







Stroke & Vascular Disorders
Neoplastic and infectious aneurysms
Dec. 29, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Worddefinition
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas.
The presence of white matter abnormalities in the brain of both symptomatic and asymptomatic individuals has been a source of interest for over a century. CT and MRI detection of these lesions has become more sensitive than even autopsy. Clinical studies have associated these lesions with cognitive decline, gait impairment, and increased cerebrovascular disease and death risk. The etiology of white matter abnormalities varies from cerebrovascular disease to metabolic and demyelinating disorders. This article primarily focuses on cerebrovascular disease.
|
• White matter abnormalities are present in at least 10% of individuals older than 65 years of age. | |
|
• These lesions correlate with an increased risk of cognitive impairment, stroke, and death. | |
|
• There are many causes of white matter abnormalities; not all are fully understood. | |
|
• The most common etiology of white matter abnormalities is CNS small vessel disease. |
In 1894, Binswanger described a male with syphilis who suffered from leg weakness, arm tremors, progressive cognitive decline, including speech and memory, depression, and personality change (13). Brain autopsy revealed white matter atrophy. Subsequently, a similar case was presented, attributing the white matter changes to arteriosclerosis of the long, penetrating vessels (02). It was not until 1962 that Binswanger's case was diagnosed as syphilis, and the term “subcortical arteriosclerotic encephalopathy” was proposed to describe cerebral arteriosclerosis affecting vessels of the white matter and subcortical grey matter (125).
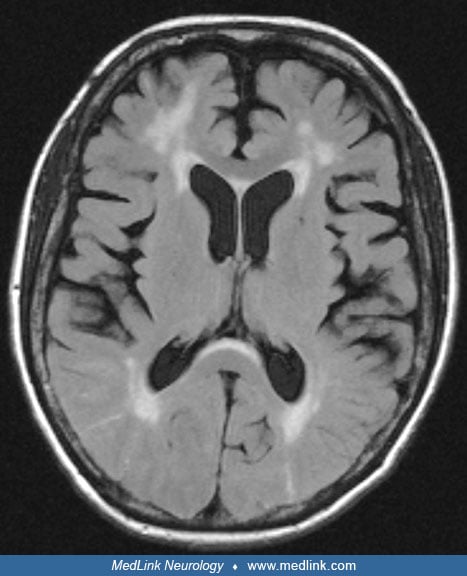
CT brain scan, followed by MRI, revealed cerebral white matter changes in both asymptomatic and cognitively impaired individuals (141; 186; 20; 59). These changes appear as hypodensities on CT and are described as white matter lucencies, leukoencephalopathy, or leukoaraiosis. On T2-weighted MRI, these lesions are hyperintense and are called white matter abnormalities, white matter hyperintensities, cerebral white matter changes, or unidentified bright objects. MRI is more sensitive to these changes than a CT scan (58). Therefore, these white matter changes will be called white matter abnormalities or disease.
|
• The burden of white matter abnormalities increases with age. | |
|
• White matter abnormalities may occur in apparently asymptomatic subjects with subtle neurologic deficits. | |
|
• The severity of white matter abnormalities is associated with dementia, depression, risk of falls, cerebrovascular disease, and premature death. |
As the quality and availability of MRI increased, so did the number of lesions diagnosed in apparently healthy subjects. Most lesions are lacunar infarcts resulting from hypertensive small vessel disease. Although asymptomatic, the patients may have subtle, often unrecognized, deficits in neurologic function. Moreover, these silent infarcts double the risk of stroke and dementia (167). Abnormal three-step motor sequencing and horizontal extraocular tracking tests can predict the presence of periventricular white matter abnormalities (08).
Cognitive dysfunction. In healthy older adults, white matter abnormalities are associated with decreased processing speed, memory deficit, executive function, and global cognitive dysfunction (38; 68; 03). A meta-analysis including 11,486 healthy older participants found an association between white matter hyperintensities and attention, memory, executive function, and global cognition (81).
In a study of pre-clinical Alzheimer disease, there was a strong association between white matter hyperintensities and amyloid-related microhemorrhages seen on brain MRI (146).
