroimaging in patients with toxoplasma encephalitis reveals multiple ring-enhancing lesions. In patients who have Toxoplasma antibodies in serum and multiple ring-enhancing lesions of brain, the diagnosis of toxoplasma encephalitis is quite certain.
Amebic encephalitis is a rare but universally fatal form of encephalitis seen infrequently in organ transplanted patients. Balamuthia mandrillaris infection is transmitted through organ transplantation with an observed incubation time of 17 to 24 days (26). Balamuthia mandrillaris presents with encephalitis with multiple ring-enhancing lesions on imaging. Frequently, diagnosis is confirmed on autopsy. Histopathology reveals Balamuthia mandrillaris in either brain tissue or cerebral spinal fluid in the donor and recipients. Balamuthia mandrillaris encephalitis is clinically characterized with headache, altered mental status, and focal neurologic deficit. CSF examination shows pleocytosis and elevated protein. Neuroimaging reveals multiple enhancing lesions of brain. The treatment for Balamuthia mandrillaris encephalitis is unknown (26).
De novo brain malignancies. Organ transplant recipients are at a high risk of de novo brain malignancies. The most frequent malignancies of the brain seen in these patients are central nervous system lymphomas and metastatic tumors. Life-long screening for malignancies is warranted for all transplantation survivors (58; 22).
Neurotoxicity associated with immunosuppressants. Immunosuppressive agents have brought a sea change in the scenario of organ transplantations. Cyclosporine and tacrolimus are two most commonly used agents. Both, cyclosporine and tacrolimus belong to the calcineurin inhibitor group of drugs. Cyclosporin causes neurologic side effects in up to 40% of patients. A reversible posterior leukoencephalopathy syndrome is the most frequent complication (31). Other neurotoxicity can manifest with tremor, acute confusional state, status epilepticus, and speech abnormalities (84; 11). Long-term calcineurin inhibitor administrations are associated with an increased risk of cognitive abnormalities (54). Tacrolimus is also associated with similar kind of neurotoxicity (68) (Table-2).
Vaccine-associated neurologic complications. Hughes and colleagues described a 65-year-old male liver transplant recipient who developed areflexic quadriparesis after first dose of the Pfizer-BioNTech mRNA COVID-19 vaccine administration (36). Nerve conduction examination confirmed acute inflammatory demyelinating neuropathy changes consistent with Guillain-Barré syndrome.
Lung transplantation. In a cohort of 759 lung transplanted patients, 70 (9.2%) patients had neurologic complications within 2 weeks after transplantation. The most common neurologic complications were stroke and severe toxic or metabolic encephalopathy. Advanced age, past coronary artery disease, prolonged use of cardiopulmonary bypass, and severe primary graft dysfunction increased the risk for death in patients with early major neurologic complications (67). Mayo Clinic Lung Transplant Registry (1988 to 2008) observed much more frequent neurologic complications following lung transplant. Among 120 lung transplant recipients, 95 experienced a neurologic complication, mostly in the form of perioperative stroke or encephalopathy (48). Neurologic complications were recorded in 68% of lung transplant recipients in a cohort of 132 lung allograft recipients at the University of Pittsburgh Medical Center USA, with follow up ranging 2 to 4 years. The most common complications were anoxic encephalopathy and injury to the phrenic and recurrent laryngeal nerves, generalized neuromuscular complications, and headache. In many cases, neurologic complications were considered to be caused either by immunosuppressant neurotoxicity or an opportunistic infection (92).
Renal transplantation. Frequently, associated illnesses like hypertension, diabetes, and cardiovascular and cerebrovascular disease contribute to some neurologic complications in the kidney transplanted population. In addition, prolonged dialysis leads beta2-microglobulin accumulation in tissues and subsequently dialysis-related amyloidosis. Amyloidosis can present with carpal tunnel syndrome and other neuropathies. Dialysis itself can directly or indirectly be associated with many of the neurologic complications in these patients (12; 58; 50). Seizures due to posterior reversible leukoencephalopathy syndrome are the commonest acute complication in the kidney transplant population (30). Femoral nerve neuropathy is an infrequent complication after kidney transplantation. Femoral nerve is involved because of nerve damage from pelvic surgery. Other factors that can play a role in the pathogenesis of femoral nerve neuropathy are direct ischemia of the nerve by clamping of the iliac artery and hematoma formation in the retroperitoneum or psoas muscle (80; 40).
