




Epilepsy & Seizures
Tonic status epilepticus
Jan. 20, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Tuberous sclerosis complex is an autosomal dominant genetic disorder affecting multiple organ systems, with protean manifestations. In this update, the authors give a succinct overview of the topic while outlining advances in the surveillance and treatment of multiple manifestations of the disease. New trials and recommendations for the management of multiple clinical manifestations using precision medicine with mTOR inhibitors, with specific attention on neurologic issues, are discussed.
|
• Tuberous sclerosis is a neurocutaneous disorder with significant neurologic implications, especially with regards to epilepsy and cognition. There have been tremendous gains made in recognizing and managing the protean disease manifestations. | |
|
• Epilepsy is a common manifestation early in life. | |
|
• Autism spectrum disorder is a very frequent manifestation of this disease, affecting about half of all patients. | |
|
• TAND, tuberous sclerosis complex associated neuropsychiatric disorders, are increasingly recognized and include a wide range of disorders such as behavioral, psychiatric, intellectual, academic, neuropsychological, and psychosocial difficulties. | |
|
• Tumors are common and have a significantly improved prognosis with advances in treatment. | |
|
• Significant progress has occurred in the last 15 years in the management of the clinical features of the disease based on advances in understanding of the pathogenesis and pathophysiology, specifically with the use of mTOR inhibitors. | |
|
• The clinical course of the disease may be modified with the prophylactic use of antiseizure medications, which can have implications on seizure occurrence, frequency, and tractability, in addition to the clinical presentation of autism. |
Désiré-Magloire Bourneville reported “tuberous sclerosis of cerebral circumvolutions” with “confluent vesiculopapular eruption on her nose, cheeks and forehead” in the necropsy of a young girl who had recurrent status epilepticus (18). The term “tuberous sclerosis” here refers solely to the discrete pathologic entity in the brain – a distinctive cortical pathology of raised, opaque, and sclerotic cerebral gyri with a potato-like firmness. Interestingly, almost 20 years previously, and perhaps unbeknownst to him, Von Recklinghausen had reported of a newborn infant with several cardiac "myomata" and numerous scleroses in the brain (132). Bourneville also reported periventricular white nodules projecting into the lateral ventricles of the brain, and tumors in the kidneys (18).
Subsequently, dermatologists in France (07) and in England (100) described a facial hamartoma, named adenoma sebaceum, now termed facial angiofibroma, which was subsequently linked to seizures and mental retardation. Later, many authors reported of the association of “tuberous sclerosis” with dermatologic (95; 97), renal, cardiac, and pulmonary (78) abnormalities. The term “tuberous sclerosis complex,” therefore, best reflects involvement of multiple organ systems with development of distinctive tumors, or hamartomas. These associations in general and the Vogt triad (epiloia, an acronym for epilepsy, low IQ, and "adenoma sebaceum") in particular helped diagnose tuberous sclerosis complex in the living (131).
Recognition of the hereditary nature (10) of tuberous sclerosis, its wide clinical spectrum and evolution of the concept of "phacomatoses" (Greek "phakos" meaning "mother spot") (127) were seminal advances in the history of tuberous sclerosis complex. The radiological identification of intracranial calcification in tuberous sclerosis in 1924 (79) and the publication of a classic paper on this disease (24) were landmarks. Molecular techniques leading to identification of two tuberous sclerosis genes, TSC1 in chromosome 9q34.3 (48) and TSC2 in 16p13.3 (59) have been of momentous significance.
In 2006, the first case series reporting success in treating human astrocytomas with tuberous sclerosis complex by targeting mammalian (now mechanistic) target of rapamycin (mTOR) with oral rapamycin was published (46). Subsequently, reports of success of rapamycin (sirolimus) and everolimus in renal angiomyolipoma and lymphangioleiomyomatosis were published (138; 15). Everolimus and sirolimus (rapamycin) are being evaluated for multiple indications in tuberous sclerosis complex including epilepsy, subependymal giant cell astrocytomas, angiolipomas, and other tumors in multiple trials. The impact of preclinical management of epilepsy on epileptogenesis and neurodevelopment is being evaluated.
Neuroendocrine tumors (NETs) have been described in the last decade, with increasing identification of these during surveillance MRIs of the abdomen. Functional and nonfunctional pancreatic neuroendocrine tumors have been identified with insulinomas as the most common functional neuroendocrine tumors, with other neuroendocrine tumors including gastrinomas, glucagonomas, ACTHomas, and GHomas (05).
Tuberous sclerosis complex is characterized by a wide phenotypic spectrum, occurring in approximately 1 in 6000 to 10,000 individuals (107; 94). The diagnosis of tuberous sclerosis complex is based on the lesions found on clinical examination, imaging, and pathologic studies.
Diagnostic criteria have been repeatedly revised and include major and minor clinical features, in addition to clinical and genetic criteria for diagnosis (104; 90; 88).
Revised consensus clinical diagnostic criteria of tuberous sclerosis complex include major and minor features (88). Fundamental to the first revision was consensus that there are no truly pathognomonic clinical signs for tuberous sclerosis complex; the signs that were once regarded as specific sometimes occur as isolated findings in individuals with no other clinical or genetic evidence of tuberous sclerosis complex. Major features are signs with a high degree of specificity for tuberous sclerosis complex, whereas minor features are less specific. Although the skin is the most involved organ, the brain, kidneys, retina, heart, lungs, and the large arteries are all frequently involved. The revision in 2013 included genetic criteria for diagnosis and eliminated probable disease as a diagnostic class (90). In 2021, only two changes were made to the clinical diagnostic criteria reported in 2013: “multiple cortical tubers and/or radial migration lines” replaced the more general term “cortical dysplasias” and sclerotic bone lesions were reinstated as a minor criterion. Genetic diagnostic criteria were reaffirmed, including highlighting recent findings that some individuals with tuberous sclerosis complex are genetically mosaic for variants in TSC1 or TSC2 (88).
Genetic diagnostic criteria. The identification of either a TSC1 or TSC2 heterozygous pathogenic variant in DNA from normal tissue is sufficient to make a definite diagnosis of tuberous sclerosis complex. This reflects the fact that clinical manifestations of TSC develop over time and at various ages. A pathogenic variant is defined as a variant that clearly inactivates the function of the TSC1 or TSC2 proteins (eg, frameshift or nonsense variant), prevents protein synthesis (eg, large genomic deletion), or is a missense variant whose effect on protein function has been established by functional assessment.
Other TSC1 or TSC2 variants whose effect on function is less certain do not meet these criteria and are not sufficient to make a definite diagnosis of tuberous sclerosis complex. Ten percent to 15% of patients with tuberous sclerosis complex meeting clinical criteria have no mutation identified by conventional genetic testing. A normal genetic result does not exclude tuberous sclerosis complex or have any effect on the application of clinical diagnostic criteria to diagnose tuberous sclerosis complex. High-read-depth approaches to next-generation sequencing yields evidence of mosaicism and intronic mutations in some of these patients.
Clinical diagnostic criteria. Two major or one major and two minor criteria are required for definite diagnosis.
|
Major features | ||
|
1. Hypomelanotic macules (> /=3, at least 5 mm diameter) | ||
|
Minor features | ||
|
1. “Confetti” skin lesions | ||
|
Definite tuberous sclerosis complex | ||
|
1. Two major features or, | ||
|
Possible tuberous sclerosis complex | ||
|
1. One major feature or, | ||
|
If both renal angiomyolipoma and lymphangioleiomyomatosis are present, other features of tuberous sclerosis complex should be present for a definite diagnosis. | ||
Clinical manifestations according to organ systems. The type, size, number, and sometimes the location of involved lesions and organ systems dictate the clinical presentation.
Skin. Skin lesions are found in 96% to 100% of patients with tuberous sclerosis complex, who usually seek medical attention because of seizures, making it a prototypical neurocutaneous disorder. There are multiple skin lesions, including facial angiofibromas, fibrous cephalic plaques, shagreen patches, ungual fibromas, confetti skin lesions, and hypomelanotic macules (85; 106).
Of all patients with tuberous sclerosis complex, 87% have hypomelanotic macules, 75% have facial angiofibromas, 50% have shagreen patches, 21% have ungual fibromas, 3% to 58% have confetti skin lesions, and almost none are without skin lesions at all. The most common skin manifestation, the hypomelanotic macule, is best seen with a Wood’s lamp and is often noted over the buttocks and trunk. The facial angiofibromata are usually bilateral, in a butterfly distribution over the nasolabial folds and malar area. They have been recognized to manifest secondary to ultraviolent sunlight exposure as a form of a second hit (124). Shagreen patches occur over the lower trunk and flank. They may appear in the neck, upper trunk, buttocks, and thighs as well. Fibrous cephalic plaques may be the most specific dermatological finding in tuberous sclerosis complex. In addition, dental pits have been noted in 90% of the patients with tuberous sclerosis complex, approximately 10 times more often than in the general population (42).
Brain. The CNS manifestations of tuberous sclerosis complex, noted in about 90% of afflicted children, include seizures, cortical tubers, tumors, intellectual disability, autism spectrum disorder, ADHD, and sleep disorders. Tuberous sclerosis complex associated neuropsychiatric disorders (TAND) is a term to describe the wide range of disorders including behavioral, psychiatric, intellectual, academic, neuropsychological, and psychosocial difficulties associated with tuberous sclerosis complex.