Severe periventricular white matter abnormalities were noted in patients with subcortical dementia, Alzheimer disease, and frontotemporal dementia (70; 75; 91). However, similar cognitive decline profiles can be caused by different conditions (165).
Different cognitive patterns are present in patients with various causes of dementia with similar severity. For example, white matter abnormalities within the periventricular area were associated with worse comprehension and attention, whereas those outside the periventricular area were associated with impaired memory and conceptualization performance (87). The severity of white matter abnormalities correlates with the decline in Wechsler Performance IQ scores, block design, object assembly, and digit symbol tests (56).
Not all cognitive decline is explained by white matter abnormalities. Between the ages of 11 and 78 years, the severity of white matter abnormalities was associated with overall cognition, independent of childhood cognitive ability. Hypertension accounted for at least some of the effects of white matter abnormalities in this study (43).
Balance impairment and risk of falls. Brain MRI scans have demonstrated an association between white matter abnormalities, mobility, and self-reported physical impairment (178; 140). An association was found between white matter abnormalities, decreased limb power and mobility, and abnormal plantar, rooting, and palmomental reflexes (151; 71).
Impaired balance leads to a four-fold increase in falls compared to controls (57; 103; 85). ApoE ε4, in addition to white matter abnormalities, has a synergistic effect on imbalance (31).
White matter disease in children. In children younger than 5 years of age, white matter abnormalities on brain MRIs are associated with spasticity (96).
Dementia. In nondisabled elderly subjects, severe white matter abnormalities are associated with medial temporal lobe atrophy and significant cognitive dysfunction (28; 159). In early Alzheimer disease, the burden of white matter abnormalities is not significantly increased (48). Silent infarcts on brain MRI are associated with decreased psychomotor speed and a 126% increased risk of dementia. Accumulation of white matter abnormalities impairs cognition, predicts progression to Alzheimer disease, and is associated with increased mortality (80; 75; 176; 166; 132).
Depression. Elderly patients diagnosed with depression may have more severe white matter abnormalities and cerebral atrophy than controls (09). Temporal lobe white matter abnormalities independently predicted Geriatric Depression Scale scores (123).
Retinopathy and stroke. White matter abnormalities in patients with prior stroke predict an increased risk of subsequent stroke (115; 162). White matter disease is associated with retinal microvascular abnormalities and predicts a significantly higher risk of stroke (20% vs. 1.4%) (179).
Imbalance, impaired gait, and falls. High-functioning elderly patients without stroke or dementia have slower gait, a shorter stride, and require longer support time (139). Patients with Alzheimer disease and white matter abnormalities may also exhibit extrapyramidal signs (150).
Premature death. The risk of death is predicted by advanced white matter abnormalities, even after adjustment for other cerebrovascular risk factors (86).
A 72-year-old male presented with impaired gait. Three years earlier, he was diagnosed with diabetes controlled with oral metformin 500 mg twice daily. For 1 year, his gait had been unstable, as if he was inebriated. He would occasionally catch his toes and fall. Over time, he needed to use the walls for guidance when walking down a hall, and he began to use a cane for mobility assistance. Walking across a dark room was particularly difficult. In addition to gait difficulties, he had become forgetful with daily tasks and sometimes could not recall the names of familiar people.
Past medical, family, and social history were unremarkable. He took no medications. On review of systems, he experienced tingling in both feet, which had become persistent about a year earlier, and he had difficulty sensing temperature if he placed his feet in bathwater.
Examination revealed mild difficulties with verbal memory and moderate to long-term recall of visually identified objects. Language, praxis, and tests of frontal lobe executive functioning were normal. The Mini-mental status examination score was 25/30. He had a mild bilateral palmomental reflex. Fundoscopy revealed arteriovenous nicking. Blood pressure was 150/95 mmHg. The visual fields were full. Visual acuity, corrected, was 20/20-2 bilaterally. Pupils and extraocular movements were normal. Strength was normal throughout. The tone was slightly spastic to the left arm and right leg. Reflexes were normal except for bilateral absent ankle jerks. Sensory examination revealed a stocking pattern of pinprick and temperature sensation loss in both feet below the ankle. Vibration and proprioception thresholds were slightly above expected for age at the great toes bilaterally. No dysmetria was present. Gait was narrow-based but slightly staggering; there was no magnetic gait. Tandem gait could not be performed without assistance. Romberg’s test was slightly positive. No other frontal lobe release signs could be elicited.
