




Movement Disorders
Acquired hepatocerebral degeneration
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
In this article, the author reviews new studies related to the pathogenesis of essential tremor, including Purkinje cell pathology as well as LINGO1 and SLC1A2 genes. Clinical diagnosis of tremor disorders and treatment strategies for essential tremor are described in detail.
|
• Two subtypes of essential tremor pathology have been identified: a primarily cerebellar variant with Bergmann gliosis and Purkinje cell torpedoes, and a Lewy body variant. | |
|
• Propranolol and primidone are useful first-line medications for essential tremor. | |
|
• Deep brain stimulation surgery continues to be useful for severe, medication-resistant tremor. |
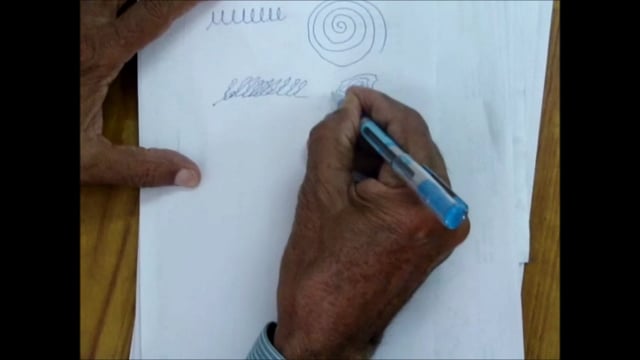
The history of tremor can be roughly divided into two phases. The first and largely descriptive phase began in the 19th century; clinicians were able to recognize the principal manifestations of tremor and characterize and classify different forms of tremor based on clinical patterns and their relationships with known pathologies. GF Most provided one of these reports of action tremor in 1836. The first known use of the term “essential tremor” was traced to Pietro Burresi in 1874 (143). The names of Romberg, Parkinson, Gowers, and Charcot all contributed extensively to our knowledge and laid the groundwork for the second phase. Charcot collected handwriting samples from his patients and differentiated between tremulous handwriting in essential tremor and micrographic handwriting in Parkinson disease (76). Gowers described rest tremor at the metacarpal-phalangeal joints as someone beating a small drum (76).
The second phase began in the latter part of this century with the explosion of newer technologies that were able to further identify the pathophysiology of tremor. This explosion also contributed to our further ability to carefully classify clinical syndromes not only in terms of their phenomenology and pathology but also their neurophysiology. This phase has led to significant improvements and advances in treatment culminating presently with surgical therapies and deep brain stimulation.
Descriptions of the contributions of early American investigators to the understanding of tremors (117), and documentation of essential tremor in Samuel Adams, an early American patriot (133), provide an interesting historical perspective on tremor.
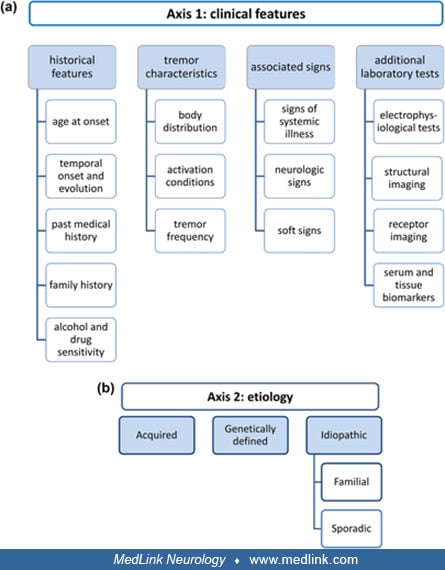
The diagnosis, classification, etiology, pathophysiology, and treatment have been controversial in the past, but progress has been made in all of these parameters. The 2018 Consensus Statement from the International Parkinson and Movement Disorder Society retains characteristic tremor syndromes but also evaluates them on clinical characteristics on Axis 1 and etiology on Axis 2 (22).
The concept of essential tremor as a single, monosymptomatic entity has changed over time (65; 137). The 2018 consensus statement addresses this heterogeneity by recognizing that there may be additional features such as dystonia, bradykinesia, cognitive impairment (Axis 1), and a heterogenous etiology (Axis 2). This improved classification system should allow for more success in clinical research of essential tremor. Given the significant potential for disability in both social and occupational settings due to tremor (61), the word “benign” was removed from the term “benign essential tremor” (153).
Tremor is the most common of all the movement disorders and is a common complaint in patients attending a general neurology clinic and the most common reason for consultations for movement disorder specialists.
It is defined as an involuntary, rhythmic oscillation of a functional body region produced by alternating or synchronous contractions of reciprocally innervated agonist and antagonist muscles (97; 43). Tremor is distinguished from other movement disorders by its rhythmicity. Signs related to tremor include tone defined as increased resistance encountered by the examiner when the limb or body part is moved about a joint in a relaxed state. Froment sign is an increase in resistance to passive movement of a limb about a joint enhanced when there is voluntary activity of another body part. Coactivation is defined as the occurrence or worsening of tremor when tone increases in the respective limb as the examiner feels the patient struggling against resistance. It is prominent part of psychogenic tremor. Dystonia is defined as muscle contraction resulting in twisting and repetitive movements or abnormal postures (45). Some patients describe “internal tremor,” which may not be observable to others (36).
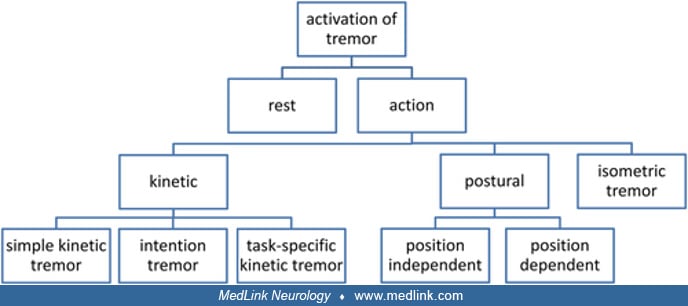
Clinical assessment. The clinical assessment of tremor relies heavily on the topography (ie, limb, truncal, or head tremor). Other parameters include activation and frequency of the tremor (less than 4 Hz is low frequency; 4 to 7 Hz is medium frequency; and greater than 7 Hz is high frequency). The patient should be observed sitting with the arms resting on the legs and in a relaxed posture in a chair. This position was shown via accelerometry to demonstrate the highest amplitude of Parkinson disease rest tremor (232). Patients should then be requested to elevate the arms against gravity and observe with fingers apart. The patient is then asked to assume the “wing beating position” in which the arms are abducted to 90 degrees, the elbows flexed with the fingers pointing toward each other, noting whether this accentuates the tremor and whether the tremor is primarily proximal or distal and significant asymmetries. The patient is then asked to execute kinetic movements, most commonly being the finger-to-nose test. They are then requested to do specific functions, such as drinking from a cup with either hand, having a cup in each hand and pouring water from one to the other, writing a sentence, and copying a concentric Archimedes spiral. They should then be observed walking looking for evidence of posturing, arm swing, ataxia, and whether there is a gait-activated tremor. If there is an associated head and voice tremor, have the patient read and count as well as maintain a sustained letter sound "E." “Tremor rating scales are discussed in the Diagnostic workup” section.
Important data from the history to complete the assessment include the age of onset and the pace of evolution. Family history of the tremor is key, as is the sensitivity of alcohol (171). The anatomic sequence of spread should be documented as well as the medical treatments tried in the past, noting those that have helped or failed. Concerns about potential alcohol abuse should be addressed (45; 171). Hopfner and colleagues compared groups of early onset to late onset essential tremor. Early onset patients were more likely to have a positive family history and alcohol sensitive tremor, whereas tremor progression was faster in late onset essential tremor (89).
