General Neurology
Fever: neurologic causes and complications
Jul. 06, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
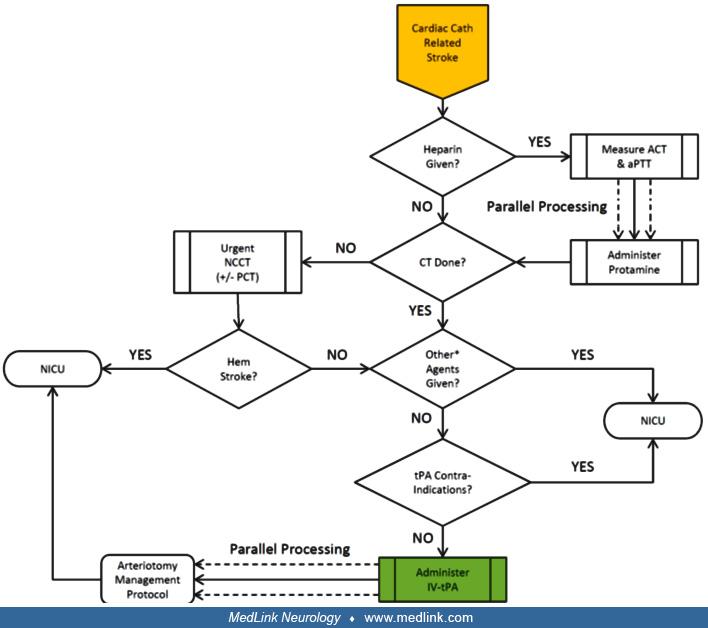
The most efficient workflow for the management of patients with suspected “off-the-table” stroke is illustrated. The recognition of acute neurologic changes typically occurs after the cardiac index procedure has been concluded and the patient is in the recovery area or the coronary care unit shortly thereafter. On recognition of acute neurologic changes, if the patient is not back at his or her baseline following the administration of sedation reversing drugs, the next step is to acquire urgent imaging of the brain and its vasculature by means of non-contrast CT and CTA studies. In addition, some recommend adding perfusion CT studies to the urgent imaging protocol. If the urgent CT imaging demonstrates a hemorrhagic stroke, the patient should be immediately transferred to the neurointensive care unit for further care per clinical practice guidelines. Conversely, if the CTA demonstrates a large arterial occlusion, the patient should be immediately transferred back to the catheterization suite for urgent thrombectomy. CTA = computed tomography angiogram; IV-tPA = intravenous tissue plasminogen activator; LAO = large arterial occlusion; NCCT = non-contrast computed tomography; NICU = neurointensive care unit; PCT = perfusion computed tomography. (Contributed by Dr. Jose Biller.)