











Neuro-Oncology
Choroid plexus tumors of childhood
Jan. 14, 2025
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
Skull base tumors are diverse in their origin, histology, treatment, and prognosis. Patients may present with a variety of neurologic symptoms caused by compression of neurologic or vascular structures. Differential diagnosis for skull base pathology is broad. Patient care is highly individual and multidisciplinary. These characteristics make treating skull base pathology both challenging and rewarding. Ongoing research involving targeted therapies and evidence-based advances predicated on clinical trials add to treatment approaches.
|
• Masses involving the skull base have a broad differential diagnosis, each entity characterized by unique biology and cellular origins. | |
|
• Standard radiographic evaluation involves the use of magnetic resonance imaging (MRI) and computed tomography (CT). Each skull base location has a relatively defined differential diagnosis in terms of neoplasms, varying depending on the anatomic site. | |
|
• Care for patients with skull base masses is highly individual and multidisciplinary. Tumor histology, size, location, and patient demographics strongly influence overall prognosis for each skull base tumor type and determine treatment approach. | |
|
• Treatment aims for tumor control and, at the same time, preservation of neurologic functions. | |
|
• Genetic characterization and targeted molecular therapies are emerging as primary or adjunct treatment options for some skull base tumors. |
Skull base tumors are located in the vicinity of the brainstem or beneath the cerebral cortex, making their treatment technically challenging. Skull (cranial) base surgery has been driven by pioneers in neurosurgery and otolaryngology. Sir Charles Balance and Harvey Cushing both had a special interest in vestibular schwannomas. Interdisciplinary cooperation for treatment of skull base tumors started at the University of Mainz many years ago (33), and consists of neurosurgery, otolaryngology, plastic surgery, ophthalmology, radiation oncology, and neuroradiology. This clinical focus has been represented by formal journals (eg, Skull Base Surgery created in 1990 and is available as part of the Journal of Neurological Surgery Part B – Skull Base as of 2012), and skull base societies.
Until recently, many deep seated, skull base tumors were either entirely inoperable or could be exposed by damaging normal brain structures. This could result in brain injury affecting movement, feeling, speech, mental abilities, and other adverse neurologic consequences. Basic concepts that underlie cranial base surgery is removal of bone and cerebrospinal fluid (CSF) drainage, often in a clever and anatomically complex manner, to reduce or even eliminate the need for brain retraction. Skull base procedures, for example, may be designed to traverse the bone containing the ear (petrous bone), around the eye (orbit), through the nose or paranasal sinuses, low on the temple beneath the brain, or even upwardly directly from the neck region. Fundamentally, these techniques afford the highest possible degree of tumor removal while preserving neurologic function to the greatest extent possible. Adjuvant treatments and advances in radiation therapy and targeted therapies have allowed skull base surgeons to enable more safe and effective treatments.
Clinical manifestations of cranial base tumors are variable and largely dependent on the anatomic location, size, and extent of edema. Typical presentations include cranial neuropathies (eg, hearing loss, double vision, facial pain, vision loss, swallowing difficulty, etc.), pituitary/hypothalamus dysfunction, seizures, brain or brainstem compression (eg, personality changes, weakness, coordination problems), and headache.
Prognosis is primarily dependent on the histology and location of the tumor. Malignant skull base tumors have a much more aggressive course with decreased survival compared to benign entities; however, histologically “benign” skull base tumors can have significant morbidity due to involvement of critical anatomic structures. All CNS tumors are defined and graded using the WHO classification.
Complications of skull base surgery and radiation relate directly to the critical structures involved by the masses. Various studies investigating overall complications in intracranial tumor surgery document overall complications incidence ranging from 9% to 40%, with overall mortality incidences of 1.5% to 16% (41). Generic complications may include neurologic deficit, seizure, hematoma, wound infection/meningitis, venous thromboembolism, or other medical complications. A common and specific complication of skull base surgery is cerebrospinal fluid (CSF) leak. Rates for this complication have been cited as high as 20% for some approaches (10).