Seizures are by far the most common presenting complaint (in 84% of patients and in greater than 95% of all infants). All types of seizures can occur, but the predilection is to present with infantile spasms when they occur in early infancy. A third of all children with tuberous sclerosis complex develop infantile spasms. The absence of seizures during infancy foreshadows better cognitive development. Patients with infantile spasms may progress to develop Lennox-Gastaut syndrome. Earlier onset portends a worse prognosis for developmental delays and subsequent intractable partial epilepsy. Improved development has been proven to occur when infantile spasms and partial seizures are controlled. Although infantile spasms in tuberous sclerosis complex are clinically similar to those due to other causes, the spasms may present very early and be preceded by, or coexist with, focal seizures. Subtle focal seizures, characterized by unilateral tonic or clonic activity affecting the face or limbs, eyes, and neck, may go unrecognized until there are more obvious infantile spasms (110).
Epilepsy in older children and adults with tuberous sclerosis complex is characterized by multiple seizure types. Most tuberous sclerosis complex adults have more than one seizure type, with focal-onset seizures in most (93%). Almost two thirds of epilepsy is refractory, despite using multiple antiepileptic medications and nonpharmacological approaches. The refractory group is characterized by onset of epilepsy under the age of 2, a previous history of infantile spasms or Lennox-Gastaut syndrome, lower educational achievement, a higher prevalence of psychiatric problems, and association with TSC2 mutations (110).
Cortical tubers and radial lines of migration occur in 90% of patients. Tubers are glioneuronal lesions, occurring in more than 90% of patients. CNS tumors are found in 5% to 15% of individuals afflicted with tuberous sclerosis complex. These tumors differ in their location, radiological characteristics, and biological behavior (119). Subependymal nodules are present in almost 80% of patients and can be identified prenatally or at birth. They are commonly low-grade dysplasias, which share histology with subependymal giant cell astrocytomas, whose presentation may vary from asymptomatic to obstructive hydrocephalus and death.
Subependymal giant cell astrocytomas are glioneuronal tumors located near the foramen of Munro, are greater than 0.5 cm in size, and grow and enhance with gadolinium on MRI, occurring in 10% to 15% of patients with tuberous sclerosis complex. Subependymal giant cell astrocytoma growth acceleration is related to young age, size greater than 2 cm, and TSC 2 genotype. They most commonly manifest between 8 and 14 years of age.
Less commonly, there are aggressive tumors like pineal giant cell astrocytomas, glioblastoma multiforme, or spongioblastoma. Ependymoma, neurinoma, acoustic neuroma, hemangioma, and neuroblastoma have also been reported. Hemimegalencephaly and scoliosis have been observed in a higher frequency of patients with tuberous sclerosis complex compared to normals.
Tuberous sclerosis complex-associated neuropsychiatric disorders (TAND) is terminology that describes the interrelated functional and clinical manifestations of brain dysfunction seen in tuberous sclerosis complex, with seven natural TAND clusters identified in the literature: autism-like, dysregulated behavior, eat/sleep, mood/anxiety, neuropsychological, overactive/impulsive, and scholastic (35). More than 90% of children and adults with tuberous sclerosis complex manifest one or more TAND concerns in their lifetime, but only a fraction receives evaluation and intervention for them. Given the high prevalence of TAND issues and that unaddressed TAND concerns significantly contribute to poor outcome, as well as the fact that individuals with tuberous sclerosis complex have remarkably high health care resource consumption, the importance of recognizing and addressing TAND concerns cannot be overestimated (37).
Sleep disorders, such as night waking, early waking, seizure-related sleep problems, and excessive daytime sleepiness, are among the most frequent behavioral features of tuberous sclerosis complex (51). A very high association was found with TAND in a questionnaire-based study of EPISTOP, suggesting that attention to sleep may have a positive impact on attention and behavior (84).
Autism spectrum disorder and ADHD occur in about 40% to 50% of patients with tuberous sclerosis complex, in contrast to 2% and 4%, respectively, in the general population. The specific phenotypic profile of autism spectrum disorder in tuberous sclerosis complex was reviewed and was found to converge significantly with non-syndromic autism spectrum disorder (53). Children with tuberous sclerosis complex and autism spectrum disorder are at a higher risk for global cognitive impairment than are children with tuberous sclerosis complex who do not have autism spectrum disorder (52).
Approximately 36% to 58% of children with tuberous sclerosis complex have serious academic difficulties (eg, learning disabilities) requiring intervention (34; 29; 62). The risk of learning and cognitive impairment increases significantly if seizure activity is not controlled. A number of investigations have demonstrated that a history of infantile spasms or poor seizure control in general are associated with lower intellectual ability (22; 33). Prophylactic management of patients based on early EEG changes was shown to improve cognition and seizure control, with lesser need for polypharmacy eventually (56). This has been recently questioned with the completion of the PREVeNT trial (09).
Eye. Astrocytic retinal hamartomas are found in about 50% of patients with tuberous sclerosis complex on indirect ophthalmoscopy (105). They are histopathologically similar to subependymal nodules and subependymal giant cell astrocytomas. They may continue to grow past adolescence, but they are seldom symptomatic. Pigmentary changes and punched out lesions may also be found on retinoscopy. An increased incidence of association with subependymal giant cell astrocytomas, angiofibrolipoma, cognitive impairment, and epilepsy has been noted in the presence of retinal findings (04).
Kidney. Renal lesions occur in more than half of children at the time of initial evaluation. Eighty percent of children are affected by 10 years of age (41).
|
• Simple epithelial cysts occur in up to 30% of patients and may appear or disappear at any time and commonly present with severe hypertension. | |
|
• Angiomyolipomas, which account for 75% of renal abnormalities, with a median age of detections of 8 to 13 years, increase in size with age and may become symptomatic, causing lumbar pain and hematuria. This is especially so in females by the third decade of life. Even when numerous, angiomyolipomas seldom cause renal failure or arterial hypertension. They, however, predispose to aneurysms and massive bleeding (Wunderlich syndrome), especially when the angiomyolipomas are greater than 4 cm in diameter and the aneurysms are greater than 5 mm in size (141). Malignant change occurs in less than 1%. | |
|
• Renal cell carcinoma occurs at an earlier age in tuberous sclerosis complex and is more frequent (2% to 3%) than in comparable cohorts (16; 23). Intriguingly, all histological types of renal cell carcinoma (clear cell, chromophobe, papillary, or oncocytic) have been reported in tuberous sclerosis complex. Age of diagnosis of angiomyolipomas in TSC2 is a decade earlier than TSC1, reiterating the severity of disease manifestation in TSC2 (81). | |
|
• Patients may manifest with autosomal dominant polycystic kidney disease phenotype, as the polycystic kidney disease gene, PKD1, is in proximity to the gene TSC2, on chromosome 16, accounting for the occurrence of both conditions in families with large rearrangements (contiguous gene syndromes) (19). Hypertension can present in the neonatal period. The size of the mass can affect achievement of infantile gross motor milestones and concentration defect can delay nocturnal bladder control (12). Patients with the TSC2/PKD1 contiguous gene deletion syndrome are at risk for other complications of autosomal dominant polycystic kidney disease, including intracerebral aneurysms and cystic lesions in the liver. | |
|
• Premature decline of glomerular filtration rate occurs in 40% of patients with tuberous sclerosis complex. |
Heart. Cardiac involvement is common in tuberous sclerosis complex and is found in up to 80% of patients (101). Rhabdomyomas are common in infants, occurring in approximately half who undergo echocardiography and can be diagnosed by fetal ultrasound. Most afflicted patients are asymptomatic, and their tumors regress spontaneously, often completely disappearing (134; 123). Prenatal identification of rhabdomyomas by fetal ultrasound appears to be sensitive in identifying tuberous sclerosis complex postnatally (06), with a 75% to 80% risk for tuberous sclerosis complex. Arrhythmias and symptoms due to mechanical effects of the rhabdomyomas on the heart can occur at any time as an initial presentation, although most likely in the perinatal period. Wolff-Parkinson-White syndrome can occur in the absence of rhabdomyomas (126). Giant intracranial aneurysms involving the internal carotid artery have also been reported (58).
Lung. Pulmonary issues include lymphangioleiomyomatosis, clear cell tumors of the lung, and multifocal micronodular pneumonocyte hyperplasia (99). Pulmonary lymphangioleiomyomatosis is the third leading cause of mortality after CNS and renal phenotypes (111) in tuberous sclerosis patients. The prevalence of lymphangioleiomyomatosis in tuberous sclerosis complex has been reported to be as high as 80% (25). It usually presents in women in their third or fourth decade with recurrent spontaneous pneumothorax, hemoptysis, chylothorax, and respiratory failure. An overwhelming majority of women have cystic lung disease by the age of 40. Female patients with tuberous sclerosis complex and lymphangioleiomyomatosis are also highly likely to manifest renal angiomyolipomas. Sporadic lymphangioleiomyomatosis occurs later, has a more severe course, and is also associated with renal angiomyolipomas about a third of the time. This has led to the consensus that the presence of both constitutes a single major criterion.
Blood vessels. The vascular lesions of tuberous sclerosis complex are secondary to a defect in the arterial walls of large and midsize arteries, resulting in aneurysms.