Liver transplantation. The three most common reasons for orthotopic liver transplantation are alcoholic cirrhosis, primary biliary cirrhosis, and hepatitis B or C. Acute liver failure due to acetaminophen ingestion accounts for another large group. Central pontine myelinolysis and metabolic encephalopathy, including hyperammonemic encephalopathy, are particularly common among liver transplanted patients. Compared to the transplantation of other solid organs, liver transplant is associated with a higher incidence of neurologic complications (43). In a cohort of 242 pediatric liver transplanted patients, neurologic events occurred in 57 (23.5%) of the patients. Encephalopathy and seizures are the most frequent neurologic events (35). Even in adults, metabolic encephalopathy with altered consciousness is the most common neurologic complication in acute stages (28; 41).
Heart transplantation. Neurologic complications in orthotopic heart transplantation adversely affects the prognosis in the posttransplant period. The most frequent neurologic complications are encephalopathy and stroke. Hemodynamic instability, cardiac arrest, extracorporeal circulation, stroke, and carotid stenosis are risk factors (03). In a retrospective study with data of 314 patients, stoke occurred in 20% of patients. Ischemic stroke was the most common subtype (78). Early strokes were associated with decreased 1-year survival (01; 13). Toxoplasmosis is a unique infectious risk, as the parasite can be in the transplanted myocardium and can become symptomatic within the first 3 months after transplantation.
Allogeneic hematopoietic stem cell transplantation. Neurologic complications adversely affect morbidity and mortality after hematopoietic cell transplantation. In a cohort of 263 hematopoietic stem cell transplanted patients, 50 patients experienced neurologic complications. One-year and 5-year cumulative incidences of all neurologic complications were 15.6% and 19.2%, respectively. Risk factors for were age, development of acute graft-versus-host disease reaction type III-IV, thrombocytopenia, and delayed platelet engraftment. Infection, intracranial hemorrhage, ischemic stroke, metabolic encephalopathy, posterior reversal encephalopathy syndrome, seizure, and peripheral neuropathy were common complications (25).
Wieczorek and colleagues retrospectively analyzed neurologic complications among 2384 adult patients transplanted in seven Italian institutions (83). In this cohort, 93 (3.9%) of patients experienced one or more neurologic complications the during follow-up period. These complications were either infectious, immune/inflammatory, drug-related, cerebrovascular, metabolic, related to pre-existing central nervous system disease relapse and malignancy, or undefined in nature. Six patients (6.4%) had neurologic manifestations because of chronic graft-versus-host disease. The overall mortality because of neurologic complications was 22.6% during a median follow-up period of 25.4 (0.4 to 163) months (83).
Graft-versus-host disease. Graft-versus-host disease is a severe immune disorder that can variably affect multiple organs. It is seen following allogeneic hematopoietic stem cell transplantation, and many neurologic complications may be associated with it. Many immune-mediated neuromuscular complications, like neuropathies, myopathy, and myasthenia gravis, and many central nervous system complications, like, stroke, demyelinating disorders, and encephalitis, are reported (34; 42).
Neurologic complications following organ transplant are cause of serious concern as they adversely affect morbidity and mortality, both in the immediate posttransplant period and several years after the transplant (59). Neurologic complications are associated with a significantly adverse morbidity and mortality after hematopoietic cell transplantation. Neurologic complications lead to poorer progression-free survival, overall survival, and non-relapse mortality. Prompt diagnosis and treatment of posttransplant neurologic complications help in reducing both morbidity and mortality (25).