A better understanding of tumor genetics has contributed to more accurate prognostication and defining tumor subtypes. The pattern of DNA methylation and burden of chromosomal losses and gains has been associated with increased recurrence risk in meningioma (32). Specific alterations in genes and methylation marks have also been associated with meningioma outcome. Mutations in the TERT promoter are associated with higher grade and tumor progression, increased high-risk of recurrence, and short intervals to progression (37). Deletion of CDKN2A/B is strongly associated with elevated risk of recurrence and a decreased time to progression (36), whereas deletions in the DMD gene on chromosome X may also identify a subset of progressive/higher grade meningiomas with shorter overall survival (16). Inactivation of BAP1 or PBRM1 is enriched in aggressive rhabdoid and papillary meningiomas (40). Loss of H3K27me3 by IHC is observed in a fraction of atypical and anaplastic meningioma and associated with poor outcome (13).
|
Tumor |
Approximate prognosis |
|
Meningioma |
86% 5-year survival (11) |
|
Chordoma |
74% 5-year survival (22) |
|
Nasopharyngeal carcinoma |
20% to 40% 5-year survival (American Cancer Society; 7th edition of the AJCC Cancer Staging Manual) |
|
Chondrosarcoma |
89% 5-year survival (03) |
|
Pituitary adenoma |
91% 5-year survival (07) |
|
Esthesioneuroblastoma |
76% 5-year survival (06) |
|
Paraganglioma |
93% 10-year survival, not measured for asymptomatic tumors; for those with nodal disease 50% to 80%; for those with distant mets 11% 5-year survival (14) |
|
Craniopharyngioma |
80% 5-year survival (05) |
|
Hemangiopericytoma |
82% 5-year survival (31) |
|
Schwannoma |
98% 5-year survival |
A 23-year old female presented at the emergency ward with progressive headache, nausea, and gait disturbance. Neurologic examination demonstrated a first-degree nystagmus to the right, right sided ataxia, and long neural tract deficits. CT and MRI of the brain revealed a very large extra-axial mass in the right lateral skull base with significant compression on the cerebellum and fourth ventricle with a subsequent triventricular hydrocephalus. Full-body CT demonstrated no other tumor lesions or metastases. A transmeatal biopsy demonstrated a giant cell tumor of the bone for which neoadjuvant denosumab was started. She completely recovered from her symptoms, and after five rounds of treatment there was a significant reduction of tumor mass, which made surgical resection possible. Postoperative imaging demonstrated a near total resection with residual tumor at the level of the clivus. This tumor residue was progressive at six months follow-up and denosumab was re-administered. Giant cell tumors were rare neoplasms with even lower incidences at the skull base. Primary treatment was complete surgical resection. Denosumab was a monoclonal antibody that activates the receptor activator of nuclear factor kappa-B ligand (RANKL), and it was an alternative treatment when surgical resection was not feasible. In 2013, denosumab became FDA approved in treatment for adults with giant cell tumors.
The etiologies of tumors of the skull base vary by tumor type. Etiologies of the most common skull base tumors are presented in Table 2.
|
Tumor |
Etiology |
|
Meningioma |
Most arise from arachnoid cap cells, but may arise from dural fibroblasts or arachnoid associated with cranial nerve or the choroid plexus. |
|
Chordoma |
Arise from notochord remnants, most commonly in the clivus and sacrum or coccyx. |
|
Nasopharyngeal carcinoma |
Arise from squamous epithelium of the nasopharynx. |
|
Chondrosarcoma |
Arise from transformed chondrocytes; most common intracranially at the petroclival synchondrosis. |
|
Pituitary adenoma |
Arise from pituitary cells of the anterior pituitary; may be hormone secreting or non-functional. |
|
Esthesioneuroblastoma |
Arise from bipolar sensory receptors in the olfactory mucosa. |
|
Glomus jugulare |
Arise from the paraganglia in chromaffin-negative glomus cells, which are neural crest in origin. |
|
Craniopharyngioma |
Arise from squamous epithelial rests from the involuted craniopharyngeal duct. |
|
Epidermoid cyst |
Arise from inclusion of epithelial elements at the time of neural tube closure or from the traumatic introduction of epithelial elements. |
|
Arachnoid cyst |
Arise from normal arachnoid cells. |
|
Hemangiopericytoma |
Arise from pericytes surrounding capillaries. |
|
Germinoma |
Arise from primordial germ cells that fail to migrate in an appropriate fashion. |
|
Plasmacytoma |
Arise from transformed plasma cells. |
|
Schwannoma |
Arise from Schwann cells along cranial nerves. |
|
Giant cell tumors |
Origin remains unclear. Many authors believe that it rises from undifferentiated cells in supporting cells of the bone. |
Meningioma. Meningiomas are comprised of whorls or sheets of cells. Frequently, small amounts of calcification (psammoma bodies) are also present.