Other findings. These include angiomyolipomas in various organs, thyroid and parathyroid adenomas, liver, colon and rectal polyps, gingival fibromas, chordomas, and bone cysts. Neuroendocrine tumors (NETs) have been described in the last decade, with increasing identification of these during surveillance MRIs of the abdomen. Functional and nonfunctional pancreatic neuroendocrine tumors have been identified with insulinomas as the most common functional neuroendocrine tumors, with other neuroendocrine tumors including gastrinomas, glucagonomas, ACTHomas, and GHomas. Standard surveillance and treatment are recommended for nonfunctional pancreatic neuroendocrine tumors (05).
Rare manifestations and malignancies. Scoliosis and hemihypertrophy were more common in comparison to the general population, as were breast cancer and thyroid cancer in a report of the TuberOus Sclerosis registry to increase disease Awareness (TOSCA) (109).
Clinical manifestations by age. The clinical findings vary according to age. The fetal period may be punctuated by seizures and arrhythmias, whereas the neonate may present with Wolff-Parkinson-White syndrome, hydrops fetalis, and ultrasound evidence of multiple renal cysts or rhabdomyomas. Infantile spasms, retinal hamartomas, and the pathognomonic hypomelanotic macules mark infancy. Developmental retardation may also present during this period. Early childhood features include autism spectrum disorder, seizures, and hypomelanotic macules, whereas subependymal giant cell astrocytomas, angiofibromas, and ungual fibromas present in late childhood. Adolescents develop shagreen patches, and adults manifest with pulmonary lymphangioleiomyomatosis and renal angiomyolipomas (50).
The spectrum and severity of organ involvement determines morbidity and mortality for patients with tuberous sclerosis complex, with complications of renal disease being the most common cause of death. In general, TSC2 mutation presents with a more severe spectrum than TSC1 mutations. This historical observation was confirmed in the prospective EPISTOP study (92).
Complicated CNS involvement is a common cause of death. Children and young adults are at particular risk from status epilepticus and sudden unexpected death in epilepsy (SUDEP). Patients with severe mental retardation are at increased risk of death from respiratory infections.
Respiratory failure occurs in about 40% of patients with biopsy-proven lymphangioleiomyomatosis (111). The risk of hemorrhage is 25% to 50% in patients with renal angiomyolipomas; these patients may present in hypovolemic shock. Cardiac dysrhythmias, including Wolff-Parkinson-White syndrome, may be problematic, although death from obstruction of ventricular outflow is rare (91). Severe congestive cardiac failure can occur in infancy. Thoracic and abdominal aneurysms can present anytime during childhood, including infancy, and have a high likelihood of rupture.
The natural history of the disease is changing with precision medicine, specifically with mTOR inhibitors to prevent progression of angiolipomas that hemorrhage, and early use of antiseizure medications, which have been shown to prevent cognitive decline. Early management of frequent interictal discharges has been shown to improve seizure control and may have a positive impact on cognitive functioning.
A 7-month-old girl presented with a history of spells manifesting for 1 week prior to presentation to the physician. These episodes were characterized by a brief flexion of her neck and abduction and extension of the arms. They occurred 15 to 20 times in a cluster, many times a day, predominantly while awakening. The clusters had been gradually lengthening in duration over time. She occasionally cried after a cluster. She had stopped smiling and tracking. She no longer cooed or played with her toys.
She was born vaginally at term following an uncomplicated pregnancy. Her birth was unremarkable except for an episode of tachycardia diagnosed as Wolf-Parkinson-White syndrome. Her development had been age appropriate, and the family history was characterized by a birthmark in her father over his back, which was consistent with a shagreen patch on examination.
On exam she was nondysmorphic and alert. She did not smile, coo, or track consistently. On Wood’s light exam, she had a few hypopigmented macules on her trunk, in addition to café-au-lait spots. Cranial nerve exam was normal for her age. There was neck lag on pulling to sit and appendicular hypotonia.
Brain MRI revealed cortical tubers and subependymal nodules on both T1 and T2 images. Cardiac echo revealed a rhabdomyoma. EEG revealed multifocal interictal discharges and electrodecrement correlating with clinical events of infantile spasms but did not reveal hypsarrhythmia. The child was initiated on vigabatrin at an escalating dose to a maximum of 150 mg/kg/day and did well without clinical seizures for the next 10 days, after which seizures recurred. She was initiated on prednisolone with good benefit.
This child met the criteria for definite tuberous sclerosis complex, having four major criteria for diagnosis. The high likelihood of seizures in the first year of life is exemplified in this case, as well as the occurrence of infantile spasms without hypsarrhythmia. The case reiterates the difficulty in the management of seizures despite the use of the currently recommended first-line therapy, vigabatrin.
mTOR dysregulation is associated with most manifestations of the disease complex.
Genetics. Tuberous sclerosis complex is an autosomal-dominant disorder caused by a genetic mutation in one of two different genes. Chromosomal bands 9q34.3 and 16p13.3 are the loci for the two genes; they are respectively called TSC1 (tuberous sclerosis complex 1) and TSC2 (tuberous sclerosis complex 2) (48; 59). The 16p13.3 TSC2 gene, identified first, and its 5.5 kilo base TSC2 transcript encode a 200 KDa protein called tuberin. The 9q34.3 TSC1 gene, identified from a 900-kilobase region containing over 30 genes, and its 8.6 kilo base TSC1 transcript encodes a 140 KDa protein called hamartin.
As of October 23, 2024, 1426 unique allelic DNA variants of TSC1 and 4580 unique DNA allelic variants of TSC2 have been reported. More information is available at LOVD tuberous sclerosis database.
Pathogenic variants in TSC2 and TSC1 occur in a 2:1 ratio among tuberous sclerosis complex patients. Only 5% to 10% of patients have no mutation identified or a variant of unknown significance after assessment with ultra-deep next-generation sequencing. Some patients previously assessed to have no mutation identified often have had low level mosaic pathogenic variants or pathogenic variants in introns that affect splicing.
There are differences in the phenotypic expressions of TSC1 and TSC2 gene mutations. For instance, TSC2 mutations express a more severe phenotype – more severe renal involvement, intellectual disability, more cerebral and facial lesions, less reproductive fitness (54), and more pulmonary involvement. Complex partial seizures, focal seizures, and infantile spasms are more likely in TSC2. There does not appear to be a strict correlation between mutation and clinical phenotype. Mutation occurrence is more common in TSC2, accounting for 75% to 80% of sporadic cases. About 80% of cases are caused by de novo mutation (104), with an estimated 15% or more of the individuals with tuberous sclerosis complex exhibiting somatic mosaicism and another 1% or so having germline mosaicism. Tuberous sclerosis complex could appear as sporadic disease in the general population.
Response of tumors including subependymal giant cell astrocytomas and angiomyolipomas to mTOR inhibitors is independent of mutation type and also occurs in patients with no mutation identified (96).
Cell biology and pathophysiology. The pathology of tuberous sclerosis complex reflects abnormalities in cell size, number, morphology, and location, implying multiple roles of the genes. Wild TSC2 and TSC1 function as tumor suppressor genes. With the mutation of either one, their defective product is unable to inactivate the tumor growth caused by a second random somatic cell mutation (loss of heterozygosity). The multifocal nature of tuberous sclerosis complex is best explained by the Knudson 2-hit hypothesis, where the second hit is a somatic mutation that completely abrogates TSC1-TSC2 function by accelerating the effect of the first systemic hit/mutation. Both alleles of TSC1 or TSC2 need to be inactivated for development of tumors, ie, loss of heterozygosity.
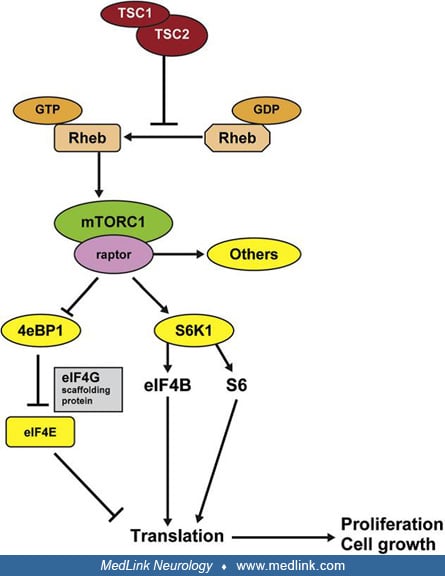
The protein products tuberin and hamartin function together with the protein product of the TBC1D7 gene in cellular signaling pathways (128; 129), forming the TSC protein complex. The TSC protein complex is purported to participate in protein translation, cell growth, proliferation, adhesion, migration, and intracellular trafficking. The TSC complex is the principal cellular inhibitor of the mechanistic target of Rapamycin (mTOR, previously called mammalian target of rapamycin) (93), while also being the sensor of cellular growth conditions. Thus, mutation of hamartin or tuberin in tuberous sclerosis complex leads to hyperactivation of the downstream mTOR pathway and the associated kinase signaling cascades and translational factors, resulting in increased cell growth and proliferation. Tuberin and hamartin are coexpressed in several cells, including kidney, brain, lung, and pancreas, and mutations in either hamartin or tuberin lead to a single disorder.
By sharing homology with a GTPase activating protein for Rap 1 and GTPase Rheb (Ras homologue enhanced in brain), the TSC complex inactivates GTP-bound Rheb (142). Active Rheb is an upstream positive modulator of mTOR (115). Therefore, a loss of function mutation in TSC1-TSC2 will enhance Rheb, activate mTOR constitutively, and critically upregulate cell growth and proliferation through p70S6kinase (72), ribosomal S6 proteins, and eukaryotic initiation factor 4E binding protein 1 (4E-BP1).