Physiologic and enhanced physiologic tremors. Physiologic and enhanced physiologic tremor is characterized by relatively fast frequencies (7 to 12 Hz). Physiologic tremors are present in many normal persons and generally have no clinical significance. The enhanced physiologic tremor is mainly postural, of high frequency between 7 and 12 Hz and relatively low amplitude. Typically, it is aggravated by endogenous or exogenous substances such as drugs, alcohol withdrawal, or hyperthyroidism. They are generally reversible, often occurring under conditions of stress, fatigue, anxiety, or hypoglycemia.
Essential tremor. Essential tremor is characterized by a postural tremor largely of the upper extremities but may also involve the head and voice. It is often accompanied by a kinetic tremor. It is the most common involuntary movement disorder afflicting approximately 1 million people in the United States. The estimated prevalence of essential tremor is 0.9% (95% CI 0.5% to 1.5%). Prevalence increases with age, to 4.6% in the 65 and older age group (134). There is a positive family history in first order relatives of about 60% to 70%. When the family history has been adequately elucidated, it generally is inherited as an autosomal dominant transmission. In the upper extremities, the tremor is a postural, distal tremor most often with flexion and extension movement of the hands with a frequency that varies between 4 and 12 Hz. With increasing age, the frequency tends to decrease. A kinetic component when present is generally at the same frequency. Although it may be unilateral at the onset, tremor becomes eventually bilateral in all. About one third of the patients with essential tremor will have a predominant head tremor (110). Head tremor usually begins with a particular directionality and develops mixed directionality over time (194). Horizontal “no-no” head tremor appears to be the most common type of head tremor in early essential tremor (194). The classification of essential tremor has been published (47). Excellent summaries of essential tremor can be found (109; 82; 56; 61).
Functional disabilities include problems with handwriting, drinking, eating, dressing, and speaking. Autonomic function is reported to be normal in essential tremor (39). Gait dysfunction, including lower tandem gait velocity, more missteps, and increased postural sway may be present in essential tremor (92; 55). Hearing loss and mild cognitive impairment have been reported in essential tremor (55). An examination finding called the “head snap” was observed by Sternberg and colleagues during finger-to-nose maneuver in patients with essential tremor and awaits independent confirmation by other groups (210). Intention tremor of the lower extremities was reported bilaterally in 14 and unilaterally in 21 out of a sample of 93 patients with essential tremor. Bilateral intention tremor of the lower extremities was associated with higher upper extremity intention tremor amplitude and longer disease duration (105).
A small group of patients otherwise have the findings of essential tremor but are distinguished by the appearance of certain signs and or symptoms that ordinarily would be excluded from the essential tremor category (149). These include findings of parkinsonism or dystonic tremor (180; 172). Head tremor in the complete absence of arm tremor is not thought to be a part of the clinical spectrum of essential tremor, but head tremor with mild hand tremor has been reported in a minority of cases (145). Uncertainty regarding the classification of parkinsonian features in essential tremor is still present. For example, decreased arm and leg swing frequencies have been found in a sample of patients with essential tremor (16). The nomenclature “ET plus” has been proposed for essential tremor with additional clinical features such as dystonia (124), but there is controversy regarding this term (138).
Although generally not appreciated, cognitive dysfunction has been documented in essential tremor (132). Lower neurocognitive test scores are being recognized as a source of functional disability in patients with essential tremor (134). Cognitive changes in elderly with essential tremor appear to worsen at a faster rate than in controls (134). It is not known whether particular clinical or pathologic features are predisposed to faster rates of cognitive decline (220), but one study suggested that greater cognitive dysfunction is associated with higher tremor scores (156).
Orthostatic tremor. Interest in the phenomena of orthostatic tremor (OT) exceeds its frequency. One paper investigated the association of parkinsonism and orthostatic tremor utilizing SPECT imaging (103). These studies were then compared with 12 age-matched normal controls and 12 patients with Parkinson disease. The outcome indicated a significant defect in presynaptic striatal dopamine function but with significant differences when compared with Parkinson disease. In Parkinson disease, the decrease in activity is seen especially the posterior putamen, whereas in orthostatic tremor, it is more evenly distributed in the striatum. A division of high frequency orthostatic tremor into categories based on degree of dopaminergic loss has been proposed: A) without dopaminergic loss, B) mild dopaminergic loss, and C) dopaminergic loss with clinical Parkinson disease) (235).
Orthostatic tremor can be palpated as well as auscultated. Littmann reported on the diagnosis of orthostatic tremor via electrocardiogram artifact at 13 to 18 Hz (129). Low frequency subtype of orthostatic tremor with EMG burst at less than 12 Hertz was also identified. A review of 45 patients with orthostatic tremor found that mild postural hand tremor was frequently associated with the disorder, as was family history of hand tremor (235).
Another study, based on a single case report, found an elevation in the CSF monoclonal IgG band and suggested that it may be an inflammatory disorder (221); this has not been confirmed by others. There is a dearth of studies of the CSF in primary orthostatic tremor.
Task- and position-specific tremors. This group of tremors is considered to contain variations of essential tremor and to include primary writing tremor and isolated voice tremor.
Primary writing tremor. This type of tremor (11) is a type of task specific tremor first described by Rothwell and Colleagues (198). There are two subtypes of this tremor including a type in which the tremor occurs during the act of writing and the second by adopting a writing position. The clinical features include absence of tremor under other conditions and lack of other neurologic signs. Its frequency is 5 to 7 Hz and may respond in some patients to drug therapy, although not to the same extent as essential tremor. In resistant and disabling cases, botulinum toxin or surgery may be helpful (168).
Vocal tremor. Isolated voice tremor occurs with tremulous vocalization in which other body parts are not affected (07; 158). It is an involuntary oscillation in pitch and loudness of vocal sounds producing a quivering of the speech at a frequency of approximately 3 to 8 Hz. Voice tremor occurs in about 15% to 25% of patients with essential tremor. It appears to affect more women than men (211). Isolated and essential voice tremor are differentiated from spasmodic dysphonia, a dysphonia of the laryngeal musculature. With dysphonia, the speech is effortful, strained, and breathy and the exact nature depends on whether the abductor or adductors are implicated. In some patients there is a combination of voice tremor as well as spasmodic dysphonia. Medical management has generally not been helpful in laryngeal tremor and dysphonia, but some patients do respond to propranolol, primidone and benzodiazepine. The majority failing to show improvement may benefit significantly from botulinum toxin injections that will be helpful in approximately half of the patients with essential or isolated voice tremor and a higher percentage of those with spasmodic dysphonia (231). Anecdotal reports support the use of deep brain stimulation in resistant cases (237).
Dystonic tremors. Dystonia is a sustained muscular contraction resulting in twisting movements or abnormal postures, whereas dystonic tremor refers to dystonia and superimposed tremor (97; 54; 110). It is often worsened when the patient voluntarily moves in the direction away from the force of the contraction. Dystonic tremor may occur in the body part affected by the dystonia, especially dystonic tremors with cervical dystonia. The tremors have a frequency of approximately 4 to 7 Hz and are mainly postural and kinetic without a rest component. The second type of dystonia and tremor is seen when the tremor involves a body part not associated with the dystonic segment; an example would be cervical dystonia in a patient with upper limb postural tremor. These tremors are generally resistant to pharmacotherapy, and they are best managed with local injections of botulinum toxin. Although head tremor occurs in essential tremor, Quinn and colleagues consider head tremor in the absence of hand tremor to be more suggestive of dystonic as opposed to essential tremor (188). Cervical dystonia with associated head tremor (which may have been position dependent) as opposed to cervical dystonia without head tremor was found to be more likely to have associated arm tremor and positive family history of tremor or dystonia (199). Twenty-two-month follow-up of patients with scan without evidence of dopaminergic deficit (SWEDD) in the PRECEPT study (163) and 4-year follow-up of SWEDD patients with dystonic rest tremor by Batla and colleagues show minimal to no clinical or dopaminergic imaging disease progression (15).