Chordoma. Chordomas are composed of fluffy vacuolated physaliferous cells that are mucinous.
Nasopharyngeal carcinoma. Carcinomas are typified by sheets of densely packed epithelioid cells.
Chondrosarcoma. Chondrosarcomas are typified by cords of cells with mucin. They are differentiated from chordomas by immunohistochemical staining.
Pituitary adenoma. Pituitary adenomas show expansion of monomorphic cells in an acinar pattern reminiscent of normal pituitary gland. Adenomas can be categorized by the pituitary hormone that is overproduced, and they can be classified into eosinophilic (over-secrete prolactin or GH), basophilic (over-secrete ACTH, LH, FSH, or TSH), or chromophobic (nonsecretory) on H&E staining. Differentiation of the hormone produced is currently carried out by immunohistochemistry.
Esthesioneuroblastoma. Esthesioneuroblastomas are typified by lobular islands of small round to oval blue cells originating in the olfactory epithelium.
Paraganglioma. Paragangliomas are composed of trabeculae or balls of cells with an abundant vascular pattern.
Craniopharyngioma. Craniopharyngiomas are notable for complex epithelial structures with keratin collections and calcifications.
Epidermoid cyst. Epidermoid cysts are notable for a stratified squamous epithelial membrane enclosing laminated keratin.
Arachnoid cyst. Cyst walls of arachnoid cysts are made of meningothelial cells on a fibrovascular stroma.
Hemangiopericytoma. Hemangiopericytomas are vascular tumors made of spindled to round cells.
Germinoma. Germinomas are large tumor cells with abundant cytoplasm often infiltrated with reactive inflammatory cells.
Schwannoma. Schwannomas often have hypercellular palisading areas with other areas of myxoid hypocellular spaces (Verocay bodies).
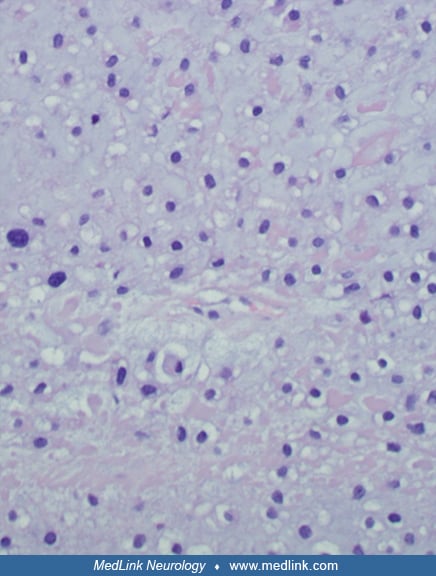
Giant cell tumors. A conventional giant cell tumor of the bone (GCTB) is a hypercellular lesion consisting of nonneoplastic multinucleated osteoclast-like giant cells, stromal neoplastic mononuclear cells (typically oval shaped), and macrophages. A conventional GCTB can undergo malignant transformation, after which highly pleomorphic mononuclear cells are found.
The characteristics of skull base tumors are listed in table 3.