Mechanistic target of rapamycin, mTOR, exists as two complexes with differing functions. mTOR complex 1 (mTORC 1) with its cofactor, Raptor (regulatory associated protein of mTOR), activates mTOR’s protein kinase domain and is sensitive to rapamycin. This activation results in increased mRNA transcription and protein synthesis. TSC mutation leads to loss of inhibition of mTORC1. This causes constitutive activation of mTOR and, in turn, abnormal cellular proliferation and differentiation, producing the hamartomatous lesions of tuberous sclerosis complex. mTOR complex 2 (mTORC 2), with its cofactor Rictor (rapamycin insensitive component of mTOR), regulates protein synthesis in a manner distinct from mTORC1 and is unaffected by Rheb or rapamycin.
Loss of TSC1 or TSC2 in mature postmitotic hippocampal neurons in vitro causes enlarged somas, abnormal dendritic spines, and enhancement of glutamatergic neurotransmission. Elevated extracellular glutamate levels are assumed to contribute to excitotoxic neuronal death, abnormal glutamatergic synaptic physiology, and impaired behavioral conditioning and learning (87). It has been shown that the seizure activity often originates from the mildly hypometabolic regions adjacent to the cortical tubers rather than directly from the tuber in humans. mTOR dysregulation is also involved in tuberous sclerosis–related epileptogenesis through a range of potential mechanisms, including alteration of neuroblast migration, cortical lamination, cell body size, and dendritic arborization, synaptic plasticity, and by altering neuronal excitability through modulation of the expression of voltage-gated potassium channels.
Risk of epilepsy and encephalopathy are associated with TSC2 genotype, TSC2 mutation, abnormal neuronal morphology, disruption of GABAergic interneuron development, abnormal astrocyte glutamate uptake, synaptic abnormalities, inflammatory changes, impaired long-term potentiation, high tuber brain proportion, and white matter abnormalities (139; 26). mTOR dysregulation is thought to affect the maturation of the GABAergic system, leading to a ‘‘GABAergic immaturity,’’ which may contribute to the development of epilepsy. Widespread hypo-/ dysmyelination has emerged as an important pathological component underlying the complex clinical phenotypes in patients with tuberous sclerosis complex.
Tuberous sclerosis complex occurs in 1 of 6000 to 10,000 individuals, with two thirds of cases being sporadic (94). A study in Sweden showed a peak prevalence of 1 in 6800 for individuals between 11 and 15 years of age, and 1 in 12,900 for all individuals younger than 20 years of age. The TSC2 gene is associated with the vast majority of cases, both familial and sporadic. Boys are typically more severely affected.
Tuberous sclerosis complex is of autosomal-dominant inheritance with high penetration; the risk of an affected parent having an affected child is 50%. However, occurrence of tuberous sclerosis complex in a majority is sporadic and, in part, may be because there exists high intrafamilial heterogeneity. Thus, a mildly affected asymptomatic parent is at considerable risk of having a child with epilepsy and severe mental retardation. The mutation rate for tuberous sclerosis complex is high, and most of the severely affected children have a new mutation. Reduced expression of the gene, non-expression, and somatic and germline mosaicism make determination of the true rate of mutation difficult. Prenatal detection of tuberous sclerosis complex in an at-risk fetus is possible by echocardiography or ultrasonography, demonstrating cardiac rhabdomyomas or multicystic kidneys. A prenatal head MRI may be helpful after the 20th week of gestation to identify large cortical tubers.
Preimplantation and prenatal genetic tests are available and should be offered in addition to genetic counseling. Linkage studies of the entire family with affected and unaffected individuals may be done. Mutational analysis and multiplex ligation-dependent probe amplification have been used to assess genotype and phenotypic correlation.
Tuberous sclerosis complex is a systemic disorder involving multiple organs, including brain, skin, heart, lungs, and kidneys; only skeletal muscle, peripheral nerves, and craniospinal nerve roots are not involved. Consequently, the differential diagnosis of each presenting symptom or constellation of symptoms is extensive. This necessitates that tuberous sclerosis complex be considered in the differential diagnosis of many presenting problems, including seizures, developmental delay or mental retardation, autism spectrum disorder, ADHD, hemiplegia, uremia, intra-abdominal hemorrhage, and respiratory failure. Similarly, tuberous sclerosis complex should be considered the underlying cause of various tumors that may occur in different organ systems. However, tumors that occur in tuberous sclerosis complex are typically rare in the general population and infrequently progress to malignancy. Only renal cell carcinoma occurs earlier and with greater frequency in tuberous sclerosis complex (16; 23).
All patients should have a 3-generation family history obtained to determine if additional family members are at risk of diagnosis. Genetic testing is recommended for counseling purposes or when the diagnosis of tuberous sclerosis complex is suspected but cannot be clinically confirmed. A negative genetic test result does not exclude tuberous sclerosis complex diagnosis. Patients that meet clinical criteria for tuberous sclerosis complex have the diagnosis regardless of the results of the genetic testing.
Evaluation for initial diagnosis and clinical monitoring requires attention to the following organ systems: (1) the skin, with natural and ultraviolet light, looking for facial angiofibroma, shagreen patches, fibrous cephalic plaques, periungual fibromas, and hypomelanotic spots; (2) the retina, by indirect ophthalmoscopy after mydriasis; (3) the brain, with MRI and EEG; (4) the kidneys, with MRI, assessment of glomerular filtration rate, proteinuria, and blood pressure; (5) the lungs, with imaging by low-dose CT in adults, particularly women and symptomatic men, in addition to pulmonary function tests; (6) the heart, with fetal echocardiogram if prenatal ultrasound reveals rhabdomyomas, echocardiogram in pediatric patients under 3 years of age, and routine ECGs in all patients (49); and (7) a detailed dental examination.
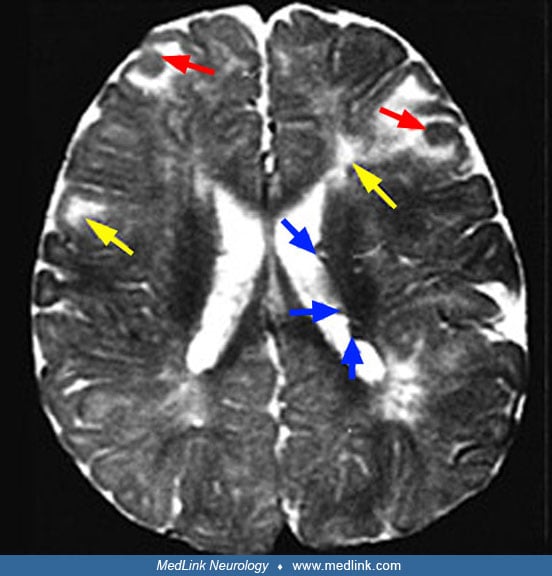
Studies with MR of the brain have found that T1-weighted imaging is best for identification of subependymal nodules, whereas fluid-attenuated inversion recovery pulse images are more sensitive than spin-echo sequences to cortical and subcortical tubers (60). T2-weighted images may show subcortical white matter changes, and shadows from subependymal nodules may indent the walls of the ventricles. It is recommended to avoid contrast agents in MRI until there is a clinical suspicion for subependymal giant cell astrocytomas or a growing lesion due to the expected need for lifelong repeated scans and the adverse effects of contrast agents. MR imaging demonstrates cyst-like structures that are commonly seen immediately adjacent to cortical tubers or within dysplastic lesions (130).
Newer imaging modalities are becoming available for evaluating the disease burden and for noninvasive surgical planning. They have added significantly to our knowledge of the disease. Magnetization transfer imaging (MTI) can depict more tubers and white matter anomalies than conventional spin echo images in older children and adults. Dual inversion recovery MRI has been reported to depict cortical tubers as very bright signals in comparison to high-resolution T2 or FLAIR imaging. Computational morphometric MRI has been used to objectively quantify the brain lesions in tuberous sclerosis complex. This has revealed that the highest frequency of tubers is in the frontal lobes and the highest density is in the parietal lobe. Decreased bilateral gray matter volumes and white matter tracts have been reported to correlate with memory deficits in tuberous sclerosis complex. Proton magnetic resonance spectroscopy (MRS) studies have shown a pattern of decreased N-acetylaspartate/creatine and increased myoinositol/creatine ratios in tubers, reflecting decreased neurons and increased glial cells, respectively. Evidence of hypomyelination in tuberous sclerosis complex is also reflected by the low fractional anisotropy values of the perilesional white matter. Increased apparent diffusion coefficient (ADC) value has been noted in epileptogenic tubers and hamartomas and may be used to identify the epileptogenic cortical tuber. Diffusion tensor imaging (DTI) can potentially be used to detect and define epileptic circuitry as it evolves with chronicity and increasing severity of epilepsy. Interictal 2-deoxy-2-[18F]fluoro-D-glucose positron emission tomography (FDG-PET) scanning in tuberous sclerosis complex has detected small cortical tubers similar to FLAIR images, but with a larger area of glucose hypometabolism. Alpha[11C]methyl-L-tryptophan positron emission tomography (AMT-PET) has been used in the identification of the epileptogenic zone (77). MRI with HASTE (Half Fourier Acquisition with Single shot Turbo spin Echo) and MPRAGE (Magnetization Prepared Rapid Gradient Echo) are newer modalities used to assess for subtle evidence of cortical tubers and subependymal nodules (68). Arterial spin labelling (ASL) sequences in MRI have been reported to help to identify tubers in early childhood in relation to EEG slow waves, but this needs further validation.