Parkinsonian tremor syndromes. There continues to be interest in the association of essential tremor and Parkinson disease (205).
Dirkx and colleagues found that a majority of postural tremor in Parkinson disease is predominantly re-emergent tremor (81% in their series) with tremor frequency correlating with rest tremor and 19% with postural tremor that demonstrated a different frequency from rest tremor and did not have a latency period (51).
A complex network analysis model, as opposed to analysis of single brain regions, may be needed to understand Parkinson disease tremor (83).
Research by Pasquini and colleagues demonstrates serotonin transporter deficiency in raphe nuclei is more correlated with severity of rest tremor in Parkinson disease than dopaminergic terminal dysfunction (96; 184). On the other hand, Loane and colleagues found serotonergic dysfunction in postural tremor (131; 96). These findings have to be reconciled in larger studies. Treatment of serotonergic dysfunction would provide a new avenue of treatment in Parkinson disease tremor.
Yahr and colleagues presented data on a multigenerational study spanning five generations of a family with well-documented essential tremor that followed an autosomal dominant pattern (234). Three brothers in their third generation, two being monozygotic twins, developed the characteristic findings of Parkinson disease occurring years after the onset of essential tremor in their teens. One of the twins’ autopsy documented Parkinson disease. Possible genetic relationships between essential tremor and Parkinson disease are discussed in the Pathogenesis and pathophysiology section.
Rajput and associates reviewed their experiences with essential tremor and parkinsonism, including 20 autopsy cases of essential tremor (191). They concluded that essential tremor and Parkinson disease are clinically, pathologically, and chemically distinct, and any co-occurrence can be attributed to chance given that they are both common. However, patients who initially had essential tremor and later developed parkinsonism were excluded from the study (94). Some patients with essential tremor will develop a rest tremor as part of the disease process. Louis and Hernandez listed rest tremor prevalence from 1.9% to 46.4% in essential tremor (Louis and Hernandez 2015).
Another review, at a referral center, examined 64 patients with essential tremor and found 12 with the rest tremor (37; 103). Those 12 patients had a longer duration of essential tremor, greater severity, and a more widely disseminated tremor, including head and voice tremor as well as limb tremor. None fit the accepted criteria for Parkinson disease.
Coexistent essential tremor and Parkinson disease (ET-PD) appears to have more significant symptomatology than just a mix of essential tremor and Parkinson disease. Louis and colleagues report an increase in cognitive sleep balance and gait dysfunction in ET-PD compared to Parkinson disease alone (157).
Lip and jaw tremor may be present in essential tremor or Parkinson disease. A study of 28 patients with facial tremor (lip and jaw) showed levodopa sensitivity in 46%. Successful treatment with levodopa was consistent with final Parkinson diagnosis with 92% sensitivity and 93% specificity (200).
Benign tremulous parkinsonism (BTP). Benign tremulous parkinsonism is defined as asymmetric rest and action tremor, which is not alcohol responsive and remains the main clinical finding for 8 years. There is minimal progression of other parkinsonian symptoms, such as bradykinesia and rigidity, during this time. This disorder responds poorly to levodopa. In small case series, there was improvement with deep brain surgical surgery to ventral intermediate thalamus or subthalamic nucleus. The pathological studies show Lewy bodies but at a lower burden than in matched controls with idiopathic Parkinson disease. There is controversy regarding whether benign tremulous parkinsonism is a separate entity or form of Parkinson disease (40).
Cerebellar tremor syndromes. In a small, randomized, crossover trial of onabotulinumtoxinA in 23 patients with disabling tremor in 33 upper limbs related to multiple sclerosis, there was a significant improvement after active treatment compared with that after placebo at 6 and 12 weeks post-injection in the Bain score for tremor, writing, Archimedes spiral drawing, and drinking from a cup and in the 9-hole peg test (226).
There was, however, no improvement in the quality of life as measured by the Quality of Life in Essential Tremor Questionnaire (QUEST). Treatment was complicated by transient weakness, noted in 42.2% of patients treated with botulinum toxin, compared to 6.1% of patients treated with placebo (p= 0.0005). The cerebellar outflow tremor may be also helped by deep brain stimulation. Cerebellar tremors are featured by intention tremor that may be unilateral or bilateral depending on the cause. The intention tremor is recognized by a tremor that often affects proximal muscles and increases as the target is approached. The frequency and amplitude are highly variable and irregular. A form of cerebellar tremor involves stance and postural systems causing a gait and truncal tremor referred to as titubation. The common causes of cerebellar tremors include multiple sclerosis, brainstem stroke, neoplasms, and degenerative disease such as parenchymatous cerebellar degenerations, multisystem atrophy (previously referred to as olivopontocerebellar atrophy), and paraneoplastic syndromes (162).
Holmes tremor. Holmes tremor is featured by a low frequency tremor of 3 to 6 Hz and is a rest, postural, and intention tremor. In the past this tremor has been referred to under a number of different names, including rubral tremor, midbrain tremor, thalamic tremor, and myorhythmia (88; 121; 12). The Holmes tremor is caused by lesions that interrupt the pathways of the midbrain, and there is often a delay between the occurrence of the underlying lesion and the onset of the tremor. As with cerebellar tremors, the Holmes tremor responds poorly to therapy in general, including pharmacotherapy. Individual cases with response to levodopa, dopamine agonists, and levetiracetam have been documented (05). Retrospective review of 29 patients by Raina and colleagues found levodopa responsiveness in 13 out of 24 treated patients and excellent results with unilateral thalamotomy in three patients (190). Overall, limited information exists on the usefulness of thalamotomy and deep brain stimulation in the treatment of this tremor (06). Vim stimulation has been reported to be successful (01).
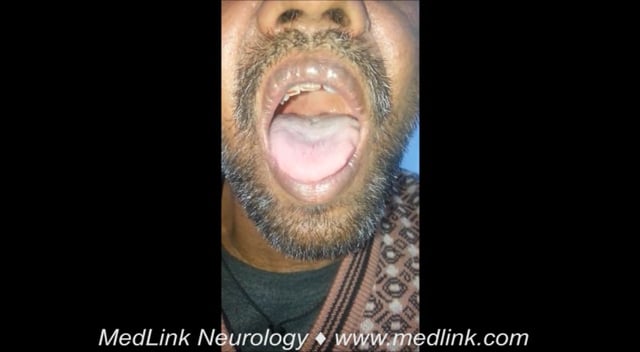
Palatal tremor. Palatal tremor, also referred to as palatal myoclonus because it consists of rhythmical contractions of agonists only, rather than alternating contractions of antagonist muscles, has lower frequency, 1 to 3 Hz, than other tremor (46; 48). It is comprised of rhythmic, involuntary movements of the soft palate and is subdivided into two types: (1) essential palatal tremor and (2) symptomatic palatal tremor. Essential palatal tremor is characterized by an absence of antecedent lesions and olivary pseudohypertrophy. In addition, the patient experiences an audible ear click due to movements of the soft palate from contraction of the tensor veli palatini. Extremity and eye muscles are not involved.
Symptomatic palatal tremor involves the brainstem and cerebellar pathways with olivary hypertrophy associated with rhythmic movements of the levator veli palatini muscle. The pathology involves the so-called Guillain-Mollaret triangle that extends from the cerebellar dentate nucleus to the contralateral red nucleus to the inferior olive via the central tegmental tract and then back to the cerebellum. Pathologies include multiple sclerosis, stroke, and degenerative diseases. Another distinguishing feature of the symptomatic tremor is its persistence through coma and sleep and once established is permanent. Both the secondary as well as the essential tremor likely arise from dysfunction of the central oscillators. There is no effective medical treatment, though there have been some reports of benefit from injection of botulinum toxin into the soft palate (32).