|
Meningioma | |
|
• Frequency: 8% of all intracranial tumors | |
|
Chordoma | |
|
• Frequency: 1% of all intracranial tumors | |
|
Nasopharyngeal carcinoma | |
|
• Frequency: 25% involve the skull base | |
|
Chondrosarcoma | |
|
• Frequency: 6% of all skull base tumors, 0.15% of all intracranial tumors | |
|
Pituitary adenoma | |
|
• Frequency: 10% of all primary intracranial neoplasms | |
|
Esthesioneuroblastoma | |
|
• Frequency: 3% of all nasal tumors | |
|
Paraganglioma (glomus jugulare, glomus tympanicum, etc.) | |
|
• Frequency: 1% of all primary intracranial neoplasms | |
|
Craniopharyngioma | |
|
• Frequency: 3% to 5% of all primary intracranial tumors | |
|
Epidermoid cyst | |
|
• Frequency: 0.2% to 1% of all primary intracranial tumors | |
|
Arachnoid cyst | |
|
• Frequency: 1% of all intracranial masses | |
|
Solitary fibrous tumor | |
|
• Frequency: 1% of all intracranial masses | |
|
Germinoma | |
|
• Frequency: 5% of all intracranial tumors in patients younger than 20 years | |
|
Schwannoma | |
|
• Frequency: 56% to 58% of all primary intracranial tumors | |
|
Giant Cell Tumor | |
|
I. Planum sphenoidale, tuberculum sella, olfactory groove, and cribriform plate | |
|
• Meningioma | |
|
II. Sella or suprasellar | |
|
• Pituitary adenoma | |
|
III. Parasellar or cavernous sinus | |
|
• Meningioma | |
|
IV. Sphenoid body and sinus | |
|
• Mucocele | |
|
V. Clivus, foramen magnum, jugular foramen | |
|
• Chordoma | |
|
VI. Petrous apex | |
|
• Schwannoma | |
|
VII. External ear canal | |
|
• Carcinomas | |
|
VIII. Cerebellopontine angle | |
|
• Vestibular schwannoma | |
Computed tomography (CT). Thin cut CT scanning is the imaging modality of choice for definition of bony anatomy of the skull base. Multiplanar imaging, including axial, sagittal, and coronal reformats, can be especially useful in defining the anatomy of the sella, cavernous sinus, and cribriform plate. The use of intravenous contrast media aids in defining soft tissue masses and in generating a differential diagnosis. CT scans also are helpful in surgical planning. CT angiography can be useful for defining the relationship between skull base anatomy and normal arteries for aneurysms requiring a skull base surgery approach.
Magnetic resonance imaging (MRI). Gadolinium enhanced MRI is currently the modality of choice for demonstrating soft-tissue anatomy. MR imaging may also show important changes such as pial invasion and normal brain or brainstem invasion by the tumor, as well as the likely consistency and vascularity of the tumor. MR angiography and MR venography can be performed without the need for intravenous contrast. These techniques can be used to provide detailed images of intracranial arteries and veins. This can be useful for defining the relationship between skull base masses and surrounding arteries and veins and ruling out lesions, such as aneurysms, which are vascular in origin. Advances in MRI and data science technology have allowed radiomics to uncover radiographic prognostic biomarkers in skull base tumors such as chordoma (39).
Cerebral angiography. The role of formal angiography is generally reserved for adjuvant preoperative embolization for highly vascular tumors such as meningioma and paraganglioma, and for test occlusion of vessels that may need to be sacrificed with tumor resection, which are generally the internal carotid or vertebral artery.
Radiographic features.
Meningioma.
CT. Seventy percent to 75% of meningiomas are homogenously hyperdense whereas 25% are isodense to brain on nonenhanced CT. Meningiomas are usually well-circumscribed, and 20% to 25% show calcification, which may be diffuse or focal. Hyperostosis is common. Contrast-enhanced CT shows uniform enhancement in 90% of cases.
MRI. Most meningiomas are iso- or slightly hypointense relative to brain on both T1-weighted sequences. Signal on T2-weighted sequences is variable. Meningiomas show avid, homogenous contrast enhancement. These lesions may or may not have an enhancing dural tail, but the presence is highly suggestive of the diagnosis. MR angiography and perfusion weighted imaging can help identify high vascularity, which could be helpful in preoperative planning.
Hemangiopericytoma/solitary fibrous tumor of the dura.
CT. Hemangiopericytomas often show heterogenous signal on both nonenhanced and contrast-enhanced CT scans. Cystic and necrotic areas are common. Contrast-enhanced CT often shows strong, vivid, heterogeneous enhancement. There may be erosion of adjacent bone.
MRI. Signal intensity is usually isointense to grey matter with brain on T1 and T2-weighted sequences, with heterogenous signal on T2-weighted sequences. Hemangiopericytomas show strong, vivid, heterogeneous enhancement on gadolinium-enhanced sequences. Dural tail may also be present, similar to meningiomas. MR angiography shows highly vascular structure, which may be helpful for preoperative embolization planning if the blood supply cannot be targeted at the beginning of the surgical resection.