Other long-term problems frequently seen in the organ transplanted population are adverse effects of continued treatment. The most commonly used antiepileptic drug used in transplanted patients is phenytoin. Phenytoin toxicity can produce nystagmus, dysarthria, and ataxia and may even lead to coma. Intravenous phenytoin may be complicated by the purple glove syndrome. Long-term usage of corticosteroids may be associated with psychotic reactions, steroid myopathy, and critical illness polyneuropathy. Serotonin reuptake inhibitors may be associated serotonin syndrome. Late-onset infections months after transplantation are likely. These infections usually occur after allograft procedures in association with graft-versus-host disease or after therapy for graft-versus-host disease.
Patients with hematopoietic stem cell transplants may experience severe cancer chemotherapy-related organ toxicity. These patients receive large doses of anticancer drugs for the treatment of cancer or conditioning for transplantation, graft-versus-host disease, or posttransplantation immunosuppression. There can be many systemic complications after hematopoietic stem cell transplantation. Posterior subcapsular cataract and keratoconjunctivitis sicca or dry eyes are common in hematopoietic stem cell transplantation recipients. Total-body irradiation is the predisposing risk factor. Other ocular adverse effects are retinopathy, infectious retinitis, and retinal hemorrhage. Chemotherapy and total-body irradiation may have adverse effects on fertility and high risks for teratogenicity. Bronchiolitis obliterans is a specific form of obstructive lung disease after hematopoietic stem cell transplantation and is associated with a fatality rate of 50%. Other lung complications are viral, bacterial, or nocardial pneumonia, acute respiratory distress syndrome, pulmonary embolism, hemorrhagic alveolitis, and congestive cardiac failure. Osteopenia, osteoporosis, and avascular necrosis are common. Musculoskeletal effects may cause adverse effects following hematopoietic stem cell transplantation. There is risk of substantial decline of neurocognitive abilities following chemotherapy and total-body irradiation. Superficial siderosis, clinically manifesting with deafness, ataxia, and myelopathy, is a newly recognized syndrome following hematopoietic stem cell transplantation (59; 60; 49; 71).
Immunosuppression is the risk factor for almost all the neurologic complications in patients who have undergone organ transplantation. Incidence of various neurologic complications are directly proportional to degree of immunosuppression. Corticosteroids, anti-inflammatory drugs (azathioprine and mycophenolate), calcineurin inhibitors (cyclosporine and tacrolimus), and mechanistic target of rapamycin (TOR) inhibitors (sirolimus and everolimus) are all associated with a variety of neurologic complications. Ueno and colleagues noted that tacrolimus induced encephalopathy in 5% of patients after pediatric living donor liver transplantation (79). In a cohort of 128 pediatric liver transplanted patients, six developed encephalopathy. Encephalopathy generally developed within 2 weeks of transplantation. Imaging changes consistent with posterior reversible encephalopathy syndrome was seen in three patients. Tacrolimus was withdrawn, which reversed encephalopathy in the majority. Reinstitution of tacrolimus therapy was safely done without any new neurologic complication (79).
In 2015, globally 126,670 solid-organ transplants were performed; the highest number of them were kidney transplants (32).
Incidence of neurologic complications following solid-organ transplantation is very high. Neurologic complications affect 30% to 60% of solid-organ transplantation recipients (08). Even hematopoietic cell transplantation recipients have a high incidence of neurologic complications. In a retrospective study of 263 patients, 50 patients experienced 63 neurologic complications following hematopoietic cell transplantation. The 1- and 5-year incidences of all neurologic complications were 15.6% and 19.2%, respectively (25). Liver transplantation is associated with a high incidence of neurologic complications. In a retrospective study of 242 patients, neurologic complications were reported in 57 (23.5%) of the patients (35). In another cohort of 443 liver transplant recipients that included 307 adults and 136 children, incidence of neurologic complications was similar: adults 15% (n = 41) and children 16% (n = 20). A complete neurologic recovery was recorded in 62% and 95% of the patients (55). A prospective study recorded higher incidence. Among 176 liver transplanted patients, neurologic complications occurred in 74 (42%) of the patients (24). A chart review of 175 renal transplant recipients revealed that 22 patients (12.5%) had neurologic disorders during their follow up. Cyclosporin-induced tremor occurred in almost all patients (02). Some reports suggest that neurologic complications occur in 9 of 10 kidney transplant recipients (56). Neurologic complications often occur following cardiac transplantation. In a series of 205 orthotopic heart transplant patients, 95 patients (48%) had neurologic complications (14). Cerebrovascular complication rate ranges between 5% and 11% (03). Even after lung transplantation, many patients experience some kind of neurologic complications; a retrospective chart review of 276 patients revealed that 123 (45%) patients had neurologic complications (70).