Palatal tremors are among those that may result from strokes. Tremor with delayed onset sometimes occurs with thalamic lesions as well as lesions that involve the subthalamic nucleus.
Myorhythmia. This repetitive, rhythmic, slow (1-4 Hz) movement affecting chiefly cranial and limb muscles overlaps phenomenologically with tremor and segmental myoclonus, including palatal myoclonus (12). It is important to recognize because it is usually associated with lesions involving the brainstem, thalamus, or other diencephalic structures with potentially treatable etiologies. One example is oculo-masticatory myorhythmia associated with Whipple disease, which is described as a slow repetitive asymmetric movement (12). Myorhythmia has been described in patients with cerebrovascular disease, encephalitis, multiple sclerosis, and autoimmune encephalopathies including anti-N-methyl-d-aspartate receptor encephalitis (14).
Neuropathic tremors. These tremors are tremulous movements that occur in the context of an established peripheral neuropathy. By and large, they are relatively uncommon and generally consist of irregular postural or kinetic tremors of variable frequency from 4 to 11 Hz. Not all peripheral neuropathies have been identified with tremor, and most of them have been demyelinating and specifically dysgammaglobulinemic neuropathies (especially IgM disorders). Tremors have also been reported in type 1 hereditary motor and sensory neuropathies (Roussy-Levy syndrome). Tremors have also been reported with chronic inflammatory demyelinating polyneuropathies in the recovering phase of Guillain-Barré syndrome (201; 58; 209; 208).
Drug-induced and toxic tremors. The list of agents that can produce a variety of tremors is long and involved. The tremor frequency also has a wide range from 3 to 12 Hz. The classes that have been implicated in tremor include neuroleptics, lithium, corticosteroids, calcium channel blockers, ethanol, beta adrenergic agonists, valproic acid, theophylline, thyroid hormones, cardiac antiarrhythmics, nicotine, and tricyclic antidepressants. If one encounters a patient with an unusual or inexplicable tremor on one of these agents, it is worthwhile withdrawing them from the agent if this is possible. The most common clinical features of these tremors are enhanced physiologic tremor in patients exposed to sympathomimetics and antidepressants. Parkinsonian tremors are well known to occur with neuroleptic and dopamine receptor blocking agents and the cerebellar syndromes occur with lithium. A variant of drug-induced tremors is the tardive tremor after long-term use of neuroleptic agents. The frequency is generally slow and predominantly postural but also can occur at rest and with intention. The association of the so-called “rabbit syndrome” is quite distinctive with this type of tremor.
Psychogenic tremor. Psychogenic tremor is not rare or uncommon. Formerly a diagnosis of exclusion, well-established criteria exist for diagnosis (111; 45). The incidence of psychogenic tremor is higher in women than men and can occur at any age, but it is unusual in children. Its onset is often abrupt but nonprogressive and fluctuates in severity. The frequencies and amplitudes vary. The tremor may be kinetic, postural, or resting; it may also lack the general physiologic pattern, in that the postural tremor may be of higher amplitude than the kinetic tremor or it may change from supination and pronation to flexion and extension. Tremor frequency is variable, synchronous in both arms, and may be entrained to the frequency of repetitive movements the patient is asked to perform (78). It is often accompanied by other findings of the somatoform disorder including multiple undiagnosed conditions and somatizations as well as an absence of objective clinical, laboratory, or radiographic findings. The treatment begins with a thorough evaluation followed by a frank discussion with the patient and, finally, psychotherapy. Pharmacotherapy is not typically helpful. In order to determine clinical features that reliably distinguish psychogenic and essential tremor, Kenney and colleagues used clinical data and “blinded” rating of videos of 45 patients with these two tremor types (104). Patients with psychogenic tremor were significantly more likely to relay a history of sudden onset, spontaneous remissions, and shorter duration of tremor. Family history of tremor was significantly more common in the essential tremor group. A moderate to marked degree of distraction with alternate finger tapping and mental concentration on serial 7s, suggestibility with a tuning fork, and exacerbation with hyperventilation were predictive of psychogenic tremor. Schwingenschuh and Deuschl propose the following as signs of psychogenic or functional tremor: "sudden tremor onset, unusual disease course, distractibility, tremor entrainment, tremor variability, and coactivation sign," in addition to appearance of exhaustion during the examination (203).
Unusual tremors. There are some interesting articles on unusual and rare tremors, including a single case report and review of the treatment of tremor in complex regional pain syndrome (174). The range of movement disorders associated with complex regional pain syndrome includes dystonia as well as tremor. Tremor is described as an enhanced physiologic tremor that may spread beyond the limb or involvement, suggesting that thalamic inputs may participate in the evolution of the tremor. Additionally, enhanced proprioceptive reflexes, which are increased by sympathetic sensitization of the muscle spindles, may play some role, particularly on peripheral mechanisms. Additionally, there simply may be a subclinical movement disorder that is uncovered by the pain syndrome. Treatments have found levodopa, as well as botulinum toxin type A, to be helpful in some instances. Other pharmacologic treatments of tremor have shown variable success.
An article by Kim and colleagues describes a “limb shaking” transient ischemic attack associated with hyperventilation in Moyamoya disease (107). The case report is that of an individual in whom these tremors can be induced either by the consumption of very spicy food or hyperventilation. The MRI showed Moyamoya disease, and the EEG was normal. Hyperventilation could result in shaking of the limb on the contralateral side after about 30 seconds. SPECT scan showed decreased perfusion on the right with hyperventilation. Limb shaking has been seen in severe stenosis and occlusion of the contralateral carotid. It is suspected to arise from the dorsal lateral frontal cortex as an ischemic phenomenon.
A novel tremor has been described in humans, referred to as bilateral high-frequency synchronous discharges (161). The frequency of this tremor is similar to that seen in orthostatic tremor. It is featured by a clinical picture of posterior fossa dysfunction with cerebellar and brainstem disorders. It is a high-frequency tremor of the outstretched limbs that is ended by forceful contracture at the wrist. Electrophysiologically, there is a high-frequency discharge in forearm muscles at 14 to 16 Hz. Stimulation of the motor cortex does not reset the tremor. Stimulation over the posterior fossa resets the high-frequency bursts. Coherence and cospectral change were seen between the agonist and the antagonist muscles in left and right upper limbs. Radiographic studies showed atrophy of the brainstem suggestive of disorders such as olivo-frontal cerebellar degeneration. It was suggested that the high-frequency discharge found in these patients was due to repetitive discharges in the cerebellar and precerebellar circuits.
Busby and colleagues report a case of severe kinetic and postural tremor that gradually developed in a patient with a nonparaproteinemic-acquired demyelinating neuropathy; both the severe and the postural tremor responded to IVIG, with marked improvement in the tremor as well as the neuropathy (27). Tremors have been well described in cases of hereditary sensory motor neuropathies and paraproteinemic neuropathies associated with IgM paraproteinemias. These also have been associated with antimyelin-associated glycoproteins (MAG). Debate in these neuropathies is centered on whether the mechanism is a central or peripheral one. Busby and colleagues’ observations with clinical and electrophysiologic data suggest a peripheral mechanism due to abnormal muscle spindle input secondary to the slow conduction velocity (27), but the precise mechanism is unknown.
Perinasal region and forehead tremor was identified in eight patients with focal or segmental dystonia and was described as irregular, with a frequency of 3 to 5 Hertz (64).