Blood tests revealed a random glucose of 12 mmol/L, and hemoglobin A1C was elevated at 7.4%. Nerve conduction studies identified mild axonal sensory-dominant peripheral neuropathy. MRI of the brain identified numerous white matter abnormalities throughout subcortical regions, along with mild diffuse cerebral atrophy.
A diagnosis of white matter abnormalities with mild cognitive impairment was made, along with a secondary diagnosis of mild diabetic peripheral neuropathy. Diabetic education was provided. Physical therapy and a walker were recommended for gait difficulties. One year later, worsening mobility led to a fall that caused an epidural hematoma and death.
|
• There is a genetic influence in the appearance of white matter abnormalities. | |
|
• Several mechanisms contribute to the etiology of white matter abnormalities: breakdown of the blood-brain barrier, circulating metabolites, impaired metabolite clearance, and decreased cerebral perfusion. | |
|
• Pathology studies reveal loss of axons, myelin, and oligodendrocytes. Thickened blood vessel walls, gliosis, increased interstitial fluid, and edema also occur. |
Circulating metabolites. Circulating metabolites of both lipid and nonlipid nature, measured by mass spectrometry and high-performance liquid chromatography, correlate with white matter abnormalities in middle-aged and older adults. Hydroxyphenylpyruvate, the most common of these metabolites, explains up to 6% and 14% of the variance in white matter abnormality volume in the pooled sample and in men as compared to hypertension (1%), type 2 diabetes (1% to 3%), or smoking (less than 0.1%). This metabolite is a potentially useful biomarker for white matter abnormalities. In women, glucuronate was the only significantly associated metabolite with white matter abnormalities (147).
Blood-brain barrier disruption. The integrity of the blood-brain barrier may play a role in the etiology of white matter abnormalities, lacunar stroke, and dementia. Endothelial dysfunction allows leakage of serum components into the surrounding tissue, leading to neuronal and glial damage. This dysfunction may be intermittent or chronic, or it may occur during a hypertensive crisis (172).
Impaired metabolism waste clearance. Clearing the cerebral metabolic waste products, including beta-amyloid, alpha-synuclein, and tau protein, occurs in part through the cerebral spinal fluid via the perivascular spaces created by the astrocytic vascular endfeet. The function of this glymphatic system is increased during nonrapid eye movement sleep (180). The number of perivascular spaces increases with age, hypertension, small vessel disease, amyloid angiopathy, CADASIL, and Alzheimer disease. Uncontrolled hypertension disrupts the CSF flow and leads to amyloid deposition in the perivascular spaces. Increased visibility of perivascular spaces may also be associated with white matter abnormality formation around them (135).
Decreased cerebral perfusion. The severity of white matter abnormalities is associated with endothelial dysfunction. This is reflected by decreased neurovascular coupling, impaired autoregulation, and diminished perfusion of the subcortical white matter (92; 01; 164). The resulting poor collateral recruitment during stroke caused by a large vessel occlusion may explain the worse outcome after mechanical thrombectomy (100; 114).
Neuropathology. Vascular etiology was present in all types of white matter abnormalities but not in the periventricular capping and the smooth halo (21; 35; 53). Pathological evaluation reveals areas of spongiosis and extracellular space expansion due to loss of axons, myelinated fibers, and oligodendrocytes. Myelin thinning and gliosis are often accompanied by small-vessel atherosclerosis and lacunar infarctions (small cavities). However, not all white matter abnormalities seen on MRI are visible at autopsy (52; 63). The periventricular and patchy deep white matter abnormalities have a different microscopic appearance.