A rigorous screening of every donor for any existing infection is crucial. The transplant team should remain alert to possible local environmental and nosocomial pathogens and should take prompt measures to recognize and treat them. A preoperative assessment for preexisting neurologic disorders is crucial as it can predict central or peripheral nerve dysfunction in the posttransplant period. Prompt diagnosis is needed to effectively handle otherwise potentially lethal central nervous system complications.
For example, early wound debridement of bacterial and fungal cutaneous lesions may be required for diagnosis to prevent them from being invasive. Recommended vaccination guidelines meant for organ transplant recipients and their households, including pets, should be strictly followed (23).
Clinicians should have a strong suspicion for any opportunistic central nervous infections in organ transplant recipients. The initial diagnostic work-up must include neuroimaging, cerebrospinal fluid analysis, and an evaluation for systemic infections.
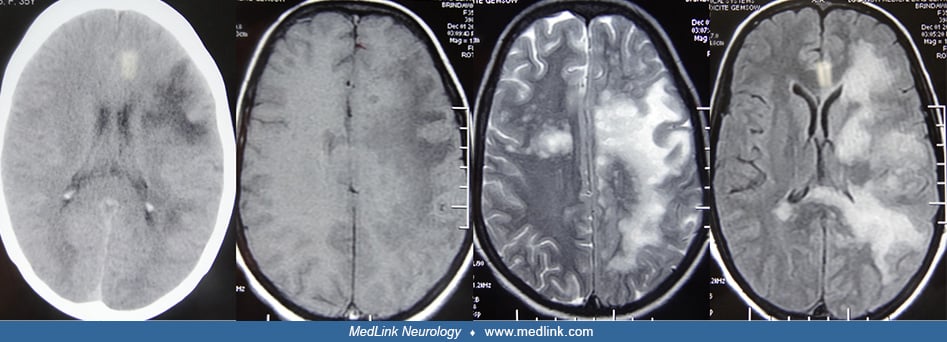
Neuroimaging. Magnetic resonance imaging is the superior imaging technique in accurately identifying many posttransplant complications in the brain. Magnetic resonance imaging data in 31 heart transplant patients revealed imaging abnormalities in 12 patients. The most common abnormality was posterior reversible leukoencephalopathy syndrome; other abnormalities were ischemic stroke, hemorrhagic stroke, intracranial abscess, and intracranial dissemination of sinusoidal fungal infection and related hemorrhagic infarct (78). A retrospective study noted that a presence of renal insufficiency and high blood tacrolimus levels were significantly associated with posterior reversible leukoencephalopathy syndrome among patients with lung transplantation (89).
Single or multiple ring-enhancing lesions have a long list of differential diagnoses, including bacterial, fungal, or nocardial abscess, tuberculoma, amebic toxoplasmosis, and metastasis. Diffusion-weighted imaging is helpful in distinguishing between tumor and abscess.
Lesions of toxoplasmosis preferentially affect basal ganglia but can be widespread (66).
White matter T2 hyperintensities with or without minimal enhancement have extensive differential diagnostic possibilities. White matter T2 hyperintensities are widespread in progressive multifocal leukoencephalopathy and are the most important differential diagnosis.
In posterior reversible encephalopathy syndrome, white matter T2 hyperintensities symmetrically involve the posterior parieto-occipital cortex.
Patchy areas of signal change in the pons are consistent with central pontine myelinolysis (66).