Unusual pediatric movement disorders. Spasmus nutans is a triad of head titubation, nystagmus, and torticollis, which presents during early childhood and has a good long-term prognosis (224). Bobble-head doll syndrome consists of head bobbing with imaging findings showing third ventricular obstruction usually via cystic structures. Ventriculoperitoneal shunt placement is a typical treatment for this disorder (224). Shuddering attacks consist of shivering movements that occur without impairment of consciousness and improve over time (102).
Prognosis for these disorders is highly variable and can be found in the clinical manifestations discussions.
A 62-year-old female presented for evaluation of tremor. She reported a 3-year history of action tremor in both hands. The tremor interfered with activities, for example, causing her to spill coffee and to have food fall off her fork when eating. Her handwriting became tremulous. The tremor seemed worse for a half hour after performing yard work or other physical exertion.
Her mother had a similar tremor that developed at 70 years of age, and her grandmother had a no-no type of head tremor.
The patient initially denied having tremor at a younger age, but on repeated questioning she volunteered that she felt an “internal tremor” during presentations in her college classes as well as at her workplace (36). She thought that this tremor was a natural reaction to stress.
Drinking a glass of wine profoundly diminished the tremor for a few hours, but her tremor was worse the day after heavier alcohol ingestion. She asked about potential pharmacotherapies, as her tremor was interfering with her daily activities.
Most tremors are either idiopathic, degenerative (Parkinson disease), genetic (essential tremor), toxic and metabolic, or secondary to some systemic or structural disorder. Many of the most obvious causes are due to medications or toxins. Medications most commonly implicated in tremor include neuroleptics, valproic acid, lithium, calcium channel blockers, amiodarone, tricyclic antidepressants, asthmatic medications, and antiepileptics, including phenytoin. Gastrointestinal medications such as metoclopramide have also been implicated (214). Some of the medications produce the tremor due to an idiosyncratic reaction, but others act by way of the sympathetic nervous system causing enhanced physiologic tremor.
Examples of reported causes include heavy metals (166), opioids (34; 197), copper, gamma-hydroxybutyrate (38), and solvents (49).
Increasingly, the late effects of stroke are related to some tremors, particularly those that involve the thalamus (31; 112).
Some unusual systemic causes include Whipple disease (187), B12 deficiency with orthostatic tremor (18), celiac disease (71), and thyrotoxicosis (167).
Essential tremor. The underlying source of essential tremor has been debated as being peripheral or central. The current wisdom suggests that the cause is central and the suggested oscillator involves the cerebellum and its pathways, especially the inferior olive and cerebellar outflow tracts. Diffusion tensor imaging has confirmed the involvement of the inferior cerebellar peduncles (108). Another diffusion tensor imaging study has found changes in the dentate nucleus (176). The effectiveness of deep brain stimulation and thalamotomy points to the involvement of ventral intermediate thalamus. Of interest, coherence between electromyography and electroencephalography has been found in tremor bursts of symptomatic essential tremor and in voluntary muscle contraction of first-degree relatives of patients with essential tremor (189). Increased coherence of subthalamic nucleus and contralateral cortical structures correlated with rest tremor amplitude in patients with Parkinson disease (87). In orthostatic tremor, a widespread thalamocortical and cerebellar oscillating network was coupled to tremor oscillations (173). Research on therapies such as closed-loop deep brain stimulation focuses on interregional coupling (85). Different clinical subtypes of essential tremor could be due to pathology in distinct cerebellar circuits: vermis and fastigial nuclei for head and proximal upper extremity tremor; lateral hemispheres and dentate nuclei for intention, postural, and isometric tremor; and interposed nuclei for intention tremor (66).
Other structures have been implicated as well. For example, reduction in tremor after putaminal infarct was reported (126). Mild impairment of the dopamine transporter in putamen was reported on a striatal dopamine transporter single photon emission computed tomography (SPECT) study (93). In patients with tremor-dominant Parkinson disease, pallidal and not striatal dopamine loss was correlated with rest tremor severity. Helmich and colleagues conclude that rest tremor in these patients results from abnormal signals from the basal ganglia affecting the cerebellothalamic circuit (84). Increased iron deposition in the bilateral globus pallidus in patients with essential tremor versus age-matched controls was found on review of T2* MRI sequences (178). Serotonergic loss in caudate, putamen, and raphe nuclei measured via PET using a serotonin transporter binding marker was shown to correlate with action but not rest tremor in Parkinson disease (131).
The “GABA hypothesis” in essential tremor implies that tremor is due to hyperactivity of cerebellothalamic circuits due to reduced GABAergic function (24; 85). Rhythmicity of the olivocerebellar system is also thought to be affected by the action of T-type calcium channels. Ca(V)3.1 is the dominant subtype expressed in the inferior olive and is a potential therapeutic target (79). Unlike wild-type mice, transgenic mice lacking Ca(V)3.1 channels did not produce 4 to 10 Hz synchronous discharges from the inferior olive after administration of harmaline (182). Although the inferior olive has been thought to be involved in essential tremor pathology, a review of 14 essential tremor cases and 15 controls by Louis and colleagues found no structural or metabolic abnormality in the inferior olive of patients with essential tremor (140).
The rs9652490 variant of the LINGO1 gene has been associated with both essential tremor and Parkinson disease (42; 41; 227). Its paralog, LINGO2, has been found to influence both risk and age of onset of essential tremor (229). A meta-analysis supports the association between LINGO1 rs11856808 polymorphism and the risk for essential tremor and familial essential tremor as well as an association between rs9652490 polymorphism and the risk for familial essential tremor (101). MAPT H1 haplotype has been identified as a risk factor for development of essential tremor in a study of 356 subjects with familial and sporadic essential tremor, 61 with multiple system atrophy, and 409 controls (228), but a study of 200 subjects with familial essential tremor and 291 healthy controls in Spain did not find increased risk for essential tremor from MAPT H1 rs1052553 single nucleotide polymorphism (73). LINGO1 is expressed in cerebellar basket cell distal axonal processes and apparently forms a “pinceau” or brush structure enveloping the Purkinje cell axon initial segment (114).
Mutation in the RNA binding protein FUS (FUsed in Sarcoma), different from the FUS mutation reported in amyotrophic lateral sclerosis, was found in a large family of patients with essential tremor (165). A separate FUS mutation was reported to cause essential tremor in Chinese patients (233). Glial glutamate transporter SLC1A2 polymorphisms were also found to be associated with essential tremor (218). SLC1A2 involvement in essential tremor was confirmed in a Chinese cohort, but a meta-analysis by Jimenez-Jimenez and colleagues found that SLC1A2 rs3794087 is not associated with essential tremor (99; 213). Whole genome sequencing of three families with essential tremor identified missense mutations in TENM, a regulator of CNS myelination and axonal guidance (91).
The ANO3 gene, suspected in torsion dystonia, is not involved in essential tremor pathology (90). The ETM1 gene on chromosome 3q13 was confirmed as a possible genetic cause of essential tremor (215). A locus on chromosome 5 was confirmed to be linked to essential tremor in a study of 48 patients (86).
Kuhlenbaumer and colleagues’ meta-analysis of essential tremor genetics studies concludes that ETM2 is the most promising candidate gene for monogenic essential tremor, whereas FUS is a rare cause of monogenic essential tremor (113). Further research on LINGO1 and SLC1A2 is needed to fully assess their roles as risk genes (100; 113). Further meta-analysis shows LINGO1 rs9652490 and STK32B rs10937625 to be most likely to be associated with essential tremor but there continues to be conflicting data (207).