Genetic testing. The gold standard genetic test recommended is a concurrent TSC1/TSC2 next-generation sequencing panel and deletion/duplication analysis. A multigene panel, including TSC1 and TSC2, among others, may be considered when the diagnosis of tuberous sclerosis complex is less certain. It is ideal that this panel includes deletion/duplication analysis.
Genetic testing is indicated if: (1) clinical features do not permit a definite diagnosis; and (2) there is benefit from identification of the causative mutation for screening of family members or for prenatal or preimplantation diagnosis.
Conventional genetic testing with Sanger sequencing and deletion/duplication analysis only yields a diagnosis in 75% to 90% of patients. Next-generation sequencing yields a higher yield, including cases with mosaicism and intronic variants affecting splicing.
The LOVD database can be used for clarification of pathogenic variants. Occasionally variants may only be detected in saliva or skin cells rather than blood. When an extremely low-level variant is identified, presence of the same variant should be confirmed in multiple tissue samples.
Multispecialty involvement is indicated in the management, and regional tuberous sclerosis complex clinics in the United States specialize in this. The website for the Tuberous Sclerosis Alliance is a comprehensive resource for physicians and patients alike. Consensus clinical management and surveillance recommendations for individuals with tuberous sclerosis complex have been published (88; 112). The TuberOus Sclerosis registry to increase disease Awareness (TOSCA registry) was established internationally to clarify the natural history and eliminate lacunae in knowledge of the disease (62).
Health care transition from pediatric to adult care is recognized to be challenging in chronic diseases, including tuberous sclerosis complex, leading to a consensus statement from the Child Neurology Foundation outlining the role of the child neurologist in this transition (20).
|
Organ system or |
Recommendations for surveillance |
|
Genetics |
1. Obtain three-generation family history to assess for additional family members at risk of tuberous sclerosis complex. |
|
Brain |
1. Obtain MRI of the brain to assess for the presence of tubers, subependymal nodules, migrational defects, and SEGA. |
|
TAND |
1. Perform comprehensive assessment for all levels of potential TAND manifestations. |
|
Kidney |
1. Obtain MRI of the abdomen to assess for the presence of angiomyolipomas and renal cysts. |
|
Lung |
1. Inquire about tobacco exposure, connective tissue disease manifestations, signs of chyle leak, and pulmonary manifestations of dyspnea, cough, and spontaneous pneumothorax in all adult patients with tuberous sclerosis complex. |
|
Heart |
1. Consider fetal echocardiography to detect individuals with a high risk of heart failure after delivery when rhabdomyomas are identified via prenatal ultrasound. |
|
Eye |
Perform a complete ophthalmologic evaluation, including dilated fundoscopy, to assess for retinal findings (astrocytic hamartoma and achromic patch) and visual field deficits. |
|
(88) | |
Surveillance for epilepsy. Seizures should be considered a medical emergency in infants as refractory epilepsy is highly correlated with poor developmental and cognitive outcomes.
The large TOSCA Registry multinational, multicenter observational study over 5 years confirmed the high prevalence of epilepsy in individuals with tuberous sclerosis complex (85%) and less severe phenotypes with TSC1 mutations. Vigabatrin improved the outcome of infantile spasms and was recommended as first-line treatment by the authors. Focal seizures were associated with high degrees of drug resistance (86).
EPISTOP, a long-term, prospective study evaluating clinical and molecular biomarkers of epileptogenesis in a genetic model of epilepsy - tuberous sclerosis complex, was the first prospective study of epileptogenesis in human infants with tuberous sclerosis complex (110). Among other things, the trial monitored babies using serial EEGs, with a choice to use vigabatrin based on a deteriorating EEG prior to clinical seizures. The study revealed that epileptiform discharges on EEG typically appear before the age of 3 months and often with a multifocal distribution. Early onset of epileptiform discharges as well as focal slowing were associated with earlier seizure onset. Early appearance of epileptiform discharges was associated with worse developmental outcome. Infants with tuberous sclerosis complex presenting with multifocal interictal discharges had a higher risk of drug-resistant epilepsy and benefited more from preventive vigabatrin treatment in delaying seizure onset (33).
EEG is recommended at the initial diagnosis of all patients, irrespective of a history of seizures. This should be followed by 8- to 24-hour video EEG monitoring if there are any abnormalities on routine EEG or if there are any symptoms of neuropsychiatric disease or suspected clinical seizures. Per European guidelines, routine EEG monitoring is recommended every 4 weeks for the first 6 to 8 months, every 4 to 8 weeks until 12 months, and then every 3 months until 2 years of age (112), although the current literature also suggests EEG every 6 weeks for the first 12 months, and every 12 weeks until 24 months of age (89).
Prophylactic management of patients based on early EEG changes has been shown to improve cognition and seizure control with lesser need for polypharmacy eventually (56). In the EPISTOP trial, preventive treatment with vigabatrin was safe and modified the natural history of epilepsy in tuberous sclerosis complex. The time to first clinical seizure was significantly longer with preventive treatment than conventional treatment, by about four times. At 24 months, the pooled analysis showed that preventive treatment significantly reduced the risk of clinical seizures by two thirds, drug-resistant epilepsy by greater than 2-fold, and completely prevented the occurrence of infantile spasms (67). Results of the PREVeNT trial were conflicting in that they did not reveal any improvement in cognition or decrease in focal seizures with preventative treatment with vigabatrin, although there was a delay in onset and decrease in incidence of infantile spasms (09). This was a phase IIb multicenter, randomized, double-blinded, placebo controlled trial, at 13 tuberous sclerosis complex clinics across the United States. Infants were placed in the watchful waiting phase until interictal discharges were identified on 6 weekly EEGs, at which time they were randomized to the blinded treatment phase of the study, with vigabatrin versus placebo. Those who seized clinically without prior abnormalities on EEG were directly treated with open-label vigabatrin. Those with no abnormalities on EEG and remained seizure-free were never randomized to treatment. With the conclusion of the study at 24 months of age, the Bayley-III cognitive assessment score and the Vineland-II adaptive behavioral score at 24 months were administered and found to have no differences between those treated early with vigabatrin at time of first abnormal EEG and those treated traditionally at the time of first seizure. There was no difference in the onset of focal seizures or the incidence of drug resistant epilepsy at 24 months of age (09).
Eligibility criteria, EEG monitoring, and follow-up procedures were similar between the two studies. The PREVeNT study was more statistically robust, with the double-blind, placebo controlled design. In contrast, EPISTOP treatment trial was open label, with randomization or study site determining whether vigabatrin therapy was started at time of EEG abnormalities versus waiting until onset of clinical seizures. A centralized EEG review process determined randomization in PREVeNT versus local EEG review and randomization in EPISTOP. Findings from both the randomized control and open label trials were combined to reach conclusions in the EPISTOP trial. Additional investigation is needed to understand what was responsible for the differences in seizure outcomes between the studies.
A new clinical trial, TSC-STEPS, is underway in the United States and Australia, evaluating the benefit of early treatment with sirolimus, an mTOR inhibitor, before 6 months of age in tuberous sclerosis complex infants, with expected completion in June 2026. Another study, ViRap, is underway, testing benefits of sirolimus versus vigabatrin on occurrence of clinical seizures in infants and the volume of tuberous sclerosis complex-associated tumors at 2 years of age, with expected completion in March 2026.
Drug treatment in epilepsy. First seizures in infancy can be focal clonic seizures or infantile spasms or both. Infantile spasms can frequently occur without hypsarrhythmia. Seizures are frequently refractory to treatment. The Updated International TSC Diagnostic Criteria and Surveillance and Management recommendations, as an outcome of the 2018 World TSC Conference (88) and the UK guidelines (01), recommend vigabatrin as the first drug of choice for both infantile spasms and focal seizures secondary to tuberous sclerosis. A literature review suggests that 25 to 50 mg/kg per day may be a good starting point, with a plan to rapidly titrate every 3 days up to 100 to 150 mg/kg per day of vigabatrin. Vigabatrin was approved in the United States in 2009 for the adjunctive treatment of refractory complex partial seizures and as treatment of infantile spasms (118). Generic vigabatrin was approved by the U.S. Food and Drug Administration in January 2019. Presymptomatic treatment with vigabatrin is the standard of care in Europe (112), upon recognition of abnormalities on scheduled EEG, although with the recently published PREVeNT trial, there is some conflict about this (03).