Chordoma.
CT. Chordomas are frequently well-circumscribed, lytic masses in the clivus on nonenhanced CT, often with mixed solid and cystic components. Enhancement is generally heterogeneous but can be strong.
MRI. Chordomas show heterogeneous hypointensity on T1-weighted sequences and are hyperintense (signal similar to CSF) on T2-weighted sequences. Enhancement is variable and frequently heterogeneous and may have a honeycomb appearance.
Chondrosarcoma.
CT. Nonenhanced CT often shows a hyperdense lesion, most commonly in the area of the petroclival synchondrosis, often with areas of calcification. Contrast-enhanced CT most often shows strong, heterogeneous enhancement.
MRI. Chondrosarcomas are hypo- to isointense on T1-weighted sequences and hyperintense on T2-weighted sequences. They show strong, but often heterogeneous, enhancement on gadolinium-enhanced sequences.
Esthesioneuroblastoma.
CT. Nonenhanced CT shows a high nasal vault mass with focal bone destruction and variable signal. Contrast-enhanced CT shows moderate to strong contrast enhancement.
MRI. Signal intensity is variable on both T1- and T2-weighted sequences. Gadolinium-enhanced sequences show moderate, heterogeneous enhancement.
Paraganglioma (glomus tumors).
CT. CT is primarily useful for delineating the extent of bony destruction surrounding the mass and involvement of skull base foramen. Contrast-enhanced CT shows strong enhancement.
MRI. Paragangliomas are hyperintense on T2-weighted sequences and hypointense on T1-weighted sequences. These masses have a speckled, salt-and-pepper appearance secondary to numerous internal flow voids. Gadolinium-enhanced sequences show strong enhancement. Perfusion weighted imaging is positive showing hypervascularity.
Nasopharyngeal carcinoma.
CT. Nasopharyngeal carcinoma appears as a soft tissue mass most commonly centered at the lateral nasopharyngeal recess. There is often surrounding bony erosion. Contrast-enhanced CT demonstrates heterogeneous contrast enhancement.
MRI. On T1-weighted sequences, signal intensity is usually isointense to muscle. On T2-weighted sequences, signal is usually iso- to slightly hyperintense to muscle. Gadolinium-enhanced sequences show strong, heterogeneous enhancement.
Craniopharyngioma.
CT. These masses appear as cystic, lobulated, primarily suprasellar masses with a solid mural nodule. They often demonstrate nodular or rim calcification. The contents of the cyst are usually slightly hyperdense to CSF. Contrast-enhanced CT usually shows nodular or rim enhancement.
MRI. Signal characteristics are highly variable but generally heterogeneous. Cystic components appear as hyper- or iso- intense to brain on T1 and hyperintense on T2. Solid components show strong enhancement with gadolinium. The most common pattern is hypointense signal on T1-weighted sequences and hyperintense on T2-weighted sequences. The gadolinium-enhanced sequences often show strong, heterogeneous enhancement.
Germinoma.
CT. Germinomas appear as hyperdense masses on nonenhanced CT due to high cellularity. Contrast-enhanced CT shows strong enhancement.
MRI. These masses are usually isointense on both T1- and T2-weighted sequences but occasionally are hyperintense on T1 and hypointense on T2. Occasionally, there may be cyst formation or areas of hemorrhage. Gadolinium-enhanced sequences show strong, homogeneous contrast enhancement.
Plasmacytoma.
CT. Plasmacytomas appear as focal destructive sphenoid sinus or cranial vault masses.
MRI. Imaging characteristics on MRI are variable and nonspecific.
Vestibular schwannoma.
CT. Vestibular schwannomas appear as a mass in the internal acoustic canal or cerebellopontine angle and are iso- or slightly hypodense to adjacent brain on nonenhanced CT. They show strong contrast enhancement on contrast-enhanced CT but can have areas of cystic degeneration with areas of poor contrast enhancement.
MRI. These masses appear as cerebellopontine angle masses that are slightly hypointense or less commonly isointense to brain on T1-weighted sequences. They are hyperintense to brain on T2-weighted sequences. Gadolinium-enhanced sequences show avid and generally homogenous contrast enhancement. These tumors may show enlargement and involvement of the internal auditory canal.