Periventricular capping and leukoaraiosis result from the patchy loss of the ependymal cell layer, fibrosis of small vessels and reactive gliosis, and increased extracellular fluid content, resulting in periependymal edema, axonal atrophy, and decreased myelin (154; 98). However, the myelin rarefaction is not true demyelination, as the process also involves axonal destruction (06; 105).
In the punctate deep white matter abnormalities, thickening of small vessels, perivascular gliosis, and dilated perivascular spaces were noted (163; 173). Transient repeated events of local hypoperfusion may induce an incomplete form of infarction (129). Confluent white matter abnormalities indicate more extensive ischemic damage (54).
Enlarged perivascular spaces may appear in the periventricular region and be confused with lacunar infarcts (83; 63). However, small perivascular spaces are found in all age groups, including newborns, suggesting they may not represent a true abnormality (154).
Noninflammatory collagenous thickening of periventricular veins resulting in severe stenosis was found in 65% of brain autopsies in elderly patients (116).
Subcortical white matter abnormalities disrupt the short corticocortical and long periventricular association fibers connecting distant cortical areas. The neuronal network disruptions lead to memory, executive, gait, and balance dysfunctions (112; 177; 38; 68; 174; 168).
Genetics may explain up to half the variation in white matter abnormalities between individuals (04). The genetic influence explains about two thirds of the variability in cognitive functioning; neurologic covariation in the presence of white matter abnormalities and cognition could be explained by genetic effect in more than 70% of cases (32).
A matched co-twin analysis of elderly monozygotic twins revealed that white matter abnormalities correlate with glucose level, high-density lipoprotein cholesterol, and systolic blood pressure. Additional correlations include decreased cognitive and physical abilities (33).
Co-occurrence of cerebrovascular disease and ApoE ε4 subtype has a synergistic effect on brain atrophy and white matter abnormalities (44). Both dizygotic and monozygotic male twins may have a higher vulnerability of ApoE ε4 carriers to injury or impaired repair (31).
Through genome-wide association studies, the rs12204590 stroke risk allele (on chromosome 6p25, near FOXF2) was associated with an increased MRI-defined burden of white matter abnormalities in stroke-free adults. Young patients (aged 2 to 32 years) with segmental deletions of FOXF2 showed an extensive burden of white matter abnormalities (121).
In the Multi‐Ethnic Study of Atherosclerosis, after adjustment for cardiovascular risk factors and socioeconomic status, white matter abnormalities were not associated with race and ethnicity (05).
Aging is an independent risk factor for the development of white matter abnormalities (06; 58; 57; 106; 183; 24; 48).
Cardiovascular risk factors. Hypertension, hypotension, orthostatic hypotension, and heart failure have been linked to white matter abnormalities (06; 133). History of atrial fibrillation, stroke, myocardial infarction, and laboratory findings like factor VIIc activity and fibrinogen level were also associated with white matter abnormalities (25; 48; 40).
Hypertension. White matter abnormalities are associated with a personal or family history of hypertension (06; 57; 17; 162; 136). Blood pressure control prevents the formation of new lesions (47).
Diabetes mellitus. Elevated glycated hemoglobin levels and diabetes mellitus have been associated with white matter abnormalities (143; 48; 119).
Additional cardiovascular risk factors for white matter abnormalities include smoking, obstructive sleep apnea, and renal dysfunction (88; 89; 101).
Migraine. Migraineurs have a high incidence of white matter abnormalities, 46% in one study (148). These abnormalities occur mostly in young patients (127). White matter abnormalities are usually seen in the periventricular white matter or near grey-white matter junctional areas and may be reversible (137; 107). No microstructural changes were detected on diffusion tensor imaging between episodic and chronic migraine (120).
Dementia. CT demonstrates lesions in 19% to 78% of patients with dementia, whereas brain MRI shows lesions in 7.5% to 100% (49; 18; 175; 92; 14; 46; 109; 104).
In Alzheimer disease, white matter abnormalities have been associated with advanced age, vascular risk factors, cerebral congophilic angiopathy, and homocysteine levels (80; 142; 78; 30). The members of an Irish family with familial Alzheimer disease due to an E280G mutation in exon 8 of presenilin-1 have developed spasticity along with white matter abnormalities (126).