Approximately one in three individuals on vigabatrin suffer visual field loss, revealing a progressive “dose-adverse response” relationship. In a study, the lowest cumulative dose causing defects was 720 g, and the shortest duration of vigabatrin causing defects was 24 months (103). Patients on vigabatrin need close monitoring for visual field defects with any of the several known ocular techniques. These could include electroretinography, multifocal electroretinography, electrooculography, field-specific visual evoked potentials, and optical coherence tomography. Some of these techniques require sedation or anesthesia and certain centers have adopted regular ophthalmology evaluations instead. Visual field testing is recommended at the onset of therapy, at 3-month intervals for the first 18 months, and every 6 months afterwards. Recent data published from the U.S. vigabatrin registry that followed greater than 9000 patients on vigabatrin for up to 16 years did not find that any patient experienced clinical vision loss, few (2%) patients experienced new vision findings over time, and none were determined to be caused by vigabatrin (43). Insomnia, agitation, and constipation occur in fewer patients. Profoundly decreased liver transaminases may occur in up to 90% of patients and mask liver injury from simultaneously used antiseizure medications and cannabidiol. Characteristic T2-weighted MRI brain changes have been observed in patients on vigabatrin in the brainstem, cerebellum, and basal ganglia, with some evidence of association with higher doses and possible abrogation with the simultaneous use of mTOR inhibitors.
If resolution of the hypsarrhythmia pattern on EEG (when present) and abatement of infantile spasms does not occur within 2 weeks, adrenocorticotropic hormone (ACTH), synthetic adrenocorticotropic hormone, or prednisolone can be added as second-line therapy.
Adults can manifest with seizures at any age, and seizures can change in type or semiology and resolve. New-onset seizures or a change in semiology must be evaluated with imaging for other etiologies, including growth of a SEGA, stroke, bleed, and new glioma, among other etiologies.
Following the EXIST-3 study, everolimus has been approved by the U.S. Food and Drug Administration for the adjunctive treatment of refractory partial-onset seizures in tuberous sclerosis complex if two antiseizure drugs have been ineffective in children older than 2 years old. As the only oral MTOR inhibitor, it works primarily on MTOR 1, leading to lesser impact on glucose tolerance. Target drug concentration of 5 to 9 ng/ml is recommended for everolimus. Sirolimus can also be used for treatment of epilepsy.
The results of a randomized, multicenter, placebo-controlled phase 3 study of adjunctive everolimus in 366 individuals for refractory focal epilepsy in tuberous sclerosis complex (EXIST-3) revealed that both low-dose and higher dose everolimus led to the primary endpoint of 50% reduction in seizure frequency (p < 0.008, and p < 0.001) in comparison to placebo (47). The percentage reduction of seizure frequency was also statistically significant. The greatest response was in the group with children younger than 6-years-old, in contrast to other older ages. The extension of the randomized control trial to 48 weeks duration involved 361 of the 366 patients receiving the everolimus from 18 weeks to over 2 years. A trough range of 3 to 15 ng/ml of the everolimus was the goal. Responses improved with time, with a response rate of at least a 50% reduction in seizure frequency reaching greater than 40% at 2 years (44) and 19% of patients achieving seizure freedom (71). A small study showed a decrease in frequency of interictal discharges and significant decrease in seizure frequency with the prolonged use of everolimus over 27 months, with improvement in cognition associated only with complete cessation of interictal discharges (137).
Cannabidiol was approved in 2021 as antiepileptic management in tuberous sclerosis complex in patients older than 12 months old following a multicenter placebo-controlled trial, GWPCARE6 (116). In the study, the maximum dose of cannabidiol 25 mg/kg/day had a similar efficacy as a higher dose of 50 mg/kg/day and fewer adverse effects. An open-label long-term extension of this trial that evaluated the long-term safety and efficacy of cannabidiol in patients with tuberous sclerosis complex revealed a median percentage decrease in seizures of 54% at week 12, which was sustained at 48 weeks (117). There was meaningful improvement in quality of life in more than 80% of patients.
There is no head-to-head study for the preferred antiepileptic medication, including everolimus and cannabidiol, for localization-related epilepsy. Several medications are used, and polypharmacy is common. It is recommended that Epidiolex be taken with high fat foods consistently, as systemic bioavailability has been shown to increase by approximately 4-fold when taken with high-fat meals and by approximately 3-fold with low-fat meals or whole milk. If Epidiolex is added to clobazam, dose reduction in clobazam is indicated if there is sedation. When Epidiolex is used with valproate, liver function tests are to be monitored regularly. Transaminitis is common within a month of initiating cannabidiol with valproate and typically resolves following dose changes or discontinuation of the antiseizure medication or cannabidiol. When Epidiolex is used with mTOR inhibitors, mTOR inhibitor levels need to be monitored, and the doses of these may need to be adjusted to avoid significant toxicity (136). GABAergic medications are suggested, including topiramate, carbamazepine, and oxcarbazepine as other choices (28). In 2022, oral ganaxolone was approved for seizures in CDKL5 deficiency disorder in patients 2 years of age and older (73). It is currently undergoing phase III evaluation for the treatment of tuberous sclerosis complex–related epilepsy.
Studies suggest that carbohydrate restriction alone (ie, modified Atkin® or low glycemic index diet) may have similar benefits to that of the classical ketogenic diet. Ketogenic diet is recommended in early childhood refractory epilepsy, even with vigabatrin (30). Ganoxolone is being evaluated in a phase III study (TRUSTTSC) for epilepsy management in tuberous sclerosis complex.
Surgery in epilepsy. Patients with focal seizures should be considered for epilepsy surgery (08), promptly if three medications have failed. The source of the seizures can be identified and resected even if other tubers or diffuse EEG abnormalities are present. In patients with unlocalized epilepsy patterns, seizure control may be obtained by corpus callosotomy (64). Surgical treatment of patients with tuberous sclerosis complex and intractable epilepsy is most effective when a single tuber or epileptogenic area can be identified. Early epilepsy surgery has been advocated for better prognosis in intractable epilepsy (140). Overall postoperative seizure freedom is achieved in 50% to 60% of tuberous sclerosis complex patients, and greater than 50% seizure reduction is seen in another 15%, even in patients with multiple tubers. A study revealed that the long-term outcomes of seizure freedom and neuropsychiatric abilities were improved with earlier surgery, early achievement of seizure freedom, and better presurgical cognitive abilities (75).
In a large, nationwide multicenter study on resective epilepsy surgery from China, surgery resulted in improved seizure outcomes, quality of life, and intelligence quotient in patients with tuberous sclerosis complex (76). Seizure freedom was more likely in patients with a large and calcified tuber on MRI, total removal of epileptogenic tubers, and tuberectomy plus lobectomy.
Vagus nerve stimulation and responsive neurostimulation may be effective in select adults with tuberous sclerosis complex in intractable seizures. MRI-guided laser interstitial thermal therapy (LITT) may be an option as well, which allows tissue to be thermocoagulated via a stereotactically placed laser for precise control of the resection topography with real-time monitoring of the delivery temperature, thereby allowing management of individuals initially recused due to proximity to eloquent brain structures (121).
Surveillance and management of subependymal giant cell astrocytomas (SEGAs). SEGAs need to be managed with serial MRI every 1 to 3 years until the age of 25 years, even if they are asymptomatic. Monitoring every 6 months is recommended for SEGAs greater than 1 cm in size. More frequent monitoring is also recommended in those with growing SEGAs or those who are impaired enough to not reliably report symptoms. Neuroimaging should be continued beyond 25 years in patients as SEGAs may grow in adulthood or, rarely, present newly in adults.
Signs of increased intracranial pressure, positional headache, irritability, and loss of seizure control should be recognized as possible indicators of a symptomatic subependymal giant cell astrocytoma and urgent neuroimaging should be performed in such an instance.
Gross total resection is the procedure of choice for management of acute deterioration due to SEGAs and is usually curative (57). Surgery is indicated for asymptomatic SEGAs, if there is ventriculomegaly, or increase in size of the lesion on imaging. Newer surgical modalities, including minimally invasive techniques, endoscopic resections, and LASER interstitial thermal therapy, have been trialed.
mTOR inhibitors are recommended in patients with asymptomatic growing, large, or multiple SEGAs as well as in those with mild or moderate symptoms, those who are not surgical candidates or have regrowth after surgery or incomplete resection, and those who prefer medical treatment over surgery. They can also be used to facilitate surgery by shrinking the tumor, reducing vascularity, and improving the tumor–brain interphase. Regrowth is known to occur on discontinuation of mTOR inhibitors (69). Everolimus was approved by the FDA in 2010 for SEGA management.
Everolimus has been used in children as young as 12 months of age with excellent benefit in SEGA size and seizure control (EXIST-1 trial) (66). An extension prospective study over 4 years confirmed the sustained efficacy of everolimus in reducing SEGA tumor burden. Almost 60% of patients who received treatment for 4 years exhibited a clinically relevant (30%) reduction in their primary SEGA (44). The EMINENTS study, performed in a small cohort of patients, revealed that a smaller and less frequent dosage of everolimus may be a reasonable maintenance protocol once the standard protocol of daily everolimus to maintain a serum level of 5 to 15 ng/ml is used with good efficacy in SEGA patients for at least a year (122). The final results of the EMINENTS study after 60 months confirmed that a similar maintenance therapy with everolimus might represent a rational therapeutic option for patients with tuberous sclerosis complex with SEGA after effective full-dose treatment (17).
Tuberous sclerosis–associated neuropsychiatric disorders (TAND). Early psycho-educational or neuropsychological assessment is important to identify problems in cognitive development and to develop appropriate teaching strategies. Problems with inattention, hyperactivity, aggression, or autistic features may necessitate psychological or psychiatric consultation. The transition from special education resources in the classroom to vocational rehabilitation opportunities in young adulthood should be carefully monitored (36). Periodic assessment is advised at each developmental age in childhood to tailor appropriate support services through the school, and psychosocially. An excellent review on TAND is available (38), as are the consensus recommendations for identification and management of TAND (35). Tools like the TAND-L or TAND-SQ checklists are well suited for regular screening and can be used by any professional who is supporting an individual who lives with TSC (TAND-L) or by families themselves (TAND-SQ). If concerns are identified on screening, referral to relevant professionals is indicated.