Increase in Purkinje cell loss with axonal torpedo pathology as well as Bergmann gliosis have been reported in essential tremor (44). The dense and tangled, “hairy” appearance of basket cells has been seen in the cerebellar cortex of essential tremor brains (63). A subset of patients with essential tremor has Lewy body pathology in the locus ceruleus (134). A postmortem study of nine patients with essential tremor who had rest tremor confirmed Purkinje torpedo pathology did not reveal any Lewy body pathology (139). Torpedoes as an indicator of Purkinje cell remodeling were associated with Purkinje cell loss (141). Interestingly, Rajput and colleagues reported no significant difference in Purkinje cell counts in pathological evaluation of 12 essential tremor cases as compared to six normal controls and 41 Parkinson disease cases (192). Increased climbing fiber to Purkinje cell spiny branch synaptic density was observed in essential tremor. This finding inversely correlated with clinical tremor severity (127). Ubiquitin-positive Purkinje cell inclusions demonstrate pathological heterogeneity in essential tremor (136). Babij and colleagues observed changes in Purkinje cell axonal connectivity and shape including torpedo pathology, and in essential tremor brains as opposed to controls, and postulated that these are responses to Purkinje cell injury (10). Inconsistencies among studies regarding the degree of Purkinje cell loss and dentate nucleus neuronal loss among multiple studies may be due to methodological differences in pathological specimen preparation as well as reliance solely on clinical phenotype without the benefit of genotyping (98). KCNS2 (KV9.2), HAPLN4 (BRAL2), and USP46 were identified as candidate cerebellum-expressed genes in autosomal dominant early-onset essential tremor via whole genome sequencing (130). Louis and Faust propose that most cases of essential tremor can be thought of as a cerebellar neurodegenerative disorder with support from volumetric studies of the cerebellum and functional magnetic resonance imaging (138).
The possibility of a relationship between essential tremor and Parkinson disease continues to be examined (67; 188; 217; 144; 95). Although there is clinical, imaging, and other evidence suggesting that a subset of patients with essential tremor later develops parkinsonism, the pathological substrate for this type of parkinsonism may be different from that of idiopathic Parkinson disease (03). Frequency of probable REM behavior disorder, a synucleinopathy, has been found to be increased in patients with Parkinson disease but not in patients with essential tremor (02), but Lacerte and colleagues found increased REM behavior disorder prevalence in patients with essential tremor as compared to the general population (115). Electromyographic differences between essential tremor and Parkinson disease in synchronicity of rest tremor have been found (177). A report of a large family with restless legs syndrome, essential tremor, and Parkinson disease provides additional support for the essential tremor and Parkinson disease link (186). Laroia and Louis conclude there is reasonable epidemiological evidence for a link between essential tremor and Parkinson disease (118). One study utilizing dopamine transporter (DAT) imaging found “a significant presynaptic dopaminergic deficit” in patients with essential tremor compared with normal volunteers (74), but this has not been a consistent finding (67). Waln and colleagues found minimal dopaminergic deficit in some patients with essential tremor on DAT imaging (230). An 18F FP-CIT study of patients with bilateral postural tremor and unilateral or bilateral rest tremor found reduced nigrostriatal activity in 22% of subjects (238). If a link between essential tremor and Parkinson disease exists, the relationship is from essential tremor to Parkinson disease and not vice versa (154). Espay and colleagues propose reclassifying essential tremor as isolated (monosymptomatic) tremor as opposed to a “combined tremor” with features such as dystonia, bradykinesia, and cerebellar features, which would be classified as having distinct etiologies (65). Ou and colleagues found slower motor and nonmotor progression in a cohort of 785 patients with Parkinson disease preceded by essential tremor as opposed to without essential tremor (179).
Various imaging modalities are supportive of a neurodegenerative model for essential tremor. Magnetic resonance volumetry studies reviewed by Louis and colleagues show cerebellar volume loss in essential tremor (136). Magnetic resonance spectroscopy as well as diffusion tensor imaging also demonstrate changes in essential tremor (136). Functional MRI studies implicate multiple cortical areas as well as posterior lobules of cerebellum in cognitive dysfunction (21).
GABAergic dysfunction has been demonstrated in essential tremor cases (21). A pathological study found decreases in dentate nucleus GABAA and GABAB receptors in essential tremor cases whereas molecular and granular layer GABA receptors are preserved (181). The authors conclude that this results in disinhibition of cerebellar output via the dentato-thalamic pathway. Severity of tremor as measured by clinical rating scales correlates with cerebellar GABA receptor binding quantified by cerebellar flumazenil uptake (75).
Research groups continue to utilize next-generation sequencing techniques for genetics discovery experiments in essential tremor, with a flurry of new mutation reports. A rare variant of HTRA2 was identified via whole exome sequencing as causing essential tremor in a single large Turkish family (223). Heterozygotes and homozygotes in this consanguineous family were reported to have essential tremor versus essential tremor plus a Parkinson disease phenotype, respectively. An association study of over 1700 Asian subjects found one control heterozygous carrier of the same HTRA2 variant and no other instances of this variant in controls, essential tremor, or Parkinson disease (29); an earlier study of four Han Chinese essential tremor families did not observe any HTRA2 mutations (219). Whole exome sequencing identified a novel genetic variant of SORT1 segregating with essential tremor in a Spanish kindred (202). A collaborative effort between Swiss and Spanish research teams identified novel mutations in TENM4 using a combination of whole exome sequencing, targeted resequencing, and follow-up studies in model organisms (91). Putative causal mutations were identified in three families. In the latest whole exome sequencing study, missense variants of highly conserved sequences in the gene coding for nitric oxide synthase 3 (NOS3) were identified in two independent families (130). Interesting single-family results were also reported for the KCNS2, HAPLN4, and USP46 genes, all highly expressed in Purkinje cells (130). The next few years will be an exciting time as replication studies reinforce and modify the latest round of whole exome sequencing driven results and research pushes into whole genome sequencing, all providing new clues on essential tremor pathogenesis. For example, the TENM4 protein regulates oligodendrocyte maturation, and in mice is expressed in adult cerebellar white matter. This very interesting result builds on LINGO1 data, reinforcing the possible role of oligodendrocytes and myelination in essential tremor pathophysiology. Caution is still required in generalizing any of these results, as little is yet known about the prevalence and significance of any of these variants: the TENM4 result was not replicated in a Chinese cohort (30) and the HTRA2 variant was found in four of 1024 Norwegian controls but was not observed in 103 essential tremor patient samples (222). The updated tremor classification system defines this clinical entity as Parkinson disease and not essential tremor syndrome plus Parkinson disease (22).
Fragile X premutation. Each year there are an increasing number of articles dealing with the neurologic syndrome associated with the Fragile X premutation. Two excellent articles and a short review have focused on this disorder, the recognition of the phenotype, and its frequency in the field of movement disorders (19; 122; 195).
The Fragile X syndrome and its carrier status is best defined genetically as an expansion of the CGG Trinucleotide repeat in the 5’ untranslated premotor region of the FMR1 gene on the X-chromosome. Normal individuals have six to 40 repeats; in the full mutation, repeats are greater than 200, producing a phenotype including mental retardation, autism, learning disorders, ADD, a long face, large ears, and microorchidism seen in young boys. The full mutation is associated with methylation and transcriptional silencing of the FMR1 gene and absence of FMRP.
The premutation occurs when there are between 55 and 200 repeats, which predisposes a person to have children and grandchildren with Fragile X syndrome but lack the hypermethylation of the FMR1 gene or the absence of FMRP. There is an elevation of FMR1 mRNA, which roughly correlates with the CGG repeat length (19). A gray area of between 40 and 55 repeats is not clearly associated with a physical disorder.
Fragile X syndrome is the most common inherited form of mental retardation. The FMR1 premutation has a frequency of about 1/250 in females and about 1/813 in males. In female carriers, about 20% will have a premature menopause. Males are more affected than females because females have a second X-chromosome that produces FMRP.