Patchy areas of gray matter hyperintensity and enhancement are seen in a variety of viral, bacterial, autoimmune, and carcinomatous encephalitis. A large cerebral infarct or hematoma results from either a cerebrovascular event or focal vascular invasion by Aspergillus fungus. Patchy or diffuse meningeal enhancement is seen in a variety of neurologic complications, including viral, bacterial, and carcinomatous encephalitis (66).
Metagenomic next generation sequencing. Metagenomic next-generation sequencing of cerebrospinal fluid is an upcoming promising technology, which has potential to detect a broad range of organism in a single platform. Metagenomic next-generation sequencing is particularly useful in organ transplant recipients who are likely to have a very wide variety of central nervous system infections (15; 91).
Brain biopsy. Brain or meningeal biopsy is needed in certain circumstances to establish the diagnosis. Debridement of fungal or bacterial abscess have both diagnostic and therapeutic advantage.
Seizure may lead to inadvertent serious medical complications like aspiration and can result in prolonged altered sensorium. In acute conditions, benzodiazepines (like lorazepam) is a preferred drug. For prolonged seizure prophylaxis, conventional antiepileptic drugs phenytoin, valproate, phenobarbital, and carbamazepine are not suitable because they are metabolized in the liver. Many of these drugs have potential to increase liver enzyme induction that can affect activity of immunosuppressive drugs. Levetiracetam is the current drug of choice for posttransplant seizures. Treatment of posterior reversible encephalopathy syndrome requires immediate treatment of hypertension, meticulous fluid and electrolyte balance, and adjustments in doses of calcineurin inhibitor.
The most important risk factors for the development of osmotic demyelination syndrome is severe pretransplant hyponatremia (less than 125 m Eq/L). Meticulous fluid and electrolyte management is needed to prevent the development of osmotic demyelination syndrome, both during and after transplant surgery (20).
If the central nervous system is suspected, empiric broad-spectrum antimicrobial therapy should be started. Vancomycin plus third-generation cephalosporins are preferred antibiotics for bacterial infections. Listeria monocytogenes infection requires ampicillin. Fungal infections require treatment with liposomal amphotericin and 5-flucytosine. Voriconazole is used for aspergillosis. Toxoplasma gondii infection is treated with pyrimethamine plus sulfadiazine. The treatment for progressive multifocal leukoencephalopathy is reduction in immunosuppression. No antiviral drug has shown any efficacy in this condition. Many other viral infections require treatment with acyclovir or ganciclovir (86).
Neurologic complications in the posttransplant period adversely affect morbidity and mortality. Many opportunistic infections and cerebrovascular events are often associated with high death rates.
Pregnancy after kidney transplantation is associated with serious maternal and fetal complications. For posttransplant women who have already given birth, it is worth considering contraceptive counseling because these women more often choose to not attempt another pregnancy (74). Preeclampsia commonly complicates pregnancies after renal transplantation but is not associated with serious complication (81). Vaginal delivery should always be contemplated and cesarean delivery is reserved only for genuine obstetric need. Toxic effects of immunosuppressive drugs exposed in utero and during breast feeding and its long-term effects in the offspring need to be considered.
A meticulous preoperative assessment is needed to identify risk factors, to improve cardiac conditions, to treat acid-base balance, and to administer the most appropriate perioperative therapy regime. Preoperative care in a kidney transplant candidate requires optimal care for the living donor, the avoidance of nephrotoxic drugs, a goal-directed hemodynamic management strategy, and optimized postoperative care. All these measures may improve outcome after renal transplant surgery (65).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Ravindra Kumar Garg DM
Dr. Garg of King George's Medical University in Lucknow, India, has no relevant financial relationships to disclose.
See Profile
Amy A Pruitt MD
Dr. Pruitt of the University of Pennsylvania School of Medicine has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 07, 2025
General Neurology
Dec. 30, 2024
General Neurology
Dec. 13, 2024
General Neurology
Dec. 13, 2024
Neuromuscular Disorders
Dec. 09, 2024