The 10 core principles for the identification and treatment of TSC-associated neuropsychiatric disorders were noted as follows (35):
|
1. Everyone with tuberous sclerosis complex is at risk of TAND. | |
|
2. Everyone with tuberous sclerosis complex needs lifelong monitoring for the emergence of TAND. | |
|
3. Screen at least annually and follow up with appropriate action. | |
|
4. The goal is early identification and early intervention. | |
|
5. TAND clusters cluster together. | |
|
6. Always consider the impact of physical health problems and medications for physical health problems on TAND. | |
|
7. Work with families and caregivers as lived experts in tuberous sclerosis complex and TAND. | |
|
8. Generate a “bio-psycho-social” “whole-system” plan for intervention. | |
|
9. Be evidence-based and evidence-informed. | |
|
10. Strive for optimal functional outcomes and quality of life throughout the journey with tuberous sclerosis complex and TAND. |
EPISTOP aimed to identify the early clinical markers of autism spectrum disorder and developmental delay in infants with an early diagnosis of tuberous sclerosis complex. Eighty-two infants with tuberous sclerosis complex (6 to 24 months of age) were prospectively evaluated using a detailed neuropsychological assessment: Bayley Scales of Infant Development (BSID) and Autism spectrum disorder Diagnostic Observation Schedule (ADOS). The normal cognitive developmental quotient at 12 months excluded subsequent autism spectrum disorder (negative predictive value 100%). The total score of ADOS at 12 months clearly differentiated children with a future diagnosis of autism spectrum disorder from children without. Atypical socio-communication behaviors were more frequently observed than stereotyped and repetitive behaviors in children with autism spectrum disorder at 24 months. The combined use of BSID and ADOS can reliably identify infants with tuberous sclerosis complex with a higher risk for autism spectrum disorder at 6 to 12 months of age, allowing clinicians to target the earliest symptoms of abnormal neurodevelopment with tailored intervention strategies (83).
The PREVeNT trial did not find any cognitive or developmental benefits of early treatment with vigabatrin in infants with tuberous sclerosis complex who had not yet developed in 2024.
Surveillance and management of renal complications. Blood pressure, urine for proteinuria, and renal function (with glomerular filtration rate) must be monitored annually. In patients with elevated office blood pressure, 24-hour ambulatory blood pressure measurement is indicated. Measurement of serum creatinine or cystatin C concentration can be used to evaluate glomerular filtration rate. Poor muscle bulk may lead to artificially elevated estimated glomerular filtration rate based on creatinine. It is critical to manage the severe hypertension associated with renal cysts appropriately, as surgical decompression alone to relieve parenchymal compression is inadequate. Lower blood pressure targets are recommended in patients with TSC2/PKD1 contiguous gene syndrome (81). Caution must be exercised in use of ACTH/prednisone for infantile spasms in the above setting, especially with coexistent polycystic kidney disease. A renin-aldosterone-angiotensin system inhibitor is advised as first-line therapy for hypertension. Evidence does not support previous recommendations to avoid angiotensin converting enzyme inhibitors in patients on mTOR inhibitors. eGFR and proteinuria should be assessed every 3 to 12 months in patients receiving an mTORC1 inhibitor. Zonisamide and topiramate used as antiseizure medications increase the risk of nephrolithiasis.
It is recommended that newly diagnosed cases of tuberous sclerosis have renal MRI scanning for early detection of polycystic kidney disease associated with contiguous gene deletions spanning the TSC2/PKD1 genes. Lifelong renal MRI is recommended every 1 to 3 years in all age groups because renal angiomyolipomas may enlarge rapidly, even in children, and recur (41). MRI is preferred over ultrasound imaging as a fourth of renal angiomyolipomas are fat poor. If MRI is unavailable, abdominal CT with contrast is recommended. Frequency of scans should be annual in patients with tumors approaching 3 cm in size or growing. Immunologic staining for HMB-45 for angiomyolipomas and cytokeratin for renal cell carcinoma is recommended as fat-poor angiomyolipomas can be hard to discern from renal cell carcinomas on imaging.
Tuberous sclerosis complex consensus guidelines are that asymptomatic, rapidly growing renal angiomyolipomas greater than 3 cm in diameter and those greater than 4 cm in diameter should be treated with an mTOR inhibitor. There may be transient or variable proteinuria as a side effect, but this is typically not an indication to discontinue the medication. It is recommended to continue mTORC1 inhibition therapy for as long as the patient tolerates it, and for a minimum of 12 months.
Everolimus was approved for renal angiomyolipomas by the FDA in 2012. A large, double-blind, placebo-controlled multicenter trial (EXIST-2) revealed clear benefit from everolimus in angiomyolipomas and sporadic lymphangioleiomyomatosis (13). The 4-year update of the open-label extension trial was positive as well, with consistent response and safety (14). An open-label long-term extension of the EXIST-1 trial revealed that 73.2% of 41 patients achieved a renal angiomyolipoma response (44). Pediatric patients being treated for SEGAs were analyzed for angiomyolipoma response in the EXIST-1 study. More than 75% of patients had a greater than 50% reduction in sum volume of the angiomyolipomata from baseline, with sustained reductions over nearly 4 years of treatment (11).
Large renal angiomyolipomas can be managed by embolization or nephron-sparing surgery. The success of transarterial therapeutic embolization, even in angiomyolipomas as large as 4cm or greater (40; 65), makes surgery a less preferred option, especially for central lesions. Acute hemorrhage is best managed with embolization followed by corticosteroids.
Routine kidney biopsy is not recommend in all fat-poor lesions in children and adults with tuberous sclerosis complex. It is recommended to obtain biopsy samples of fat-poor kidney lesions only if their growth rate is above 5 mm/year and/or if they do not respond to mTORC1 inhibition (81). Patients with renal or pulmonary failure require meticulous medical care and may be candidates for organ transplant. They may also benefit from mTOR inhibitors to prevent bleeding and progression of disease. Nephrectomy should be avoided in patients.
Surveillance and management of pulmonary complications. Importantly, it is recommended that women with tuberous sclerosis complex, and symptomatic men, have a non-contrast chest CT once at 18 years of age, then every 5 to 7 years through menopause if asymptomatic in the absence of lung cysts in the baseline CT examination at age 18, and at any time if inexplicable or persistent respiratory symptoms occur (70). If there are lung cysts consistent with lymphangioleiomyomatosis on the baseline CT examination, scan intervals are determined on a case-by-case basis. Ultra-low-dose CT acquisition protocols are recommended to limit radiation exposure. High-resolution CT can be useful to differentiate other associated issues, such as effusions or atelectasis, but is not needed to diagnose typical cysts in lymphangioleiomyomatosis.
Baseline pulmonary function test is indicated in women at age 18. Baseline and annual pulmonary function tests and a baseline 6-minute walk test are also indicated in patients with lymphangioleiomyomatosis and lung cysts.
A serum vascular endothelial growth factor type D (VEGF-D) level may be helpful to establish a baseline for future lymphangioleiomyomatosis development or progression. This cannot be recommended routinely yet, as it has not been prospectively evaluated as a screening tool.
All adult patients should be questioned about smoking, occupational exposures, connective tissue disease symptoms, chyle leak, cough, and spontaneous pneumothorax in follow-up visits. Counseling on smoking risks and estrogen use in oral contraceptive preparations, which can compound the impact of lymphangioleiomyomatosis, should also occur. Talc pleurodesis and pleurectomy are avoided in patients who are candidates for lung transplantation in the future. Doxycycline should be avoided in the treatment of lymphangioleiomyomatosis. Patients should be vaccinated for influenza and pneumococcus (45).
More frequent spirometry (every 3 to 6 months) should be considered in patients with a new lymphangioleiomyomatosis diagnosis to establish a trajectory of disease progression, patients with progressive symptoms, patients with advanced disease and limited pulmonary reserves, and to monitor treatment response in patients taking mTOR inhibitors. Postbronchodilator spirometry is preferred for all patients to limit variability due to reversible airflow obstruction. In patients who are unable to perform pulmonary function tests because of cognitive impairment or other reasons, serial CT imaging may be the best method to assess progression.
Sirolimus is recommended as the first-line treatment for qualifying patients with lymphangioleiomyomatosis (80). Everolimus has been proven to be effective in a large trial for sporadic lymphangioleiomyomatosis (13). If patients are already on everolimus for other indications, treatment is continued with everolimus and serial pulmonary function test monitoring, instead of transitioning to sirolimus.
Lymphangioleiomyomatosis-associated chylous pleural effusions have been shown to decrease or even resolve with sirolimus therapy. Also, pulmonary function seems to stabilize or improve with sirolimus treatment of lymphangioleiomyomatosis, and this response seems to be durable for at least 2 years (114). The U.S. Food and Drug Administration approved mTOR inhibitors for lung issues in patients with tuberous sclerosis complex in 2015. Pregnancy in the presence of lymphangioleiomyomatosis has been associated with an increased rate of decline in lung function and increased risk of pneumothorax. Lung transplant should be considered in end stage lymphangioleiomyomatosis. Talc pleurodesis is not a contraindication for transplant.