White matter abnormalities may also occur in patients with Lewy body disease and patients with vascular dementia have higher numbers of white matter abnormalities than those with either Lewy body disease or Alzheimer disease (09).
Apolipoprotein E (Apo E) ε4. An association between the carriers of ApoE ε4, hypertension, and white matter hyperintensities was suggested by a study of 971 participants in the Rotterdam Scan Study (41). However, in another study, the association was no longer found after controlling for age and hypertension (77). Moreover, a meta-analysis including 16,738 adult subjects found no such association (152).
AIDS dementia. Patients with AIDS dementia complex can have associated cerebral atrophy and white matter abnormalities in the splenium and deep subcortical areas (26).
Psychiatric disorders. Although methodological problems were found in many studies, white matter abnormalities have been associated with depression, bipolar disease, late-onset mania, and late-onset schizophrenia (23; 36; 153; 108; 07; 76; 79; 67).
CADASIL. Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) is characterized by white matter abnormalities caused by multiple subcortical infarcts. The patients also suffer from migraine, mood disturbances, recurrent strokes, progressive subcortical dementia, and premature death. Pathological examination reveals multiple small, deep strokes. Concentric thickening of tunica media due to granular eosinophilic infiltration was seen in the small arteries. The genetic defect is on chromosome 19q12 (11; 155; 64). The white matter abnormalities progress with age and occur more often in the insula, temporal lobes, external capsule, and corpus callosum. The brainstem can also be Involved, most frequently the pons (34; 128).
CARASIL. Cerebral autosomal recessive arteriopathy with subcortical infarcts and leukoencephalopathy (CARASIL), like CADASIL, is associated with multiple subcortical infarctions due to a mutation in the HTRA1 gene. This prevents effective regulation of TGF-beta signaling and causes abnormal angiogenesis. Symptoms typically begin in the third or fourth decade and are characterized by leg spasticity and gait ataxia. About half of patients suffer from a stroke before 40 years of age. Dementia and memory loss typically occur within 20 years of onset. Scalp alopecia and attacks of low back pain are characteristic of the disease (74).
Susac syndrome. This small artery vasculopathy is characterized by recurrent flares of encephalopathy, retinopathy, and hearing loss (62; 182).
Trauma. Brain trauma may result in white matter abnormalities and abnormal perfusion on SPECT scan 6 months after injury. Abnormal perfusion to the frontal or temporal lobes is associated with worse outcomes 2 years after the event (169).
Electrical injury. Electrocution can result in brain atrophy and supratentorial white matter abnormalities (113). The acute effects include amnesia, seizures, or coma. The delayed complications include choreoathetosis, cerebellar ataxia, and parkinsonism. MRI may demonstrate acute subcortical white matter and basal ganglia lesions that may persist for several weeks, as well as cerebellar and cerebral atrophy (84).
Metabolic disorders.
Wilson disease. Also known as hepatolenticular degeneration, this is an autosomal recessive disorder of copper metabolism. MRI is characterized by increased T2 signal within the putamen and caudate, thalamus, dentate nuclei, midbrain, and subcortical white matter (131).
Hallervorden-Spatz disease. This progressive movement disorder is associated with abnormal iron deposition in the globus pallidus, substantia nigra, and red nucleus. MRI may reveal a decreased T2 signal in the lentiform nuclei and the surrounding white matter but an increased T2 signal within the periventricular white matter (55).
Neuroacanthocytosis. This uncommon neurodegenerative disorder is characterized by movement disorders, dementia, and acanthocytosis (abnormal, spiculated, or star-shaped red blood cells). T2-weighted MRI may identify regions with increased signal within the white matter of the periventricular regions and corpus callosum (122).
Dystonia. Dystonia has not been associated with traditional MRI changes, but diffusion tensor imaging may detect subcortical white matter asymmetry in dystonia patients (15).