Epidermoid cyst.
CT. CT shows well defined lobulated masses with attenuation similar to CSF. Calcification is present in 10% to 25% of cases. Contrast-enhanced CT sequences show a lack of contrast enhancement.
MR. Most epidermoid cysts show signal intensity similar to CSF on both T1- and T2-weighted sequences. Gadolinium-enhanced sequences show a lack of contrast enhancement. Diffusion-weighted imaging shows restriction of diffusion in epidermoid cysts and no diffusion restriction in arachnoid cysts.
Arachnoid cyst.
CT. Arachnoid cysts appear as well-demarcated extra-axial masses with signal similar to CSF. Smooth erosion of adjacent bone is sometimes seen. Contrast-enhanced CT does not show contrast enhancement.
MR. Signal is similar to CSF on both T1- and T2-weighted sequences. The mass is well-demarcated and extra-axial. There is no contrast enhancement on gadolinium-enhanced sequences. Diffusion-weighted sequences do not show restricted diffusion.
Management of skull base tumors is largely dependent on the location and the histology of the tumor. Management of the most benign entities may involve watchful waiting, but for lesions requiring intervention, surgical resection, and radiotherapy play important roles in the treatment of skull base tumors.
One of the hallmarks of surgical advancement has been the development of techniques to increase bony exposure in order to minimize brain retraction and improve outcomes (34; 01; 35; 17; 04; 27). A subset of skull base masses can be approached using transnasal endoscopic approaches that allow more direct exposure while eliminating external incisions and minimizing brain retraction. Common management strategies include surgical resection with or without preoperative embolization with possible postoperative radiation stereotactic or conventional radiation therapy and/or chemotherapy depending on the pathology. Stereotactic radiosurgery also is an option for some lesions, particularly those with high operative morbidity. For example, aggressive surgical resection of cavernous sinus masses has been replaced with stereotactic radiosurgery (12; 21).
One of the major considerations in determining the appropriate operative approach is the preoperative function of the patient’s cranial nerves and other neurologic function and the expected postoperative function. Any potential loss of cranial nerve function must be weighed against any survival advantage that is afforded through operative resection. The aggressiveness of resection may also be in part determined by the relationship of the mass to important vascular structures. If dynamic information regarding the capacity of sacrificing a crucial blood vessel is being considered, formal cerebral angiography with balloon test occlusion may be warranted.
Operative tools that have improved skull base surgery include use of endoscopy, intra-operative image-guidance with preoperative MRI and/or CT, ultrasonic surgical aspirator, and cranial nerve and long neural tract monitoring. The endoscope can be used as the primary tool for visualization or as an adjunct to an open surgical approach. Image guidance may allow for precise tumor exposure. The ultrasonic surgical aspirator allows for tumor debulking and more rapid tumor excision.
Advances in 3-dimensional printing has been helpful in many patient care applications ranging from preoperative surgical planning to surgical education to the development of novel prostheses for skull base reconstructions (25; 23). Virtual reality and augmented reality simulators and intraoperative adjuncts are being developed in order to provide more comprehensive intraoperative anatomic information (19; 28). These technologies are also invaluable for surgical education.
Intraoperative electrophysiological monitoring (IOM) is an indispensable tool to protect normal nerve structures to resect skull base tumors. Intraoperative electrophysiological monitoring allows identification of crucial neural structures intraoperatively and alerts the surgeon when critical structures are being manipulated, allowing surgeons to reduce injuries to cranial nerves and critical neural tracts. For example, in hearing preservation operations for vestibular schwannomas, cranial nerve VII are monitored through EMG, and VIII are often monitored through brainstem auditory-evoked responses (BAERs). This monitoring improves function of these nerves after surgery, as they are difficult to distinguish from the tumor. As neurophysiologic monitoring continues to improve, it is likely that outcomes, particularly with regard to cranial nerve function, will continue to improve (29). Cranial nerves III, IV, and VI can be monitored when tumors in the parasellar, tentorial, or orbital apex region are approached, as there's high likelihood of manipulating these nerves. Lower cranial nerves can be monitored through their innervated structures (eg, XI - trapezius and sternocleidomastoid). Long neural tracts can be monitored with somatosensory-evoked potentials (SSEPs) and motor-evoked potentials (MEPs). Alteration of these potentials suggests that injury may have occurred or may be occurring and demands the surgeon's attention to assess whether damage has occurred and if the operative strategy must be changed.