Surveillance and management of cardiac complications. All patients younger than 3 years of age should have a 12-lead EKG and an echocardiogram to evaluate for arrhythmias and rhabdomyomas, respectively. In newly diagnosed adults, a baseline EKG alone is recommended. In patients with asymptomatic rhabdomyomas, a follow-up echocardiogram should be performed every 1 to 3 years until regression of the rhabdomyomas is documented. An ECG is recommended at minimum every 3 to 5 years to monitor for conduction defects. Screening abdominal sonography and chest radiography should be performed every 2 to 3 years before puberty and every year after puberty for vascular aneurysms (55).
Cardiac symptoms including congestive cardiac failure and arrhythmias may require symptomatic treatment, including medications, ablative procedures, pacemakers, resective surgery for obstructive tumors and, rarely, heart transplant (32). The ORACLE trial was planned to be the first randomized clinical trial assessing the efficacy of everolimus as a specific therapy for symptomatic cardiac rhabdomyoma (113). No updates are available on this trial.
Surveillance and management of ophthalmological complications. A baseline dilated funduscopic exam is recommended to screen for retinal astrocytic hamartomas and retinal achromic patches. Annual eye examination is advised in asymptomatic patients. In patients with symptomatic retinal hamartomas with persistent and recurrent vitreous hemorrhage, pars plana vitrectomy is a therapeutic strategy (82). Other interventions include laser, photodynamic therapy, intravitreal anti-VEGF, intravitreal steroids, and surgery. Surveillance of lesion growth by periodic imaging has been advised, although no conclusive guidelines exist yet.
Surveillance and management of dermatological manifestations. An annual skin survey is recommended to assess for symptomatic or rapidly changing lesions in children. Frequency in adults depends on severity of dermatological manifestations. Digital photographic records are irreplaceable in serial monitoring. A Wood lamp is helpful in detecting hypomelanotic macules. Sun protection is recommended due to photosensitivity of hypomelanotic macules.
The TREATMENT trial randomized patients to 1% rapamycin, 0.1% rapamycin, and vehicle alone in ages 3 through 61 years. There was clinical response to both doses of rapamycin on the angiofibroma grading scale. Highest benefit was within 6 months of initiation of treatment (63). Other studies have evaluated sirolimus as well, and children were noted to respond better than adults, perhaps due to lesser size and fibrosis (74; 133). Patients with tuberous sclerosis complex being treated with oral everolimus for SEGAs and renal angiomyolipomas had a significant decrease in size (p < 0.001), density (p< 0.001), percent involvement (p< 0.001) of angiofibromas, and erythema (p< 0.001) on the forehead, nose, cheeks, and chin (135). The risk–benefit ratio, however, is inadequate to recommend the use of mTOR inhibitors systemically for skin lesions alone. Topical sirolimus is available at 0.1% to 1% concentrations and can be used once or twice daily for skin lesions. Sun protection is indicated while using topical sirolimus. Various surgical methods of management are also available.
Surveillance and management of dental manifestations. Establishment of dental care is recommended at the time of eruption of the first tooth and no later than 12 months of age. Dental assessments are advised every 3 to 6 months, and panoramic x-rays should be performed by 7 years of age, if not performed previously. Dental pits can be managed by preventative measures. such as fluoride and sealants.
Surveillance and management of endocrine manifestations. Pancreatic tumors are treatable and can be easily recognized through annual abdominal MRIs, with fine pancreatic cuts. They were a preventable cause of death in a mortality study (02). Functional pancreatic neuroendocrine tumors require standard of care evaluation and management similar to those without tuberous sclerosis complex.
mTOR inhibitors. Since 2010, sirolimus and everolimus have been approved in various countries for various indications in tuberous sclerosis complex. Everolimus is the only orally available mTOR inhibitor, which is typically titrated up from a dose of 4.5 mg/m2 body surface area to achieve a drug level in the range of 5 to 15 ng/ml. Rapamycin or sirolimus is available for parenteral and topical use. When initiating therapy with an mTOR inhibitor, baseline laboratory studies should include a fasting lipid panel, comprehensive metabolic panel, cystatin C quantification, urine analysis, and complete blood count with differential. These panels should be repeated shortly after treatment is started in addition to measurements of mTOR inhibitor trough level and levels of concomitant medications, particularly if they are strong enzyme inhibitors or inducers. Practical information for the management of side effects of mTOR inhibitors is available in the literature (31). A Cochrane review on rapalogs has been published (108).
The most common side effects of mTOR inhibitors are stomatitis and upper respiratory tract infections. Other side effects include rash, gastrointestinal symptoms, increased total cholesterol, decreased fibrinogen levels, decreased white blood cell counts, anorexia, and urinary tract infections. Increased creatinine, glucose, and triglycerides have been noted. Death and pneumonia were recorded as adverse effects of everolimus, attributed to decreased immune function. Stomatitis can be worsened by alcohol and peroxide-containing wipes.
mTOR inhibitor levels may increase when taking CYP3A4 inhibitors, such as clarithromycin, erythromycin, ketoconazole, verapamil, and grapefruit. Higher doses may be needed while using CYP3A4 inducers, such as phenobarbital, phenytoin, St. John’s wort, and glucocorticoids. mTOR inhibitor dose may need to be decreased with PGP inhibitors, such as amiodarone, quinidine, and erythromycin (125). Cannabidiol is reported to increase mTOR inhibitor levels. mTOR inhibitor dose needs to be decreased in the presence of moderate hepatic impairment. Live vaccines and contact with those who have received live vaccines need to be avoided.
Due to the potential of impaired healing and immunosuppressive properties, standard practice is to temporarily halt mTOR inhibitor therapy 1 to 2 weeks before planned surgeries or live vaccine immunizations or during any prolonged or new-onset significant infections or other adverse effects and then resume treatment after recovery (typically 1 to 2 weeks after vaccination and 2 to 4 weeks after surgery).
Death is most likely due to renal causes. Epilepsy and SUDEP (sudden unexpected death in epilepsy) are important causes of death as well. Pulmonary lesions are causes as well. Renal cysts may be associated with renal failure, and renal angiomyolipoma may cause occasional massive intra-abdominal bleeding.
Seizures are harder to control, with more than two thirds of patients having intractable epilepsy in comparison to the general population. Seizures persist in about 40% of surgically treated patients (21). Unfavorable prognostic factors for epilepsy include onset in infancy, presence of several seizure types, multifocal electroencephalogram (EEG) discharges when awake that generalize in sleep or secondary bilateral synchrony, and occurrence of new EEG foci during evolution of the disease (27).
Prognostic markers of intellectual disability include cortical tubers in the frontal and temporal regions (102), cerebellar tubers, TSC2 mutations, and refractory seizures. Infantile spasms and early age of epilepsy onset also correlate with poor cognition. A longitudinal observational study conducted by the TACERN (Tuberous Sclerosis Complex Autism Center of Excellence Research Network) study group supports some of these historical observations (22).
Obstructive hydrocephalus caused by a subependymal giant cell astrocytoma was an important cause of death before contemporary neuroimaging and neurosurgical techniques. Bleeding within a subependymal giant cell astrocytoma is a rare complication that may be fatal.
Complications during pregnancy relate chiefly to renal disease and the risk of rupture of renal angiomyolipoma vessels (98; 61). There is a greater risk of pneumothorax and chylous effusion during pregnancy. Renal failure, preeclampsia, and severe intrauterine growth retardation may also occur. Renal ultrasonography or CT is recommended in pregnant patients to evaluate renal function.
Prenatal testing for a pregnancy at increased risk and preimplantation genetic testing are possible if a pathogenic variant has been identified in an affected family member.
Antiseizure medications have teratogenic effects and need to be monitored appropriately. Everolimus may be teratogenic. Women of childbearing potential should be advised to use an effective contraceptive during and for 8 weeks after treatment. Estrogen in oral contraceptives is to be avoided.
Careful prenatal ultrasound survey is indicated to look for cardiac rhabdomyomas and rare brain anomalies as clinical features of tuberous sclerosis complex, most evident in the third trimester. Fetal brain MRI needs to be planned for, if necessary. Maternal sirolimus to achieve a target trough level of 10 to 12 ng/mL has been suggested to manage rhabdomyomas prenatally (39). Postnatally, cardiac ultrasound, ECG, and MRI brain are indicated, along with establishment of care with a pediatric neurologist (120).
Avoid:
|
• Estrogen use in teenage and adult females | |
|
• Smoking at all ages | |
|
• Nephrectomy |
Special precautions for general anesthesia are related to CNS involvement by tumors (subependymal giant cell astrocytomas) causing intracranial hypertension or status epilepticus, to the kidneys causing renal failure, to the lungs causing respiratory failure, to the great vessels with aneurysm that may rupture, or to the heart with cardiac arrhythmia.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.

Hema R Murali MD MBBS
Dr. Murali of Marshfield Clinic has no relevant financial relationships to disclose.
See ProfileNarayana S Murali MD
Dr. Murali of the Marshfield Clinic and Geisinger Health System has no relevant financial relationships to disclose.
See Profile
Bernard L Maria MD
Dr. Maria of Thomas Jefferson University has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Epilepsy & Seizures
Jan. 20, 2025
Sleep Disorders
Jan. 18, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuromuscular Disorders
Dec. 29, 2024