Fragile X-associated tremor and ataxia syndrome. FXTAS is an adult-onset neurodegenerative disorder mainly seen in carriers, usually males, of premutation alleles (55 to 200 CGG repeats) of the fragile X mental retardation 1 (FMR1) gene. The neuropathological hallmark of FXTAS is an intranuclear inclusion found in neurons and astrocytes throughout the CNS (66). FXTAS may present with progressive intention tremor and gait ataxia. Brain MRI demonstrates white matter abnormalities within the cerebral and cerebellar locations (65).
Pediatric diseases.
Cerebral palsy. Children with cerebral palsy have frequent white matter abnormalities. Eighty-eight percent of these children have abnormal findings on MRI. Although focal infarcts are identified in 7% of children with cerebral palsy, periventricular leukomalacia is identified in 43% of children. Lesions within the basal ganglia and cortical or subcortical regions are commonly seen (12). The location of the white matter lesions in diplegic patients was posterior dominant, whereas patients with quadriplegia had evidence of diffuse white matter changes (12).
Leukodystrophies. Several disorders with childhood onset lead to white matter hyperintensities formation. Although similar to the white matter abnormalities in adults, their nature differs. Additionally, the grey matter and peripheral nervous system may be affected. These genetic disorders lead to the accumulation of abnormal metabolites that disrupt the myelin.
Adrenoleukodystrophy. Adrenoleukodystrophy is a peroxisomal disorder causing the accumulation of very long-chain fatty acids. It is both a demyelinating and dysmyelinating disorder. Over time, the initial lesions of the parietal and occipital lobes progress towards the frontotemporal regions. In advanced disease, the internal capsule, corpus callosum, corticospinal tracts, and other white matter fiber tracts in the brainstem can be involved. The lesions tend to be contiguous within fiber tracts and confluent within the white matter regions. Typically, the white matter abnormalities are large and symmetric (94).
Krabbe disease. Krabbe disease (globoid cell leukodystrophy) is an autosomal recessive disorder that presents shortly after birth and progresses rapidly. The galactocerebroside beta-galactosidase deficiency leads to abnormal production and maintenance of myelin. MRI reveals bilateral, confluent white matter abnormalities within the cerebrum and cerebellum (45).
Metachromatic leukodystrophy. Metachromatic leukodystrophy is an autosomal recessive lysosomal disorder caused by a deficiency of arylsulfatase A. This dysmyelinating disorder affects the thalamus, posterior limb of the internal capsule, cerebellum, and quadrigeminal plate (90).
Other leukodystrophies include Alexander disease, Canavan disease, Pelizaeus-Merzbacher disease, Cockayne syndrome, Hurler disease, and Lowe syndrome.
Mitochondrial diseases. These disorders of mitochondria metabolism may present with white matter abnormalities.
Leigh disease. Leigh disease (subacute necrotizing encephalomyelopathy) is an autosomal recessive disorder with childhood onset. T2 MRI may reveal symmetric areas of increased signal within the basal ganglia, brainstem, and cerebellum (111).
Kearns-Sayre syndrome. Kearns-Sayre syndrome in children may appear as T2 hyperintensities of the basal ganglia and brainstem (158).
Mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS). MELAS causes metabolic ischemia and infarcts within the subcortical white matter that do not correspond to vascular territories (158).
Combined complex I and IV deficiency. Combined complex I and IV deficiency in children leads to extensive white matter abnormalities (158; 42).
Pyridoxine deficiency. Pyridoxine deficiency should be suspected in infants with epilepsy and frontal or occipital white matter lesions (82).
Cytomegalovirus. Cytomegalovirus infection can present with white matter abnormalities on MRI, including multifocal lesions within deep parietal white matter (160).