Radiation therapy for skull base tumors in conjunction with surgery and chemotherapy or as an independent treatment modality has grown greatly over the past decade. It may be used as a primary or adjuvant treatment. The majority of radiation therapy for brain tumors deliver LINAC generated photon radiation particles, with few institutions also offering proton-based radiation. Photon-based treatment of brain tumors can be delivered via conventional radiation therapy (including external beam radiation therapy – EBRT), intensity modulated radiation therapy (IMRT), or stereotactic radiosurgery (SRS). 2D x-ray films provide positioning of radiation beams, and when used with image guidance (stereotactic CT scan merged with MRI) the radiation beams are conformed to the tumor shape. Similarly, radiation dosage to normal and radiosensitive structures can be monitored and reduced.
IMRT allows for a radiation shape that better matches the tumor volume, maximizing tumor dose while minimizing the radiation exposure of normal tissues. The “intensity modulation” changes the intensity of the beam while targeting multiple small margins in combination. This allows for more effective radiation doses with less treatment toxicity and, therefore, fewer side effects. Stereotactic radiosurgery uses stereotactic CT and MRI imaging to precisely outline the tumor and protect normal anatomic structures. Stereotactic radiosurgery delivers high-dose radiation through converging beams of radiation to minimizing radiation to healthy surrounding tissue. Micromovements of the patient during treatment is adjusted through the incorporation of radiographs taken during treatment. The indications, limitations, and target dosage in stereotactic radiosurgery varies depending on tumor location and pathology.
Advances in genetic sequencing has led to an improved understanding of molecular biology in skull base tumors. Discoveries in common gene mutations in meningioma reveal novel potential targets for treatment (30). Many genetic alterations in meningioma correspond with distinct clinical characteristics. For instance, SMO, AKT1, and PIK3CA mutations occur more commonly in meningiomas of the anterior skull base (09; 02). Based on these findings, there are ongoing clinical trials targeting these mutations in patients with meningioma. For instance, the SMO inhibitor, vismodegib, is being investigated in combination with a focal adhesion kinase (FAK) inhibitor, GSK2256098, for patients with neurofibromatosis type 2 (NF2) under a phase II trial sponsored by the Alliance for Clinical Trials in Oncology (NCT02523014). There is also evidence of overexpression of PD-L1 in higher grade meningiomas, providing preclinical support for the investigation of immune checkpoint blockade (38). Molecular targeted therapies are also being studied in rarer skull base tumors such as chordoma and chondrosarcoma. The growth factor receptor inhibitors, imatinib and erlotinib, are under investigation for use in PDGFR-positive and/or EGFR-positive chordoma (26), and pazopanib in metastatic chondrosarcoma (NCT01330966). Axitinib, lapatinib, and bevacizumab are being studied in neurofibromatosis type 2 patients with vestibular schwannoma (NCT02129647; NCT01767792).
There is a strong correlation between the level of circulating female sex hormones and the growth of meningiomas. Radiation is generally avoided during pregnancy, and frequently, tumors cannot be evaluated with contrast-weighted MRI. Large and symptomatic meningiomas may require surgical resection regardless of the stage of pregnancy. The complexity of each individual case precludes rigorous uniform analysis and concrete treatment guidelines. However, a metaanalysis revealed that surgical resection during pregnancy may be associated with increased maternal and fetal mortality, though outcomes are similar to patients undergoing surgery postpartum (24). Although the mother’s health and well-being are the priority, clinical decision making must occur on a case-by-case basis to optimize outcomes for both the patient and child.
Major anesthetic concerns relative to skull base operations fall into seven major categories: (1) airway, (2) patient positioning, (3) blood loss, (4) neuroprotection, (5) intraoperative monitoring, (6) trigeminocardiac reflex, and (7) immediate postoperative care.
Airway. In most skull base approaches, airway concerns are limited to those associated with any operation. However, several skull base approaches, including the transoral, transmandibular, and transmaxillary approaches, require that the anesthesiologist share the airway with the surgeon and upper airway edema must be considered. Lower cranial nerve dysfunction may make it difficult for a patient to cough and swallow appropriately, and post-operative tracheostomy may be necessary.