Male carriers with low premutation frequencies of 55 to 100 repeats have FMR1 mRNA increase of two to four times normal and normal FMRP. Those with 100 to 200 repeats have FMR1 mRNA four to 10 times normal and a mild decrease in FMRP. In a mouse model, loss of FMRP has been associated with decoupling of metabotropic glutamate receptor-dependent priming of long-term potentiation from protein synthesis (08).
In 2001, Hagerman and colleagues at the University of California, Davis, identified a group of older men with the Fragile X premutation who had intention tremor, ataxia, and some dementia (77). Each man was the grandfather of one or more boys with Fragile X syndrome. They found these men to have the FMR1 premutation with a range of between 50 and 200 repeats.
Although there is overlap in clinical features between essential tremor and FMR1 premutation phenotype, analysis of 321 essential tremor cases and 296 controls by Clark and colleagues found no association between FMR1 and essential tremor (35).
In 2003, Hagerman and colleagues published a blinded videotape study using standard scales for tremor, ataxia, and parkinsonism (19). They compared this to other groups including controls, male non-carriers, female carriers, and female non-carriers. The male premutation carriers, which numbered seven, had significantly higher scores on all of the UPDRS III scales and subscales. The typical subject was 67 years of age plus or minus 8 years and had a rest tremor, postural tremor, action tremor, and ataxia as well as parkinsonian rigidity. The ataxia was not only of stance and gait but also of the limbs. Other symptoms occurred variably, such as cognitive impairment and autonomic dysfunction, including impotence and incontinence. The mixture of parkinsonian features, ataxia of gait and limbs, and tremor was not typical of any previously described neurodegenerative disease. Females with the premutations did not show any of these signs and were indistinguishable from controls.
In the field of epidemiology, a study looked at the risk factors associated with head tremor and essential tremor (152). Head tremor was seen in approximately one third of patients with essential tremor. Those with head tremor had both the least and the worst tremor scores for arm tremor. There was no change with age or duration of the tremor. There was an increased incidence for head tremor in those with a positive family history.
A community-based study of northern Manhattan residents (148) examined the association of disease duration and age with tremor severity. Disease duration and age were independently associated with tremor severity in essential tremor, leading to the observation that the increase of tremor severity is related to inherent worsening with disease duration.
In a meta-analysis, prevalence increased with age, especially at or above 65 years of age. More than one third of the included studies referenced a gender difference, with a higher prevalence in men (135).
Prevention largely relates to the avoidance of the known toxic causes of the tremor, which are noted elsewhere. In addition, the effective treatment of risk factors for stroke should help to limit those tremors that occur in the aftermath of stroke and are small in number.
The differential diagnosis for tremors includes (57):
|
• Psychologic tremor | ||
|
- Classical essential tremor | ||
|
• Dystonic tremor | ||
These are discussed further in the “Clinical manifestation section.
The diagnostic workup for most individuals with tremor is limited to the careful clinical observations and categorization. For the most common tremors, no further studies are necessary. In the young individuals who develop a movement disorder, all should have a slit lamp examination as well as an analysis of serum and urine copper and serum ceruloplasmin to exclude Wilson disease. A patient suspected of having tremor secondary to structural disease should have MRI studies looking particularly for alterations in the basal ganglia and posterior fossa contents. Extensive studies with functional MRI, PET scanning, and spectral analysis of the tremor are largely in the realm of research. Alternating, asynchronous tremor is more associated with essential tremor, whereas Parkinson disease has more synchronous pattern on research-based coherence analysis (225). Resting state networks visualized via fMRI are being studied as a potential biomarker for essential tremor (17).
Fragile X premutation. Because the premutation carrier in males is 1/813, this syndrome is likely to be underdiagnosed.
Hagerman and colleagues reported two cases presenting as essential tremor, a 68-year-old who had tremor for 10 years and a 63 year old who had tremor since the age of 49 years (19).
There are significant abnormalities on MRI, including atrophy of the cortex and cerebellum and symmetric nonenhancing hyperintensities of the middle cerebellar peduncle on T2-weighted images.
Pathology includes neuronal and astrocytic intranuclear inclusions in the cerebrum and cerebellum, especially in the hippocampus. There is a loss of cerebellar Purkinje cells and dystrophic cerebellar white matter.
There are several rating scales used to assess tremor. The Tremor Research Group (TRG) Essential Tremor Rating Scale (TETRAS) has been validated and has been found to correlate well with quantitative assessments using the KinesiaTM (CleveMed) system (170; 169). The severity of the tremor should be assessed on a 0 to 4 scale. Zero is equal to none; 1 is equivalent to a minimal; 2 is a moderate tremor that is detectable, but the procedure such as drinking from a cup can be completed; 3 is a severe tremor in which the patient will spill water, for example, pouring one cup to another or bringing the cup to their lips; and 4 is inability to perform the task at all. Whenever possible, videotape these relevant findings. Observations as to the presence or absence of bradykinesia, altered tone, or whether there are elements of Froment sign or co-contraction, when applicable, are recorded. Postural abnormalities should include gait and stance as well as response to the push-pull test. The absence or presence of dystonia is noted, as are cerebellar findings. Finally, neuropathic findings with sensory and reflex loss as well as distal weakness and pyramidal findings associated with spasticity are recorded. Any assessment of tremor must take into account minute-to-minute and hour-to-hour amplitude variability, which can vary up to 23% during a 6-hour period (169).
Additional tremor severity scales validated by the Movement Disorders Society Task Force are: Fahn-Tolosa-Marin Tremor Rating Scale, Bain and Findley Clinical Tremor Rating Scale, Bain and Findley Spirography Scale, as well as Washington Heights-Inwood Genetic Study of Essential Tremor Rating Scale. The MDS Task Force recommends one ADL/disability scale (the Bain and Findley Tremor ADL Scale), one quality-of-life scale (the Quality of Life in Essential Tremor Questionnaire), and one screening instrument (the Washington Heights-Inwood Genetic Study of Essential Tremor Rating Scale, version 1) (55).
Lyons and colleagues provide an excellent overview of therapy (159). They point out that either primidone or propranolol works equally well in the aggregate, with about half of the patients responding with 50% to 60% improvement. A number of second-line agents were examined, including benzodiazepines, topiramate, and gabapentin, and show some promise. Botulinum toxin type A has shown some good results for voice tremor. Botulinum toxin may be offered for upper extremity essential tremor (206). Targeting contracting muscles with more precision using techniques such as EMG guidance, electrical stimulation, and ultrasound along with novel approaches such as kinematics can allow for more successful treatment of tremor with better avoidance of side effects (239). Evidence-based guidelines from the American Academy of Neurology (AAN) support primidone, propranolol, and propranolol LA as Level A recommendations (241). Alprazolam, atenolol, sotalol, gabapentin, and topiramate are AAN Level B recommendations for limb tremor in essential tremor (241). Systematic review by the Italian Movement Disorders Association (DISMOV-SIN) also recommends primidone, propranolol, and propranolol LA in addition to topiramate as first-line agents (240). Metaanalysis by Chang and colleagues supports the efficacy of topiramate, but use of this medication is limited by potential side effects (28). The 2019 Movement Disorders Society evidence-based review found primidone, propranolol, and topiramate to be efficacious and clinically useful (68).
Primidone in low dose, up to 250 mg/day, may be useful in patients unable to tolerate high doses (204). In a study of 528 patients with essential tremor, nearly one third stopped their pharmacotherapy, potentially due to troublesome side effects (134). Intolerability of primidone may be occurring at higher rates in essential tremor compared to epilepsy, based on rates in existing published studies (123).
