Acid sphingomyelinase deficiency
Dec. 13, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
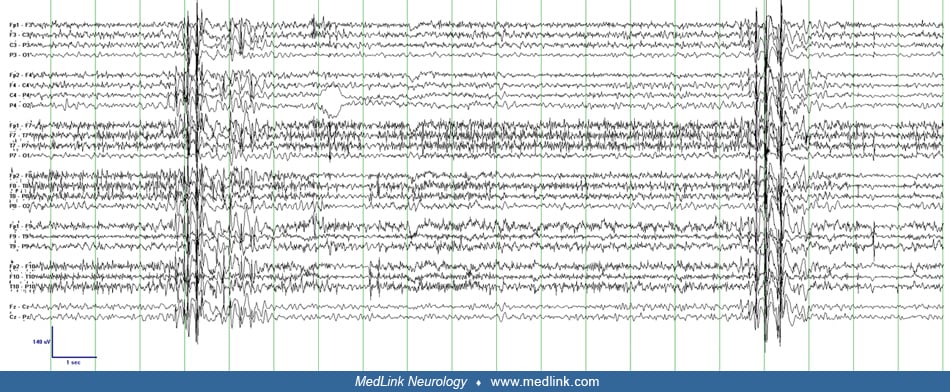
This 86-year-old woman with a history of atrial fibrillation suffered a cardiac arrest of unclear etiology and duration. On examination 18 hours after resuscitation, the patient was in coma with intact brainstem reflexes. She demonstrated frequent rhythmic movements of her facial muscles, including eyelid twitching tongue and jaw protrusion. EEG background is diffusely slow. Myoclonic movements recur every 3 to 5 seconds corresponding to 4 to 7 Hz centrally predominant, generalized spike-wave activity lasting 3 to 5 seconds. The movements did not respond to levetiracetam but abated to some degree with benzodiazepines. Epileptiform discharges and myoclonus resolved within 72 hours. SSEPs performed 3 weeks after resuscitation demonstrated intact cortical responses. The patient died 6 weeks after presentation due to a combination of progressive neurologic decline and renal failure. (Video-EEG courtesy of Dr. Sara Inati.)