Patient positioning. Patient positioning for skull base operations can be complex, and the operations are frequently of significant duration. As for any operation, ensuring that all bony protuberances are well padded and that no joints are placed in abnormal positions is essential to preventing position-related neuropathies and other complications. Intraoperative monitoring of somatosensory evoked potentials may help detect position-related complications and allow them to be addressed. Another consideration is the position of the head relative to the heart. Positions in which the head is above the heart decrease intracranial pressure and venous pressure, allowing for improved hemostasis. However, positions in which the head is above the heart increase the risk of venous air embolism, and in some cases, precordial Doppler monitoring could be considered.
Blood loss. The overall goal in skull base surgery is to maintain euvolemia. Many skull base operations have the risk of significant blood loss given the high vascularity of some tumors as well as the intimate relationship of many skull base tumors with vascular structures, including the venous sinuses and major intracranial arteries. The risk of significant blood loss should be discussed by the anesthesia and surgical teams, and appropriate blood products should be readily available. In addition, appropriate vascular access should be obtained preoperatively. In the case of uncontrolled arterial vascular injury, adenosine allows brief cardiac arrest, which affords the surgeon precious moments to gain vascular control and to address the vascular injury.
Neuroprotection. Often the first neuroprotective measure is achieving brain relaxation during surgical exposure. This may be achieved by release of cerebral spinal fluid (CSF), a temporary mild hyperventilation, head elevation, mannitol or hypertonic saline. CSF diversion can be achieved through an anatomic site (eg, cisterna magna) or a preoperative lumbar drain or ventriculostomy. Brain relaxation allows safe tumor exposure, requiring less brain retraction for exposure.
Intraoperative monitoring. Intraoperative neurophysiologic monitoring is being increasingly utilized, as described above. The ability to monitor these neurophysiologic parameters is highly dependent on the anesthetics being employed. When cranial nerves are being monitored with EMG, the major consideration is the use of paralytics. Although some have reported the ability to monitor the facial nerve with low-dose paralytic infusions, the use of paralytics reduces the ability to detect nerve irritation (08). Thus, at most institutions, paralytics are avoided when cranial nerve EMG is used.
Trigeminocardiac reflex. Surgical manipulation of the trigeminal nerve during skull base surgery of the anterior, middle, and posterior fossa may elicit a trigeminocardiac reflex (TCR). This phenomenon consists of bradycardia and hypotension, and can include asystole if extreme. This reflex has been reported to occur in 8% of cases involving surgery for skull base tumors (20). In all reported cases, hemodynamic instability resolves by simply pausing surgical manipulation and rarely requires pharmacologic intervention (20). Continuous hemodynamic monitoring and communication between the surgical and anesthesia teams are nonetheless essential in order for proper recognition and management of this reflex.
Immediate postoperative care. Most patients are able to be extubated immediately following skull base procedures; however, this timing may vary depending on case duration, airway edema, blood loss, and cranial neuropathy. Postoperative nausea and vomiting must be aggressively prevented and treated, particularly as it leads to elevations in intracranial pressure and systemic blood pressure. Elevations in these parameters place patients at risk of postoperative bleeding in the surgical bed and increased risk of cerebrospinal fluid leak. Evaluation of CSF leak and mitigation of postoperative complications due to cranial neuropathy are essential (15).
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Yasin Temel MD PhD
Dr. Temel of Maastricht University Medical Center has no relevant financial relationships to disclose.
See ProfilePawan Kishore Ravindran MD
Dr. Ravindran of Maastricht University Medical Center has no relevant financial relationships to disclose.
See ProfileMax Keizer MD
Dr. Keizer of Maastricht University has no relevant financial relationships to disclose.
See ProfileRemco Santegoeds MD PhD
Dr. Santegoeds of Maastricht University Medical Center has no relevant financial relationships to disclose.
See Profile
Peter J Koehler MD PhD
Dr. Koehler of Maastricht University has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
Neuro-Oncology
Jan. 14, 2025
General Neurology
Jan. 13, 2025
General Neurology
Jan. 13, 2025
Neuro-Ophthalmology & Neuro-Otology
Jan. 08, 2025