Myotonic dystrophy. Most patients with type 1 or 2 myotonic dystrophy exhibit white matter abnormalities or cerebral atrophy. In type 1, intellectual dysfunction is associated with white matter abnormalities in the anterior temporal lobe (93).
|
• Up to 80% of elderly individuals have white matter abnormalities. | |
|
• The burden of white matter abnormalities increases with age. | |
|
• Cerebrovascular risk factors and disease increase the risk of white matter abnormalities. | |
|
• African Americans have a lower burden of white matter abnormalities than European Americans. |
White matter abnormalities are detected by CT and MRI in asymptomatic subjects as well as in individuals with cognitive impairment and vascular dementia (49; 151; 51; 75; 19; 102; 157; 133; 145). The proportion of subcortical and periventricular white matter abnormalities increases by 0.2% and 0.4% per year, respectively. Nearly all patients 80 to 90 years of age exhibit subcortical and periventricular white matter abnormalities on brain MRI. There was no significant difference between men and women (39; 179). African Americans had a lower prevalence of white matter abnormalities but a higher proportion of more severe lesions than European Americans. White matter abnormalities were significantly associated with smoking, lower education, systolic blood, and pulse pressure (99).
|
• Control of the cerebrovascular risk factors seems reasonable to prevent white matter abnormalities. | |
|
• Intensive blood pressure control is more effective than standard blood pressure control at delaying an increase in white matter abnormality burden. | |
|
• Angiotensin-converting enzyme inhibitors were associated with the best prevention of white matter abnormality progression. | |
|
• Statin use may reduce the risk of dementia, but the effect on white matter abnormalities and intracerebral hemorrhage is unclear. | |
|
• There is no evidence for using antiplatelet medication for white matter abnormality prevention. |
As white matter abnormalities share the risk factors with cerebrovascular disease, it is reasonable to assume that prevention should involve control of vascular risk factors, such as diabetes, hyperlipidemia, or hypertension. However, the benefit of various measures should be weighed against the potential side effects.
Dietary measures do not seem to prevent the development of white matter abnormalities or cognitive decline (10).
Control of hypertension reduces the burden of white matter abnormalities (161). In an observational cohort analysis of the SPRINT-MIND trial (Systolic Blood Pressure Trial Memory and Cognition in Decreased Hypertension), which included 448 individuals, angiotensin-converting enzyme inhibitors were associated with the best prevention of white matter abnormality progression over 4 years. This effect was independent of blood pressure control or age (60). On the other hand, intensive blood pressure treatment (systolic blood pressure lower than 120 mm Hg), compared with standard therapy (systolic blood pressure lower than 140 mmHg), was associated with a slower increase of white matter abnormalities (134). The beneficial effects of blood pressure control should be balanced against the increased risk of brain volume loss, syncope, and renal dysfunction (149).
In a study of 73 healthy adults with normal cognitive function, simvastatin helped preserve the white matter volume but did not influence the white matter hyperintensities at 18 months (170). In a retrospective case-control study, there was a negative association between statin dose and the risk of dementia (185). However, statin use in elderly patients was associated with either prevention or progression of white matter abnormalities (69; 61). Of additional concern is the increased risk of intracerebral hemorrhage with intensive cholesterol reduction (138). However, statin use before intracerebral hemorrhage does not adversely influence the outcome (97).
Antiplatelets are used for secondary stroke prevention. It is unclear if antiplatelets prevent dementia in patients with white matter abnormalities, but there may be an increased risk for hemorrhagic complications (95).
Lacunar stroke appears on T2 MRI as a white matter hyperintensity surrounding a small cavity. However, approximately 20% of recent small subcortical strokes lack this cavitation (130). The fluid-containing spaces, including cystic infarction and brain cysts, appear as isointense relative to CSF (22). However, the FLAIR sequence may not distinguish white matter abnormalities from lacunes or perivascular spaces (117). Moreover, approximately 50% of enlarged spaces are surrounded by a FLAIR hyperintensity reflecting perivascular spaces, gliosis, or both (29). The frontal lobes are more affected by subcortical small vessel ischemia. Regardless of location, white matter abnormalities are associated with hypometabolism of the frontal lobes and executive dysfunction (156).