An open-label study investigated the effects of olanzapine on essential tremor in 37 patients with dose ranges of 5 to 20 mg daily (236). There was a significant decrease in tremor score; however, there were also limiting complications, particularly sedation and weight gain, but the sedation tended to wane in the first week.
Arotinolol, a beta-blocker, was investigated and compared with the standard beta-blocker treatment (120). In a randomized, crossover, multiple-dose comparison study, it was shown to be as effective as propranolol. Arotinolol is a nonselective, hydrophilic beta-blocker that does not cross the blood-brain barrier; hence, the presumed mechanism is peripheral. It was as effective as propranolol and found to be safe but offered no significant advantage over the standard treatment. This medication along with sotalol, zonisamide, gabapentin, alprazolam, clozapine, and olanzapine are recommended as second-line treatment by the DISMOV-SIN; other considerations for second-line treatment are experimental drugs with primarily beta adrenergic blockade effects: ICI 118.551 and LI 32-468 (240).
Octanoic acid at 4 mg/kg was well tolerated but unfortunately did not show a benefit at the primary outcome of 80 minutes in a double-blind, placebo-controlled trial. There was effective tremor control at 180 minutes, which was a secondary measure for the trial (81).
Surgical therapy continues to gain acceptance in patients who have refractory, severe tremor for which medical therapy is ineffective. Increasingly, thalamotomy is being replaced by deep brain stimulation as the modality of choice. One study assesses stability of the procedure in patients with both Parkinson disease and essential tremor for up to 6 to 7 years (193). Twenty-five patients completed the long-term evaluation in a prospective blinded analysis. Thirty-nine patients were enrolled with the UPDRS III and essential tremor rating scales 2 years and 6 to 7 years before surgery, by different evaluators at each segment. In the Parkinson disease group, deep brain stimulation significantly suppressed the tremor by two grades or more at the second half of the seventh year. The total motor score in Parkinson disease remained stable, with continuing decrease in tremor and akinesia despite progression of the disease in general. Similar changes were noted in patients with essential tremor, showing stability at 2 years and 6 to 7 years. In addition, the stimulator parameters also remained stable. Long-term follow-up of a patient with deep brain stimulation for essential tremor showed only minimal foreign body reaction and gliosis around the electrodes 12 years after implantation (50). Systematic evidence review by the Italian Movement Disorders Association recommends thalamic deep brain stimulation and botulinum toxin type A for refractory cases of essential tremor (240). Thirteen patients with deep brain stimulation for essential tremor were shown to have 37.2% improvement in Fahn-Tolosa-Marin motor scores during “on” versus “off” evaluation by a blinded rater at a mean time of 132.5 months after implantation (13). In this group, electrode revision or internal pulse generator change occurred on average every 4 years. There appears to be tolerance to deep brain stimulation therapy that may develop over time requiring increases in voltage, pulse width, and frequency of stimulation (196). Speech disturbance can occur as a side effect of deep brain stimulation for essential tremor (04).
Pilot studies of focused ultrasound thalamotomy have been reported, but larger trials are needed to understand efficacy and safety of this procedure (59; 128). Unlike with deep brain stimulation surgery, there is no ability to adjust the intervention to account for side effects or worsening of tremor amplitude over time. Elias and colleagues reported results of a trial of 76 patients receiving either focused ultrasound thalamotomy or sham procedure at 3:1 ratio (60). Although hand tremor was reduced, there were side effects of gait disturbance and paresthesias or numbness, which persisted in a subset of patients even at 1-year postprocedure. Another 12-month follow-up study of patients with medication refractory tremor-dominant Parkinson disease randomized to unilateral focused ultrasound thalamotomy versus sham in a 3:1 ratio demonstrated improvement in Clinical Rating Scale for Tremor scores and UPDRS motor scores (25). Adverse events included mild hemiparesis, orofacial paresthesia, finger paresthesia, and ataxia. There was no statistically significant difference in Clinical Rating Scale for Tremor scores analyzed 1 year after focused ultrasound thalamotomy in different skull density ratio groups; rates of adverse events were lower for skull density ratio < 0.45 and target temperature was achieved more often in skull density ratio => 0.45 (53). Four-year open-label follow-up of 12 patients after MR-guided focused ultrasound thalamotomy by Park and colleagues showed improvement compared to baseline presurgical tremor scores (183). Potential advantages of MR-guided focused ultrasound compared to deep brain stimulation surgery in essential tremor include not making any skin incisions or skull lesions, thus having no infection risk, but those need to be counterbalanced with inability to adjust for side effects or tremor exacerbation due to disease progression (69).
Vim thalamic stimulation has been reported to be effective in Holmes tremor in addition to its usual role in the treatment of essential tremor (01). Deep brain stimulation of the posterior subthalamic area in essential tremor has also been investigated (23). Only modest overall efficacy was reported in a small series of patients who underwent gamma knife thalamotomy (125).
Another study looked at the neuropsychological and quality-of-life outcomes at 1 year in patients with essential tremor undergoing unilateral thalamic deep brain stimulation (70). Overall, there were improvements in cognitive performance and visuomotor and visuospatial skills as well as verbal memory evident at 3 and 12 months. About 10% showed declines in verbal fluency; this was believed to be due to the stimulation itself. There was improvement in the quality-of-life outcomes, which remain stable over the years.
Noninvasive treatment options may be considered in the future. By their design, they may be neutral to tremor classification (essential tremor syndrome, dystonic tremor, tremor in parkinsonism) or underlying etiology, in contrast to most medication and stereotactic surgical interventions. Forms of noninvasive external tremor control, including self-balancing prosthetics, wearable robotics, and vibration dampening devices are under development (72; 106; 26; 212; 33). Related mildly invasive approaches such as out of phase electrical stimulation of muscles are also in development (52). Assistive devices designed to smooth out or cancel tremor signals rather than impact the limb tremor itself include a handheld spoon (185). As these approaches target tremor at the level of the limb or the adaptive device rather than targeting central pathophysiology, interventions developed for other primary tremor disorders, such as a modified computer mouse for tremor in Parkinson disease (80), may be of use in essential tremor treatment.
Research. A new area of research entails evaluating the effect of hormones on essential tremor. Neurosteroids are hormones that can also act on GABA signaling pathways (116). SAGE-547, an intravenous infusion of allopregnanolone, has been shown to reduce accelerometer-measured kinetic tremor scores and TETRAS ratings in a 25-patient pilot study (62). Further research on delivery systems is needed as an intravenous formulation is clearly not amenable for regular use. Essential tremor pathology includes abnormal burst firing of cerebello-thalamo-cortical neurons, and this function can be regulated by T-type calcium channels (164). These channels are a topic of active clinical research. T-type calcium channel (Cav3) blocker CX-8998 is being studied for essential tremor (20; 175). Results of transcranial magnetic stimulation for essential tremor are inconclusive (119).
Studies implicating serotonergic dysfunction in generation of tremor in Parkinson disease should prompt evaluation of existing serotonin modulators, such as pimavanserin or nelotanserin, and future selective 5-HT 1 and 2 agonists in the treatment of tremor (96).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Robert Fekete MD
Dr. Fekete of New York Medical College received consultation fees from Acadia Pharmaceutical, Acorda, Adamas/Supernus Pharmaceuticals, Amneal/Impax, Kyowa Kirin, Lundbeck Inc., Neurocrine Inc., and Teva Pharmaceutical, Inc.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Movement Disorders
Jan. 20, 2025
Movement Disorders
Dec. 29, 2024
Movement Disorders
Dec. 29, 2024
Movement Disorders
Dec. 29, 2024
Movement Disorders
Oct. 24, 2024
Neurogenetic Disorders
Oct. 23, 2024
Peripheral Neuropathies
Aug. 22, 2024
Movement Disorders
Aug. 22, 2024