Demyelinating lesions seen in multiple sclerosis and Sjögren disease represent the most common differential diagnosis for white matter abnormalities (118). MRI cannot distinguish noncystic infarction from gliosis or demyelination (22). Diagnosis of multiple sclerosis relies on two or more central nervous system white matter lesions, called plaques, separated in time and space, not caused by another condition. Most early acute plaques are hyperintense with a hypointense ring on T2-weighted MRI and may be enhanced with gadolinium. Typically, the plaques are ovoid, larger than 5 mm, and end abruptly at the junction with the gray matter. They are found in the periventricular region, corpus callosum, and the cerebellar peduncles. Late active plaques are hyperintense on T2-MRI and often appear hypointense on T1-MRI (124; 27).
|
• Brain CT identifies white matter lesions as hypodensities. | |
|
• MRI is more sensitive in detecting white matter abnormalities than CT. | |
|
• MRI can better differentiate white matter abnormalities from lacunes and enlarged perivascular spaces. |
Due to the unknown significance of the periventricular and subcortical areas of hypodensity on CT or hyperintensity on T2-weighted MRI, the term leukoaraiosis was coined from the Greek leuko [white] and araiosis [rarefaction] (72; 73). MRI can detect leukoaraiosis earlier than CT (70).
White matter abnormalities help differentiate vascular dementia from Alzheimer disease, although they can coexist (49). In patients with vascular dementia, white matter abnormalities are more visible in those with basal ganglia, thalamus, or thromboembolic infarctions and confluent, irregular periventricular white matter disease. In Alzheimer disease, the lesions are more confined to the uncal-hippocampal and insular cortex (143; 171).
A visual rating scale possibly useful in quantifying white matter abnormalities in patients with cognitive decline is the Cholinergic Pathways HyperIntensities Scale, which identifies white matter abnormalities within the well-identified cholinergic pathways (16).
|
• White matter disease and cerebrovascular disease share the same risk factors. | |
|
• There is no treatment for the white matter abnormalities. | |
|
• The risks and benefits of controlling the risk factors should be carefully weighed. |
Because white matter abnormalities share risk factors, such as diabetes, hyperlipidemia, and hypertension, with cerebrovascular disease, it is reasonable to control them. However, the side effects of any intervention should be considered.
In an observational study, statins slowed the progression of white matter hyperintensities and dementia (181). However, a meta-analysis of two clinical trials that enrolled 26,340 participants found that statin did not prevent cognitive decline or dementia (110). More recently, in a randomized controlled trial, low-dose rosuvastatin reduced the risk of new white matter hyperintensities and cognitive impairment, but telmisartan did not (184).
In patients with vascular dementia, the cholinergic deficits due to basal forebrain ischemia can be slightly improved with donepezil, galantamine, and rivastigmine (50).
Visual and auditory gamma-sensory stimulation is a noninvasive way of decreasing white matter atrophy and myelin loss, especially in the entorhinal region, which is still in the experimental phase (37). Physical therapy and assistive devices, such as canes or walkers, are indicated for gait difficulty and imbalance.
Progression of white matter hyperintensities is associated with an increased risk of cognitive and gait decline. Aside from risk factor modification, there is no specific treatment. Because of the heterogeneous nature of the disorder, treatment should be tailored to the individual’s needs to limit the risks of treatment-related complications, such as excessive reduction in cerebral perfusion in those with poor cerebral perfusion as a mechanism.
No specific precautions are known in women with white matter disease who become pregnant.
Avoidance of excessive fluctuations in blood pressure during surgery is reasonable. Severe hypotension or hypertension can contribute to neuronal injury in patients with impaired cerebral microcirculation.
All contributors' financial relationships have been reviewed and mitigated to ensure that this and every other article is free from commercial bias.
Adrian Marchidann MD
Dr. Marchidann of Kings County Hospital has no relevant financial relationships to disclose.
See Profile
Steven R Levine MD
Dr. Levine of the SUNY Health Science Center at Brooklyn has no relevant financial relationships to disclose.
See ProfileNearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Stroke & Vascular Disorders
Dec. 29, 2024
Neurogenetic Disorders
Dec. 26, 2024
Neurogenetic Disorders
Dec. 23, 2024
Neurogenetic Disorders
Dec. 23, 2024
Sleep Disorders
Dec. 15, 2024
Neurogenetic Disorders
Dec. 13, 2024
Neurogenetic Disorders
Dec. 02, 2024
Neurogenetic Disorders
Nov. 27, 2024